



-
Enteroviruses A–D (human enteroviruses A–D, HEVs), are members of the Enterovirus genus of the Picornaviridae (small RNA virus) family, and were historically classified into poliovirus (PV), echovirus (Echo), coxsackievirus group A and B (CVA and CVB), and new HEVs, divided into four species (enterovirus A–D) based on similarity of molecular genetics and phylogeny[1-3]. To date, a total of 116 HEV serotypes have been reported (see www.picornaviridae.com). It is known that the sequence of the VP1 capsid gene correlates with the serotype determined by genetic analysis. Partial VP1 genes are ideal molecular targets for rapid identification of clinical HEV serotypes, and complete VP1 genes are widely used in molecular epidemiology studies for tracking the genetic diversity of circulating HEVs[1,3,4]. However, the current recommended protocol of amplifying partial VP1 genes of HEVs from clinical samples is relatively complicated and cumbersome, although there is no universal protocol capable of amplifying complete VP1 genes of HEVs from clinical samples. This inconvenience has hindered routine HEV surveillance and molecular epidemiological investigation of enterovirus-related illness in clinical virology laboratories.
HEVs are common human pathogens that may cause a wide spectrum of clinical outcomes ranging from asymptomatic infection to hand, foot and mouth disease (HFMD), meningitis, acute flaccid paralysis, respiratory illness, and myocarditis. During the past decade, the pathogenic spectrum of HFMD worldwide has changed; typical EV-A71 or CVA16 infection-related HFMD cases are declining, while other human enteroviruses (termed as other HEVs, or non-EV-A71 non-CVA16 HEVs) including CVA6 and CVA10 now account for a considerable proportion of confirmed HFMD cases[5-7]. Additionally, HEV-infection associated diseases such as aseptic meningeal encephalitis has gradually increased[8,9]. In clinical virology laboratories, multiple commercial real-time RT-PCR kits are available for the detection of common HEV members such as EV-A71 and CVA16, but no real-time RT-PCR kits were developed for identifying or typing of other uncommon HEVs. To address this issue, several reverse transcription nested polymerase chain reaction (RT-nPCR) assays were established for amplifying and sequencing partial or complete VP1 genes of HEVs directly from clinical specimens in our laboratory, thus providing a satisfactory resolution for studying the pathogenic spectrum and molecular epidemiological characte-ristics of HFMD and other HEV-related diseases. Additionally, to verify the feasibility of use in clinical laboratories, hundreds of clinical specimens of HFMD linked to other HEVs were tested with this amplification protocol during recent HFMD surveillance seasons.
-
RT-nPCR primer sets from previous reports were selected and assembled to amplify partial VP1 genes of HEV A–C directly from clinical samples[10-12]. Genome sequences of three serotypes of HEV-D prototype strains were downloaded from GenBank (Accession numbers: NC_038308, DQ201177, and DQ916376) and aligned. The primers for the complete VP1 gene of HEV-D were designed by Prime 5.0 software (Premier, Palo Alto, CA, USA). The resulting sense primer targeted highly conserved regions between primer AMTH and upstream of the VP1-encoding sequence; the anti-sense primer was selected between primer GDCL and downstream of the VP1 gene. The sequences and other information of primers are shown in Table 1.
Primer Assay Sequence (5'–3') Location (nt) Reference strain sequence Source AMTH first RT-PCR GCIATGYTIGSIACICAYVT 2207–2226 PV1-Mahoney Bessaud et al.[10] GDCL first RT-PCR ARIABICCICCRCARTCICC 3723–3704 AN89 nPCR (partial VP1) CCAGCACTGACAGCAGYNGARAYNGG 2602–2627 Nix et al.[11] AN88 nPCR (partial VP1) TACTGGACCACCTGGNGGNAYRWACAT 2977–2951 486 nPCR (Enterovirus A1) TGGTAICARACIAAITWYGTIGTNCC 2297–2322 CVA2-Fleetwood Oberste et al.[12] 487 nPCR (Enterovirus A2) ATGTWYGYICCICCIGGIGCNCC 2894–2916 488 nPCR (Enterovirus A1) GTIGGRTAICCITCITARAACCAYTG 3063–3038 489 nPCR (Enterovirus A2) AYIGCICCISWITGYTGNCC 3348–3329 490 nPCR (Enterovirus B1) TGIGTIYTITGYRTICCITGGAT 2226–2248 E1-Farouk 491 nPCR (Enterovirus B2) ATGTAYRTICCICCIGGNGG 2883–2902 492 nPCR (Enterovirus B1) GGRTTIGTIGWYTGCCA 2953–2934 493 nPCR (Enterovirus B2) TCNACIANICCIGGICCYTC 3541–3522 494 nPCR (Enterovirus C1) GAYGAYWSITTIACIGAIGGNGG 2306–2328 PV1-Mahoney 495 nPCR (Enterovirus C2) ATGTAYRTICCICCIGGIGCNCC 2951–2973 496 nPCR (Enterovirus C1) CCRTCITARAARTGISIRTANGC 3111–3089 497 nPCR (Enterovirus C2) GCITTITTITGRTGICCRAANCC 3408–3386 498 nPCR (Enterovirus D) GCHAARKCMAYMAATGCWAATGT 2227–2249 EV-D68-Fermon This study 499 nPCR (Enterovirus D) TCTGATTGCCARTCHACATA 3422–3403 Table 1. Primers for amplifying and sequencing of partial and complete VP1 genes of HEVs in clinical specimens
-
Viral RNA was extracted using a QIAamp Viral RNA Mini Kit (Qiagen, Hilden, Germany) in accordance with the manufacturer’s instructions. Total RNA (50 μL) was eluted from 140 μL of throat swab, cell supernatant, and other specimens and then stored at –80 °C.
-
The partial VP1 gene of HEVs was amplified by RT-nPCR methods, consisting of a first RT-PCR step with the outer primers and a second-round PCR with the inner primers. The first RT-PCR step used the Access One Step RT-PCR Kit (Promega, Madison, USA) with primer pairs of AMTH and GDCL. The first RT-PCR was carried out in a 50-μL reaction mixture containing 8 μL of viral RNA, 10 μL of AMV/Tfl 5× Reaction Buffer, 1 μL of dNTP Mix (10 mmol/L each dNTP), 50 pmol of outer primers AMTH and GDCL, 2 μL of 25 mmol/L MgSO4, 1 μL of each of AMV Reverse Transcriptase (5 U/µL) and Tfl DNA Polymerase (5 U/µL). The reaction conditions were: reverse transcription at 45 °C for 45 min, denaturing at 94 °C for 2 min; 40 cycles of thermocycling at 94 °C for 30 s, 45 °C for 30 s, 68 °C for 2 min; and a final incubation step at 68 °C for 10 min.
The second-round PCR (final volume, 50 μL) used the Ex-Taq polymerase of Takara Company (Takara, Dalian, China), consisting of 1 μL of the first-round RT-PCR reaction, 5 μL of 10 × Ex Taq Buffer (Mg2+ plus) (20 mmol/L), 4 μL of dNTP Mixture (2.5 mmol/L each dNTP), 50 pmol of each primer, 0.25 μL of TaKaRa Ex Taq (5 U/μL). The inner primers AN88 and AN89 were used to amplify partial VP1 genes, the reaction conditions consisted of 95 °C for 2 min; 40 cycles of 94 °C for 30 s, 55 °C for 30 s, 72 °C for 40 s; and 72 °C for 10 min.
The PCR products were initially analyzed by 1.5% agarose gel electrophoresis. Positive amplicons with expected size were recovered from the gel, purified using a QIAquick gel extraction kit (Qiagen, Hilden, Germany) and sequenced by an ABI 3500 automated sequencer (Applied Biosystems, Foster City, CA, USA) using the inner primer AN88 and AN89. Viral serotypes were determined using an online typing tool[13] (
http://www.rivm.nl/mpf/enterovirus/typingtool ), based on partial VP1 sequences of approximately 350 bp in size. -
The complete VP1 gene of HEVs was also amplified by RT-nPCR methods, consisting of a first RT-PCR step with the outer primers and a second-round PCR with the inner primers. RT-nPCR of the complete VP1 gene was identical in the first RT-PCR step with RT-nPCR of partial VP1 gene, using the Access One Step RT-PCR Kit (Promega, Madison, USA) with primer pairs of AMTH and GDCL.
The second-round PCR of complete VP1 gene used the same kit as in the second-round PCR of partial VP1 gene. The amplification of complete VP1 genes was performed in several species-specific assays for HEV A–D. The species-specific reactions for VP1 genes of HEV A–C used previously reported primers (486/488 and 487/489, 490/492 and 491/493, and 494/496 and 495/497) were incubated at 95 °C for 2 min; 40 cycles of 94 °C for 30 s, 50 °C for 30 s, 72 °C for 1 min; and 72 °C for 10 min. Similarly, the complete VP1 gene of HEV-D was amplified by in-house designed primers (498 and 499), and the reaction parameters were: 95 °C for 2 min; 40 cycles of 94 °C for 30 s, 50 °C for 30 s, 72 °C for 1 min 20 s; and 72 °C for 10 min.
PCR positive products were gel extracted and sequenced with the second-round PCR primers as described previously in RT-nPCR of the partial VP1 gene. The complete VP1 sequences of HEV A–C were then assembled with SeqMan software (DNASTAR, Madison, USA) using the two spliced VP1 regions, along with the complete VP1 sequence of HEV-D, for further molecular epidemiological study of HEVs.
-
The sensitivity of the RT-PCR assay was tested by using isolates of EV-A71 and CVA6 as representative strains for HEV-A, CVB3 for HEV-B, CVA21 for HEV-C, and EV-D68 for HEV-D. The EV-A71 strain (FY17.08-4/AH/CHN/2008, GenBank: JX678875) was obtained from the World Health Organization WPRO Regional Polio Reference Laboratory, National Institute for Viral Disease Control and Prevention, Chinese Center for Disease Control and Prevention. The other four strains of CVA6 (2012FJFZ655), CVB3 (2012FJZZ015), CVA21 (2013FJPTN012), and EV-D68 (2014FJQZ344) were isolated from our laboratory and confirmed by sequencing of the VP1 gene and the whole genome. Titers of these virus stocks expressed as CCID50 per μL were determined according to the standard protocol[14]. The virus copy number quantification of these virus stocks expressed as copies per μL was obtained by Shanghai Sangon Biotech using the Bio-Rad QX200 Droplet Digital PCR System. Two serial 10-fold dilutions of these strains were prepared in Maintenance Media (Life, NY, USA) from 100 CCID50 per μL to 0.01 CCID50 per μL and from 103 copies per μL to 0.1 copies per μL. Viral RNA was extracted in 140 μL aliquot of each dilution using the aforementioned kit.
-
As a routine surveillance step for HFMD, clinical specimens were collected and screened by local Center for Disease Control and Prevention (CDC) laboratories in Fujian province, to confirm enterovirus infection and typing for common serotypes of CA16 and EV-A71, using commercial real-time RT-PCR kits (Jiangsu Bioperfectus Technologies, China; Shanghai ZJ Bio-Tech, China). Any enterovirus (+) EV-A71 (-) CVA16 (-) specimen is defined as uncharacterized and transferred to our laboratory for further typing. During recent HFMD surveillance seasons from 2011 to 2018, a total of 909 clinical specimens, mainly throat swabs suspected of infection with HFMD associated other HEVs (non-EV-A71 and non-CVA16 EVs), were collected for molecular typing with the RT-nPCR assay by amplifying and sequencing partial VP1 genes of HEVs. Several serotyped clinical specimens were tested with our RT-PCR assay to amplify and sequence the complete VP1 genes of HEV A–D, according to the patient’s onset time and geographic distribution of each serotype.
-
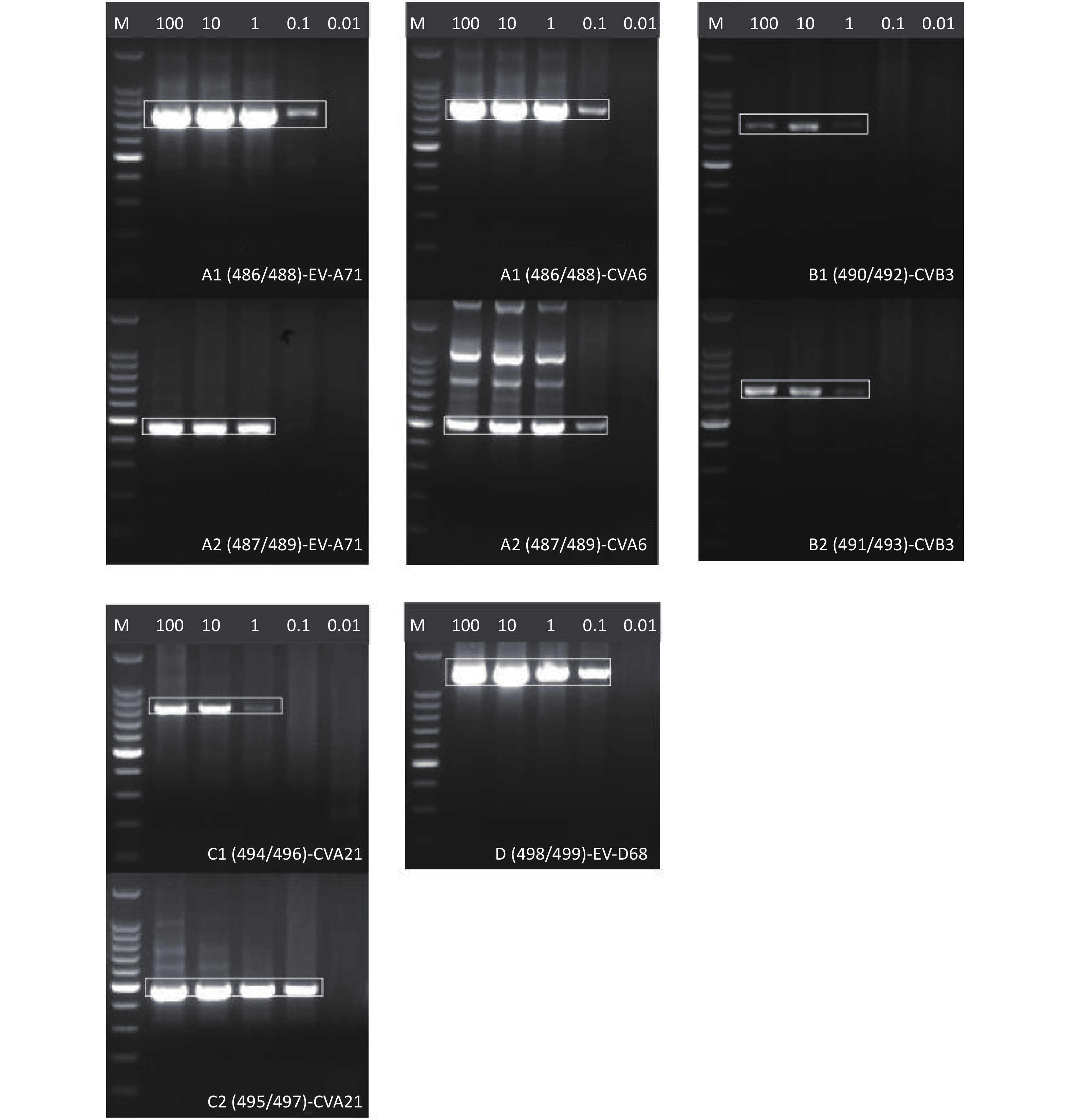
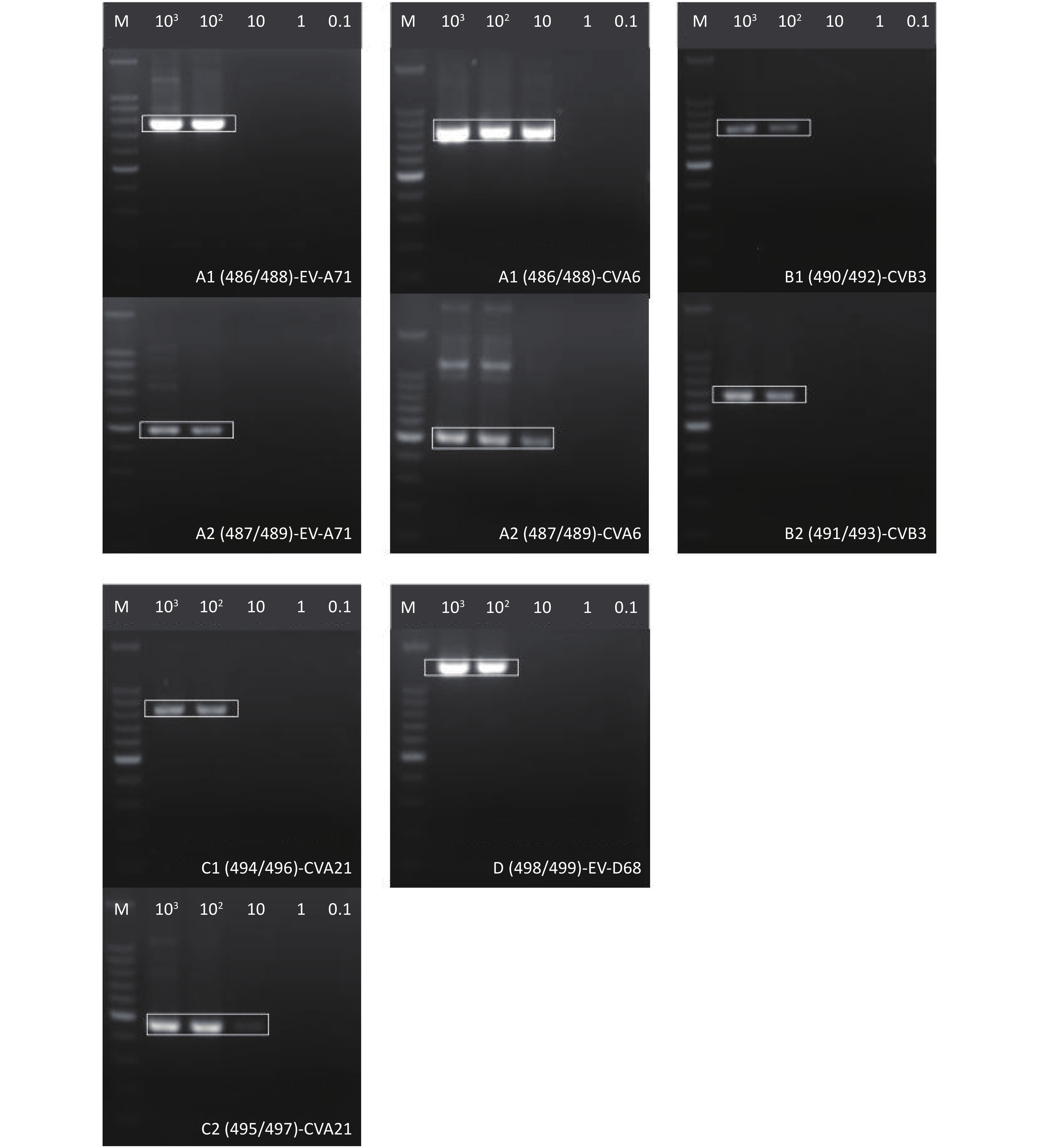
To evaluate the RT-PCR assay sensitivity of this combined RT-nPCR system for amplification of partial VP1 genes in HEVs, five virus stocks (i.e., EV-A71 and CVA6 of HEV-A, CVB3 of HEV-B, CVA21 of HEV-C, and EV-D68 of HEV-D) were prepared and serially 10-fold diluted from 100 CCID50 per μL to 0.01 CCID50 per μL and from 103 copies per μL to 0.1 copies per μL. Viral RNA extracted from each diluted virus stock were used as templates in these assays. As indicated in Figure 1 and Figure 2, clear bands of approximately 350 bp in size were visualized on 1.5% agarose gels, each serotype was verified by subsequent sequencing of these amplicons; therefore, the detection limits for the above five serotypes in the partial VP1 amplification assay were 0.1 CCID50 per μL and 10 copies per μL (Table 2).
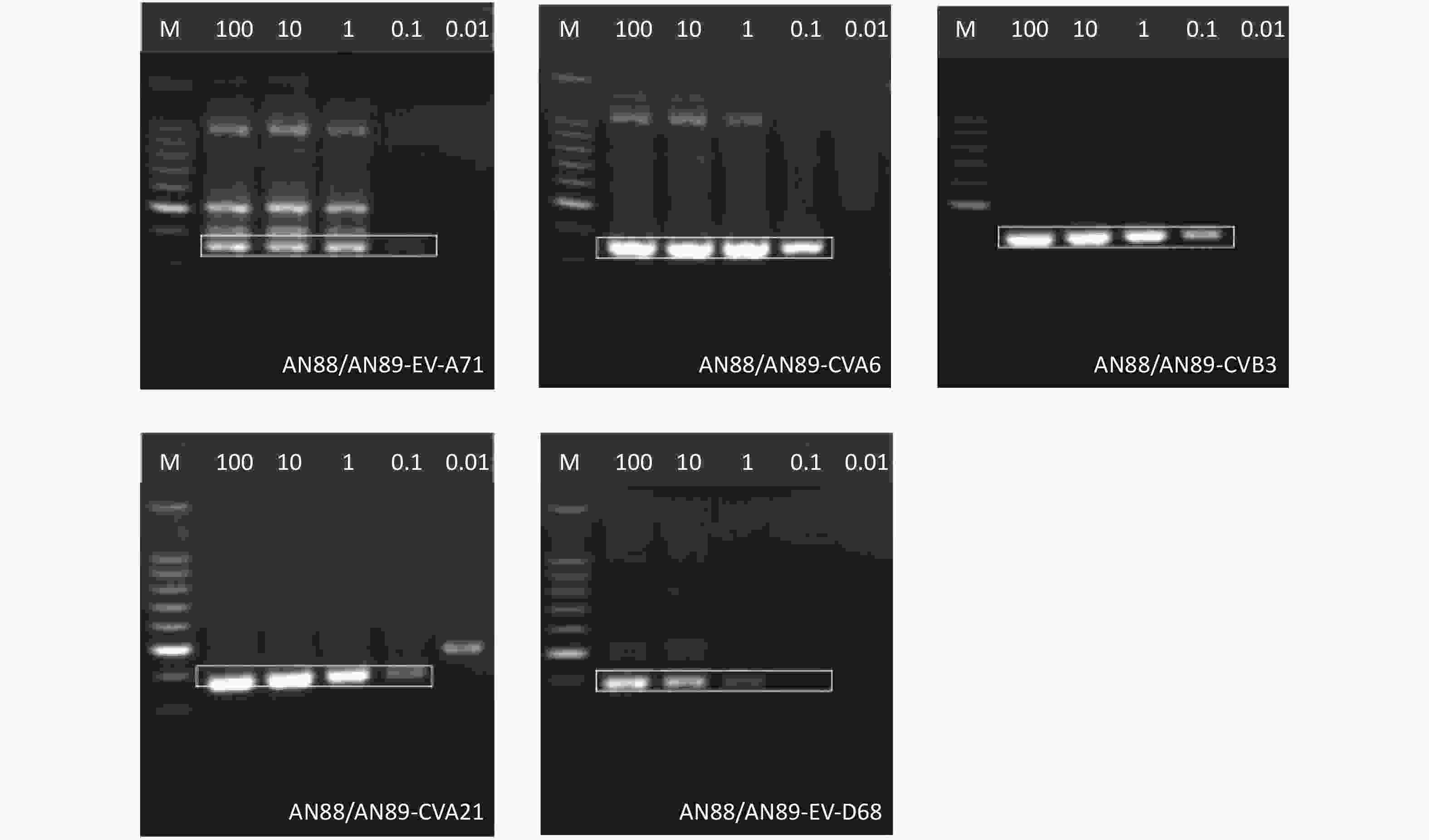
Figure 1. Agarose gel electrophoresis of partial VP1 genes of representative HEV strains. Lane 100–0.01: serially diluted titers of the virus stock (CCID50/μL). M: 100 bp DNA ladder marker. Amplicons are shown in white boxes.
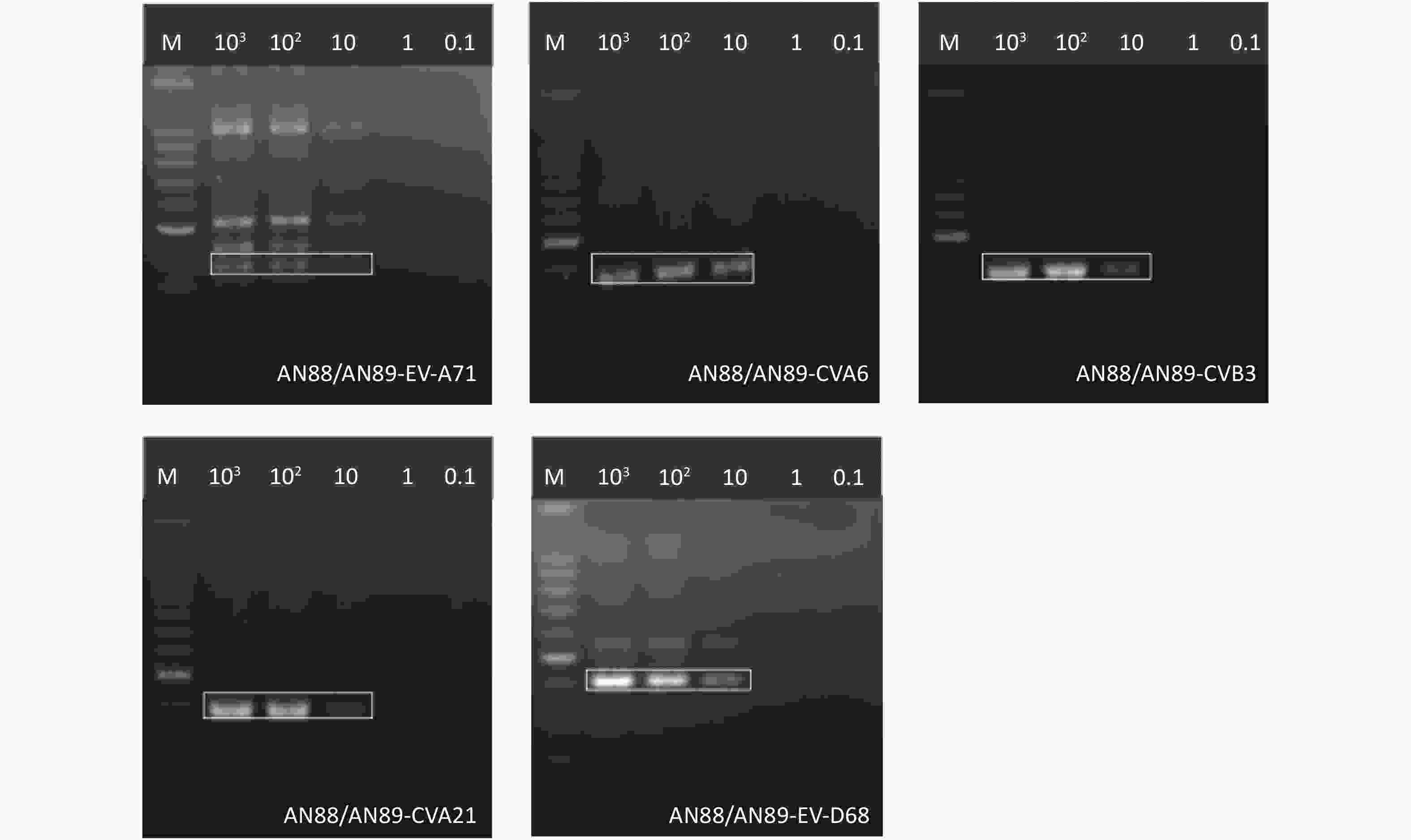
Figure 2. Agarose gel electrophoresis of partial VP1 genes of representative HEV strains. Lane 103–0.1: serially diluted titers of the virus stock (copies/μL). M: 100 bp DNA ladder marker. Amplicons are shown in white boxes.
HEVs CCID50/μL Copies/μL Partial VP1 Full-length VP1 Split VP1 Partial VP1 Full-length VP1 Split VP1 HEV-A (EV-A71) 0.1 1 0.1 (A1), 1 (A2) 10 100 100 (A1), 100 (A2) HEV-A (CVA6) 0.1 0.1 0.1 (A1), 0.1 (A2) 10 10 10 (A1), 10 (A2) HEV-B (CVB3) 0.1 1 1 (B1), 1 (B2) 10 100 100 (B1), 100 (B2) HEV-C (CVA21) 0.1 1 1 (C1), 0.1 (C2) 10 100 100 (C1), 10 (C2) HEV-D (EV-D68) 0.1 0.1 − 10 100 − Table 2. The detection limit of the RT-nPCR system in amplification of the VP1 gene of HEVs
-
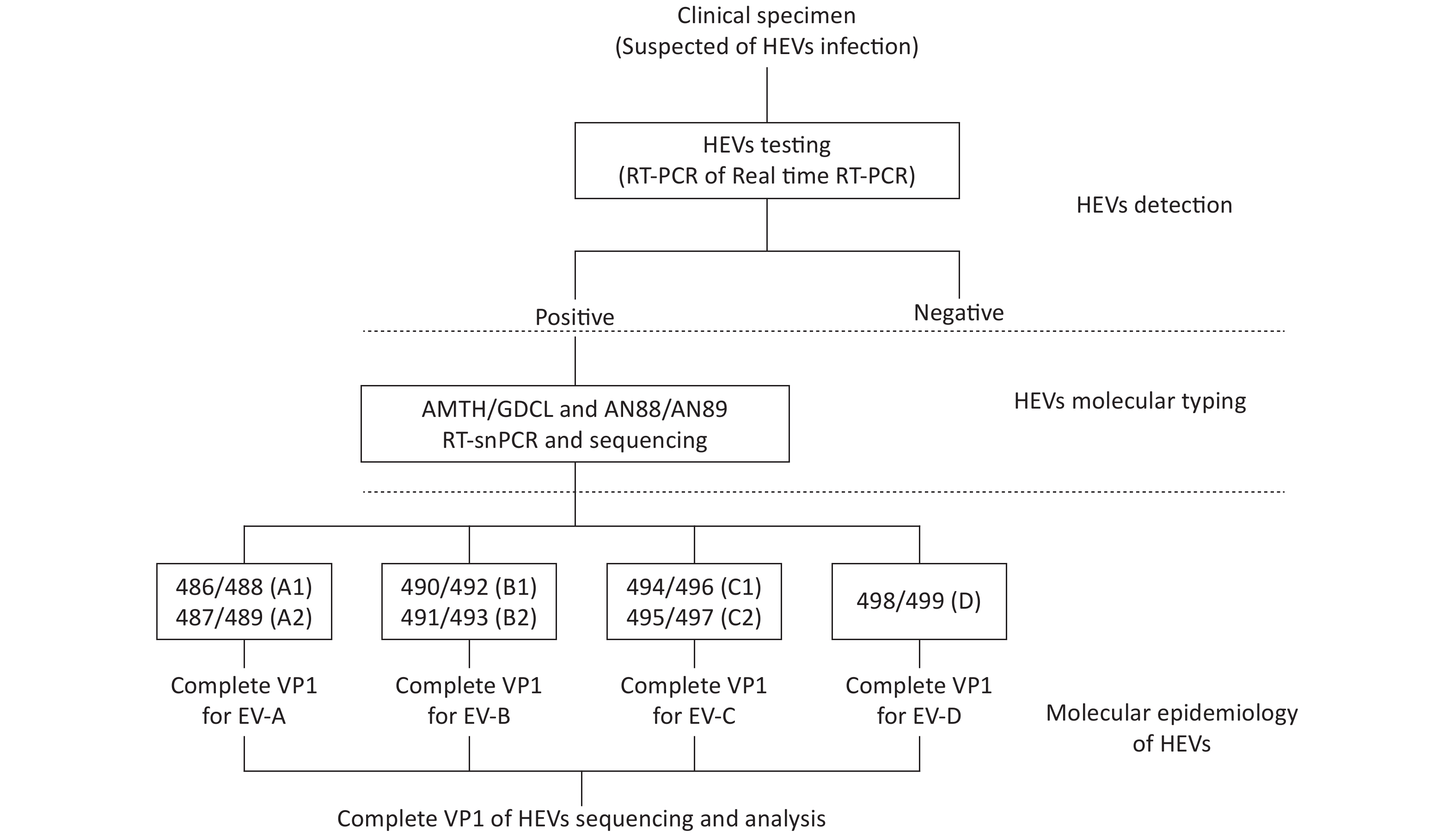
The sensitivity of this RT-nPCR system for complete VP1 gene amplification of HEVs was evaluated, as shown in Figures 3–4, and Table 2. For example, the detection limit for EV-A71 was 1 CCID50 per 1 μL and 100 copies per μL, whereas that for EV-A71-A1 was 0.1 CCID50 per μL and 100 copies per μL, and for EV-A71-A2 the limit was 1 CCID50 per 1 μL and 100 copies per μL. Therefore, the complete VP1 RT-nPCR assay detected RNA extracted from as little as 1 CCID50 per μL and 100 copies per μL for the above five serotypes stocks.
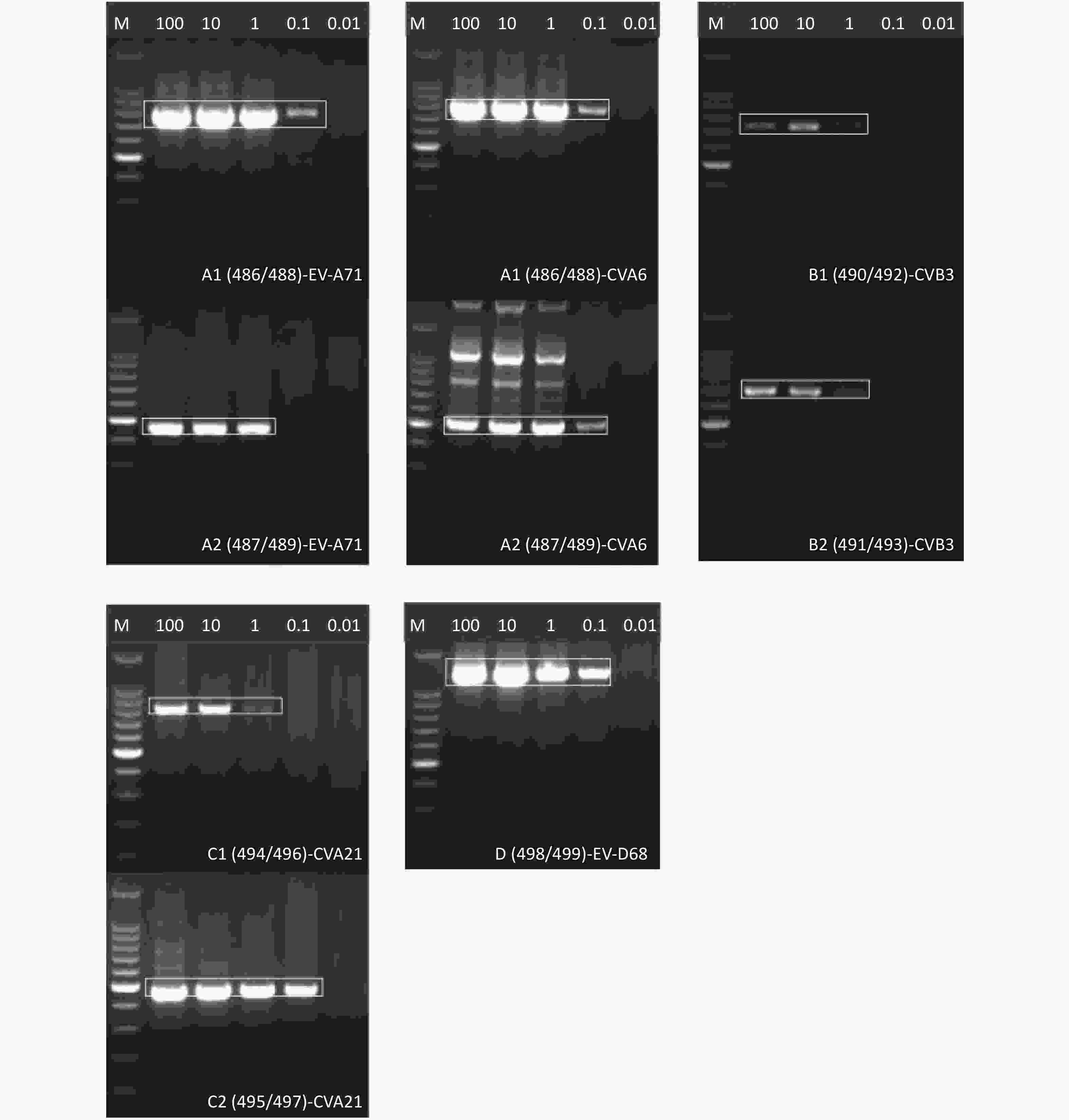
Figure 3. Agarose gel electrophoresis of complete VP1 fragments of representative HEV strains. Lane 100–0.01: serially diluted titers of the virus stock (CCID50/μL). M: 100 bp DNA ladder marker. Amplicons are shown in white boxes.

Figure 4. Agarose gel electrophoresis of complete VP1 fragments of representative HEV strains. Lane 103–0.1: serially diluted titers of the virus stock (copies/μL). M: 100 bp DNA ladder marker. Amplicons are shown in white boxes.
-
The RT-nPCR strategy for amplification of the partial and complete VP1 genes of HEVs contains two steps, a first RT-PCR step with the Access One Step RT-PCR Kit (Promega, Madison, USA) and a second-round PCR with the Ex-Taq polymerase of Takara Company (Takara, Dalian, China). In the first RT-PCR step, primers AMTH and GDCL[10] were involved; primers AN88 and AN89[11] were then used in the second-round PCR for partial VP1 genes. For full-length VP1 genes, the in-house designed primers 498 and 499 were prepared for HEV-D in the second-round PCR; notably, the VP1 genes of HEVs A–C were predicted in two fragments by two pairs of primers, namely 486/488 (A1) and 487/489 (A2), 490/492 (B1) and 491/493 (B2), and 494/496 (C1) and 495/497 (C2), respectively[12].
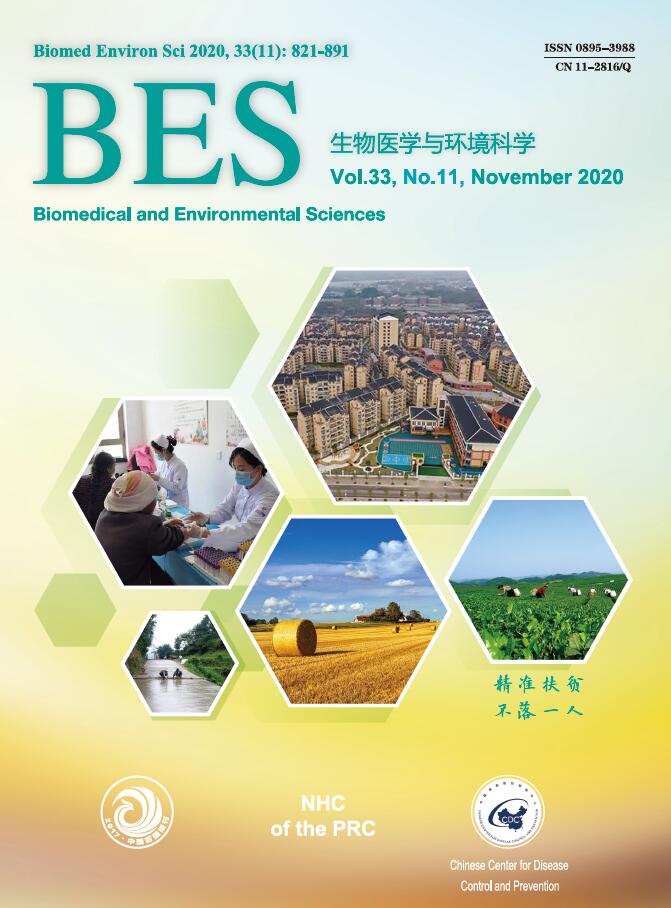
The RT-PCR assay established in this study was capable of amplifying partial and complete VP1 genes of HEVs in clinical samples and provided a satisfactory resolution for molecular typing and molecular epidemiology of HEVs. The routine workflow of HEV molecular typing and molecular epidemiology investigation was proposed in our laboratory as shown in Figure 5 and consists of three steps: detecting enterovirus; typing HEVs with the RT-PCR assay and sequencing of partial VP1; and molecular epidemiology of HEVs using species-specific RT-PCR assays and sequencing of complete VP1 based on HEV serotypes.
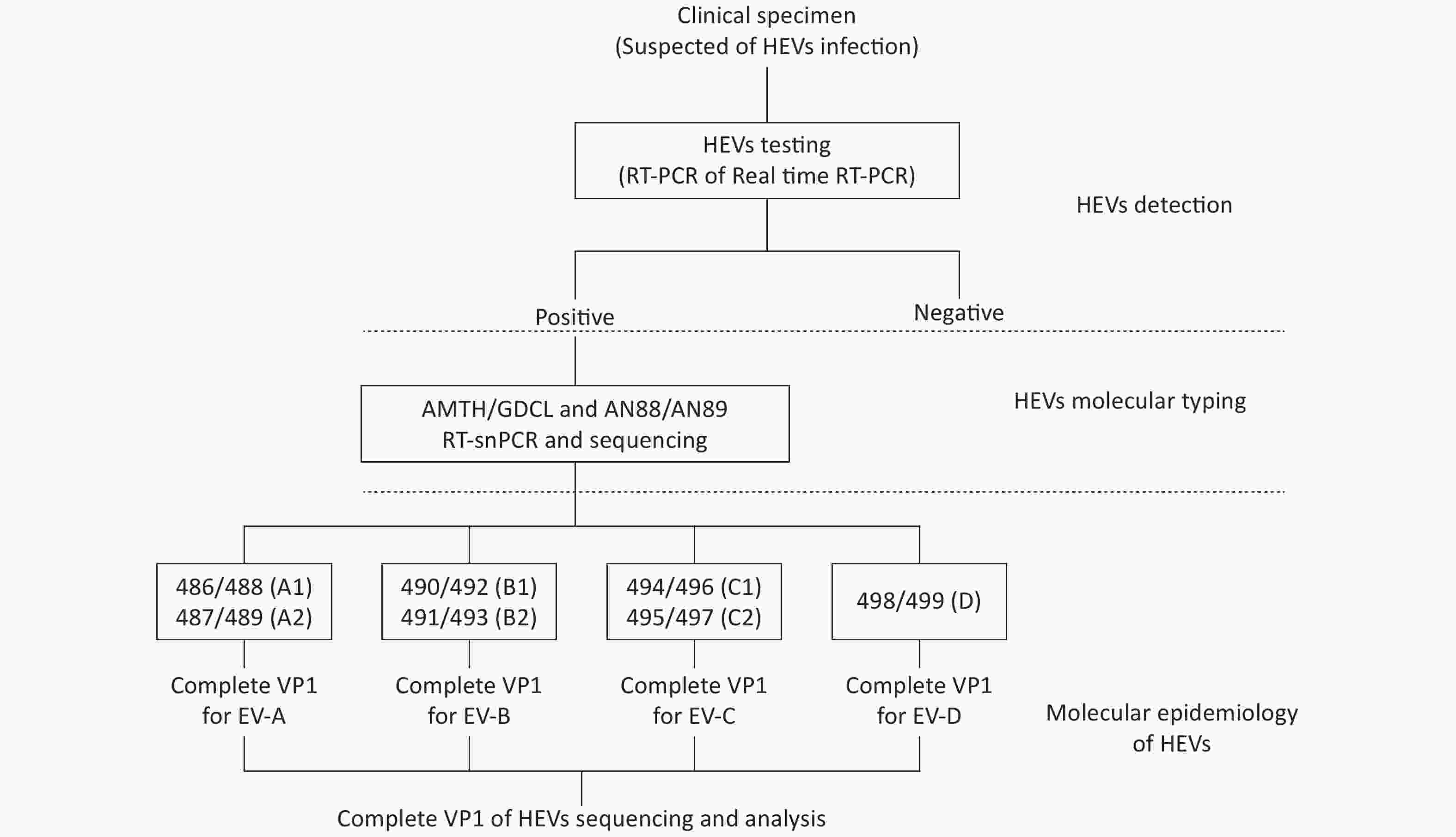
Figure 5. Workflow of HEV typing and molecular epidemiology from clinical specimens.
-
While this RT-nPCR system was established and its sensitivity was confirmed, we performed HEV identification, molecular typing, and molecular epidemiology investigation with this strategy in routine HFMD surveillance from clinical samples in our laboratory. During surveillance seasons from 2011 to 2018, a total of 909 clinical specimens suspected of other HEV infection were collected from HFMD patients in Fujian province, China. The majority of specimens, 858 (94.4%) were positive for HEV molecular typing, consisting of 25 serotypes on the basis of this typing strategy. Notably, seven serotypes of HEV-A and 15 serotypes of HEV-B were detected, while EV-D68 was the only member from HEV-D, and another two HEV-C serotypes, CVA21 and CVA24, were identified (Table 3). Depending on the patient’s onset time and geographic distribution of each serotype, several serotyped clinical specimens were tested for the complete VP1 sequences of HEV A–D with our RT-PCR assay. Except for one E5 strain and another CVA24 strain, complete VP1 sequences of the other 23 serotypes were successfully obtained with this RT-nPCR protocol. The entire VP1 sequences are applicable to molecular epidemiological studies of HEVs[7,15-17], including inter-species single nucleotide polymorphism, evolutionary dynamics study, and phylogenetic analysis.
Species Serotype Number of positive
specimens (%)Number of specimens with
entire VP1 sequencesGenBank accession No. A CVA2 17 (1.98) 15 − A CVA4 49 (5.71) 33 − A CVA5 8 (0.93) 8 − A CVA6 674 (78.55) 154 KJ743208–KJ743243 A CVA8 3 (0.35) 3 − A CVA10 75 (8.74) 51 − A CVA12 2 (0.23) 2 − B CVA9 2 (0.23) 2 MG922503, MG922507 B CVB1 1 (0.12) 1 MG922510 B CVB2 1 (0.12) 1 MG922511 B CVB3 4 (0.47) 4 MG922515–MG922518 B CVB4 2 (0.23) 2 MG922522, MG922523 B CVB5 3 (0.35) 3 MG922527–MG922529 B E3 1 (0.12) 1 MG922530 B E5 1 (0.12) − − B E6 2 (0.23) 2 MG922532, MG922534 B E7 1 (0.12) 1 MG922535 B E9 3 (0.35) 3 MG922544–MG922546 B E11 2 (0.23) 1 MG922543 B E16 1 (0.12) 1 MG922536 B E25 1 (0.12) 1 MG922538 B E30 2 (0.23) 2 MG922540, MG922542 C CVA21 1 (0.12) 1 − C CVA24 1 (0.12) − − D EV-D68 1 (0.12) 1 − Table 3. Summary of other HEV serotypes identified by the RT-nPCR system from clinical specimens of HFMD patients
-
Genomic analysis has revealed that the 5’ non-translated region (5’-UTR) of enteroviruses are highly conserved. Consequently, a wide range of RT-PCR assays have been developed to target this region for detection of enteroviruses in clinical specimens[4,11]. However, owing to the degree of conservation in the 5’-UTR, such assays are not suitable for typing of enterovirus groups with more than 100 members. A number of important serotype-specific neutralization epitopes reside in the VP1 region of enterovirus, and therefore it is widely accepted that the partial or complete VP1 sequence correlates well with its serotype. Hence, amplification of partial or complete VP1 sequences has been gradually employed in enterovirus typing and molecular epidemiology of enteroviral disease outbreaks[1,3,4,18].
Human enterovirus typing by RT-PCR and amplicon sequencing targeting partial VP1 genes has been continuously improved and optimized[4, 19] since Oberste et al. proposed the application of the VP1 gene nucleotide sequences for molecular identification of HEVs[3]. Due to the low virus loads in original clinical specimens, Nix et al.[11] developed a nested PCR method for the detection and identification of HEVs. Other researchers, such as Iturriza-Go´mara[20], have also established methods of RT-PCR and DNA sequencing for molecular typing HEVs from original clinical samples. At present, the method established by Nix et al. is recommended in routine HEV surveillance by the World Health Organization and the Center for Disease Control and Prevention, USA. In that protocol, degenerate primer sets 222/224 and AN88/AN89 were selected as the primers for the first step RT-PCR and the second PCR, respectively. In the first step RT-PCR, the reverse transcription step and the PCR amplification step are performed separately, additionally, cDNA primers (primers AN32, AN33, AN34, and AN35) need to be added to the RT reaction mixture. Thus, the method is relatively complex and cumbersome. However, the new RT-nPCR assay described in this report uses degenerate primer sets AMTH/GDCL and AN88/AN89 as the primers for the first step RT-PCR and the second PCR step, respectively, to develop the nested PCR method for partial VP1-based molecular typing of HEVs directly from clinical specimens. Unlike the protocol of Nix et al, the first RT-PCR step in our study is a one-step approach with the primers AMTH/GDCL, and hence, it is simple to carry out, improves work efficiency, and reduces cross contamination.
Prior to this study, a strategy of amplifying full VP1 genes of HEV A–D directly from clinical samples has not been reported, although most of the primer sets were designed a decade ago. This innovative combination of RT-nPCR assays resolved the problem of obtaining complete VP1 sequences of HEVs from original clinical specimens, rather than cultured virus isolates, and would thus reduce the virus isolation workload, improve work efficiency, and save manpower, material, and financial resources. Notably, this RT-nPCR system can amplify partial VP1 or complete VP1 fragments in the first-round RT-PCR amplification with the degenerate primers, AMTH/GDCL. The amplicon of the first RT-PCR, of approximately 1,500 bp in size, acts as a common template for the second-round PCR amplification. Although these degenerate, inosine-containing primers may yield non-specific amplification, our data showed that the detection limits of this system for amplifying the partial VP1 gene of HEVs were 0.1 CCID50 per μL and 10 virus copies per μL and for the complete VP1 gene were 1 CCID50 per μL and 100 virus copies per μL. These detection limits were promising in routine HEV surveillance of clinical specimens: A 94.4% positive rate from molecular typing of 25 serotypes of HEV was demonstrated, and the complete VP1 sequences of 23 serotypes during the 2011 to 2018 HFMD surveillance seasons were obtained in our laboratory. Therefore, these data were sufficient to prove the feasibility of this novel system in clinical virology laboratories.
Among the 116 serotypes of HEVs reported thus far, which induce a wide variety of clinical illnesses, the pathogen spectrum of HFMD has changed dramatically during the past decade in mainland China and other countries. Although the proportion of other enteroviruses (non-EV-A71 non-CVA16 enteroviruses) in the pathogenic profile of HFMD has increased significantly, the proportion for traditional HFMD pathogens such as EV-A71 and CVA16 has declined. To reveal the ongoing etiological spectrum of HFMD, it is undoubtedly ideal to precisely identify putative serotypes and genotypes of circulating HFMD-associated HEVs, regardless of the relatively complicated and cumbersome protocols required to amplify partial VP1 genes and the lack of reliable protocols to amplify complete VP1 genes from clinical samples. Therefore, the RT-nPCR methods for amplifying partial and complete VP1 genes of HEVs from clinical specimens developed in this study provide a satisfactory resolution for studying the pathogenic spectrum and molecular epidemiological characteristics of HFMD and other HEVs-related diseases.
-
Not applicable.
-
The authors declare that they have no competing interests.
-
We are grateful to the National HFMD Laboratory Monitoring Network of China and especially to laboratory staff from local CDCs in Fujian province. Without their efforts, this study would not have been possible.
Funds:
This study was supported by National Science and Technology Major Projects [No. 2017ZX10104001 and No. 2017ZX10103008] and Fujian Provincial Natural Science Foundation [No. 2016J01350]

 Quick Links
Quick Links
 DownLoad:
DownLoad: