


-
Pneumoconiosis refers to a group of interstitial lung diseases that arise from the prolonged inhalation of occupational dust, resulting in chronic inflammation, immune dysregulation, and lung fibrosis[1]. According to the 2019 Burden of Disease database, there are currently 3.1 million cases of pneumoconiosis worldwide, with developing countries such as China experiencing a particularly significant burden. The complex pathogenesis of pneumoconiosis, along with the irreversible nature of pulmonary fibrosis, has led to a scarcity of effective therapeutic options. While the aetiology of pneumoconiosis is well established, additional factors, including diet, genetic susceptibility, and lifestyle habits, may influence an individual’s risk of developing the disease or its progression. Notably, moderate intake of polyunsaturated fatty acids (PUFAs) has been associated with a reduced risk of chronic respiratory diseases and the modulation of lung inflammation through the regulation of antioxidant signaling pathways[2]. However, the potential impact of PUFAs on pneumoconiosis remains an area requiring further investigation.
Mendelian randomization (MR) utilizes genetic variation as an IV to simulate a naturally randomized trial, with the aim of investigating potential causal relationships between exposure factors and outcomes[3]. Unlike randomised controlled trials (RCTs), which necessitate considerable time and financial resources, MR leverages existing genetic data for analysis. Furthermore, the utilisation of single nucleotide polymorphisms (SNPs) as instrumental variables (IVs) mitigates the impact of confounding factors, such as lifestyle and environmental variables, thereby enhancing the reliability of causal estimates.
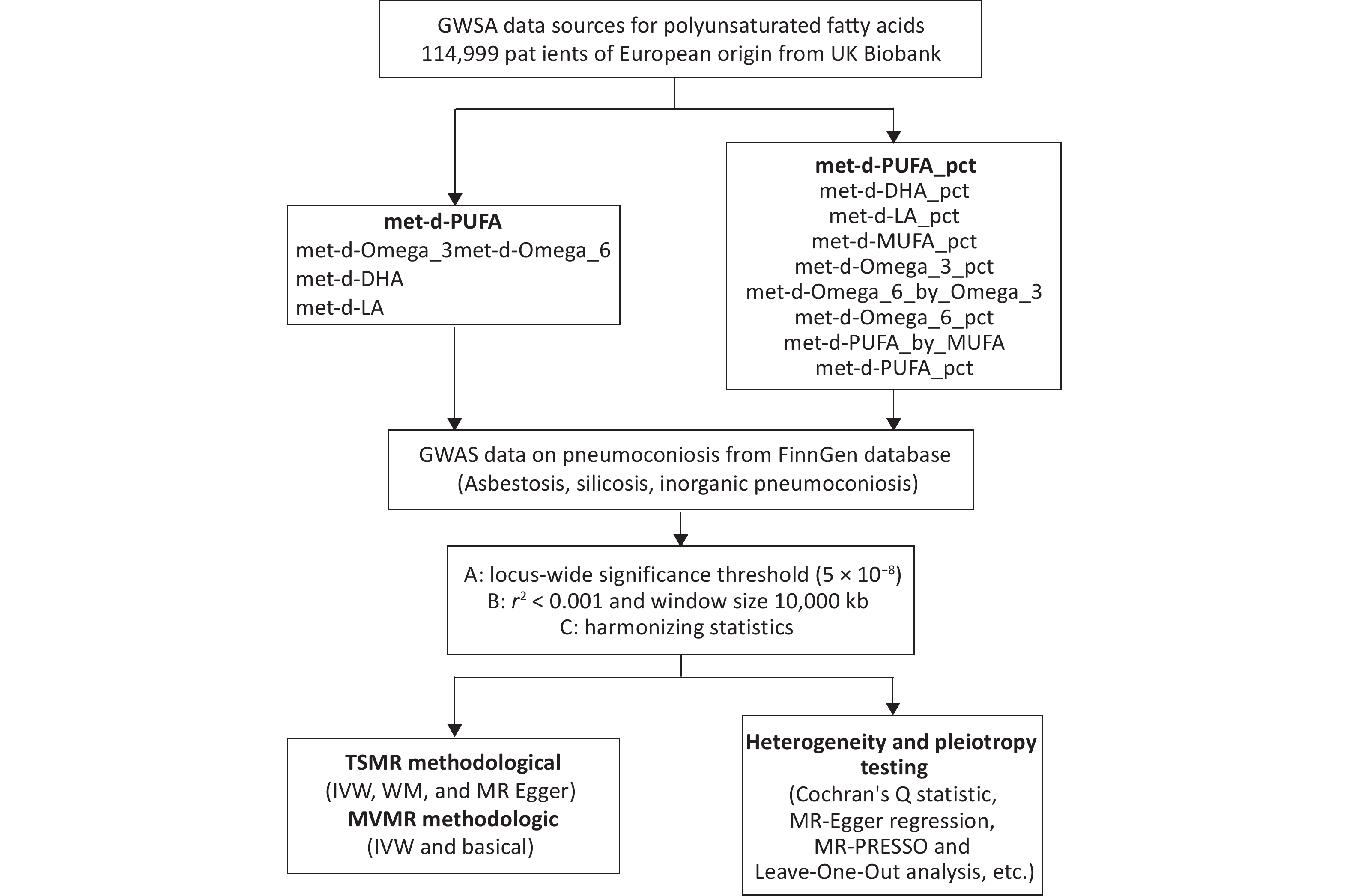
In this study, two-sample Mendelian randomization (TSMR) and multivariate Mendelian randomization approaches were utilized to examine the potential causal relationship between the intake and proportions of PUFAs and the risk of pneumoconiosis. The objective was to provide evidence supporting the adjustment of dietary PUFA types and proportions as an early preventive measure for this disease. The genetic IVs adhered to three fundamental assumptions: a strong correlation between the IVs and the exposure; the absence of any association between the IVs and known or potential confounders; and the influence of the IVs on the outcome occurring solely through the exposure. The specific study design is illustrated in Figure 1.
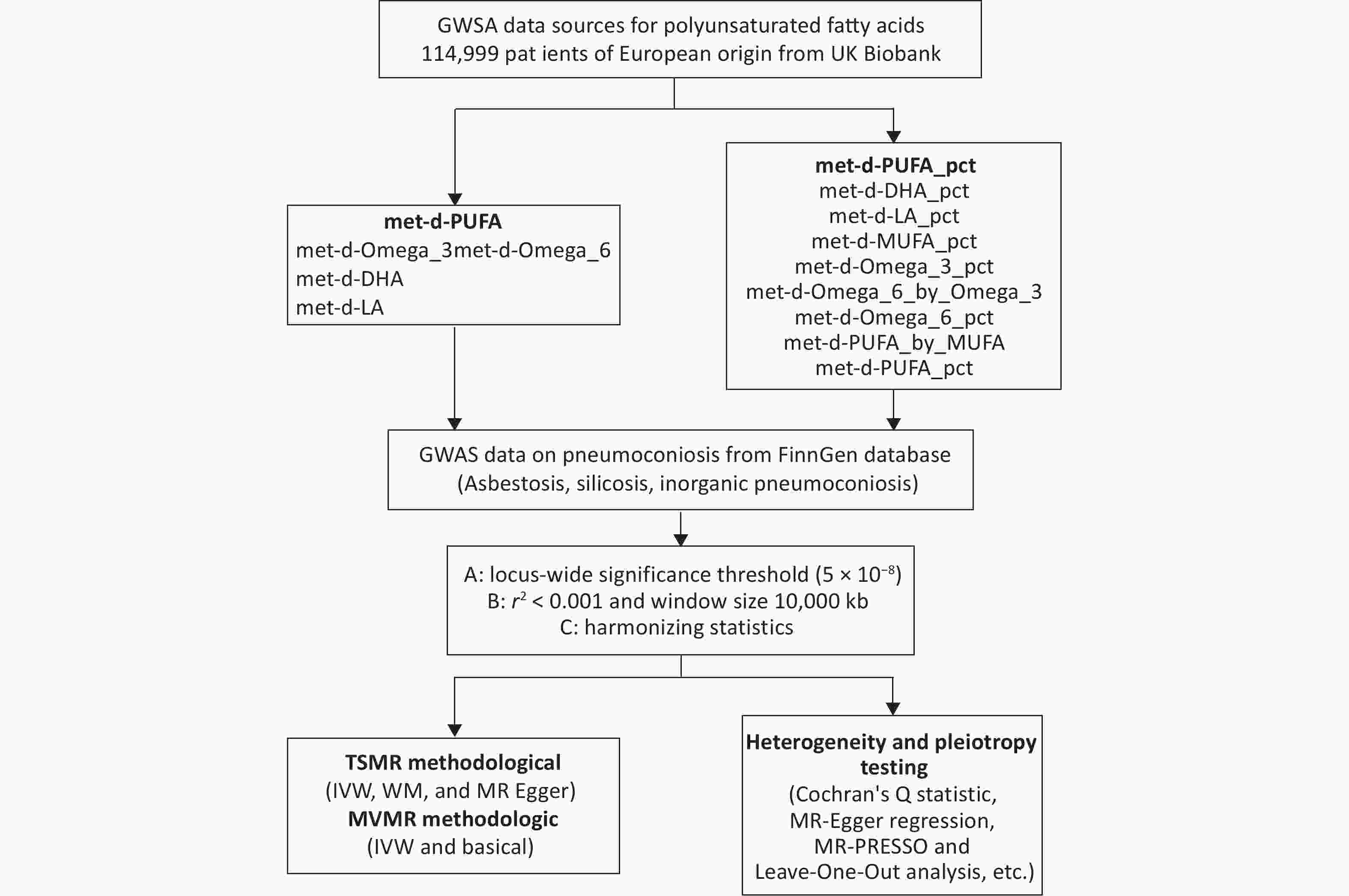
Figure 1. Research flowchart for two-sample and multivariate Mendelian randomization. MR, Mendelian randomization; TSMR, two-sample Mendelian randomization; IVW, inverse-variance weighted; WM, weighted median; MR-PRESSO, Mendelian randomization pleiotropy residual sum and outlier; MVMR, multivariable Mendelian randomization.
The UK Biobank includes around 500,000 participants, providing an extensive array of data regarding their lifestyles, health conditions, genetic profiles, and biospecimens. The genome-wide association study (GWAS) data related to fatty acids were sourced from this repository and include four primary exposures: omega-3 fatty acids, omega-6 fatty acids, monounsaturated fatty acids, and PUFAs. Additionally, secondary exposures comprise various ratios, such as the ratio of docosahexaenoic acid to total fatty acids, the ratio of linoleic acid to total fatty acids, and several other ratios involving monounsaturated, omega-3, and omega-6 fatty acids. The UK Biobank assessed circulating concentrations of omega-3 and omega-6 fatty acids, including linoleic acid and total omega-6, utilising a targeted high-throughput nuclear magnetic resonance (NMR) metabolomics platform. Pre-release data from a randomised subset of 126,846 non-fasting plasma samples, collected either at baseline or during the first repeat assessment, were made available to early access analysts. Following the removal of duplicate samples and the exclusion of those that did not meet quality control (QC) standards, a total of 121,577 samples were retained for analysis[4]. Further details regarding the study design, participant selection, and QC methods are available in prior publications.
FinnGen (https://www.finngen.fi/en), launched in Finland in 2017, represents a pioneering endeavour that integrates genomic data with digital healthcare records to promote advancements in medical research and clinical practices[5]. We selected FinnGen as the source of GWAS data on pneumoconiosis, specifically focusing on three subtypes categorised according to the International Classification of Diseases, Tenth Revision (ICD-10): asbestosis (J61), a pneumoconiosis resulting from the inhalation and retention of asbestos fibres; silicosis (J62), a respiratory disease caused by the inhalation of silica dust; and inorganic dust pneumoconiosis (J63), a form of pneumoconiosis due to other inorganic dusts. Detailed information regarding these conditions can be accessed at https://r11.risteys.finregistry.fi/endpoints. After adjusting for age, sex, genetic correlation, genotyping batch, and the first ten principal components, the number of SNPs for the three types of pneumoconiosis was found to be 16,380,466, 21,306,676, and 21,306,682, respectively. Further details on the pneumoconiosis GWAS data are provided in
Supplementary Table S1 (available in www.besjournal.com).SNPs associated with unsaturated fatty acids and their proportional distribution were initially screened using a stringent threshold of P < 5.0 × 10-8. To ensure the independent validity of the SNPs, we subsequently excluded potential linkage disequilibrium using the criterion of r² < 0.001. Additionally, we removed palindromic SNPs to mitigate correlations among IVs. An F-statistic greater than 10 is a commonly used threshold to ensure the strength and validity of IVs, thereby minimising the potential for weak instrumental bias. A comprehensive breakdown of this data is provided in
Supplementary Table S1 . PhenoScanner was utilised to retrieve all eligible SNPs while excluding those associated with potential confounders, such as smoking. The elimination of SNPs significantly associated with the outcome (P < 5 × 10-8) ensures that the IVs were not influenced by genetic factors related to the outcome.The Inverse Variance Weighted (IVW) approach, which integrates effect estimates from multiple IVs with the highest statistical power, serves as the primary and predominant method in TSMR analyses, providing a comprehensive and weighted estimate of the causal effect3. The weighted median method requires that over 50% of the selected SNPs are valid IVs to ensure the reliability of the overall causal effect. The MR-Egger method relaxes the Instrumental Strength Independent of Direct Effects assumption, allowing for the possibility that IVs may exert a direct influence on the outcomes. We conducted a thorough assessment of the causal relationships between different subtypes of PUFAs and pneumoconiosis using multivariate MR, focusing on the Basic model and the IVW methods.
Horizontal pleiotropy, in the context of MR, denotes that SNPs exert additional effects on the relationship between the exposure of interest and the outcome variable[3]. This occurrence may stem from complex biological pathways, the choice of IVs, and the characteristics of the study sample. The MR-Egger intercept analysis was employed to detect horizontal pleiotropy, with IVs deemed to exhibit horizontal pleiotropy if the intercept of the regression line significantly deviated from zero (P < 0.05). Furthermore, the MR-PRESSO method, which identifies and removes outliers, was utilised to assist in the detection and correction of horizontal multiplicity. To assess heterogeneity within the IVW and MR-Egger models, we applied the Cochran Q statistic to quantify its magnitude. Finally, leave-one-out analyses were conducted to assess the robustness of the results and identify SNPs that might have had a significant impact on the outcomes.
The study included a total of 627 SNPs, with each exposure having between 24 and 60 associated SNPs. Additionally, all selected IVs demonstrated F-statistics exceeding 10, with a mean value of 159.49, thereby confirming the statistical adequacy of these IVs (
Supplementary Table S1 ). Several smoking-related SNPs were excluded in the analysis for the second phenotype, including rs273912, rs11976955, rs13389219, rs1716407, rs2943656, rs6905288, rs4766578, and rs1800978.A total of seven subtypes of unsaturated fatty acids were identified as causally associated with pneumoconiosis in this study (Figure 2 and
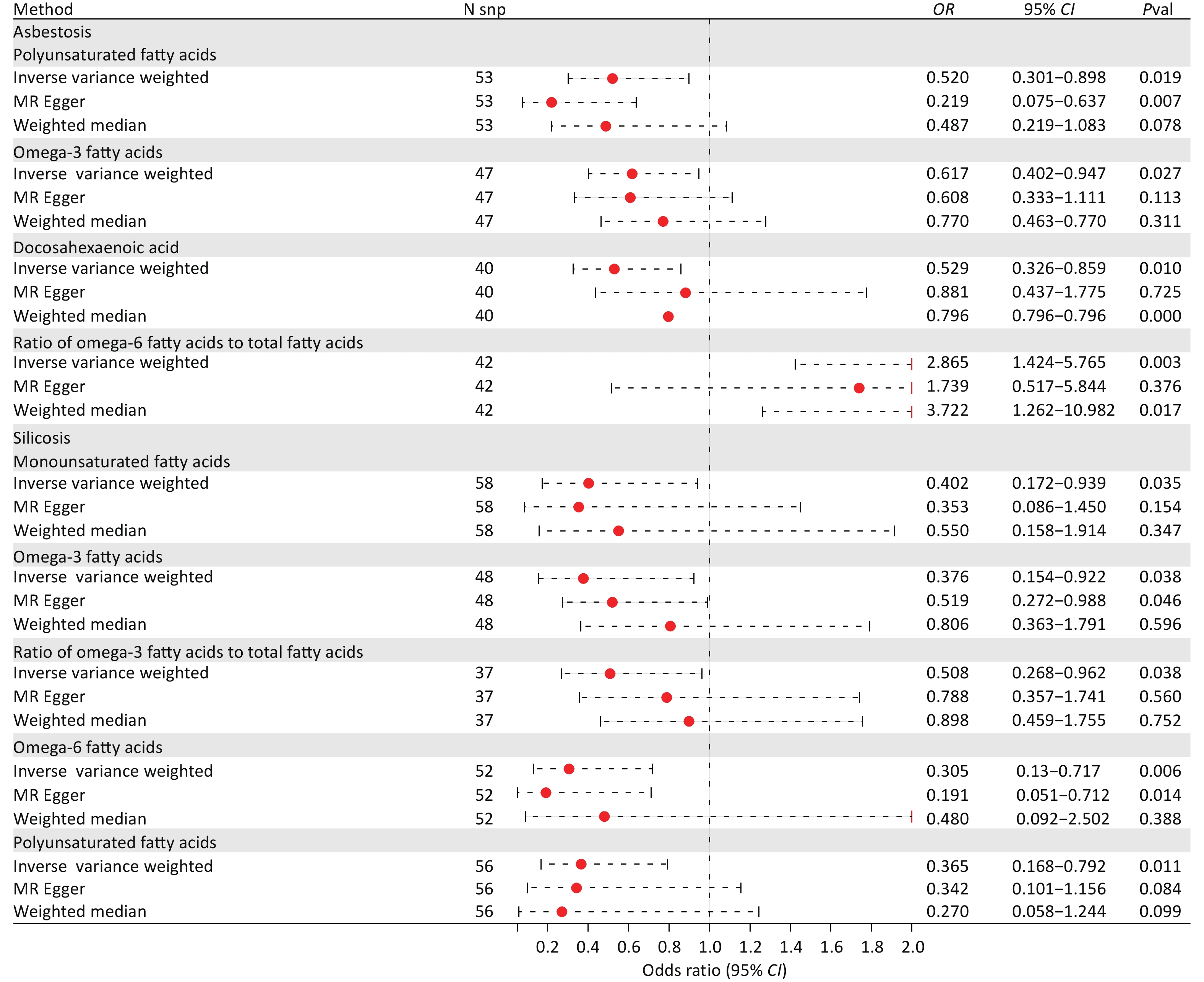
Supplementary Tables S2–S7 , available in www.besjournal.com). Among these, PUFAs, specifically omega-3 fatty acids, were linked to an increased risk of asbestosis and silicosis. Furthermore, we conducted a multivariate MR analysis examining the associations between all fatty acid subtypes and pneumoconiosis. Notably, only omega-3 fatty acids exhibited a significant causal effect on silicosis, despite the presence of other exposing factors. The IVW analysis method demonstrated that elevated levels of PUFAs (odds ratio [OR] = 0.520, 95% confidence interval [CI] = 0.301–0.898, P = 0.019), omega-3 fatty acids (OR = 0.617, 95% CI = 0.402–0.947, P = 0.027), and docosahexaenoic acid (OR = 0.529, 95% CI = 0.326–0.859, P = 0.010) were associated with a decreased risk of developing asbestosis, suggesting potential protective effects. In contrast, higher levels of the ratio of omega-6 fatty acids to total fatty acids (OR = 0.529, 95% CI = 0.326–0.859, P = 0.010) were correlated with an increased risk of developing the disease (Supplementary Table S3 ). For silicosis, monounsaturated fatty acids (OR = 0.402, 95% CI = 0.172–0.939, P = 0.035), PUFAs (OR = 0.365, 95% CI = 0.168–0.792, P = 0.011), omega-3 fatty acids (OR = 0.376, 95% CI = 0.154–0.922, P = 0.038), omega-6 fatty acids (OR = 0.305, 95% CI = 0.130–0.717, P = 0.006), and omega-3 fatty acids as a percentage of total fatty acids (OR = 0.508, 95% CI = 0.268–0.962, P = 0.038) were identified as protective factors for silicosis according to the IVW method (Supplementary Table S5 ).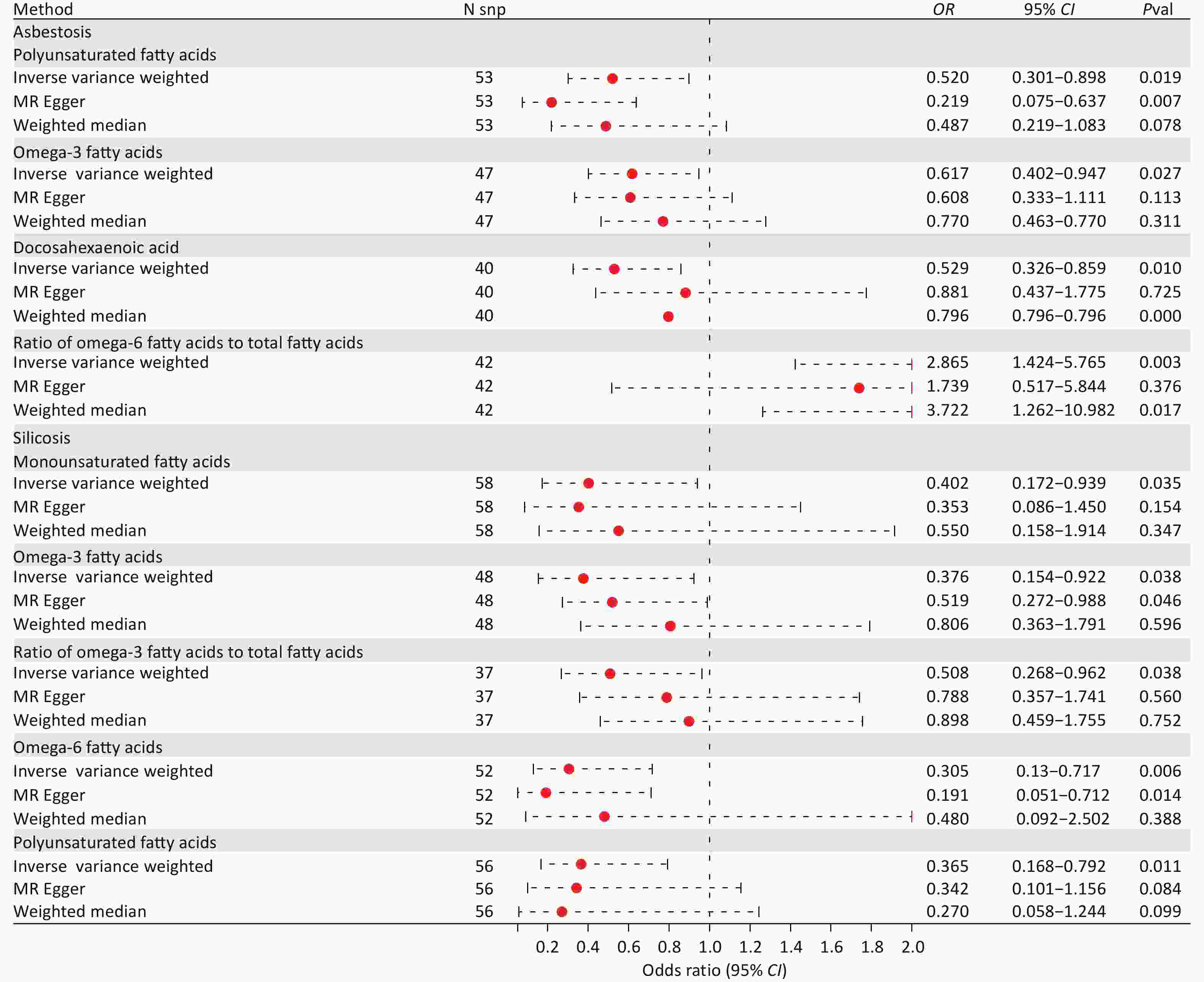
Figure 2. The forest plot showed primary results of the causal associations between PUFA and pneumoconiosis. OR, odds ratio; CI, confidence interval; Pval, P-value; SNP, single nucleotide polymorphism.
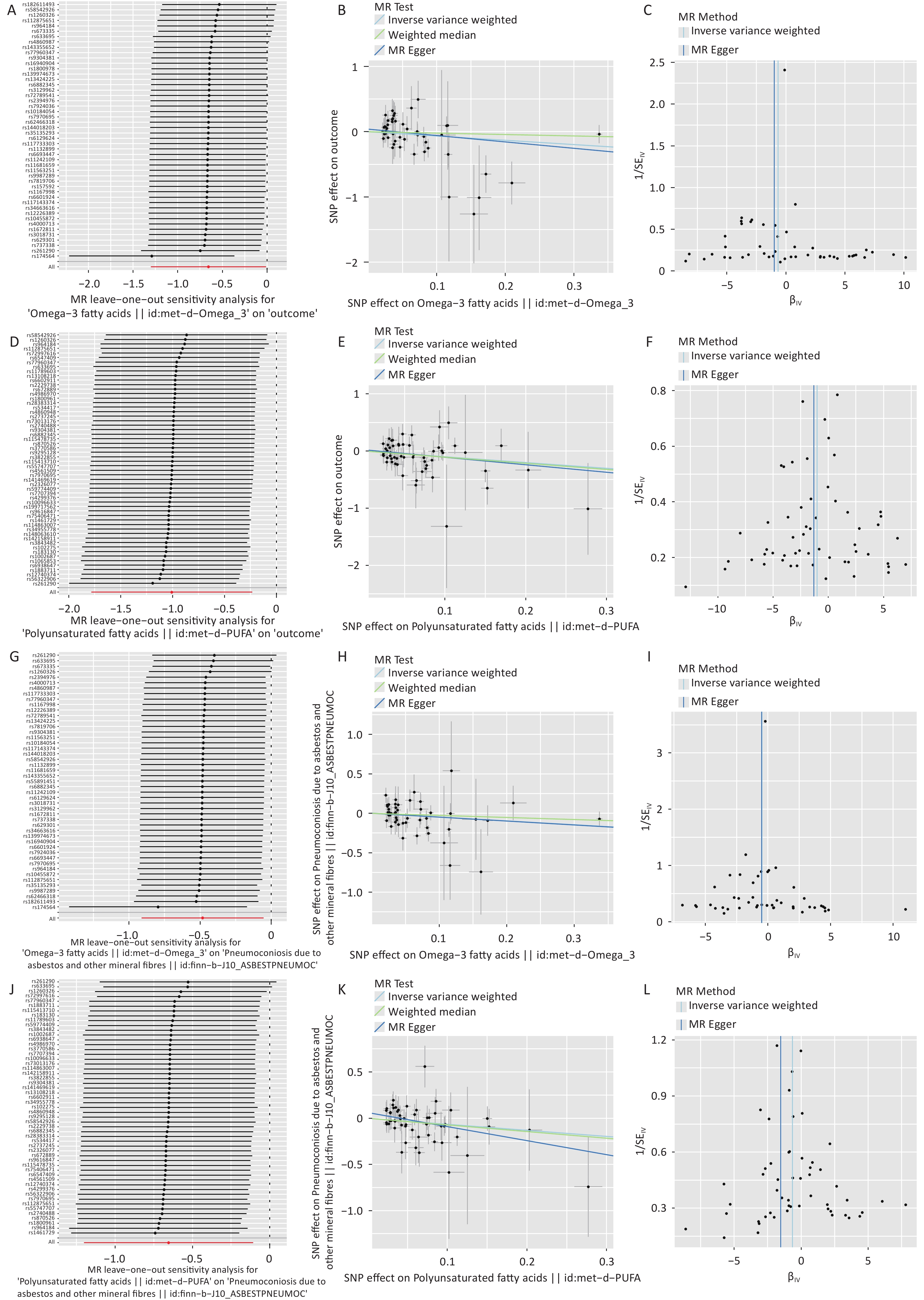
In light of the positive findings, the IVW model was subjected to a heterogeneity test. The results indicated that Cochrane’s Q statistic exceeded 0.05, signifying a consistent trend of effects across various IVs (Table 1). The minimum P-value observed in the MR-Egger regression was 0.055, suggesting an absence of substantial evidence for horizontal pleiotropy and reinforcing that the effect of IVs on the outcome variable primarily functions through the exposure factors, in accordance with the fundamental assumptions of MR analysis. Subsequent MR-PRESSO global tests further corroborated the absence of horizontal pleiotropy and outliers in the MR analysis. The symmetrical characteristics observed in all funnel plots indicate a reduced likelihood of publication bias in the study’s results (
Supplementary Figure S1C , F, I, L, available in www.besjournal.com). Finally, the leave-one-out analysis, which estimated the mean effect of individual IVs on the outcomes along with confidence intervals, revealed that no single IV significantly impacted the overall results (Supplementary Figure S1A , D, G, J). Overall, the absence of both heterogeneity and pleiotropy in this study’s analyses suggests that the selected SNPs as IVs exhibited consistent associations with exposure factors, thereby enhancing the accuracy and reliability of the MR results.Exposure Heterogeneity P MR-Egger regression MR-PRESSO outliner test Trait MR Egger Inverse variance weighted intercept SE Pval Pval Asbestosis Polyunsaturated fatty acids 0.412 0.325 0.061 0.034 0.073 0.254 Omega-3 fatty acids 0.221 0.252 0.002 0.026 0.945 0.438 Docosahexaenoic acid 0.722 0.59 −0.057 0.029 0.055 0.498 Ratio of omega-6 fatty acids to total fatty acids 0.419 0.419 0.035 0.035 0.329 0.33 Silicosis Monounsaturated fatty acids 0.185 0.210 0.009 0.040 0.819 0.195 Omega-3 fatty acids 0.202 0.200 0.039 0.039 0.318 0.364 Ratio of omega-3 fatty acids to total fatty acids 0.321 0.237 −0.071 0.040 0.089 0.376 Omega-6 fatty acids 0.366 0.389 −0.031 0.049 0.531 0.214 Polyunsaturated fatty acids 0.344 0.372 0.022 0.048 0.653 0.257 Note. MR, Mendelian randomization; SE, standard error; Pval, P−value. Table 1. Heterogeneity and sensitivity analysis of positive results
The findings of this study suggest that PUFAs, particularly omega-3 fatty acids, may serve as protective factors against asbestosis and silicosis. This observation prompts us to hypothesise that these fatty acids could play distinct roles in the progression of these diseases. Previous research supports the notion that targeting lung inflammation and fibrosis is crucial for preventing the onset and progression of pneumoconiosis.
Omega-3 PUFAs, which are an essential nutrient, have been extensively studied for their diverse health benefits, including reducing the risk of chronic respiratory conditions, mitigating inflammation, and ameliorating symptoms of autoimmune diseases. One study demonstrated that oral supplementation with omega-3 fatty acids reduced PM2.5-induced lung injuries in vivo, effectively alleviating lung parenchymal lesions, restoring normal levels of inflammatory cytokines, and decreasing oxidative stress markers[6]. Additionally, omega-3 PUFAs may attenuate PM2.5-induced lung injury in mice by remodelling the gut microbiota and modulating lung metabolism. Eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), key components of omega-3 PUFAs, are recognised for their potent antioxidant properties. Enriched fish oils containing EPA and DHA have demonstrated promising results in preventing lung inflammation and pulmonary fibrosis induced by bleomycin and nopaline in animal studies[7]. While current evidence supports the protective effects of omega-3 PUFAs, it is important to note that excessive intake may suppress essential inflammatory responses. Future research should investigate this dual effect, considering individual differences such as genetic susceptibility and underlying health conditions (
Supplementary Tables S8–S13 , available in www.besjournal.com).Additionally, the findings underscore the importance of giving special consideration to the beneficial role of DHA, a component of omega-3 PUFAs, in the prevention of pneumoconiosis. An experiment demonstrated that mice pretreated with DHA experienced significantly lower body weight loss and mortality following bleomycin injury, as well as a notable reduction in lung fibrosis. Furthermore, there is evidence indicating that DHA may attenuate the onset of cellular inflammation in bronchoalveolar lavage fluid (BALF) and lung tissues by reducing the pathways of IL-6, LTB4, and PGE2, while elevating IL-10[8]. Moreover, an experiment provided further evidence that DHA may protect against lung inflammation arising from chronic agricultural dust exposure through its derived lysophospholipids and endogenous cannabinoids. Significantly, it is worth noting that animals exposed to organic dust and treated with DHA exhibited considerable reductions in neutrophil infiltration and the production of pro-inflammatory cytokines and chemokines in the BALF[9]. Furthermore, a meta-analysis of data from population-based cohort studies indicated that elevated levels of DHA were associated with a reduced risk of hospitalization and mortality in patients with interstitial lung disease, as well as fewer abnormalities evident in lung computed tomography scans[10]. In conclusion, dietary DHA intake has the potential to serve as an effective early preventive measure for reducing lung injury in individuals exposed to dusty environments.
This study boasts several notable strengths. Firstly, it directly establishes a robust causal relationship between PUFAs and pneumoconiosis, utilising genetic variation as an IV through the TSMR method. Secondly, in contrast to conventional RCTs, our approach operates at the genetic level, thus offering advantages in terms of time and cost efficiency while maintaining scientific validity through random sample allocation. Lastly, we employed a variety of statistical techniques to mitigate the impact of heterogeneity and pleiotropy. Additionally, we utilised visualisation methods to enhance the presentation of our findings.
However, it is important to acknowledge several limitations of our study. Firstly, our research was confined to European populations; future efforts will encompass East Asian and African populations to broaden the generalizability of our findings. Secondly, although the three classifications of pneumoconiosis were considered in this study, the number of individuals with pneumoconiosis in the dataset was still small. Therefore, expanding the data sources is a critical focus area. Lastly, our study was primarily based on statistical outcomes; substantial foundational research and clinical validation are necessary to translate our findings into practical clinical application.
-
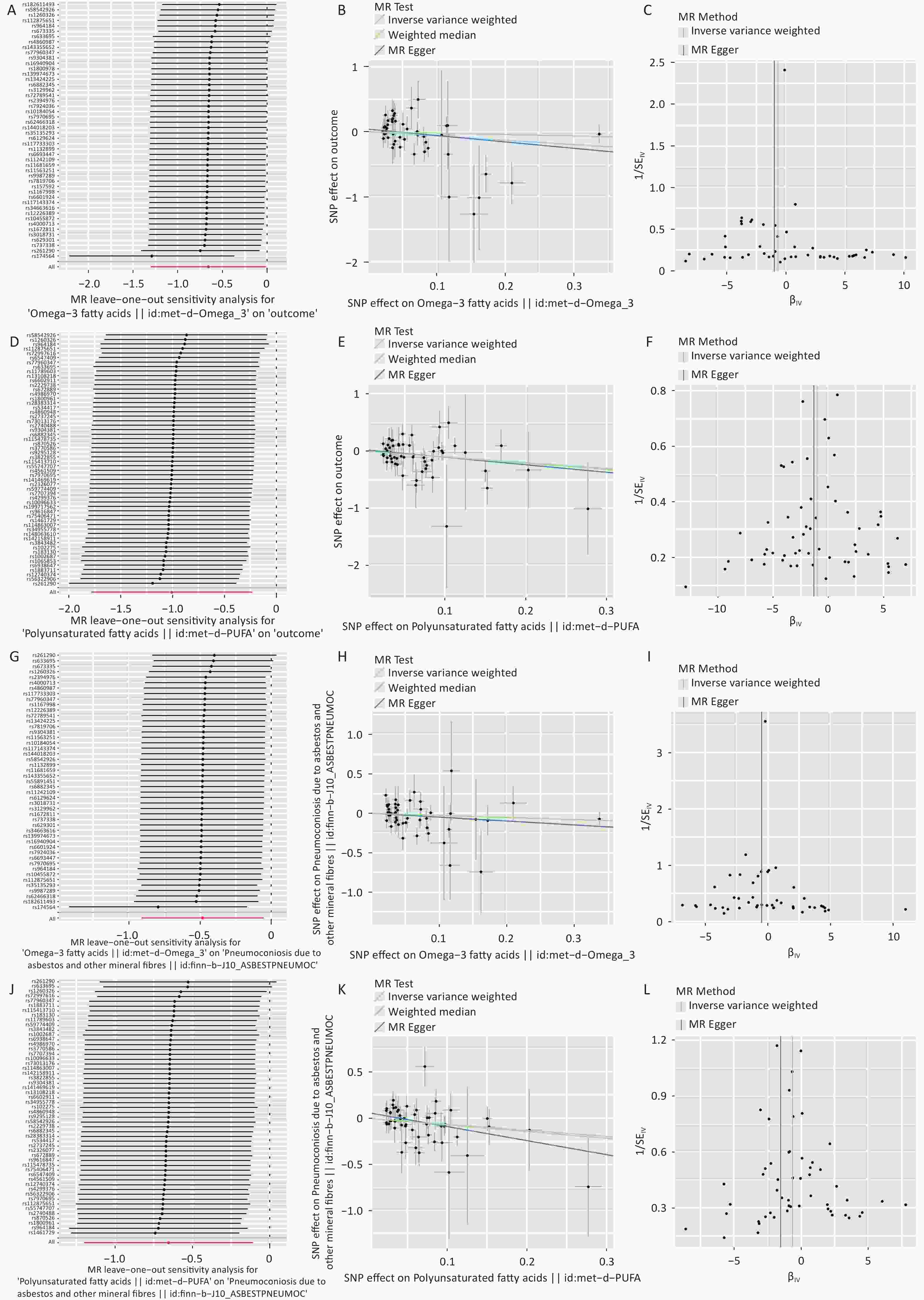
Figure S1. Scatter plot, funnel plot and LLO plot of polyunsaturated fatty acids, Omega-3 polyunsaturated fatty acids versus asbestosis and silicosis. SE, standard error; SNP, single nucleotide polymorphism.
HTML
 24072+Supplementary Materials.pdf
24072+Supplementary Materials.pdf
|

|

 Quick Links
Quick Links
 DownLoad:
DownLoad: