
-
Diabetes is the eighth leading cause of death worldwide, with 6.7 million deaths, and approximately 966 billion USD of diabetes-related expenditure in 2021[1,2]. China accounted for 1.4 million diabetes-related deaths in 2021 (the largest annual number), and 165.3 billion USD of diabetes-related expenditure (the second highest expenditure in the World)[3,4]. Type 2 diabetes mellitus (T2DM) is the dominant type of the disease, accounting for over 90% of all cases, and can be effectively managed by disease prevention and control measures[5].
The mortality of T2DM is linked to many factors, such as biological and behavioral factors, but its association with socioenvironmental factors are still unclear. Studies have indicated that high mortality tends to be associated with economic development, such as changes in food consumption patterns with increasing red meat consumption[6,7], air pollutants, and industrial expansion[8]. Long term exposure to ambient air pollutants, including ozone (O3) and particulate matter with particle size below 2.5 microns (PM2.5), increase the risk of T2DM. Environmental endocrine disruptors such as phthalates are linked to T2DM via inducing insulin resistance or gene-environment interactions[10-12]. Further evidence is required to verify the impact of socioenvironmental factors. China, as one of the emerging economies, has ever-changing disease patterns, including an increase in T2DM mortality, along with economic transition. Its T2DM mortality distribution in space and time should be studied to explore the associations with economic levels and assess the impact of different air pollutants.
Spatial analysis is used to visualize the geographic distribution patterns of diseases and identify their clustering, thereby helping to identify high-risk areas. Temporal analysis, however, highlights disease trends over time and assesses the potential impact of risk factors on diseases using time series models[13]. Previous studies have generally considered the association between diabetes and socioenvironmental factors from either a temporal or spatial perspective. For example, a spatial analysis in Indonesia showed a positive correlation between PM2.5 exposure and diabetes prevalence[14]. Other studies have focused solely on temporal aspects, such as a multi-regional time series study in South Korea, which examined the association between cold spells and diabetes mortality[15], and a study in Jiangsu Province, China, which evaluated the effect of temperature on diabetes deaths without considering the spatial effects between cities[16].
Globally, there has been growing recognition of the value of spatiotemporal analyses in chronic disease epidemiology. Advances in geographic information systems (GIS) and statistical modeling have enabled more detailed studies on the incidence and mortality of diabetes. For example, in a study in Denmark examining the link between long-term exposure to air pollutants and the incidence of diabetes in a cohort of nurses found a significant positive correlation between PM2.5 exposure and diabetes incidence (Relative Risk, [RR] = 1.11; 95% CI: 1.02−1.22), but no significant association with particulate matter with particle size below 10 microns (PM10), nitrogen dioxide (NO2), and NOx[17]. Similarly, a US study found that PM2.5 (Prevalence Ratio, [PR] = 1.10; 95% CI: 1.03−1.17) and O3 (PR = 1.06; 95% CI: 1.03−1.09) were associated with higher diabetes prevalence[18]. Recent research efforts in China have begun to incorporate socioeconomic and environmental disparities; however, comprehensive analyses of spatiotemporal clustering remain limited. In terms of the analysis of mortality and socioenvironmental factors of T2DM in China, a spatiotemporal analysis is essential to fully understand the complex patterns of diabetes deaths across areas and at different times. Currently, there are few studies on the spatiotemporal analyses of T2DM mortality. Ten years ago, a relevant national study on the spatiotemporal analysis of diabetes deaths in China used data from national disease surveillance points (DSPs), in which the overall risk of death from diabetes was assessed in seven zones instead of administrative provinces or municipals[19]. A recent provincial study conducted a spatiotemporal analysis of the association between T2DM deaths and socioenvironmental factors in elderly individuals in Shandong Province, China. The study found that temperature and relative humidity were significantly associated with T2DM deaths; however, it focused solely on elderly people living in temperate monsoon climates with distinct seasons[20]. As a result, there remains a significant gap in research that systematically examines the interplay between T2DM and socioenvironmental factors over time across the entire population, particularly in a subtropical monsoon climate characterized by abundant precipitation and high temperature. This is particularly important when considering spatiotemporal clustering analyses of China’s leading industrial and populous provinces.
China is a large country with diverse economic patterns, living habits, and food culture. To conduct the study in a more consistent social, economic, and cultural context, our study was conducted in Guangdong Province, China. Guangdong has been the largest economic province in China since 1989 with the most rapid development rate. Its total gross domestic product (GDP) ranks among the top ten in the world, surpassing Spain, Australia, and the Netherlands, and is equivalent to that of Canada and South Korea in 2022[21,22]. If GDP per capita is taken as an estimate of the gross national income per capita (GNI per capita) of the World Bank Analytical Classification[23], the GDP per capita values of Guangdong from 2014 to 2018 increased from upper-middle to high income as a whole. It is the most populous province in China since 2007 and had 126 million people according to the Seventh Population Census in 2020[24,25]. Similar to many emerging economies, Guangdong considers industry as its main driving force for economic development[26,27].
This study aimed to provide novel insights into diabetes mortality clustering in Guangdong Province. We estimated the mortality of T2DM in Guangdong using spatiotemporal clustering analysis, identified high-risk districts and counties, preliminarily explored their association with economic development and relevant air pollutants, and analyzed the contributing risk factors for further research. Spatiotemporal cluster analysis is crucial for understanding the dynamics of T2DM mortality. By identifying geographic hotspots and temporal peaks, this approach provides insight into targeted public health interventions. The integration of spatial and temporal dimensions allows a nuanced exploration of the influence of environmental and socioeconomic factors, which is essential for effective diabetes prevention and control strategies.
-
Guangdong, the industrial province that ranks first in China, has geographically uneven economic development, similar to that of China. Guangdong consists of four geographic zones covering 21 cities: The Pearl River Delta, East Guangdong, West Guangdong, and North Guangdong (Supplementary Figure S1), accounting for 79.52%, 6.71%, 7.65%, and 6.13% of the total provincial GDP, respectively[28].
We applied for and obtained the diabetes mortality data of 28 national DSPs in 18 cities extracted from the China Mortality Surveillance System by residence in Guangdong Province (Supplementary Figure S1). The national DSPs in the China Mortality Surveillance System were mainly determined by GDP per capita and population, which were divided into 54 layers over the whole country by the national health authority, and a representativeness evaluation was conducted[29].
