


-
Global warming is one of the most pressing environmental problems and received burgeoning attention in the past decades [1, 2]. The increasing frequency of extreme weather caused by global warming makes adaptation difficult for populations, thereby aggravating the disease burden caused by high temperatures [3, 4]. Multiple studies revealed that more intense and frequent heat waves due to global warming would affect human health and increase the risk of death [5, 6]. A global assessment estimated the number of death and disability-adjusted life years (DALYs) attributable to high temperature as 0.31 [95% uncertainty interval (UI): 0.22–0.46] million and 11.70 (95% UI:8.19–19.37) million, which may contribute to the potential risk of life expectancy loss and mortality [7].
Cardiovascular disease (CVD) remains the leading cause of death and disability worldwide [8, 9]. A systematic analysis revealed nearly doubled prevalent cases of total CVD and years lived with disability (YLDs) in the past three decades and an increased number of CVD deaths by almost six million [10]. The cardiovascular system is particularly vulnerable to the negative effects of global warming [11]. Increased risks of CVD morbidity and mortality associated with high temperatures have been widely reported in numerous observational and modeling studies globally [12-14]. However, existing studies focusing on the heat-related burden of CVD were mainly conducted in individual countries and regions [15-17]. The analytical methods used in studies across periods and locations have considerable heterogeneity, thereby causing substantial uncertainty in evaluations for temperature-related CVD burden when comparing estimates between studies [18-20].
This study descriptively analyzed the temporal trends and spatial distribution of CVD burden due to high temperatures from 1990 to 2019 using datasets and statistical methods provided by the Global Burden of Disease Study 2019 (GBD 2019). Our goal is to identify vulnerable groups most affected by heat and areas requiring priority intervention and predict subsequent temporal trends.
-
Comparative estimates of the burden of CVD due to high temperature were derived from the GBD 2019 for 204 countries and territories from 1990 to 2019. GBD 2019 (
http://ghdx.healthdata.org/gbd-results-tool , assessed on April 1, 2022) is a systematic scientific survey that assesses the burden of disease and health effects of risk factors by age, sex, and region. It divides 204 countries and territories into 21 regions [8]. Based on the socio-demographic index (SDI), 204 countries and territories are divided into five super regions [21]: low SDI (< 0.46), medium-low SDI (0.46–0.60), medium SDI (0.61–0.69), medium-high SDI (0.70–0.81), and high SDI (> 0.81). SDI is a composite indicator of income per capita, years of schooling, and fertility rate in females younger than 25 years [22]. -
GBD defines the theoretical minimum risk exposure level for temperature as the temperature associated with the lowest overall mortality attributable to the risk in a given location and year [22]. The annual mean temperature higher than the theoretical minimum risk exposure level was defined as high temperature. This study focused on analyzing temporal trends in CVD burden attributable to high temperature from 1990 to 2019, using indicators, including mortality, DALYs, and age-standardized rates (ASR). Mortality is the proportion of the total number of deaths in a population over a certain period and is the most commonly used measure of mortality risk. DALYs were calculated as the sum of YLDs and years of life lost, which is a composite measure of the impact of disease on life expectancy loss in a population [23]. ASR was calculated according to the age composition of the GBD 2019 standard population. This standard population was generated by taking the non-weighted mean of the age-specific proportional distributions for national locations from 2010 to 2035 reported by the UN Population Division World Population Prospects 2012 revision and updated using the non-weighted mean of the GBD year’s age-specific distributions for national locations with populations more than 5 million in the GBD year [24].
-
We applied the age-standardized mortality rate (ASMR) and DALY rate (ASDR) per 100,000 population to evaluate the burden of CVD attributable to high temperature for regional and national comparison. Estimated annual percentage change (EAPC) was used to describe temporal trends in ASMR and ASDR for CVD attributable to high temperature [25]. The ASR could be fitted in a regression model:
$$ {\rm{ln}}ASR={\text{α} }+{\text{β} }{\rm{x}}+{\epsilon } $$ (1) where x is the calendar year, β represents the annual change, and ε refers to the error term. EAPC can be calculated as 100 × [exp (β) − 1], assuming that the ASR in log transformation is normally distributed [25]. The ASR is considered to be trending upward, while the upper boundary of < 0 represents a downward trend in ASR if the lower boundary of 95% confidence intervals (CI) in EAPC is > 0. Otherwise, the ASR is deemed to be steady. The Spearman rank test was used to measure the correlation between SDI and EAPC at the national level. We performed all statistical analyses in R version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria). A two-sided P-value of < 0.05 was considered statistically significant.
-
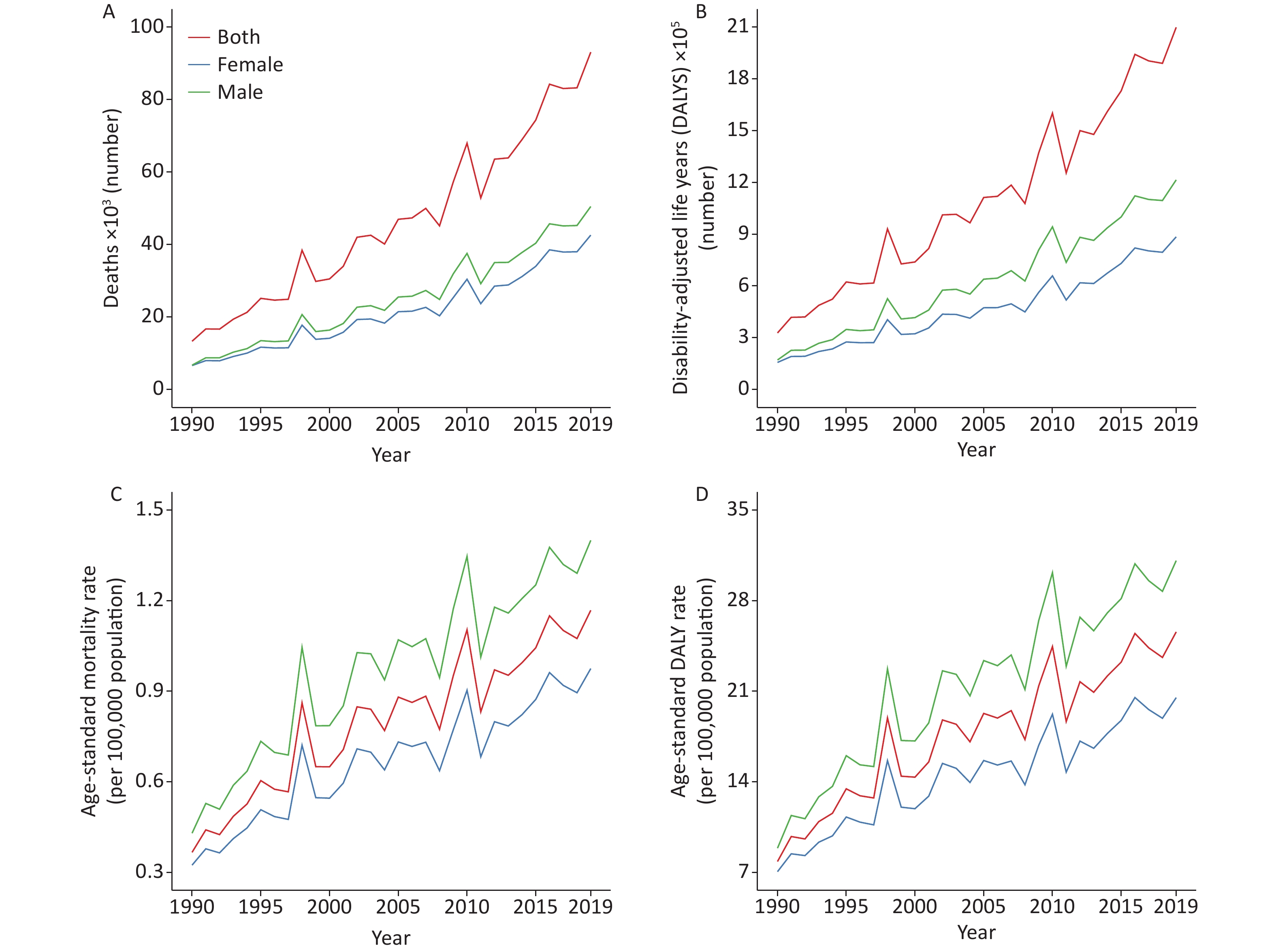
Trends in the burden of CVD due to high temperature between 1990 and 2019 are presented in Figure 1. The number of deaths from CVD attributable to high temperature was 93.10 thousand (95% CI: 10.83–258.39) in 2019, increasing approximately six-fold compared to 1990 (13.30, 95% CI: −85.96 to 56.06). High-temperature effects on CVD burden have varied over the past three decades but overall are on the rise. The ASMR (per 100,000 population) dramatically increased from 0.37 (95% CI: −2.27 to 1.51) in 1990 to 1.17 (95% CI: 0.13–1.98) in 2019. The corresponding ASDR increased markedly from 7.84 (95% CI: −53.68 to 33.10) to 25.59 (95% CI: 2.07–44.17) per 100,000 population.
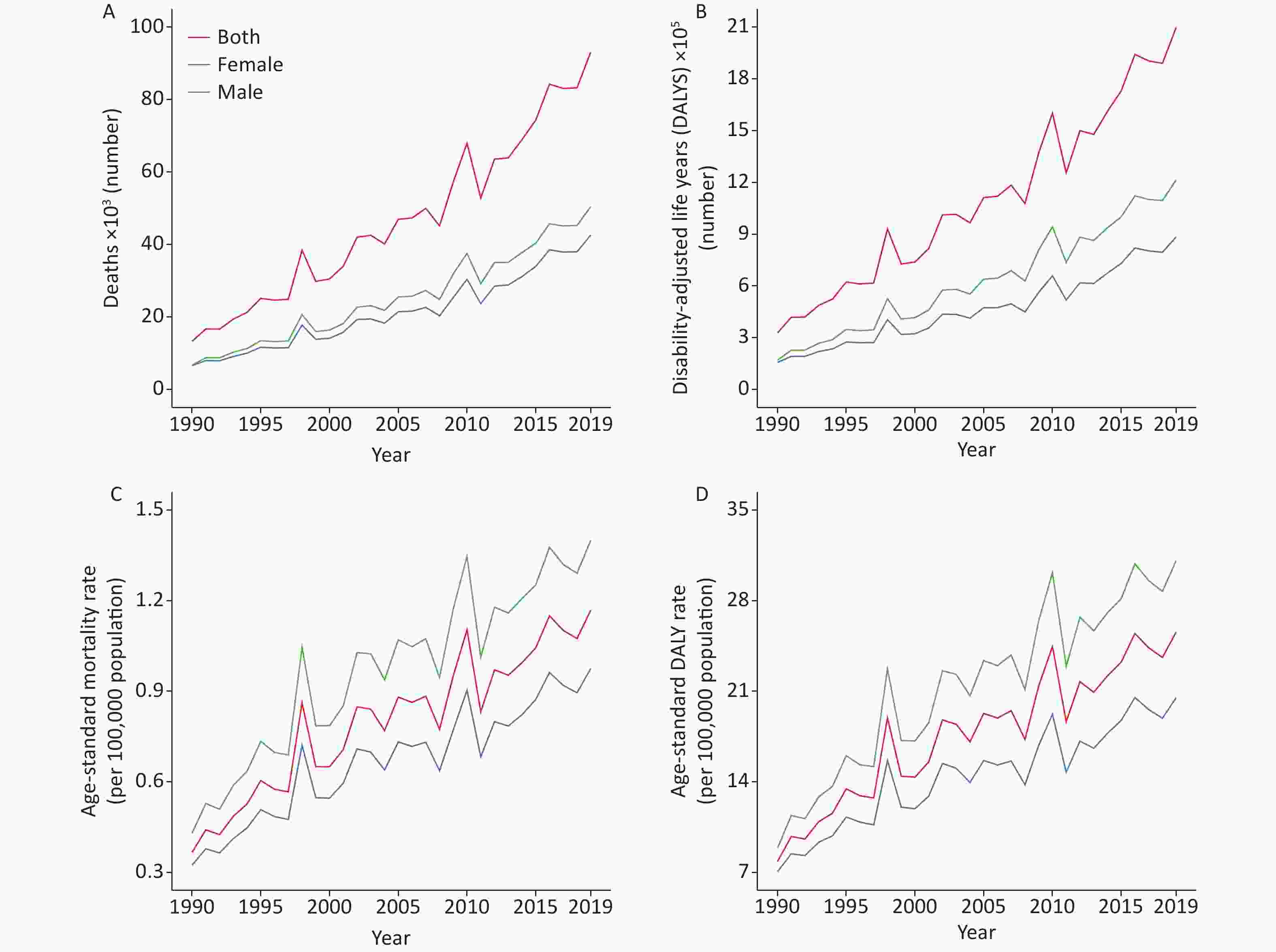
Figure 1. Global burden of cardiovascular disease (CVD) attributable to high temperature from 1990 to 2019. (A) Global number of deaths from CVD for high temperature; (B) Global disability-adjusted life years (DALYs) number from CVD for high temperature; (C) Global age-standardized mortality rate from CVD for high temperature; (D) Global age-standardized DALY rate from CVD for high temperature.
-
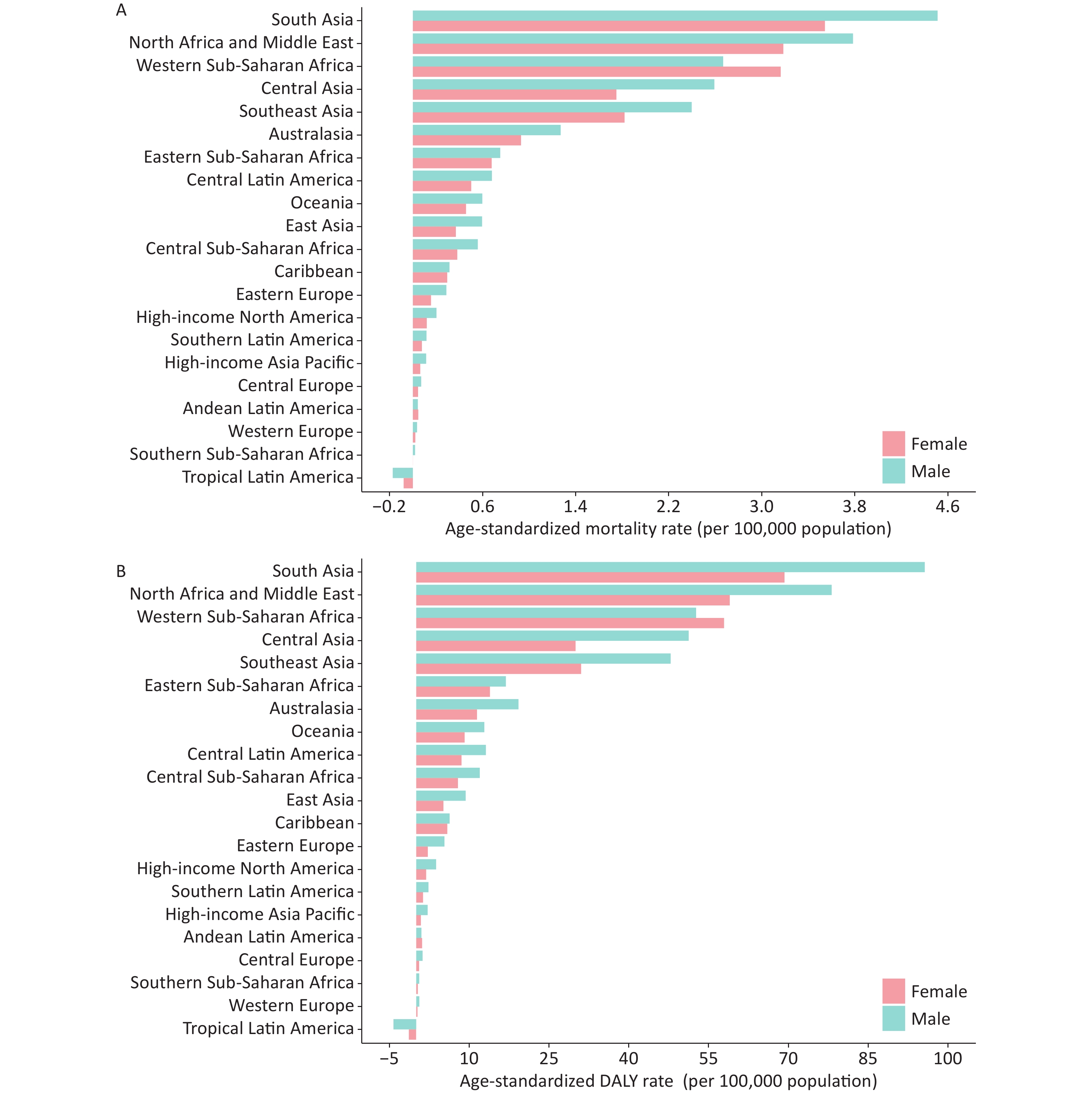
Both ASMR and ASDR of CVD attributable to high temperature were higher in males (Figures 1 and 2). In 2019, the global ASMR of CVD attributable to high temperature was 1.40 (95% CI: 0.08–2.45) for males and 0.98 (95% CI: 0.13–1.66) for females per 100,000 population. The corresponding risk estimate for ASDR was 31.10 (95% CI: 0.49–54.55) and 20.51 (95% CI: 2.57–35.23) per 100,000 population. From 1990 to 2019, the CVD burden attributable to high temperature showed a sharply upward trend in both sexes (Figure 1), which was more noticeable in males. For instance, in China, the ASDR increased from 4.95 (95% CI: −4.53 to 17.50) to 9.68 (95% CI: 3.26–20.36) per 100,000 population for males and from 3.97 (95% CI: −3.41 to 13.00) to 5.30 (95% CI: 1.82–10.31) for females over these 30 years. The discrepancy in CVD burden associated with high temperature between males and females has been increasing during the past three decades.
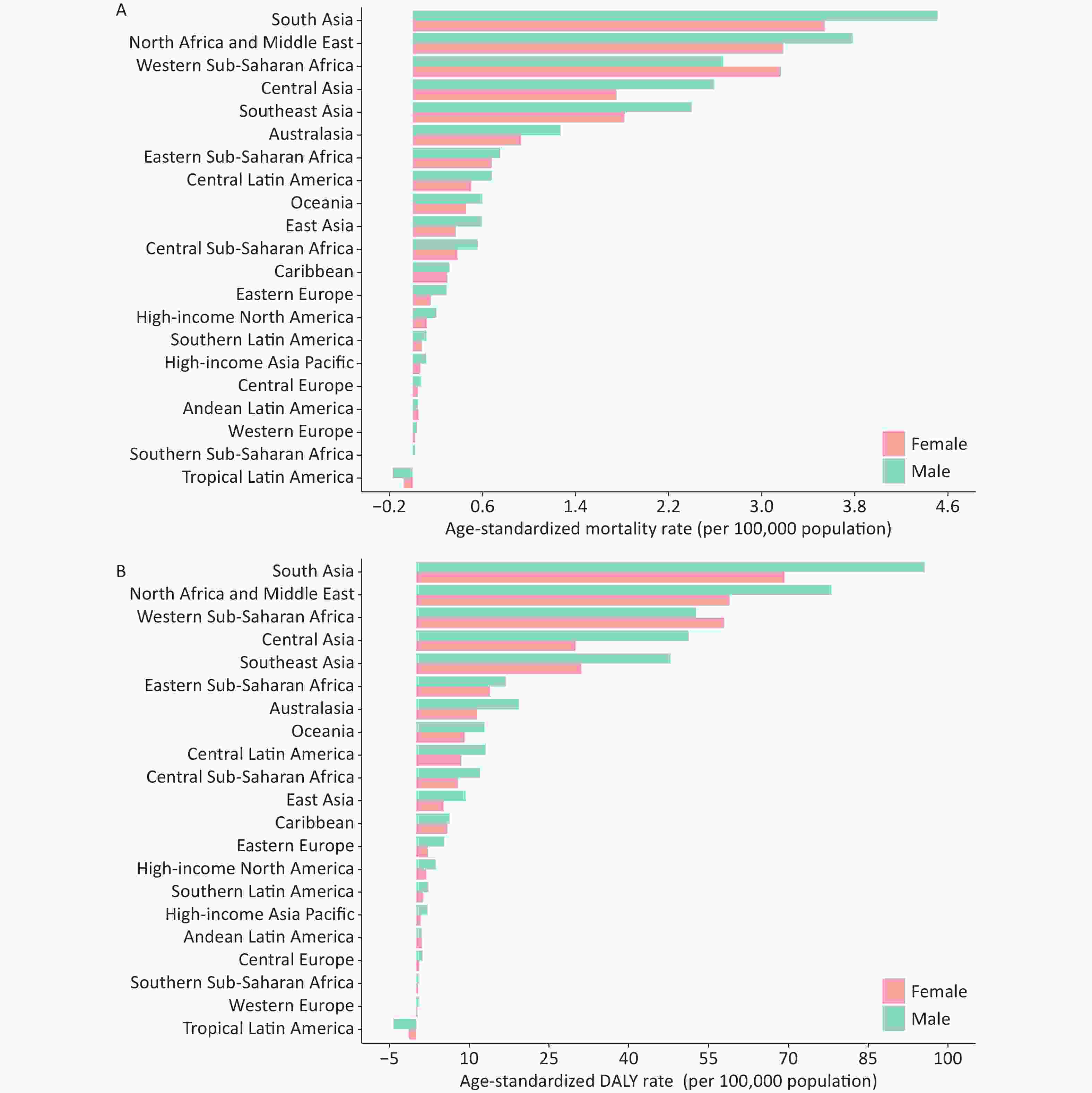
Figure 2. Age-standardized rates of cardiovascular disease (CVD) attributable to high temperature for gender by GBD regions in 2019. (A) Age-standardized mortality rate of CVD attributable to high temperature for 21 regions in 2019; (B) Age-standardized DALY rate of CVD attributable to high temperature for 21 regions in 2019. DALY, disability-adjusted life year.
-
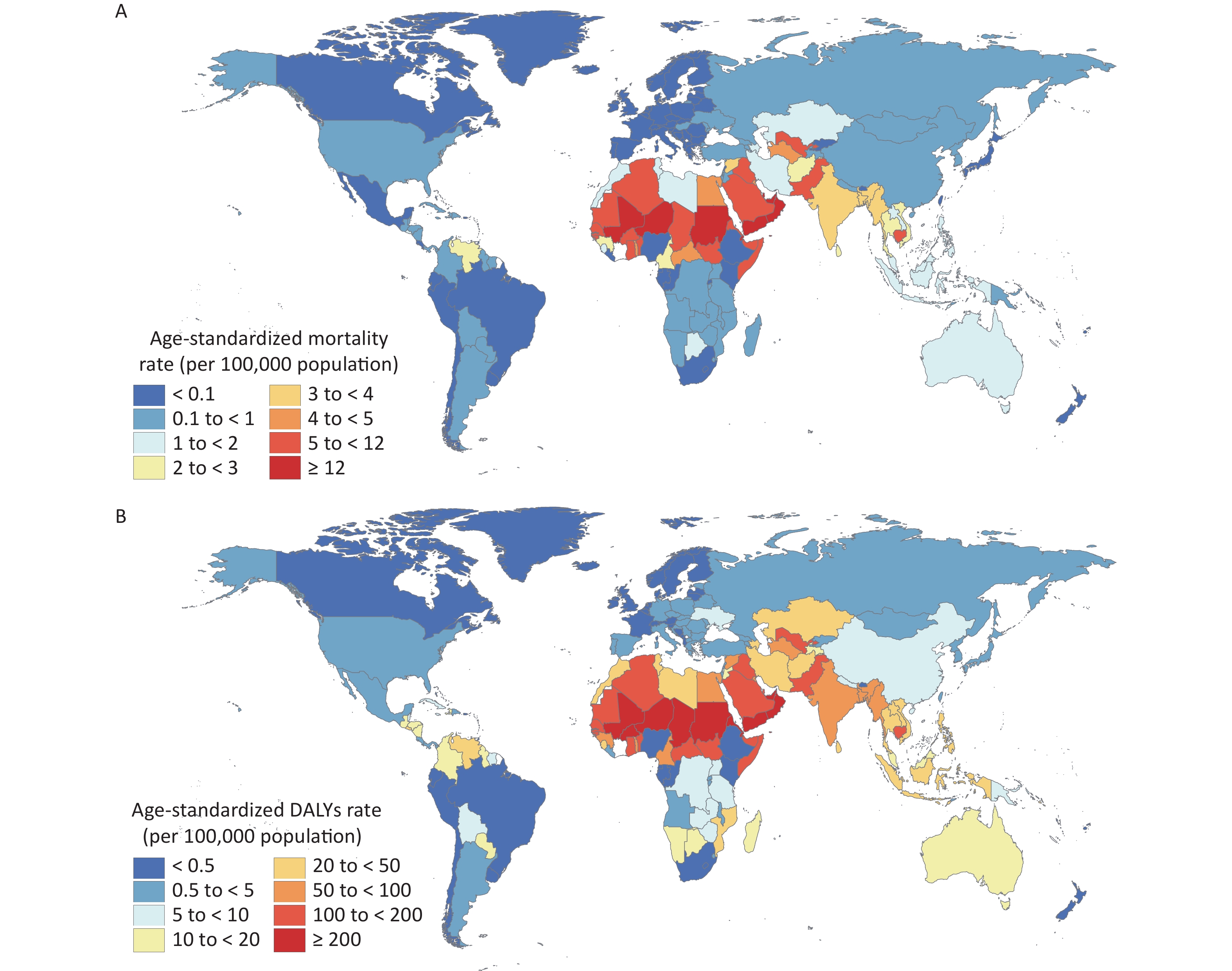
The burden of CVD due to high temperature considerably varies between countries and regions (Figures 2 and 3). In 2019, the largest ASMR (per 100,000 population) of heat-related CVD burden was found in South Asia (4.02, 95% CI: 0.25–7.15), followed by North Africa and the Middle East (3.49, 95% CI: 1.06–6.29) and Western Sub-Saharan Africa (2.93, 95% CI: −8.23 to 8.00). For ASDR, the rank of CVD burden caused by high temperature had the same pattern. Compared with 1990, the CVD burden attributable to high temperature had increased in nearly 80% of countries for death and 60% for DALYs worldwide. In 2019, the top three countries for ASMR (per 100,000 population) were Oman (21.52, 95% CI: 1.90–33.63), United Arab Emirates (17.88, 95% CI: 3.89–29.16), and Mali (14.29, 95% CI: 7.09–22.09). The same went for ASDR, with 344.83 (95% CI: 33.87–544.23), 323.90 (95% CI: 61.13–537.39), and 259.99 (95% CI: 119.09–404.00) in these three countries per 100,000 population, respectively. Some tropical countries presented a very slight disease burden, such as the Congo (0.31, 95% CI: −17.02 to 20.32) and the Democratic Republic of Congo (6.97, 95% CI: −8.44 to 32.65).
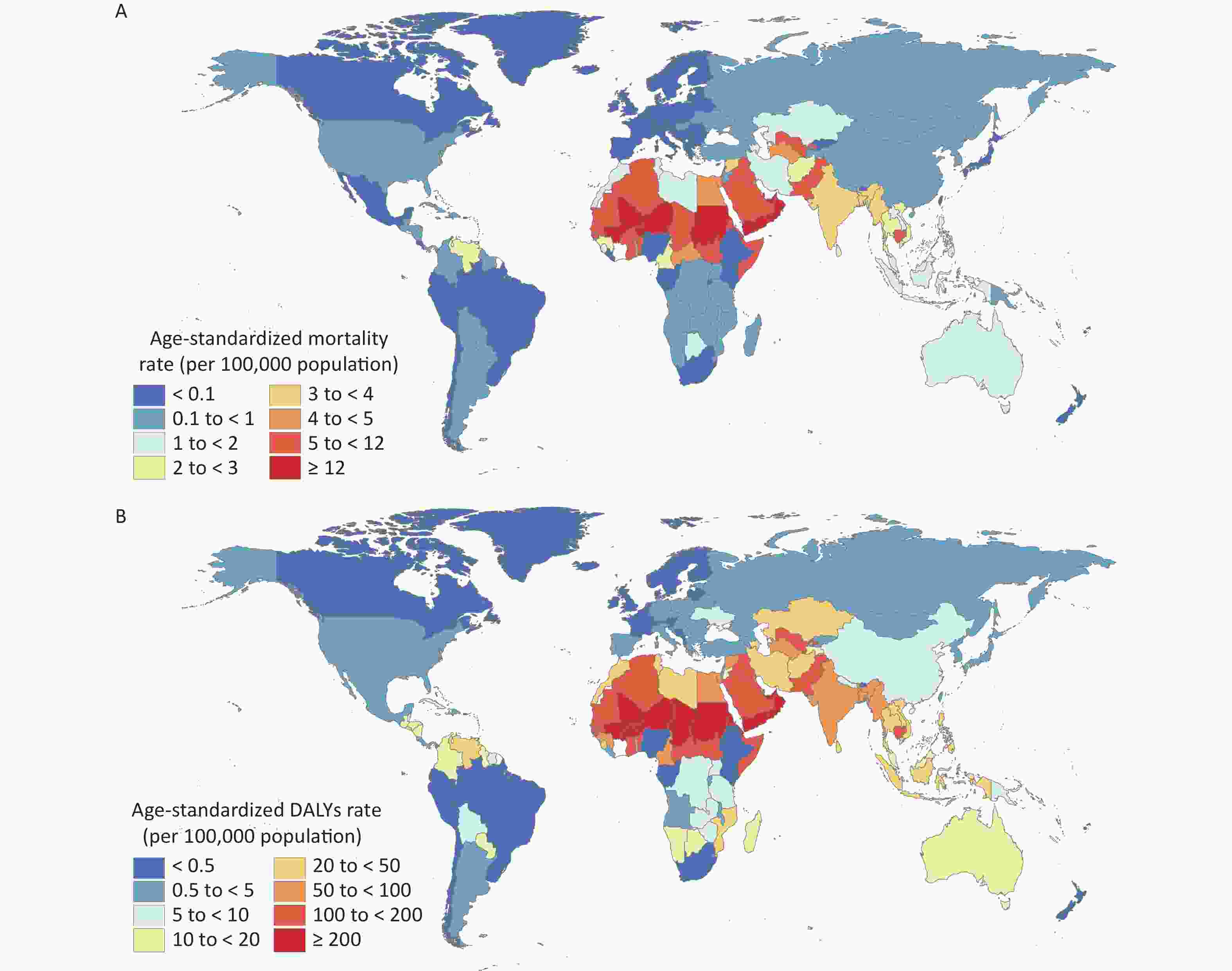
Figure 3. Age-standardized rates of cardiovascular disease (CVD) attributable to high temperature by country in 2019. (A) Age-standardized mortality rate of CVD attributable to high temperature by country in 2019; (B) Age-standardized DALY rate of CVD attributable to high temperature by country in 2019. DALY, disability-adjusted life year.
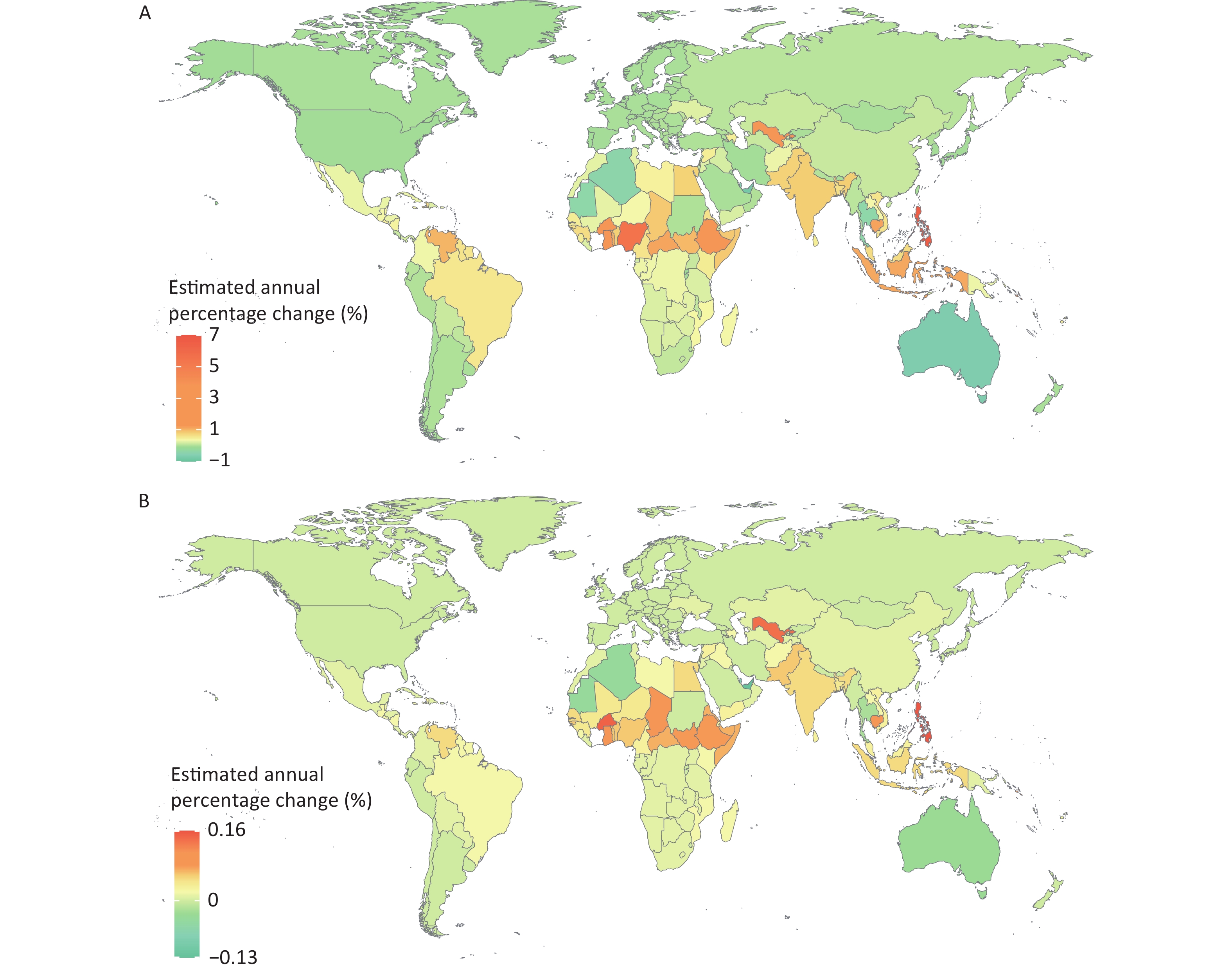
Among 204 countries and territories, the most remarkable increase in EAPC of ASMR attributable to high temperature was found in the Philippines (6.61%, 95% CI: 5.03%–8.21%), Nigeria (5.54%, 95% CI: 3.87%–7.23%), and Nauru (4.22%, 95% CI: 0.33%–8.26%). The top three countries with the largest EAPC of ASDR were the Philippines (0.16%, 95% CI: 0.14%–0.18%), Burkina Faso (0.15%, 95% CI: 0.13%–0.17%), and Uzbekistan (0.14%, 95% CI: 0.11%–0.17%). The trend in the spatial distribution of ASDR of CVD attributed to high temperature was similar to ASDR (Figure 4). Tropical countries have the highest CVD burden related to high temperature, possessing a higher trend of growth as well.
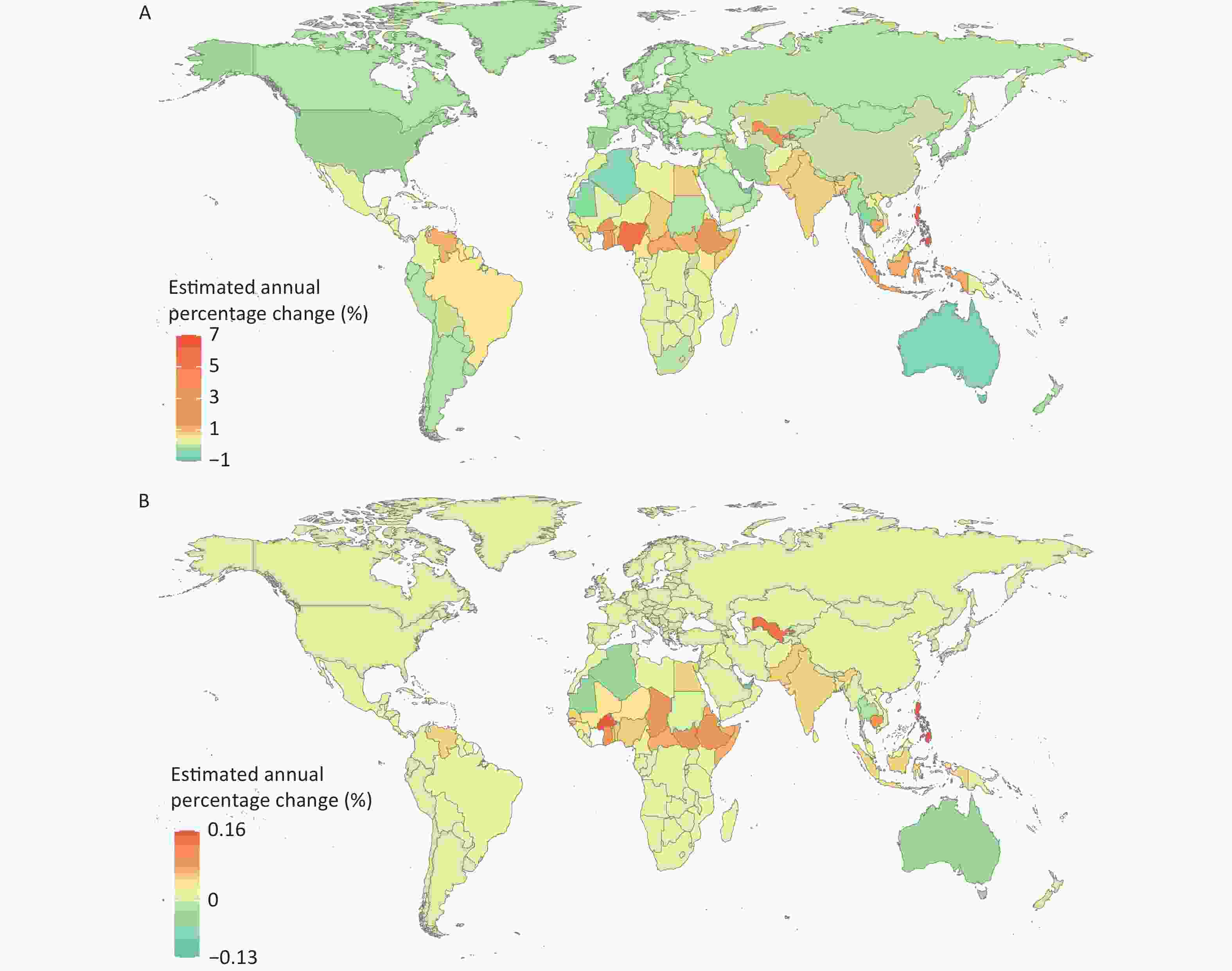
Figure 4. Estimated annual percentage change (EAPC) in age-standardized mortality rate (ASMR) and age-standardized disability-adjusted life year rate (ASDR) of cardiovascular disease (CVD) attributable to high temperature by country from 1990 to 2019. (A) EAPC in the ASMR of CVD attributable to high temperature by country from 1990 to 2019; (B) EAPC in the ASDR of CVD attributable to high temperature by country from 1990 to 2019.
-
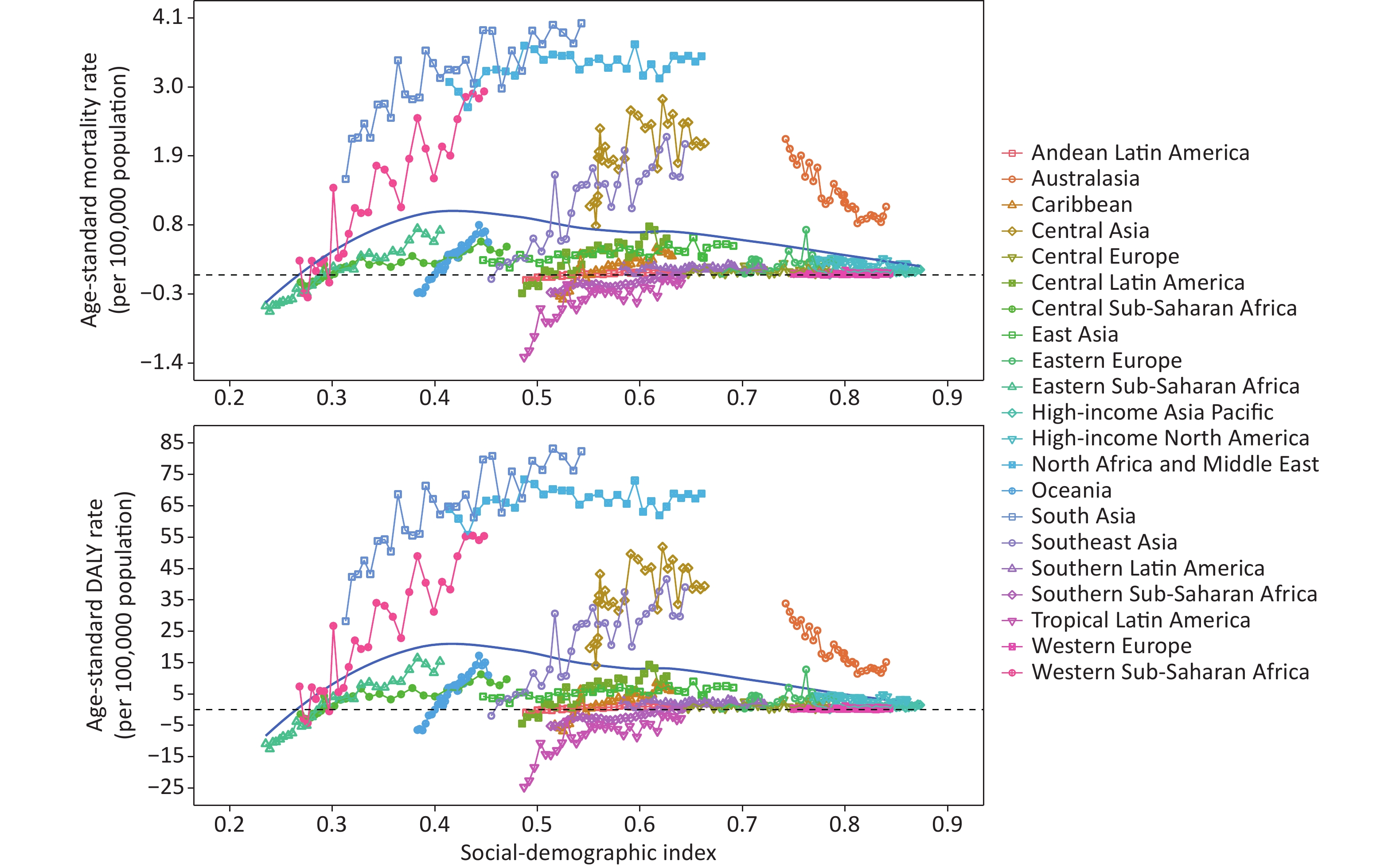
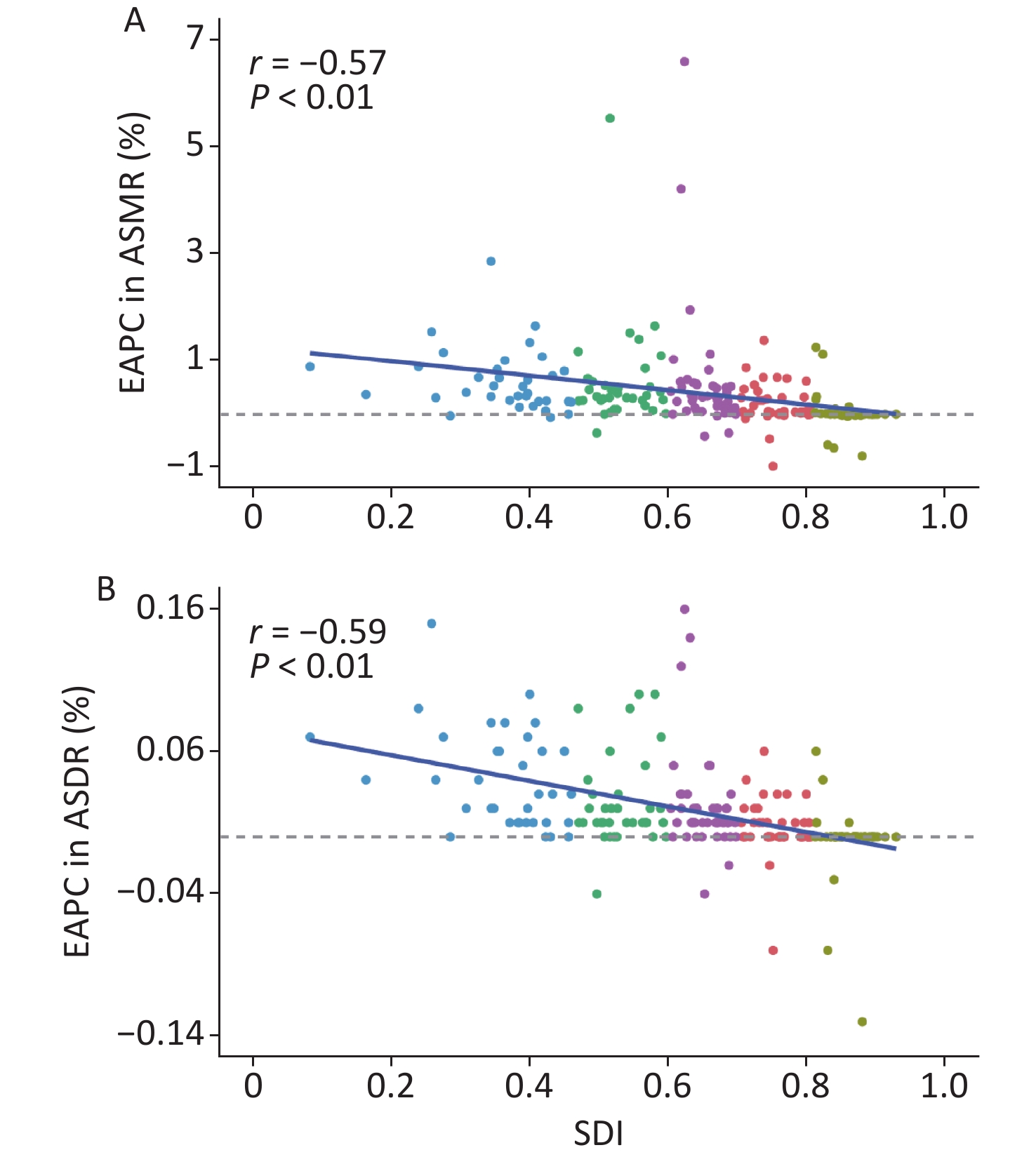
The fitted curve showed a nonlinear relationship between SDI and ASR, with a left-skewed inverted U-shaped curve that peaked at low SDI. The CVD burden associated with high temperature significantly increased in low-SDI regions (SDI < 0.4). In other SDI regions, the CVD burden slowly decreased as SDI increased (Figure 5). Over the past 30 years, the CVD burden attributable to high temperature increased in low and low-middle SDI regions and was higher than the global level. In contrast, the disease burden fluctuated less in high-middle and high-SDI regions (Supplementary Figures S1–S2, available in www.besjournal.com). We observed a negative correlation between SDI and EAPC in ASMR (rs = 0.57, P < 0. 01) and ASDR (rs = −0.59, P < 0. 01) among 204 countries, suggesting that regions with lower SDI might have a larger increase in CVD burden (Supplementary Figure S3, available in www.besjournal.com).
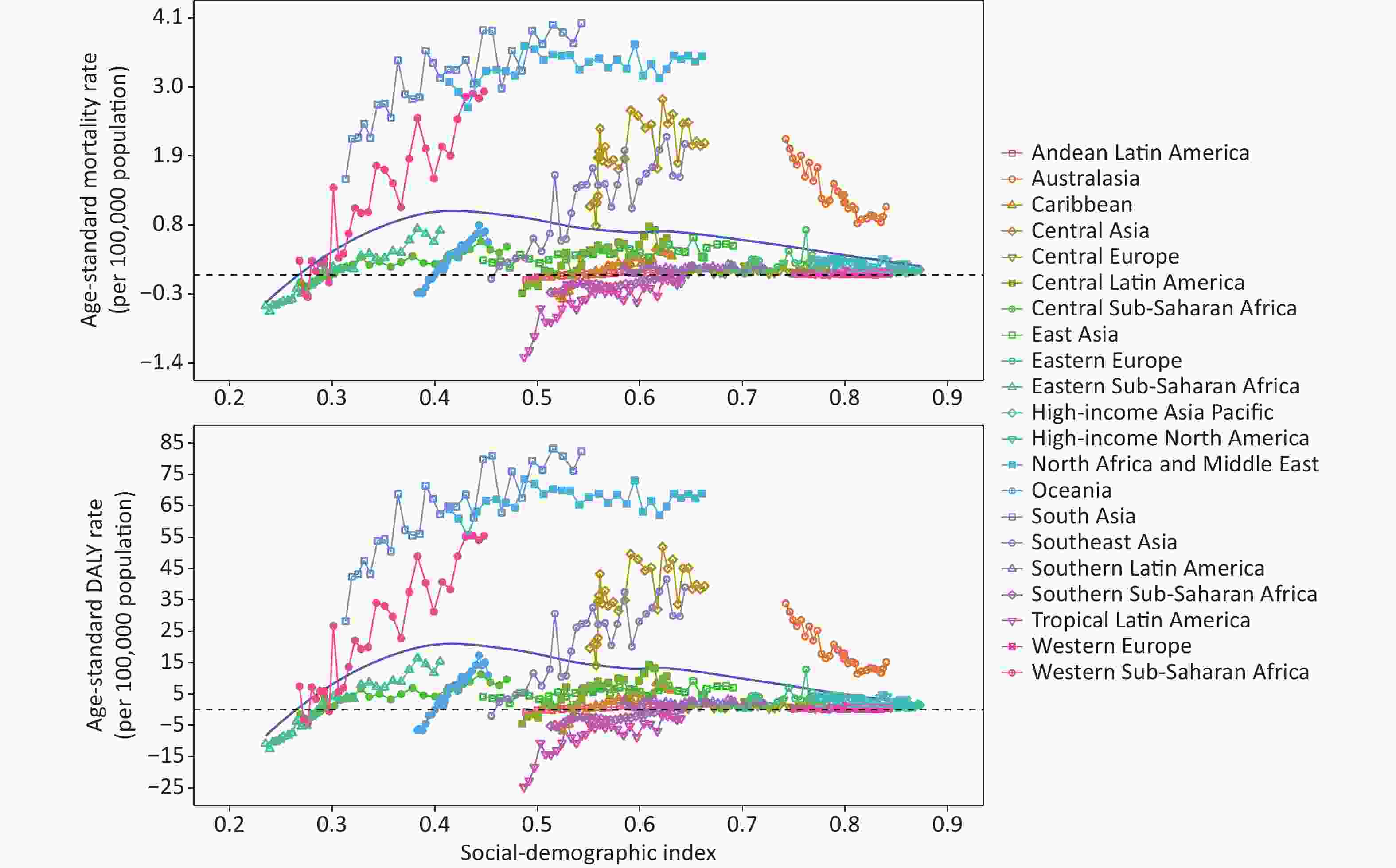
Figure 5. Age-standardized mortality rate and DALY rate of cardiovascular disease attributable to high temperature by region from 1990 to 2019. DALY, disability-adjusted life year.
-
This study provided a systematic analysis of the spatiotemporal changes in the CVD burden attributable to high temperature from 1990 to 2019 globally by sex, region, and SDI. From 1990 to 2019, the global burden of disease attributable to high temperature showed an overall increasing trend and varied across countries and regions. The highest disease burden was in low-SDI regions and low-latitude countries. In addition, the EAPC of ASR was negatively correlated with SDI among 204 countries, suggesting that low-SDI countries were associated with higher EAPC in ASR.
Health loss was consistently greater in males, and this gender inequality could have multiple explanations. First, males who work outdoors for a long time are more likely to be exposed to high temperatures, which can lead to CVD [26, 27]. Furthermore, in terms of thermoregulation, female-specific hormones, such as progesterone, can increase core body temperature and delay the sweating threshold [28]. Estradiol can lower the sweating threshold, leading to an increased sweating rate at specific core body temperatures, which facilitates heat dissipation. In contrast, males lack the protection of corresponding hormones, which cause them to be more intolerant to high temperature. Therefore, the government needs to develop better policies to reduce the chance of hot weather exposure, especially for males, to minimize the impact of such factors for decades to come.
The CVD burden due to high temperatures considerably varies across countries and regions from 1990 to 2019. South Asia, North Africa, and the Middle East with lower latitudes had the greatest burden. Meanwhile, the burden is more severe in low and middle-SDI countries. Nearly 80% of global CVD deaths occurred in low and low-middle SDI countries [29, 30]. This may be due to differences in healthcare resources due to economic development imbalances between countries and regions. Low and low-middle SDI regions have fragile healthcare systems and lower effective coverage of health services compared with high-SDI countries [31-33]. Further, higher population proportions chronically engaged in long-term outdoor physical labor in low- and low-moderate SDI countries resulted in greater heat exposure compared to high-SDI regions. Differences in geography and climate distribution may be potential factors for low-latitude countries. Countries and regions near the equator have significantly higher average annual temperatures and greater incidences of heatwaves, making people in these regions more vulnerable to high temperatures[34, 35]. Several studies have also demonstrated that the underlying tropical climate types, such as dry tropical and moist tropical, are significantly associated with increased CVD mortality [36, 37].
Therefore, 178 countries and territories signed the Paris Agreement at the UN Climate Conference in 2015, which aims to limit global warming to below 2 °C to cope with the health challenges caused by global warming [38]. Our results revealed that ASR, due to high temperatures, showed a brief downward trend before rising again after 2015, indicating that these measures and policies may have little impact on addressing global warming. The global average surface temperature is projected to increase by approximately 3.7 °C– 4.8 °C over the next 100 years under the “no policy” reference scenario, which will result in an increasing number of people suffering from CVD due to high temperatures [39]. The impact of high temperatures on CVD has mainly occurred in the poorest and most vulnerable populations. This suggests that low-income countries with high greenhouse gas emissions have a heightened need to reduce carbon emissions to diminish the heat-related CVD burden [40]. Regions most affected by high temperatures should pay more attention to the impact of high temperatures on CVD due to global warming to reduce their health burden. Reducing the impact of heat on CVD depends on the overall policy framework and commitment, which requires concerted efforts by governments [41].
This study specifically elucidated the spatiotemporal trends of CVD burden attributable to high temperature from 1990 to 2019 by different countries, regions, and sex, using metrics, including numbers of deaths and DALYs, ASR, and EAPC. In particular, this study has far-reaching implications for low- and middle-income and low-latitude countries. However, our study has several limitations. First, CVD-related deaths might be underestimated, considering the difficulty in distinguishing mortality from CVD and death due to its comorbidities. Second, the climate varies within some countries, such as China, the United States, and several other countries with large geographical areas. Therefore, further assessing the temporal trends of susceptible populations and diseases in different regions of each country is necessary. Furthermore, the data are highly dependent on GBD, and its data availability and quality vary across locations, with only a few countries and regions providing actual data, while data in some countries rely heavily on simulation models and extrapolations from other regions. This unavoidable drawback has been reported in other articles [42, 43]. In addition, relatively few studies reported on the association of temperature with health outcomes, such as CVD, and the temperature-related burden estimated by GBD based on these studies is much smaller than the actual.
-
In summary, we systematically assessed the global burden of CVD due to heat exposure, providing a comparative analysis among 204 countries and territories. We found that the high-temperature effect on CVD burden has varied over the past three decades but overall is on the rise. Moreover, the burden considerably differs across countries and regions from 1990 to 2019, with the highest burden in low-income and tropical countries. Health losses in males were consistently greater. These findings will be committed to promoting the achievement of carbon neutrality and improving cardiovascular health.
-
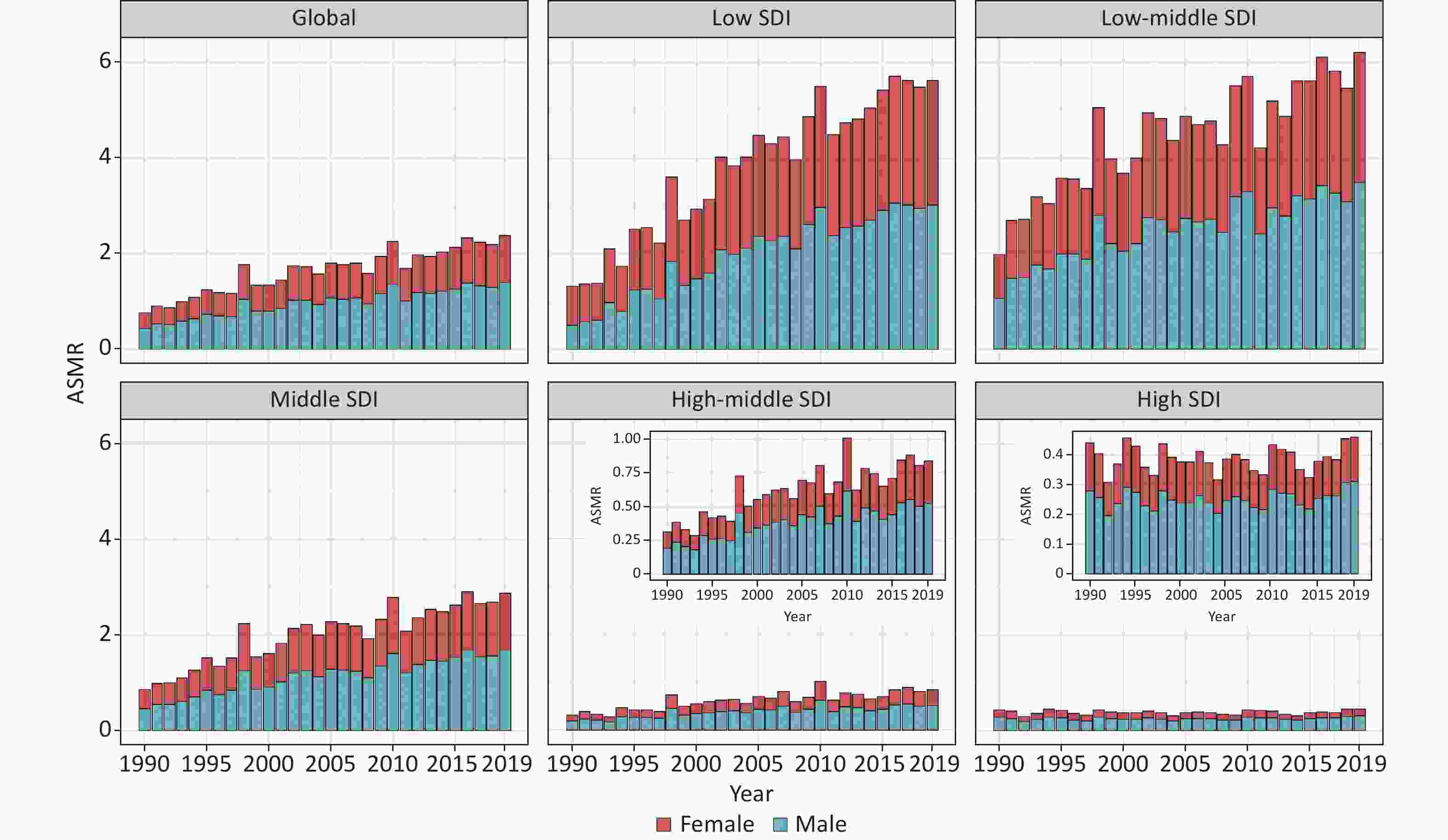
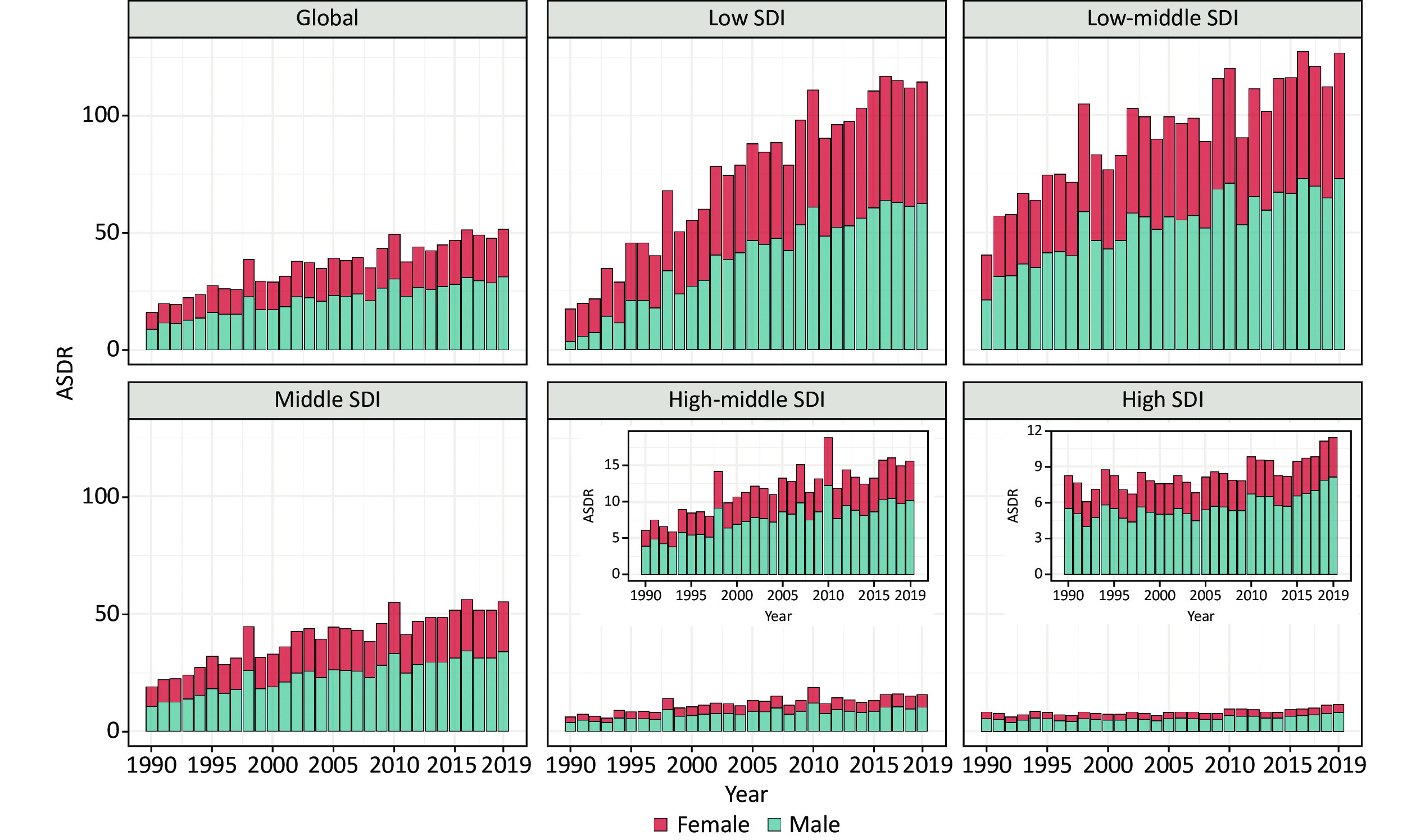
Figure S1. Age-standardized mortality rate of global and different SDI regions divided by sex from 1990 to 2019. SDI, socio-demographic index; ASMR, age-standardized mortality rate.
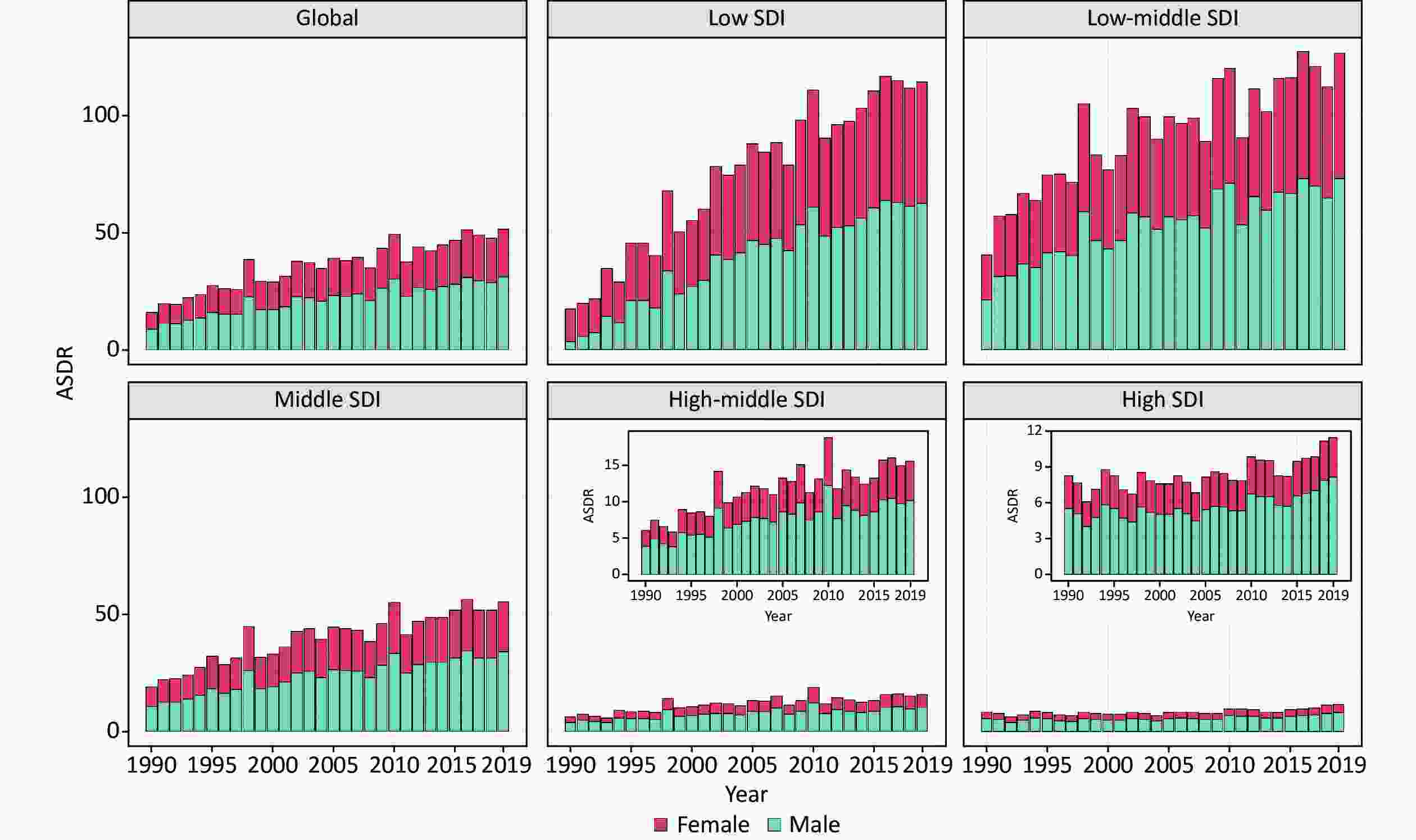
Figure S2. Age-standardized DALYs rate of global and different SDI regions divided by sex from 1990 to 2019. SDI, socio-demographic index; DALYs, disability-adjusted life years; ASDR, age-standardized DALYs rate.
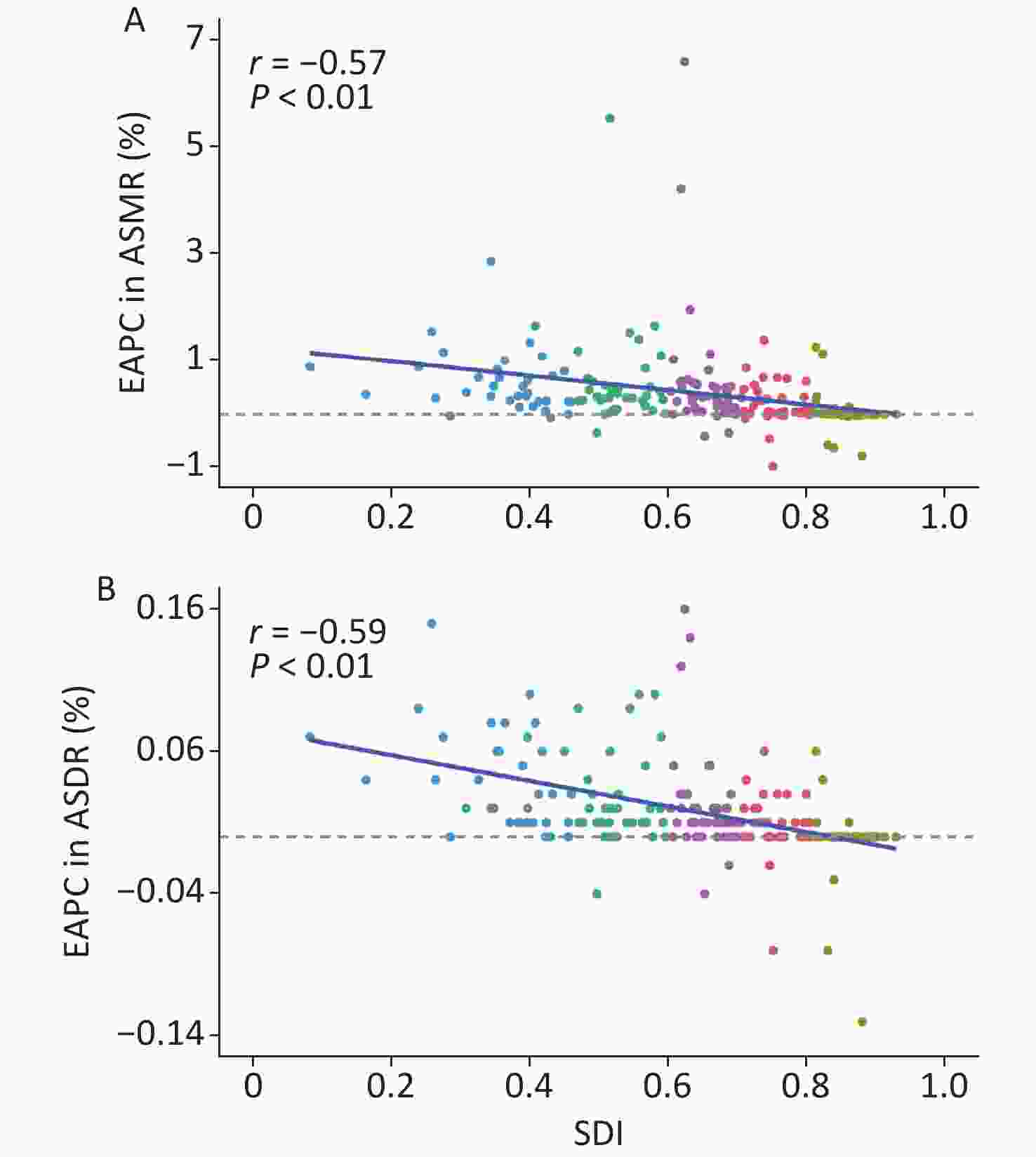
Figure S3. The correlation between Socio-demographic index and estimated annual percentage change of CVD attributable to ambient high temperature. (A) The relationship between SDI and EAPC in ASMR; (B) The relationship between SDI and EAPC in ASDR. DALYs, disability-adjusted life years; ASMR, age-standardized mortality rate; ASDR, age-standardized DALYs rate; EAPC, estimated annual percentage change; CVD, cardiovascular disease.
HTML
Data Sources
Exposure and Health Outcome
Statistical Analysis

Global Burden of CVD Attributable to High Temperatures
Global Burden of CVD Attributable to High Temperature by Gender
Global CVD Burden Attributable to High Temperature by Countries and Regions
Global CVD Burden Attributable to High Temperature by SDI
CONFLICTS OF INTEREST The authors declare no competing financial interests.
&These authors contributed equally to this work.
 22191Supplementary Materials.pdf
22191Supplementary Materials.pdf
|

|

 Quick Links
Quick Links
 DownLoad:
DownLoad: