

 下载:
下载:




-
Lung cancer is associated with high rates of morbidity and mortality worldwide[1], with non-small cell lung cancer (NSCLC) most commonly presenting as lung adenocarcinoma (LUAD). Due to the absence of early stage symptoms in patients diagnosed with LUAD, the disease often progresses to advanced stages before the first diagnosis; consequently, treatment effectiveness is severely limited[2]. LUAD is currently treated with surgery and a variety of other treatments; however, patients with lung cancer are at risk of mortality due to local recurrences and distant metastases. The metastatic processes of LUAD includes invasion, circulatory dissemination, distant cloning, and angiogenesis. Understanding the pathogenesis, progression, and molecular mechanisms of drug resistance in LUAD is key to precision therapy. Biomarker screening is vital for accurate diagnosis and effective treatment of LUAD. Previous studies of LUAD have found potential epidermal growth factor receptor (EGFR) mutations and anaplastic lymphoma kinase (ALK) fusions or rearrangements in patients. In clinical practice, only a few patients are eligible for targeted therapies; therefore, treatment and prognosis of LUAD are greatly influenced by validating clinically useful targets.
Recent research has identified PRR11 as a gene on chromosome 17q22 that performs specific functions in lung cancer development and cell cycle regulation. PRR11 contains a zinc finger domain and two proline-rich regions; double-stranded DNA binds to zinc regulators that regulate gene transcription. PRR11 is widely distributed throughout the cytoplasm, cytoskeleton, and nucleus[3]. The biological structure of the PRR11 protein is comprised of three main parts: a binary nuclear localization signal, proline-enriched region, and zinc finger domain including a proline-enriched motif associated with SH3, which regulates protein-protein interactions, participates in intracellular signal transduction, and triggers tumor malignant biological behavior.
Significant evidence suggests that PRR11 is highly expressed in tumors associated with gastric cancer, breast cancer, and hilar cholangiocarcinoma, and plays a critical role in maintaining malignant phenotypes in cancer cells. PRR11 knockdown in lung cancer cells inhibits cell proliferation, cell cycle progression, migration, invasion, and colony formation in vitro. Although the involvement of PRR11 in lung cancer has been established, the relationship between PRR11 and immune infiltration has not comprehensively explored. Thus, the purpose of this study was to classify lung adenocarcinoma patients using bioinformatics methods to examine the relationship between PRR11 and immune infiltration. The findings of this study will aid in the use of PRR11 as a potential marker for the diagnosis, treatment, and prognosis of LUAD.
We obtained gene expression, clinical, and immune infiltration data from TCGA database (https://gdc.nci.nih.gov). The lung adenocarcinoma transcriptome dataset included 539 tumor samples and 59 adjacent tissue samples. Gene enrichment analysis (GSEA) was performed using normalized RNA-Seq data from TCGA. To investigate the potential biological functions of PRR11, GSEA was used to identify Gene Ontology (GO) functions and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathways. To be considered statistically significant, enrichment results must meet two conditions: false discovery rate (FDR) < 0.05 and P < 0.05. Using the Gene Expression Profiling Interactive Analysis (GEPIA) online database (
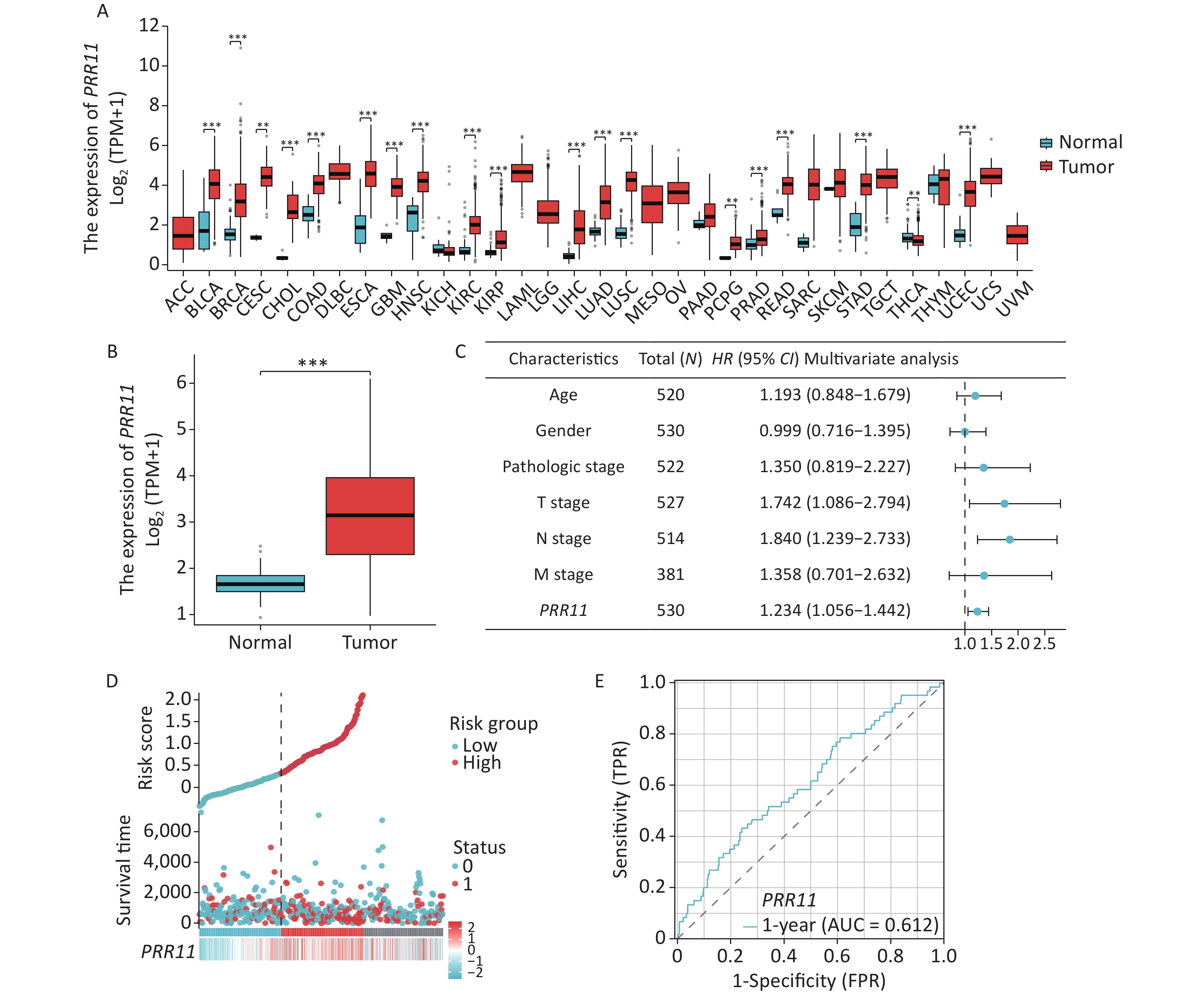
http://gepia.cancerpku.cn/ ), PRR11 expression in lung adenocarcinomas was compared to that in normal tissues and the relationship between overall survival (OS) and PRR11 expression in LUAD was determined. The Human Protein Atlas Database (HPA) (http://protein atlas.org ) was used to compare the protein expression of PRR11 in lung adenocarcinoma and normal lung tissues. The TIMER (https://cistrome.shinyapps.io/timer/ ) analysis tool was used for systematic analysis of immune infiltrates in various types of cancer. Evaluation of the potential relationship between PRR11 expression and tumor-infiltrating immune cells was performed using the TIMER correlation module. A literature search was used to identify 24 tumor-infiltrating immune cells and single-sample gene set enrichment analysis (ssGSEA) was carried out using the “GSVA” R package to determine their relationship with PRR11 expression in LUAD. R software v.4.2.1 (R Core Team 2022) was used for all statistical analyses. Univariate and Multivariate Cox models were used to calculate 95% CIs and HRs. Univariate survival analysis was performed to examine the relationships between several clinical characteristics and survival. The impact of PRR11 expression and other pathological and clinical factors on overall survival were evaluated based on the results of Multivariate Cox analysis. Logistic Regression analysis was used to analyze the association between the clinical characteristics and PRR11 expression.Bioinformatics analysis identified high PRR11 expression in most of cancers (Figure 1A). PRR11 mRNA expression levels in normal tissues and lung adenocarcinomas were studied using TCGA database. Differential analysis was performed on data from 59 normal and 539 tumor tissue samples. PRR11 expression was significantly higher in tumor tissue samples than that in normal samples (P < 0.001, Figure 1B). As shown in Supplementary Table S1 (available in www.besjournal.com), the association between PRR11 expression and several characteristic variables of OS in patients with lung adenocarcinoma was examined using Cox regression analysis. Pathological stage (P < 0.001), tumor TNM stage (P < 0.01), and PRR11 expression (P < 0.001) were significantly associated with OS. Multivariate analysis results are shown in Figure 1C; PRR11 expression (P = 0.008) played a significant role in prognosis (Supplementary Table S2, available in www.besjournal.com). Patient PRR11 expression distributions and survival statuses are shown in Figure 1D. The AUC value of PRR11 expression on the ROC curve was 0.612 (Figure 1E), indicating PRR11 as a predictor of prognosis.
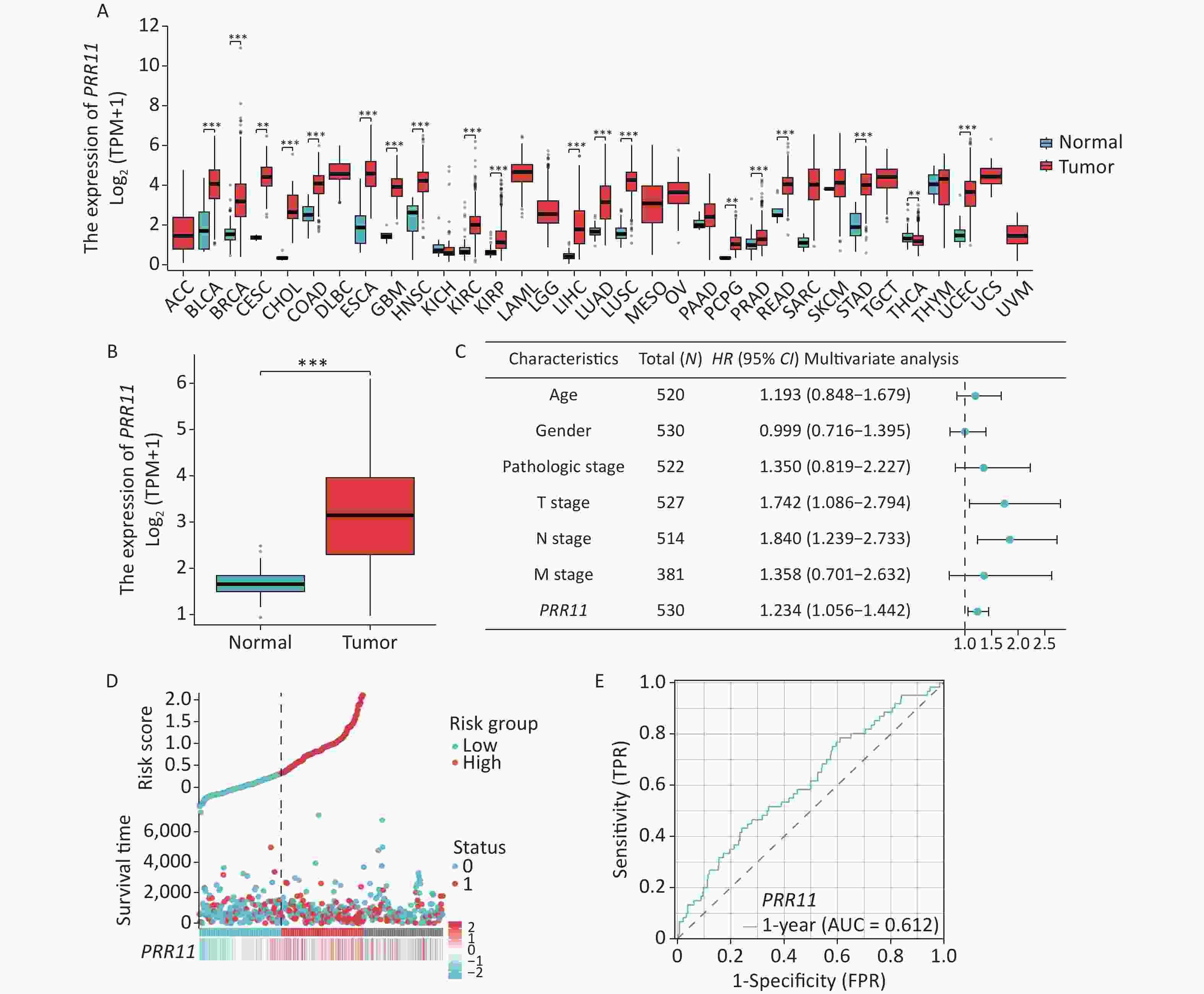
Figure 1. Expression and survival analysis of PRR11 in lung adenocarcinoma. (A) The expression of PRR11 in pan-cancer; (B) Differences in PRR11 expression between normal and LUAD tissues; (C) PRR11 expression and clinicopathological variables examined using Multivariate Cox regression; (D) Distribution of PRR11 expression and survival status; (E) An analysis of PRR11 in LUAD using ROC curve. (**, P < 0.01; ***, P < 0.001)
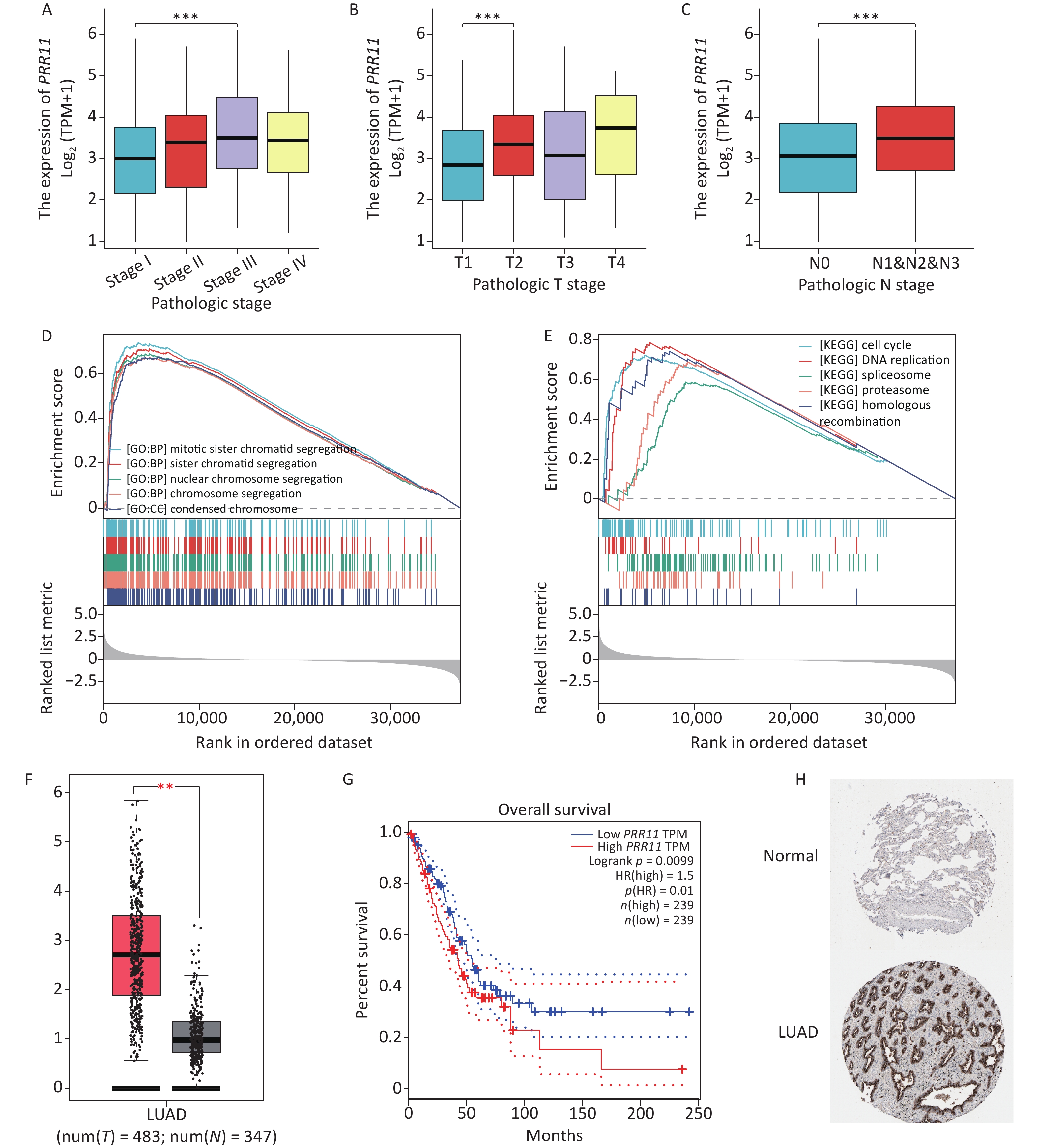
This study evaluated whether PRR11 expression levels were correlated with several clinical parameters in patients with lung adenocarcinoma. A total of 539 lung adenocarcinoma samples were obtained from TCGA, including PRR11 expression data from various clinical conditions. The analysis revealed that PRR11 expression levels were significantly correlated with pathological stage (III vs. I, P < 0.001), T grade (T2 vs. T1, P < 0.001), and N grade (N1 + N2 + N3 vs. N0, P < 0.001) (Figure 2A–C). Logistic regression analysis revealed that PRR11 expression was associated with adverse clinicopathological and prognostic characteristics (Supplementary Table S3, available in www.besjournal.com). PRR11 expression level was significantly correlated with the pathological stages, T grade and N grade (P < 0.01) in lung adenocarcinoma tissues. High PRR11 expression was associated with more aggressive, poorly developed tumor morphologies and stage progression in patients.
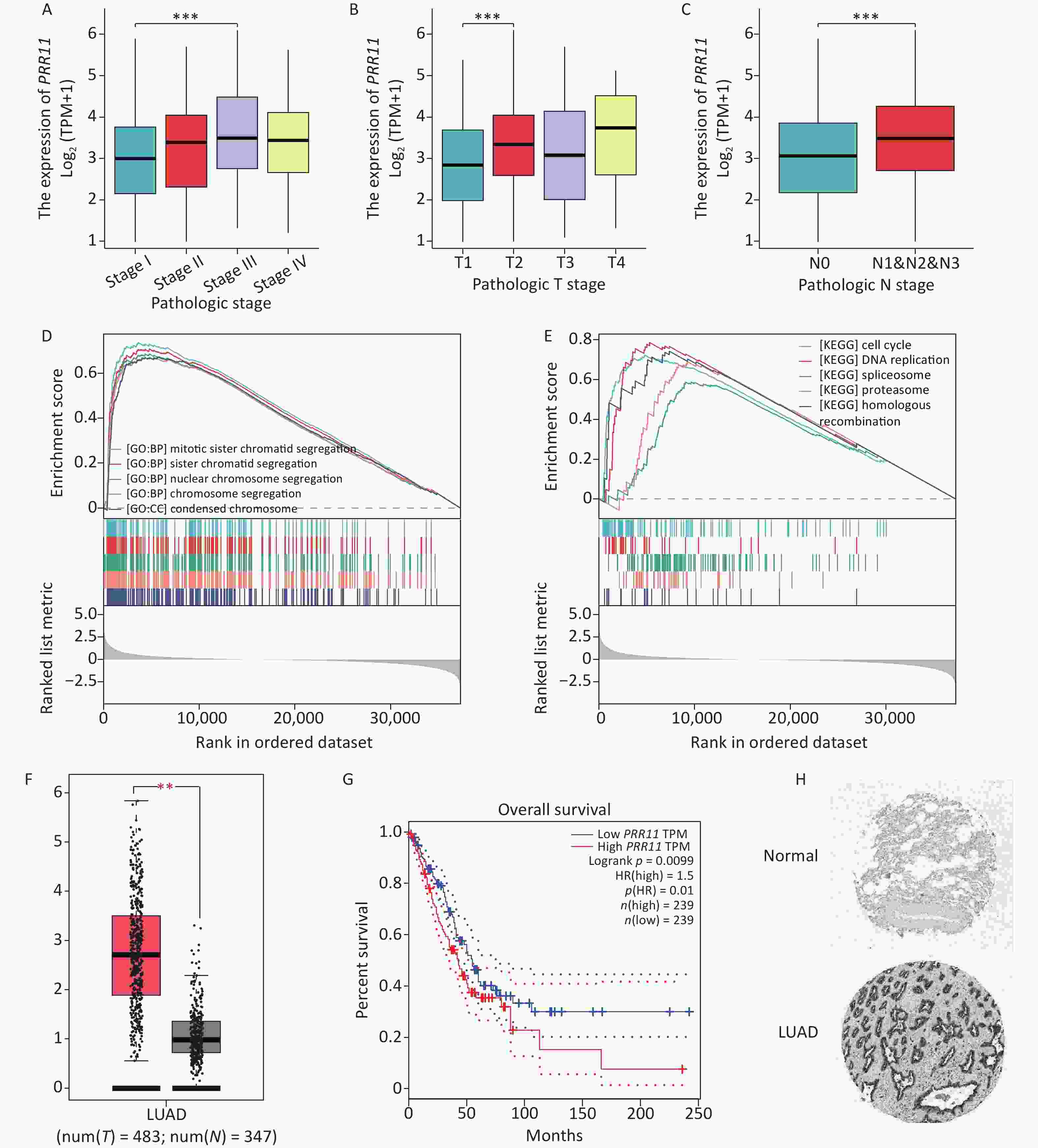
Figure 2. Analysis of PRR11 expression and clinicopathological factors, PRR11 enrichment analysis, and verification of data results. (A–C) PRR11 expression showed a significant correlation with histological pathologic grade (A), T stage (B), and N stage (C); (D–E) GO and KEGG enrichment pathway analysis; (F–G) The comparison of PRR11 expression levels and overall survival based on GEPIA data; (H) Immunohistochemical analysis of lung adenocarcinoma expression of the PRR11 protein was conducted using HPA. (**, P < 0.01; ***, P < 0.001)
GSEA showed significant differences for samples with high PRR11 levels in GO and KEGG pathway enrichment (FDR < 0.05, P < 0.05). GO functional analysis revealed five categories positively associated with high PRR11 expression (Figure 2D): mitotic sister chromatid segregation, sister chromatid separation, nuclear chromosome segregation, chromosome segregation, and condensed chromosomes. KEGG pathway analysis revealed five pathways positively associated with PRR11 expression (Figure 2E): cell cycle, DNA replication, spliceosome, proteasome, and homologous recombination. These findings suggest that pathways regulating cell cycle control and amino acid metabolism are critical in the development of lung adenocarcinoma. PRR11 mRNA expression was significantly higher in lung adenocarcinoma tissues than that in normal tissues (|Log2FC| > 1, P < 0.001) (Figure 2F). As shown in Figure 2G, PRR11 mRNA levels were correlated with poor overall survival (P < 0.01). PRR11 expression was higher in lung adenocarcinoma tissues than that in non-neoplastic tissues by HPA immunohistochemistry (Figure 2H).
We investigated whether tissue PRR11 expression correlated with immune infiltration using TIMER. As shown in Figure 3A, PRR11 expression was positively correlated with CD8+T cells (P = 5.58 × 10−7), neutrophils (P = 2.79 × 10−12) and dendritic cells (P = 2.95 × 10−5), thus indicating PRR11 as crucial for immune cell infiltration in LUAD. ssGSEA revealed that the levels of PRR11 mRNA were correlated with immune cell infiltration levels in LUAD. As shown in Figures 3B and 3C, a significant positive correlation was found between PRR11 mRNA levels and immune cell abundance [T helper 2 (Th2) cells] (P < 0.001). In addition, our heat map assessing correlations among the 24 immune cell types (Figure 3D) revealed an important relationship between different subsets of tumor-infiltrating immune cells.
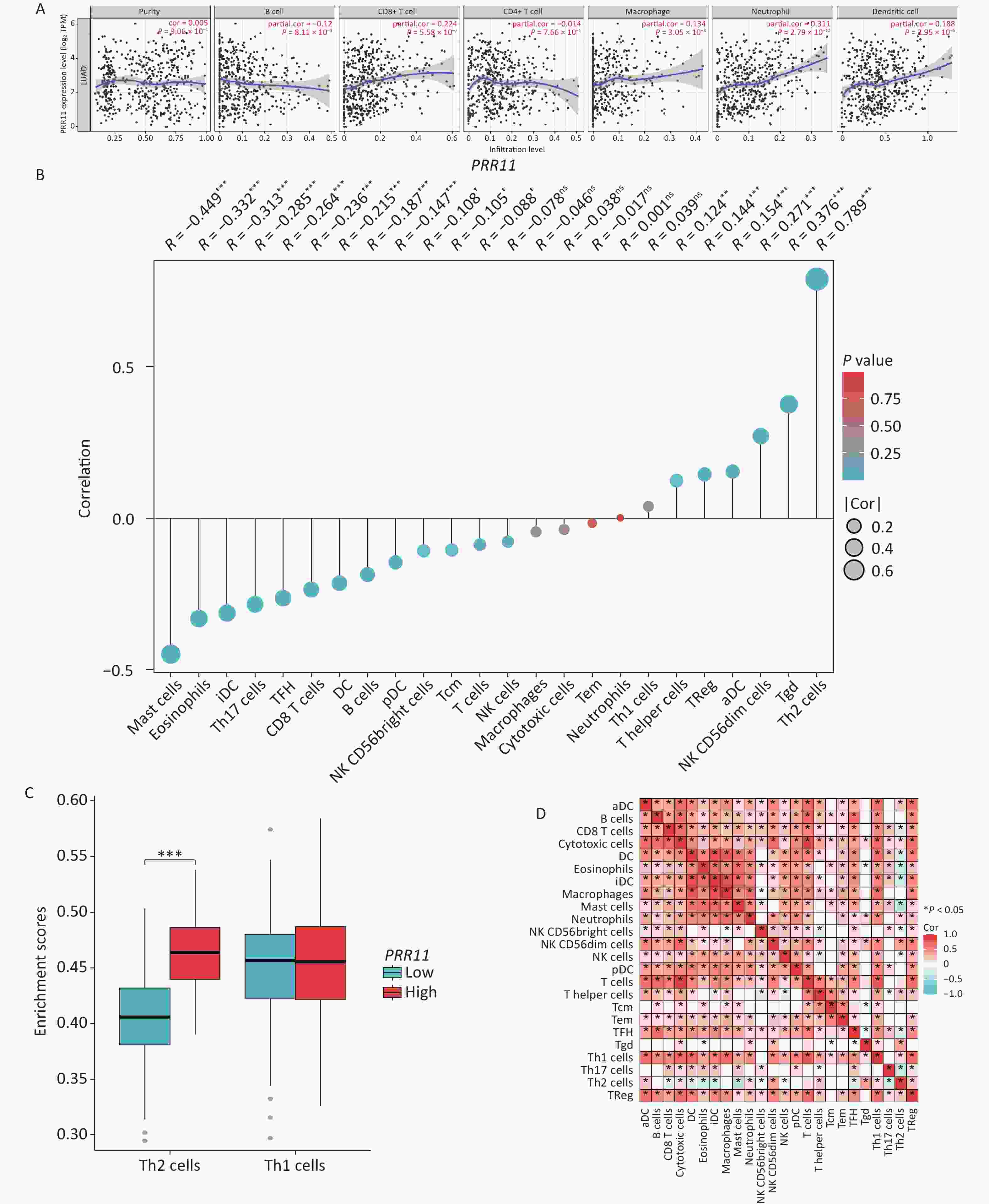
Figure 3. Association between PRR11 and immune infiltration. (A) Relationship between PRR11 and immune cells in TIMER; (B) Correlation between the relative abundances of 24 immune cell types and PRR11 levels; (C) Differences between tumor samples with high and low PRR11 expression in Th2 and Th1 cell proportions; (D) Heatmap of 24 immune infiltration cells in LUAD samples. (***, P < 0.001)
LUAD is one of the most aggressive cancers due to the associated mortality rate, which has gradually increased in prevalence. The development of targeted therapy and immunotherapy has benefited many patients with LUAD by significantly prolonging survival[4]. The identification of meaningful gene targets for LUAD is valuable for guiding diagnosis and treatment[5]. Previous research has shown that PRR11 expression is markedly low in normal tissues but significantly upregulated in some tumors[6]. In the current study, the cell cycle was significantly arrested and the ability of cells to invade and migrate was reduced after PRR11 knockdown. Further, microarray analysis revealed the downregulation of key genes in several important pathways involved in cell cycle regulation, tumorigenesis, and metabolism. Notably, PRR11 has been validated to be associated with tumor initiation and progression and can be used as a prognostic indicator for a variety of tumors[7].
Using bioinformatics tools and methods, data on lung adenocarcinoma subtypes were obtained from 59 normal and 539 tumor tissue samples and subsequently analyzed. Studies have investigated PRR11 expression as a prognostic biomarker for lung adenocarcinoma. Based on TCGA data, PRR11 was assessed for its prognostic value in patients with lung adenocarcinoma. The association of PRR11 upregulation with various tumor characteristics and immune responses revealed its prognostic significance in patients with poor OS. In lung adenocarcinoma patients with high PRR11 expression, stage and tumor status were more advanced than those in lung adenocarcinoma patients with low expression. Thus, high levels of PRR11 expression may affect the progression of lung adenocarcinoma and the immune response.
PRR11 upregulation was predominantly related to the cell cycle and amino acid metabolism pathways based on GO function and KEGG pathway analysis. PRR11 is known to be involved in signaling pathways related to cell cycle progression and may be closely associated with malignant tumor development in certain cancers, such as lung cancer. Silencing PRR11 expression in lung cancer cells inhibited tumor growth and arrested the cell cycle. Consequently, cell cycle regulatory genes (e.g., CCNA1, CCNA2, and CDK6) were altered. The discovery of the biological processes and pathways in which PRR11 is involved in regarding LUAD may help verify its role in promoting cancer progression.
According to the TIMER database, PRR11 expression was associated with immune cell infiltration in lung adenocarcinoma. PRR11 is strongly associated with CD8+T cells, neutrophils, and dendritic cells. Furthermore, our analysis revealed a significant relationship between PRR11 expression and immune cell infiltration, particularly of Th2 cells, thus potentially revealing the mechanism by which PRR11 regulates Th1/Th2 cell function in lung cancer. Helper T cells (Th cells) are important immunoregulatory cells that can be categorized into two main types: Th1 and Th2[8]. Th1 can produce cytokines such as IL-2, IFN-γ, TNF-β and others, which participate in cellular immunity. Th2 cells can produce cytokines such as IL-4, IL-5, and IL-10, which mediate humoral immunity. In particular, Th1 cells inhibit tumor growth by producing proinflammatory cytokines such as IFN-γ and IL-2, whereas Th2 cells produce anti-inflammatory cytokines such as IL-4 and IL-10 that promote tumor growth and metastasis[9]. Cellular immunity is a major component of the human immune response against cancer[10]. However, tumors have an immune escape mechanism that can lead to immune dysfunction, which allow them to evade or avoid immune strikes. In the lung cancer microenvironment, a shift in the Th1/Th2 balance is closely associated with tumor progression. Lung cancer cells can interact with Th1 and Th2 cells and cause a shift in Th1/Th2 balance, consequently accelerating lung cancer metastasis and progression. In this study, PRR11 and Th2 cells decreased, thus indicating the superiority of humoral immunity, inhibiting the secretion of cytokines and cellular immune function of the body, and enabling tumor cells to survive and proliferate. The Th1/Th2 balance shift makes tumor cells more vulnerable to immune surveillance and attack, and accelerates the metastatic progression of lung adenocarcinoma. These findings suggest that PRR11 is important for the regulation and recruitment of immune-infiltrating cells in lung cancer. However, to better understand the relationship between PRR11 and Th1/Th2 cell balance in vivo, controlled experiments and multicenter clinical trials are necessary.
In conclusion, this study used bioinformatic techniques to identify PRR11 as a biomarker in lung adenocarcinoma. As a regulatory and immune cell-infiltrating factor, PRR11 appears to be associated with a poor prognosis in LUAD. With further investigation into its functional scope, PRR11 may be a potential target for the diagnosis and treatment of lung adenocarcinomas.
-
Table S1. Correlation between overall survival (OS) and multivariable characteristics in TCGA-LUAD patients via Cox regression
ID HRs 95% CI P value Age 1.216 0.910–1.625 0.186 Gender 1.087 0.816–1.448 0.569 Pathologic stage 2.710 1.994–3.685 < 0.001 T stage 2.352 1.614–3.426 < 0.001 N stage 2.547 1.904–3.407 < 0.001 M stage 2.176 1.272–3.722 0.005 PRR11 1.268 1.117–1.441 < 0.001 Table S2. Correlation between overall survival (OS) and multivariable characteristics in TCGA-LUAD patients via a Multivariate survival model
ID HRs 95% CI P value Age 1.193 0.848−1.679 0.31 Gender 0.999 0.716−1.395 0.996 Pathologic stage 1.350 0.819−2.227 0.239 T stage 1.742 1.086−2.794 0.021 N stage 1.840 1.239−2.733 0.003 M stage 1.358 0.701−2.632 0.364 PRR11 1.234 1.056−1.442 0.008 Table S3. Association between PRR11 expression and clinical characteristics using Logistic Regression
Clinical characteristics Total (N) Odds ratio (OR) P value Age (> 65 vs. ≤ 65) 520 0.819 (0.580−1.155) 0.255 Gender (Male vs. Female) 539 1.380 (0.982−1.938) 0.063 Pathologic stage (Stage II & Stage III & Stage IV vs. Stage I) 531 1.707 (1.208−2.412) 0.002 T stage (T2 & T3 & T4 vs. T1) 536 1.938 (1.343−2.798) < 0.001 N stage (N1 & N2 & N3 vs. N0) 523 1.836 (1.267−2.661) 0.001 M stage (M1 vs. M0) 390 1.508 (0.660−3.445) 0.330
doi: 10.3967/bes2023.111
Role of Prognostic Marker PRR11 in Immune Infiltration for Facilitating Lung Adenocarcinoma Progression
-
Abstract: The PRR11 gene (Proline Rich 11) has been implicated in lung cancer; however, relationship between PRR11 and immune infiltration is not clearly understood. In this study, we used The Cancer Genome Atlas (TCGA) data to analyze the lung adenocarcinoma patients; PRR11 gene expression, clinicopathological findings, enrichment, and immune infiltration were also studied. PRR11 immune response expression assays in lung adenocarcinoma (LUAD) were performed using TIMER, and statistical analysis and visualization were conducted using R software. All data were verified using Gene Expression Profiling Interactive Analysis (GEPIA), and the Human Protein Atlas (HPA). We found that PRR11 was an important prognostic factor in patients with LUAD. PRR11 expression was correlated with tumor stage and progression. Gene Set Enrichment Analysis (GSEA) showed that PRR11 was enriched in the cell cycle regulatory pathways. Immune infiltration analysis revealed that the number of T helper 2 (Th2) cells increased when PRR11 was overexpressed. These results confirm the role of PRR11 as a prognostic marker of lung adenocarcinoma by controlling the cell cycle and influencing the immune system to facilitate lung cancer progression.
-
Key words:
- Bioinformatics /
- Lung adenocarcinoma /
- PRR11 /
- Cell cycle /
- Th2 cell
&These authors contributed equally to this work.
注释:1) Conflicts of Interest: -
Figure 1. Expression and survival analysis of PRR11 in lung adenocarcinoma. (A) The expression of PRR11 in pan-cancer; (B) Differences in PRR11 expression between normal and LUAD tissues; (C) PRR11 expression and clinicopathological variables examined using Multivariate Cox regression; (D) Distribution of PRR11 expression and survival status; (E) An analysis of PRR11 in LUAD using ROC curve. (**, P < 0.01; ***, P < 0.001)
Figure 2. Analysis of PRR11 expression and clinicopathological factors, PRR11 enrichment analysis, and verification of data results. (A–C) PRR11 expression showed a significant correlation with histological pathologic grade (A), T stage (B), and N stage (C); (D–E) GO and KEGG enrichment pathway analysis; (F–G) The comparison of PRR11 expression levels and overall survival based on GEPIA data; (H) Immunohistochemical analysis of lung adenocarcinoma expression of the PRR11 protein was conducted using HPA. (**, P < 0.01; ***, P < 0.001)
Figure 3. Association between PRR11 and immune infiltration. (A) Relationship between PRR11 and immune cells in TIMER; (B) Correlation between the relative abundances of 24 immune cell types and PRR11 levels; (C) Differences between tumor samples with high and low PRR11 expression in Th2 and Th1 cell proportions; (D) Heatmap of 24 immune infiltration cells in LUAD samples. (***, P < 0.001)
S1. Correlation between overall survival (OS) and multivariable characteristics in TCGA-LUAD patients via Cox regression
ID HRs 95% CI P value Age 1.216 0.910–1.625 0.186 Gender 1.087 0.816–1.448 0.569 Pathologic stage 2.710 1.994–3.685 < 0.001 T stage 2.352 1.614–3.426 < 0.001 N stage 2.547 1.904–3.407 < 0.001 M stage 2.176 1.272–3.722 0.005 PRR11 1.268 1.117–1.441 < 0.001  下载: 导出CSV
下载: 导出CSV
S2. Correlation between overall survival (OS) and multivariable characteristics in TCGA-LUAD patients via a Multivariate survival model
ID HRs 95% CI P value Age 1.193 0.848−1.679 0.31 Gender 0.999 0.716−1.395 0.996 Pathologic stage 1.350 0.819−2.227 0.239 T stage 1.742 1.086−2.794 0.021 N stage 1.840 1.239−2.733 0.003 M stage 1.358 0.701−2.632 0.364 PRR11 1.234 1.056−1.442 0.008
下载: 导出CSV
S3. Association between PRR11 expression and clinical characteristics using Logistic Regression
Clinical characteristics Total (N) Odds ratio (OR) P value Age (> 65 vs. ≤ 65) 520 0.819 (0.580−1.155) 0.255 Gender (Male vs. Female) 539 1.380 (0.982−1.938) 0.063 Pathologic stage (Stage II & Stage III & Stage IV vs. Stage I) 531 1.707 (1.208−2.412) 0.002 T stage (T2 & T3 & T4 vs. T1) 536 1.938 (1.343−2.798) < 0.001 N stage (N1 & N2 & N3 vs. N0) 523 1.836 (1.267−2.661) 0.001 M stage (M1 vs. M0) 390 1.508 (0.660−3.445) 0.330
下载: 导出CSV
-
[1] Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin, 2021; 71, 209−49. doi: 10.3322/caac.21660 [2] Denisenko TV, Budkevich IN, Zhivotovsky B. Cell death-based treatment of lung adenocarcinoma. Cell Death Dis, 2018; 9, 117. doi: 10.1038/s41419-017-0063-y [3] Zhang L, Lei YL, Zhang Y, et al. Silencing of PRR11 suppresses cell proliferation and induces autophagy in NSCLC cells. Genes Dis, 2018; 5, 158−66. doi: 10.1016/j.gendis.2017.12.003 [4] Cao DD, Sha J, Cui R, et al. Advances in research of spreading through air spaces and the effects on the prognosis of lung cancer. Cancer Manag Res, 2019; 11, 9725−32. doi: 10.2147/CMAR.S232187 [5] Jonna S, Subramaniam DS. Molecular diagnostics and targeted therapies in non-small cell lung cancer (NSCLC): an update. Discov Med, 2019; 27, 167−70. [6] Huang YJ, Ni R, Wang J, et al. Knockdown of lncRNA DLX6-AS1 inhibits cell proliferation, migration and invasion while promotes apoptosis by downregulating PRR11 expression and upregulating miR-144 in non-small cell lung cancer. Biomed Pharmacother, 2019; 109, 1851−9. doi: 10.1016/j.biopha.2018.09.151 [7] Lee KM, Guerrero-Zotano AL, Servetto A, et al. Proline rich 11 ( PRR11) overexpression amplifies PI3K signaling and promotes antiestrogen resistance in breast cancer. Nat Commun, 2020; 11, 5488. doi: 10.1038/s41467-020-19291-x [8] Stefaniuk P, Szymczyk A, Podhorecka M. The Neutrophil to lymphocyte and lymphocyte to Monocyte ratios as new prognostic factors in hematological malignancies - a narrative review. Cancer Manag Res, 2020; 12, 2961−77. doi: 10.2147/CMAR.S245928 [9] Wei B, Li CS. Changes in Th1/Th2-producing cytokines during acute exacerbation chronic obstructive pulmonary disease. J Int Med Res, 2018; 46, 3890−902. doi: 10.1177/0300060518781642 [10] Wang XE, Wang YH, Zhou Q, et al. Immunomodulatory effect of Lentinan on aberrant T subsets and cytokines profile in non-small cell lung cancer patients. Pathol Oncol Res, 2020; 26, 499−505. doi: 10.1007/s12253-018-0545-y -
 23114+Supplementary Materials.pdf
23114+Supplementary Materials.pdf

-

 点击查看大图
点击查看大图
计量
- 文章访问数: 391
- HTML全文浏览量: 182
- PDF下载量: 38
- 被引次数: 0

 Quick Links
Quick Links