

 下载:
下载:

-
Non-Hodgkin lymphoma (NHL) is a common malignant tumor that originates in the lymphoid hematopoietic system and constitutes 2.8% of all cancers and 2.6% of all cancer-related deaths worldwide per year [1]. Diffuse large B-cell lymphoma (DLBCL) represents approximately 33.37% of all lymphomas and is the most common subtype [2,3]. Bone marrow infiltration is considered stage IV, and its strong invasiveness, easy extranodal invasion, and high risk of recurrence make treatment difficult [4,5]. Routine bone marrow examinations (bone marrow smears, biopsy, immunopathology, flow cytometry, cytogenetics, and molecular biology) are prone to misdiagnosis due to the limited location and quality of bone biopsy. In recent years, patients with DLBCL have been accurately diagnosed with systemic involvement due to the development and popularization of PET/CT examination; however, only a few studies on bone marrow are available [6-8]. Herein, we evaluated the efficacy and applicability of 2-deoxy-2-(18F) fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) for the diagnosing of DLBCL bone marrow infiltration compared to bone marrow aspiration and biopsy and described the PET/CT imaging characteristics of bone marrow infiltration.
-
This retrospective study evaluated 102 patients diagnosed at PLA General Hospital between September 2019 and August 2022. The inclusion criteria were as follows: primary DLBCL diagnosed by pathological histomorphology and immunohistochemistry according to the World Health Organization (WHO) classification system; age ≥ 18 years old; PET/CT examination and bone marrow biopsy (bone marrow smear, bone marrow biopsy and immunopathology, and bone marrow flow cytometry) were optimized at the first visit. The exclusion criteria were as follows: a second tumor (with or without bone metastasis); active inflammation or diffuse liver lesions during PET/CT examination; unstable blood glucose and fasting blood glucose ≥ 8.8 mmol/L during PET/CT examination; and patients who underwent treatment, such as radiotherapy, chemotherapy, or received granulocyte colony-stimulating factor (G-CSF), erythropoietin (EPO), and thrombopoietin (TPO) within 3 months.
-
A Discovery VCT PET/CT imager (GE Company) was used for detection. Before examination, patients were asked to fast for > 6 hours to bring their fasting blood glucose below 8.8 mmol/L. The intravenous injection dose of 18F-FDG was 4−5 MBq/kg. The patients were asked to empty their bladders 1 h after injection and scanned from the top of the skull to the bottom of the plantar surface using PET/CT. During reconstruction, PET images are required for anatomical localization and attenuation correction using an ordered subset expectation maximization (OSEM) algorithm. The scan results were analyzed by at least two experienced nuclear medicine radiologists. The PET/CT diagnostic criteria for bone marrow infiltration were according to the European Society for Medical Oncology (ESMO) clinical guidelines: the presence of increased FDG metabolism in the liver with or without increased diffuse uptake in focal bone marrow.
-
The anterior/posterior superior iliac spine was used as the entry point for the first biopsy. Bone marrow aspirates were examined using smear, biopsy, immunopathology, and flow cytometry. If the bone biopsy result was negative, but PET/CT detected abnormal metabolic signals, a second biopsy was performed. Hematologists performed bone marrow biopsy and flow cytometry, and the smear and biopsy immunopathology results were analyzed in the bone marrow morphology laboratory.
-
The results of bone marrow aspiration and biopsy of lymphoma cells (bone marrow smear, biopsy, immunopathology, and flow cytometry) were used as the gold standard to calculate several PET/CT indices for the diagnosis of DLBCL bone marrow infiltration, including sensitivity, specificity, total accuracy, positive predictive value, negative predictive value, and Youden’s index. All data were analyzed using SPSS 20.0. The McNemar’s test was used to compare the diagnostic efficiency of the two inspection methods. Kappa tests were used to measure the agreement between the two methods, with kappa coefficients ≥ 0.75, 0.4 ≤ k < 0.75, and k < 0.4, indicating strong, moderate, and weak agreement, respectively. A two-tailed P < 0.05 indicated statistical significance.
-
The study design and protocols were approved by the Ethics Committee of Chinese PLA General Hospital. Written informed consent was obtained from all participants.
-
In total, 102 patients were included in this study, 56 males (54.9%) and 46 females (45.1%). The cohort comprised 88 (86.3%) patients with Ann Arbor stage IV, 0 (0%) with stage III, and 14 (13.7%) with an international prognostic index (IPI) score of 4−5. The median and average ages at onset were 50 and 47 (range, 18–65) years, respectively. The clinical characteristics of the 102 patients with newly treated DLBCL are presented in Table 1.
Table 1. Clinical baseline characteristics of 102 diffuse large B-cell lymphoma patients
Clinical characteristics N (%) Age (year) ≥ 60 30 (29.4) Sex Male 56 (54.9) Female 46 (45.1) Ann-Arbor stage I 10 (9.8) II 4 (3.9) III 0 (0) IV 88 (86.3) IPI Score 3 15 (14.7) 4–5 14 (13.7) B symptoms 85 (83.3) ECOG score ≥ 3 38 (37.3) LDH > 250 U/L 79 (77.5) Hans subtype GCB 36 (35.3) Non-GCB 66 (64.7) Ki-67 ≥ 75% 34 (33.3) Blood routine HGB < 100 g/L 48 (47.1) WBC < 4.0 × 109/L 16 (15.7) PLT < 100 × 109/L 27 (26.5) Splenomegaly 32 (31.4) Hepatomegaly 10 (9.8) Lymphadenopathy 92 (90.2) Note. IPI: International prognostic index; ECOG: Eastern cooperative oncology group performance score; LDH: Lactate dehydrogenase; GCB: Germinal center B cell-like; HGB: Hemoglobin; WBC: White blood cell; PLT: Platelet count. -
Among the 102 patients, 21 cases of bone marrow infiltration were detected by initial bone marrow aspiration and biopsy (14 bone marrow smears, 21 immunopathology biopsies, and 18 flow cytometry results). The total detection rate was 20.6% (21/102); the detection rate of bone marrow smears was 13.7% (14/102), biopsy immunopathology was 20.6% (21/102), and flow cytometry was 17.6% (18/102).
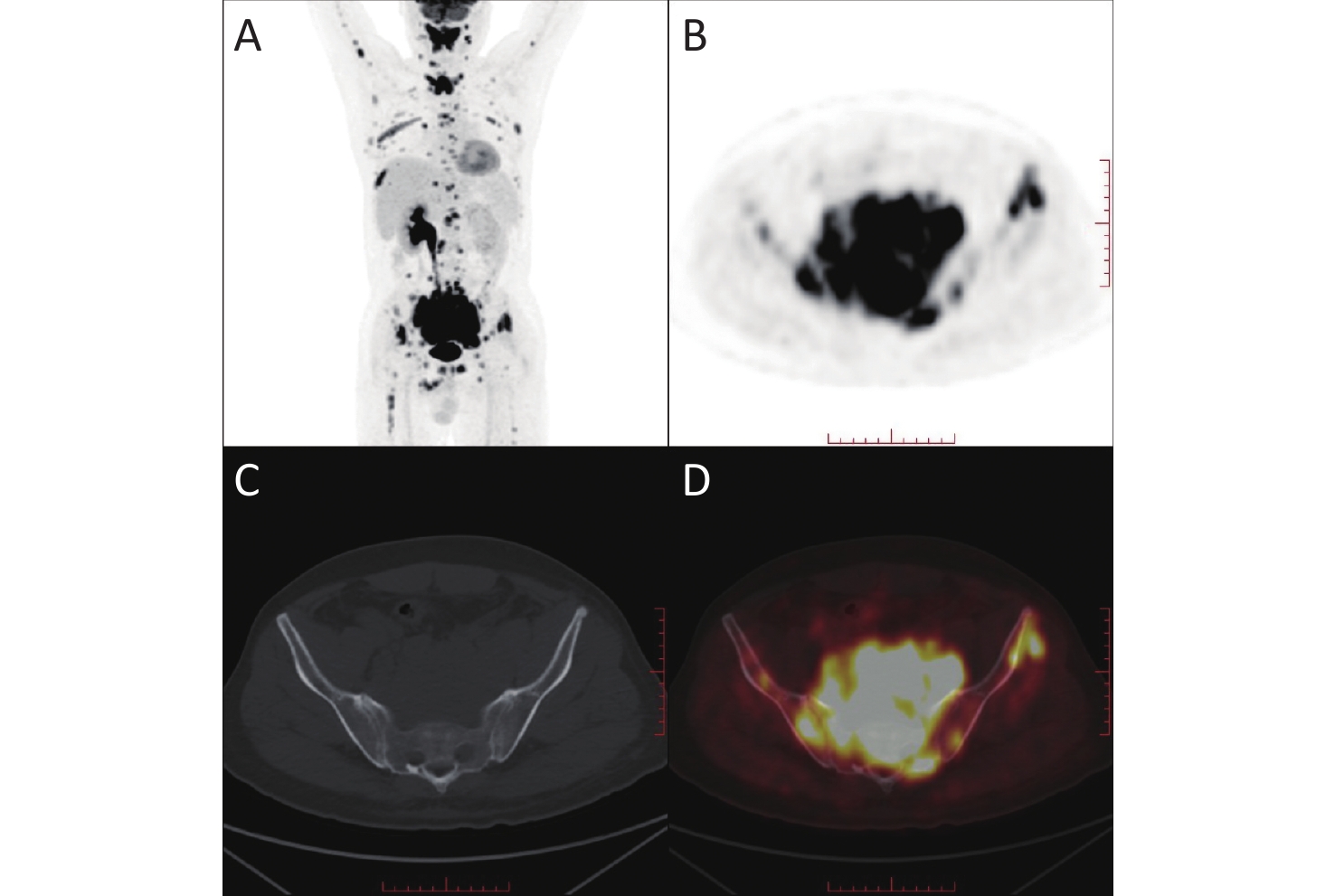
Patients with negative bone biopsy results but abnormal metabolic signals on PET/CT underwent a second biopsy of the abnormal bone marrow metabolic sites (Figure 1). Consequently, eight cases of bone marrow infiltration were detected. In total, 29/102 cases of bone marrow infiltration were detected in patients with DLBCL by bone marrow bone marrow aspiration and biopsy (including 20 iliums, 28 biopsy immunopathology, and 24 flow cytometry). The total detection rate of bone marrow infiltration in the combination of the first and second bone marrow aspiration and biopsy was 28.4% (29/102), and the detection rates of bone marrow smear, biopsy immunopathology, and flow cytometry were 19.6% (20/102), 27.5% (28/102), and 23.5% (24/102), respectively.

Figure 1. 18F-FDG PET/CT image of a patient with diffuse large B-cell lymphoma. (A) Maximum intensity projection (MIP)-PET/CT shows an increased FDG uptake in the pelvic cavity and bones. (B) Coronal PET, (C) Coronal CT, (D) Coronal fused PET/CT images show high metabolism in the left anterior superior iliac spine.
A total of 26/102 (25.5%) cases of bone marrow infiltration were detected using PET/CT, and the detection rate was not significantly different from that of the first bone marrow aspiration and biopsy (P = 0.302) or the combination of the two procedures (P = 0.453) (Table 2). However, the detection rate of PET/CT was higher than that of the initial bone marrow smear examination (P = 0.002) (Table 2). Moderate agreement was observed between PET/CT and the first DLBCL bone marrow infiltration (k = 0.587, P < 0.001), while strong agreement was detected between PET/CT and the combination of the two DLBCL bone marrow infiltrations (k = 0.826, P < 0.001).
Table 2. Comparison of detection rate of DLBCL bone marrow infiltration between biopsy and PET/CT
Detection methods S+T+ S+T- S-T+ S-T- P (McNemar test) Kappa P (Kappa) Total of first bone marrow examination 16 5 10 71 0.302 0.587 < 0.001 Bone marrow smear 13 1 13 75 0.002 0.574 < 0.001 Bone marrow biopsy immunopathology 16 5 10 71 0.302 0.587 < 0.001 Bone marrow flow cytometry 14 4 12 72 0.077 0.541 < 0.001 Combination of the first and second bone marrow examination 24 5 2 71 0.453 0.826 < 0.001 Bone marrow smear 19 1 7 75 0.070 0.777 < 0.001 Bone marrow biopsy immunopathology 23 5 3 71 0.727 0.799 < 0.001 Bone marrow flow cytometry 20 4 6 72 0.754 0.735 < 0.001 Note. S+, Gold standard positive; S-, Gold standard negative; T+, PET/CT positive; T-, PET/CT negative. DLBCL: Diffuse large B-cell lymphoma. -
Compared to standard first bone marrow aspiration and biopsy, the sensitivity of PET/CT in the diagnosis of DLBCL bone marrow infiltration was 0.615 [95% confidence interval (CI): 0.425−0.776], the specificity was 0.934 (95% CI: 0.855−0.972), and Youden’s index was 0.549 (Table 3). When the first and second bone marrow aspiration and biopsy were combined as the gold standard, the sensitivity, specificity, and Youden’s index of PET/CT were 0.923 (95% CI: 0.759−0.979), 0.934 (95% CI: 0.855−0.972), and 0.857, respectively (Table 3).
Table 3. Diagnostic efficacy of PET/CT for DLBCL bone marrow infiltration
Variables S+T+ S+T- S-T+ S-T- Sensitivity
(95% CI)Specificity
(95% CI)Youden’s index First bone marrow examination 16 5 10 71 0.615 (0.425–0.776) 0.934 (0.855–0.972) 0.549 Combination of the first and second bone marrow examination 24 5 2 71 0.923 (0.759–0.979) 0.934 (0.855–0.972) 0.857 Note. S: Diagnosis by DLBCL; T: Diagnosis by PET/CT; DLBCL: Diffuse large B-cell lymphoma. -
A total of 26 patients were diagnosed with bone marrow infiltration by PET/CT according to the ESMO clinical practice guidelines: 23/26 (88.5%) showed focally increased 18FDG uptake and 3/26 (11.5%) showed an increase in diffuse FDG metabolism in the bone marrow throughout the body. Among them, the top three incidence sites of increased focal metabolism were the ilium (21/26), 3−5 lumbar vertebrae (16/26), and femur (8/26), and the lower incidence sites were the sternum (1/26), humerus (1/26), and ribs (1/26). Of the three patients with diffuse FDG metabolism in the whole-body bone marrow, one patient was diagnosed with bone marrow infiltration by two bone biopsies and two patients were diagnosed without bone marrow infiltration (Table 4).
Table 4. Distribution and characteristics of bone marrow infiltration sites detected by PET-CT (a total of 26 cases)
Site and characteristics Cases (%) Focal increased 18FDG uptake 23 (88.5) Focal and systematic diffuse bone marrow 18FDG uptake 3 (11.5) Ilium 2 (80.8) Lumbar vertebra (L3–L5) 16 (61.5) Femur 8 (30.8) Sternum 1 (3.8) Humerus 1 (3.8) Ribs 1 (3.8) Among the 29 patients with DLBCL diagnosed by bone marrow infiltration, 23 showed only focally increased 18FDG uptake, one showed focally increased 18FDG uptake with increased systemic bone marrow diffuse FDG metabolism, two showed only increased systemic bone marrow diffuse FDG metabolism, and three did not show obvious abnormalities in bone marrow FDG metabolism.
-
Accurate staging of patients with DLBCL is a prerequisite to improve prognosis and treatment selection. In recent years, 18F-FDG PET/CT has been used for the clinical staging of lymphoma due to its accurate assessment of systemic lymphoma involvement; however, the currently recognized gold standard for assessing bone marrow is still bone marrow aspiration and biopsy [6,7]. In addition, the presence of bone marrow infiltration is a key issue not only for lymphoma patients but also for patients with refractory leukemia, and PET/CT is also used to detect bone marrow involvement in leukemia [8]. However, the following limitations of bone marrow aspiration and biopsy should be considered. First, the common point for bone marrow aspiration was the anterior iliac/posterior superior iliac spine; however, common focal occurrences of DLBCL bone marrow infiltration were in the vertebral body, pelvis, and femur. Therefore, false-negative results are likely to occur without lymphoma infiltration at the entry site [9,10]. Second, the quality of the specimens significantly affects the accuracy of the results. Third, invasive bone marrow aspiration and biopsy are inconvenient, and patients who undergo multiple punctures experience great pain during diagnosis and treatment. Furthermore, PET/CT can replace bone marrow aspiration and biopsy to assess the occurrence of bone marrow involvement in most cases of DLBCL, according to the 2016 ESMO guidelines and the 2014 Lugano classification [11,12].
Previous studies have confirmed that FDG uptake rates vary significantly in pathological types of lymphoma on PET/CT examination and that DLBCL is a highly sensitive type of cancer [13-17]. A meta-analysis by Adams et al.[18] on the diagnosis of DLBCL infiltration using FDG PET/CT showed that the diagnostic sensitivity and specificity of PET/CT were 88.7% and 99.8%, respectively, similar to those of the present study. In this study, 18F-FDG PET/CT had a high diagnostic efficiency for DLBCL bone marrow infiltration, in agreement with the gold standard (k = 0.826). Patients with a poor condition or poor bone marrow biopsy results due to age and mental state and who could not provide a high-quality specimen could be assessed for bone marrow infiltration using noninvasive PET/CT. It could also be used as an examination option in follow-up patients to track and evaluate bone marrow involvement and has been recommended internationally [6,19-26]. In the present study, we found that another eight patients with negative bone marrow infiltration for the first bone penetration had a second bone penetration due to the positive results of PET/CT, suggesting that biopsy combined with PET/CT guidance increases the detection rate. For newly diagnosed patients, bone marrow aspiration and biopsy could be performed according to PET/CT results, which improved the sensitivity of the examination and avoided repeated bone penetration pain.
Previous studies have found that the incidence of bone marrow infiltration in DLBCL at the first diagnosis was 11%–34% [27,28], consistent with our results (28.9%). The International Atomic Energy Agency sponsored a prospective international cohort study to better define the use of PET in DLBCL in eight countries that contributed to 327 cases; the hazard ratios for PET-negative/biopsy-negative cases versus PET-positive/biopsy-positive cases were 2.67 for EFS and 3.94 for OS. This large study showed that positive iliac crest biopsy histology only confers a poor prognosis to patients with abnormal marrow 18F-FDG uptake identified on the staging PET scan [29]. In this study, lymphoma cells detected using any method, including bone marrow smear, biopsy, immunopathology, and flow cytometry, were diagnosed as DLBCL bone marrow infiltration. When comparing the three methods, the sensitivity of bone marrow biopsy and immunopathology at the first diagnosis was higher than that of the smear, making it the first choice for patients with DLBCL. The current results suggest that the sites most likely for bone marrow infiltration on PET/CT examination were the iliac bone, lumbar spine (L3–5), and femur, consistent with most previous studies. Most patients with bone marrow infiltration [24,29] showed increased focal FDG uptake with or without increased systemic bone marrow diffuse FDG uptake on PET/CT instead of increased focal FDG uptake or tumor proliferation and invasiveness. Only two cases had elevated systemic bone marrow diffuse FDG uptake. Although some studies have noted that approximately 29% of newly diagnosed patients with lymphoma have diffusely elevated bone marrow FDG uptake, most have false-positive results. Therefore, diffuse uptake of FDG in the bone marrow is associated with bone marrow inflammation, systemic inflammation, and hematopoietic activity. Shagera et al. [30-32] showed that only IPI and 18F-PET/CT bone marrow status were independent factors for progression-free survival (PFS), as evaluated by multivariate analysis of newly treated DLBCL patients. Some studies [33,34] have shown that 18F-PET/CT-related parameters are closely related to overall survival and PFS and are critical for predicting the prognosis of DLBCL. This showed that the stratification rate of 18F-PET/CT was higher than that of bone marrow examination in patients with newly diagnosed DLBCL. Taken together, these studies suggest that PET/CT imaging should be combined with routine blood tests, C-reactive protein (CRP), and other results to evaluate the clinical correlation between increased FDG uptake and bone marrow infiltration. Meanwhile, as a single-center retrospective study, the sample size was acceptable compared to previous studies; however, some patients were in a relatively late stage, which could have resulted in selection bias. This is the main limitation of this study. Therefore, further studies with larger sample sizes and well-designed sampling methods are required.
In Summary, 18F-FDG PET/CT can be an alternative method for assessing bone marrow infiltration in patients with DLBCL who cannot tolerate a bone biopsy due to its high diagnostic efficiency. Bone marrow aspiration and biopsy guided by PET/CT improve the sensitivity of the overall diagnosis and reduce the missed diagnosis rate. PET/CT-guided secondary puncture can reduce missed diagnosis rates according to the gold standard and has potential clinical significance. -
The study design and protocols were approved by the Ethics Committee of the Chinese PLA General Hospital. Written informed consent was obtained from all enrolled subjects.
doi: 10.3967/bes2023.062
Diagnostic Efficacy of 18F-FDG PET/CT in Detecting Bone Marrow Infiltration in Patients with Newly Diagnosed Diffuse Large B-Cell Lymphoma
-
Abstract:
Objective Diffuse large B-cell lymphoma (DLBCL) is often associated with bone marrow infiltration, and 2-deoxy-2-(18F) fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) has potential diagnostic significance for bone marrow infiltration in DLBCL. Methods A total of 102 patients diagnosed with DLBCL between September 2019 and August 2022 were included. Bone marrow biopsy and 18F-FDG PET/CT examinations were performed at the time of initial diagnosis. Kappa tests were used to evaluate the agreement of 18F-FDG PET/CT with the gold standard, and the imaging features of DLBCL bone marrow infiltration on PET/CT were described. Results The total detection rate of bone marrow infiltration was not significantly different between PET/CT and primary bone marrow biopsy (P = 0.302) or between the two bone marrow biopsies (P = 0.826). The sensitivity, specificity, and Youden index of PET/CT for the diagnosis of DLBCL bone marrow infiltration were 0.923 (95% CI, 0.759−0.979), 0.934 (95% CI, 0.855−0.972), and 0.857, respectively. Conclusion 18F-FDG PET/CT has a comparable efficiency in the diagnosis of DLBCL bone marrow infiltration. PET/CT-guided bone marrow biopsy can reduce the misdiagnosis of DLBCL bone marrow infiltration. -
Key words:
- Diffuse large B-cell lymphoma /
- Bone marrow infiltration /
- Positron emission computed tomography (PET/CT) /
- Bone marrow biopsy /
- Diagnostic efficacy
The authors declare that they have no conflict of interest.
&These authors contributed equally to this work.
注释:1) AUTHORS’ CONTRIBUTIONS: 2) COMPETING INTERESTS: -
Figure 1. 18F-FDG PET/CT image of a patient with diffuse large B-cell lymphoma. (A) Maximum intensity projection (MIP)-PET/CT shows an increased FDG uptake in the pelvic cavity and bones. (B) Coronal PET, (C) Coronal CT, (D) Coronal fused PET/CT images show high metabolism in the left anterior superior iliac spine.
Table 1. Clinical baseline characteristics of 102 diffuse large B-cell lymphoma patients
Clinical characteristics N (%) Age (year) ≥ 60 30 (29.4) Sex Male 56 (54.9) Female 46 (45.1) Ann-Arbor stage I 10 (9.8) II 4 (3.9) III 0 (0) IV 88 (86.3) IPI Score 3 15 (14.7) 4–5 14 (13.7) B symptoms 85 (83.3) ECOG score ≥ 3 38 (37.3) LDH > 250 U/L 79 (77.5) Hans subtype GCB 36 (35.3) Non-GCB 66 (64.7) Ki-67 ≥ 75% 34 (33.3) Blood routine HGB < 100 g/L 48 (47.1) WBC < 4.0 × 109/L 16 (15.7) PLT < 100 × 109/L 27 (26.5) Splenomegaly 32 (31.4) Hepatomegaly 10 (9.8) Lymphadenopathy 92 (90.2) Note. IPI: International prognostic index; ECOG: Eastern cooperative oncology group performance score; LDH: Lactate dehydrogenase; GCB: Germinal center B cell-like; HGB: Hemoglobin; WBC: White blood cell; PLT: Platelet count.  下载: 导出CSV
下载: 导出CSV
Table 2. Comparison of detection rate of DLBCL bone marrow infiltration between biopsy and PET/CT
Detection methods S+T+ S+T- S-T+ S-T- P (McNemar test) Kappa P (Kappa) Total of first bone marrow examination 16 5 10 71 0.302 0.587 < 0.001 Bone marrow smear 13 1 13 75 0.002 0.574 < 0.001 Bone marrow biopsy immunopathology 16 5 10 71 0.302 0.587 < 0.001 Bone marrow flow cytometry 14 4 12 72 0.077 0.541 < 0.001 Combination of the first and second bone marrow examination 24 5 2 71 0.453 0.826 < 0.001 Bone marrow smear 19 1 7 75 0.070 0.777 < 0.001 Bone marrow biopsy immunopathology 23 5 3 71 0.727 0.799 < 0.001 Bone marrow flow cytometry 20 4 6 72 0.754 0.735 < 0.001 Note. S+, Gold standard positive; S-, Gold standard negative; T+, PET/CT positive; T-, PET/CT negative. DLBCL: Diffuse large B-cell lymphoma.
下载: 导出CSV
Table 3. Diagnostic efficacy of PET/CT for DLBCL bone marrow infiltration
Variables S+T+ S+T- S-T+ S-T- Sensitivity
(95% CI)Specificity
(95% CI)Youden’s index First bone marrow examination 16 5 10 71 0.615 (0.425–0.776) 0.934 (0.855–0.972) 0.549 Combination of the first and second bone marrow examination 24 5 2 71 0.923 (0.759–0.979) 0.934 (0.855–0.972) 0.857 Note. S: Diagnosis by DLBCL; T: Diagnosis by PET/CT; DLBCL: Diffuse large B-cell lymphoma.
下载: 导出CSV
Table 4. Distribution and characteristics of bone marrow infiltration sites detected by PET-CT (a total of 26 cases)
Site and characteristics Cases (%) Focal increased 18FDG uptake 23 (88.5) Focal and systematic diffuse bone marrow 18FDG uptake 3 (11.5) Ilium 2 (80.8) Lumbar vertebra (L3–L5) 16 (61.5) Femur 8 (30.8) Sternum 1 (3.8) Humerus 1 (3.8) Ribs 1 (3.8)
下载: 导出CSV
-
[1] Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin, 2021; 71, 209−49. doi: 10.3322/caac.21660 [2] Liu WP, Liu JM, Song YQ, et al. Burden of lymphoma in China, 2006-2016: an analysis of the global burden of disease study 2016. J Hematol Oncol, 2019; 12, 115. doi: 10.1186/s13045-019-0785-7 [3] Morton LM, Wang SS, Devesa SS, et al. Lymphoma incidence patterns by WHO subtype in the United States, 1992-2001. Blood, 2006; 107, 265−76. doi: 10.1182/blood-2005-06-2508 [4] Sehn LH, Scott DW, Chhanabhai M, et al. Impact of concordant and discordant bone marrow involvement on outcome in diffuse large B-cell lymphoma treated with R-CHOP. J Clin Oncol, 2011; 29, 1452−7. doi: 10.1200/JCO.2010.33.3419 [5] Li SY, Young KH, Medeiros LJ. Diffuse large B-cell lymphoma. Pathology, 2018; 50, 74−87. [6] Chen-Liang TH, Martin-Santos T, Jerez A, et al. The role of bone marrow biopsy and FDG-PET/CT in identifying bone marrow infiltration in the initial diagnosis of high grade non-Hodgkin B-cell lymphoma and Hodgkin lymphoma. Accuracy in a multicenter series of 372 patients. Am J Hematol, 2015; 90, 686−90. doi: 10.1002/ajh.24044 [7] Chen YM, Zhou MG, Liu JJ, et al. Prognostic value of bone marrow FDG uptake pattern of PET/CT in newly diagnosed diffuse large B-cell lymphoma. J Cancer, 2018; 9, 1231−8. doi: 10.7150/jca.23714 [8] Kaya Z, Akdemir OU, Atay OL, et al. Utility of 18-fluorodeoxyglucose positron emission tomography in children with relapsed/refractory leukemia. Pediatr Hematol Oncol, 2018; 35, 393−406. doi: 10.1080/08880018.2018.1557306 [9] Adams HJA, Nievelstein RAJ, Kwee TC. Opportunities and limitations of bone marrow biopsy and bone marrow FDG-PET in lymphoma. Blood Rev, 2015; 29, 417−25. doi: 10.1016/j.blre.2015.06.003 [10] El-Galaly TC, d'Amore F, Mylam KJ, et al. Routine bone marrow biopsy has little or no therapeutic consequence for positron emission tomography/computed tomography-staged treatment-naive patients with Hodgkin lymphoma. J Clin Oncol, 2012; 30, 4508−14. doi: 10.1200/JCO.2012.42.4036 [11] Vitolo U, Seymour JF, Martelli M, et al. Extranodal diffuse large B-cell lymphoma (DLBCL) and primary mediastinal B-cell lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol, 2016; 27, v91−102. doi: 10.1093/annonc/mdw175 [12] Cheson BD, Fisher RI, Barrington SF, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol, 2014; 32, 3059−68. doi: 10.1200/JCO.2013.54.8800 [13] Cottereau AS, Meignan M, Nioche C, et al. Risk stratification in diffuse large B-cell lymphoma using lesion dissemination and metabolic tumor burden calculated from baseline PET/CT. Ann Oncol, 2021; 32, 404−11. doi: 10.1016/j.annonc.2020.11.019 [14] Kurch L, Hüttmann A, Georgi TW, et al. Interim PET in diffuse large B-cell lymphoma. J Nucl Med, 2021; 62, 1068−74. doi: 10.2967/jnumed.120.255034 [15] Freeman CL, Savage KJ, Villa DR, et al. Long-term results of PET-guided radiation in patients with advanced-stage diffuse large B-cell lymphoma treated with R-CHOP. Blood, 2021; 137, 929−38. doi: 10.1182/blood.2020005846 [16] Zhang XH, Chen L, Jiang H, et al. A novel analytic approach for outcome prediction in diffuse large B-cell lymphoma by [18F]FDG PET/CT. Eur J Nucl Med Mol Imaging, 2022; 49, 1298−310. doi: 10.1007/s00259-021-05572-0 [17] Burggraaff CN, Eertink JJ, Lugtenburg PJ, et al. 18F-FDG PET improves baseline clinical predictors of response in diffuse large B-cell lymphoma: the HOVON-84 study. J Nucl Med, 2022; 63, 1001−7. doi: 10.2967/jnumed.121.262205 [18] Adams HJA, Kwee TC, De Keizer B, et al. FDG PET/CT for the detection of bone marrow involvement in diffuse large B-cell lymphoma: systematic review and meta-analysis. Eur J Nucl Med Mol Imaging, 2014; 41, 565−74. doi: 10.1007/s00259-013-2623-4 [19] Aguado-Vázquez TM, Olivas-Martínez A, Cancino-Ramos U, et al. 18f-fluorodeoxyglucose positron emission tomography versus bone marrow biopsy for the evaluation of bone marrow infiltration in newly diagnosed lymphoma patients. Rev Invest Clin, 2020; 73. [20] Teagle AR, Barton H, Charles-Edwards E, et al. Use of FDG PET/CT in identification of bone marrow involvement in diffuse large B cell lymphoma and follicular lymphoma: comparison with iliac crest bone marrow biopsy. Acta Radiol, 2017; 58, 1476−84. doi: 10.1177/0284185117701305 [21] Zaucha JM, Chauvie S, Zaucha R, et al. The role of PET/CT in the modern treatment of Hodgkin lymphoma. Cancer Treat Rev, 2019; 77, 44−56. doi: 10.1016/j.ctrv.2019.06.002 [22] El Karak F, Bou-Orm IR, Ghosn M, et al. PET/CT scanner and bone marrow biopsy in detection of bone marrow involvement in diffuse large B-cell lymphoma. PLoS One, 2017; 12, e0170299. doi: 10.1371/journal.pone.0170299 [23] Ujjani CS, Hill EM, Wang HK, et al. 18F-FDG PET-CT and trephine biopsy assessment of bone marrow involvement in lymphoma. Br J Haematol, 2016; 174, 410−6. doi: 10.1111/bjh.14071 [24] Moulin-Romsee G, Hindié E, Cuenca X, et al. 18F-FDG PET/CT bone/bone marrow findings in Hodgkin's lymphoma may circumvent the use of bone marrow trephine biopsy at diagnosis staging. Eur J Nucl Med Mol Imaging, 2010; 37, 1095−105. doi: 10.1007/s00259-009-1377-5 [25] Lakhwani S, Cabello-García D, Allende-Riera A, et al. Bone marrow trephine biopsy in Hodgkin's lymphoma. Comparison with PET-CT scan in 65 patients. Med Clín, 2018; 150, 104−6. [26] Kaddu-Mulindwa D, Altmann B, Held G, et al. FDG PET/CT to detect bone marrow involvement in the initial staging of patients with aggressive non-Hodgkin lymphoma: results from the prospective, multicenter PETAL and OPTIMAL>60 trials. Eur J Nucl Med Mol Imaging, 2021; 48, 3550−9. doi: 10.1007/s00259-021-05348-6 [27] Schaefer NG, Strobel K, Taverna C, et al. Bone involvement in patients with lymphoma: the role of FDG-PET/CT. Eur J Nucl Med Mol Imaging, 2007; 34, 60−7. doi: 10.1007/s00259-006-0238-8 [28] Pelosi E, Penna D, Douroukas A, et al. Bone marrow disease detection with FDG-PET/CT and bone marrow biopsy during the staging of malignant lymphoma: results from a large multicentre study. Q J Nucl Med Mol Imaging, 2011; 55, 469−75. [29] Cerci JJ, Györke T, Fanti S, et al. Combined PET and biopsy evidence of marrow involvement improves prognostic prediction in diffuse large B-cell lymphoma. J Nucl Med, 2014; 55, 1591−1597. doi: 10.2967/jnumed.113.134486 [30] Shagera QA, Cheon GJ, Koh Y, et al. Prognostic value of metabolic tumour volume on baseline 18F-FDG PET/CT in addition to NCCN-IPI in patients with diffuse large B-cell lymphoma: further stratification of the group with a high-risk NCCN-IPI. Eur J Nucl Med Mol Imaging, 2019; 46, 1417−27. doi: 10.1007/s00259-019-04309-4 [31] Cottereau AS, Nioche C, Dirand AS, et al. 18F-FDG PET dissemination features in diffuse large B-cell lymphoma are predictive of outcome. J Nucl Med, 2020; 61, 40−5. doi: 10.2967/jnumed.119.229450 [32] Islam P, Goldstein J, Flowers CR. PET-derived tumor metrics predict DLBCL response and progression-free survival. Leuk Lymphoma, 2019; 60, 1965−71. doi: 10.1080/10428194.2018.1562181 [33] Araz M, Soydal C, Ozturk C, et al. An uncommon presentation of diffuse large B cell lymphoma with multiple peripheral nerve involvement demonstrated BY 18F-FDG PET/CT. Eur J Nucl Med Mol Imaging, 2020; 47, 218−9. doi: 10.1007/s00259-019-04428-y [34] Lee JW, Oh D, Eom KY, et al. The prognostic value of PET/CT evaluation with Deauville score on the recurrence and survival in diffuse large B-cell lymphoma: a multi-institutional study of KROG 17-02. Clin Exp Metastasis, 2020; 37, 125−31. doi: 10.1007/s10585-019-09992-z -

 点击查看大图
点击查看大图
计量
- 文章访问数: 418
- HTML全文浏览量: 195
- PDF下载量: 32
- 被引次数: 0

 Quick Links
Quick Links