



-
The public health problem caused by disease outbreak cause increasing global concern. Field epidemiology investigation (FEI), which involves dthe timely use of epidemiology to solve urgent public health problems, is a crucial core capacity for the public health workforce[1]. When an acute public health problem occurs, there is an urgent need to identify the origin, path, cases, and vulnerable population, and to implement timely intervention. FEI can be conducted not only for infectious disease epidemics but also for non-communicable events[2] such as poisoning, vaccination accidents, and environmental pollution. While situations do not always meet the statutory standard of a public health emergency, it remains necessary to conduct an investigation to prevent event from becoming a serious public health problem.
In view of the fundamental role of FEI in coping with outbreaks, numerous training programs have been conducted worldwide. This concept has been gradually accepted in China, and a 2-year on-the-job Chinese Field Epidemiology Training Program (CFETP) was established in 2001 by Chinese Center for Disease Control and Prevention. The training model for the CFETP originated from the Epidemiological Information Service (EIS) in the United States established in 1951[3, 4], which was promoted as a global epidemiological training network by the World Health Organization. FEI is viewed as an essential skill that all professionals in a given field should be competent[5], suboptimal investigation and control measures based on it could jeopardize the reputations of public health and government. The response to outbreak of severe acute respiratory syndrome in the early phase of the epidemic in 2003 reflected the severe shortage of well-trained epidemiological professionals in China[6]; therefore, measures were taken to improve the overall competency in the public health system. Since then, the task of conducting FEI in China has been undertaken mainly by the Centers for Disease Control and Prevention (CDCs) at all levels, with multi-sectoral cooperation. However, FEI capacity of CDC professionals remains unclear after years of institutions building and health-related human resource construction.
The results of FEIs are often reported, but there is limited information reflecting the factors associated with FEI in the literature. This study aimed to gather first-hand information regarding FEI capacity and determine factors associated with investigation, via a case study conducted in Heilongjiang province, to provide evidence-based options for future capacity building programs of CDC staff.
A stratified cluster sampling method was used to select CDCs. 2 to 4 counties in each of the 13 city (Prefecture) in Heilongjiang province were selected at random to participate in the study. In total, 40 CDC institutions were sampled. Eligible target participants were the professionals who had worked at the CDCs for more than 1 year and were members of the health emergency detachment of the CDCs. After excluding unqualified participants and incomplete questionnaires, we obtained 1, 507 valid responses. In-depth interviews were conducted among 22 CDC emergency managers to understand the factors affecting FEI, and obtain their opinions about potential causes of hindering personnel capacity building from the perspectives of individual, institution and society.
Of the 1, 507 CDC professionals, 42.40% were men and 57.60% were women. Almost half (47.18%) had completed a college education or higher, and 26.40% had background of preventive medicine education. In addition, 32.58% had conducted FEI more than two times during the preceding year. Furthermore, 27.60% and 43.40% had never participated in training and drills related to epidemic response, respectively. Only 30.92% of the CDC professionals rated themselves as 'good' in terms of FEI capacity (Table 1).
Characteristics N (%) FEI Capacity, n (%) χ 2 P Not Good Good Gender Male 639 (42.40) 429 (67.14) 210 (32.86) 1.958 0.176 Female 868 (57.60) 612 (70.51) 256 (29.49) Age (year) ≤ 40 737 (48.91) 537 (72.86) 200 (27.14) 9.676 0.002 > 40 770 (51.09) 504 (65.45) 266 (34.55) Education level Junior college and below 796 (52.82) 585 (73.49) 211 (26.51) 15.406 0.000 College 643 (42.67) 412 (64.07) 231 (35.93) Master degree or above 68 (4.51) 44 (64.71) 24 (35.29) Majored in preventative medicine Yes 398 (26.40) 222 (55.78) 176 (44.22) 44.749 0.000 No 1, 109 (73.60) 819 (73.85) 290 (26.15) Professional title < Senior title 1, 206 (80.03) 870 (72.14) 336 (27.86) 26.497 0.000 Senior title 301 (19.97) 171 (56.81) 130 (43.19) Work experience ≤ 20 years 1, 036 (68.75) 744 (71.81) 292 (28.19) 11.625 0.001 > 20 years 471 (31.25) 297 (63.06) 174 (36.94) The frequency of FEI ≤ 2 times 1, 017 (67.49) 806 (79.25) 211 (20.75) 151.601 0.000 > 2 times 490 (32.51) 235 (47.96) 255 (52.04) Training Yes 1, 091 (72.40) 718 (65.81) 373 (34.19) No 416 (27.60) 323 (77.64) 93 (22.36) 19.742 0.000 Drill Yes 853 (56.60) 544 (63.77) 309 (36.23) 25.875 0.000 No 654 (43.40) 497 (75.99) 157 (24.01) CDC level Municipal 330 (21.90) 231 (70.00) 99 (30.00) 0.168 0.736 District/county 1, 177 (78.10) 810 (68.82) 367 (31.18) All participants 1, 507 1, 041 (69.08) 466 (30.92) Table 1. Characteristics of the Questionnaire Respondents and FEI Capacity (n = 1, 507)
The dependent variable in the study was measured using the item, 'What do you think of your overall capacity to perform field epidemiology investigation?' The answer was given using a 5-point Likert scale ranging from 1 ('very poor') to 5 ('very good'). For modelling purposes, we created a dichotomous variable, where respondents with 1, 2, and 3 on the Likert scale were classified as 'not good', and 4, 5 were classified as 'good'. The independent variables included sex, age, educational level, professional title, work time, EFI frequency, training, drills, and the level of CDC institutions. Logistic regression was conducted to identify factors influencing individual FEI capacity (performed using SPSS 18.0). The significance level was set at P < 0.05.
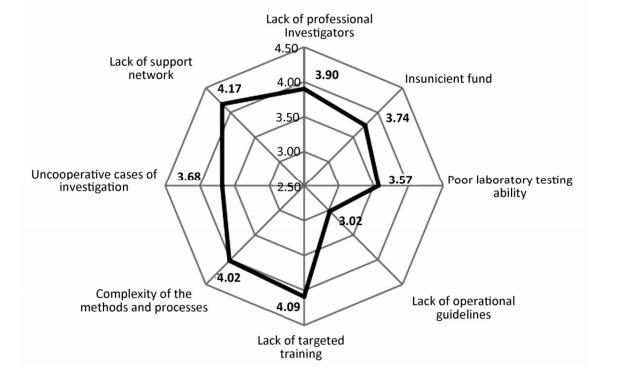
Participants were asked to rate the degree of factors (8 items) hindering EFI performance, including (1) lack of professional investigators, (2) complexity of methods and processes, (3) insufficient funding, (4) lack of operational guidelines, (5) poor laboratory testing ability, (6) lack of training and drills, (7) uncooperative cases, and (8) lack of a support network. The scores of the 8 items ranged from 1 to 5.
The results of the multivariate analysis suggested that participants who had conducted FEI more than two times (OR = 3.478, 95% CI: 2.724-4.440), who majored in preventative medicine (OR = 1.85, 95% CI: 1.43-2.39), and who had been trained to conduct investigations (OR = 1.57, 95% CI: 1.17-2.09) tended to exhibit higher self-ratings compared with other participants.
This study showed that only 26.40% of the participants had education background in the field of preventive medicine. Field epidemiology is an interdisciplinary methodology, and the knowledge domains of FEI include epidemiology, statistics, clinical medicine, social science, management, and communication. Professional background in preventive medicine indicated that such participants had completed basic education in most of these necessary knowledge in colleges, which would contribute to the capacity to address the complexity of FEI tasks. In addition, FEI capacity could also be improved through on-the-job public health practice and formal professional training. FEI is an interdisciplinary field, and the technology used in FEI is complex and varies according to the situation, requiring both individual and teamwork skills. Further, experience in emergency response activities is invaluable to improve the capacity of CDC workforce during complex investigations. Indeed, FEI practice as a must for training is an important course for both EIS and CFETP, in which 'keep learning by doing' is promoted[3, 6]. Participation in targeted FEI training programs was another key factor in self-rated FEI capacity for public health workforce. Professionals should gain theoretical knowledge, practical skills and abilities in systematic formal training for the response to public health emergencies. However, the schedules of grassroots CDC professionals are often occupied by heavy workloads and daily routines, and training often gives place to organization's other priorities which usually incorporated only a small number of investigative skills.
In the current study, participants were asked to score 8 items related with the factors that hinder FEI (Figure 1). Lack of a support network was shown to be the most significant barrier to FEI, with a score of 4.17. The law endows CDC investigators with a duty to conduct FEI in China, but they often encounter resistance due to the lack of concretely stipulated laws and regulations that meet the specific requirement of FEI. Moreover, the investigations require cooperation with other departments and access to premises or records related to emergency[7]; however, it is difficult to obtain substantial support when there is a disagreement between departments, which hinders the availability of resources within a community and limits timely intervention. Previous studies have shown an overlap of responsibilities, poor communication between CDCs and other health sectors[8]. Furthermore, rising concern on privacy also plays a role in causing difficulties that hinder FEI.
Figure 1. Degree of hindrance of negative factors to FEI.
Another important obstructive factor was the lack of targeted training (4.09); consistent with the findings of the logistic regression analysis. The complexity of the methods and processes of FEI (4.02) was the third most important obstacle reported. In addition, previous research has shown that the capabilities of data collection and statistical analysis are always important but weak in public health workforce[3, 9]. Local CDC professionals are obliged to conduct investigations; however, even those who have performed FEI for numerous times may not be valued as epidemiologists. In fact, grass-roots investigators usually have a lower education level and lack of training and investigation experience; therefore, the methods and processes involved in conducting FEI are usually complicated and difficult for them. When an investigation is in a jam or does not know how to execute it, grass-roots CDCs have to turn to the higher level for help, and this may miss the best time for intervene.
The findings of the quantitative investigation were partly verified by the interviews. Investigators often lacked of sufficient and targeted training for FEI. Moreover, support networks were not conducive to the implementation of FEI. Investigators are empowered to conduct investigations on site and gain access to data which was private and confidential, and this requires supports from the public, communities, organizations, and other government agencies; however, they are often challenged by those who question their rationality for enquiries, particularly when interests are threatened. Other unfavourable factors for the investigation were as follows: heavy work schedules and lower incomes led to increased staff turnover and negative attitudes; new staff members' education background did not match the job requirements when they were recruiteds; and deficiency of laboratory capacity at the district and county level, resulting in difficulties in providing accurate and timely support for investigations.
In practice, FEI is often conducted by a team of professionals through cooperation[9]. Field epidemiology is a branch of applied epidemiology, but the lack of sufficiently competent staff in this area has been identified as a major challenge in the public health field for many years[10]. Not all professionals are expected to be equally capable in all steps and types of investigation, but they should have the capacity to conduct epidemiological surveys[6]. So, It is necessary to develop a work manual for FEI, which is scarce in China now, to describe the basic skills in each step of FEI, address the knowledge and skills deficiency and outline the detailed tasks to be accomplished for each investigation step. In addition, new tools, such as epidemiological analysis and investigation software based on artificial intelligence, should be developed and made easy available for investigators, to reduce the barriers to FEI resulting from weaknesses in identifying biological characteristics of diseases, and application of statistical method.
In conclusion, almost 70% of the professionals in the current study were not confident in their FEI capacity. In addition, FEI experience, formal training, and educational background had influences on FEI capacity. Moreover, defective support network, the complexity of FEI methods and processes, and lack of training and drills were considered as major factors hindering FEI. It is necessary to consider the key obstruction of factors in decision making, personnel recruitment systems involving highly relevant educational background should be established, tasks and responsibilities should be clarified in multi-sectoral collaboration and co-operation in FEI.
The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the article. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
The authors wish to thank those who participated in the questionnaire survey and qualitative interview.
HTML
Scientific Research of Ministry of Health of China 201002028

 Quick Links
Quick Links
 DownLoad:
DownLoad: