

 下载:
下载:



-
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a single-stranded, positive-sense, non-segmented enveloped RNA virus belonging to the genus Betacoronavirus of the family Coronaviridae. It causes the coronavirus disease-19 (COVID-19) in humans. Identified in December 2019 [1], COVID-19 has caused a global pandemic beginning from March 2020. As per the report by the World Health Organization (WHO), there are 599.8 million confirmed cases of COVID-19, and 6.4 million confirmed deaths globally as of September 1, 2022 (
https://www.who.int/emergencies/diseases/novel-coronavirus-2019 ). The symptoms of COVID-19 include dry cough, fever, sore throat, and loss of taste and smell, and serious complications such as septic shock, severe pneumonia, renal failure, and acute respiratory distress syndrome (ARDS), and presentations may range from asymptomatic to pneumonia and ARDS [2, 3]. Transmission of SARS-CoV-2 is through contact, droplets, fomites, or airborne or fecal-oral routes.In general, symptomatic SARS-CoV-2-positive patients are detected when they seek medical attention; however, without imperative testing, asymptomatic carriers can be missed and contribute to the spread of SARS-CoV-2. In addition, for any region where testing is not required for all individuals, asymptomatic cases can compromise the control programs implemented. Therefore, asymptomatic carriers are believed to be the main drivers of the SARS-CoV-2 pandemic [4, 5]. Many studies have reported the detection of SARS-CoV-2-positive individuals among different populations, including healthcare workers, children, pregnant patients, cruise ship passengers and staff, airplane passengers, close contacts of SARS-CoV-2-positive patients, and individuals from homeless shelters, nursing facilities, military quarantine facilities, rehabilitation facilities, and jails[6-26] (Supplementary Tables S1 and S2, available in www.besjournal.com). Several factors, including the total number of testing populations and conflation of true asymptomatic and pre-symptomatic individuals, affect the percentage of SARS-CoV-2-positive asymptomatic individuals in the defined populations.
Table S1. Studies on testing SARS-CoV-2 in populations containing asymptomatic individuals
Populations Total tested Asymptomatic positive/total positive, n (%) Asymptomatic positive/total tested (%) Reference Iceland residents 13,080 43/100 (43) 0.3 Spread of SARS-CoV-2 in the Icelandic Population Italy Vo’ residents 5,155 42/102 (41.2) 0.8 Suppression of a SARS-CoV-2 outbreak in the Italian municipality of Vo’ Ethiopia residents 61,599 1,935/2,617 (73.9) 3.1 Clinical features and risk factors associated with morbidity and mortality among patients with COVID-19 in northern Ethiopia Japan Diamond Princess cruise 3,711 328/634 (51.7) 8.8 Estimating the asymptomatic proportion of coronavirus disease 2019 (COVID-19) cases on board the Diamond Argentine cruise 217 104/128 (81.3) 47.9 COVID-19: in the footsteps of Ernest Shackleton New York obstetrical patients 215 29/33 (87.9) 13.5 Universal Screening for SARS-CoV-2 in Women Admitted for Delivery Spain obstetrical patients 11,728 174/279 (62.4) 1.5 Obstetric Outcomes of SARS-CoV-2 Infection in Asymptomatic Pregnant Women West French Guiana obstetrical patients 507 87/137 (63.5) 17.2 Maternal, fetal and neonatal outcomes of large series of SARS-CoV-2 positive pregnancies in peripartum period: A single-center prospective comparative study Flight back to Greece from United Kingdom, Spain, and Turkey 783 35/40 (87.5) 4.5 High prevalence of SARS-CoV-2 infection in repatriation flights to Greece from three International Entrants to China from 90 countries 19,398,384 1,612/3,103 (51.9) 0.008 Asymptomatic SARS-CoV-2 Infections Among Persons Entering China From April 16 to October 12, 2020 Washington Nursing Facility 76 27/48 (56.3) 35.5 Presymptomatic SARS-CoV-2 Infections and Transmission in a Skilled Nursing Facility 76 13/23 (56.5) 17.1 Asymptomatic and Presymptomatic SARS-CoV-2 infections in residents of a long-term care skilled Chicago Nursing Facility 204 50/172 (29.1) 24.5 Management and outcomes of a COVID-19 outbreak in a nursing home with predominantly Black residents France nursing home 456 14/161 (8.7) 3.1 Atypical symptoms, SARS-CoV-2 test results and immunisation rates in 456 residents from eight nursing homes facing a COVID-19 outbreak Long-term care facilities residents 116 10/111 (9) 8.6 Clinical Presentation, Course, and Risk Factors Associated with Mortality in a Severe Outbreak of COVID-19 in Rhode Island, USA, April–June 2020 New Jersey hospital and university employees 829 27/41 (65.9) 3.3 Prevalence of SARS-CoV-2 infection in previously undiagnosed health care workers at the onset of the U.S. COVID-19 epidemic Italy healthcare workers 1,573 17/139 (12.2) 1.1 Characteristics of 1573 healthcare workers who underwent nasopharyngeal swab testing for SARS-CoV-2 in Milan, Lombardy, Italy New York city jail system 978 58/568 (10.2) 5.9 COVID-19 in the New York City Jail System: Epidemiology and Health Care Response, March–April 2020 Boston homeless shelter 408 129/147 (87.8) 31.6 Prevalence of SARS-CoV-2 infection in residents of a large homelss shelter in boston India military quarantine facilities 26 25/25 (100) 96.2 Spread of COVID-19 by asymptomatic cases: evidence from military quarantine facilities Pediatric patients (< 18 years old) 2,135 94/728 (12.9) 4.4 Epidemiology of COVID-19 among children China Children patients in Wuhan (1day-15 years old) 1,391 27/171 (15.8) 1.9 SARS-CoV-2 infection in children US sailors 4,085 146/736 (19.8) 3.6 Symptom Characterization and Outcomes of Sailors in Isolation After a COVID-19 Outbreak on a US Aircraft Carrier Close contact of 314 Spain patients 753 240/449 (53.5) 31.9 Transmission of COVID-19 in 282 clusters in Catalonia, Spain: a cohort study Table S2. Studies on characterizing SARS-CoV-2 positive patients containing asymptomatic individuals
Populations Total of
PositiveAsymptomatic positive/total positive,
n (%)Reference Note Kuwait residents 1,096 473/1,096 (43.2) Characteristics, risk factors and outcomes among the first consecutive 1,096 patients diagnosed with COVID-19 in Kuwait 35 presymptomatic UK rehabilitation facility 45 15/45 (33.3) Asymptomatic severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in a rehabilitation facility Patients in Beijing 262 13/262 (4.9) Characteristics of COVID-19 infection in Beijing Patients in Shanghai 328 13/328 (4.0) Follow-up of asymptomatic patients with SARS-CoV-2 infection Residents in South Korea 199 53/199 (26.6) Asymptomatic infection and atypical manifestations of COVID-19: Comparison of viral shedding duration Patients in People’s Hospital of Daofu county 83 18/83 (21.7) A considerable proportion of individuals with asymptomatic SARS-CoV-2 infection in Tibetan population Children in Zhejiang
(1–16 years old)36 10/36 (28) Clinical and epidemiological features of 36 children with coronavirus disease 2019 Children in Kuwait 134 91/134 (67.9) Clinical characteristics of pediatric SARS-CoV-2 infection and coronavirus disease 2019 (COVID-19) in Kuwait 3 presymptomatic Bahrain patients and their contacts 320 index cases
1,289 positive contacts160/320 (50)
1,127/1,289 (87.4)The high prevalence of asymptomatic SARS-CoV-2 infection reveals the silent spread of COVID-19 Air passengers to Brunei 138 16/138 (11.6) High proportion of asymptomatic and presymptomatic
COVID-19 infections in air passengers to BruneiAlthough many studies have reported the detection of SARS-CoV-2-positive asymptomatic populations in different countries, immune responses in asymptomatic individuals are understudied, and data have been inconsistent. In addition, the durability of the protective immune responses against SARS-CoV-2 remains unclear. A seroprevalence study from the United States using an immunoassay to detect antibodies to the SARS-CoV-2 nucleocapsid protein showed that 6.6% (4,094 of 61,910) of asymptomatic population was seropositive [27]. A study from China reported that of 63 asymptomatic individuals tested positive for SARS-CoV-2 utilizing both molecular tests and immunoglobulin (Ig) M- and IgG-based serological tests, 39 (61.9%) produced low titers of neutralizing antibodies, which started as early as 7 days post-exposure, peaked between 10 and 25 days post-exposure, and subsequently dropped rapidly. In contrast, 45 of 51 patients with mild symptoms produced higher neutralizing antibodies, which peaked around 22 days post-symptom onset and were maintained for at least 65 days [28].
In the present study, we measured the neutralizing antibodies of asymptomatic and symptomatic individuals with COVID-19 at three time points post-polymerase chain reaction (PCR) confirmation and summarized meta-analysis studies on asymptomatic SARS-CoV-2 infection.
-
In this study, 69 symptomatic [42 males and 27 females, average age of 43.4 years (standard deviation = 16.5)] and 27 asymptomatic [13 males and 14 females, average age of 35.8 years (standard deviation = 13.9)] patients were confirmed SARS-CoV-2-positive by a PCR assay targeting the ORF1ab and N genes. These individuals were infected during the outbreak period from June to December 2020, and their serum samples were collected at different time points from June 2020 to October 2021 in Beijing. The symptomatic patients were hospitalized with no previous medical history and characteristic chest computed tomography (CT) findings of COVID-19 pneumonia. These symptomatic patients had respiratory symptoms and pneumonia on CT and were SARS-CoV-2 PCR-positive, whereas the asymptomatic patients were only PCR-positive without the respiratory symptoms or pneumonia. Blood samples were collected from symptomatic patients at 3, 6, and 10 months post-PCR confirmation and from asymptomatic patients at 1, 2, and 6 months post-PCR confirmation. This study was reviewed and approved by the Ethics Committee of Beijing Center for Disease Control and Prevention (2020026). Written informed consent was obtained from all patients.
-
A SARS-CoV-2 microneutralization assay was performed using Vero cells as previously described [29, 30]. Serum samples were heat-inactivated at 56 ℃ for 30 min. The serum samples were subsequently serially diluted two fold and equally added to 100 µL of cell medium containing 100 cell culture infectious dose. The serum-virus mixture was incubated for 2 h at 37 ℃ with 5% CO2. Subsequently, 96-well cell culture plates with semi-confluent Vero cell monolayers were inoculated with 100 µL of the mixture at each dilution, in duplicate. The plates were incubated for 5 days at 37 ℃ and subsequently examined for cytopathic effects. The highest serum dilution that inhibited at least 50% of the cytopathic effects was considered as the neutralization titer.
Virus antibody mix was subsequently added to cells in 96-well plates, and the plates were incubated at 37 °C with microscopic examination for cytopathic effects after 5-day incubation.
-
SPSS software (version 19.0) was used for statistical analysis. The Kruskal-Wallis test was used to compare the neutralizing antibody titers of the symptomatic and asymptomatic groups at different time points after PCR confirmation. Statistical significance was set at a P value < 0.05.
-
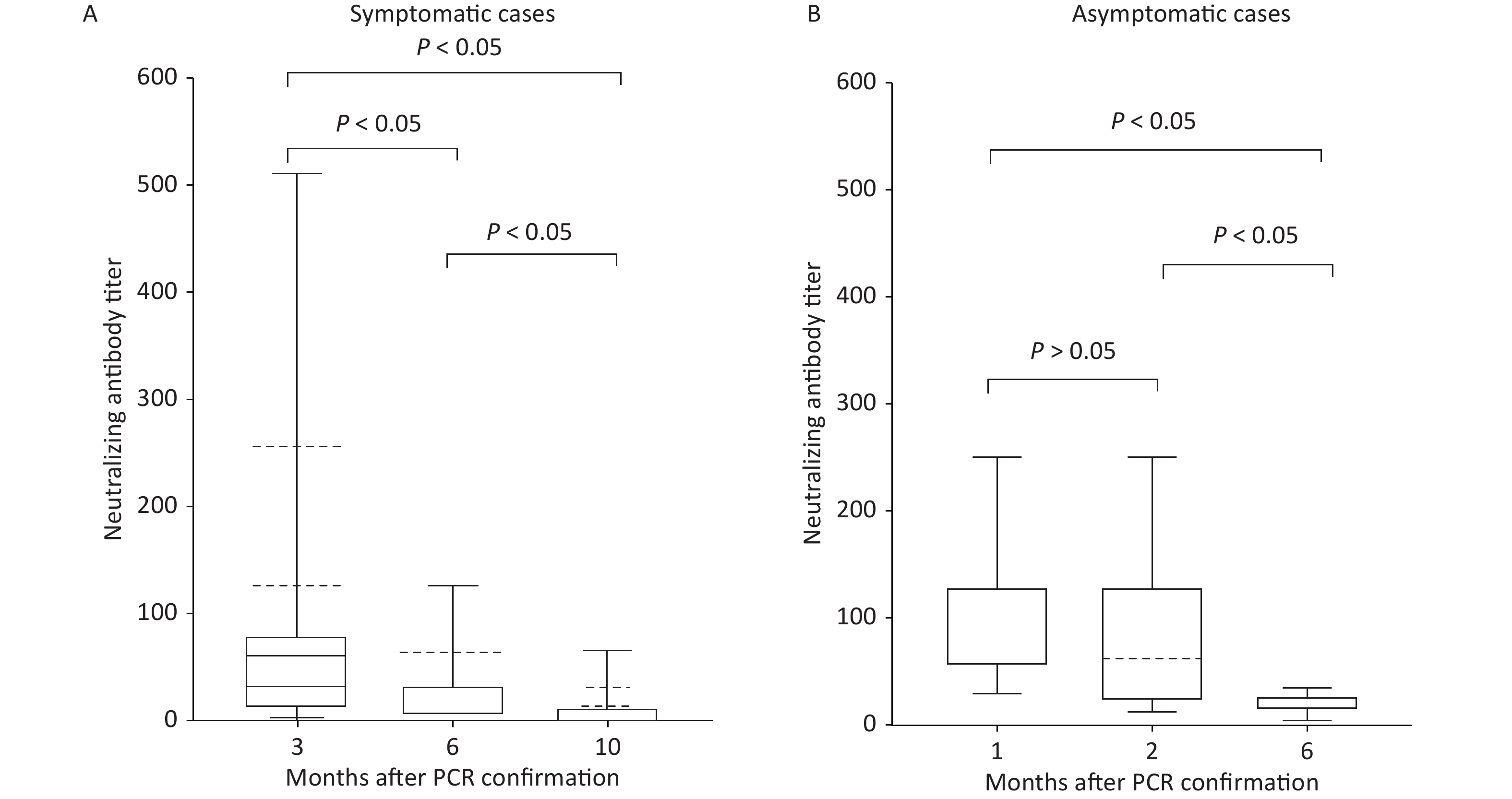
All symptomatic and asymptomatic individuals were confirmed to be SARS-CoV-2 positive by PCR. Neutralizing antibodies of 69 symptomatic patients peaked (83.3 ± 105.9) at 3 months post-PCR confirmation and significantly dropped at 6 (22.9 ± 22.6) and 10 months (7.7 ± 10.1) post-confirmation (Figure 1). Neutralizing antibodies in 27 asymptomatic patients showed a similar trend with relatively higher levels at 1 month post-confirmation (103.1 ± 64.8), lower levels at 2 months post-confirmation (81.2 ± 64.1), and significantly lower levels at 6 months post-confirmation (19.6 ± 10.3) (Figure 1). Compared with the symptomatic group, the asymptomatic group had relatively lower levels of neutralizing antibodies at 2 and 6 months post-confirmation.
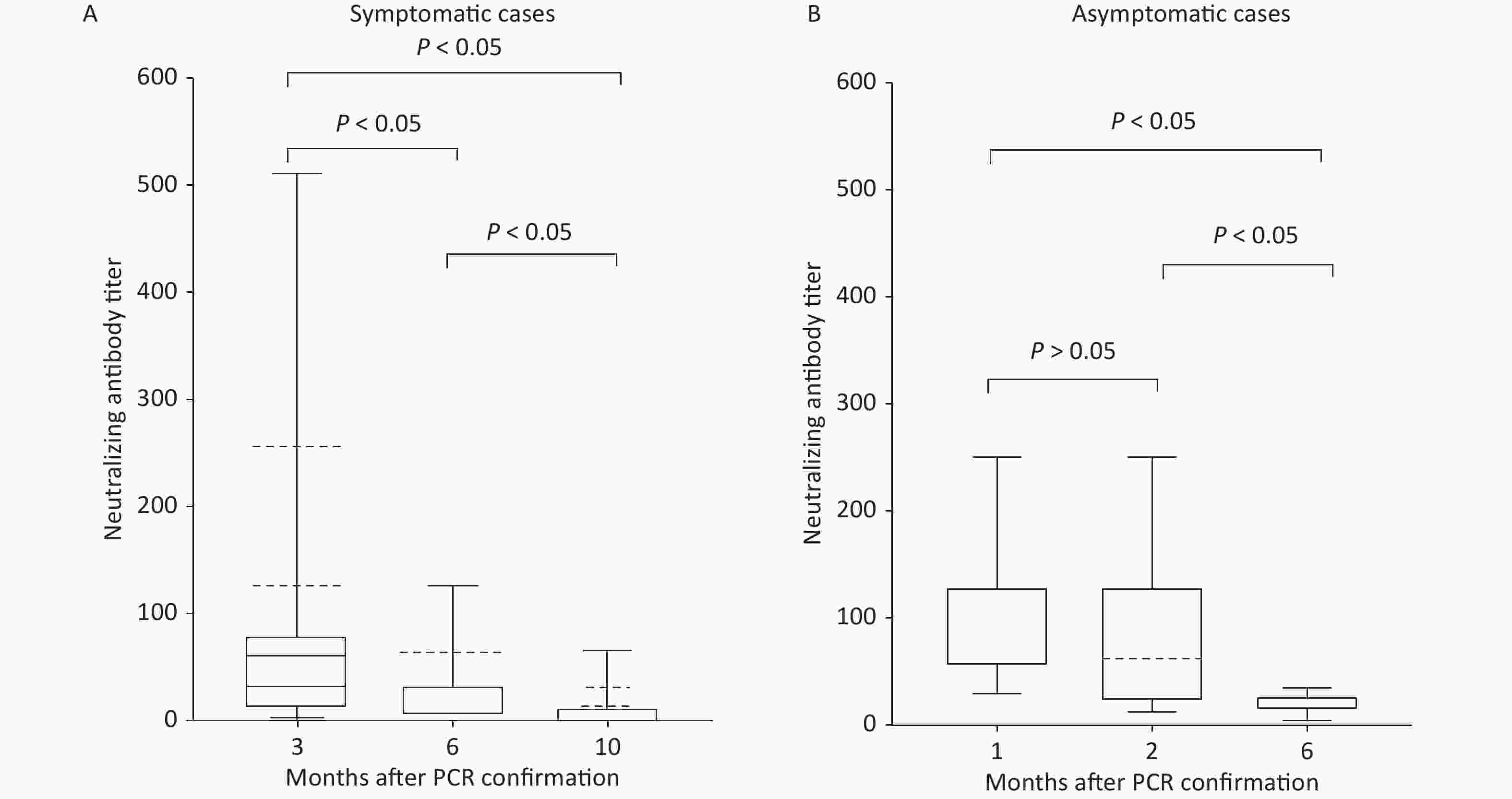
Figure 1. SARS-CoV-2 neutralizing antibody titers at three different time points (Statistical significance was set at P < 0.05). (A) 3, 6, and 10 months post-PCR confirmation for symptomatic patients. (B) 1, 2, and 6 months post-PCR confirmation for asymptomatic patients.
Overall, our data showed that neutralizing antibodies gradually dropped to lower levels in both symptomatic and asymptomatic individuals with COVID-19, and symptomatic patients had relatively higher levels of neutralizing antibodies at 6 months post-confirmation, consistent with the previous findings that the levels of neutralizing antibodies were correlated with disease severity [31]. A study from South Korea analyzed antibody status in seven asymptomatic individuals and 11 patients with pneumonia at 2 and 5 months after symptom onset [30]. This study showed that both asymptomatic and symptomatic patients had neutralizing antibodies at 2 and 5 months after infection, and antibody levels decreased from 219.4 at 2 months post-infection to 143.7 at 5 months post-infection. At 8 months post-infection, 4 of 7 asymptomatic individuals were still positive for neutralizing antibodies [32, 33]. In the aforementioned study, neutralizing antibody titers decreased more in symptomatic than in asymptomatic patients [30], which differs from our finding that neutralizing antibody titers of asymptomatic patients decreased in a similar trend as those of symptomatic patients. A follow-up study of 31 asymptomatic patients with COVID-19 showed that 74% of the patients did not have circulating immunoglobulins against SARS-CoV-2 at 8 weeks post-testing. Over 40% of these patients had no detectable immunoglobulin at either time point with an 8-week interval [34].
In the present study, we observed that the neutralization titers of both asymptomatic and symptomatic groups dropped to very low levels at 6 months post-PCR confirmation. This indicates that higher levels of neutralizing antibodies elicited through one-time infection of SARS-CoV-2 only persist for less than half a year. Therefore, SARS-CoV-2 immunization would be still required for protection against future infection.
The data of the present study were obtained from SARS-CoV-2 outbreaks in Beijing, China. The present study has a few limitations. First, our study was not prospectively controlled, and patient demographic factors, such as drug history and radiology findings in the symptomatic group, were not evaluated. Second, the evaluation periods post-PCR confirmation for the symptomatic and asymptomatic groups were different, which made data analysis between the groups difficult. Third, the sample sizes of the groups (n = 27 and n = 69) were not sufficiently large. Fourth, the study could not include data related to the immune responses against SARS-CoV-2 variants.
In contrast to the limited number of studies on immune responses of asymptomatic patients with COVID-19, there are several studies on the prevalence of asymptomatic infection[35]. There have been seven meta-analyses on the prevalence of asymptomatic COVID-19 infection. These seven studies analyzed the data from 6–390 published studies, and reported the percentage of asymptomatic individuals with COVID-19 to be 15.6% (41 studies) [36], 17% (13 studies) [37], 20% (79 studies) [38], 24.2% (6 studies) [4], 25% (28 studies) [39], 35.1% (390 studies) [40], and 48.2% (16 studies) [41] (Table 1). Among these, the meta-analysis with 16 studies indicated a significant heterogeneity among the studies, and the actual proportion of asymptomatic COVID-19 cases was reported to be 31.1% [41]. Subgroup analysis of different age groups showed similar percentages of asymptomatic COVID-19 cases in children (27.7%) and older adults (28.3%) in one study [36]; however, this was significantly higher in children than in older adults in two studies (46.7% vs. 19.7%, and 49.6% vs. 16.9%) [40, 41]. In addition, one study analyzed the radiology results in patients with COVID-19 and revealed that individuals with normal radiology results were significantly younger 19.59 ± 17.17 years than those with abnormal radiology results 39.14 ± 26.70 years [4]. Overall, these studies suggested that asymptomatic individuals accounted for 15.6%–35.1% of the total number of SARS-CoV-2-positive individuals.
Table 1. Meta-analysis studies on asymptomatic COVID-19 cases
Total number of studies included % of asymptomatic
individualsNote Reference Publication time 6 24.2 (SD, 22.06) 34 studies were included in the qualitative synthesis, and 17 studies (13 case reports and 4 case series) for meta-analysis contained CT or lab test results. Individuals with normal radiology results were significantly younger (19.59 ± 17.17 years) than patients with abnormal radiology results (39.14 ± 26.70 years). Data from 6 case series were used to calculate the percentage of asymptomatic individuals Ref [4] June 17, 2020 41 15.6 (95% CI: 10.1–23.0) 180 asymptomatic individuals reported from 10 studies included 48.9% pre-symptomatic individuals. 24: all ages, 9% 11: children, 27.7% 3: older adults, 28.3% 4: pregnant women, 49.9% Ref [36] July 21, 2020 79 20 (95% CI: 17–25) 7 studies screening all potentially exposed people in the defined populations and followed-up after testing, 31% (59% CI: 26%–37%) remained asymptomatic Ref [38] July 28, 2020 13 17 (95 CI : 14–20) 4% in Korea to 40% in Vo, Italy, and in an aged care facility in the United States Non-aged care, 16% and aged care, 21%. Ref [37] September 13, 2020 16 48.2 (95% CI: 30.0–67.0)
with significant heterogeneity
noted among studies. Actual
proportion of asymptomatic
cases, 31.1%8 studies with age subgroup analysis, children, 49.6%; adults, 30.3%; and older adults, 16.9%. 39% prevalence of true asymptomatic cases versus 15.3% of pre-symptomatic cases in 10 studies Ref [41] January 20, 2021 28 25 (95% CI: 16–38) Ref [39] March 23, 2021 390 35.1 (95% CI: 30.7–39.9) 42.8% of cases without symptoms at the time of testing. Children: 46.7% Older adults: 19.7% Comorbidities had significantly lower asymptomaticity compared with cases without underlying medical conditions. Ref [40] August 10, 2021 Note. SD, standard deviation; CI , confidence interval; CT, computed tomography. Two of the three above-mentioned meta-analysis studies showed that children had a higher percentage of asymptomatic SARS-CoV-2 infection than older adults [40, 41]. The asymptomatic group of children could be a main concern as they may spread the virus to classmates and family members if no active testing and quarantine program is in place. Data used in the present and previous studies were collected from the pre-SARS-CoV-2 vaccination period. With more people immunized with SARS-CoV-2 inactivated vaccines since late 2020, the number of asymptomatic SARS-CoV-2-positive individuals will be higher. These asymptomatic individuals can be either vaccinated or non-vaccinated. Therefore, continued monitoring of asymptomatic groups is essential for controlling the spread of SARS-CoV-2 in humans.
-
Neutralizing antibodies in the symptomatic and asymptomatic groups with COVID-19 dropped significantly to lower levels at 6 months post-PCR confirmation, and continued monitoring of both symptomatic and asymptomatic individuals will be vital in controlling the spread of SARS-CoV-2.
-
All data generated or analyzed during this study are included in this published article (and its Supplementary Information files).
doi: 10.3967/bes2022.139
Symptomatic and Asymptomatic SARS-CoV-2 Infection and Follow-up of Neutralizing Antibody Levels
-
Abstract:
Objective To investigate neutralizing antibody levels in symptomatic and asymptomatic patients with coronavirus disease 2019 (COVID-19) at 6 and 10 months after disease onset. Methods Blood samples were collected at three different time points from 27 asymptomatic individuals and 69 symptomatic patients infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Virus-neutralizing antibody titers against SARS-CoV-2 in both groups were measured and statistically analyzed. Results The symptomatic and asymptomatic groups had higher neutralizing antibodies at 3 months and 1–2 months post polymerase chain reaction confirmation, respectively. However, neutralizing antibodies in both groups dropped significantly to lower levels at 6 months post-PCR confirmation. Conclusion Continued monitoring of symptomatic and asymptomatic individuals with COVID-19 is key to controlling the infection. -
Key words:
- SARS-CoV-2 /
- Symptomatic /
- Asymptomatic /
- Neutralizing antibody
The authors declare that they have no conflicts of interest.
注释:1) AUTHOR CONTRIBUTIONS: 2) CONFLICTS OF INTEREST: -
Figure 1. SARS-CoV-2 neutralizing antibody titers at three different time points (Statistical significance was set at P < 0.05). (A) 3, 6, and 10 months post-PCR confirmation for symptomatic patients. (B) 1, 2, and 6 months post-PCR confirmation for asymptomatic patients.
S1. Studies on testing SARS-CoV-2 in populations containing asymptomatic individuals
Populations Total tested Asymptomatic positive/total positive, n (%) Asymptomatic positive/total tested (%) Reference Iceland residents 13,080 43/100 (43) 0.3 Spread of SARS-CoV-2 in the Icelandic Population Italy Vo’ residents 5,155 42/102 (41.2) 0.8 Suppression of a SARS-CoV-2 outbreak in the Italian municipality of Vo’ Ethiopia residents 61,599 1,935/2,617 (73.9) 3.1 Clinical features and risk factors associated with morbidity and mortality among patients with COVID-19 in northern Ethiopia Japan Diamond Princess cruise 3,711 328/634 (51.7) 8.8 Estimating the asymptomatic proportion of coronavirus disease 2019 (COVID-19) cases on board the Diamond Argentine cruise 217 104/128 (81.3) 47.9 COVID-19: in the footsteps of Ernest Shackleton New York obstetrical patients 215 29/33 (87.9) 13.5 Universal Screening for SARS-CoV-2 in Women Admitted for Delivery Spain obstetrical patients 11,728 174/279 (62.4) 1.5 Obstetric Outcomes of SARS-CoV-2 Infection in Asymptomatic Pregnant Women West French Guiana obstetrical patients 507 87/137 (63.5) 17.2 Maternal, fetal and neonatal outcomes of large series of SARS-CoV-2 positive pregnancies in peripartum period: A single-center prospective comparative study Flight back to Greece from United Kingdom, Spain, and Turkey 783 35/40 (87.5) 4.5 High prevalence of SARS-CoV-2 infection in repatriation flights to Greece from three International Entrants to China from 90 countries 19,398,384 1,612/3,103 (51.9) 0.008 Asymptomatic SARS-CoV-2 Infections Among Persons Entering China From April 16 to October 12, 2020 Washington Nursing Facility 76 27/48 (56.3) 35.5 Presymptomatic SARS-CoV-2 Infections and Transmission in a Skilled Nursing Facility 76 13/23 (56.5) 17.1 Asymptomatic and Presymptomatic SARS-CoV-2 infections in residents of a long-term care skilled Chicago Nursing Facility 204 50/172 (29.1) 24.5 Management and outcomes of a COVID-19 outbreak in a nursing home with predominantly Black residents France nursing home 456 14/161 (8.7) 3.1 Atypical symptoms, SARS-CoV-2 test results and immunisation rates in 456 residents from eight nursing homes facing a COVID-19 outbreak Long-term care facilities residents 116 10/111 (9) 8.6 Clinical Presentation, Course, and Risk Factors Associated with Mortality in a Severe Outbreak of COVID-19 in Rhode Island, USA, April–June 2020 New Jersey hospital and university employees 829 27/41 (65.9) 3.3 Prevalence of SARS-CoV-2 infection in previously undiagnosed health care workers at the onset of the U.S. COVID-19 epidemic Italy healthcare workers 1,573 17/139 (12.2) 1.1 Characteristics of 1573 healthcare workers who underwent nasopharyngeal swab testing for SARS-CoV-2 in Milan, Lombardy, Italy New York city jail system 978 58/568 (10.2) 5.9 COVID-19 in the New York City Jail System: Epidemiology and Health Care Response, March–April 2020 Boston homeless shelter 408 129/147 (87.8) 31.6 Prevalence of SARS-CoV-2 infection in residents of a large homelss shelter in boston India military quarantine facilities 26 25/25 (100) 96.2 Spread of COVID-19 by asymptomatic cases: evidence from military quarantine facilities Pediatric patients (< 18 years old) 2,135 94/728 (12.9) 4.4 Epidemiology of COVID-19 among children China Children patients in Wuhan (1day-15 years old) 1,391 27/171 (15.8) 1.9 SARS-CoV-2 infection in children US sailors 4,085 146/736 (19.8) 3.6 Symptom Characterization and Outcomes of Sailors in Isolation After a COVID-19 Outbreak on a US Aircraft Carrier Close contact of 314 Spain patients 753 240/449 (53.5) 31.9 Transmission of COVID-19 in 282 clusters in Catalonia, Spain: a cohort study  下载: 导出CSV
下载: 导出CSV
S2. Studies on characterizing SARS-CoV-2 positive patients containing asymptomatic individuals
Populations Total of
PositiveAsymptomatic positive/total positive,
n (%)Reference Note Kuwait residents 1,096 473/1,096 (43.2) Characteristics, risk factors and outcomes among the first consecutive 1,096 patients diagnosed with COVID-19 in Kuwait 35 presymptomatic UK rehabilitation facility 45 15/45 (33.3) Asymptomatic severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in a rehabilitation facility Patients in Beijing 262 13/262 (4.9) Characteristics of COVID-19 infection in Beijing Patients in Shanghai 328 13/328 (4.0) Follow-up of asymptomatic patients with SARS-CoV-2 infection Residents in South Korea 199 53/199 (26.6) Asymptomatic infection and atypical manifestations of COVID-19: Comparison of viral shedding duration Patients in People’s Hospital of Daofu county 83 18/83 (21.7) A considerable proportion of individuals with asymptomatic SARS-CoV-2 infection in Tibetan population Children in Zhejiang
(1–16 years old)36 10/36 (28) Clinical and epidemiological features of 36 children with coronavirus disease 2019 Children in Kuwait 134 91/134 (67.9) Clinical characteristics of pediatric SARS-CoV-2 infection and coronavirus disease 2019 (COVID-19) in Kuwait 3 presymptomatic Bahrain patients and their contacts 320 index cases
1,289 positive contacts160/320 (50)
1,127/1,289 (87.4)The high prevalence of asymptomatic SARS-CoV-2 infection reveals the silent spread of COVID-19 Air passengers to Brunei 138 16/138 (11.6) High proportion of asymptomatic and presymptomatic
COVID-19 infections in air passengers to Brunei
下载: 导出CSV
Table 1. Meta-analysis studies on asymptomatic COVID-19 cases
Total number of studies included % of asymptomatic
individualsNote Reference Publication time 6 24.2 (SD, 22.06) 34 studies were included in the qualitative synthesis, and 17 studies (13 case reports and 4 case series) for meta-analysis contained CT or lab test results. Individuals with normal radiology results were significantly younger (19.59 ± 17.17 years) than patients with abnormal radiology results (39.14 ± 26.70 years). Data from 6 case series were used to calculate the percentage of asymptomatic individuals Ref [4] June 17, 2020 41 15.6 (95% CI: 10.1–23.0) 180 asymptomatic individuals reported from 10 studies included 48.9% pre-symptomatic individuals. 24: all ages, 9% 11: children, 27.7% 3: older adults, 28.3% 4: pregnant women, 49.9% Ref [36] July 21, 2020 79 20 (95% CI: 17–25) 7 studies screening all potentially exposed people in the defined populations and followed-up after testing, 31% (59% CI: 26%–37%) remained asymptomatic Ref [38] July 28, 2020 13 17 (95 CI : 14–20) 4% in Korea to 40% in Vo, Italy, and in an aged care facility in the United States Non-aged care, 16% and aged care, 21%. Ref [37] September 13, 2020 16 48.2 (95% CI: 30.0–67.0)
with significant heterogeneity
noted among studies. Actual
proportion of asymptomatic
cases, 31.1%8 studies with age subgroup analysis, children, 49.6%; adults, 30.3%; and older adults, 16.9%. 39% prevalence of true asymptomatic cases versus 15.3% of pre-symptomatic cases in 10 studies Ref [41] January 20, 2021 28 25 (95% CI: 16–38) Ref [39] March 23, 2021 390 35.1 (95% CI: 30.7–39.9) 42.8% of cases without symptoms at the time of testing. Children: 46.7% Older adults: 19.7% Comorbidities had significantly lower asymptomaticity compared with cases without underlying medical conditions. Ref [40] August 10, 2021 Note. SD, standard deviation; CI , confidence interval; CT, computed tomography.
下载: 导出CSV
-
[1] Zhou P, Yang XL, Wang XG, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature, 2020; 579, 270−3. doi: 10.1038/s41586-020-2012-7 [2] Hu B, Guo H, Zhou P, et al. Characteristics of SARS-CoV-2 and COVID-19. Nat Rev Microbiol, 2021; 19, 141−54. doi: 10.1038/s41579-020-00459-7 [3] Huang DZ, Lian XJ, Song FE, et al. Clinical features of severe patients infected with 2019 novel coronavirus: a systematic review and meta-analysis. Ann Transl Med, 2020; 8, 576. doi: 10.21037/atm-20-2124 [4] Kronbichler A, Kresse D, Yoon S, et al. Asymptomatic patients as a source of COVID-19 infections: A systematic review and meta-analysis. Int J Infect Dis, 2020; 98, 180−6. doi: 10.1016/j.ijid.2020.06.052 [5] Nikolai LA, Meyer CG, Kremsner PG, et al. Asymptomatic SARS Coronavirus 2 infection: Invisible yet invincible. Int J Infect Dis, 2020; 100, 112−6. doi: 10.1016/j.ijid.2020.08.076 [6] Gudbjartsson DF, Helgason A, Jonsson H, et al. Spread of SARS-CoV-2 in the Icelandic population. N Engl J Med, 2020; 382, 2302−15. doi: 10.1056/NEJMoa2006100 [7] Lavezzo E, Franchin E, Ciavarella C, et al. Suppression of a SARS-CoV-2 outbreak in the Italian municipality of Vo'. Nature, 2020; 584, 425−9. doi: 10.1038/s41586-020-2488-1 [8] Abraha HE, Gessesse Z, Gebrecherkos T, et al. Clinical features and risk factors associated with morbidity and mortality among patients with COVID-19 in northern Ethiopia. Int J Infect Dis, 2021; 105, 776−83. doi: 10.1016/j.ijid.2021.03.037 [9] Ing AJ, Cocks C, Green JP. COVID-19: in the footsteps of Ernest Shackleton. Thorax, 2020; 75, 693−4. doi: 10.1136/thoraxjnl-2020-215091 [10] Mizumoto K, Kagaya K, Zarebski A, et al. Estimating the asymptomatic proportion of coronavirus disease 2019 (COVID-19) cases on board the Diamond Princess cruise ship, Yokohama, Japan, 2020. Euro Surveill, 2020; 25, 2000180. [11] Sutton D, Fuchs K, D'Alton M, et al. Universal screening for SARS-CoV-2 in women admitted for delivery. N Engl J Med, 2020; 382, 2163−4. doi: 10.1056/NEJMc2009316 [12] Cruz-Lemini M, Perez EF, De La Cruz Conty ML, et al. Obstetric outcomes of SARS-CoV-2 infection in asymptomatic pregnant women. Viruses, 2021; 13, 112. doi: 10.3390/v13010112 [13] Hcini N, Maamri F, Picone O, et al. Maternal, fetal and neonatal outcomes of large series of SARS-CoV-2 positive pregnancies in peripartum period: A single-center prospective comparative study. Eur J Obstet Gynecol Reprod Biol, 2021; 257, 11−8. doi: 10.1016/j.ejogrb.2020.11.068 [14] Wong J, Abdul Aziz ABZ, Chaw L, et al. High proportion of asymptomatic and presymptomatic COVID-19 infections in air passengers to Brunei. J Travel Med, 2020; 27, taaa066. doi: 10.1093/jtm/taaa066 [15] Lytras T, Dellis G, Flountzi A, et al. High prevalence of SARS-CoV-2 infection in repatriation flights to Greece from three European countries. J Travel Med, 2020; 27, taaa054. doi: 10.1093/jtm/taaa054 [16] Ren RQ, Zhang YP, Li Q, et al. Asymptomatic SARS-CoV-2 infections among persons entering China from April 16 to October 12, 2020. JAMA, 2021; 325, 489−92. doi: 10.1001/jama.2020.23942 [17] Arons MM, Hatfield KM, Reddy SC, et al. Presymptomatic SARS-CoV-2 infections and transmission in a skilled nursing facility. N Engl J Med, 2020; 382, 2081−90. doi: 10.1056/NEJMoa2008457 [18] Kimball A, Hatfield KM, Arons M, et al. Asymptomatic and presymptomatic SARS-CoV-2 infections in residents of a long-term care skilled nursing facility - King County, Washington, March 2020. MMWR Morb Mortal Wkly Rep, 2020; 69, 377−81. doi: 10.15585/mmwr.mm6913e1 [19] Beiting KJ, Huisingh-Scheetz M, Walker J, et al. Management and outcomes of a COVID-19 outbreak in a nursing home with predominantly Black residents. J Am Geriatr Soc, 2021; 69, 1155−65. doi: 10.1111/jgs.17126 [20] Blain H, Gamon L, Tuaillon E, et al. Atypical symptoms, SARS-CoV-2 test results and immunisation rates in 456 residents from eight nursing homes facing a COVID-19 outbreak. Age Ageing, 2021; 50, 641−8. doi: 10.1093/ageing/afab050 [21] Atalla E, Zhang RN, Shehadeh F, et al. Clinical presentation, course, and risk factors associated with mortality in a severe outbreak of COVID-19 in Rhode Island, USA, April-June 2020. Pathogens, 2020; 10, 8. doi: 10.3390/pathogens10010008 [22] Baggett TP, Keyes H, Sporn N, et al. Prevalence of SARS-CoV-2 infection in residents of a large homeless shelter in Boston. JAMA, 2020; 323, 2191−2. doi: 10.1001/jama.2020.6887 [23] Harris BHL, Zuhair M, Di Giovannantonio M, et al. Asymptomatic severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in a rehabilitation facility: evolution of the presence of nasopharyngeal SARS-CoV-2 and serological antibody responses. J Infect Dis, 2021; 223, 192−6. doi: 10.1093/infdis/jiaa610 [24] Oran DP, Topol EJ. Prevalence of asymptomatic SARS-CoV-2 infection. Ann Intern Med, 2021; 174, 286−7. doi: 10.7326/L20-1280 [25] Almadhi MA, Abdulrahman A, Sharaf SA, et al. The high prevalence of asymptomatic SARS-CoV-2 infection reveals the silent spread of COVID-19. Int J Infect Dis, 2021; 105, 656−61. doi: 10.1016/j.ijid.2021.02.100 [26] Marks M, Millat-Martinez P, Ouchi D, et al. Transmission of COVID-19 in 282 clusters in Catalonia, Spain: a cohort study. Lancet Infect Dis, 2021; 21, 629−36. doi: 10.1016/S1473-3099(20)30985-3 [27] Stout RL, Rigatti SJ. Seroprevalence of SARS-CoV-2 antibodies in the US adult asymptomatic population as of September 30, 2020. JAMA Netw Open, 2021; 4, e211552. doi: 10.1001/jamanetworkopen.2021.1552 [28] Lei Q, Li Y, Hou HY, et al. Antibody dynamics to SARS-CoV-2 in asymptomatic COVID-19 infections. Allergy, 2021; 76, 551−61. doi: 10.1111/all.14622 [29] Matusali G, Colavita F, Lapa D, et al. SARS-CoV-2 serum neutralization assay: a traditional tool for a brand-new virus. Viruses, 2021; 13, 655. doi: 10.3390/v13040655 [30] Manenti A, Maggetti M, Casa E, et al. Evaluation of SARS-CoV-2 neutralizing antibodies using a CPE-based colorimetric live virus micro-neutralization assay in human serum samples. J Med Virol, 2020; 92, 2096−104. doi: 10.1002/jmv.25986 [31] Wang PF, Liu LH, Nair MS, et al. SARS-CoV-2 neutralizing antibody responses are more robust in patients with severe disease. Emerg Microbes Infect, 2020; 9, 2091−3. doi: 10.1080/22221751.2020.1823890 [32] Choe PG, Kim KH, Kang CK, et al. Antibody responses 8 months after asymptomatic or mild SARS-CoV-2 infection. Emerg Infect Dis, 2021; 27, 928−31. doi: 10.3201/eid2703.204543 [33] Choe PG, Kang CK, Suh HJ, et al. Waning antibody responses in asymptomatic and symptomatic SARS-CoV-2 infection. Emerg Infect Dis, 2021; 27, 327−9. doi: 10.3201/eid2701.203515 [34] Milani GP, Dioni L, Favero C, et al. Serological follow-up of SARS-CoV-2 asymptomatic subjects. Sci Rep, 2020; 10, 20048. doi: 10.1038/s41598-020-77125-8 [35] Kato Y, Bloom NI, Sun PF, et al. Memory B-cell development after asymptomatic or mild symptomatic SARS-CoV-2 infection. J Infect Dis, 2022. [36] He JJ, Guo YF, Mao RC, et al. Proportion of asymptomatic coronavirus disease 2019: A systematic review and meta-analysis. J Med Virol, 2021; 93, 820−30. doi: 10.1002/jmv.26326 [37] Byambasuren O, Cardona M, Bell K, et al. Estimating the extent of asymptomatic COVID-19 and its potential for community transmission: Systematic review and meta-analysis. Off J Association of Med Microbiol Infect Dis Canada, 2020; 5, 223−34. [38] Buitrago-Garcia D, Egli-Gany D, Counotte MJ, et al. Occurrence and transmission potential of asymptomatic and presymptomatic SARS-CoV-2 infections: A living systematic review and meta-analysis. PLoS Med, 2020; 17, e1003346. doi: 10.1371/journal.pmed.1003346 [39] Alene M, Yismaw L, Assemie MA, et al. Magnitude of asymptomatic COVID-19 cases throughout the course of infection: A systematic review and meta-analysis. PLoS One, 2021; 16, e0249090. doi: 10.1371/journal.pone.0249090 [40] Sah P, Fitzpatrick MC, Zimmer CF, et al. Asymptomatic SARS-CoV-2 infection: A systematic review and meta-analysis. Proc Natl Acad Sci USA, 2021; 118, e2109229118. doi: 10.1073/pnas.2109229118 [41] Syangtan G, Bista S, Dawadi P, et al. Asymptomatic SARS-CoV-2 carriers: a systematic review and meta-analysis. Front Public Health, 2021; 8, 587374. -
 22241Supplementary Materials.pdf
22241Supplementary Materials.pdf

-

 点击查看大图
点击查看大图
图(1) / 表ll (3)
计量
- 文章访问数: 490
- HTML全文浏览量: 166
- PDF下载量: 48
- 被引次数: 0

 Quick Links
Quick Links