
-
The Global Burden of Disease (GBD) study defines lower respiratory infections (LRIs) as clinically diagnosed pneumonia or bronchitis. According to the 2021 World Health Organization’s “Global Health Estimates Report,” respiratory infections are the fifth leading cause of death globally, aside from COVID-19, which is the leading cause of death from infectious diseases[1]. The GBD study estimates that in 2021 there were 344 million (95% CI: 325 million to 364 million) new cases of LRIs worldwide, with 2.18 million (95% CI: 1.98 million to 2.36 million) deaths. LRIs are a major cause of death in children under 5 years of age and adults over 70[2].
The mortality rate of respiratory infections increases significantly with age. Globally, approximately 3 million people die from pneumonia and influenza each year, with the majority being the elderly[3]. Data from Germany show that the in-hospital mortality rate for pneumonia increased from 1.2% in those aged 18–50 to 9.57% in those aged 60–70, and to 25.45% in those aged 90 years and above[4]. Multiple studies in China have indicated that over 80% of influenza-related deaths occur in the elderly (aged 65 and older[5-7].
Lower respiratory infections represent a significant public health issue in China, with risk factors such as environmental particulate pollution, smoking, and alcohol consumption being prevalent[8]. From 2014 to 2017, the national average concentrations of PM2.5 and PM10 in China were 50 μg/m³ and 89 μg/m³, respectively[9]. In 2018, 26.6% of the population aged > 15 were smokers[10]. In 2016, the proportion of current drinkers was 48% among men and 16% among women[11]. Additionally, the novel coronavirus pandemic at the end of 2019 has introduced new challenges. Therefore, the prevention and control of lower respiratory tract infections should be considered. However, few studies on the burden of lower respiratory tract infections in China exist, with most focusing on young children, neglecting the significant burden on the elderly population. The new challenges posed by the coronavirus disease (COVID-19) pandemic further highlight the need for ongoing attention to the prevention and control of lower respiratory tract infections.
The Institute for Health Metrics and Evaluation (IHME) Global Burden of Disease (GBD) study sources its data primarily through global literature reviews and relevant monitoring data, thereby providing detailed forecasts of global disease burdens[12]. Analyzing GBD predictions for lower respiratory tract infections among older adults 70 and older in China can determine the severity of the burden on the elderly population, understand disease trends, and identify possible prevention and control strategies. This is crucial for the rational allocation of health resources and the optimization of medical service distribution, offering crucial scientific evidence for future health policy development.
-
Using the Global Burden of Disease (GBD) Prediction Tool (2021), data were collected on the mortality rates of lower respiratory infections (LRI) per 100,000 people aged 70 and older in G20 countries and globally from 1990 to 2050. Additionally, data were gathered on the number of LRI deaths, mortality rates (per 100,000), Years of Life Lost (YLLs) rates (per 100,000), Years Lived with Disability (YLDs) rates (per 100,000), and disability-adjusted life year (DALYs) rates (per 100,000) in China, segmented by age group and sex.
GBD 2021 collects data from all vital registration systems, monitoring systems, and verbal autopsies; checks for and excludes outliers from data across countries or regions; and then inputs cause-of-death data into the cause-of-death ensemble model (CODEm) to estimate LRI mortality rates. The detailed methods have been described in previous studies. CODEm is a Bayesian hierarchical spatio-temporal ensemble model. The estimates were then adjusted using CodCorrect to ensure consistency and interpretability of the GBD estimates for specific causes of death[13].
Based on GBD 2021, GBD predicts the disease burden for specific causes from 1990 to 2050, including death, life expectancy, Years of YLLs, YLDs, and DALYs. The GBD uses a cohort-specific age model to derive the implicit age-specific fertility rate (ASFR), applies a decay function to forecast the future GDP of each country and region, and predicts the per capita lagged distribution income (LDI). It also standardizes education levels to obtain sociodemographic index (SDI) predictions for specific locations. Subsequently, the GBD employed a mixed-effects model to simulate mortality rates for specific diseases, using SDI and time as covariates. The model included the combined effects of various risk factors as adjustments to predict the mortality rates for different diseases. At the all-cause mortality level, an autoregressive integrated moving average model (including drift and decay) was used to capture unexplained variability. Predictions of specific causes were further constrained by the all-cause mortality forecast based on the GBD hierarchy, ensuring a reliable estimation of cause-specific mortality rates. At the all-cause mortality level, an autoregressive integrated moving average model (including drift and decay) was used to capture unexplained variation. Predictions of specific causes were further constrained by all-cause mortality forecasts within the GBD disease hierarchy to ensure reliable estimates of disease-specific mortality rates. For non-fatal indicators, GBD uses SDI as the main covariate in mixed-effects models to predict incidence and prevalence and calculates YLDs based on prevalence and the average disability weights from GBD. Due to the limited time-series data, the GBD used a 10-year holdout period to evaluate the model. The squared error between the observed and predicted values for each cause-gender-region-year was calculated and the errors were winsorized at the 95%. GBD then calculated the root mean square error (RMSE) by taking the square root of the average of the winsorized squared errors and used this to assess the model. GBD also predicts the burden of lower respiratory tract infections under different scenarios, which arise from various sets of risk factors: environmental risks (safe environment scenario), risks related to infectious diseases, maternal and child diseases, neonatal and nutritional conditions (improved child nutrition and vaccination scenario), risks related to major noncommunicable diseases (improved behavioral and metabolic risk scenario), and the combined effects of these three scenarios[12]. Using the GBD prediction tool, you can obtain data on the burden of lower respiratory infections in China from 1990 to 2050. This tool allows for selecting data subsets for different age groups and sexes.
-
Use the relative changes in LRI deaths from 1990- 2050 to describe the trend in the number of deaths from lower respiratory infections among elderly aged 70 and over in China, which were defined as Percentage change = $ \dfrac{{{\text{Deaths2050 - Deaths1990}}}}{{{\text{Deaths1990}}}} $ × 100%. The annual percentage change (EAPC) was used to describe the temporal trend in mortality rates from 1990 to 2050 for this age group[14,15]. A linear regression model is used to describe the relationship between time and the natural logarithm of mortality rates, $ Y = \alpha + \beta {\text{x}} + \varepsilon $, where y is the natural logarithm of the mortality rate, x is the year, and ε is the error term. $ EAPC = 100 \times \left[ {{\text{exp}}\left( \beta \right) - 1} \right] $95% confidence intervals (CI) are obtained from the regression model. If both the EAPC value and the lower bound of the CI are positive, it indicates an increasing mortality trend. Conversely, if both the EAPC value and the upper bound of the CI were negative, a decreasing mortality trend was indicated. All statistical analyses were performed using R version 4.4.1.
-
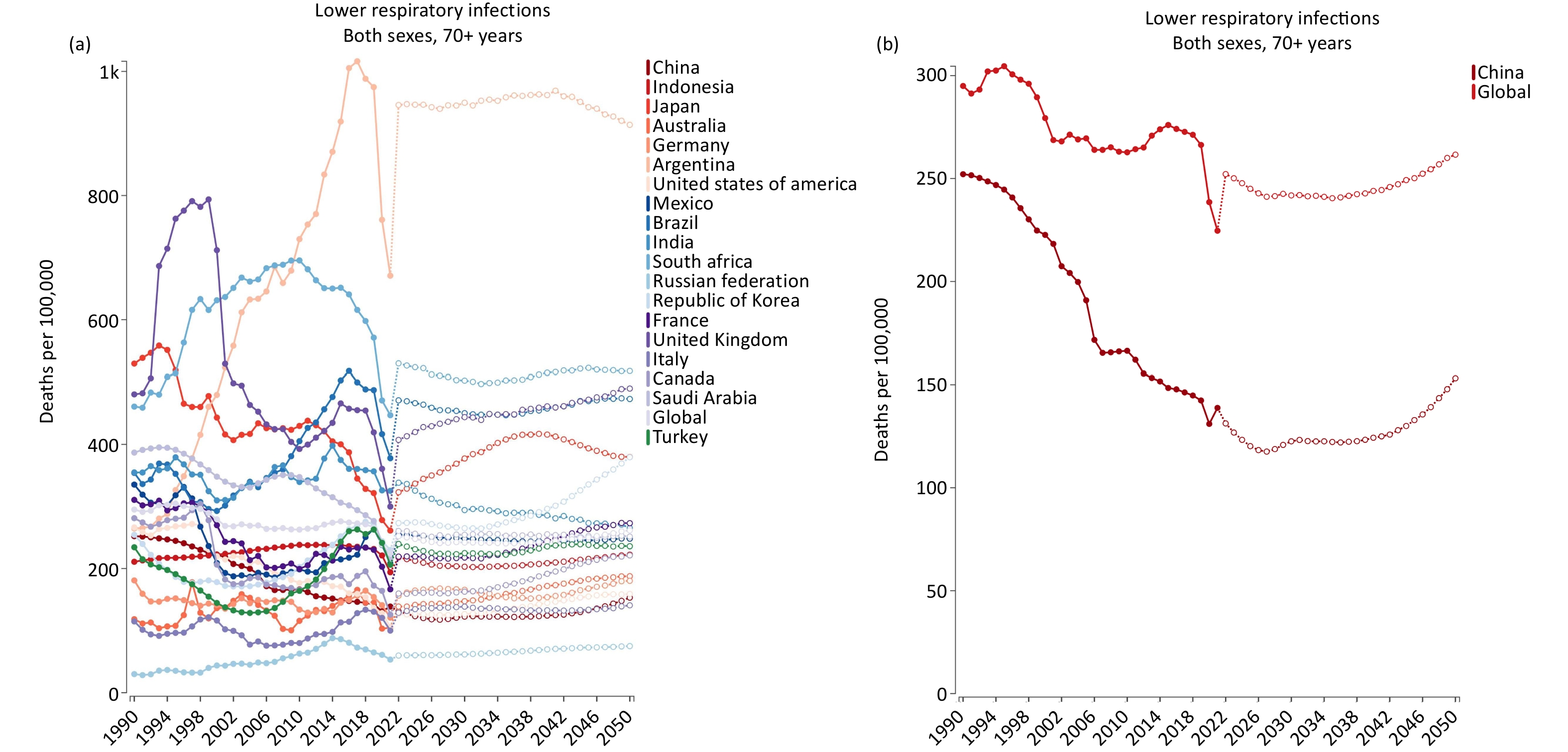
In 1990, the mortality rate for lower respiratory infections among the elderly aged 70 years and over in China was ranked 13th among the G20 countries and is predicted to be ranked 17th by 2050. In most countries, the mortality rate for lower respiratory infections among elderly aged 70 and over declined in 2020 and 2021 but increased in 2022. From 1990 to 2050, the mortality rate of lower respiratory infections in China’s elderly population was consistently below the global average and showed a declining trend. However, according to predictions, the mortality rate from lower respiratory tract infections among older adults in China is expected to increase gradually from 2040 to 2050. The specific trends are shown in Figure 1.
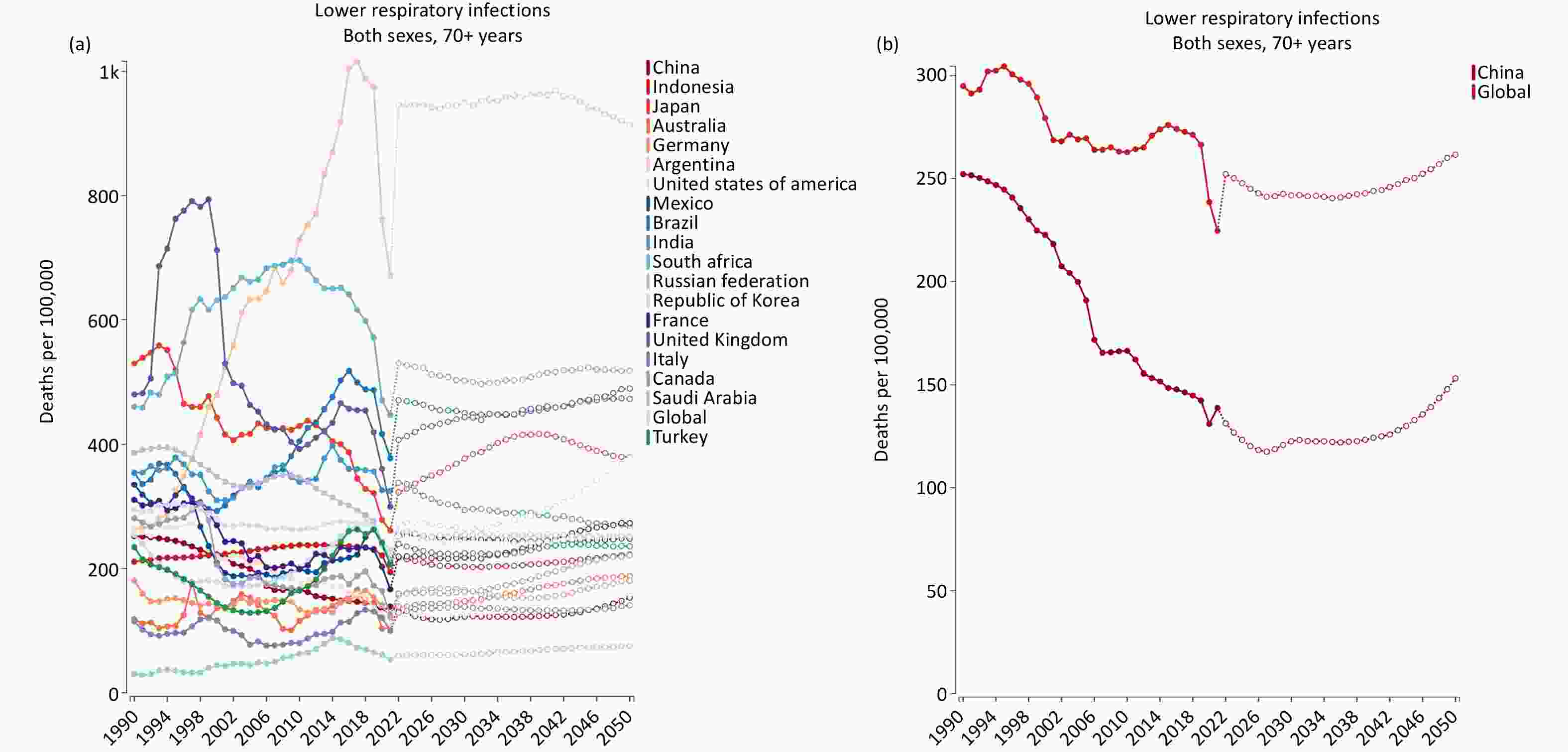
Figure 1. (A) LRI mortality among elderly aged 70 and over in global and G20 countries from 1990 to 2050. (B) LRIs mortality among the elderly aged 70 and over globally and China from 1990 to 2050.
-
In 1990, the mortality rate from lower respiratory infections in China was 60.64 (53.39, 66.98) for all age groups and 252.11 (204.84, 282.59) for those aged 70 and over. Among the causes of death in the elderly aged 70 years and older, lower respiratory infections ranked eighth. By 2050, it is projected that the mortality rate from lower respiratory infections will decrease to 9.54 (7.57, 11.65) for all age groups and 153.16 (120.96, 190.22) for those aged 70 and over, with the rank for lower respiratory infections among causes of death in this age group falling to fourteenth. From 2020 to 2050, the mortality rate from lower respiratory infections for all age groups is expected to decrease, whereas for those aged 70 years and older, it is expected to increase. The mortality rate in older men was consistently higher than that in older women, and the annual average rate of decrease in lower respiratory infection mortality was higher in women than in men. The specific data are listed in Table 1.
Variables Deaths, thousands (95% UI) 1990−2050 Percentage change (%) Deaths per 100,000 people (95% UI) 1990−2050 Estimated APC (%) 1990 2020 2050 1990 2020 2050 All ages/
age−standardizedMale 257.16
(226.33,
2,
924.04)108.55
(88.28,
133.99)251.05
(178.58,
348.49)−2.38 71.30
(64.52,
78.60)19.29
(16.00,
23.32)15.11
(11.92,
18.82)−1.04
(−1.24,
−0.84)Female 217.61
(183.77,
247.40)79.90
(60.83,
110.46)205.09
(133.88,
293.15)−5.75 54.50
(44.38,
61.46)9.81
(7.66,
13.05)6.60
(4.81,
9.28)−1.13
(−1.36,
−0.90)Both 474.77
(415.13,
530.97)188.46
(156.05,
224.81)456.14
(337.83,
579.37)−3.92 60.64
(53.39,
66.98)13.31
(11.16,
15.6)9.54
(7.57,
11.65)−1.03
(−1.24,
−0.82)Adults older
than 70 yearsMale 45.15
(38.60,
51.71)82.37
(66.24,
102.05)234.88
(165.11,
326.45)420.22 276.97
(236.81,
317.26)159.02
(127.89,
197.02)191.37
(147.91,
241.66)−1.04
(−1.22,
−0.86)Female 49.46
(33.18,
59.38)65.76
(48.54,
91.49)197.62
(127.77,
284.01)299.56 233.02
(156.29,
279.68)107.34
(79.24,
149.36)123.51
(83.77,
170.56)−1.40
(−1.61,
−1.19)Both 94.61
(76.87,
106.05)148.12
(121.39,
178.43)432.50
(317.75,
554.33)357.14 252.11
(204.84,
282.57)131.02
(107.37,
157.83)153.16
(120.96,
190.21)−1.22
(−1.41,
−1.02)Note. APC, annual percentage change Table 1. Number and Mortality Rates of Lower Respiratory Infections among Elderly Aged 70 and Over by Gender in China for 1990, 2020, and 2050
-
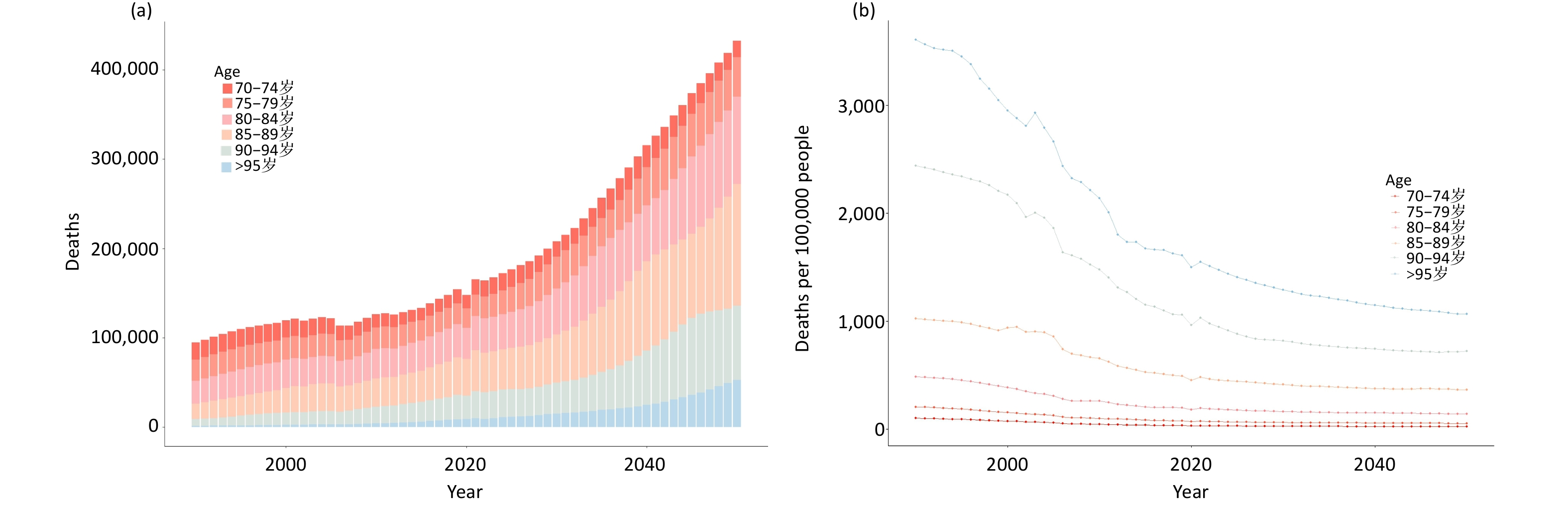
Research indicates that from 1990 to 2050, among older adults aged 70 years and over in China, older age will be associated with higher mortality rates from lower respiratory infections, while the rate of decrease in mortality will be faster. The mortality rate for those aged 95 and over has always been the highest. In 2020, the mortality rate from lower respiratory infections for those aged 95 and over was 1502.67 (1067.43, 1981.39), while for those aged 70-74 it was 30.53 (24.21, 38.06). The burden of lower respiratory tract infection-related deaths was significantly greater in older age groups than in younger age groups. The specific trends are shown in Figure 2.

Figure 2. Number(A) and mortality rates(B) of lower respiratory infections among different age groups aged 70 and over in China from 1990 to 2050.
-
In 1990, the DALYs for lower respiratory infections among older adults aged 70 years and over in China was 3570.18 (2890.97, 4012.46), while in 2050 it is projected to be 1713.70 (1379.27, 2095.62), representing a 52.0% decrease. From 1990 to 2050, the YLLs rate, YLDs rate, and DALYs rate for lower respiratory infections in the 70 and over age group were higher than those for the entire population. The burden of premature death due to lower respiratory tract infections far exceeds that due to disability. The burden of premature death and disability due to lower respiratory tract infections has consistently been higher in males compared to females, with the annual average rate of decrease in female mortality being greater than that in males.
Variables YLL per 100,000 people (95% UI) YLD per 100,000 people (95% UI) DALY per 100,000 people (95% UI) 1990−2050 Estimated APC of DALY Change (%) 1990 2020 2050 1990 2020 2050 1990 2020 2050 Age−standardized Male 3,332.04 (2,880.36, 3,816.17) 423.69 (361.97, 497.12) 247.21 (201.94, 300.34) 7.46 (4.97, 10.30) 4.59 (3.09, 6.39) 4.35 (2.74, 6.24) 3340.53 (2883.47, 3810.16) 428.18 (365.58, 500.58) 251.56 (205.51, 305.07) −4.49 (−4.87, −4.12) Female 2,938.44 (2,536.39, 3,390.77) 258.21 (215.74, 314.30) 126.39 (94.70, 173.17) 7.22 (4.85, 10.06) 3.62 (2.42, 5.07) 2.96 (1.73, 4.40) 2946.21 (2542.50, 3390.86) 261.85 (220.31, 313.48) 129.35 (97.31, 176.13) −5.43 (−5.85, −5.01) Both 3,120.30 (2,718.02, 3,566.20) 331.21 (286.12, 385.88) 175.53 (144.71, 213.35) 7.29 (4.91, 10.09) 4.01 (2.71, 5.57) 3.50 (2.16, 5.04) 3128.38 (2724.11, 3579.57) 335.18 (289.45, 389.2) 179.03 (147.41, 217.57) −4.98 (−5.38, −4.58) Adults older than 70 years Male 3,978.76 (3,380.41, 4,605.69) 1968.55 (1581.27, 2439.09) 1956.76 (1497.46, 2473.06) 26.56 (17.89, 36.410 24.53 916.35, 33.84) 31.32 (20.06, 45.80) 4005.81 (3421.91, 4649.99) 1992.39( 1616.49, 2462.96) 2214.77 (1719.72, 2778.90) −1.34 (−1.53, −1.16) Female 3,209.40 (2,130.82, 3,853.20) 1258.14 (944.88, 1748.59) 1153.28 (802.95, 1636.99) 25.90 (17.36, 35.13) 18.40 (12.76, 25.37) 21.18 (12.96, 30.38) 3235.71 (2116.57, 3870.24) 1276.72 (958.44, 1741.16) 1326.76 (935.75, 1860.87) −1.78 (−2.00, −1.57) Both 3,543.55 (2,879.88, 3,978.97) 1583.62 (1297.45, 1909.00) 1503.40 (1193.63, 1838.39) 26.19 (17.76, 35.48) 21.21 (14.41, 29.09) 25.60 (16.52, 36.53) 3570.18 (2890.97, 4012.46) 1604.61 (1317.84, 1912.62) 1713.70 (1379.27, 2095.62) −1.56 (−1.75, −1.36) Note. APC, annual percentage change; DALY, disability−adjusted life years; YLL, years of life lost; YLD, years lived with disability. Table 2. YLL, YLD, and DALY rates of Lower Respiratory Infections in China from 1990 to 2050
-
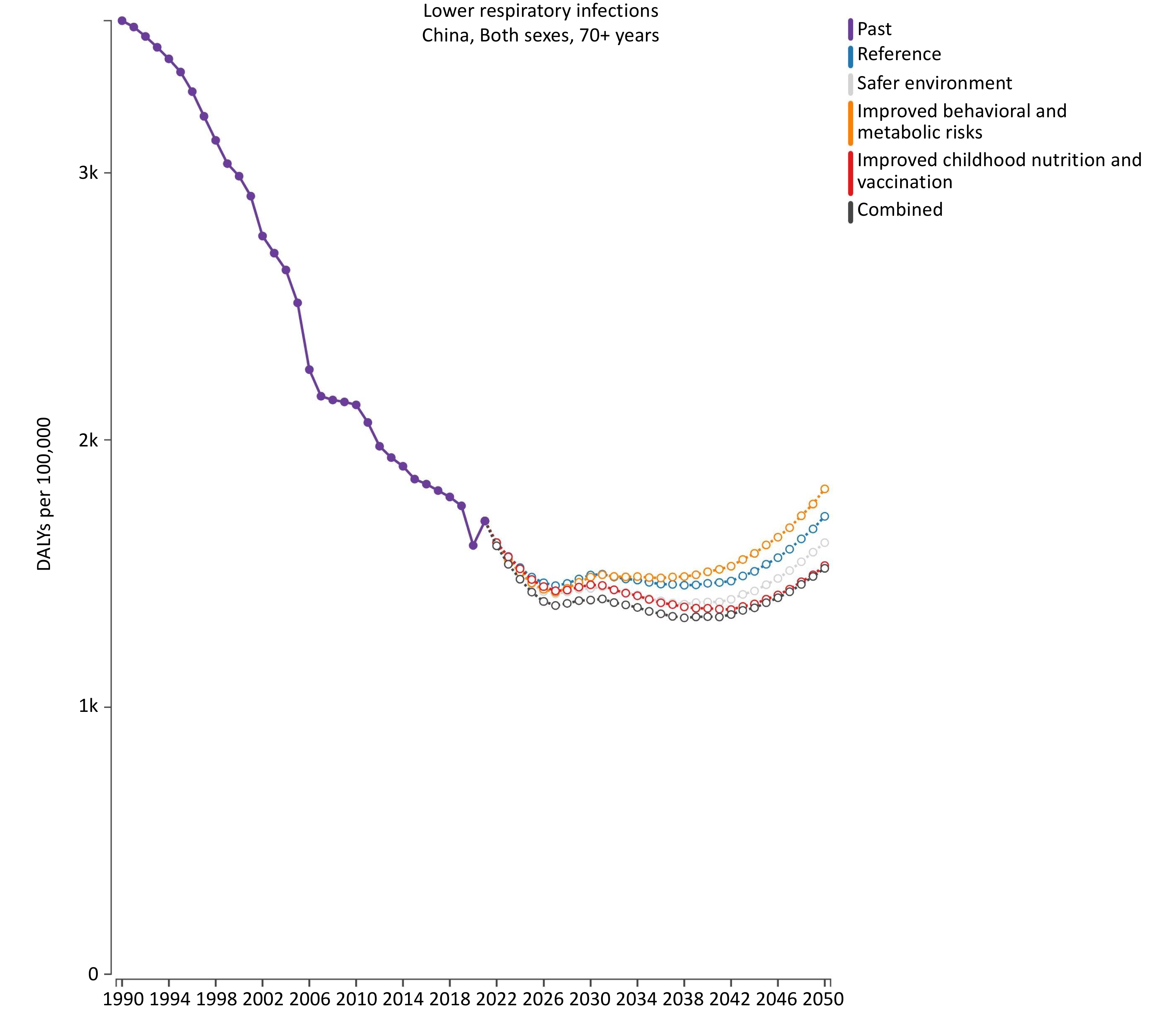
Forecasts indicate that the DALY rate for lower respiratory infections among older adults aged 70 years and older in China will rise from 2040 to 2050. Among the single scenarios, the lowest DALY rate was observed with child nutrition and vaccination changes. In contrast, the highest DALY rate was observed in scenarios addressing behavioral and metabolic risks. The combined effect of changes in the environment, behavior, metabolism, child nutrition, and vaccination results in a lower DALY rate than in any scenario.
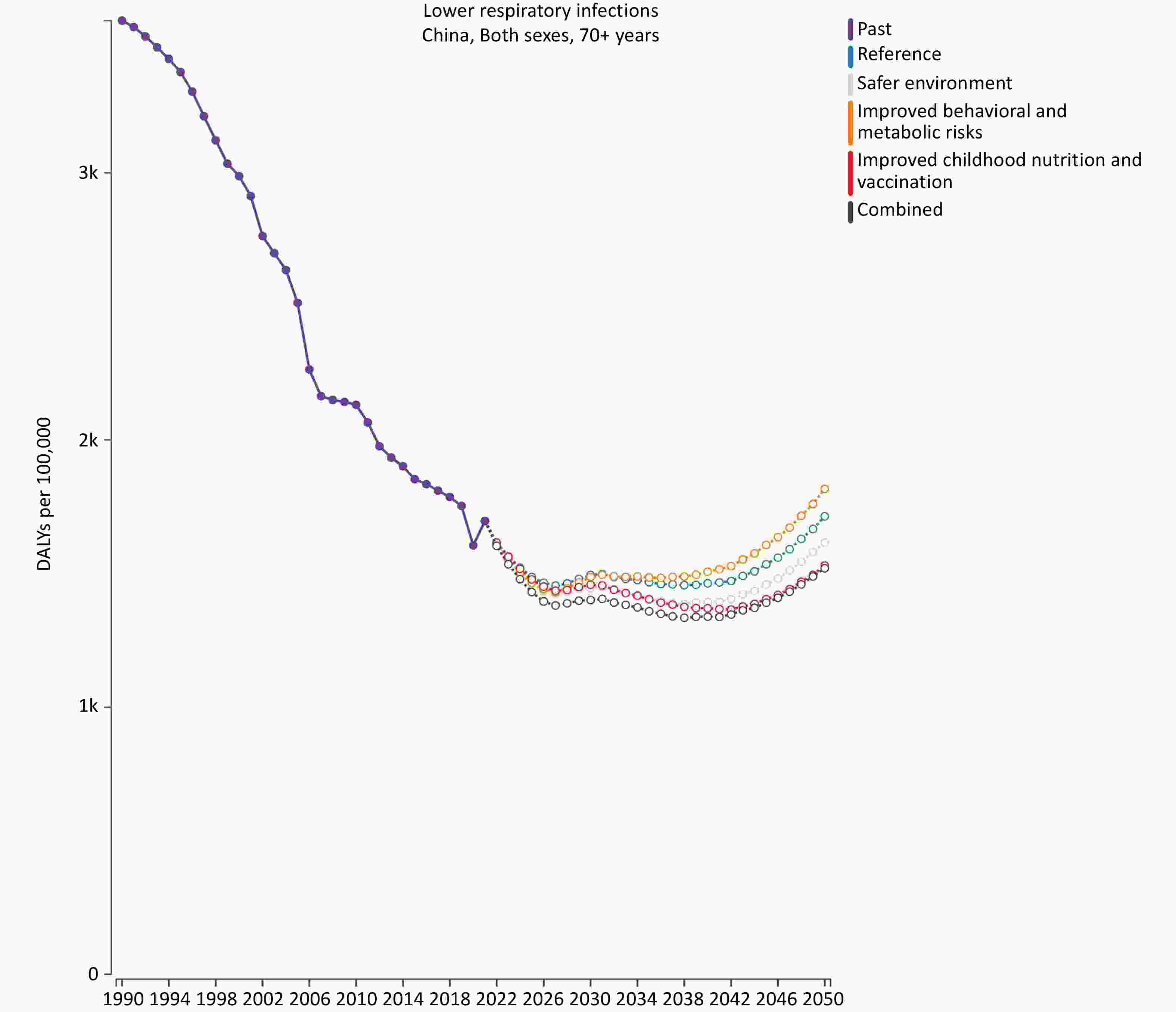
Figure 3. Forecast of DALYs rate for lower respiratory infections in China’s 70 and over age group from 1990 to 2050 under Different Scenarios.
-
Our study comprehensively describes the disease burden of lower respiratory infections among elderly aged 70 and over in China from 1990 to 2050. The mortality rate for lower respiratory infections in this age group decreased from 252.11 (204.84, 282.57) in 1990 to 131.02 (107.37, 157.83) in 2020, and is projected to rise to 153.16 (120.96, 190.21) by 2050. The Estimated Annual Percentage Change (EAPC) in mortality rate for this age group from 1990 to 2050 is -1.22 (-1.41, -1.02), indicating an overall declining trend. The changes in the disease burden of lower respiratory infections in China are similar to global trends but below the average worldwide.
The mortality rate for lower respiratory infections (LRI) among the elderly aged 70 years and older is significantly higher than that in the entire age group and increases with age. The decline in respiratory, immune, and digestive system functions in the elderly leads to reduced immunity and resistance to respiratory pathogens[16]. In addition, an increase in age-related underlying conditions contributes to a higher frequency and severity of LRI. The disease burden of lower respiratory tract infections is higher in men than in women. This sex difference may be related to biological differences, lifestyle habits (such as higher smoking rates), and variations in health behaviors.
In the future, the elderly population in China is expected to continue to grow. According to the United Nations Population Fund projections, the population aged 65 years and older in China will reach 334 million by 2050, making it the country with the largest elderly population in the world[17]. China is facing severe challenges related to population aging. However, as a developing country, China still has significant gaps in social welfare areas such as healthcare, elderly care, and education, compared with developed countries. Therefore, the burden of lower respiratory tract infections in the elderly cannot be ignored. Simultaneously, it is essential to strengthen the community and clinical management of lower respiratory infections in the elderly, and further research on effective treatments for lower respiratory infections should be conducted. Older people have relatively weak immune and physiological functions, so it is essential to use antibiotics rationally to avoid complications and sequelae as much as possible.[23]
Forecasts of mortality rates from lower respiratory infections (LRI) under different scenarios indicate that vaccination plays a crucial role in protecting elderly individuals from LRI-related deaths. A study shows that in 2017, the coverage rate of the 23-valent pneumococcal polysaccharide vaccine (PPV23) was 2.98% in a population over 2 years of age, with coverage among older people ranging from 0.17% to 0.69%[18]. Additionally, many respiratory pathogen vaccines are not included in China’s national immunization program; therefore, with a few exceptions, most cities lack vaccine subsidies, resulting in low vaccination uptake among older people[19]. Furthermore, no licensed vaccine against respiratory syncytial virus (RSV) exists. One study suggested that the highly dispersed prevalence of certain viruses makes it difficult to establish effective herd immunity[24]. Therefore, to address the disease burden of lower respiratory tract infections in elderly individuals in China, it is essential to promote relevant vaccines and increase vaccination coverage.
Environmental factors are also significant risk factors for mortality due to lower respiratory infections. Research has shown that air pollution can adversely affect the respiratory, circulatory, urinary, nervous, and immune systems[20]. Research has also shown that the concentration of PM2.5 is negatively correlated with the health status of older people[22]. With rapid economic development, industrialization, and urbanization, the threat of particulate matter pollution to public health in China is increasing.
In 2020 and 2021, there was a dramatic decrease in the mortality rate from lower respiratory infections in China, the G20 countries, and globally. However, this rate is expected to increase again in 2022, which may be related to the implementation and subsequent removal of various non-pharmaceutical interventions for COVID-19[21]. During the pandemic, China implemented measures such as wearing masks, maintaining social distancing, and restricting gatherings in public places to reduce the transmission of respiratory pathogens. After the Chinese government lifted these restrictions in 2022, the mortality rate from lower respiratory infections increased again, although it remained slightly below pre-pandemic levels.
The GBD 1990-2050 projections for the burden of lower respiratory infections among people aged 70 and above in China provide a basis for developing related prevention and control strategies for the elderly. However, this study has limitations. The GBD research did not forecast specific etiologies, so the impact of various causes on lower respiratory infections cannot be observed. In addition, we could not obtain forecast data for individual Chinese provinces, making it impossible to analyze regional differences. Furthermore, the GBD does not provide monthly data, whereas respiratory infections exhibit seasonal variations. The GBD predictive model framework relies on past estimates from GBD 2021 and does not incorporate other driving factors or potential threats to population health. The projections are constrained by data quality and limitations inherent in the GBD estimates. Additionally, due to reporting delays, COVID-19 case and death data for 2022 and 2023 are still limited, and the pandemic’s long-term direct and indirect impacts remain highly uncertain. In the absence of data indicating future trends in the COVID-19 burden, the GBD assumes that COVID-19 deaths and DALYs will decline linearly to zero between 2023 and 2030, based on research into the virulence of the coronavirus. If more data on the impact of COVID-19 become available in the future, the GBD will revise the model accordingly.
-
In summary, lower respiratory infections remain a significant health issue for elderly 70 and above in China, and the burden of these diseases may increase. Therefore, it is crucial to focus on preventing and controlling lower respiratory tract infections in this age group. The government must strengthen its prevention and management efforts, including increasing vaccination rates, providing regular health checkups, managing chronic diseases, enhancing population immunity, improving public health management, and establishing a comprehensive epidemic warning system for respiratory infections. These measures aim to improve the health and QoL of the elderly population.
Forecast of the Burden of Lower Respiratory Infections in the Elderly Aged 70 and Above in China from 1990 to 2050, GBD2021
doi: 10.3967/bes2025.036
- Received Date: 2024-10-11
- Accepted Date: 2025-02-10
-
Key words:
- Lower respiratory infections /
- China /
- Mortality rate /
- Trends /
- DALY
Abstract:
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The data in this study were obtained from public databases and did not require an ethical review.
| Citation: | Miaomiao Zhang, Ruiyi Zhang, Yuchang Zhou, Maigeng Zhou. Forecast of the Burden of Lower Respiratory Infections in the Elderly Aged 70 and Above in China from 1990 to 2050, GBD2021[J]. Biomedical and Environmental Sciences. doi: 10.3967/bes2025.036

|

 Quick Links
Quick Links
 DownLoad:
DownLoad: