

 下载:
下载:


-
Dental caries is a highly prevalent, chronic childhood disease[1]. Childhood dental caries contributes to oral health problems such as toothache, dental tissue defects, tooth loss, permanent tooth malformation, and malocclusion[2]. The World Health Organization has emphasized that dental caries has already affected 60%-90% of schoolchildren in most developed countries[1]. Childhood caries is also prevalent among young children in China[3]. The 4th National Oral Health Survey in 2016 reported that 70.9% of 5-year-old children and 34.5% of 12-year-old had experienced caries[4, 5]. Childhood dental caries has aroused worldwide concern and is regarded as an important public health issue. Understanding the basic epidemiology and disease burden of childhood dental caries is a prerequisite of children's caries control and prevention.
The latest national oral health surveys provided a nationwide scope of the oral health situation among the Chinese population, but it failed to provide data at the microscale level, which might be more useful in tailoring public health strategy. In addition, only a small number of studies at regional or district levels reported the prevalence, distribution, and temporal trend of childhood dental caries[6]. These sparse studies can hardly provide reliable knowledge without data integration under standard methodology. The Global Burden of Disease, Injuries, and Risk Factors Study 2016 (GBD 2016) provided information on disease prevalence and severity by age, gender, geography, and time. It used all available data of sufficient quality to generate reliable estimates of prevalence and years lived with disability (YLD) for oral conditions spanning the period 1990 to 2016. By using GBD 2016 results, this study assessed and analyzed the up-to-date disease burden of childhood dental caries in China, as well as its temporal trend since 1990.
Data on prevalence of dental caries for China in GBD 2016 were mainly from the systematic literature review led by Marcenes in 2013[7] and an updated version conducted by Kassebaum et al.[8]. Both reviews used the same case definitions and inclusion/exclusion criteria. The case definition for dental caries in the deciduous dentition is 'teeth with unmistakable coronal cavity at dentin level.' This definition corresponds to an ICD-9 code of 521.0 and an ICD-10 code of K02.3-K02.9. The case definition for dental caries in the permanent dentition is 'teeth with unmistakable coronal cavity at dentin level or root cavity in cementum that feel soft or leathery to probing.' This definition corresponds to an ICD-9 code of 521.0 and an ICD-10 code of K02.3-K02.9. The search strategy in the reviews was elaborated in a previous publication[9]. A full set of input sources for dental caries is available on the Global Health Data Exchange[10]. All data were de-identified. As this was a secondary data analysis, our research was Institutional Review Board -exempted.
Basically, GBD 2016 aimed to quantify population health losses from a wide array of fatal and nonfatal diseases, injuries, and risk factors[9]. These losses were expressed in the metric of disability-adjusted life-years, which was defined as the sum of years of life lost due to mortality and YLD[9]. Since death directly attributed to oral disease is rare, in the current study we used only YLD to estimate the disease burden of childhood dental caries aged 0 to 14 years in China[7]. Prevalence estimates for dental caries were assessed by using the database for all age-gender-province-year groups, and the Bayesian meta-regression method was applied to estimate the nonfatal health outcomes including prevalence estimates and uncertainty distribution[9] between 1990 and 2016. YLD was calculated as the prevalence of dental caries times the disability weight of the corresponding sequelae[7]. The disability weights used in GBD 2016 were the same as those used in GBD 2013. The disability weights was generated by using collected data based on household surveys and open-access, Web-based surveys in nine countries, including Bangladesh, Indonesia, Peru, Tanzania, USA, Hungary, Italy, the Netherlands, and Sweden. All the participants in the survey were ≥ 18 years[7]. This approach provided quantitative estimates of health losses associated with nonfatal outcomes. The GBD 2016 also reported 95% uncertainty intervals (UI) for each estimated quantity. The uncertainty from all data inputs into the calculations of YLD were propagated through Monte Carlo simulation techniques by taking 1, 000 draws for each age, gender, province, year, and cause[11]. The 95% UI for each quantity were determined by taking 1, 000 samples from the posterior distribution of prevalence and 1, 000 samples of the YLD distribution[9, 11].
The number of cases, prevalence, YLD, and age-standardized YLD rate were used as indicators to estimate dental caries burden among Chinese children aged 0 to 14 years. The disease burden in 2016 was analyzed and compared by different gender, age groups (under 5 and 5-14 years), and causes [deciduous caries (DC) and permanent caries (PC)]. Arc Info GIS software V10.3 (Environmental Systems Research Institute, Redlands, CA, USA) was used to develop a choropleth map to demonstrate the spatial pattern of childhood dental caries burden throughout China at the provincial level in 2016. Provincial units include 31 provinces (autonomous regions and direct-controlled municipalities, Hong Kong, and Macao Special Administrative Region of China). We also analyzed the temporal trend in those disease-burden indexes from 1990 to 2016. Age standardization was performed in the spatial and temporal analysis, with the estimated China population by age for 2010 to 2035 from the World Population Prospects 2012[12] as the standard population. Data management and analysis were performed in SAS 9.4 (SAS Institute Inc, Cary, NC, USA).
In 2016, > 93.0 million children aged 0 to 14 years suffered from dental caries. As Table 1 shows, in 2016 the number of cases, prevalence, YLD, and age-standardized YLD rate caused by dental caries were 93.0 million, 43.0%, 32, 200 person-years, and 14.8 per 100, 000, respectively. Girls aged 0-14 years with dental caries (prevalence: 44.1%; YLD rate: 15.6 per 100, 000) showed a comparatively higher disease burden than did boys (prevalence: 41.9%; YLD rate: 14.2 per 100, 000). For children under 5 with DC, (prevalence: 39.8%, YLD rate: 9.4 per 100, 000) the prevalence and YLD rate were nearly 1.5 times that of children 5 to 14 (prevalence: 26.2%, YLD rate: 6.2 per 100, 000). For children 5 to 14 years with PC only, the prevalence and YLD rate were 18.0% and 10.8 per 100, 000, respectively. Compared with boys, girls appeared to have an equivalent DC burden at ages 0 to 14 years, and a higher PC burden at 5 to 14 years.
Table 1. Number of Cases, Prevalence, YLD, and Age-standardized YLD Rate of Dental Caries among Chinese Children Aged 0-14 Years, 2016
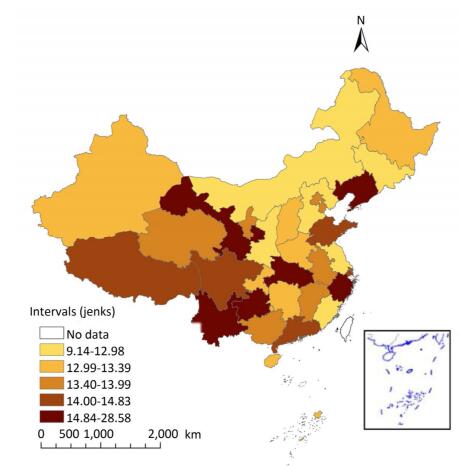
Characteristic Sex Deciduous Caries (DC) Permanent Caries (PC) Dental Caries Under 5 (95% UI) 5-14 (95% UI) 5-14 (95% UI) 0-14 (95% UI) Number of cases (million) Male 13.2 (10.5, 16.0) 21.9 (17.0, 28.0) 13.7 (10.4, 17.4) 48.8 (37.8, 61.4) Female 10.9 (8.6, 13.2) 19.0 (14.9, 24.1) 14.3 (11.0, 18.0) 44.2 (34.5, 55.3) Total 24.1 (19.1, 29.1) 40.9 (31.8, 52.1) 28.0 (21.4, 35.3) 93.0 (72.2, 116.5) Prevalence (%) Male 40.7 (32.2, 49.2) 26.1 (20.3, 33.4) 16.3 (12.4, 20.8) 41.9 (32.5, 52.8) Female 38.7 (30.6, 47.0) 26.4 (20.6, 33.4) 19.9 (15.3, 25.0) 44.1 (34.4, 55.2) Total 39.8 (31.5, 48.0) 26.2 (20.4, 33.4) 18.0 (13.7, 22.6) 43.0 (33.4, 53.8) YLD (10, 000 person years) Male 0.3 (0.1, 0.6) 0.5 (0.2, 1.1) 0.8 (0.4, 1.7) 1.7 (0.7, 3.4) Female 0.3 (0.1, 0.5) 0.5 (0.2, 0.9) 0.9 (0.4, 1.7) 1.6 (0.7, 3.2) Total 0.6 (0.2, 1.1) 1.0 (0.4, 2.0) 1.7 (0.7, 3.4) 3.2 (1.4, 6.6) Age-standardized YLD rate (per 100, 000) Male 9.6 (4.0, 18.9) 6.2 (2.6, 12.6) 9.8 (4.2, 20.2) 14.2 (6.0, 28.9) Female 9.2 (3.8, 18.1) 6.2 (2.6, 12.8) 11.9 (5.1, 24.2) 15.6 (6.6, 31.7) Total 9.4 (3.9, 18.5) 6.2 (2.6, 12.8) 10.8 (4.6, 22.1) 14.8 (6.3, 30.3) Note. 95% UI represents 95% Uncertainty Intervals. No clustering was seen among 33 provincial units for age-standardized YLD rate of dental caries, but notable provincial variations were observed in 2016 (Figure 1). Hubei (28.6 per 100, 000), Gansu (16.7 per 100, 000), Yunnan (16.4 per 100, 000), Liaoning (15.7 per 100, 000) and Guizhou (15.0 per 100, 000) led as the five provinces with the heaviest burden, while Macao (9.1 per 100, 000), Jiangsu (11.7 per 100, 000), Shaanxi (11.8 per 100, 000), Fujian (11.9 per 100, 000), and Inner Mongolia (12.7 per 100, 000) had the lowest burden.
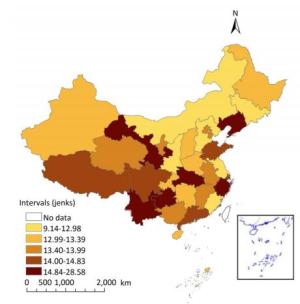
Figure 1. Spatial pattern of age-standardized YLD rate (per 100, 000) of dental caries among Chinese children aged 0-14 years in 2016.
From 1990 to 2016, the prevalence of dental caries among Chinese children aged 0 to 14 decreased gradually from 46.8% to 43.0%, and the YLD rate decreased from 16.5 per 100, 000 to 14.8 per 100, 000 (Figure 2). For children who suffered from DC, the prevalence and YLD rate for those under 5 years decreased slightly from 40.3% to 39.8%, and 9.5 per 100, 000 to 9.4 per 100, 000, respectively. Among children 5 to 14 years, DC prevalence decreased from 27.2% to 26.2%, and the YLD rate decreased from 6.4 per 100, 000 to 6.2 per 100, 000. In children aged 5 to 14 years who suffered from PC only, the prevalence decreased from 23.2% to 18.0% in 2016, while the YLD rate decreased from 13.9 per 100, 000 to 10.8 per 100, 000. Compared with boys, girls exhibited similar temporal changes in both DC and PC disease burden.

Figure 2. Temporal trend of disease burden for dental caries among Chinese children aged 0-14, 1990-2016. (A) Prevalence of dental caries among children aged 0-14, (B) YLD rate of dental caries among children aged 0-14, (C) Prevalence of DC among children aged 0-14, (D) YLD rate of DC among children aged 0-14, (E) Prevalence of PC among children aged 5-14, (F) YLD rate of PC among children aged 5-14. YLD represents years lived with disability. YLD rate represents age-standardized years lived with disability rate. DC represents deciduous caries. PC represents permanent caries.
In this study, we found that there was a slight decrease, between 1990 and 2016, in dental caries burden among children aged 0 to 14 years. However, Chinese children still suffer from considerable disease burden, with significant variations by gender, age, and region. The geographical pattern for burden of dental caries at the provincial level is not clear, making it difficult to develop an oral health promotion strategy at macro-scale.
This study found a reduction trend in dental caries burden among Chinese children aged 0 to 14 years. This decline may be attributed largely to several factors, including improved lifestyle, superior oral hygiene condition, effective use of an approved toothbrush, and fluoride toothpaste, regular oral health examination, and extensive community, school, and health-care-organization-based preventive programs.
However, dental caries is still of great concern among Chinese children 0 to 14 years. Particularly, children under 5 years with DC experienced the highest burden compared with other age groups. This confirmed the findings of previous studies. National oral health surveys and several regional studies[4, 5] have reported elevated DC prevalence among preschool children, with regional disparities from 30% to > 70%[2]. Compared with children of other developed countries, Chinese children have borne a higher burden of dental caries. The 2016 under-5 prevalence of DC in China was 43.0%, much higher than the estimated prevalence in the United States (18.22%), UK (10.39%), Australia (13.80%), France (14.79%), and Canada (19.81%)[10]. While in some developing countries, the 2016 under-5 prevalence of DC in South Africa was 26.04%; in Brazil, 27.12%; in Russia, 33.27%; and in India, 43.48%[10]. Compared with above developing countries that have a similar booming economy, the situation in China is not optimistic either. Reasons for the high burden were multiple. Since children at this stage received family care predominantly, parental factors, especially from mothers, may play a leading role in DC's occurrence and development. Parental factors found related to children's dental caries were low education level, ignorance of oral health, and underuse of childhood oral health services[1]. In addition to parents' poor oral health practices, the transition of daily lifestyle, family structure, child-rearing pattern, and food pyramid may also be factors in dental caries prevalence[1, 2]. Children from an early age had been carefully fed over processed foods such as refined rice and sugar, which probably increased the risk of deciduous caries. To effectively reduce the prevalence of childhood dental caries, interventions including broadened caries risk assessment, fluoride varnish application, and oral behavior improvement are vital[1, 2].
Gender difference in dental caries was significant. We found that more girls suffered from dental caries than did boys, which was consistent with previous studies[13]. The difference in inherent physiological characteristics and lifestyles were regarded as common factors contributing to the gap between boys' and girls' susceptibility[13]. Compared with boys, the higher prevalence in girls could be explained by the earlier eruption of deciduous teeth and frequent snacking, which left permanent teeth exposed to a cariogenic oral environment at an early stage. What is more, the biochemical composition of saliva and saliva flow rate are modified in several important ways by hormonal fluctuations during events such as puberty, making the oral environment significantly more cariogenic for girls than for boys[13].
Our analysis failed to detect any geographical patterns of dental caries at the provincial level. It seems that few links exist between the disease burden of dental caries in children and their level of economic development, as the classic east-central-west gradient was not observed, which had often been seen in other diseases' distribution. However, a marked variation with a twofold difference across provinces was observed. Such spatial inequity could result in higher costs and difficulty in tailoring a strategy for oral health promotion, since geographical targeting at a more local level is required to inform appropriate policymaking.
This study had several limitations. On the one hand, the conclusions were partially influenced by the inherent data quality of GBD 2016, such as definite data source, sampling and nonsampling error, model specification, model parameter estimation, and data interpretation. On the other hand, the disability weights of YLD estimation ware derived mainly from the Western population; the cultural diversities between China and the Western countries may reduce the validity and comparability of disease burden estimation. Furthermore, the differences in age grouping between GBD 2016 and some domestic oral health studies may influence the interpretation of disease burden estimation of children's dental caries.
The burden of dental caries among children aged between 0 and 14 years saw a slight decrease in the past 20-plus years. However, the prevalence and disease burden are still at a high level, compared with other countries. Given the marked variation at provincial level, strategies for addressing the spatial inequity of childhood dental caries require geographical targeting.
No conflict of interest to declare.
doi: 10.3967/bes2018.048
Prevalence and Years Lived with Disability for Dental Caries among Children Aged 0-14 Years in China, 1990-2016
-
Abstract: The estimate of dental caries among Chinese children at the microscale level using standard methodology remains unclear. In this study, we assessed and analyzed the disease burden of childhood dental caries in China by extracting data from the Global Burden of Disease, Injuries, and Risk Factors Study 2016 (GBD 2016). In 2016, the number of cases, prevalence, years lived with disability (YLD), and age-standardized YLD rate of dental caries was 93.0 million, 43.0%, 32, 200 person years, and 14.8 per 100, 000, respectively. Across 33 provincial units, the disease burden was highest in Hubei (YLD rate 28.6 per 100, 000), lowest in Macao (9.1 per 100, 000), while geographical clustering was not observed. Compared with 1990, the prevalence in 2016 decreased from 46.8% to 43.0%, and the YLD rate decreased from 16.5 per 100, 000 to 14.8 per 100, 000. Given the slight decrease in dental caries burden, the prevalence and disease burden remained high among Chinese children. Strategies for addressing the spatial inequity of childhood dental caries require geographical targeting.
-
Figure 1. Spatial pattern of age-standardized YLD rate (per 100, 000) of dental caries among Chinese children aged 0-14 years in 2016.
Figure 2. Temporal trend of disease burden for dental caries among Chinese children aged 0-14, 1990-2016. (A) Prevalence of dental caries among children aged 0-14, (B) YLD rate of dental caries among children aged 0-14, (C) Prevalence of DC among children aged 0-14, (D) YLD rate of DC among children aged 0-14, (E) Prevalence of PC among children aged 5-14, (F) YLD rate of PC among children aged 5-14. YLD represents years lived with disability. YLD rate represents age-standardized years lived with disability rate. DC represents deciduous caries. PC represents permanent caries.
Table 1. Number of Cases, Prevalence, YLD, and Age-standardized YLD Rate of Dental Caries among Chinese Children Aged 0-14 Years, 2016
Characteristic Sex Deciduous Caries (DC) Permanent Caries (PC) Dental Caries Under 5 (95% UI) 5-14 (95% UI) 5-14 (95% UI) 0-14 (95% UI) Number of cases (million) Male 13.2 (10.5, 16.0) 21.9 (17.0, 28.0) 13.7 (10.4, 17.4) 48.8 (37.8, 61.4) Female 10.9 (8.6, 13.2) 19.0 (14.9, 24.1) 14.3 (11.0, 18.0) 44.2 (34.5, 55.3) Total 24.1 (19.1, 29.1) 40.9 (31.8, 52.1) 28.0 (21.4, 35.3) 93.0 (72.2, 116.5) Prevalence (%) Male 40.7 (32.2, 49.2) 26.1 (20.3, 33.4) 16.3 (12.4, 20.8) 41.9 (32.5, 52.8) Female 38.7 (30.6, 47.0) 26.4 (20.6, 33.4) 19.9 (15.3, 25.0) 44.1 (34.4, 55.2) Total 39.8 (31.5, 48.0) 26.2 (20.4, 33.4) 18.0 (13.7, 22.6) 43.0 (33.4, 53.8) YLD (10, 000 person years) Male 0.3 (0.1, 0.6) 0.5 (0.2, 1.1) 0.8 (0.4, 1.7) 1.7 (0.7, 3.4) Female 0.3 (0.1, 0.5) 0.5 (0.2, 0.9) 0.9 (0.4, 1.7) 1.6 (0.7, 3.2) Total 0.6 (0.2, 1.1) 1.0 (0.4, 2.0) 1.7 (0.7, 3.4) 3.2 (1.4, 6.6) Age-standardized YLD rate (per 100, 000) Male 9.6 (4.0, 18.9) 6.2 (2.6, 12.6) 9.8 (4.2, 20.2) 14.2 (6.0, 28.9) Female 9.2 (3.8, 18.1) 6.2 (2.6, 12.8) 11.9 (5.1, 24.2) 15.6 (6.6, 31.7) Total 9.4 (3.9, 18.5) 6.2 (2.6, 12.8) 10.8 (4.6, 22.1) 14.8 (6.3, 30.3) Note. 95% UI represents 95% Uncertainty Intervals.  下载: 导出CSV
下载: 导出CSV
-
[1] World Health Organization. WHO expert consultation on public health intervention against early childhood caries: report of a meeting, Bangkok, Thailand, 26-28 January 2016. 2017. [2] Selwitz RH, Ismail AI, Pitts NB. Dental Caries. Lancet, 2007; 369, 51-9. doi: 10.1016/S0140-6736(07)60031-2 [3] Chen K, Gao S, Duangthip D, et al. Managing Early Childhood Caries for Young Children in China. Healthcare, 2018; 6, 11. doi: 10.3390/healthcare6010011 [4] The Report of the Forth National Oral Health Survey. Beijing: National Health and Family Planning Commission of the People's Republic of China, 2017. http://www.nhfpc.gov.cn/jkj/s5879/201709/9b4d4a4ec1c54723820dbaedf97a6d26.shtml. [2017-03-18] [5] Xiaoqiu Q. Report of the 3rd National Oral Health Epidemiological Investigatiom, Beijing, China. The People's Medical Publishing House, 2008; 1. [6] Tu R, Zhong Y, Li X, et al. Three Years Follow-up Observation and Analysis of Caries Status of Primary and Permanent Teeth among 652 6-Year-Old Children in Sichuan Province. West China Journal of Stomotology, 2015; 33, 45-9. http://labs.europepmc.org/abstract/MED/25872298 [7] Marcenes W, Kassebaum NJ, Bernabé E, et al. Global Burden of Oral Conditions in 1990-2010:A Systematic Analysis. J Dent Res, 2013; 92, 592-7. doi: 10.1177/0022034513490168 [8] Kassebaum NJ, Bernabe E, Dahiya M, et al. Global Burden of Untreated Caries:A Systematic Review and Metaregression. J Dent Res, 2015; 94, 650-8. doi: 10.1177/0022034515573272 [9] Vos T, Allen C, Arora M, et al. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 310 Diseases and Injuries, 1990-2015:A Systematic Analysis for the Global Burden of Disease Study 2015. Lancet, 2016; 388, 1545-602. doi: 10.1016/S0140-6736(16)31678-6 [10] Institute for Health Metrics and Evaluation (IHME). GBD Compare Data Visualization. Seattle, WA: IHME, University of Washington, 2017. https://vizhub.healthdata.org/gbdcompare/. [2018-03-21] [11] Salomon JA, Haagsma JA, Davis A, et al. Disability Weights for the Global Burden of Disease 2013 Study. Lancet Global Health, 2015; 3, e712-e23. doi: 10.1016/S2214-109X(15)00069-8 [12] United Nations, DESA/Population Devision. World Population Prospects 2012: United Nations. https://esa.un.org/unpd/wpp/. [2018-03-21] [13] Lukacs JR, Largaespada LL. Explaining Sex Differences in Dental Caries Prevalence:Saliva, Hormones, and 'Life-History' Etiologies. Am J Hum Biol, 2006; 18, 540-55. doi: 10.1002/(ISSN)1520-6300 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 1782
- HTML全文浏览量: 628
- PDF下载量: 86
- 被引次数: 0

 Quick Links
Quick Links