


-
The current standard treatment of nasopharyngeal carcinoma (NPC) is radiation therapy or a combination of radiation and chemotherapy. Although the initial rate of response and the five-year survival rate for early stage patients with NPC are promising when compared to other malignancies, recurrences and post-treatment metastases often appear in advanced-stage NPC patients. Patients with NPC recurrence and metastasis have poor prognosis, and no curative therapeutic options are available. There is substantial evidence that Epstein-Barr virus (EBV) plays an important role in NPC development[1,2]. A limited array of EBV antigens, including latent membrane proteins (LMP) 1 and 2, and EBV nuclear antigen 1 (EBNA1), are expressed in NPC cells[3]. Of these, LMP2 epitopes are the most frequently recognized by CD8+ cytotoxic T lymphocytes (CTLs)[4], and CTLs specific to LMP2 have been shown to efficiently kill NPC cells both in vivo and in vitro[5–7]. The results of these studies suggest that patients with NPC could benefit from immunotherapy.
DCs are the most potent antigen-presenting cells, are widely distributed throughout the body, and have the ability to stimulate both native and secondary immune responses to antigen(Ag)-specific T cells[8–10]. Genetic modification of DCs with genes encoding immunoregulatory molecules provides a potential approach for Ag-specific T cell-mediated immunity by selectively targeting antigen-specific T cells[11,12]. A cellular vaccine based on DCs pulsed with LMP2-antigen has previously been reported at the Global Virus Networks meeting in 2015[13]. The results showed that the vaccine induced specific CTLs were sufficient for NPC control and treatment.
With these recent studies in mind, we designed and conducted a pilot clinical study to test the biological effects of LMP2-DCs in 29 patients with NPC after conventional radiotherapy and chemotherapy. We report here the promising immunological and clinical results.
-
Autologous mononuclear cells were isolated by the Ficoll-Hypaque density gradient centrifugation (Pharmacia, 30 min, 4 °C, 800 ×g from peripheral blood). Peripheral blood monocytes (PBMCs) were cultured in six-well plates at 5 × 106 cells/well (37 °C, 5% CO2) for 2 h. Supernatant PBMCs were removed, and adherent monocytes were cultured for 7 d in six-well plates in 3 mL/well with 500 U/mL IL-4 (Pepretech) and 500 U/mL GM-CSF (Pepretech) in a DC medium (Cell-GRO® DC). On day 3, half of the medium was replaced with fresh DC medium. The morphology of monocytes was observed by optical microscope.
The immature DCs were aspirated and harvested (250 ×g, 10 min) on day 7 and then transferred to new 6-well plates at 106 cells/well. DCs were then infected with rAd-LMP2 (Shen Zhen Tsinghua Yuanxing Pharmaceutical Co, Ltd, MOI100) for 2 h. DCs expressing LMP2 (LMP2-DCs) were induced to maturity by replacing cells with fresh medium containing IL-4 (500 U/mL), GM-CSF (500 U/mL), and tumor necrosis factor-alpha (TNF-α 400 U/mL Pepretech) for another two days. Mature LMP2-DCs (mLMP2-DCs) were stained with immunofluorescence antibodies CD83, CD86, and HLA-DR (BD Bioscience) and then analyzed using flow cytometry. The mLMP2-DCs were harvested by centrifugation at 250 × g for 10 min.
The pellets of mLMP2-DCs (250 ×g, 10 min) were collected and washed with PBS three times and then resuspended in freezing medium containing 10% dimethyl sulfoxide (Sigma), 20% autologous serum, and 70% DC medium 2 × 106/mL (0.5 mL/dosage). Cells were frozen at −80 °C overnight using a Cryo 1 °C Freezing Container (Nalgene) filled with isopropanol. The frozen cells were then transferred to liquid nitrogen.
-
Cell smears were prepared from mLMP2-DCs and fixed in cold acetone at 4 °C for 15 min. The slides were allowed to dry in air and were incubated with anti-LMP2 monoclonal antibody (Santa Cruz Biotechnology, diluted 1:100 with phosphate buffer saline, PBS) at 37 °C for 40 min. After primary antibody incubation, the slides were washed three times with PBS. Biotin-conjugated anti-human IgG antibody (diluted 1:100 with PBS) was added to the slide at 37 °C for 40 min, and the slides were washed three times with PBS. Horseradish/peroxidase-conjugated anti-biotin IgG antibody (diluted 1:100 with PBS) was added to the slides at 37 °C for 40 min. The slides were incubated with diaminobenzidine (Sigma) and H2O2 for 10 min and washed in distilled water. The slides were then air dried and examined under an optical microscope.
-
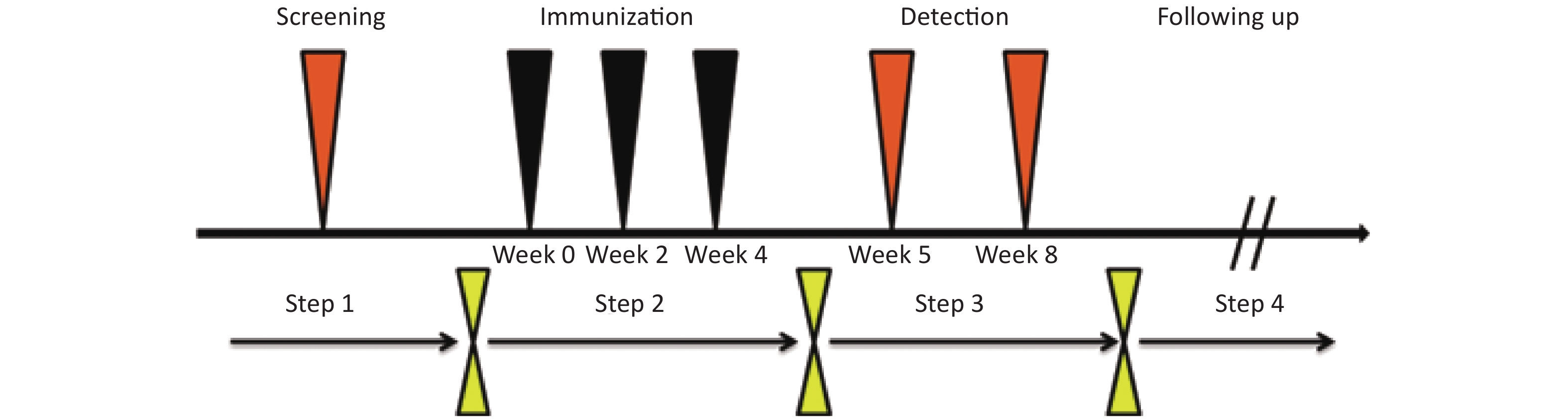
We performed a pilot study in patients with NPC to determine the safety, immunogenicity, and clinical efficacy of a mLMP2-DCs vaccine. Eligible cases were histopathologically confirmed cases of NPC (stage I-IV), in which the patient’s age was ≤ 70 years and the patient was at least three months post-chemotherapy and -radiotherapy and at least three months into remission with no acute diseases and normal function of liver, kidney, and marrow. Enrollment was allowed at least three months after conventional radiotherapy and chemotherapy. The demographic information regarding all patients is summarized in Supplementary Table S1 available in www.besjournal.com. PBMCs were harvested for LMP2-DCs vaccine manufacturing at the Clinical Cell and Vaccine Production Facility at the People's Hospital of Guangxi Zhuang Autonomous Region. Vaccines were cryopreserved at −196 °C, thawed and washed before administration. Patients with NPC received three doses of the vaccine (≥ 5 × 105 DCs/dose) intradermally every two weeks. The procedure is shown in Figure 1. Patients with NPC were evaluated every two weeks. Safety was determined using the China Food and Drug Administration Grading Standard of Adverse Events in Clinical Trials (
http://www.cde.org.cn/zdyz.do?method=list ). Clinical indications, including breathing, heart rate, blood pressure, and body temperature were monitored. The temperature was documented when fever occurred (body’s temperature over 38 °C). Subjects underwent full examination (blood, urine, hepatorenal function, electrocardiogram) pre- and post-immunotherapy.Patient ID Sex Age Stage at
enrollmentTime after radiotherapy and
chemotherapy (months)1 M 37 I 9 2 F 39 I 3 3 M 37 I 9 4 M 49 II 6 5 F 61 II 3 6 F 37 II 3 7 M 34 II 6 8 F 34 II 7 9 F 53 II 3 10 F 34 II 5 11 F 61 II 3 12 F 30 II 8 13 F 51 II 3 14 M 44 II 3 15 M 66 III 8 16 M 36 III 4 17 M 24 III 9 18 F 35 III 6 19 M 39 III 3 20 M 36 III 6 21 F 37 III 5 22 M 55 III 3 23 F 60 III 9 24 F 33 III 4 25 M 28 IV 7 26 M 33 IV 3 27 M 36 IV 9 28 F 50 IV 8 29 M 30 IV 3 Table S1. Characteristics of NPC patients in this study
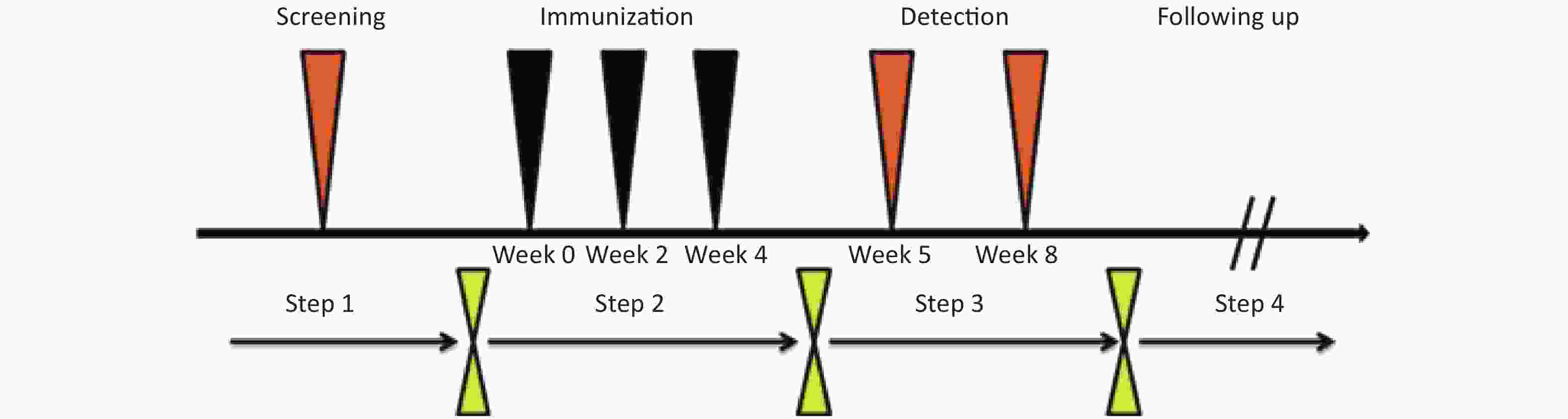
Figure 1. Steps of the study. Yellow triangle: border of different trial stage; Black triangle: time of immunotherapy; Orange triangle: time of LMP2 specific cellular immunity test.
This study was approved by Institutional Review Board of the People's Hospital of Guangxi Zhuang Autonomous Region on September 24, 2008. All the procedures meet the ethics requirement. All patients gave written informed consent prior to initiation of any study procedures.
-
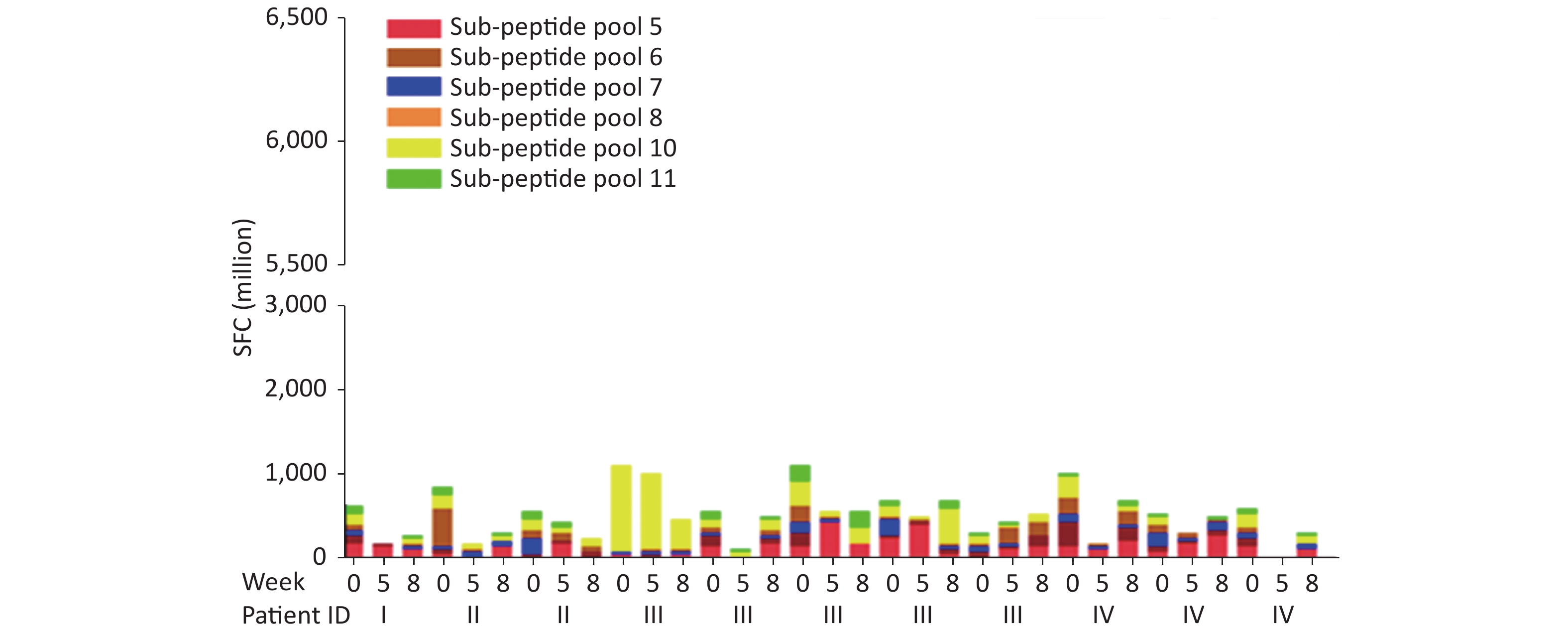
PBMCs were isolated from immunized patients by Ficoll-Hypaque density gradient centrifugation at week 0 and at 5 and 8 weeks 800 ×g, 15 min non-stop). Specific responses of CTLs to LMP2 were analyzed using human IFN-γ Elispot kit (BD Bioscience). The kit was used according to the manufacturer's protocol. PBMCs were plated at 2 × 105 cells/well, and six sub-peptide pools (Supplementary Table S2 available in www.besjournal.com) screened from the LMP2 pool were added to the wells at a final concentration of 5 μg/mL per peptide for overnight stimulation. Wells containing media alone were used as negative controls, and cells incubated with 1 μg/mL PhosPhomolybdic Acid (PMA) and ionomycin (Ion) (Da Kewei Co, Ltd) were used as positive controls. The chromogenic reaction was terminated by distilled water as soon as spots were ready for counting. The plate was allowed to dry in air for 10–30 min. The number of spots per well were read using Bioreader 4000 PRO, and statistic data analysis (GraphPad Prism 5) was performed. A positive response was defined as a two-fold or greater increase in the number of spot-forming cells per million PBMC in immunized wells compared to pre-immunized wells. Additionally, we tested the plasma for changes of the EBV DNA genome copies and titers of IgA antibody to VCA. If the titers of IgA were elevated more than four-fold compared to levels in pre-immunization, the difference was considered significant.
Sub-peptide pool Sequences of amino
acids in LMP2Purity (%) 5 MGSLEMVPM 95 5 LPVIVAPYL 95 5 PYLFWLAAI 95 5 FTASVSTVV 95 5 IEDPPFNSL 95 5 RRRWRRLTV 95 5 RRWRRLTVC 95 5 RRLTVCGGIMF 95 5 TVCGGIMFL 95 5 SSCSSCPLSKI 95 5 ILLARLFLY 95 5 TYGPVFMCL 95 5 LTAGFLIFL 95 5 LIVDAVLQL 95 6 LFWLAAIAASCF 75 6 AAIAASCFTASV 75 6 STVVTATGLALS 75 6 LALSLLLLAAVA 75 7 LTAVVTFFAICL 75 7 FNSLLFALLAAA 75 7 LFALLAAAGGLQ 75 7 CGGIMFLACVLV 75 7 MFLACVLVLIVD 75 8 CVLVLIVDAVLQ 75 8 TVVSMTLLLLAF 75 8 MTLLLLAFVLWL 75 8 LLTLAAALALLA 75 8 LTTMFLLMLLWT 75 10 AGILFILAILTE 75 10 GLLTMVAGAVWL 75 10 MVAGAVWLTVMS 75 10 SAWILTAGFLIF 75 10 FLIFLIGFALFG 75 11 IYVLVMLVL 95 11 LLWTLVVLL 95 11 WTLVVLLI 95 11 FLYALALLL 95 11 CLGGLLTMV 95 11 VMSNTLLSAW 95 11 LLSAWILTA 95 Table S2. Peptide mixes from LMP2
-
The benefit of LMP2-DCs to patients with NPC was investigated through follow-up and tracking of the study subjects. Admission data was reviewed every three months and close follow-up of individual subjects was performed every half year after immunotherapy was completed. Follow-up included phone inquiry to determine physical condition and clinical monitoring of NPC progression.
-
Patients with NPC began to enroll in this study in April 2009. We completed the study in October 2010. Twenty-nine patients with NPC (age 24–66) were enrolled at the hospital for treatment with intradermal injections and agreed to participate in follow up for five years.
-
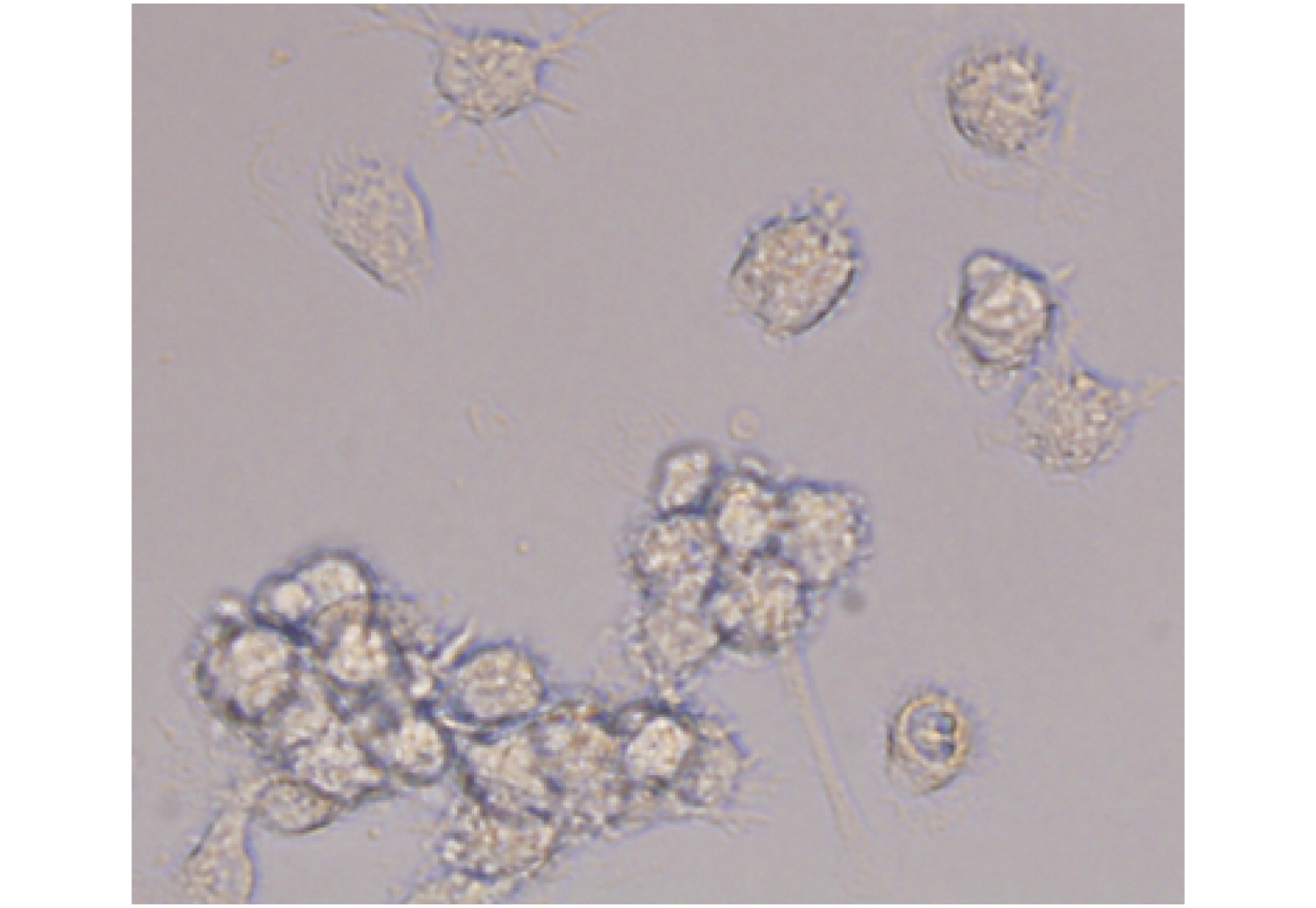
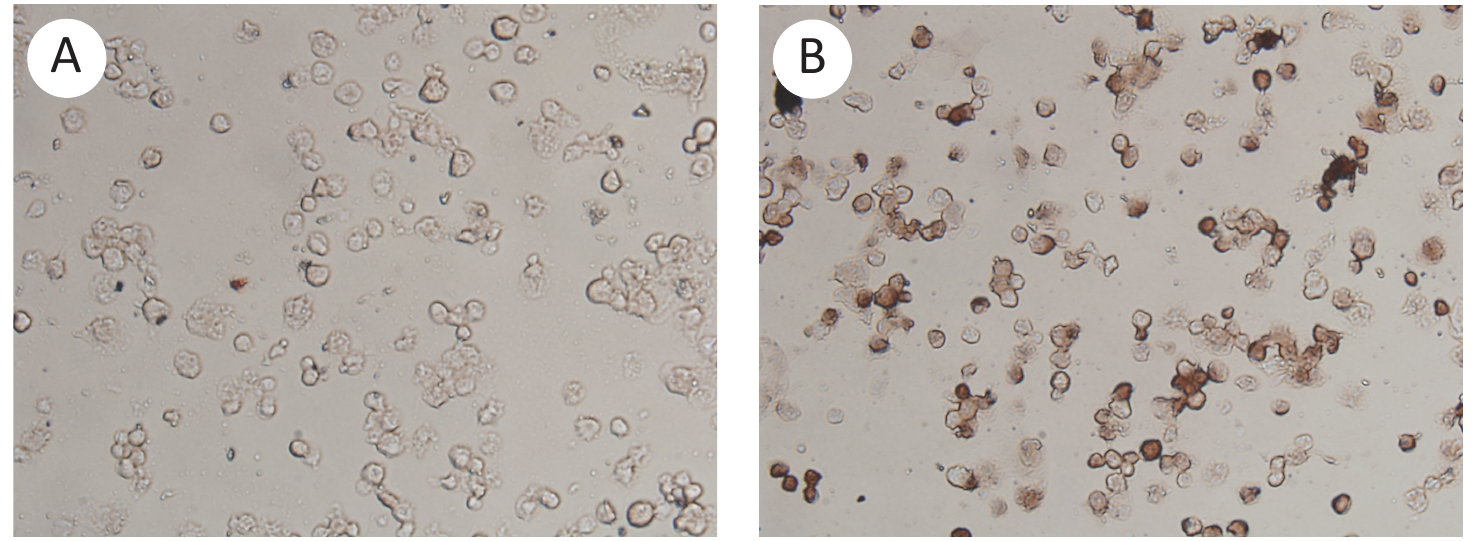
Monocytes isolated from PBMCs were cultured and induced to DC differentiation in vitro. During differentiation, cells progressively acquired DC morphological features. Cells were loosely adherent and irregularly netted. We observed the formation of cell mass, increased cell size, folding on the cellular surface, and the formation of cytoplasmic projections (Figure 2). Immunocytochemical assay, using a LMP2 monoclonal antibody, was performed to confirm the expression of LMP2 in 100 MOI rAd-LMP2 infected DCs. An optical microscope was used to illuminate DCs expressing LMP2 (Figure 3).
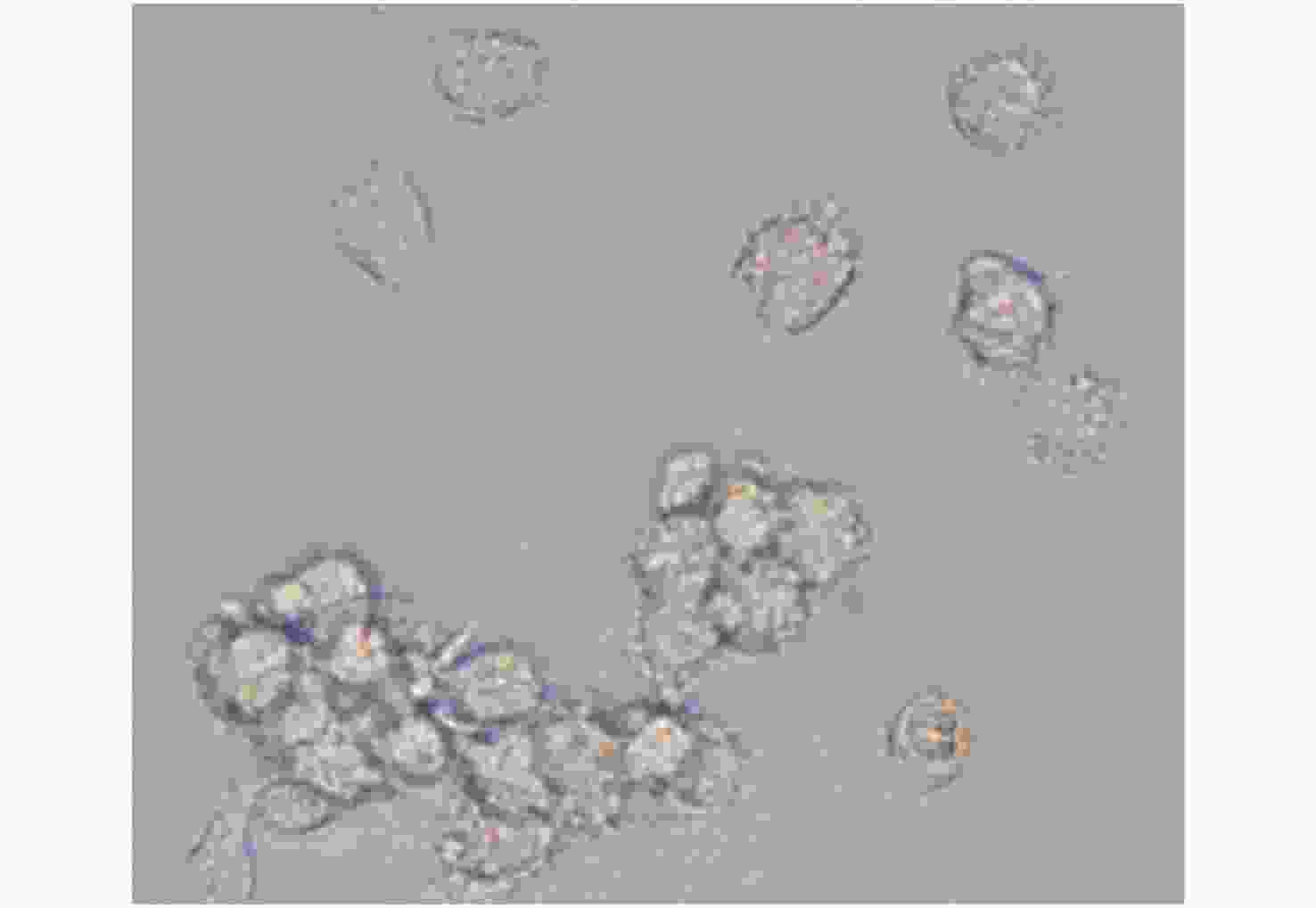
Figure 2. Morphology of mature DCs expressing LMP2. Magnification, 400×.
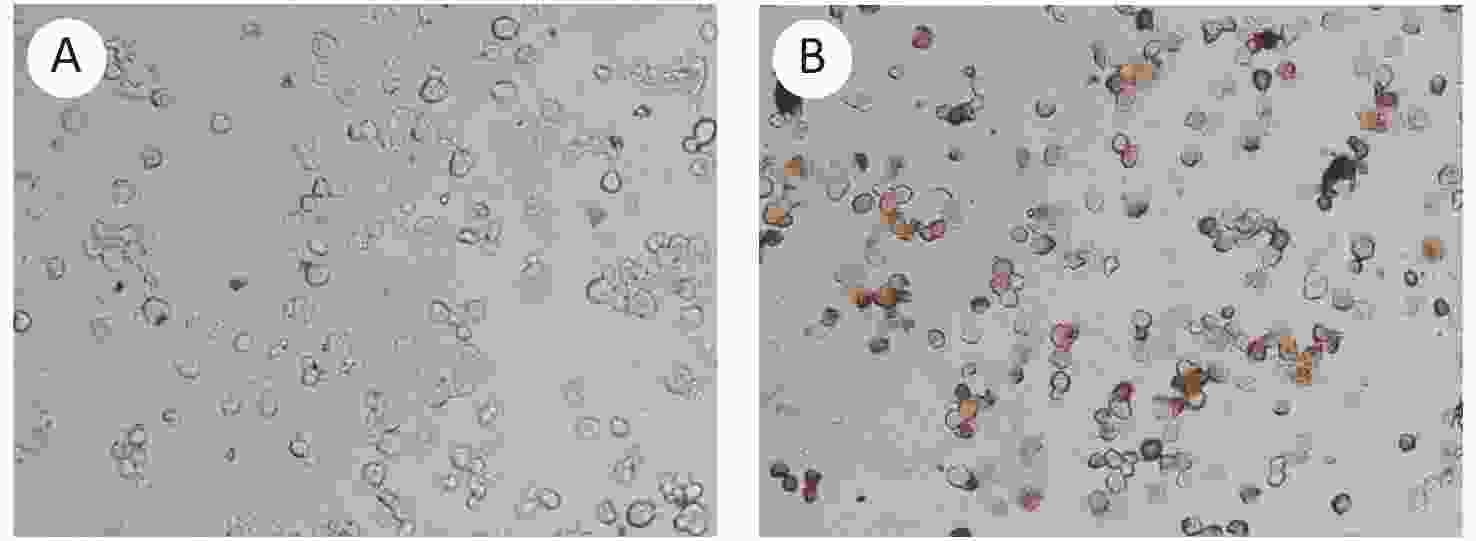
Figure 3. LMP2-expression in monocyte-derived DC infected by rAd-LMP2 with 100 MOI. (A) Negative control; (B) LMP2-DCs. Magnification, 200×.
-
We tested LMP2-pulsed matured DCs for vaccine production in a pilot study of patients with NPC after conventional radiotherapy and chemotherapy. Elutriated monocytes were obtained from the PBMCs of the study subjects and cultured in six-well plates with IL-4 and GM-CSF for 7 d. On day 8 of culturing, DCs were pulsed with rAd-LMP2 for 2 h, followed by treatment with TNF-α, IL-4, and GM-CSF for two days. mLMP2-DCs were harvested and cryopreserved before administration. At the same time, the expression of CD83, CD86, and DC-DR on DC surface was confirmed by flow cytometry. Expression of CD molecules on the surface of DCs showed considerable variation (from 10.57% to 99.87%) in 22 patients with NPC, which may be due to the different responses to LMP2 (Supplementary Table S3 available in www.besjournal.com); i.e., NPC (as indicated by CD83, CD86, and DR molecules) was not detected in seven of the patients (Patients No 4, 15, 16, 17, 18, 19, 25). mLMP2-DCs vaccines were administered through intradermal injection. Each of the study subjects received three vaccinations. In total, 87 intradermal vaccinations were performed. All vaccines were well tolerated, with only local rigor and swelling at the injection site, which subsided the following day without treatment. Weight, blood pressure, heart rate, respiratory signs, and other clinical monitoring data were within the normal range before and after injection, and no serious side effects were observed.
Patients ID DC-CD83 (%) DC-CD86 (%) DC-DR (%) 1 99.32 99.76 99.61 2 67.24 47.54 66.86 3 64.07 44.24 57.27 4 Missed Missed Missed 5 84.45 94.92 93.74 6 99.39 84.88 88.09 7 60.65 52.13 61.61 8 17.02 52.67 37.26 9 55.17 42.34 53.40 10 76.77 77.48 92.56 11 49.53 51.08 81.82 12 74.76 65.75 78.67 13 69.80 71.86 67.83 14 99.86 99.87 99.52 15 Missed Missed Missed 16 Missed Missed Missed 17 Missed Missed Missed 18 Missed Missed Missed 19 Missed Missed Missed 20 91.52 97.53 97.45 21 53.10 59.51 87.67 22 68.51 57.63 72.53 23 54.99 38.25 52.29 24 98.91 86.72 96.93 25 Missed Missed Missed 26 83.28 94.22 92.25 27 10.57 60.12 47.38 28 29.13 36.80 20.92 29 80.31 72.40 80.28 Note. The positive rates of CD83, CD86, and DC-DR on DC surface were also detected by flow cytometry. Expression of CD molecules on the surfaces of DCs varied widely in patients with NPC. Table S3. Detection of CD83, CD86, and DR molecules on the cell surface in LMP2-DCs
-
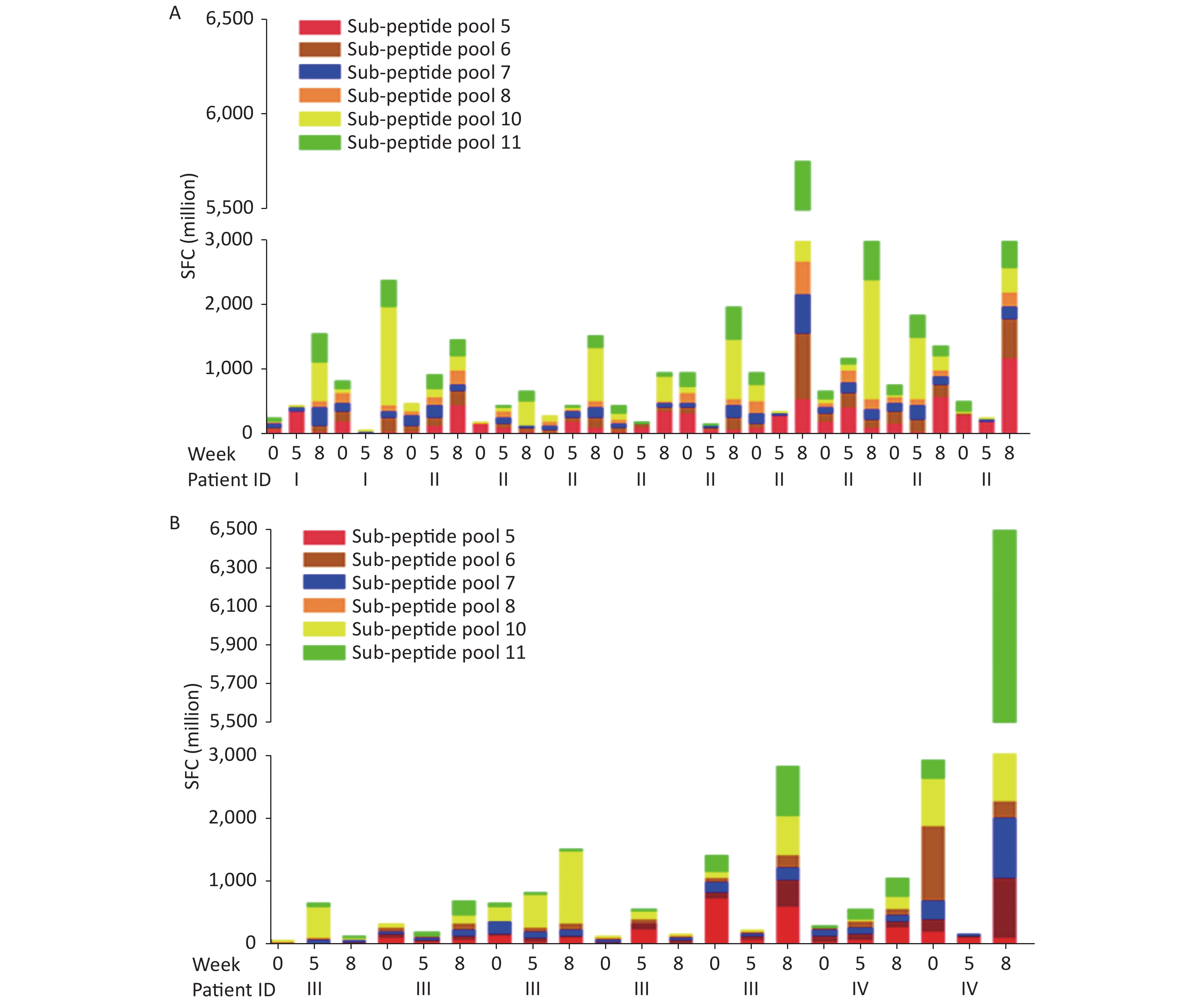
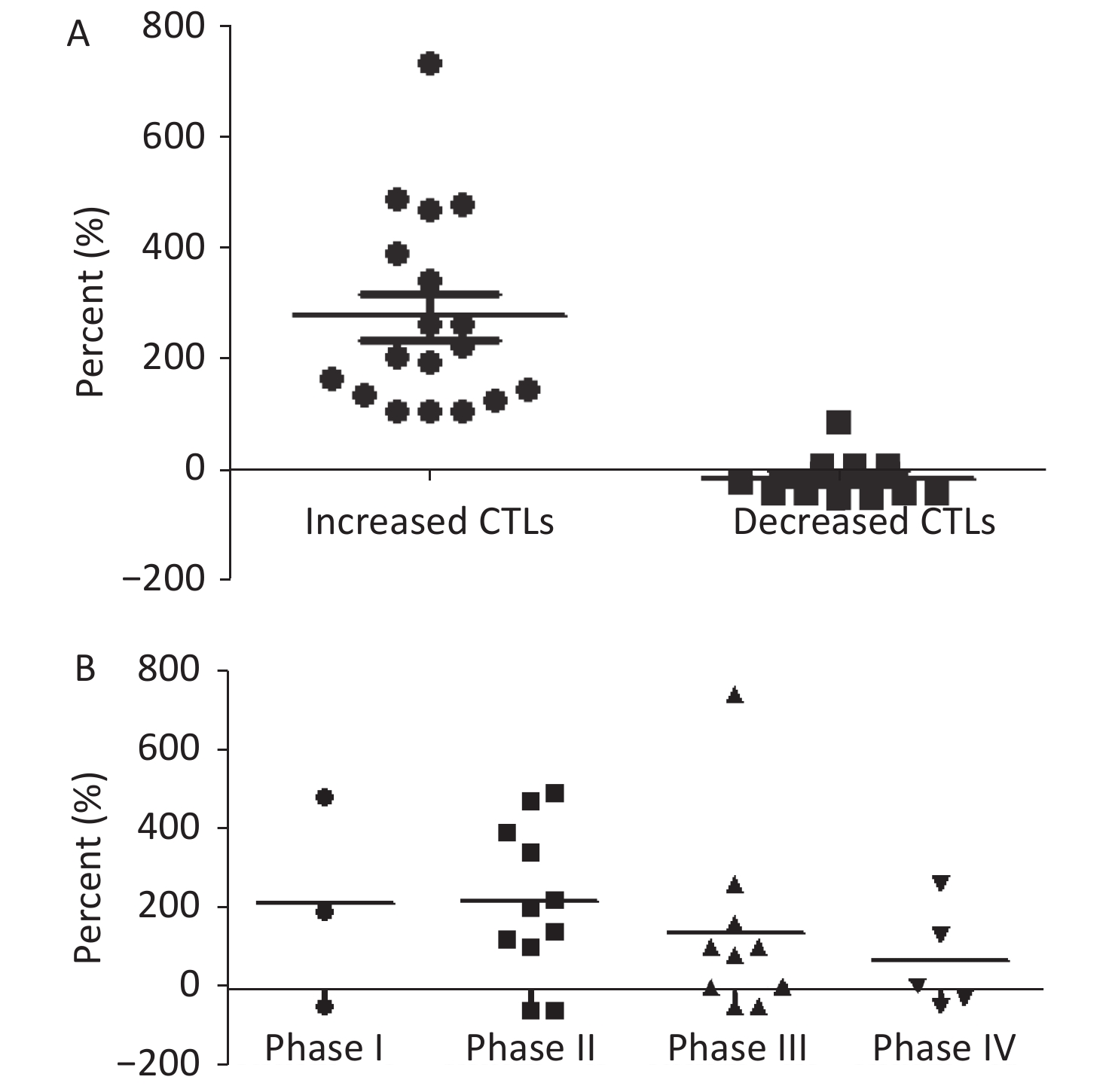
To analyze the effects of vaccination, specific CTL responses to LMP2 were examined pre- and post-injection for each of the three injections. CTL responses to LMP2 increased in 18 of 29 immunized NPC patients (62.1%), compared with pre-immunized subjects (Figure 4A, B). The size of responses varied from 2.0 to 8.4-fold (Figure 5A). Among these 18 patients, two (2/3, 66.7%) were in stage I of the disease, nine (9/11, 81.8%) in stage II, five (5/10, 50.0%) in stage III, and two (2/5, 40.0%) in stage IV (Figure 5B). There was a higher incidence of increased specific responses median 4.3 and 3.2-fold) in subjects at an early stage of NPC (than in advanced stage subjects (median 3.1 and 2.9-fold) (Supplementary Table S4 available in www.besjournal.com). However, 11 of the 29 patients did not show any difference in CTL responses to LMP2 (Figure 6). CTL responses to LMP2 increased (1.8-fold) in Patient No. 24 but were still below two-fold and the case was therefore defined as a non-responder. Of the 11 non-responder patients, one was in stage I, two in stage II, five in stage III, and three in stage IV. The expression of CD83, CD86, and DC-DR on the surface of DCs was lower in non-responders than in responders, which caused no CTL responses to LMP2. The titer of IgA antibody to VCA did not show obvious variation (≥ 4-fold titer changes defined as positive responses) (Supplementary Table S5 available in www.besjournal.com). A test for EBV DNA proved to be negative for both pre- and post-immunization of DC-LMP2 in all 29 patients. All the patients were clinically disease-free after treatment with chemotherapy and radiotherapy (Supplementary Table S6 available in www.besjournal.com). However, EBV DNA was detected in the plasma of one patient (No. 22) and increased along with the development of disease (578 copies/mL in 2012 and 4.6 × 104 copies/mL in 2013) (Supplementary Table S6). The size of LMP2-specific T cell responses gradually decreased with development of cancer in patients with NPC (Figure 6).
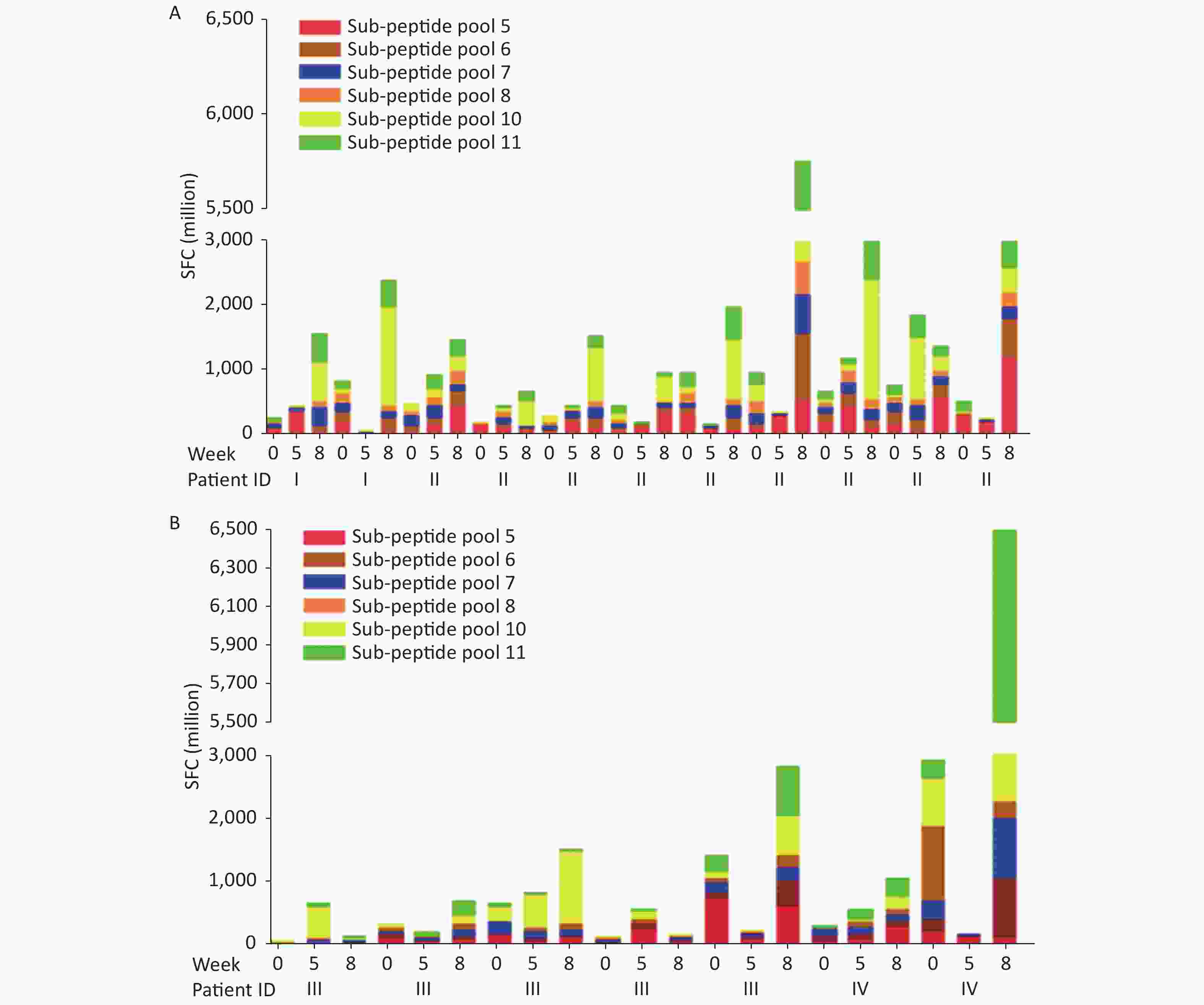
Figure 4. Boosted CTLs responses to LMP2 peptide sub-pools before and after immunization. (A) CTLs responses specific to LMP2 peptide sub-pools before and after immunization in early-stage NPC patients. Boosted T-cell responses to LMP2 in 11 of 14 NPC stage I and II patients. 18 of 29 NPC patients (62.1%) had boosted CTL responses to LMP2, as shown in Figures 4–5. However, 11 of 19 patients did not show positive CTL responses to LMP2. Of 18 patients, 2 (2/3, 66.7%) were in stage I, 9 (9/11, 81.8%) were in stage II, 5 (5/10, 50.0%) were in stage III, and 2 (2/5, 40.0%) were in stage IV. Specific CTL responses were augmented 2.0 to 8.4-fold compared with pre-immunization. Increased size of specific responses is higher in early stage (median 4.3- and 3.2-fold) than at advanced stage (median 3.1- and 2.9-fold). (B) specific responses of CTLs to LMP2 peptide sub-pool before and after immunization in advanced patients with NPC. T-cell responses to LMP2 were boosted in 7 of 15 stage III and IV patients. CTL, cytotoxic T lymphocyte; SFC, spot-forming cell.
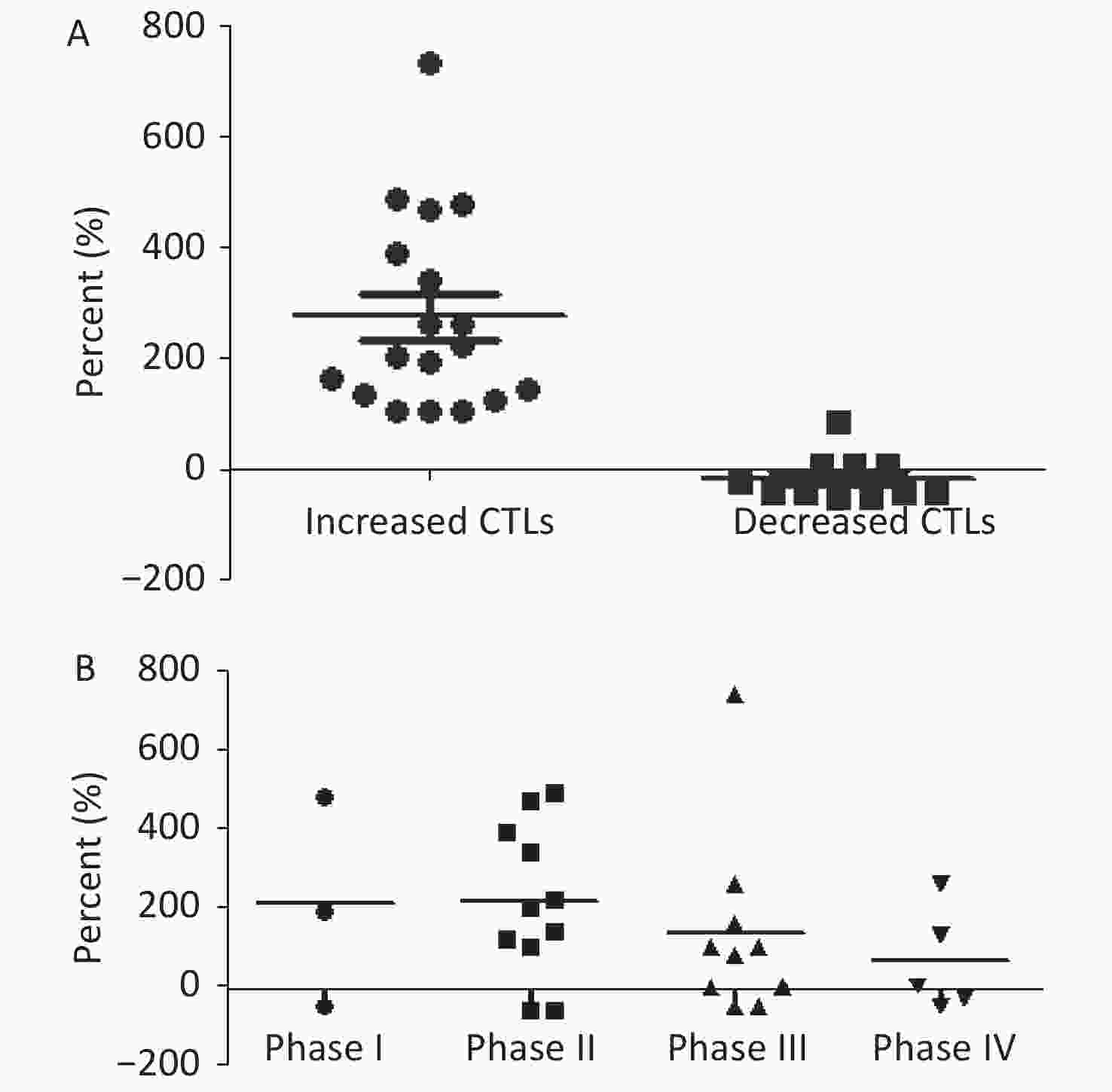
Figure 5. The size of responses to DC vaccine in patients with NPC. (A) size (percent increase) of LMP2-specific T cell responses stimulated by LMP2-DCs vaccine. (B) size (percent increase) of the responses in patients at different stages of NPC. CTL, cytotoxic T lymphocyte
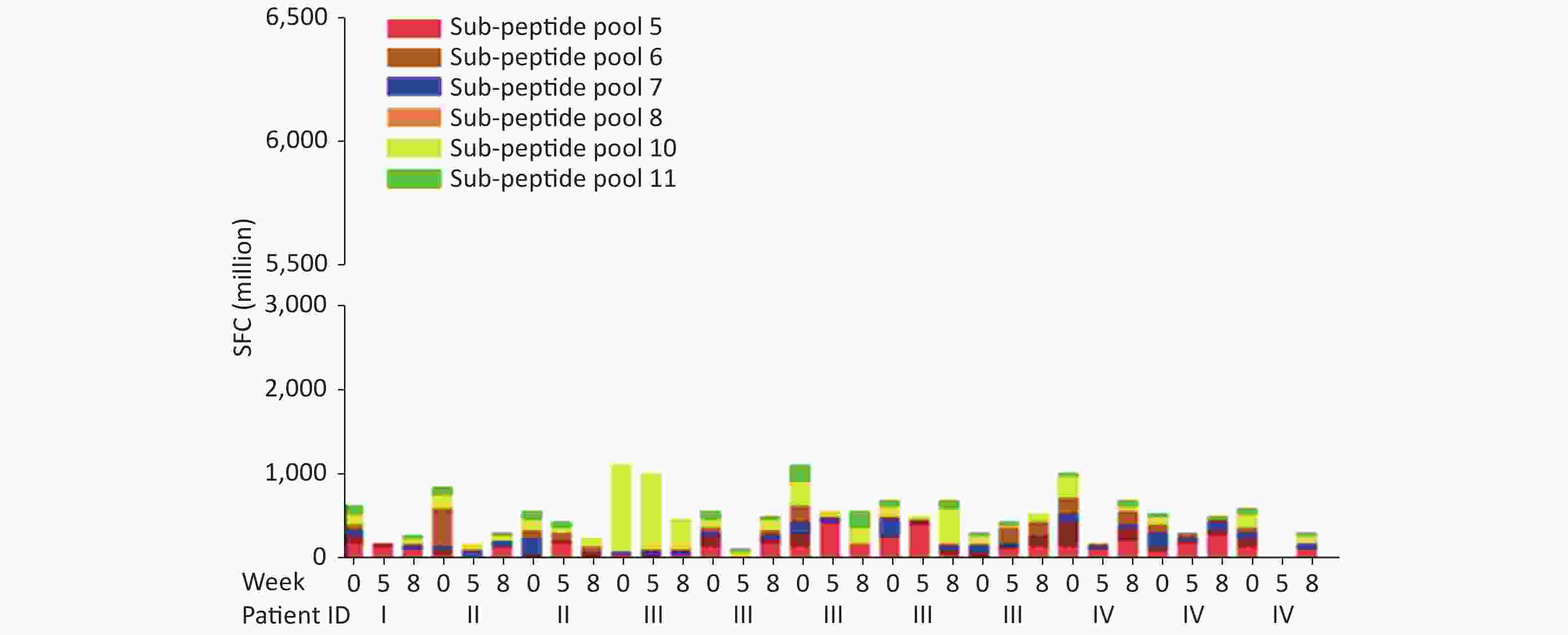
Figure 6. CTL responses to LMP2 peptide sub-pool before and after immunization. In 11 of 29 patients, there were no positive CTL responses to LMP2; rather, CTL levels were slightly elevated, unchanged, or decreased. 72.7% of the patients were in later stages of NPC (stage III and stage IV). Patient characteristics are presented in Supplementary Table S1. CTL, cytotoxic T lymphocyte; SFC, spot-forming cell.
Patient ID Stage at enrollment Pre-vaccination
(Spot-forming cells/million PBMC)Post-vaccination
(Spot-forming cells/million PBMC)Percent increase (%) 1 I 270 1,576 484 3 I 840 2,395 185 4 II 500 1,478 196 5 II 212 670 216 6 II 310 1,530 394 9 II 450 977 117 10 II 975 1,980 103 11 II 980 5,760 488 12 II 680 2,995 340 13 II 770 1,850 140 14 II 534 3,023 466 17 III 80 673 741 18 III 350 685 96 19 III 675 1,775 163 20 III 160 580 263 23 III 1,420 2,805 98 26 IV 293 1,055 260 29 IV 2,910 6,590 126 Table S4. Specific-CTLs responses induced by LMP2-DCs in NPC patients
Patient ID Stage at enrollment Week 0 Week 5 Week 8 1 I 320 160 160 2 I 80 80 80 3 I 40 40 40 4 II 160 80 160 5 II 20 40 20 6 II 160 160 160 7 II 40 40 40 8 II 80 80 80 9 II 40 40 40 10 II 80 40 80 11 II 160 160 160 12 II 20 20 20 13 II 80 80 80 14 II 80 80 80 15 III 20 20 20 16 III 40 40 40 17 III 40 80 40 18 III 40 40 40 19 III 40 40 40 20 III 320 320 160 21 III 40 40 40 22 III 80 160 80 23 III 40 40 40 24 III 20 20 20 25 IV 40 40 40 26 IV 80 40 80 27 IV 80 80 80 28 IV 320 320 320 29 IV 80 80 80 Table S5. IgA /VCA antibody titer in plasma
Patient ID Stage at enrollment Year (2011) Year (2012) Year (2013) Year (2014) Year (2015) 1 I – – – – Neg 2 I Neg – Neg – Neg 3 I Neg Neg – Neg Neg 4 II Neg Neg Neg Neg Neg 5 II Neg Neg Neg – Neg 6 II – – – – – 7 II Neg Neg Neg Neg Neg 8 II – – Neg – – 9 II Neg Neg Neg – – 10 II Neg – – – – 11 II – – – – – 12 II – – Neg – – 13 II Neg 1.6 × 103 – – – 14 II Neg Neg Neg Neg – 15 III Neg – Neg Neg 16 III Neg – – – Neg 17 III Neg Neg Neg Neg – 18 III – – – – – 19 III Neg – Neg Neg – 20 III Neg Neg Neg – – 21 III Neg – – – – 22 III Neg 578 4.6 × 104 23 III Neg Neg Neg Neg – 24 III – – – – – 25 IV – Neg – – – 26 IV Neg Neg Neg Neg Neg 27 IV – – – – – 28 IV – – – – – 29 IV Neg Neg Neg Neg 3 × 103 Table S6. EBV-DNA concentration in plasma
-
To evaluate the long-term therapeutic efficacy after vaccination, we followed up with the study subjects for five years (from October 2009 to December 2015). Seven patients died, of whom one (1/11) had stage II NPC, four (4/10) had stage III NPC, and two (2/5) had stage IV NPC. Only one of the deceased subjects was a responder, the other six of the seven deceased subjects were non-responders (Supplementary Table S7 available in www.besjournal.com). The five-year survival rate, from immunotherapy completion to the end of 2015, was 94.4% in responders and 45.5% in non-responders (Table 1). The survival durations were 1–4 years in the seven patients who died within five years, with durations in most patients being 2–3 years (Supplementary Table S8 available in www.besjournal.com). This suggests that CTLs responses that are specific to LMP2 play a role in controlling and preventing NPC recurrence and metastasis.
Patient ID Stage at enrollment Pre-vaccination
(Spot-forming cells/million PBMC)Post-vaccination
(Spot-forming cells/million PBMC)Percent increase (%) 2 I 630 285 –54.8 7 II 855 320 –62.6 8 II 575 245 –57.4 15 III 1,278 1,300 1.7 16 III 928 495 –46.7 21 III 1,095 570 –47.9 22 III 690 685 –0.7 24 III 300 540 80.0 25 IV 995 700 –29.6 27 IV 525 500 –4.8 28 IV 609 300 –50.7 Table S7. Non-specific CTLs responses induced by LMP2-DCs vaccine in NPC patients
Stage Early stage Advanced stage 5-year survival rate (%) (n = 29) I (n = 3) II (n = 11) III (n = 10) IV (n = 5) Positive reaction 2 9 5 2 18/29 (62.1) Death 0 0 1 0 1/18 (5.6) Survival 2 9 4 2 17/18 (94.4) 5-years survival rate (%) 100.0 85.7 Negative reaction 1 2 5 3 11/29 (37.9) Death 0 1 3 2 6/11 (54.5) Survival 1 1 2 1 5/11 (45.5) 5-years survival rate (%) 66.7 37.5 Total death rate (%) 0.0 9.1 40.0 40.0 7/29 (24.1) Total survival rate (%) 100.0 90.9 60.0 60.0 22/29 (75.9) Table 1. Specific CTLs responses in patients with NPC after immunization with LMP2-DC
Patient ID Stage at enrollment Fold Percent increase (%) Survival period (year) Year of death Cause of death 7 II N –54.8 2 2012 metastatic carcinoma of bone 16 III N –62.6 4 2013, 7 pulmonary metastasis 22 III N –57.4 3 2013, 4 multiple metastasis 23 III N 1.7 3 2013, 12 pulmonary metastasis 24 III N –46.7 1 2011, 4 multiple metastasis 25 IV N –47.9 3 2013, 8 multiple metastasis 28 IV N –0.7 3 2013, 7 pulmonary metastasis Table S8. Characteristics of NPC patients who were immunized by LMP2-DCs and died within five years of cancer treatment
-
DC-based immunotherapy shows great potential for the treatment of cancer[14,15]. DC immunotherapy is conducted mostly through tumor antigen peptides or tumor gene-loaded DCs. However, few tumor-specific or associated antigens have been identified. EBV infection is closely associated with NPC and is recognized as an etiological agent. LMP2 encoded by EBV is detected in most NPC biopsies. This protein contains CD8 T cell epitopes and is considered one of the ideal target antigens for immunotherapy[5]. Therefore, LMP2 was selected as the target antigen for NPC immunotherapy in our study. Although DC vaccine could be administered by venous transfusion, lymph node, and intra-tumoral injection; fewer DCs were required for intra-tumoral injection to stimulate an efficient Th1/Th2 response[16–18]. Thus, it is more practical to administer DC vaccination to tumor patients via intradermal injection. Our group has previously reported nine NPC patients who received 60Co irradiated LMP2-DCs through intradermal injection, and the CTL responses specific to LMP2 were boosted in five of these nine NPC patients[19]. rAd-LMP2 is a replication-defective adenovirus which has a good safety and may affect the function of LMP2-DCs that were irradiated by 60Co. In the present study, LMP2-DCs were directly immunized through intradermal injection instead of 60Co irradiation. Our results suggest that CTL responses specific to LMP2 in the early stage of NPC are much better than that in the advanced stage of the disease (Table 2). Therefore, we consider intradermal injection more suitable for patients with early-stage NPC than those in the advanced stage. Among the 29 patients, 11 had been for 3 months after radiotherapy or/and chemotherapy, and specific CTL responses improved in nine of these eleven patients after injection of LMP2-DCs, which indicates that immunity levels were back to normal for most of the patients three months after radiation and chemotherapy. The LMP2-specific responses of CTL in some responsive NPC patients are reduced very quickly. One of our main concerns is how to maintain LMP2-specific CTL responses at a certain level. We are currently testing if we can maintain LMP2-specific CTL responses by increasing injections and using multi-vector forms of immunity. We did not detect changes in IgA antibody titers to EBV-VCA, since our experimental design was to activate LMP2 specific cellular immune responses, not humoral immune responses. In addition, two months was not sufficient to detect the changes in IgA antibody levels.
Stage Cases LMP2 CTLs POS (%) LMP2 CTLs NEG (%) Total (%) I 3 2 (66.7) 1 (33.3) 100.0 II 8 7 (87.5) 1 (12.5) 100.0 III 5 3 (60.0) 2 (40.0) 100.0 IV 3 1 (33.3) 2 (66.7) 100.0 Total 19 13 (68.4) 6 (31.6) 100.0 Table 2. Relation between the stage of NPC and LMP2 specific-CTLs
In previous studies it has been reported that EBV genome copies could serve as an index of treatment efficacy for early diagnosis and prognosis of NPC[20,21]. We therefore examined plasma EBV genome copies of NPC patients before and after DC immunotherapy, but the plasma data results were negative in all NPC patients, which suggests that clinical post-radiotherapy and post-chemotherapy may inhibit the replication of the EB virus. However, EBV DNA was detected in the plasma of one patient (No. 22) and increased along with the development of the disease (578 copies/mL in 2012 and 4.6 ×104 copies/mL in 2013).
Each subject received three consecutive injections of LMP2-DCs: at week 0 and after at thesecond and fourth weeks. LMP2-specific CTL responses were examined pre-injection, at week 0, and at the fifth and eighth weeks. To further confirm the therapeutic efficacy of LMP2-DCs vaccines in treating NPC, future studies should include follow-up for long-term therapeutic effects, the launch of large multicenter clinical trials, and so on. How to best combine laboratory data with efficacious clinical treatment is a topic for future research.
-
Zeng Y designed the experiments and supervised the project. Si YF, Du HJ, and Lin H supervised the project. SJ O'Brien, Lan GP, Wang Z, Zhou L, Tang MZ, Lan J, Zhou XY, Wang YL, and Tang J designed and conducted the experiments and analyzed results. Du HJ and Zhou ZX wrote the manuscript. Zeng Y gratefully acknowledges the founding support. The authors declare no competing financial interests
Funds:
Mega Project of Research on the Prevention and Control of HIV/AIDS, Viral Hepatitis Infectious Diseases [Grant No:2018ZX10102001]; the Key Science and Technology Program of Guangxi Zhuang Autonomous Region [Grant No. 14124003-3]; the National High Technology Research and Development Program of China [Grant No. 2007AA021107]; and the National Basic Research Program of China [973 Program, Grant No. 2011CB504800]

 Quick Links
Quick Links
 DownLoad:
DownLoad: