



-
With a total of 697.5 million patients globally[1], chronic kidney disease (CKD) has become a major public health problem; especially, China reports 132.3 million cases, accounting for approximately 20% of the global burden [1, 2]. A better understanding of the potential risk factors of CKD would shed light on the early detection and prevention of the disease.
Uric acid is the main metabolite of purine compounds in humans [3]. Past studies have suggested that serum uric acid (SUA) plays a role in hypertension, cardiovascular diseases, and kidney diseases [4, 5]. However, previous studies report mixed results on whether SUA is an independent risk factor for the development of kidney diseases [6, 7]. A study from the United States with a long-term follow-up reported that elevated SUA levels were associated with progressive kidney function impairment and the development of CKD among the Jackson Heart Study population [8]. A Japanese cohort study suggested higher SUA levels as a risk factor for the development of kidney dysfunction in the general population [9]. However, Chonchol et al. [10] evaluated the Cardiovascular Health Study individuals detected SUA level was associated with a subsequent decrease in the estimated glomerular filtration rate (eGFR) but without any association with CKD. Some reports have concluded that SUA is not a risk factor for kidney failure in patients with CKD [11]. The existing evidence is inconsistent. In addition, most studies focused on a composite CKD outcome, and the exploration of whether SUA is associated with the early marker of kidney function decline (eGFR) is limited. There are only a few national population-based studies in this regard, especially from developing countries [6, 12]. Therefore, whether SUA is a predictor for the early change in kidney function decline remains to be elucidated.
This study used data from the China Health and Retirement Longitudinal Study (CHARLS), a nationally representative longitudinal cohort sample, to analyze the association between SUA and the early marker of kidney function decline among the Chinese population aged ≥ 45 years to further explore the potential modifiers for CKD prevention.
-
The CHARLS study is a national longitudinal survey conducted by the National School of Development of Peking University on the Chinese population aged ≥ 45 years, including information regarding demographics, health status, physical function, and venous blood sample data, among others. This study aims to establish a high-quality public micro-database with a wide range of information sourced, ranging from socioeconomic status to health circumstances [13].
To date, four waves of the nationwide survey have been conducted in 2011 (visit 1), 2013 (visit 2), 2015 (visit 3), and 2018 (visit 4). The blood sample data were collected only at visits 1 and 3. The details of the design and conduct of CHARLS are described elsewhere [13]. In this study, only participants who had blood sample data at visits 1 and 3 were enrolled. Individuals who lacked SUA data at visit 1 or who lacked creatine data at visits 1 or 3 were also excluded. A total of 7,520 participants had blood sample data at visits 1 and 3, with 174 individuals lacking SUA data at visit 1 or creatine data at visits 1 or 3. A total of 7,346 participants were finally included in the assessment. The study protocol was approved by the Ethical Review Committee of Peking University (IRB00001052-11015). All methods were conducted in accordance with the relevant guidelines and regulations (Declaration of Helsinki). All participants provided their signed informed consent.
-
The target exposure variable was baseline SUA. The baseline SUA can be classified into five categories (Q1: 0–3.39, Q2: 3.39–3.97, Q3: 3.97–4.57, Q4: 4.57–5.36, and Q5: ≥ 5.36 mg/dL) according to quintiles at the baseline SUA at visit 1. The outcome was kidney function decline, which is defined as an annual eGFR decrease by > 3 mL/min per 1.73 m2 [14-17]. eGFR (mL/min per 1.73 m2) was estimated from the baseline serum creatinine using the CKD-EPI creatinine equation (2009)[18]: 141 × min(Scr/κ, 1)α × max(Scr/κ, 1)−1.209 × 0.993Age[× 1.018 if female][× 1.159 if black], where Scr is serum creatinine, κ is 0.7 for women and 0.9 for men, α is −0.329 for women and −0.411 for men, min is the minimum of Scr/κ or 1, and max is the maximum of Scr/κ or 1. The rate of annual change in eGFR was calculated by using the following equation: (eGFR in 2015 − eGFR in 2011)/4.
-
Based on the biological plausibility or with reference to the past studies [19-21], the following candidate covariates were examined as potential confounding factors: age (years), sex (male, female), gross domestic product (GDP) per capita (low: < 24.41 thousand ¥, middle: 24.41 to 31.57 thousand ¥, high: ≥ 31.57 thousand ¥), baseline eGFR (mL/min per 1.73 m2), hypertension, diabetes, smoking (never or current/former), drinking (never or current/former), body mass index (BMI) (kg/m2), low-density lipoprotein (LDL) cholesterol (mg/dL), high-density lipoprotein (HDL) cholesterol (mg/dL), triglycerides (mg/dL), and C-reactive protein (mg/L). GDP per capita was classified into three groups by tertiles of 2010 GDP per capita of the included provinces [22]. Hypertension was defined by self-reported physician diagnosis of hypertension or blood pressure (BP) measurements ≥ 140/90 mmHg or the use of antihypertensive agents. Diabetes was defined by self-reported physician diagnosis of diabetes, a random blood sugar level ≥ 200 mg/dL, a fasting blood sugar level ≥ 126 mg/dL, a glycated hemoglobin level (HbA1c) ≥ 6.5%, or the use of hypoglycemic agents. BMI was calculated by dividing weight (kg) by the square of height (m), and BMI was classified into four levels (underweight: < 18.5 kg/m2, normal: ≥ 18.5 to 24 kg/m2, overweight: ≥ 24 to 28 kg/m2, obesity: ≥ 28 kg/m2).
-
Group comparisons of continuous and categorical variables were performed using one-way ANOVA and χ2 test, respectively. Multivariable logistic regression was performed to obtain the Odds ratios (ORs) and 95% confidence intervals (CIs) for the association of kidney function decline with the SUA level.
Three logistic regression models were considered to adjust the potential covariates defined a priori. Model 1 was adjusted for age, sex, GDP per capita, and the baseline eGFR. Model 2 was additionally adjusted for hypertension and diabetes. In Model 3, the adjustment further included smoking, drinking, BMI, LDL cholesterol, HDL cholesterol, triglycerides, and C-reactive protein. In these models, both continuous (for investigating linear trends) and categorical (for promoting interpretability) SUA variables were used with Q1 as the reference category. The shape of the association between SUA and kidney function decline was investigated through restricted cubic splines adjusted for the same potential confounders in Model 3, with 2 mg/dL SUA serving as the reference. Subgroup analyses by sex (male, female), age (< 60, 60 to 70, ≥ 70), or hypertension and diabetes status (without hypertension and without diabetes, with hypertension and without diabetes, with diabetes and without hypertension, and with hypertension and with diabetes) were performed using Model 3, considering the possibility that these variables at the baseline might modify the association of kidney function decline with the SUA level [23, 24]. Using the likelihood ratio test, the P for interaction was calculated between the SUA level (Q1: 0–3.39 mg/dL, Q2: 3.39–3.97 mg/dL, Q3: 3.97–4.57 mg/dL, Q4: 4.57–5.36 mg/dL, Q5: ≥ 5.36 mg/dL) and the stratification variables (i.e., sex, age, hypertension, and diabetes status) for each scenario by comparing models with and without an interaction term.
The complex survey design and the non-response rate were considered by using the inverse probability weighting method. Those with missing values in some variables were not included in the analyses containing the corresponding variables. Stata 15.0 (StataCorp, College Station, TX, USA) (
https://www.stata.com/ ) was applied for all statistical analyses, and two-sided P < 0.05 was considered to indicate statistical significance. -
A total of 7,346 participants were included in this study (3,387 men, 3,959 women). The mean age (standardized deviation, SD) of all participants was 58.91 (9.16) years (Table 1). The participants with higher SUA levels were more likely to be older, of the male gender, hypertensive, smokers, and drinkers. Table 2 depicts the baseline characteristics of the participants in accordance with the kidney function decline status. Those with kidney function decline were more likely to be older, of the male gender, hypertensive, diabetic, and smokers. In addition, they had a higher average eGFR and triglycerides.
Characteristics Overall Q1 Q2 Q3 Q4 Q5 P Participants, n (%) 7,346 (100.00) 1,528 (20.06) 1,610 (20.02) 1,521 (19.96) 1,411 (20.02) 1,276 (19.95) – Age (years, SD) 58.91 (9.16) 56.37 (8.79) 58.74 (8.85) 58.85 (9.07) 59.16 (8.82) 61.44 (9.56) < 0.001 Sex < 0.001 Men 3,387 (47.26) 280 (23.21) 494 (35.89) 674 (47.58) 856 (58.80) 1,083 (70.98) GDP per capita < 0.001 Low 2,814 (34.43) 488 (29.38) 605 (34.35) 564 (33.35) 550 (35.63) 607 (39.44) Middle 2,150 (27.02) 569 (33.58) 510 (30.39) 441 (28.41) 381 (24.96) 249 (17.71) High 2,382 (38.56) 471 (37.04) 495 (35.26) 516 (38.24) 480 (39.41) 420 (42.85) eGFR (mL/min per 1.73 m2, SD) 92.31 (14.51) 100.09 (10.49) 95.15 (12.37) 93.01 (13.64) 90.05 (13.89) 83.18 (15.92) < 0.001 Hypertension, n (%) 3,195 (43.60) 535 (33.55) 587 (40.99) 609 (41.19) 674 (47.91) 790 (54.39) < 0.001 Diabetes, n (%) 1,146 (15.69) 228 (13.27) 211 (16.13) 206 (13.96) 236 (14.81) 265 (20.27) < 0.001 Smoking < 0.001 Current/former 2,855 (38.79) 315 (25.11) 447 (32.75) 564 (39.75) 682 (45.61) 847 (50.79) Drinking < 0.001 Current/former 2,782 (38.65) 328 (26.70) 449 (31.76) 536 (38.64) 666 (44.60) 803 (51.62) BMI (kg/m2), n (%) < 0.001 Underweight 419 (5.27) 105 (7.46) 94 (6.17) 83 (4.93) 65 (3.44) 72 (4.33) Normal 3,760 (50.00) 818 (56.00) 774 (53.21) 771 (52.45) 705 (45.73) 692 (45.52) Overweight 2,198 (32.15) 393 (27.48) 432 (31.36) 435 (30.33) 485 (36.30) 453 (35.33) Obesity 929 (12.58) 145 (9.06) 164 (9.26) 174 (12.28) 202 (14.53) 244 (32.15) Systolic blood pressure (mmHg, SD) 130.62
(21.28)127.98
(20.00)129.26
(21.33)129.14
(20.83)132.78
(22.45)134.15
(21.17)< 0.001 Diastolic blood pressure (mmHg, SD) 79.30
(52.72)76.25
(34.07)80.30
(63.69)78.68
(54.10)80.06
(43.28)81.37
(62.58)0.116 HbA1c (%, SD) 5.26 (0.81) 5.32 (1.02) 5.22 (0.81) 5.22 (0.74) 5.25 (0.72) 5.27 (0.72) 0.006 Triglycerides (mg/dL, SD) 136.95
(109.57)119.70
(83.88)123.54
(86.50)131.58
(91.28)140.45
(112.50)169.62
(151.69)< 0.001 LDL cholesterol (mg/dL, SD) 115.20
(34.56)114.83
(32.95)116.30
(32.83)115.05
(33.14)116.44
(35.33)113.37
(38.23)0.104 HDL cholesterol (mg/dL, SD) 49.64 (15.24) 51.84 (14.35) 51.29 (13.73) 50.38 (15.86) 48.27 (14.97) 48.38 (16.50) < 0.001 C-reactive protein (mg/L, SD) 2.58 (6.71) 2.08 (5.78) 2.25 (5.74) 2.52 (7.28) 2.99 (7.58) 3.05 (6.89) < 0.001 Note. Q1: 0 to 3.39 mg/dL, Q2: 3.39 to 3.97 mg/dL, Q3: 3.97 to 4.57 mg/dL, Q4: 4.57 to 5.36 mg/dL, Q5: ≥ 5.36 mg/dL. There were 20, 25, 25, 26, 40, 894, 872, 46, and 13 individuals with missing information in hypertension, diabetes, smoking, drinking, BMI, systolic blood pressure, diastolic blood pressure, HbA1c and LDL-c, respectively. The inverse probability weighting method was applied in calculating the SDs, proportions and P values. SUA, serum uric acid; SD, standard deviation; GDP, gross domestic product; eGFR, estimated glomerular filtration rate; BMI, body mass index; HbA1c, hemoglobin A1c; LDL, low-density lipoprotein; HDL, high-density lipoprotein. Table 1. Participants characteristics at baseline, by SUA levels
Characteristics Kidney function decline P No Yes Participants, n (%) 6,342 (86.33) 1,004 (13.67) – Age (years, SD) 58.75 (9.12) 59.93 (9.35) < 0.001 Sex, n (%) < 0.001 Men 2,893 (47.02) 494 (48.82) GDP per capita < 0.001 Low 2,354 (33.29) 460 (41.61) Middle 1,910 (27.90) 240 (21.43) High 2,078 (38.81) 304 (36.96) eGFR (mL/min per 1.73 m2, SD) 91.89 (14.24) 94.96 (15.83) < 0.001 Hypertension, n (%) 2,718 (42.77) 477 (48.80) < 0.001 Diabetes, n (%) 978 (15.38) 168 (17.60) < 0.001 Smoking < 0.001 Current/former 2,434 (38.53) 421 (40.41) Drinking < 0.001 Current/former 2,388 (38.78) 394 (37.85) BMI (kg/m2) < 0.001 Underweight 353 (5.12) 66 (6.22) Normal 3,231 (50.07) 529 (49.55) Overweight 1,910 (31.95) 288 (33.43) Obesity 815 (12.86) 114 (10.80) Systolic blood pressure (mmHg, SD) 129.97 (20.57) 134.52 (24.76) < 0.001 Diastolic blood pressure (mmHg, SD) 79.05 (52.52) 80.83 (53.90) 0.341 SUA (mg/dL, SD) 4.52 (1.32) 4.57 (1.27) 0.219 HbA1c (%, SD) 5.25 (0.80) 5.30 (0.88) 0.076 Triglycerides (mg/dL, SD) 135.32 (98.94) 147.23 (160.85) 0.001 LDL cholesterol (mg/dL, SD) 115.79 (34.33) 111.46 (35.80) < 0.001 HDL cholesterol (mg/dL, SD) 49.61 (15.01) 49.83 (16.64) 0.668 C-reactive protein (mg/L, SD) 2.59 (7.00) 2.49 (4.39) 0.664 Note. There were 20, 25, 25, 26, 40, 894, 872, 46, and 13 individuals with missing information in hypertension, diabetes, smoking, drinking, BMI, systolic blood pressure, diastolic blood pressure, HbA1c and LDL cholesterol, respectively. SD, standard deviation; GDP, gross domestic product; eGFR, estimated glomerular filtration rate; BMI, body mass index; SUA, serum uric acid; HbA1c, hemoglobin A1c; LDL, low-density lipoprotein; HDL, high-density lipoprotein. Table 2. Baseline characteristics of individuals without or with kidney function decline
-
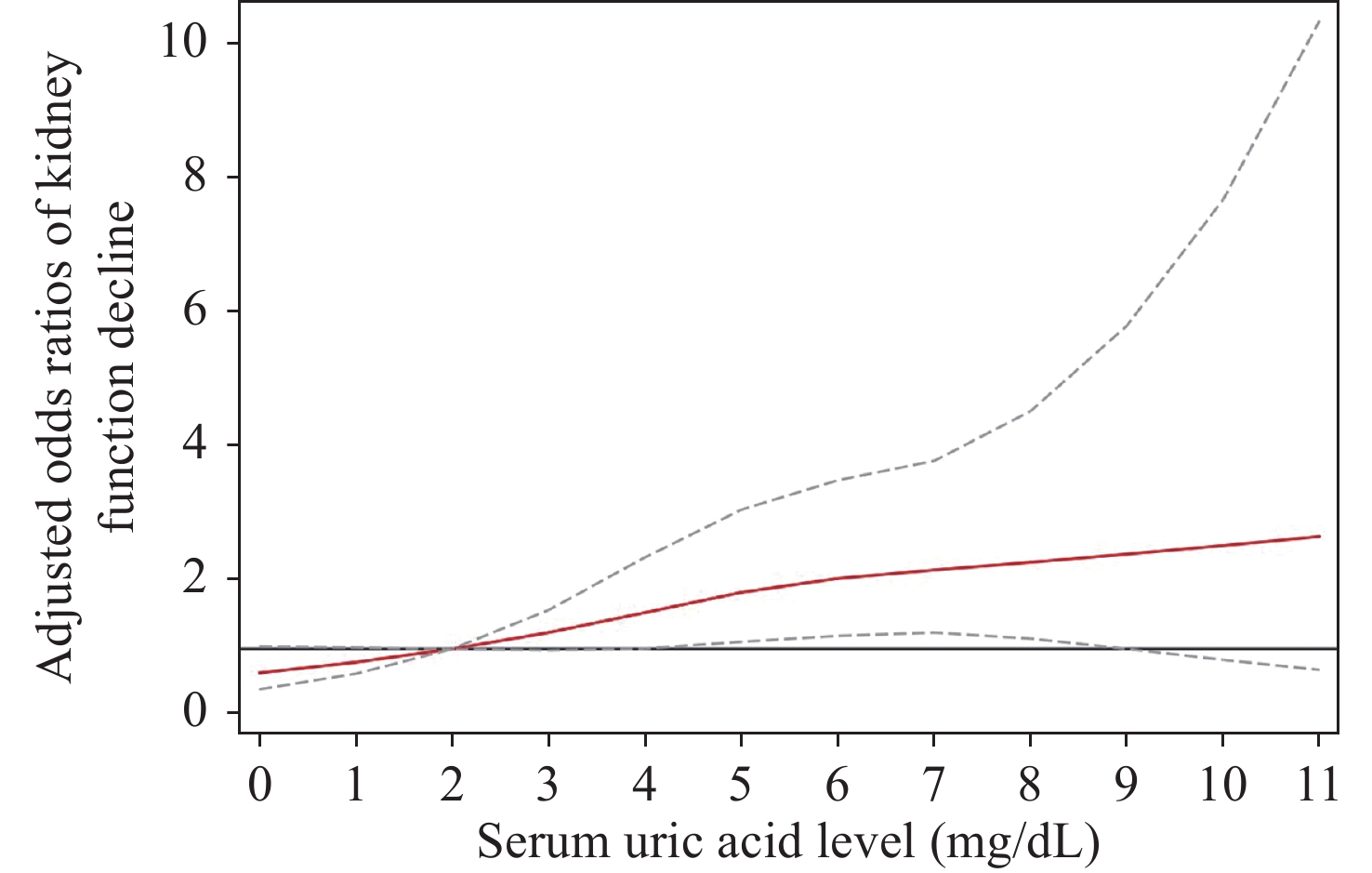
A total of 1,004 individuals (13.67%) developed a kidney function decline during the follow-up of 4 years. After adjusting for all potential covariates (such as age, sex, GDP per capita, baseline eGFR, hypertension, diabetes, smoking, drinking, BMI, LDL cholesterol, HDL cholesterol, triglycerides, and C-reactive protein), for every additional 1 mg/dL SUA, the risk of kidney function decline increased by 14% (OR 1.14, 95% CI 1.03–1.27), with a significant dose-response relation (Table 3). After adjusting for all potential covariates, the ORs for the second, third, fourth, and fifth versus the first quintile of SUA were 1.23 (95% CI 0.94–1.62), 1.41 (95% CI 1.06–1.87), 1.72 (95% CI 1.02–2.89), and 1.71 (95% CI 1.18–2.47), respectively. The restricted cubic spline analysis with 2 mg/dL SUA as the reference indicated that SUA > 5 mg/dL (which corresponds to the median of the fourth quintile) was associated with a significantly higher risk of kidney function decline (Figure 1).
SUA level Model 1 Model 2 Model 3 Q1 Ref Ref Ref Q2 1.27 (0.96–1.67) 1.24 (0.95–1.63) 1.23 (0.94–1.62) Q3 1.41 (1.06–1.88)* 1.39 (1.05–1.84)* 1.41 (1.06–1.87)* Q4 1.80 (1.04–3.10)* 1.72 (1.03–2.89)* 1.72 (1.02–2.89)* Q5 1.80 (1.24–2.60)** 1.70 (1.18–2.43)** 1.71 (1.18–2.47)** 1 mg/dL increase 1.14 (1.02–1.28)* 1.13 (1.02–1.26)* 1.14 (1.03–1.27)* Note. Q1: 0– < 3.39 mg/dL, Q2: 3.39– < 3.97 mg/dL, Q3: 3.97– < 4.57 mg/dL, Q4: 4.57– < 5.36 mg/dL, Q5: ≥ 5.36 mg/dL. *P < 0.05, **P < 0.01. Model 1 was adjusted for age, sex, GDP per capita and baseline eGFR. Model 2 was additionally adjusted for hypertension and diabetes. In Model 3, adjustment further included smoking, drinking, BMI, LDL cholesterol, HDL cholesterol, triglycerides and C-reactive protein. SUA, serum uric acid; eGFR, estimated glomerular filtration rate; GDP, gross domestic product; BMI, body mass index; LDL, low-density lipoprotein; HDL, high-density lipoprotein. Table 3. Odds ratios and 95% CIs for the association of SUA level with kidney function decline
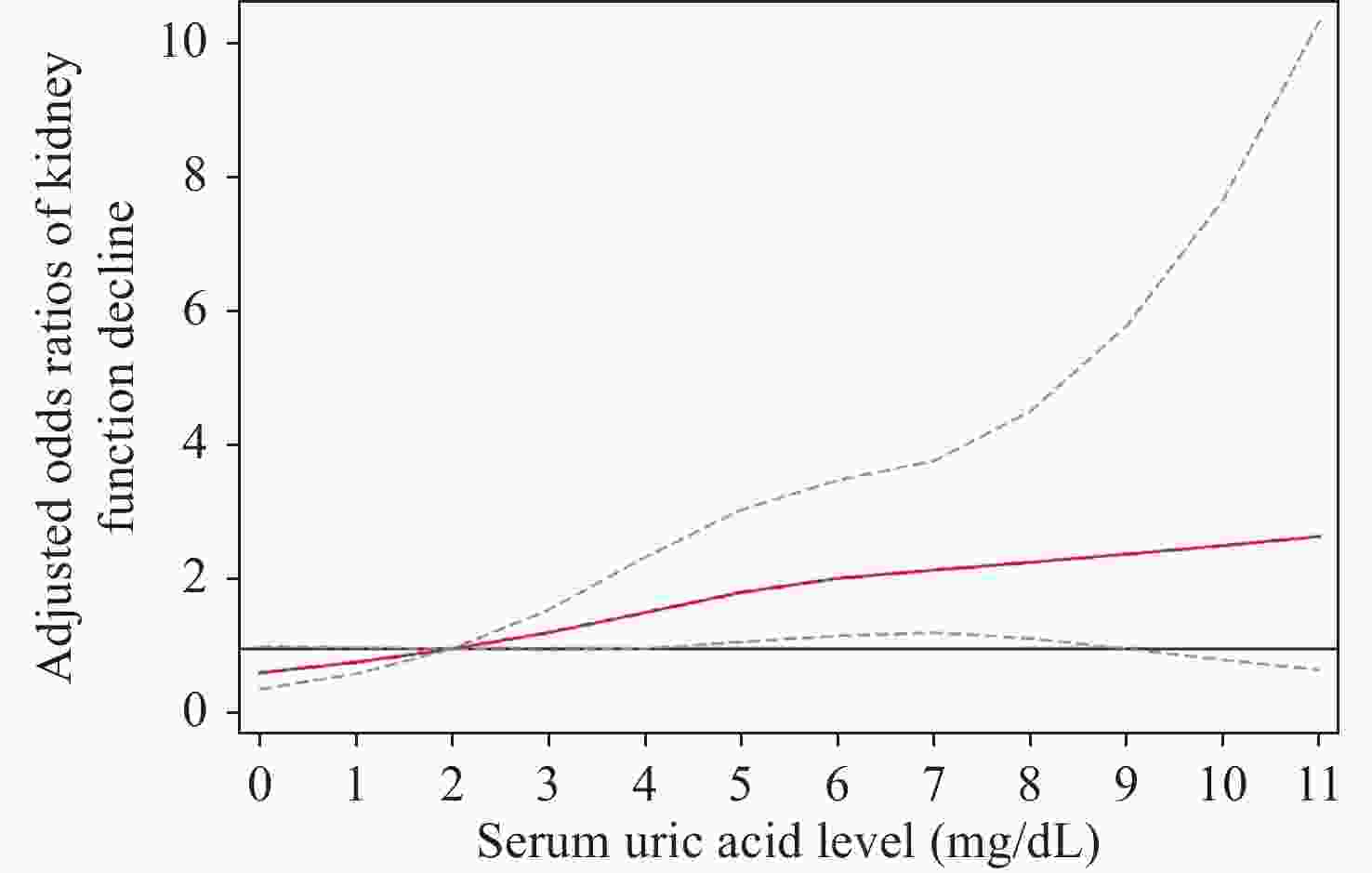
Figure 1. Restricted cubic splines analysis of the association between the SUA level and kidney function decline The red solid line represents age-adjusted odds ratios. The gray dashed lines represent 95% confidence intervals. The serum uric acid level was modeled by both-tail restricted cubic spline in a multivariable logistic regression model. The reference value is 2 mg/dL. SUA, serum uric acid.
-
After repeating the logistic model adjusted for all potential covariates among males and females, respectively, a significant positive dose-response relation was noted between the SUA and kidney function decline for women (OR 1.22, 95% CI 1.03–1.45). Although the dose-response relation was not recorded in men (OR 1.09, 95% CI 0.97–1.23), the high level of baseline SUA was found to be related to the kidney function decline (OR 1.83, 95% CI 1.05–3.17) (Table 4). In different age groups, only those aged < 60 years saw a significant positive dose-response relation between the SUA and kidney function decline (OR 1.22, 95% CI 1.05–1.42). Subgroup analyses by hypertension and diabetes status indicated a positive dose–response relation between SUA and kidney function decline only among those without hypertension and without diabetes, with an OR of 1.22 (95% CI 1.06–1.41). Subgroup analyses by hypertension status (not considering the diabetes status) revealed a positive dose-response relation only among those without hypertension (OR 1.22, 95% CI 1.07–1.39). For those without diabetes (not considering the hypertension status), a positive dose-response relation (OR 1.14, 95% CI 1.01–1.28) was noted, which was not detected among those with diabetes. The relationship between the SUA level and the risk of kidney function decline may depend on sex, age, or hypertension and diabetes status (All P for interaction < 0.001).
Subgroup Number Serum uric
acid levelOR Men 3,387 Q1 – Q2 1.38 (0.79–2.41) Q3 1.64 (0.95–2.83) Q4 1.33 (0.77–2.30) Q5 1.83 (1.05–3.17)* 1 mg/dL
increase1.09 (0.97–1.23) Women 3,959 Q1 – Q2 1.16 (0.84–1.59) Q3 1.21 (0.85–1.71) Q4 2.31 (1.13–4.72)* Q5 1.38 (0.75–2.50) 1 mg/dL
increase1.22 (1.03–1.45)* < 60 years 4,026 Q1 – Q2 1.19 (0.82–1.74) Q3 1.43 (0.97–2.12) Q4 2.13 (1.05–4.33)* Q5 2.00 (1.18–3.39)* 1 mg/dL
increase1.22 (1.05–1.42)* 60 to < 70 years 2,323 Q1 – Q2 1.28 (0.80–2.05) Q3 1.41 (0.88–2.27) Q4 1.16 (0.71–1.89) Q5 1.36 (0.77–2.39) 1 mg/dL
increase1.14 (0.99–1.31) ≥ 70 years 997 Q1 – Q2 1.25 (0.63–2.51) Q3 1.20 (0.58–2.45) Q4 1.48 (0.70–3.10) Q5 1.62 (0.72–3.63) 1 mg/dL
increase1.04 (0.85–1.26) Without hypertension &
without diabetes3,664 Q1 – Q2 1.60 (1.08–2.39)* Q3 1.75 (1.18–2.60)** Q4 1.87 (1.22–2.88)** Q5 2.77 (1.71–4.50)*** 1 mg/dL
increase1.22 (1.06–1.41)** With hypertension &
without diabetes2,511 Q1 – Q2 0.77 (0.50–1.17) Q3 0.88 (0.54–1.41) Q4 1.16 (0.48–2.82) Q5 0.78 (0.42–1.43) 1 mg/dL
increase1.02 (0.86–1.22) With diabetes &
without hypertension464 Q1 – Q2 2.52 (0.91–6.95) Q3 3.47 (1.32–9.14)* Q4 2.14 (0.66–6.96) Q5 2.75 (0.77–9.80) 1 mg/dL
increase1.21 (0.91–1.62) With hypertension &
diabetes679 Q1 – Q2 0.82 (0.34–1.99) Q3 1.24 (0.50–3.10) Q4 1.92 (0.80–4.56) Q5 1.43 (0.58–3.52) 1 mg/dL
increase1.12 (0.90–1.40) Note. Q1: 0 to 3.39 mg/dL, Q2: 3.39 to 3.97 mg/dL, Q3: 3.97 to 4.57 mg/dL, Q4: 4.57 to 5.36 mg/dL, Q5: ≥ 5.36 mg/dL. *P < 0.05, **P < 0.01, ***P < 0.001. The covariates were age, sex, GDP per capita, baseline eGFR, hypertension, diabetes, smoking, drinking, BMI, LDL cholesterol, HDL cholesterol, triglycerides and C-reactive protein. There were 28 individuals with missing information on hypertension (20 individuals) or diabetes (25 individuals). SUA, serum uric acid; eGFR, estimated glomerular filtration rate; OR, odds ratio; GDP, gross domestic product; BMI, body mass index; LDL, low-density lipoprotein; HDL, high-density lipoprotein. Table 4. Subgroup analyses for dose-response association between SUA and kidney function decline
-
In this study, in accordance with the large nationally representative sample, we found that, among the Chinese population aged ≥ 45 years, a high level of SUA was related to the risk of kidney function decline, which can also present in a positive dose–response manner. When stratified by sex, age, hypertension, and diabetes status, such a positive dose-response association was recorded among women, people aged < 60 years, and those without hypertension and diabetes. In men, although the dose-response relation was not observed, the high level of baseline SUA was found to be related to kidney function decline. SUA > 5 mg/dL was found to be associated with a significantly higher risk of kidney function decline.
Consistency with a past study [25], the present study demonstrated that a higher SUA level was associated with kidney function decline. A positive dose-response verified this result. Chonchol et al. [10] reported that, with an increase in the SUA levels by 1 mg/dL, the risk of kidney function decline increased by 14% among the participants of the Cardiovascular Health Study. Hsieh et al. [26] investigated the CKD stage 3–5 patients and noted a significant association with an odds ratio of 1.27 for kidney function decline with an SUA increased by 1 mg/dL. Moreover, the risk of kidney function decline started even in the normal range of the SUA level. Similar findings were determined in studies based on diabetes patients, according to which, a high-normal SUA may predict the development of CKD [27, 28]. Moreover, another two population studies found an association between the normal range of SUA and the increased risk of kidney function decline [15, 29]. The potential reasons and precisely from which SUA level this risk starts remain unknown. However, the data so far should provide a clue to the clinical consideration in this context.
The potential mechanisms behind the SUA-related kidney function decline may be as follows. First, elevated SUA levels could cause vessel endothelial dysfunction, prejudice endothelial nitric oxide (NO) production, and stimulate vascular smooth muscle cell proliferation in afferent arterioles [30, 31]. Second, uric acid is proinflammatory, which can increase the synthesis of monocyte chemoattractant protein 1, interleukin 1, interleukin 6, and tumor necrosis factor, possibly leading to the development of vascular diseases and atherosclerosis [32, 33]. Third, elevated SUA levels may stimulate the renin-angiotensin system, thereby promoting kidney injury [34]. Fourth, it was reported that an increase in SUA causes a greater microvascular remodeling mediated by endothelial function and NO availability [35]. These factors can induce a rigid artery wall and decrease its autoregulatory function, which can lead to the development of an impaired capacity of preglomerular vessels to maintain the constancy of glomerular pressure in the arterial phase [36]. Arterial pressure is then transmitted directly to the glomerulus, causing glomerular hypertension and resulting in glomerular hypertrophy and sclerosis [36]. In addition, elevated SUA induces high BP and type 2 diabetes mellitus, which can further lower kidney functions [37, 38].
In our study, women were found to be more vulnerable to elevated SUA level-induced kidney function decline. A previous cohort study demonstrated that women were more susceptible to SUA-mediated decline in eGFR [39]. Another population study in Japan also illustrated that hyperuricemia is an independent predictor of end-stage renal disease (ESRD) in women [40]. In addition, SUA was considered to be a predictive factor of residual renal dysfunction after renal donation only in women[41]. Although there is no clear mechanism for the sex difference in renal dysfunction related to the change of SUA, considering the existing evidence, we speculated that sex hormones (i.e., estrogen) may play a role in it. First, the incidence of high SUA-promoted elevation of plasma creatinine was greater in female mice in a past study [42]. Second, estrogen possibly induced kidney injury in female obese Zucker rats by increasing the triglyceride-rich lipoproteins concentration in the plasma [43]. Third, estrogen promoted microvascular pathology in the kidney of female stroke-prone spontaneously hypertensive rats [44].
The kidney function of people without hypertension and diabetes were more likely to be affected by elevated SUA level in this study. Zhang et al. [29] demonstrated that the uric acid level is independently associated with kidney function decline, wherein a higher odd ratio was detected among hypertension-free and diabetes-free participants (1.51) versus that in overall individuals (1.19). Hypertension could induce glomerulosclerosis, further leading to hypertensive nephropathy through renal vascular hemodynamics, renin-angiotensin system over-activation, and oxidative stress pathways, which result in eGFR decline [45-47]. Poor glycemic control has been associated with the development of diabetic nephropathy through increased production of free radicals, the accumulation of advanced glycation end-products (AGEs), and the activation of the RAS system and the protein kinase C (PKC) [48]. Therefore, the relationship between SUA and kidney function decline may tend to be more difficult to detect among those with hypertension or diabetes due to the aforementioned confounding factors. Similarly, when stratified by age group, the association between SUA ascending and kidney function decline was only observed among patients aged < 60 years. Since the older population suffers more from comorbidities such as DM and HT[49, 50], the relationship between the SUA level and eGFR decline may be difficult to comprehend.
Our study offers several strengths. The CHARLS is a nationwide longitudinal project conducted among middle-aged and older adults in China. This nationally representative large-scale study also contains blood sample tests and follow-ups that allow the detection of the relation between SUA and kidney function decline. In addition, the survey of CHARLS contains comprehensive related risk factors with rigorous measurements and quality assurance that provided an opportunity to adjust more potential confounding variables. Moreover, we further conducted dose-response and restricted cubic splines analysis on the basis of logistic regression to ensure the validity of our findings. Our findings will be useful in disease prevention and health management as well as provide information for further studies. However, there were still some limitations to this study. First, the follow-up duration was only 4 years, which limited us to exploring the longer-term effects of SUA on kidney function decline; therefore, further follow-up will be conducted in the future. Second, the covariates considered in this study cannot preclude all possible confounding factors, but almost all important cofounders considered in other studies were included in the present one [19-21]. Third, this study only uses creatinine to estimate the eGFR without considering cystatin C, but it has been reported that the performance of the creatinine equation, the cystatin C equation, and the creatinine-cystatin C equation are similar [18].
The present study demonstrated that SUA was associated with kidney function decline with a significant dose–response relation. Since hyperuricemia is prevalent, kidney dysfunction provides a great threat to the health of the general public, and our findings may shed light on SUA control and monitoring to help prevent the progression of kidney dysfunction. The elevation of uric acid level should be focused on to prevent possible kidney function decline.
HTML
Database and Study Population
Exposure and Outcome Assessment
Covariate Assessment
Statistical Analysis
Baseline Characteristics
SUA Level and Risks of Kidney Function Decline
Subgroup Analyses
CONFLICT OF INTEREST The authors declared no conflict of interest.

 Quick Links
Quick Links
 DownLoad:
DownLoad: