

 下载:
下载:

-
Lead occurs naturally in the environment and enters the atmosphere during the production of coal, oil, iron, steel, and batteries, as well as from smelters, solid waste, and tobacco smoke. Because of human activities like road constructions and the increase of motor vehicles, environmental levels of lead increased more than 100-fold over the past three centuries[1]. Gas and dust mixtures in coal mines involve particles of air-borne lead that are inhaled by the miners. Ingestion and inhalation are the primary routes of lead entering the body[2]. The distribution of lead in the body is route independent and, in adults, approximately 94% of the total body burden of lead is in the bones compared to approximately 73% in children. Lead in blood is primarily deposited in red blood cells[3]. The mechanism of lead-induced oxidative stress involves the depletion of antioxidative reserves and the increased generation of reactive oxygen species. Lead inactivates glutathione by binding to glutathione's sulfhydryl group, which causes glutathione replenishment to become inefficient, thereby increasing oxidative stress. Prolonged exposure to lead insidiously affects the different body systems leading to hematopoietic, cardiovascular, renal, and hepatic dysfunction[4].
The pharmacokinetics of lead in humans is complex. After being absorbed, lead is distributed throughout the body, and is often stored in soft organs like the liver, kidney, and brain. Lead levels are measured in the blood, hair, urine, and saliva. Measuring blood lead is the most common method used for confirming the presence of lead. The elimination half-lives for inorganic lead in blood and bone are approximately 30 days and 27 years, respectively. Lead is mainly excreted through the urine ( > 90%) while lesser amounts are eliminated via the feces, sweat, hair, and nails[5]. The threshold for occupational lead exposure should not exceed 30 μg/dL during random blood testing, and the National Institute for Occupational Safety and Health (NIOSH) in the United States urged that the normal blood lead level for adults should be lower than 5 μg/dL[6]. Workers in polluted environments have higher baseline blood lead levels due to long-term exposure. Nevertheless, when those workers are directly exposed to lead, its values can elevate from the baseline quickly and reach levels where serious health damage may be occurring, even if there are no symptoms[7].
Research Design A nonrandomized control group pretest-posttest sample design was used[8]. The control group included miners who returned to work after five days of holiday; baseline control measurements were made before the start of the shift. The first group included miners who worked in the coal mine for a single day. The second and third groups included miners who worked in the coal mine for two and three consecutive days, respectively. Miners from all three experimental groups started to work on Monday after a free weekend. Experimental measurements were made on Monday (first group), Tuesday (second group), and Wednesday (third group), after the shift in the coal mine.
Sample Description The study involved 169 male coal miners from the Velenje Coal mine. The health condition of each miner was confirmed by his general practitioner who provided written confirmation that the miner's health status is adequate. Ninety-four (n = 94) coal miners passed strict inclusion criteria and were a) non-smokers, b) without chronic diseases, and c) without any drug therapy. The selected groups of miners were not significantly different in their ages and (P = 0.696) number of working years (P = 0.552) in the coal mine. Informed consent was obtained from each study participant.
The Use of 8-isoprostane as an Oxidative Stress Marker 8-isoprostane is a prostaglandin-like compound belonging to the F2-isoprostane class that is produced in vivo by the free radical-catalyzed peroxidation of arachidonic acid. Literature suggests that of all oxidized fatty acids, the best indicators of oxidative stress in vivo are currently the F2-isoprostanes. Available data indicate that quantification of F2-isoprostanes in either plasma or urine gives a highly precise and accurate index of oxidative stress. 8-isoprostane was used many times as a biomarker of lipid peroxidation and oxidative stress.
8-isoprostane in Plasma Blood ethylenediamine-tetraacetic acid (EDTA) samples were obtained from the antecubital vein. Plasma was supplemented with 0.005% butylated hydroxytoluene and stored at -80 ℃. 8-isoprostane was measured with competitive enzyme immunoassay for the quantification of 8-isoprostane by the manufacturer's instructions (8-Isoprostane EIA KIT, Cayman Chemical Company, USA).
Blood Lead Analysis Blood for lead determination was taken into special tubes for trace elements (Beckton Dickinson). The samples were stored in polyethylene tubes at -80 ℃ until further processing. Blood samples were analyzed by inductively coupled plasma mass spectrometry (Agilent 7700x ICP-MS). Instrumental limit of detection (LOD) for lead was 0.2 ng/mL. For quality control, the RIQAS Trace Elements in Blood (RANDOX) control was used.
Statistical Analysis Results were expressed as mean value ± standard deviation or by median and interquartile range. Key demographic data between groups were compared using the Kruskal-Wallis H test. Differences in blood levels of lead and 8-isoprostane between groups were compared using Mann-Whitney U test. Spearman's correlation coefficient was used to calculate correlation between blood levels of lead and 8-isoprostane. Statistical analysis was performed with IBM SPSS 22.0 software (IBM Corp., Armonk, NY). Statistical significance was assumed at P < 0.05.
This study was approved by the Slovenian National Medical Ethics Committee.
Coal miners were 39.2 ± 4.9 [median 39.0 (IR 35.0-43.0)] years of age and had 11.6 ± 4.8 [median 11.0 (IR 8.0-15.0)] years of working in the coal mine. All miners resided in rural areas surrounding the Velenje coal mine. Regarding education, all miners finished a four-year mining school. Before entering the coal mine shafts, they also had 14 days on-site education, following by 6 months of mentorship. After this, miners started to work on their own, and each year they attend mandatory education about mining safety and technology.
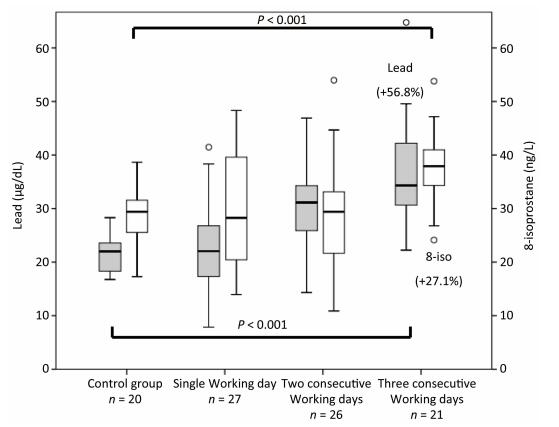
Results in Figure 1 show that 8-isoprostane in plasma was significantly higher in miners at the end of the third consecutive working day (group 3). The median value of 8-isoprostane in plasma in the control group and group 3 was 29.5 (IR 24.7, 32.3) ng/L and 37.5 (IR 33.4, 41.3) ng/L, respectively (P < 0.001). Blood lead levels were significantly higher in miners at the end of the second consecutive working day (group 2). The median blood lead value in the control group and group 2 was 22.0 (IR 18.3, 23.8) μg/dL and 31.0 (IR 25.3, 34.0) μg/dL, respectively (P < 0.001). The highest median blood lead value of 34.5 (IR 30.0, 42.8) μg/dL was measured in group 3 (P < 0.001; in comparison to control group).
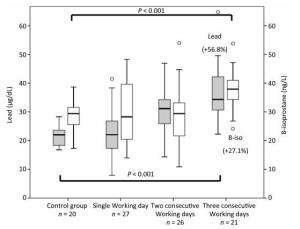
Figure 1. Blood levels of lead (gray boxes) and 8-isoprostane (white boxes) in groups of miners with one, two, or three consecutive working days in the coal mine.
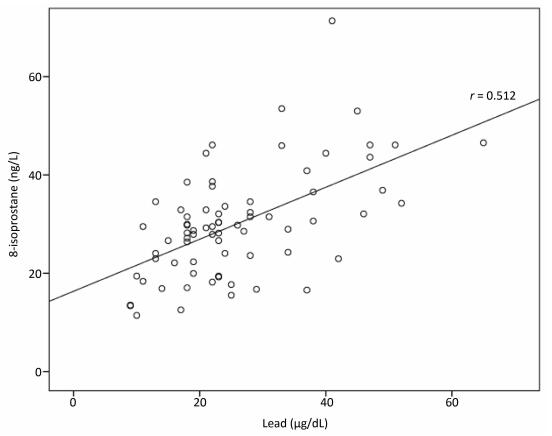
Correlation between blood levels of lead and 8-isoprostane is shown in Figure 2. The Spearman's correlation coefficient resulted in a positive correlation coefficient of medium strength (r = 0.512, P < 0.001).
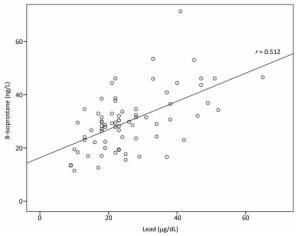
Figure 2. Correlation between blood levels of lead and 8-isoprostane.
Our control group of miners had increased baseline blood lead levels (mean value of 21.7 μg/dL) which were similar to the control group of Al-Neamy et al.[9] with mean blood lead levels of 20 μg/dL and were higher compared to non-exposed controls in Khan et al.[4] with median lead levels of 8.3 μg/dL. Blood lead levels of 10 μg/dL or higher are considered toxic and result in neurological disorders, cognitive impairments, hypertension, and other disorders[6]. Our objective was not to concentrate on long-term exposure to lead but to study its short-term development in the human body. Our results showed that blood lead levels significantly increased from the baseline value after the second consecutive working day. After the third working day we registered additional blood lead increases. Van Eijkeren et al.[7] found that blood lead levels can double or even more from the baseline in a day or two, and that the immediate (few days) elimination to baseline was possible by chelation therapy. Literature also suggests that the percentage and timing of excretion of newly absorbed lead depend on several factors. Therefore, it may also be possible that long-term occupational exposure, workers' preparedness for a potentially strong reaction, removal of the lead source, and perfect renal function, may contribute to similar results.
Blood lead levels were not in total compliance with oxidative stress development as 8-isoprostane increased with a 24 h delay, after the third working day only. This indicates the latency between lead-induced oxidative stress and formation of 8-isoprostane points to the multicausality of oxidative stress in miners and might be triggered by other factors, like hypoxia, increased gas concentrations, or dust particles in the mine atmosphere. Nevertheless, we found a positive correlation of medium strength between blood lead levels and oxidative stress generation. Some previous studies also reported correlations of medium strength. Gurer-Orhan et al.[10] who analyzed battery plants worker, reported antioxidant enzyme correlations with lead of r = 0.62 for catalase and r = 0.64 for glutathione. Khan et al.[4] reported correlation of r = 0.63 for gamma glutamyltransferase (antioxidant enzyme) in metal workers who performed lead smelting operations.
Study Limitations Our intention was to arrange four groups of 30 min. Since we were requested not to interfere with production, we could only follow 47 min after the first working day; 16 min unexpectedly received other assignments and did not work their entire second consecutive working day in the coal mine under increased gas and dust exposure. It was also not possible to arrange for more than 20 min to have a five-day holiday to ensure a larger control group.
Since the participants were all healthy non-smokers and the groups closely matched according to age and working years, we believe that the increase in blood levels of 8-isoprostane and lead clearly represents the influence of longer exposure to mine gases and dust particles. To reduce influence of other conditions such as body fluids lost due to heavy physical work, we measured miners who only excavated coal and did not construct rails for transportation or complete other similar construction or manufacturing tasks. In that manner typical working process of miners represented the control of heavy mining equipment. In addition, study participants were asked to maintain their usual food intake and usual daily activities and to avoid second-hand smoke and drinking alcohol.
The primary constraint of our sampling approach is that posttest differences between groups may be attributable to essential differences between groups rather than to the intervention. To isolate this effect, the basic demographic and health characteristics (age, working experiences, education, residency, being non-smokers, avoidance of passive smoking, no alcohol consumption, without chronic disease and drug therapy, moderate daily activities) were controlled in our control and experimental groups. The inability to control confounding variables (for example, disregard of advice to avoid second-hand smoke, drinking alcohol and strenuous activities) may influence oxidative stress development.
Anticipated elimination of blood lead was not in concordance to the literature, where blood lead half-life elimination of approximately 30 days was reported with no intervention. According to our study, this should have occurred much faster. The only reasonable explanation is that blood lead levels in miners must have dropped to baseline during three or four days of rest (free weekend), because otherwise, the blood lead would reach levels of heavy intoxication in a few weeks. Nevertheless, further studies are warranted to confirm rise and elimination of blood lead and to identify exposure sources and pathways.
For more accurate blood lead and oxidative stress development, it would be better to follow one group of miners for several days to reduce inter-individual factors that may affect the results. It would also be advisable to include additional days of measurement to clarify whether blood lead and 8-isoprostane levels remain constant or continue to rise after the fourth consecutive working day, and to test our hypothesis that newly absorbed lead can be extracted much faster than suggested in literature. Unfortunately, such a study design faces two major problems, as it would interfere with coal mine production and blood samples would need to be taken on several consecutive days which may be ethically questionable.
Our major finding was the significant increase in the 8-isoprostane levels in plasma in coal miners on the third consecutive working day, showing increased oxidative stress after a short-term working exposure. Rising blood lead levels resulted in a correlation of medium strength with oxidative stress generation. Our results show that even a short-term lead exposure can be potentially harmful and should be considered when formulating improvements in working processes.
We would like to thank all miners from the Velenje Coal mine who participated in the research.
The authors declare that they have no conflicts of interest. The authors confirm that the study content was not influenced by the study sponsors.
This study was financed by the Velenje coal mine.
Study design: ZZ, MB, JO; data collection and analysis: ZZ, JO, TF, KS; and manuscript preparation: ZZ, MB, JO, BP.
doi: 10.3967/bes2017.113
-
Abstract: We aimed to investigate the short-term correlation between blood lead levels and oxidative stress generation in coal miners. The study involved 94 male coal miners from the Velenje Coal mine, arranged into four groups: three groups according to the number of consecutive working days, and a fourth control group. Miners who worked for three consecutive days had higher blood levels of lead and 8-isoprostane than the control group (P < 0.001). Correlation between lead and 8-isoprostane was of medium strength (r = 0.512, P < 0.001). Short-term lead environmental exposure can potentially harmful and should be considered when formulating improvements in working processes.
-
Figure 1. Blood levels of lead (gray boxes) and 8-isoprostane (white boxes) in groups of miners with one, two, or three consecutive working days in the coal mine.
-
[1] Chen RH, Wang BQ, Wang ZB, et al. The pollution character analysis and risk assessment for metals in dust and PM10 around road from China. Biomed Environ Sci, 2015; 28, 44-56. http://www.ncbi.nlm.nih.gov/pubmed/25566862 [2] Meyer SA, Kulkarni AP. Hepatotoxicity. In: Introduction to Biochemical Toxicology, vol. 3 (E Hodgson and RC Smart, Eds), New York: John Wiley, 2001; 487-90. [3] Agency for Toxic Substances and Disease Registry. Toxicological profile for lead, US Department of Health and Human services. Atlanta Georgia: US Government Printing, 2005. [4] Khan DA, Qayyum S, Saleem S, et al. Lead-induced oxidative stress adversely affects health of the occupational workers. Toxicol Ind Health, 2008; 24, 611-8. doi: 10.1177/0748233708098127 [5] World Health Organization. Biological indices of lead exposure and body burden. In: IPCS, Inorganic lead, Environmental Health Criteria 165, Geneva, Switzerland: WHO. 1995; 114-8. [6] National Institute for Occupational Safety and Health. Adult Blood Lead Epidemiology & Surveillance (ABLES). https://www.cdc.gov/niosh/topics/ables/description.html. [2017-01-29]. [7] van Eijkeren JC, Olie JD, Bradberry SM, et al. Modeling the effect of succimer (DMSA; dimercaptosuccinic acid) chelation therapy in patients poisoned by lead. Clin Toxicol (Phila), 2017; 55, 133-41. doi: 10.1080/15563650.2016.1263855 [8] Dimitrov DM, Rumrill PD Jr. Pretest-posttest designs and measurement of change. Work 2003; 20, 159-65. https://content.iospress.com/articles/work/wor00285 [9] Al-Neamy FRM, Almehdi AM, Alwash R, et al. Occupational lead exposure and amino acid profiles and liver function tests in industrial workers. Int J Environ Health Res, 2001; 11, 181-8. doi: 10.1080/09603120020047564 [10] Gurer-Orhan H, Sabır HU, Özgünes H. Correlation between clinical indicators of lead poisoning and oxidative stress parameters in controls and lead-exposed workers. Toxicology, 2004; 195, 147-54. doi: 10.1016/j.tox.2003.09.009 -

 点击查看大图
点击查看大图
图(2)
计量
- 文章访问数: 2104
- HTML全文浏览量: 710
- PDF下载量: 150
- 被引次数: 0

 Quick Links
Quick Links