

 下载:
下载:




-
Monkeypox virus was first identified in captive monkeys in 1958, and in a child from the Democratic Republic of the Congo (DR of the Congo) in 1970[1]. Human monkeypox, a sporadic zoonosis in rural rainforest villages of western and central Africa, is caused by two variants of orthopoxvirus, namely, the Central African clade (clade I) and the West African clade (clade II)[1, 2]. Human infections have been documented through the handling of infected monkeys, Gambian giant rats, and squirrels, with rodents being the most likely reservoir of the virus[3]. The symptoms of monkeypox include skin rashes, fever, intense headache, swelling of lymph nodes, back pain, muscle ache, and lack of energy[3]. Monkeypox spreads by close contact with an animal infected with monkeypox virus, and also by skin-to-skin contact, respiratory droplets, or oral fluids during intimate sexual contact, and contact with fabrics, objects, or surfaces contaminated with monkeypox virus to achieve human-to-human spread[4].
Prior to May 2022, human monkeypox was an epidemic in African countries[3], and it was only occasionally imported to non-epidemic countries, such as Singapore[5], the United States[6], and the United Kingdom (UK) by travelling to places with circulating monkeypox (endemic areas) or with exposure to infected animals[7]. However, at the beginning of May 2022, the UK informed the World Health Organization (WHO) about a confirmed case of monkeypox in an individual who returned from Nigeria to the UK; there were subsequently clusters of monkeypox virus infections in multiple non-epidemic countries[4, 8]. As of July 29, 2022, a total of 22,485 confirmed cases of monkeypox across 79 countries or territories were reported globally[9]. The International Health Regulations Emergency Committee officially announced that the monkeypox epidemic had constituted Public Health Emergency of International Concern (PHEIC) on July 23, 2022[10]. In order to prepare for prevention and control of the monkeypox epidemic in advance, the National Health Commission of People’s Republic of China issued the “Monkeypox Diagnosis and Treatment Guidelines (2022 Edition)” on June 10, 2022[11]. On July 24, the General Administration of Customs of the People’s Republic of China announced that in accordance with the “Frontier Health and Quarantine Law of the People’s Republic of China” and other regulations, it had formulated relevant prevention and control measures to prevent the importation of monkeypox and protect the health and safety of people[12].
Although up to now, there are no local monkeypox cases in Chinese mainland, with the deepening of trade exchanges between countries in the world and frequent personnel exchanges, China still faces the importation risk of monkeypox infection. Especially the under the implementation of China’s “Silk Road Economic Belt” and “21st Century Maritime Silk Road” initiative (hereinafter referred to as the “Belt and Road” Initiative), the construction of infrastructure such as strengthening the interconnection of international railways, highways, aviation, and waterways has promoted the increase personnel exchanges and its speed[13]. Therefore, we analyzed the global epidemic situation of monkeypox infection and applied the risk matrix method to assess the importation risk into China, so as to make targeted and detailed preparations for prevention in advance.
-
In our study, we extracted 2022 multiple-country monkeypox outbreak data of 79 countries on monkeypox confirmed cases from United States Centers for Disease Control and Prevention as of July 29, 2022[9]. The annual number of foreign students in China from the dataset “Chinese Concise Statistics of International Students 2018” in China was used to represent personnel flows to China from monkeypox infection outbreaking countries and assess the possibility importation risk in this study[14]. The specific number of monkeypox cases reported at July 29, 2022 and 2018 international students entering China was seen in Supplementary Table S1, available in www.besjournal.com.
Table S1. The number of monkeypox cases reported at July 29, 2022 and 2018 international students entering China
Region Number of country or territories (%, n/N) Country or territories (number of cases) Country or territories (number of 2018 international students entering China) African 10 (12.66%, 10/79) Democratic Republic of the Congo (163), Nigeria (133), Ghana (30), Central African Republic (8), Cameroon (7), South Africa (3)
Benin (3), Republic of the Congo (2), Morocco (1), Liberia (1)Nigeria (6,845), Ghana (6,475), South Africa (2,981), Morocco (2,612), Cameroon (2,535), Democratic Republic of the Congo (2,246), Republic of the Congo (2,173), Liberia (802), Benin (634), Central African Republic (188) American 18 (22.78%, 18/79) United States (4,906), Brazil (978), Canada (803), Peru (269), Mexico (59), Chile (45), Argentina (20), Colombia (12), Ecuador (3), Costa Rica (3), Dominican Republic (3), Jamaica (2), Panama (1), Venezuela (1), Bahamas (1), Barbados (1), Bermuda (1), Martinique (1) United States (20,996), Canada (4,322), Mexico (1,540), Brazil (1,463), Colombia (879), Panama (738), Venezuela (629), Jamaica (539), Ecuador (519), Peru (502), Argentina (499), Chile (347), Costa Rica (279), Dominican, Republic (173), Bahamas (173), Barbados (104), Bermuda (0), Martinique (0) Asian 14 (17.72%, 14/79) Israel (133), United Arab Emirates (16), Singapore (11), India (4). Lebanon (4), Saudi Arabia (3), Japan (2), Thailand (2), Qatar (2), Taiwan (province of China, 2), South Korea (1), Philippines (1), Turkey (1), Georgia (1) South Korea (50,600), Thailand (28,608), India (23,198), Japan (14,230), Singapore (4,718), Philippines (2,786), Turkey (1,854), Saudi Arabia (783), Israel (449), Georgia (301), Lebanon (193), United Arab Emirates (78), Qatar (13), Taiwan (province of China, -)* European 34 (43.04%, 34/79) Spain (4,298), Germany (2,595), United Kingdom (2,546), France (1,955), Netherlands (879), Portugal (633), Italy (479), Belgium (393), Switzerland (264), Austria (124), Sweden (88), Ireland (85), Denmark (81), Poland (59), Norway (51), Hungary (37), Slovenia (33), Greece (32). Luxembourg (28), Romania (21), Czechia (19), Finland (17), Malta (17), Croatia (12), Serbia (10), Iceland (9), Estonia (6), Slovakia (6), Gibraltar (5), Bulgaria (4), Andorra (3), Latvia (3), Russia (1), Bosnia and Herzegovina (1) Russia (19,239), France (10,695), Germany (8,079), United Kingdom (6,415), Italy (5,386)
Spain (2,650), Netherlands (2,393), Poland (1,926), Belgium (1,502), Denmark (1,122), Sweden (1,080), Switzerland (884), Norway (813), Ireland (717), Portugal (633), Czechia (611), Romania (594), Hungary (587), Finland (585), Austria (517), Bulgaria (429), Serbia (394), Slovakia (329), Greece (252), Bosnia and Herzegovina (193), Latvia (162), Slovenia (123), Croatia (118), Estonia (86), Luxembourg (37), Iceland (30), Malta (11), Andorra (3), Gibraltar (0)Oceania 3 (3.80%, 3/79) Australia (45), New Zealand (2), New Caledonia (1) Australia (4,058), New Zealand (767), New Caledonia (0) Note. We could not get the number of students entering Chinese mainland in 2018 from Taiwan (province of China). -
We described the epidemic situation of monkeypox infection using the total cases reported by USA CDC (Centers for Disease Control and Prevention) on July 29, 2022. Then, the history of monkeypox infection was defined as yes or no. There were 7 countries with the history of monkeypox infection including DR of the Congo, Nigeria, Ghana, Central African Republic, Cameroon, Republic of the Congo and Liberia based on reported data by USA CDC. Because specific clade data were not always reported in the literature, we used the geographical spread of the clades as described by the WHO[15, 16] to assign the clade variant. Monkeypox cases from the DR of the Congo, Gabon, Central African Republic, South Sudan, and Republic of the Congo were assumed to be of the clade I, while cases in all of the other countries were assumed to be of the clade II. Clade I historically caused more severe disease and was thought to be more transmissible and had higher case fatality rate.
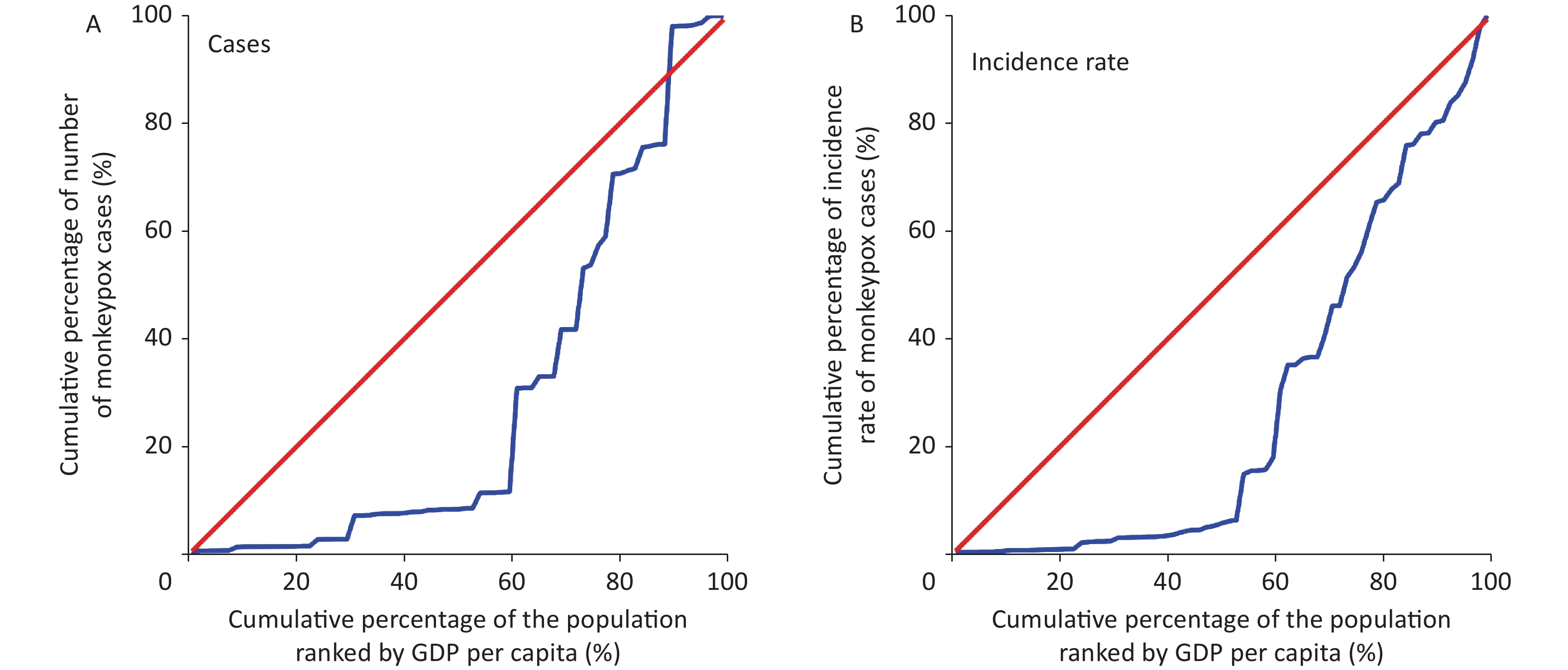
In addition, we assessed the economic-related inequality in monkeypox infection by calculating concentration index (C) and Lorenz curve[17, 18]. In this study, the distribution of infectious diseases was examined by GDP per capita in 2021. The Lorenz curve is obtained by plotting the cumulative percentage of cases (Y-axis) against the cumulative percentage of the population ranked by GDP per capita (X-axis). The C can be calculated using the following formula[19].
$$ {{C}}\;=\;\frac{2}{\mu\;\times\;cov\;(h,\;r)} $$ (1) where h refers to the health outcome,
$ \mu $ is the mean of h, and r denotes the fractional rank of individuals in the distribution used (economic status). The concentration index ranges between −1 and +1. A value of zero for concentration index represents absolute fairness and there exists no economic-related inequality. If the concentration index takes a negative value, indicating infectious diseases is more concentrated among poor people (pro-rich). Conversely, if concentration index is a positive value, it indicates that infectious diseases is more concentrated among rich people (pro-poor)[20]. We also extracted the number of 2021 population from world bank data (https://data.worldbank.org/indicator/SP.POP.TOTL ) to calculated the incidence rate per 100,000 population for sensitivity analysis of economic-related inequality. -
We applied the risk matrix method to assess the importation risk of monkeypox cases into China based on two dimensions of importation possibility and importation severity[21-23], with the risk assessment indicators and scores showed in Table 1. First, the score of importation possibility considered the number of 2018 international student’s number entering China and history of reported monkeypox. We derived the final importation possibility risk score and shown below in five levels: rare (2 points), unlikely (3 points), possible (4 points), very possible (5 points), inevitable (6 points). Second, the score of importation severity considered the number of total cases and the type of clades. We also classified the final importation severity risk score into five levels and as shown below: negligible (2 points), minor (3 points), moderate (4 points), serious (5 points), catastrophic (6 points). Finally, we divided the importation risk of monkeypox infection into four levels of low, moderate, high and extremely high, based on the levels of importation possibility and importation severity in the risk matrix assessment index table (Table 2).
Table 1. Risk assessment indicators of importation possibility and importation severity and their scores
Assessment indicators Factors Classification Risk scores Importation possibility The number of international students entering China in 2018 (number) < 500 1 500–1,000 2 1,001–5,000 3 5,001–10,000 4 > 10,000 5 History of reported monkeypox No 1 Yes 2 Importation severity The number of monkeypox cases < 10 1 10–50 2 51–100 3 101–1,000 4 > 1,000 5 The type of clades West African Clade 1 Central African clade 2 Note. Taiwan (province of China) was excluded in the risk estimation because we could not get the number of students entering Chinese mainland in 2018. Table 2. Risk matrix assessment index table
Importation
possibilityImportation severity Negligible Minor Moderate Serious Catastrophic Inevitable H H E E E Very possible M H H E E Possible L M H E E Unlikely L L M H E Rare L L M H H Note. L, low importation risk; M, moderate importation risk; H, high importation risk; E, extremely high importation risk. -
Borda count method was used to rank the importation risks of monkeypox infection. First, the Borda points of importation risks equaled to the sum of the ranks of importation possibility and importation severity risk levels. Then, we sorted Borda points of importation risks from the largest to the smallest and set the corresponding count as 0, 1..., N−1. The smaller Borda count was, the more possibility of importation risk of monkeypox infection into China, and the more serious the consequences would be. Borda points were calculated with the following formula [23, 24]:
$$ {b}_{i}=\sum _{k=1}^{m}(N-{r}_{ik}) $$ (2) N: the number of countries or territories was 78, respectively; m: risk assessment index of monkeypox infection, set the value as 2;
$ {r}_{ik} $ : levels of risk for indicator i under criterion k;$ {b}_{i} $ : Borda points of the assessment indicator i. -
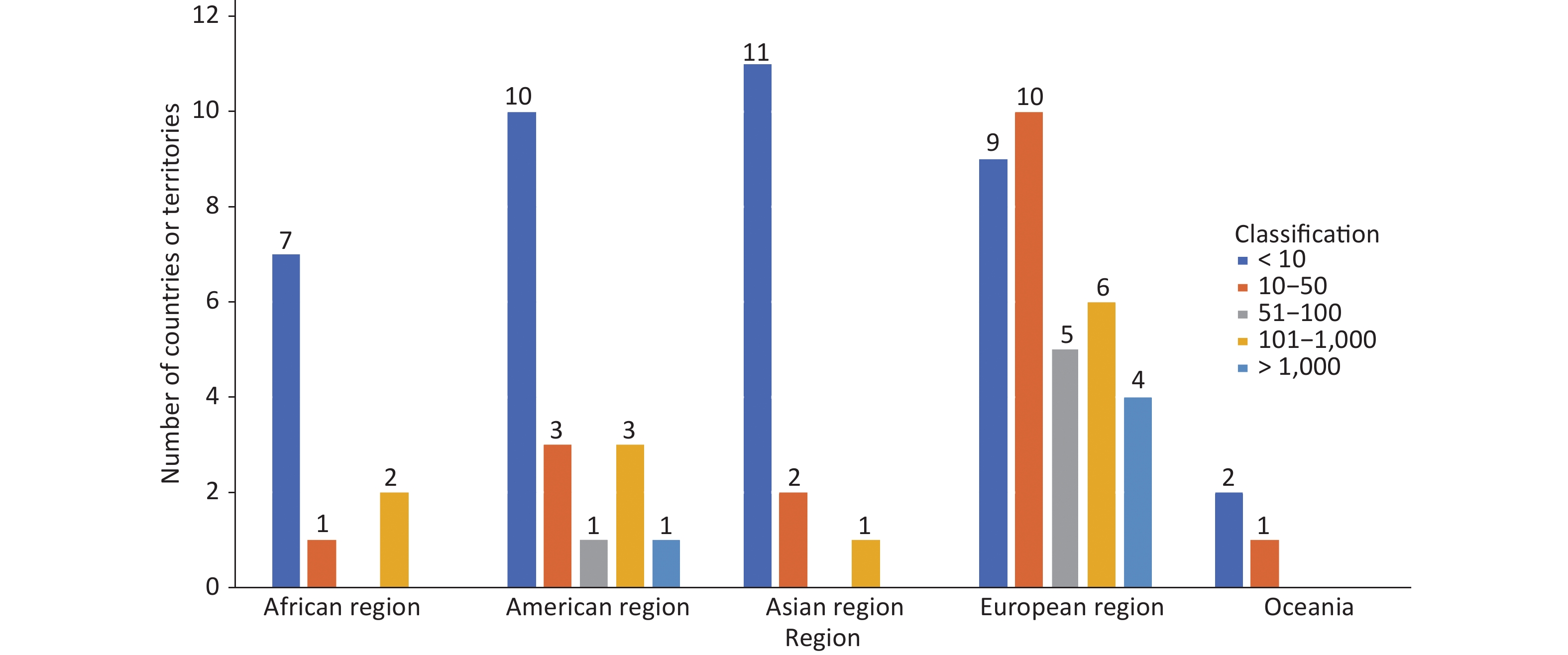
As July 29, 2022, there were 10 (12.66%, 10/79), 18 (22.78%, 18/79), 14 (17.72%, 14/79), 34 (43.04%, 34/79), 3 (3.80%, 3/79) countries or territories reported monkeypox cases in African region, American region, Asian region, European region and Oceania, respectively (Supplementary Table S1). The top three country or territories of number of monkeypox cases were United States (4,906), Spain (4,298) and Germany (2,595) (Supplementary Table S1). There were 39 (49.37%, 39/79), 17 (21.52%, 17/79), 6 (7.59%, 6/79), 12 (15.19%, 12/79), and 5 (6.33%, 5/79) with cases less than 10, 10−50, 51−100, 101−1,000, and more than 1,000, respectively. Of five country or territories with cases more than 1,000, four was in European region and one in American region (Figure 1).
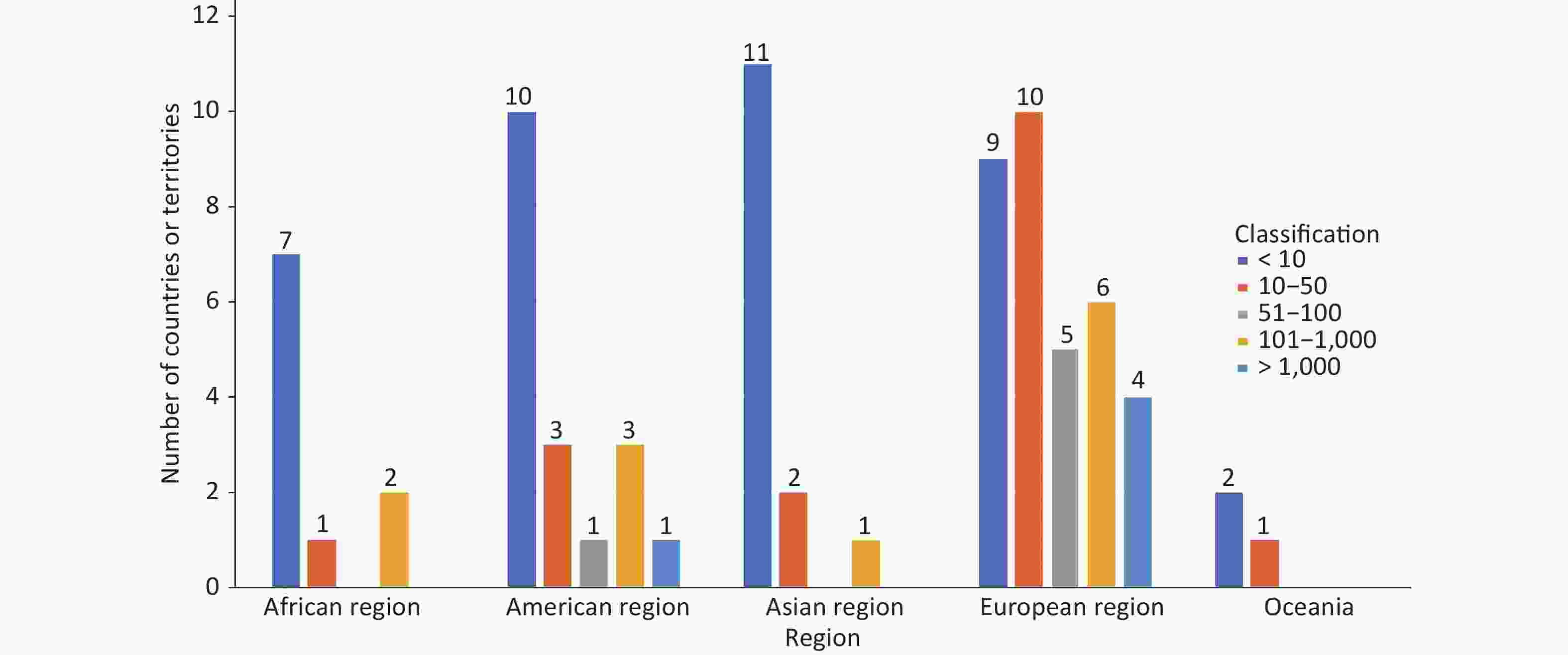
Figure 1. The distribution of monkeypox infection among different region.
The Lorenz curves of number of cases and incidence rate were shown in Figure 2. The curve of monkeypox infections (the concentration index = 0.42, P = 0.027, Figure 2A) and incidence rate (the concentration index = 0.46, P < 0.001, Figure 2B) both lay below the equality line, with the positive value which indicated that economic-related health disparities and the inequality disadvantageous to the rich (pro-poor) that these infectious diseases infection were more concentrated among population with higher economic status. Although the concentration indexes of number of cases and incidence rate were stable among different regions (all P > 0.05), the concentration index of both cases and incidence rate were negative value in African region (Figure 3).
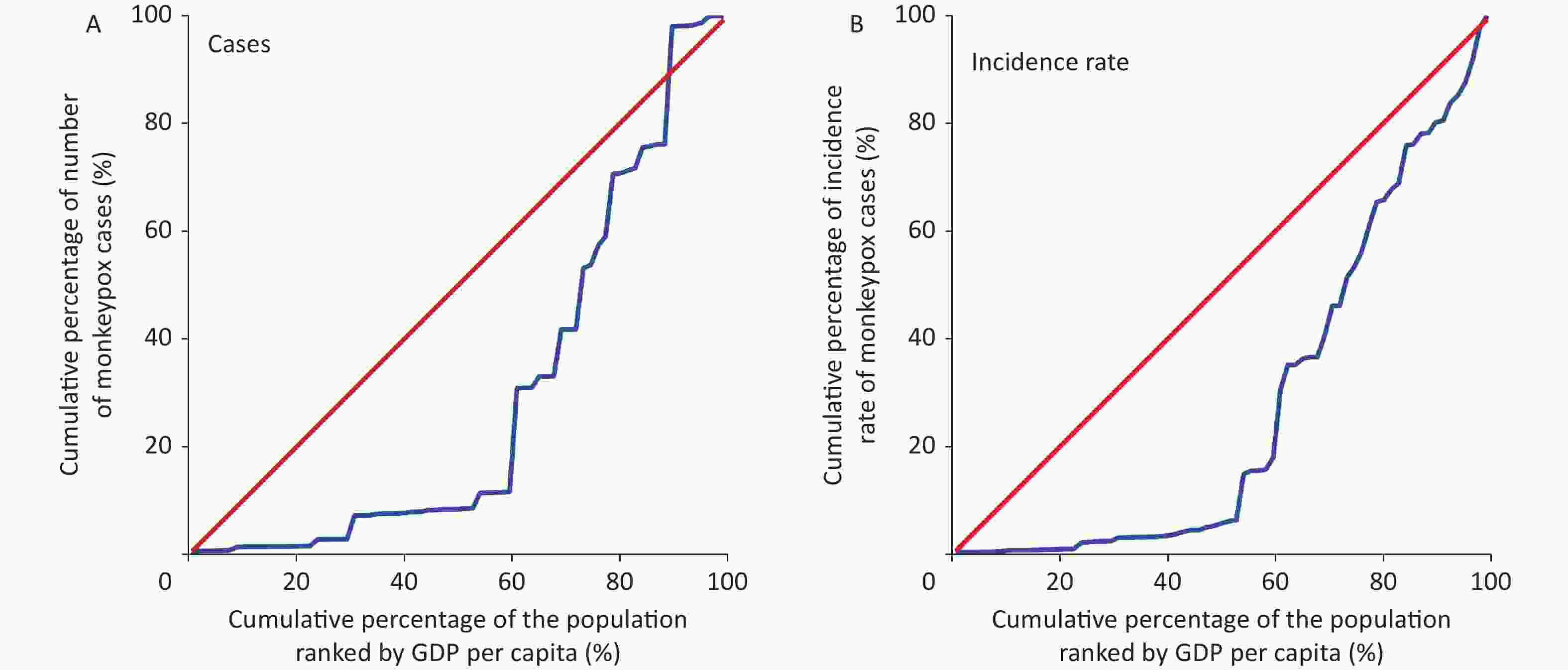
Figure 2. Lorenz curves of cases or incidence rate of monkeypox infection. Red line was the equality line; Blue line was the Lorenz curve. (A) Cases: the concentration index = 0.42, P = 0.027. (B) Incidence rate: the concentration index = 0.46, P < 0.001.
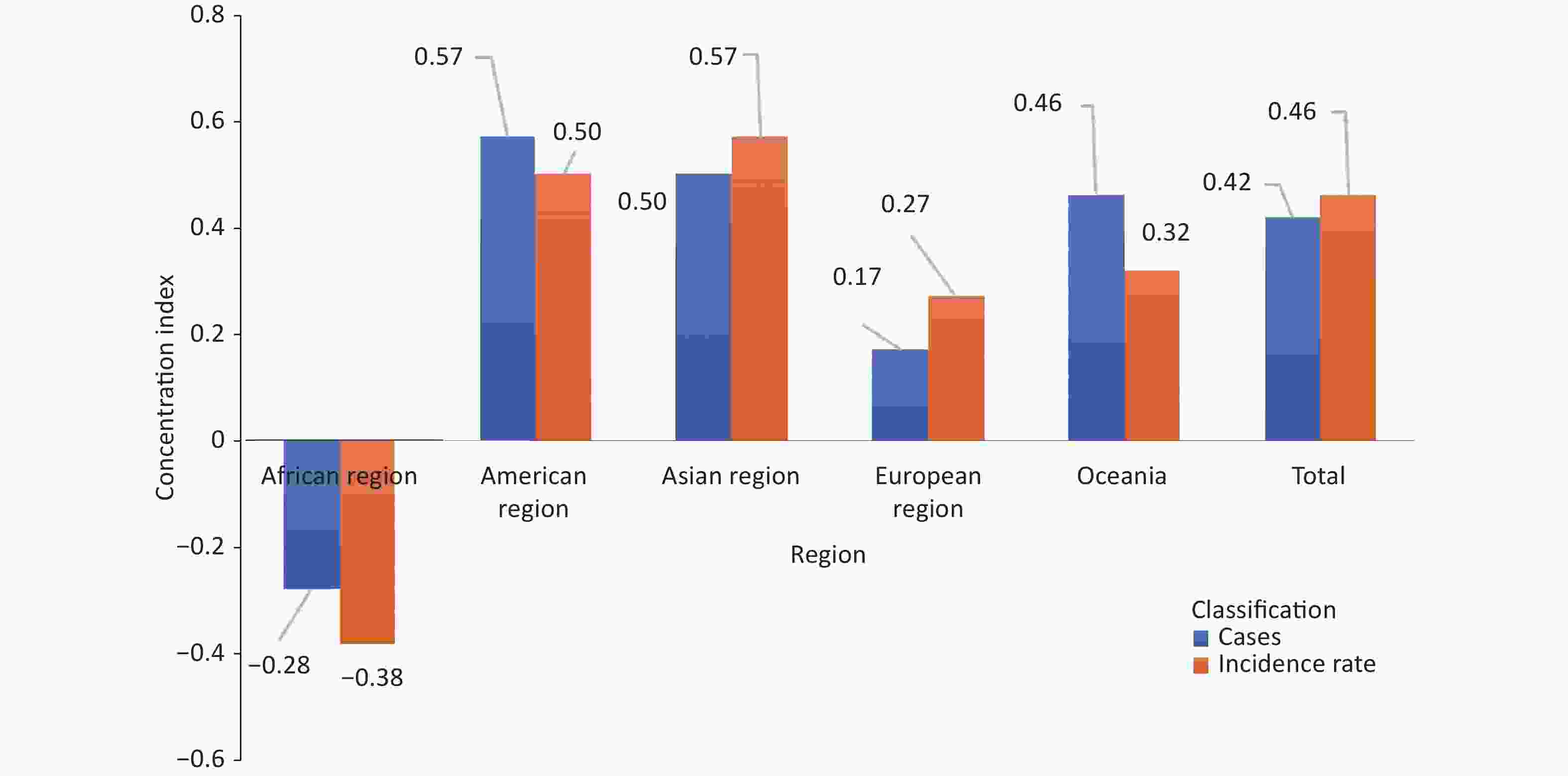
Figure 3. The concentration index on monkeypox infection among different region. The differences between regions both were not significant (all P > 0.05). Blue histogram means the concentration index was the monkeypox cases: African region, the concentration index = −0.28, P = 0.411; American region, the concentration index = 0.57, P = 0.157; Asian region, the concentration index = 0.50, P = 0.288; European region, the concentration index = 0.17, P = 0.456; Oceania, the concentration index = 0.46, P was missing because of observations < 2; Total: the concentration index = 0.42, P = 0.027. Orange histogram means the concentration index was the incidence rate of monkeypox: African region, the concentration index = −0.38, P = 0.036; American region, the concentration index = 0.50, P = 0.009; Asian region, the concentration index = 0.57, P = 0.219; European region, the concentration index = 0.27, P = 0.017; Oceania, the concentration index = 0.32, P was missing because of observations < 2; Total, the concentration index = 0.46, P < 0.0001.
-
China was under the risk of monkeypox importation. For importation possibility, the highest risk was from nine countries or territories (United States, South Korea, Thailand, etc.), with score of six, while the lowest risk was from 28 countries or territories (Argentina, Israel, Bulgaria etc.), with score of two. For importation severity, the highest risk was from six countries or territories (United States, France, Germany, etc.), with scores of six, while the lowest risk was from 36 countries or territories (South Korea, Thailand, India, etc.), with scores of two (Table 3).
Table 3. Importation risks from countries or territories with monkeypox infection to China in the 2022 multiple-country monkeypox outbreak
Countries or
territoriesThe score of importation severity The score of importation possibility Risk levels Borda points Borda count Risk sequence of importation United States 6 6 E 156 0 1 France 6 6 E 156 0 1 Nigeria 5 6 E 150 6 7 Germany 6 5 E 147 9 10 United Kingdom 6 5 E 147 9 10 Democratic Republic of the Congo 6 5 E 147 9 10 Italy 5 5 E 141 15 16 Spain 6 4 E 141 15 16 Canada 5 4 E 135 21 22 Netherlands 5 4 E 135 21 22 Belgium 5 4 E 135 21 22 Brazil 5 4 E 135 21 22 Ghana 3 6 H 133 23 24 Republic of the Congo 3 5 H 124 32 33 Poland 4 4 H 124 32 33 Mexico 4 4 H 124 32 33 Denmark 4 4 H 124 32 33 Switzerland 5 3 H 119 37 38 Portugal 5 3 H 119 37 38 Austria 5 3 H 119 37 38 Peru 5 3 H 119 37 38 South Korea 2 6 H 114 42 43 Thailand 2 6 H 114 42 43 India 2 6 H 114 42 43 Russia 2 6 H 114 42 43 Japan 2 6 H 114 42 43 Israel 5 2 H 100 56 57 Sweden 4 4 M 124 32 33 Singapore 3 4 M 118 38 39 Australia 3 4 M 118 38 39 Norway 4 3 M 108 48 49 Ireland 4 3 M 108 48 49 Cameroon 2 5 M 105 51 52 Colombia 3 3 L 102 54 55 Czechia 3 3 L 102 54 55 Romania 3 3 L 102 54 55 Hungary 3 3 L 102 54 55 Finland 3 3 L 102 54 55 Central African Republic 3 3 L 102 54 55 South Africa 2 4 L 99 57 58 Philippines 2 4 L 99 57 58 Morocco 2 4 L 99 57 58 Turkey 2 4 L 99 57 58 Liberia 2 4 L 99 57 58 Saudi Arabia 2 3 L 83 73 74 New Zealand 2 3 L 83 73 74 Panama 2 3 L 83 73 74 Benin 2 3 L 83 73 74 Venezuela 2 3 L 83 73 74 Jamaica 2 3 L 83 73 74 Ecuador 2 3 L 83 73 74 Argentina 3 2 L 83 73 74 Serbia 3 2 L 83 73 74 Chile 3 2 L 83 73 74 Greece 3 2 L 83 73 74 Slovenia 3 2 L 83 73 74 Croatia 3 2 L 83 73 74 United Arab Emirates 3 2 L 83 73 74 Luxembourg 3 2 L 83 73 74 Malta 3 2 L 83 73 74 Bulgaria 2 2 L 64 92 93 Slovakia 2 2 L 64 92 93 Georgia 2 2 L 64 92 93 Costa Rica 2 2 L 64 92 93 Lebanon 2 2 L 64 92 93 Bosnia and Herzegovina 2 2 L 64 92 93 Dominican Republic 2 2 L 64 92 93 Bahamas 2 2 L 64 92 93 Latvia 2 2 L 64 92 93 Barbados 2 2 L 64 92 93 Estonia 2 2 L 64 92 93 Iceland 2 2 L 64 92 93 Qatar 2 2 L 64 92 93 Andorra 2 2 L 64 92 93 Gibraltar 2 2 L 64 92 93 Bermuda 2 2 L 64 92 93 Martinique 2 2 L 64 92 93 New Caledonia 2 2 L 64 92 93 Note. Country names were ranked in descending order of the risk levels. L, low importation risk; M, moderate importation risk; H, high importation risk; E, extremely high importation risk; Taiwan (province of China) was excluded in the risk estimation because we could not get the number of students entering Chinese mainland in 2018. Comprehensively, an extremely high importation risk of monkeypox cases was from 12 (15.38%, 12/78) countries or territories including United States, France, Germany, Nigeria, UK, Italy, Canada, Spain, Netherlands, Democratic Republic of the Congo, Belgium and Brazil (Table 3). There were 15 (19.23%, 15/78), 6 (7.69%, 6/78) and 45 (57.69%, 45/78) countries or territories with high, moderate and low importation risk, respectively (Table 3).
United States and France had the highest Borda points of 156, and their counts were zero, ranking first (Table 3).
-
Our study described the global epidemic of the 2022 multiple-country monkeypox outbreak and calculated concentration index to measure economic-related inequality for monkeypox infection. Our results showed that as of July 29, 2022, there were 79 countries or territories reported monkeypox cases, which of them, European region had the most countries or territories (43.04%, 34/79). There were 39, 17, 6, 12, and 5 country or territories with cases less than 10, 10−50, 51−100, 101−1,000, and more than 1,000, respectively. Of five country or territories with cases more than 1,000, four was in European region and one in American region. The top country of number of monkeypox cases was United States (4,906). There was economic-related health disparity in the distribution of monkeypox cases, and the inequality disadvantageous to the rich (pro-poor), while it conversed in African region. We further assessed its importation risk into China by using risk matrix method and Borda count method. This study found that importation risk into China varies across disease-outbreaking countries, there 12, 15, 6, and 45 countries or territories with extremely high, high, moderate and low importation risk, respectively. United States and France ranked first with the highest Borda points of 156, and counts of zero. To our knowledge, this was the first study that applied risk assessment matrix method to assess the importation risk of monkeypox infection into China with two dimensions of the possibility and severity. Our findings were beneficial to distinguish levels of risk and identify countries with high importation risk rapidly.
In the 2022 multiple-country monkeypox outbreak, European region had the highest infection burden than other four regions. Additionally, United States also faced the greatest monkeypox infections among 79 countries or territories. Before May 2022, Monkeypox virus infection mainly occurred in the Central and West African regions. The 2003 monkeypox outbreak in the United States marked the first reported human monkeypox cases outside Africa, with 47 confirmed and probable monkeypox cases, all closely associated with groundhogs imported from Ghana[25, 26]. Except for history of contact with animals, for non-epidemic countries including the UK, United States, and Spain, travel may be an important factor for promoting human-to-human transmission[6, 25, 27, 28]. However, in this outbreak, the proportion of history of travel was less. Nicolò et al.[29] reported that from 14 May to 25 May 2022, there were only 46% patients with frequent travel outside the UK during the past 2 months among 54 male confirmed cases in London, UK. Of the 21 cases who reported travel locations, there were no cases with travel history to sub-Saharan Africa[29]. Similarly, at July 21, 2022, The New England Journal of Medicine reported the largest case series study with 528 cases in 16 countries between April 27 and June 24, 2022, and showed that the proportion of patients with the history of travel outside their countries within 1 month before diagnosis was 28%[30]. Above information indicated that monkeypox virus may form local transmission rather than imported cases in these non-epidemic countries.
Based on the risk assessment results, we considered that the United States and France, rather than other 76 countries had the higher importation risk into China. Monkeypox spreads by close contact with an animal infected with monkeypox virus[4]. Human infections have been documented through the handling of infected monkeys, Gambian giant rats, and squirrels, with rodents being the most likely reservoir of the virus[3]. China does not import primates, jungle meat products, so the flow of people should be the main way for be imported into China. The implementation of China’s “Belt and Road” has promoted the increase personnel exchanges and its speed[13]. By 2018, there were 196 countries or territories with international students into China, except Oceania, other four regions had more than 10,000 students[14]. Although up to now, Chinese mainland had no local cases, the National Health Commission of People’s Republic of China and the General Administration of Customs of the People’s Republic of China both issued documents to guide the prevention and control of risk of monkeypox importation[11, 12]. The latest studies revealed that more than 95% monkeypox cases were men who make sex with men (MSM), and the common sites of rash changed from face to genital[29, 30]. There may be sexual transmission which need more studies to confirmed, one way or another, it should be focused on the progress of the international epidemic, the characteristics of the epidemic to further reduce the risk of monkeypox importation.
We applied risk matrix method to assess the importation risk of countries with monkeypox outbreaks into China, and we integrated variables more related including the history of reported monkeypox cases, the number of international students entering China, the type of clades. The risk matrix method was a commonly used method to assess the importation risk of infectious diseases, such as poliomyelitis, leishmaniasis and coronavirus disease 2019[31-33]. However, there were some limitations in our study. First, we only used the number of international students into China to represent personnel exchanges, and lacked other personnel exchanges from official business, commerce, tourism, visiting relatives and other people in China, etc. Therefore, our study showed that risk of importation was relative, and might underestimate the actual importation risk into China.
-
China had the low risk of monkeypox importation because of prepared prevention and control measure. However, given the multiple-country monkeypox outbreak and frequent personal exchanges with other countries or territories, China still faced the monkeypox threat. Of 78 countries or territories, the key attention need be paid to the United States and France, relatively. Therefore, paying attention to the progress of the international epidemic, understanding the characteristics of the epidemic, and preparing prevention and control measures to further reduce the risk of importation were crucial.
doi: 10.3967/bes2022.115
2022 Multiple-country Monkeypox Outbreak and Its Importation Risk into China: An Assessment Based on the Risk Matrix Method
-
Abstract:
Objective To analyze the 2022 multiple-country monkeypox outbreak and assess its importation risk into China. Methods Data was from United States Centers for Disease Control and Prevention. We described the global epidemic and calculated concentration index to measure economic-related inequality. Importation risk into China was evaluated and ranked by using risk matrix method and Borda count method, respectively. Results As of July 29, 2022, of 79 countries or territories, 39 (49.37%, 39/79), 17 (21.52%, 17/79), 6 (7.59%, 6/79), 12 (15.19%, 12/79), and 5 (6.33%, 5/79) country or territories identified cases < 10, 10–, 51–, 101–, and > 1,000. There were economic-related health disparities exist in the distribution of cases (the concentration index = 0.42, P = 0.027), and the inequality disadvantageous to the rich (pro-poor). There were 12 (15.38%, 12/78), 15 (19.23%, 15/78), 6 (7.69%, 6/78), and 45 (57.69%, 45/78) countries or territories with extremely high, high, moderate, and low importation risk. United States and France ranked first with the highest Borda points of 156, and counts of zero. Conclusion Of 78 countries or territories, the key attention need be paid to the United States and France, relatively. As the epidemic progresses, preparing prevention and control measures to further reduce importation risk was crucial. -
Key words:
- Monkeypox /
- Importation risk /
- China /
- Risk matrix method
The authors declare that they have no conflict of interest to this work.
注释:1) AUTHOR CONTRIBUTIONS: 2) CONFLICTS OF INTEREST: -
Figure 2. Lorenz curves of cases or incidence rate of monkeypox infection. Red line was the equality line; Blue line was the Lorenz curve. (A) Cases: the concentration index = 0.42, P = 0.027. (B) Incidence rate: the concentration index = 0.46, P < 0.001.
Figure 3. The concentration index on monkeypox infection among different region. The differences between regions both were not significant (all P > 0.05). Blue histogram means the concentration index was the monkeypox cases: African region, the concentration index = −0.28, P = 0.411; American region, the concentration index = 0.57, P = 0.157; Asian region, the concentration index = 0.50, P = 0.288; European region, the concentration index = 0.17, P = 0.456; Oceania, the concentration index = 0.46, P was missing because of observations < 2; Total: the concentration index = 0.42, P = 0.027. Orange histogram means the concentration index was the incidence rate of monkeypox: African region, the concentration index = −0.38, P = 0.036; American region, the concentration index = 0.50, P = 0.009; Asian region, the concentration index = 0.57, P = 0.219; European region, the concentration index = 0.27, P = 0.017; Oceania, the concentration index = 0.32, P was missing because of observations < 2; Total, the concentration index = 0.46, P < 0.0001.
S1. The number of monkeypox cases reported at July 29, 2022 and 2018 international students entering China
Region Number of country or territories (%, n/N) Country or territories (number of cases) Country or territories (number of 2018 international students entering China) African 10 (12.66%, 10/79) Democratic Republic of the Congo (163), Nigeria (133), Ghana (30), Central African Republic (8), Cameroon (7), South Africa (3)
Benin (3), Republic of the Congo (2), Morocco (1), Liberia (1)Nigeria (6,845), Ghana (6,475), South Africa (2,981), Morocco (2,612), Cameroon (2,535), Democratic Republic of the Congo (2,246), Republic of the Congo (2,173), Liberia (802), Benin (634), Central African Republic (188) American 18 (22.78%, 18/79) United States (4,906), Brazil (978), Canada (803), Peru (269), Mexico (59), Chile (45), Argentina (20), Colombia (12), Ecuador (3), Costa Rica (3), Dominican Republic (3), Jamaica (2), Panama (1), Venezuela (1), Bahamas (1), Barbados (1), Bermuda (1), Martinique (1) United States (20,996), Canada (4,322), Mexico (1,540), Brazil (1,463), Colombia (879), Panama (738), Venezuela (629), Jamaica (539), Ecuador (519), Peru (502), Argentina (499), Chile (347), Costa Rica (279), Dominican, Republic (173), Bahamas (173), Barbados (104), Bermuda (0), Martinique (0) Asian 14 (17.72%, 14/79) Israel (133), United Arab Emirates (16), Singapore (11), India (4). Lebanon (4), Saudi Arabia (3), Japan (2), Thailand (2), Qatar (2), Taiwan (province of China, 2), South Korea (1), Philippines (1), Turkey (1), Georgia (1) South Korea (50,600), Thailand (28,608), India (23,198), Japan (14,230), Singapore (4,718), Philippines (2,786), Turkey (1,854), Saudi Arabia (783), Israel (449), Georgia (301), Lebanon (193), United Arab Emirates (78), Qatar (13), Taiwan (province of China, -)* European 34 (43.04%, 34/79) Spain (4,298), Germany (2,595), United Kingdom (2,546), France (1,955), Netherlands (879), Portugal (633), Italy (479), Belgium (393), Switzerland (264), Austria (124), Sweden (88), Ireland (85), Denmark (81), Poland (59), Norway (51), Hungary (37), Slovenia (33), Greece (32). Luxembourg (28), Romania (21), Czechia (19), Finland (17), Malta (17), Croatia (12), Serbia (10), Iceland (9), Estonia (6), Slovakia (6), Gibraltar (5), Bulgaria (4), Andorra (3), Latvia (3), Russia (1), Bosnia and Herzegovina (1) Russia (19,239), France (10,695), Germany (8,079), United Kingdom (6,415), Italy (5,386)
Spain (2,650), Netherlands (2,393), Poland (1,926), Belgium (1,502), Denmark (1,122), Sweden (1,080), Switzerland (884), Norway (813), Ireland (717), Portugal (633), Czechia (611), Romania (594), Hungary (587), Finland (585), Austria (517), Bulgaria (429), Serbia (394), Slovakia (329), Greece (252), Bosnia and Herzegovina (193), Latvia (162), Slovenia (123), Croatia (118), Estonia (86), Luxembourg (37), Iceland (30), Malta (11), Andorra (3), Gibraltar (0)Oceania 3 (3.80%, 3/79) Australia (45), New Zealand (2), New Caledonia (1) Australia (4,058), New Zealand (767), New Caledonia (0) Note. We could not get the number of students entering Chinese mainland in 2018 from Taiwan (province of China).  下载: 导出CSV
下载: 导出CSV
Table 1. Risk assessment indicators of importation possibility and importation severity and their scores
Assessment indicators Factors Classification Risk scores Importation possibility The number of international students entering China in 2018 (number) < 500 1 500–1,000 2 1,001–5,000 3 5,001–10,000 4 > 10,000 5 History of reported monkeypox No 1 Yes 2 Importation severity The number of monkeypox cases < 10 1 10–50 2 51–100 3 101–1,000 4 > 1,000 5 The type of clades West African Clade 1 Central African clade 2 Note. Taiwan (province of China) was excluded in the risk estimation because we could not get the number of students entering Chinese mainland in 2018.
下载: 导出CSV
Table 2. Risk matrix assessment index table
Importation
possibilityImportation severity Negligible Minor Moderate Serious Catastrophic Inevitable H H E E E Very possible M H H E E Possible L M H E E Unlikely L L M H E Rare L L M H H Note. L, low importation risk; M, moderate importation risk; H, high importation risk; E, extremely high importation risk.
下载: 导出CSV
Table 3. Importation risks from countries or territories with monkeypox infection to China in the 2022 multiple-country monkeypox outbreak
Countries or
territoriesThe score of importation severity The score of importation possibility Risk levels Borda points Borda count Risk sequence of importation United States 6 6 E 156 0 1 France 6 6 E 156 0 1 Nigeria 5 6 E 150 6 7 Germany 6 5 E 147 9 10 United Kingdom 6 5 E 147 9 10 Democratic Republic of the Congo 6 5 E 147 9 10 Italy 5 5 E 141 15 16 Spain 6 4 E 141 15 16 Canada 5 4 E 135 21 22 Netherlands 5 4 E 135 21 22 Belgium 5 4 E 135 21 22 Brazil 5 4 E 135 21 22 Ghana 3 6 H 133 23 24 Republic of the Congo 3 5 H 124 32 33 Poland 4 4 H 124 32 33 Mexico 4 4 H 124 32 33 Denmark 4 4 H 124 32 33 Switzerland 5 3 H 119 37 38 Portugal 5 3 H 119 37 38 Austria 5 3 H 119 37 38 Peru 5 3 H 119 37 38 South Korea 2 6 H 114 42 43 Thailand 2 6 H 114 42 43 India 2 6 H 114 42 43 Russia 2 6 H 114 42 43 Japan 2 6 H 114 42 43 Israel 5 2 H 100 56 57 Sweden 4 4 M 124 32 33 Singapore 3 4 M 118 38 39 Australia 3 4 M 118 38 39 Norway 4 3 M 108 48 49 Ireland 4 3 M 108 48 49 Cameroon 2 5 M 105 51 52 Colombia 3 3 L 102 54 55 Czechia 3 3 L 102 54 55 Romania 3 3 L 102 54 55 Hungary 3 3 L 102 54 55 Finland 3 3 L 102 54 55 Central African Republic 3 3 L 102 54 55 South Africa 2 4 L 99 57 58 Philippines 2 4 L 99 57 58 Morocco 2 4 L 99 57 58 Turkey 2 4 L 99 57 58 Liberia 2 4 L 99 57 58 Saudi Arabia 2 3 L 83 73 74 New Zealand 2 3 L 83 73 74 Panama 2 3 L 83 73 74 Benin 2 3 L 83 73 74 Venezuela 2 3 L 83 73 74 Jamaica 2 3 L 83 73 74 Ecuador 2 3 L 83 73 74 Argentina 3 2 L 83 73 74 Serbia 3 2 L 83 73 74 Chile 3 2 L 83 73 74 Greece 3 2 L 83 73 74 Slovenia 3 2 L 83 73 74 Croatia 3 2 L 83 73 74 United Arab Emirates 3 2 L 83 73 74 Luxembourg 3 2 L 83 73 74 Malta 3 2 L 83 73 74 Bulgaria 2 2 L 64 92 93 Slovakia 2 2 L 64 92 93 Georgia 2 2 L 64 92 93 Costa Rica 2 2 L 64 92 93 Lebanon 2 2 L 64 92 93 Bosnia and Herzegovina 2 2 L 64 92 93 Dominican Republic 2 2 L 64 92 93 Bahamas 2 2 L 64 92 93 Latvia 2 2 L 64 92 93 Barbados 2 2 L 64 92 93 Estonia 2 2 L 64 92 93 Iceland 2 2 L 64 92 93 Qatar 2 2 L 64 92 93 Andorra 2 2 L 64 92 93 Gibraltar 2 2 L 64 92 93 Bermuda 2 2 L 64 92 93 Martinique 2 2 L 64 92 93 New Caledonia 2 2 L 64 92 93 Note. Country names were ranked in descending order of the risk levels. L, low importation risk; M, moderate importation risk; H, high importation risk; E, extremely high importation risk; Taiwan (province of China) was excluded in the risk estimation because we could not get the number of students entering Chinese mainland in 2018.
下载: 导出CSV
-
[1] Rezza G. Emergence of human monkeypox in west Africa. Lancet Infect Dis, 2019; 19, 797−9. doi: 10.1016/S1473-3099(19)30281-6 [2] Mukinda VBK, Mwema G, Kilundu M, et al. Re-emergence of human monkeypox in Zaire in 1996. Lancet, 1997; 349, 1449−50. doi: 10.1016/S0140-6736(05)63725-7 [3] African CDC. Monkeypox.https://africacdc.org/disease/monkeypox/. [2022-09-05]. [4] Walter K, Malani PN. What is monkeypox? JAMA, 2022; 328, 222. doi: 10.1001/jama.2022.10259 [5] Ng OT, Lee V, Marimuthu K, et al. A case of imported Monkeypox in Singapore. Lancet Infect Dis, 2019; 19, 1166. [6] Costello V, Sowash M, Gaur A, et al. Imported Monkeypox from International Traveler, Maryland, USA, 2021. Emerg Infect Dis, 2022; 28, 1002−5. doi: 10.3201/eid2805.220292 [7] Vaughan A, Aarons E, Astbury J, et al. Two cases of monkeypox imported to the United Kingdom, September 2018. Euro Surveill, 2018; 23, 1800509. [8] World Health Organization. Multi-country monkeypox outbreak: situation update.https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON393. [2022-09-05]. [9] USA Centers for Disease Control and Prevention. 2022 Monkeypox Outbreak Global Map.https://www.cdc.gov/poxvirus/monkeypox/response/2022/world-map.html. [2022-09-05]. [10] World Health Organization. Second meeting of the International Health Regulations (2005) (IHR) Emergency Committee regarding the multi-country outbreak of monkeypox.https://www.who.int/news/item/23-07-2022-second-meeting-of-the-international-health-regulations-(2005)-(ihr)-emergency-committee-regarding-the-multi-country-outbreak-of-monkeypox. [2022-09-05]. [11] Notice on printing and distributing the monkeypox diagnosis and treatment guide (2022 Edition). http://www.nhc.gov.cn/yzygj/s7653p/202206/d687b12fe8b84bbfaede2c7a5ca596ec.shtml. [2022-09-05]. (In Chinese) [12] Announcement No. 65 of the General Administration of Customs in 2022 (announcement on preventing monkeypox epidemic from being introduced into China). http://www.customs.gov.cn/customs/302249/302266/302267/4482275/index.html. [2022-09-05]. (In Chinese) [13] Zhou XW, Yang R, Jiang JY, et al. Lancang-Mekong collaboration in response to the challenge of vector-borne diseases: Control of malaria and dengue through Lancang-Mekong Cooperation. J Pathog Biol, 2021; 16, 109−16. (In Chinese [14] Ministry of Education, Department of International Cooperation and Exchange. Concise statistics of International Students 280 in 2018, 2018; 348. (In Chinese) [15] World Health Organization. Monkeypox. https://www.who.int/news-room/fact-sheets/detail/monkeypox. [2022-09-05]. [16] Bunge EM, Hoet B, Chen L, et al. The changing epidemiology of human monkeypox-A potential threat? A systematic review. PLoS Negl Trop Dis, 2022; 16, e0010141. doi: 10.1371/journal.pntd.0010141 [17] López-Feldman A. Decomposing inequality and obtaining marginal effects. Stata J, 2006; 6, 106−11. doi: 10.1177/1536867X0600600107 [18] Espy MJ, Cockerill FR III, Meyer RF, et al. Detection of smallpox virus DNA by LightCycler PCR. J Clin Microbiol, 2002; 40, 1985−8. doi: 10.1128/JCM.40.6.1985-1988.2002 [19] Chen PJ, Li FZ, Harmer P. Healthy China 2030: moving from blueprint to action with a new focus on public health. Lancet Public Health, 2019; 4, e447. doi: 10.1016/S2468-2667(19)30160-4 [20] Wang XY, Liu J, Wang Q, et al. Economic-related inequalities in hepatitis B virus infection among 115.8 million pregnant women in China from 2013 to 2020. EClinicalMedicine, 2022; 49, 101465. doi: 10.1016/j.eclinm.2022.101465 [21] Yang Y, Sun H, Kang Z, et al. Health emergency assessment: Risk matrix and Borda sequence value method. Chin J Public Health, 2016; 32, 815−7. (In Chinese [22] Kang LY, Liu J, Liu M. Progress in researches on methods for risk assessment of infectious diseases. Chin J Public Health, 2021; 37, 1454−8. (In Chinese [23] Yun L, Wang FC, Zhang QF, et al. Integrated application of risk matrix method and borda sequence value method to assess the risks of vectors for 2016 international horticultural exposition. Chin J Vect Bio Control, 2017; 28, 557−60. (In Chinese [24] Przybyła-Kasperek M, Marfo KF. Neural network used for the fusion of predictions obtained by the K-nearest neighbors algorithm based on independent data sources. Entropy (Basel), 2021; 23, 1568. doi: 10.3390/e23121568 [25] USA Centers for Disease Control and Prevention. Past U. S. Cases and Outbreaks. https://www.cdc.gov/poxvirus/monkeypox/outbreak/us-outbreaks.html. [2022-09-05]. [26] Reynolds MG, Yorita KL, Kuehnert MJ, et al. Clinical manifestations of human monkeypox influenced by route of infection. J Infect Dis, 2006; 194, 773−80. doi: 10.1086/505880 [27] Rao AK, Schulte J, Chen TH, et al. Monkeypox in a traveler returning from Nigeria - Dallas, Texas, July 2021. MMWR Morb Mortal Wkly Rep, 2022; 71, 509−16. doi: 10.15585/mmwr.mm7114a1 [28] Angelo KM, Petersen BW, Hamer DH, et al. Monkeypox transmission among international travellers-serious monkey business? J Travel Med, 2019; 26, taz002. doi: 10.1093/jtm/taz002 [29] Girometti N, Byrne R, Bracchi M, et al. Demographic and clinical characteristics of confirmed human monkeypox virus cases in individuals attending a sexual health centre in London, UK: an observational analysis. Lancet Infect Dis, 2022; 22, 1321−8. doi: 10.1016/S1473-3099(22)00411-X [30] Thornhill JP, Barkati S, Walmsley S, et al. Monkeypox virus infection in humans across 16 countries - April-June 2022. N Engl J Med, 2022; 387, 679−91. doi: 10.1056/NEJMoa2207323 [31] Han TL, Duan XJ, Wang Y, et al. Risk assessment of poliomyelitis imported into China from Afghanistan using risk matrix. Int J Virol, 2021; 28, 321−4. (In Chinese [32] Hao YW, Tian T, Zhu ZL, et al. Transmission risk matrix assessment of imported leishmaniasis in China. Chin J Schistosom Control, 2018; 30, 428−32. (In Chinese [33] Abuhabib AA, Abu-Aita SN, Procter C, et al. Unique situation of Gaza Strip dealing with COVID-19 crisis. Int J Infect Dis, 2020; 100, 149−51. doi: 10.1016/j.ijid.2020.08.070 -
 22267Supplementary Materials.pdf
22267Supplementary Materials.pdf

-

 点击查看大图
点击查看大图
计量
- 文章访问数: 574
- HTML全文浏览量: 262
- PDF下载量: 65
- 被引次数: 0






 Quick Links
Quick Links