The collected data included diabetes as the underlying cause of death from 2014 to 2018, including sex, age, place of residence, underlying cause of death, occupation, education, and place of death from the Guangdong Provincial Center for Disease Control and Prevention (Guangdong CDC), China. The underlying cause of death was classified using ICD-10 (International Classification of Diseases 10) codes and the national DSPs were representative, as proven in previous studies[29]. These data are death data covering the entire population in the administrative areas of the DSPs. The vector map was obtained from the Ministry of Natural Resources of the People’s Republic of China and covers 122 administrative districts/counties and two cities without districts/counties over the entire province. Population information and GDP per capita values integrated with administrative districts/counties were collected from the Health Commission of Guangdong Province and Guangdong Provincial Bureau of Statistics, China. Air pollutant data were obtained from the Ministry of Ecology and Environment of the People’s Republic of China using the National Urban Air Quality Real-time Publishing Platform (http://106.37.208.233:20035/), which included CO, O3, PM2.5, PM10, NO2 and sulphur dioxide (SO2) monitored by the national air pollutant surveillance stations.
-
The age-standardized mortality (ASMR) of T2DM was estimated using Empirical Bayesian Kriging using the data from the 28 national DSPs in Guangdong. The reference population for ASMR calculation was the cumulative number of registered populations of different ages from the 28 DSPs. We used the DSP populations from 2014 to 2018 to calculate the ASMR of T2DM for each corresponding year. The mapping of the estimated age-standardized mortality (EAM) for all counties/districts was performed using ESRI ArcGIS 10.8.
-
Based on the above EAM for 2014–2018, the geolocation (geometric center) and demographic data of Guangdong and Kulldorff’s space-time scan statistic[30] were used to test the distribution of T2DM deaths over space and time and identify high-risk spatiotemporal clusters. Within the study area, assuming that the deaths due to T2DM satisfied the Poisson distribution, a cylindrical window of different sizes was allowed at each location (the bottom of the cylinder corresponds to the geographical location, and the height corresponds to the time), and the size and position of the window were dynamically changed. For each change in the window, the log-likelihood ratio (LLR) calculates the ratio of the actual and expected cases inside and outside the window, and determines the maximum LLR value for all windows in all areas as possible spatiotemporal clusters. It then calculated the inside and outside RRs of the clusters, and statistical tests were performed to generate a simulated data set that uses Monte Carlo randomization to calculate the P-value. LLRs represent the degree of clustering.
Our study period was from January 1, 2014, to December 31, 2018, and the geographical overlap was set to "none". The maximum spatial cluster size was set to 10% of the population at risk, and the maximum temporal cluster size was one year. The number of Monte Carlo simulations was 999. When the hypothesis test of LLR had a P-value < 0.05, counties/districts were considered clustered. ESRI ArcGIS 10.8 was used to map all clusters from 2014 to 2018 over Guangdong Province.
To understand sex differences, we conducted the above spatiotemporal cluster analysis separately for males and females.
-
Based on the results of the spatiotemporal cluster analysis, we assessed the relationship between GDP per capita values and RRs in Guangdong from 2014 to 2018. The GDP per capita was used to estimate the GNI per capita that is used by the World Bank Analytical Classification for low, lower middle, upper middle, and high income, as GDP was similar to GNI, but did not include income from employees overseas or property that adds to the national total income production[23]. Curvilinear regression analysis was conducted using IBM SPSS Statistics version 21.0, including a group of analyses of Linear, Logarithmic, Inverse, Quadratic, Cubic, Power, Compound, S-curve, Logistic, Growth and Exponential Regressions.
-
To further understand and explore the association between air pollutants and mortality of T2DM, which might be influenced by economic and industrial development, weekly data of air pollutants and T2DM deaths was analyzed using the Spearman Correlation and the Poisson Log-linear Model for the pilot assessments on the districts/counties with the highest, second highest, and high mortality of T2DM. Analyses were conducted using IBM SPSS Statistics version 21.0.
-
A total of 13,919 patients died of diabetes at 28 DSPs in Guangdong Province, China, between 2014 and 2018. Among these, 1,383 with type 1 diabetes mellitus (T1DM), three with neonatal diabetes mellitus, and two with gestational diabetes mellitus were excluded. Ultimately, 12,531 T2DM cases were selected for the current analysis, with a slowly increasing trend in age-standardized mortality from approximately 10.28/100,000 to 12.17/100,000 ( Supplementary Figures S2 and S3). A total of 12,409 (99.03%) cases were reported in persons aged > 40 years old. The number of cases in working age patients (those under 60 years old) were 1,956 (15.61%). Grouping by age in 5-year intervals (≥ 30 years) showed that ≥ 85 years group (17.15%) had the highest mortality (170.78/100,000, χ2 = 85696.587, P < 0.01) and the mortality showed an increasing trend with age (Linear-by-Linear Association value = 50,775.38, P < 0.01). The number of male patients (6,419, 51.22%) was slightly higher than the reported number of female patients (6,112, 48.78%), and the mortality in males and females showed no significant difference (See Supplementary Figure S2). Moreover, regarding educational background, junior high school or below accounted for the vast majority of deaths (89.17%). The highest represented occupations were farmers, retired personnel, and the unemployed (47.90%, 22.28%, and 13.59%, respectively). Furthermore, 65.23% of the patients died at home and 31.34% died in hospitals. The details are provided in Supplementary Table S1.
-
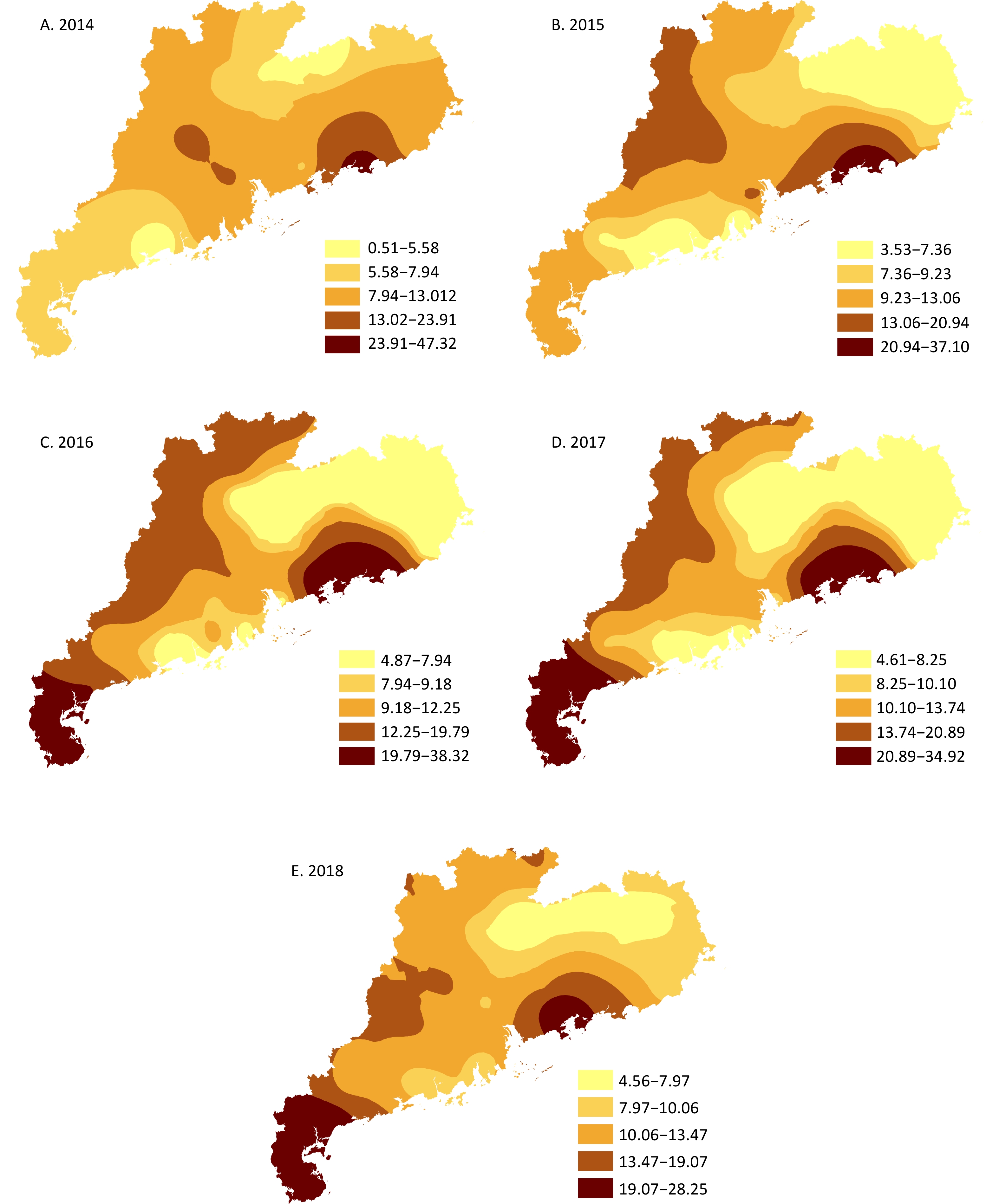
The mortality distribution of districts/counties over Guangdong Province was estimated based on the age-standardized mortality of T2DM in 28 DSPs from 2014 to 2018: A high mortality coastal area on East Guangdong had been formed since 2014. By 2016, the coasts of East and West Guangdong were the main areas with high mortality, which gradually decreased to the surrounding areas. Finally, in 2017 and 2018, the overall pattern continued, but with a slow decrease in mortality (Figure 1). In 2014, the EAM ranged from 0.51 to 47.32, including a coastal district in East Guangdong located in the highest EAM area (23.91 to 47.32). In 2015, the EAM ranged from 3.53 to 37.10, including a coastal district and part of a neighboring county of the same city in East Guangdong located in the highest EAM area (20.54 to 37.10). In 2016, the EAM ranged from 4.87 to 38.32, including one coastal district and two coastal counties of the same city in East Guangdong, and three districts of two cities in the Pearl River Delta located in the highest EAM area (19.79 to 38.32). In 2017, the EAM ranged from 4.61 to 34.92, including one coastal district and two coastal counties of the same city in East Guangdong, three districts of two cities in the Pearl River Delta, a coastal city (including four districts and seven counties), and parts of one county and one district of a neighboring city in West Guangdong located in the highest EAM area (20.89 to 34.92). In 2018, the EAM ranged from 4.56 to 28.25, including three districts of two cities in the Pearl River Delta, a coastal city (including four districts and seven counties), and part of one county of a neighboring city in West Guangdong located in the highest EAM area (19.07 to 28.25).
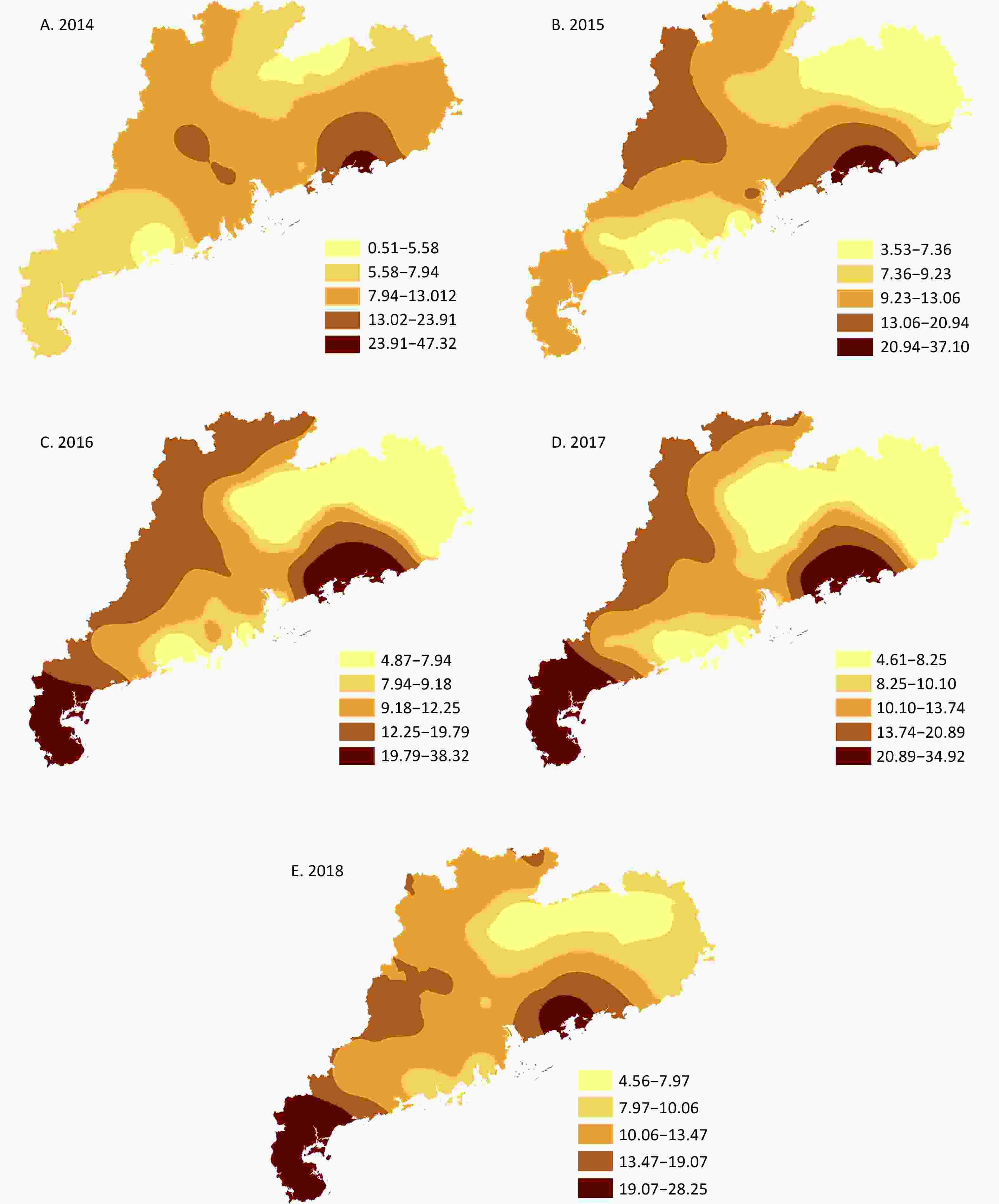
Figure 1. The spatial distribution of EAM (estimated age-standardized mortality) on T2DM (type 2 diabetes mellitus) over Guangdong Province, China from 2014 to 2018. GS(2020)4619.
-
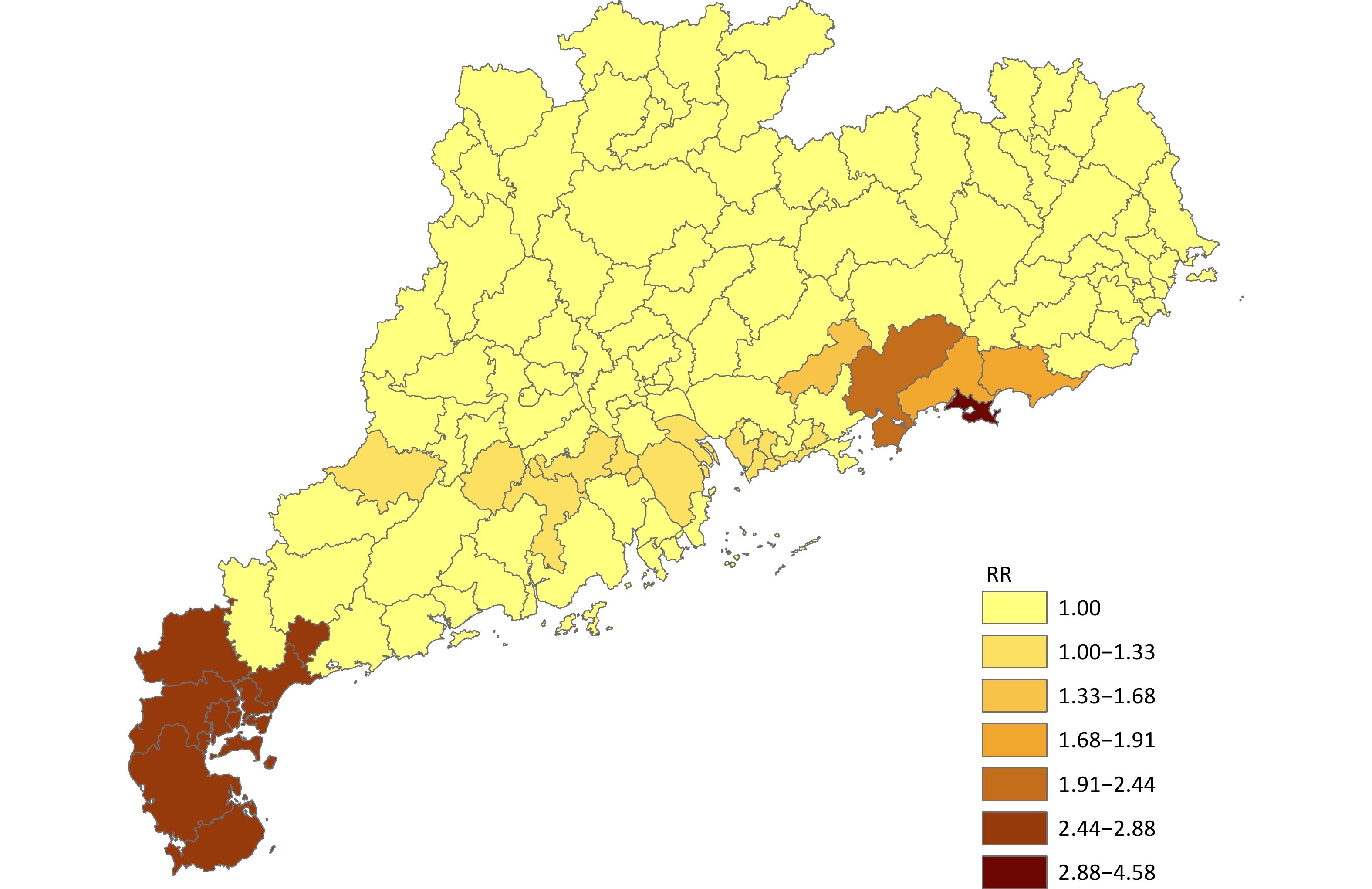
Spatiotemporal clustering analysis revealed six clusters in Guangdong from 2014 to 2018. The high-risk clusters were generally concentrated in the coastal areas of East and West Guangdong, and the cluster with the highest risk was a coastal district of East Guangdong (RR = 4.58, Log Likelihood Ratio, [LRR] = 191.45, P < 0.01), followed by 10 coastal districts/counties of West Guangdong (RR = 2.88, LRR = 1,131.70, P < 0.01); the third was a coastal county of the Pearl River Delta (RR = 2.24, LRR = 56.02, P < 0.01), followed by two coastal counties of East Guangdong (RR = 1.91, LRR = 100.86, P < 0.01), a coastal district of the Pearl River Delta (RR = 1.68, LRR = 20.39, P < 0.01), 13 districts/counties of the Pearl River Delta and two counties of North Guangdong (RR = 1.33, LRR = 53.40, P < 0.01) (Table 1 and Figure 2).
Cluster District/ County City Time Frame Cases Expected cases *LLR P value RR 1 Chengqu Shanwei 2014/1/1 to 2014/12/31 259 56.72 191.45 < 0.01 4.58 2 Chikan Zhanjiang 2017/1/1 to 2017/12/31 2879 1,037.12 1131.70 < 0.01 2.88 Xiashan Potou Mazhang Suixi Xuwen Lianjiang Leizhou Wuchuan Maonan Maoming 3 Huidong Huizhou 2017/1/1 to 2017/12/31 223 99.98 56.02 < 0.01 2.24 4 Haifeng Shanwei 2016/1/1 to 2016/12/31 593 311.70 100.86 < 0.01 1.91 Lufeng 5 Huicheng Huizhou 2017/1/1 to 2017/12/31 179 106.66 20.39 < 0.01 1.68 6 Nansha Guangzhou 2018/1/1 to 2018/12/31 1451 1,095.95 53.40 < 0.01 1.33 Luohu Shenzhen Futian Nanshan Baoan Yantian Pingshan Longhua Dapeng Pengjiang Jiangmen Jianghai Kaiping Heshan Daya Bay Huizhou Zhongshan Zhongshan Luoding Yunfu Xinxing Note. *LLR refers to Log Likelihood Ratio. Table 1. The Spatiotemporal Clusters of T2DM (type 2 diabetes mellitus) Mortality and Related RRs (relative risks) in Guangdong Province, China from 2014 to 2018
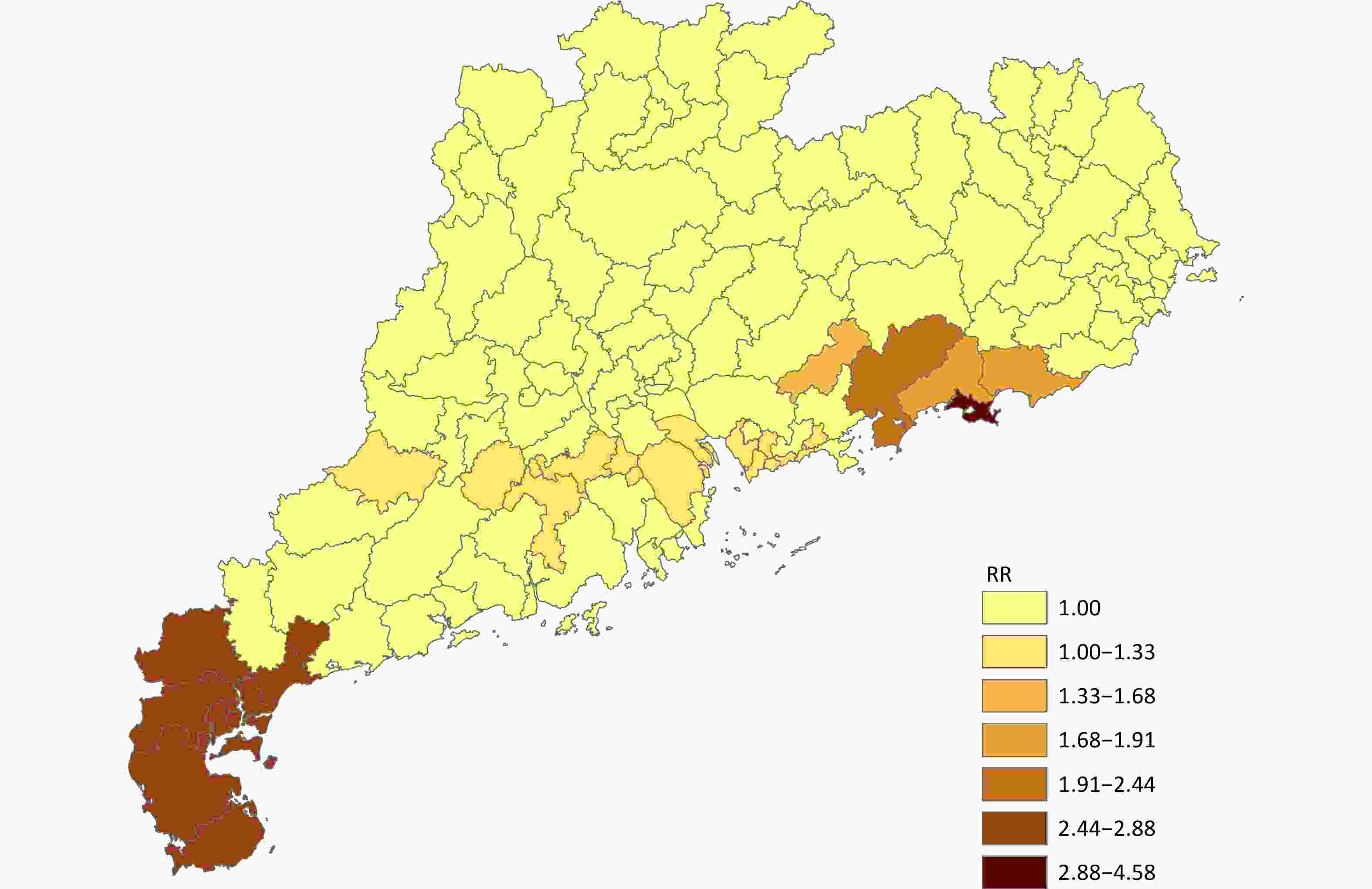
Figure 2. The map of RRs (relative risks) of T2DM (type 2 diabetes mellitus) mortality in Guangdong Province, China from 2014 to 2018. GS(2020)4619.
The geographic distribution of T2DM mortality in males and females showed similar trends to the overall analysis. The difference was that the RRs of females among the high-risk clusters were narrower in the range (1.67 ≤ RR ≤ 2.55, P < 0.01) than that of males (1.25 ≤ RR ≤ 4.29, P < 0.01). The specific manifestation was that, except for the district (male RR = 4.29, female RR = 1.67) and two counties (male RR = 1.76, female RR = 1.27) in East Guangdong, females were at higher risk than counterpart males in related high-risk districts and counties in West Guangdong and the Pearl River Delta (Supplementary Figures S4 - S7 and Supplementary Tables S2 - S3).
-
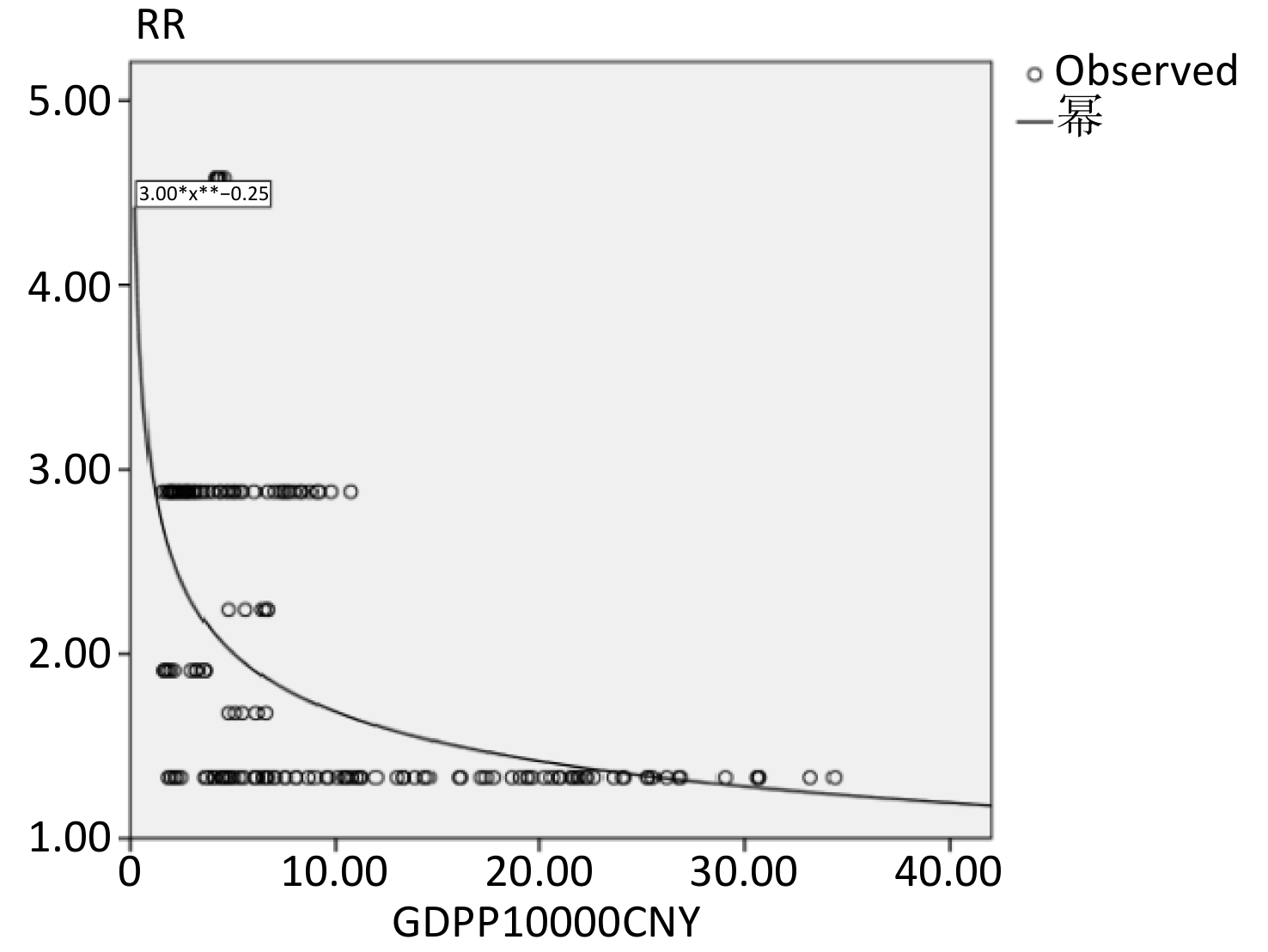
According to the results of the spatiotemporal clustering analysis, there were in total 30 counties/districts (RRs between 1.33 to 4.58) of 8 coastal cities belonging to East Guangdong (Shanwei), West Guangdong (Zhanjiang, Maoming), the Pearl River Delta (Guangzhou, Shenzhen, Zhongshan, Huizhou, Jiangmen) within the above six clusters, which were highlighting the coastal areas. We conducted a curvilinear regression to analyze the relationship between GDP per capita values and RRs in the 30 counties/districts from 2014 to 2018. The GDP per capita values (CNY 15,261.09, CNY 343,936.00) were approximately equal to USD 2,389.89 to USD 53,860.38. The results demonstrated that 11 regression models (linear, logarithmic, inverse, quadratic, cubic, power, compound, s-curve, logistic, growth, and exponential) fit this association significantly.
The performance of the above 11 models included an ANOVA (F value) between 19.86 and 67.19, and all P values were < 0.01. Therefore, we considered that the Power Regression fit the relationship better:
y = 3.00x −0.25 (F = 67.19, P < 0.01) (See Figure 3).
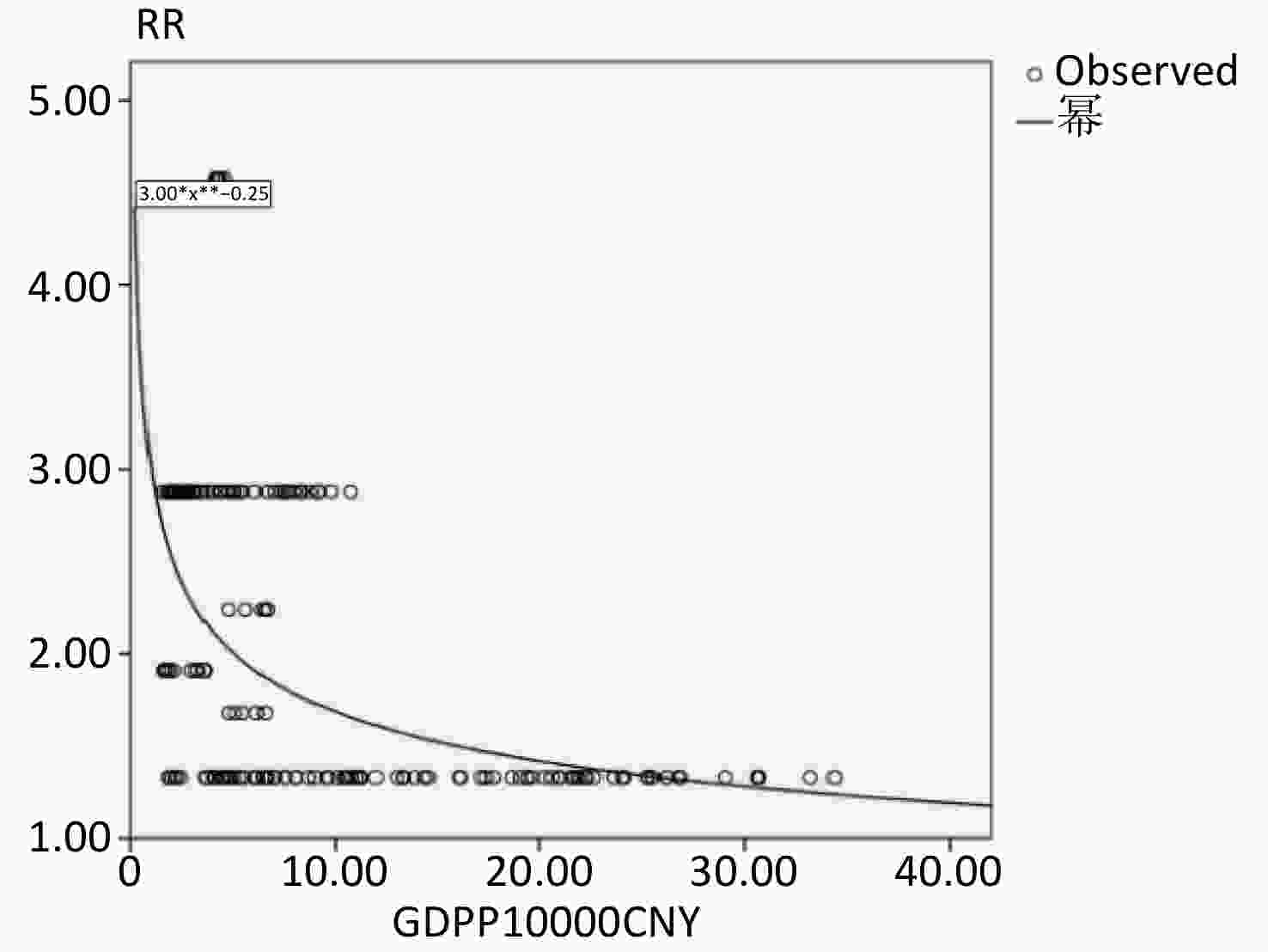
Figure 3. The Power Regression Fitting the Relationship between gross domestic product per capita values (GDP per capita values) and relative risks (RRs) in 30 Counties/Districts in Guangdong Province, China from 2014 to 2018.
According to the Power Regression, those counties/districts that were progressing from lower-middle income (GNI per capita values between USD 996 and USD 4,125 ) to upper-middle income (GNI per capita values between USD 3,896 and USD 12,735) according to the World Bank Analytical Classifications criteria from 2014 to 2018[32] had higher RRs for T2DM mortality.
-
The Spearman Correlations between air pollutants and deaths from T2DM based on weekly data from the district (RR = 4.58) with the highest mortality in East Guangdong and the district (RR = 1.33) with high mortality in the Pearl River Delta of Guangdong showed no significant correlations between air pollutants and deaths from T2DM. When it came to the county (RR = 2.88) with the second highest mortality in West Guangdong, the correlation analyses demonstrated that only CO ( r = −0.49, 95% CI: −0.67 to −0.29, P < 0.05) had a significant correlation with mortality. The correlations between CO, PM2.5, O3, PM10, NO2 and SO2 showed r values < 0.70 in the correlation analyses of the two districts and one county, respectively.
According to the correlation analyses and relevant literature[33-35], the final multivariate models included CO, O3, and PM2.5 for the two districts and one county, respectively. Results of the final model in the district with the highest mortality were as followings: The relative risk of deaths due to T2DM increased by 158.6% for every 1 mg/m3 of CO (IRR = 2.59, 95% CI: 1.31 to 3.87, P < 0.05) concentration in the air; O3 and PM2.5 were not significantly associated with the mortality risk of T2DM (
Supplementary Tables S4 - S5 ). While the RR of death in the final models in the county with the second highest mortality and the district with high mortality decreased along with the CO concentration in the air (IRR = −0.98, 95% CI: −1.24 to −0.72, P < 0.05 and IRR = −1.69, 95% CI: −1.15 to −0.28, P < 0.05, respectively). O3 and PM2.5 were not significantly associated with the mortality risk of T2DM (Supplementary Tables S6–S9). -
This study was conducted in Guangdong Province in South China, the leading industrial and populous province with uneven economic development like China, as an example for all age groups of county-level analysis, and found that the main areas with high mortality of T2DM were in the coastal areas of East and West Guangdong, especially those with economies progressing towards the upper-middle income level. CO was significantly associated with T2DM mortality in the pilot exploration.
This was the first study on the spatiotemporal clustering of T2DM mortality for all age groups in South China at the county level[19] and was a follow-up study to that conducted by Zhou et al. (2015) concluded that diabetes mortality was higher in Northwest and Northeast China than in South China, and was higher in urbanized areas than in rural areas, based on data from 161 national DSPs of 31 provinces across the country from 2006 to 2012[19]. In patients with T2DM, the risk of death is mostly due to poor blood glucose control and life-threatening complications[36]. T2DM management includes priorities such as a healthy diet, regular physical exercise, maintaining a healthy weight, and prescribing oral hypoglycemic drugs and insulin, if necessary, to control blood glucose levels. In this study, the clusters with the highest risk were located on the coasts of East and West Guangdong, in which the economy was developing towards upper-middle income, but not in the developed districts and counties. Possible reasons for this are as follows.
First, although the economy is developing, the comparative lack of medical and healthcare resources has led to an increased risk of mortality from T2DM. The International Diabetes Federation (IDF) found that low and middle income countries, especially those developing from low to middle income ones, had the highest diabetes mortality[2,3,37]. Meanwhile, the lack of timely medical and healthcare treatment for complications[38,39] due to poverty could also increase the risk of T2DM deaths. Among the death cases in this study, in terms of the location of death, more than 60% (65.23%) of the deaths occurred at home. Meanwhile, although the economy was developing in high-risk counties/districts in this study, T2DM is a costly disease owing to its chronic nature[40,41]. Previous literature[42-45] demonstrated that the average annual expenditure for T2DM in low- and middle-income countries ranged from USD 29.91 to USD 237.38, including direct and indirect costs; in China, the average annual expenditure for diabetes patients in rural areas reached CNY 6,450 (approximately USD 998.46), and that in cities was CNY 15,652 (approximately USD 2,442.93), accounting for approximately 46% of per capita disposable income in 2016. In contrast to the IDF, the high-risk counties/districts in this study, especially those ranking among the top three, were developing from lower-middle income towards upper-middle income in the emerging economy according to the World Bank Analytical Classification criteria from 2014 to 2018[32]. Therefore, the above expenses would still lead to a heavy economic burden for a lifetime once the disease is diagnosed, which would probably hamper people from continuing medical treatment and going to hospitals.
Second, the pilot exploration in the two districts and the county with the highest, second-highest, and high mortality rates found that CO was significantly associated with T2DM deaths. This result is consistent with a few previous studies in which CO exposure was significantly associated with gestational diabetes mellitus (GDM) and increased GDM severity in a cohort living in Northeast China[46-49]. A retrospective population-based cohort study[50] showed that CO poisoning made people more susceptible to diabetes due to the possible disruption of the endocrine system caused by hypoxic injury, with impacts on oxidative stress and endothelial dysfunction[51-54]. As an air pollutant, CO has not received much attention when analyzing the association between pollution and diabetes outcomes compared to PM2.5, PM10, NO2, SO2 and O3. For example, a systematic review by Li et al. (2014) found that air pollution was associated with diabetes-related mortality, with only 2 out of 12 studies including CO as a pollutant[8]. Another example is the study conducted by Wu et al. (2021), who also explored the relationship between air pollutants and diabetes-related mortality, but without CO[48]. However, CO emissions have been increasing with the rapid development of the economy, such as the construction of civil airports, coal-fired power plants, and car emission[55-57]. More attention is worth paying to verifying the association between CO and T2DM mortality[8,46,58-60].
Third, insufficient self-care awareness regarding the risk of death caused by T2DM leads to an increased risk of death. Owing to the complex interactions between the environment, lifestyle, and clinical and genetic factors, self-management of diabetes is multidimensional. Education and self-care awareness has greatly influenced clinical progress and results. The patients who died in this study were not well educated, and most completed junior high school or lower level of education (89.17%). Farmers and the unemployed accounted for the majority of occupations (47.90% and 13.59%, respectively). The awareness of self-care for diseases is generally weak among the above groups of people[61]. Even for patients with T2DM who took oral medications and diet, and engaged in exercise, the monthly self-blood glucose monitoring was less than once, and the rate of blood glucometer ownership in high-income areas (GNI per capita > USD 12,735) was less than 18% in Guangdong[62]. Meanwhile, they were reluctant to take the initiative to seek medical treatment, and only 31.34% of the deaths in this study occurred in medical institutions. It was also shown that even for people who often need to visit medical institutions for treatment, awareness of diabetes self-care still needed to be improved through health education, and their needs were still strong for designated professionals from hospitals to follow up and guide the self-monitoring and management of diabetes outside the hospital[63-65]. Thus Patient-Centered Collaborative Care is an actual need and future trend that should be supported by a combination of policy, system, and patient[66,67].
Finally, the management of diabetes was strengthened at the national and provincial levels from 2014 to 2018, which was a potential reason for the spatial distribution to show a slow decrease in T2DM mortality in 2017 and 2018. At the national level, the number of patients with diabetes managed nationwide reached 25 million by the end of 2014, gradually forming a comprehensive and continuous standardized management system for diabetes in China[68]. In 2015, the General Office of the State Council of the People’s Republic of China issued guidelines on promoting the construction of a graded diagnosis and treatment system[69], considering diabetes as one of the breakthrough diseases in the graded diagnosis and treatment of chronic diseases, and carrying out pilot projects nationwide. Through graded diagnosis and treatment, patients can enjoy higher levels of medical services at the local level. In combination with basic public health service projects, Guangdong Province, China, has focused on promoting the management of patients with chronic diseases, including diabetes. According to the national guidelines for the prevention and management of diabetes at local levels (2018)[70], basic medical and health institutions in Guangdong Province were equipped with corresponding testing equipment and essential drugs to provide comprehensive, continuous, and responsible medical and health management services for patients with diabetes, and established a cooperation mechanism with superior hospitals to achieve two-way referral.
Based on the above discussion, it will be necessary to investigate the proportion of healthcare institutions compared to the population they serve in high-risk districts/counties and provide feasible suggestions on improving the healthcare services for T2DM in future studies if there is still a need for primary healthcare after the strengthening of diabetes management at local levels. Second, the focus on CO in this study was determined by the availability and reliability of CO data during the study period alongside preliminary findings that indicated a stronger association between CO exposure and T2DM mortality than with other pollutants. CO may contribute to T2DM mortality through its effects on oxidative stress and endothelial dysfunction, as suggested in the existing literature. Future research should prioritize multi-pollutant models to comprehensively evaluate the combined effects of CO, NO₂, SO₂, and other socioenvironmental factors on T2DM mortality outcomes. Moreover, effect modifiers such as area economic development levels and air pollution variations were explored through stratified analyses to identify differential impacts across geographic areas. Future studies could enhance these analyses by incorporating additional behavioral and healthcare-related factors to assess potential confounders and effect modifiers more comprehensively.
The strengths include that the study provides a detailed analysis of the districts/counties level T2DM mortality data in a more consistent social, economic, and cultural context, as it was conducted within the most populous economic province with high GDP data that surpassed that of many developed countries in the world and was progressing towards a high income level during the study period. Second, unlike most previous studies, the analyzed data only included T2DM, which could be effectively improved by disease prevention and control interventions. T1DM and other types of diabetes mellitus were excluded. Third, through geographic and spatial maps, the estimated situation of the province's mortality due to T2DM and the distribution of high-risk clusters can be visually displayed, which is convenient for further exploration and analysis and the adoption of targeted intervention measures.
However, this study also has its limitations. There are many factors that affect the development of T2DM, the most influential one being the lifestyle related to urbanization, but limited by data sources, behavioral risk factors for deaths from T2DM, such as smoking, drinking, sedentary lifestyle, diet, metabolic risk factors (such as overweight/obesity, high blood pressure, and cholesterol levels), and the prevalence of T2DM were not available in the death surveillance data, and thus were not able to be evaluated. Moreover, limited by data availability, the study period covered 5 years only, which is comparatively short, and further studies are necessary in the future. Therefore, future research should focus on collecting data on the risk factors for behavior and metabolism based on the collection of mortality surveillance data for an in-depth evaluation, combined with expanded socioenvironmental factors for a longer period. Moreover, future research should consider employing a robust Bayesian spatiotemporal model, rather than relying solely on traditional spatiotemporal clustering analysis, to assess the relationship between T2DM mortality and socioenvironmental factors. Bayesian models offer a more flexible and statistically rigorous framework that can better account for uncertainties in both the spatial and temporal data dimensions. By integrating prior knowledge and providing probabilistic estimates, these models can enhance the accuracy and reliability of the analysis, offering a deeper understanding of the complex interactions between environmental factors and disease outcomes over time and across different regions. This approach is particularly valuable for identifying subtle trends and providing nuanced insights into the spatial and temporal dynamics of T2DM mortality.
-
The coastal areas in East and West Guangdong have a higher risk of mortality from T2DM and a gradually decreasing geographic distribution trend into the surrounding areas. In high-risk areas, coastal districts/counties in which the economy was progressing from lower-middle to upper-middle income levels, had a higher risk. Pilot assessments have indicated that air pollutants, specifically CO, was significantly associated with T2DM mortality. This study provides the first step in conducting research on the socioeconomic factors related to T2DM mortality in South China.
Identifying High-Risk Areas for Type 2 Diabetes Mellitus Mortality in Guangdong, China: Spatiotemporal Clustering and Socioenvironmental Determinants
doi: 10.3967/bes2025.048
- Received Date: 2024-10-07
- Accepted Date: 2025-02-27
-
Key words:
- Mortality /
- Type 2 diabetes mellitus /
- Spatiotemporal clustering /
- Economy /
- Air pollutants
Abstract:
The authors declare no competing interests relevant to this article.
All the data used in this study were aggregated data with no identifiable individual information, which were processed by designated professionals from the Guangdong CDC before being authorized for use in the study. Ethical approval for this study was obtained from the Medical Research Ethics Review Committee of the Guangdong Provincial Center for Disease Control and Prevention, China (No. W96-027E-202307).
| Citation: | Haiming Luo, Wenbiao Hu, Yanjun Xu, Xueyan Zheng, Qun He, Lu Lv, Ruilin Meng, Xiaojun Xu, Fei Zou. Identifying High-Risk Areas for Type 2 Diabetes Mellitus Mortality in Guangdong, China: Spatiotemporal Clustering and Socioenvironmental Determinants[J]. Biomedical and Environmental Sciences. doi: 10.3967/bes2025.048

|

 Quick Links
Quick Links
 DownLoad:
DownLoad: