-
Stroke is the third leading cause of death and one of the leading causes of disability worldwide, as in 2021[1,2]. From 1990 to 2021, the global burden of stroke has increased significantly, with a 70.0% increase in stroke incidence, 44.0% increase in stroke deaths, 86.0% increase in stroke prevalence, and a 32% increase in disability-adjusted life years (DALYs)[3]. Worldwide, the incidence of stroke is highest in Asia[4], and China has the highest stroke incidence in Asia and even the world[5,6]. Common risk factors for stroke include active smoking, hypertension, and a family history of stroke[7,8].
The tobacco epidemic is one of the most significant public health issues worldwide[9]. In the four-stage conceptual model of the tobacco epidemic[10], because the initiation and development of tobacco use in Asian countries occurred later than that in Western countries, the tobacco epidemic stages of Asian and Western countries are inconsistent, and the cumulative effects of tobacco hazards in Asian and Western developed countries have diverse temporal concepts. Currently, Asian countries have a higher prevalence of tobacco use. In a World Health Organization (WHO) report[11], the smoking prevalence in adults was 24%–28% in Asia, including 25–30% in China, while that in Western countries such as America was 11%–12% and Britain was 12–14%. Additionally, there is a competitive effect of smoking and indoor coal use owing to the generally specific cooking practices[12], as well as the more severe ambient air pollution in Asian countries[13]. Therefore, the Relative Risk (RR) values of diseases caused by smoking in Asian populations, including Chinese, are significantly different from those in Western countries. For example, a previous study[14] analyzed the smoking exposure risk of lung cancer in China, and demonstrated that the RR value was 3.26 (2.79, 3.82) in males, and 3.18 (2.78–3.63) in females. The RRs of lung cancer attributed by smoking in European males and females were 23.6 (20.4, 27.2) and 7.8 (6.8–9.0), respectively[15].
However, there have been no separate literature searches for related RR in Asian countries. Whether the risk estimates of smoking-related stroke in China differ from those of other Asian countries or across the whole of Asia remains unclear and requires further investigation. Therefore, distinguishing between the risk effects of smoking-related diseases in Asian and Western countries and comparing China, other Asian countries, and the whole of Asia is necessary.
Thus, this study aims to evaluate the RR of stroke attributed by active smoking among ever, current, and former smokers in China, other Asian countries, and the whole of Asia, and discuss the possible reasons for the observed differences.
-
The English databases PubMed, Web of Science, Embase, Cochrane Library, and the Chinese databases China National Knowledge Infrastructure (CNKI), WanFang, and VIP were comprehensively searched according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. All published cohort and case-control studies on smoking and its related diseases among Asian populations were gathered from the inception to September 10, 2022. The search indices were as follows: tobacco, smoking, cigarette, smoker, smokers, nicotine, cohort, case control, case-control, Asia or Asian, China or Chinese, and other Asian country names. The retrieval key words for Pubmed were: (“tobacco”[Title/Abstract] OR “smoking”[Title/Abstract] OR “cigarette”[Title/Abstract] OR “smoker”[Title/Abstract] OR “smokers”[Title/Abstract]) AND (“case control”[Title/Abstract] OR “cohort”[Title/Abstract] OR “case-control”[Title/Abstract]) AND (“OR”[Title/Abstract] OR “HR”[Title/Abstract] OR “RR”[Title/Abstract]) AND ( “Asia”[Title] OR “Asian”[Title] OR “China”[Title/Abstract] (or other concrete Asian countries’ names) NOT (“meta-analysis”[Title/Abstract] OR “animal”[Title/Abstract] OR “gene*”[Title/Abstract]) AND (“1948/01/01”[Date - Publication]: “2022/09/10”[Date - Publication]).
-
Inclusion criteria: Articles were included by referring to the PECOS format: (1) Participants (P): study objects were from the Asian population; (2) Exposure (E): exposure factor was active smoking; (3) Comparison (C): active smoking contained ever, current, or former smoking, with non-smoking regarded as control; (4) Outcomes (O): Risk effects for active smoking and corresponding outcome, including RR, Odds Ratios (OR), or Hazard Ratios (HR) and its 95% confidence interval (CI); (5) Type of study (S): the study design was cohort study or case-control study; and (6) The full article is available.
Exclusion criteria: (1) Smoking-related diseases were not included; (2) The article is not original research, such as comments, reviews, meta-analyses, letters, or meeting abstracts; (3) The article belongs to molecular mechanism research, animal experiments, or in vitro experiments; (4) The participants are a special population, for example, nurses, pregnant women, newborns, and the like; and (5) The article was republished.
-
The included cohort and case-control studies were evaluated for quality using the Newcastle-Ottawa scale (NOS). The NOS comprises eight items with a total score of nine and is divided into three sections: selection of study objects, comparability between groups, and evaluation of exposure factors or outcomes. Detailed scoring items and criteria were introduced on the Cochrane website (https://cmr.cochrane.org/?CRGReportID=2972). Literatures with a total score of ≥ 6 points were included to ensure the quality of the study.
-
The following information were extracted from the included literatures: (1) Basic information: research day or duration, place, sample size, sex, age, study type, and journal of publication; (2) Smoking exposure situation: smoking status (ever smoker, current smoker, and former smoker), pack years (PY), cigarettes per day (CPD), smoking years and quit years (QY); (3) Outcome: stroke; and (4) Effect values (RR, OR or HR) with its 95% confidence interval (CI), statistical method and correction factors.
Literature screening, NOS, and data extraction were performed independently by two researchers and verified by the third researcher. Data from the literature search contained risk estimates with 95% CI of ever, current, and former smokers versus non-smokers in males and females, and stroke subtypes were not subdivided for a limited amount of literature. Additionally, the study type, country, start age, study year, sex, smoking status, stroke type, and stroke outcome were described. The adjusted risk estimate was first extracted if the study included both simple and adjusted risk estimates.
-
Dichotomous data were extracted from each included study, including smoking status (ever, current, and former smokers vs. never smokers) and health outcome (stroke). Analyses were performed based on the number of studies within each subgroup. For subgroups containing only one or two studies, a descriptive summary was provided with RR, and its 95% CI reported as available. For subgroups that included three or more studies, meta-analyses were conducted using R version 4.4.1 (R Foundation for Statistical Computing, https://www.r-project.org). Heterogeneity was assessed using the I2 statistic. A fixed-effect model was used when heterogeneity was low (I2 < 50% and P > 0.05), and a random-effects model was used when heterogeneity was substantial (I2 ≥ 50% or P ≤ 0.05). Publication bias was evaluated using Egger’s regression test and the visual inspection of funnel plots. P < 0.05 indicated the existence of publication bias, whereas indicated no publication bias. Sensitivity analyses were performed using the “leave-one-out” method, whereby each study was sequentially removed to assess its influence on the pooled estimate and heterogeneity.
-
A total of 6232 Chinese and 10,579 English articles were retrieved. Approximately 16,279 articles were excluded because they did not meet these requirements. Of these, 480 were excluded for NOS < 6, and 522 were excluded because they did not include active smokers or stroke outcomes. Finally, 52 articles were included (Figure 1).
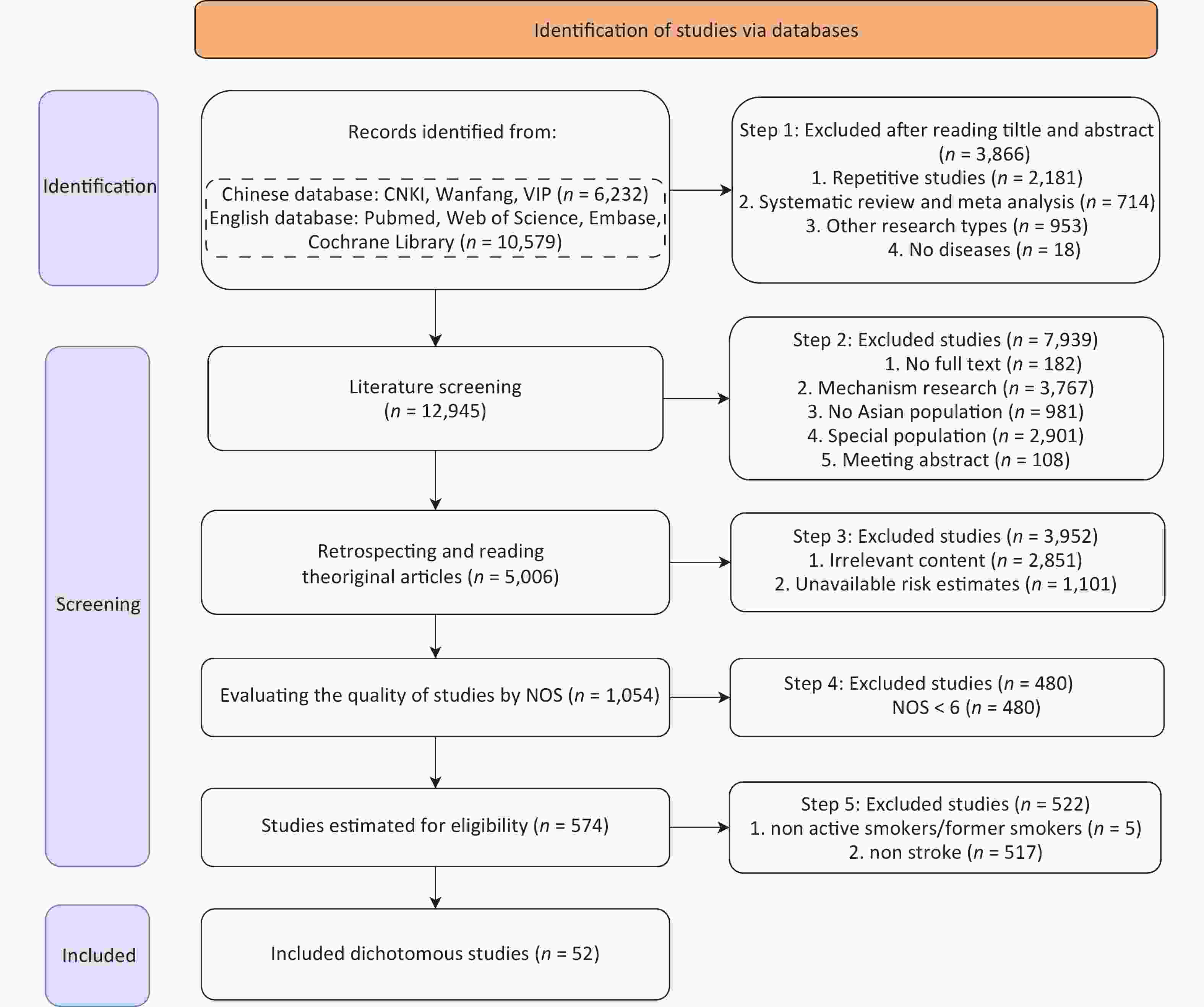
Figure 1. Flow chart of the study selection process.
-
There were 20 (38.46%) Chinese and 17 (32.69%) English articles concerning China, and 15 (28.85%) articles concerning other Asian countries, with a mean NOS of 7.25 (Table 1). Since some articles reported more than one subtype, the statistical numbers of sex, smoking status, and stroke type were more than 52 articles. Approximately 53.85% of the studies were cohort studies, with a mean NOS of 7.61. The study years of China were divided into two periods: before 2000 and after 2000. In contrast, studies from other Asian countries were more common before 2000 than in the later period. Most studies reported on both sexes, followed by males and females. Regarding smoking status, 34, 22, and 17 articles included information on ever, current, and former smokers, respectively. Most studies reported total stroke (30 articles), and the most common stroke outcome was morbidity (34 articles).
Characteristic Groups Published Country NOS China (%#) Other Asian countries (%#) All Chinese English Total 20 (38.46) 17 (32.69) 15 (28.85) 52 7.25 Study type Cohort 8 (28.57) 14 (50.00) 6 (21.43) 28 7.61 Case-control 12 (50.00) 3 (12.50) 9 (37.50) 24 6.83 Study year −1999 8 (25.81) 11 (35.48) 12 (38.71) 31 7.32 2000− 12 (57.14) 6 (28.57) 3 (14.29) 21 7.14 Sex* Both 17 (48.57) 10 (28.57) 8 (22.86) 35 7.06 Male 2 (8.70) 9 (39.13) 12 (52.17) 23 7.70 Female 0 (0.00) 5 (33.33) 10 (66.67) 15 7.73 Smoking status* Ever smoker 16 (47.06) 10 (29.41) 8 (23.53) 34 6.85 Current smoker 5 (22.73) 10 (45.45) 7 (31.82) 22 7.91 Former smoker 4 (23.53) 9 (52.94) 4 (23.53) 17 7.82 Stroke type* Stroke 13 (43.33) 11 (36.67) 6 (20.00) 30 7.5 Ischemic stroke 6 (40.00) 6 (40.00) 3 (20.00) 15 6.80 Hemorrhagic stroke 1 (12.50) 1 (12.50) 6 (75.00) 8 7.13 Stroke outcome Morbidity 18 (52.94) 8 (23.53) 8 (23.53) 34 7.06 Mortality 2 (11.11) 11 (61.11) 5 (27.78) 18 7.78 Note. NOS, Newcastle-Ottawa Scale; *, The articles reported more than one subtype; #, Percentage of the subtype sum of horizontal statistics. Table 1. Characteristics of included studies
-
Meta-analyses of the nine groups stratified by smoking status (ever-smokers, current smokers, and former smokers) and sex in China, other Asian countries, and all Asian countries are shown in Table 2. The RRs of the nine groups stratified by smoking status and sex in China and all Asian countries showed no significant differences, but the RRs of males in ever smokers between China and other Asian countries were statistically different.
Smoking status Sex China Other Asian countries Asian country No. of studies Pooled RR
(95% CI)I2 (%) Model No. of studies Pooled RR
(95% CI)I2 (%) Model No. of studies Pooled RR
(95% CI)I2 (%) Model Ever smokers Both 21 1.76
(1.50, 2.56)90.2 Random effect 6 2.01
(1.29, 3.14)81.2 Random effect 27 1.81
(1.56, 2.10)92.4 Random effect Male 9 1.21
(1.15, 1.26)41.3 Fixed effect 5 2.31
(1.38, 3.86)78.2 Random effect 14 1.56
(1.24, 1.97)88.8 Random effect Female 4 1.26
(0.94, 1.68)91.0 Random effect 4 1.78
(0.82, 3.86)58.1 Random effect 8 1.49
(1.02, 2.18)91.2 Random effect Current smokers Both 11 1.49
(1.29, 1.80)99.5 Random effect 7 1.63
(1.31, 2.02)57.1 Random effect 18 1.56
(1.34, 1.80)99.1 Random effect Male 6 1.54
(0.93, 2.53)95.1 Random effect 6 1.27
(1.15, 1.41)0.0 Fixed effect 12 1.42
(1.13, 1.80)95.3 Random effect Female 2 1.60
(0.90, 2.86)
1.55
(1.43, 1.66)— — 6 1.65
(1.40, 1.94)47.5 Fixed effect 8 1.57
(1.46, 1.68)46.4 Fixed effect Former smokers Both 9 1.19
(1.03, 1.38)80.2 Random effect 4 0.97
(0.86, 1.10)19.2 Fixed effect 13 1.15
(1.02, 1.29)74.0 Random effect Male 6 1.15
(0.82, 1.61)76.5 Random effect 4 0.91
(0.81, 1.03)24.5 Fixed effect 10 1.05
(0.88, 1.25)67.2 Random effect Female 2 1.31
(0.87, 1.99)
0.86
(0.63, 1.17)— — 4 1.16
(0.87, 1.55)0.0 Fixed effect 6 1.07
(0.88, 1.29)1.4 Fixed effect Note. RR, Relative Risk; CI: Confidence Interval. * Never smokers were used as the reference group for each analysis. Table 2. Pooled Relative Risk stratified by smoking status and sex*
The pooled RRs of ever smokers in China were 1.76 (1.50, 2.56), 1.21 (1.15, 1.26) and 1.26 (0.94, 1.68) in both sexes, males and females, respectively, with a heterogeneity of RRs (I2both = 90.2, I2female = 91.0), and those of other Asian countries were 2.01 (1.29, 3.14), 2.31 (1.38, 3.86), and 1.78 (0.82, 3.86) in both sexes, males and females, with a heterogeneity of RRs across studies (I2both = 81.2, I2male = 78.2, I2female = 58.1). Although the RRs of both sexes and females in other Asian countries were slightly higher than those of China, there was no statistical difference between them.Whereas, the RR of males in other Asian countries (2.31 (1.38, 3.86)) was higher than that in China (1.21 (1.15, 1.26)). The RR values of all Asian countries were 1.81 (1.56, 2.10), 1.56 (1.24, 1.97) and 1.49 (1.02, 2.18) in both sexes, males and females, showing no statistical difference compared with China.
As for current smokers, the pooled RRs of both sexes, males, females in China were 1.49 (1.29, 1.80), 1.54 (0.93, 2.53) and 1.60 (0.90, 2.86), respectively, and significant heterogeneity existed among the studies of both sexes and males (I2both = 99.5, I2male = 95.1), which did not reach a statistical significance with those of other Asian countries (1.63 (1.31, 2.02) in both sexes, 1.27 (1.15, 1.41) in males and 1.65 (1.40, 1.94) in females), or the whole of Asian countries (1.56 (1.34, 1.80), 1.42 (1.13, 1.80) and 1.57 (1.46, 1.68) in both sexes, males and females, respectively).
As for former smokers, the pooled RRs of the Chinese were 1.19 (1.03, 1.38), 1.15 (0.82, 1.61), 1.31 (0.87, 1.99) in both sexes, males, and females, respectively, and significant heterogeneity was tested in both sexes and males (I2both = 80.2, I2male = 76.5). Although the RRs of China were slightly larger than those of other Asian countries, there was no statistical difference between China and other Asian countries, with 0.97 (0.86, 1.10) in both sexes, 0.91 (0.81, 1.03) in males and 1.16 (0.87, 1.55) in females, or even in the whole of Asia, with 1.15 (1.02, 1.29), 1.05 (0.88, 1.25), and 1.07 (0.88, 1.29) in both sexes, males, and females, respectively. Because of the limited number of studies on current and former female smokers in China, the RRs were reported without pooling.
-
Despite the heterogeneity, further stratified analyses were conducted for ever, current, and former smokers in China (Table 3), other Asian countries (Table 4), and all Asian countries (Table 5). As for ever smokers in China, there was no article on subgroup hemorrhagic stroke in both sexes, males or females, and ischemic stroke in females. The RRs of ever smokers in both sexes ranged from 1.46 (1.18, 1.80) to 2.22 (1.66, 2.97) in China, which were almost equal to those of other Asian countries, except for one article with RR 4.81 (2.67, 10.25) for small sample, and the RRs were similar to those in the whole of Asia (ranged from1.46 (1.18, 1.80) to 2.24 (1.71, 2.93)). The RRs of males ranged from 1.20 (1.15, 1.25) to 1.77 (0.91, 3.42) in China, while they ranged from 1.10 (0.53, 2.26) to 3.76 (3.02, 4.67) in other Asian countries, while the subgroup of morbidity had a higher RR 3.76 (3.02, 4.67), which had no statistical difference with the same subgroup of China. The RRs of females ranged from 1.26 (0.94, 1.68) to 1.81 (0.31, 10.60), which were similar to those of other Asian countries, ranging from 1.53 (0.52, 4.53) to 1.81 (0.72, 4.60), except for a single article with RR 2.21 (0.71, 6.87) for a small sample. Besides, the RRs of China were quite similar to the whole of Asian countries; as for males, the RRs of Asian countries ranged from 1.20 (1.15, 1.26) to 3.43 (1.31, 9.02). The RRs of females ranged from 1.26 (0.95, 1.66) to 2.21 (0.71, 6.88). The results were stable in different subgroups.
Sex Group Subgroup Ever smokers Current smokers Former smokers No. of
studyRR (95% CI) I2(%) No. of
studyRR (95% CI) I2(%) No. of
studyRR (95% CI) I2(%) Both Study year −1999 12 1.53 (1.30, 1.80) 91.6 7 1.58 (1.24, 2.02) 99.3 7 1.23 (1.04, 1.47) 82.2 2000− 9 2.22 (1.66, 2.97) 67.0 4 1.27 (0.99, 1.64) 96.2 2 1.28 (0.77, 2.14)
0.98 (0.91, 1.06)− Outcome Morbidity 17 1.84 (1.52, 2.22) 77.1 5 1.65 (1.20, 2.25) 99.6 4 1.00 (0.96, 1.05) 65.5 Mortality 4 1.54 (1.20, 1.99) 96.9 6 1.32 (1.08, 1.62) 89.9 5 1.31 (1.08, 1.59) 65.2 Study type Cohort 7 1.46 (1.18, 1.80) 78.0 11 1.49 (1.23, 1.80) 99.5 8 1.23 (1.05, 1.45) 79.7 Case-control 14 1.97 (1.60, 2.42) 92.3 0 − − 1 0.99 (0.92, 1.06) − Stroke type Stroke 13 1.68 (1.47, 1.93) 91.7 8 1.60 (1.28, 1.99) 99.2 8 1.23 (1.05, 1.45) 79.5 Ischemic stroke 8 1.95 (1.29, 2,96) 87.4 2 1.20 (1.16, 1.24)
1.89 (1.11, 3.22)− 1 0.98 (1.91, 1.06) − Hemorrhagic stroke 0 − − 1 1.02 (1.00, 1.04) − 0 − − Male Study year −1999 6 1.24 (1.08, 1.43) 53.0 4 1.99 (1.18, 3.38) 90.3 4 1.00 (0.87, 1.57) 53.3 2000− 3 1.32 (1.16, 1.49) 0.0 2 0.57 (0.33, 0.99)
1.37 (1.15, 1.64)− 2 3.24 (1.79, 5.86)
0.98 (0.79, 1.22)− Outcome Morbidity 2 1.77 (0.91, 3.42)
1.26 (1.00, 1.58)− 3 1.32 (0.57, 3.08) 97.4 3 1.43 (0.71, 2.86) 85.6 Mortality 7 1.25 (1.13, 1.39) 50.9 3 1.78 (0.88, 3.60) 80.3 3 0.94 (0.83, 1.05) 48.6 Study type Cohort 6 1.27 (1.14, 1.42) 27.0 5 1.81 (1.19, 2.75) 94.7 5 0.99 (0.92, 1.08) 38.0 Case-control 3 1.26 (1.09, 1.46) 64.7 1 0.57 (0.33, 0.99) − 1 3.24 (1.79, 5.86) − Stroke type Stroke 8 1.20 (1.15, 1.25) 42.4 6 1.54 (0.93, 2.53) 95.1 6 1.02 (0.94, 1.10) 76.5 Ischemic stroke 1 1.32 (1.13, 1.54) − 0 − − 0 − − Hemorrhagic stroke 0 − − 0 − − 0 − − Female Study year −1999 4 1.26 (0.94, 1.68) 91.0 2 1.60 (0.90, 2.86)
1.55 (1.43, 1.66)− 2 1.31 (0.87, 1.99)
0.86 (0.63, 1.17)− 2000− 0 − − 0 − − 0 − − Outcome Morbidity 0 − − 1 1.55 (1.43, 1.66) − 1 0.86 (0.63, 1.17) − Mortality 4 1.26 (0.94, 1.68) 91.0 1 1.60 (0.90, 2.86) − 1 1.31 (0.87, 1.99) − Study type Cohort 2 1.39 (0.97, 1.99)
1.81 (0.31, 10.60)− 2 1.60 (0.90, 2.86)
1.55 (1.43, 1.66)− 2 1.31 (0.87, 1.99)
0.86 (0.63, 1.17)− Case-control 2 1.51 (1.23, 1.64)
0.97 (0.91, 1.03)− 0 − − 0 − − Stroke type Stroke 4 1.26 (0.94, 1.68) 91.0 2 1.60 (0.90, 2.86)
1.55 (1.43, 1.66)− 2 1.31 (0.87, 1.99)
0.86 (0.63, 1.17)− Ischemic stroke 0 − − 0 − − 0 − − Hemorrhagic stroke 0 − − 0 − − 0 − − Note. RR: Relative Risk; CI: Confidence Interval. Table 3. Subgroup analysis investigating the association between ever, current, and former smokers and stroke risk in China
Sex Group Subgroup Ever smokers Current smokers Former smokers No. of
studyRR (95% CI) I2(%) No. of
studyRR (95% CI) I2(%) No. of
studyRR (95% CI) I2(%) Both Study year −1999 5 1.92 (1.14, 3.24) 84.9 7 1.63 (1.31, 2.02) 57.1 4 0.97 (0.86, 1.10) 19.2 2000− 1 2.67 (1.33, 5.36) − 0 − − 0 − − Outcome Morbidity 5 2.26 (1.44, 3.57) 79.6 4 2.08 (1.60, 2.68) 0.0 2 1.11 (0.78, 1.58)
1.48 (0.88, 2.49)− Mortality 1 1.02 (0.54, 1.92) − 3 1.30 (1.16, 1.45) 0.0 2 1.02 (0.59, 1.78)
0.92 (0.80, 1.06)− Study type Cohort 0 − − 5 1.33 (1.21, 1.48) 12.5 4 0.97 (0.86, 1.10) 19.2 Case-control 6 2.01 (1.29, 3.14) 81.2 2 2.70 (1.70, 4.20)
1.80 (0.90, 3.40)− 0 − − Stroke type Stroke 0 − − 5 1.34 (1.20, 1.48) 12.5 4 0.97 (0.86, 1.10) 19.2 Ischemic stroke 2 2.67 (1.33, 5.35)
4.81 (2.67, 10.25)− 0 − − 0 − − Hemorrhagic stroke 4 1.62 (1.00, 2.62) 86.9 2 2.70 (1.70, 4.20)
1.80 (0.90, 3.40)− 0 − − Male Study year −1999 3 2.43 (1.16, 5.09) 81.6 6 1.27 (1.15, 1.41) 0.0 4 0.91 (0.81, 1.03) 24.5 2000− 2 1.42 (0.80, 2.60)
3.43 (1.31, 9.02)− 0 − − 0 − − Outcome Morbidity 3 3.76 (3.02, 4.67) 0.0 3 1.36 (1.07, 1.71) 16.5 2 1.02 (0.68, 1.51)
1.56 (0.84, 2.90)− Mortality 2 1.42 (0.80, 2.60)
1.10 (0.53, 2.26)− 3 1.25 (1.13, 1.40) 0.0 2 0.82 (0.65, 1.04)
0.91 (0.78, 1.06)− Study type Cohort 0 − − 5 1.27 (1.15, 1.41) 0.0 4 0.91 (0.81, 1.03) 24.5 Case-control 5 2.31 (1.38, 3.86) 78.2 1 1.10 (0.42, 2.91) − 0 − − Stroke type Stroke 1 1.42 (0.79, 2.56) − 5 1.27 (1.15, 1.41) 0.0 4 0.91 (0.81, 1.03) 24.5 Ischemic stroke 1 3.43 (1.31, 9.00) − 0 − − 0 − − Hemorrhagic stroke 3 2.43 (1.16, 5.09) 81.6 1 1.10 (0.42, 2.91) − 0 − − Female Study year −1999 3 1.53 (0.52, 4.54) 71.7 6 1.65 (1.40, 1.94) 47.5 2 1.31 (0.87, 1.99)
0.86 (0.63, 1.17)− 2000− 1 2.21 (0.71, 6.87) − 0 − − 0 − − Outcome Morbidity 3 1.81 (0.72, 4.60) 69.1 3 2.65 (1.74, 4.04) 0.0 1 0.86 (0.63, 1.17) − Mortality 1 1.28 (0.22, 7.39) − 3 1.52 (1.27, 1.81) 43.1 1 1.31 (0.87, 1.99) − Study type Cohort 0 − − 5 1.78 (1.34, 2.36) 51.2 2 1.31 (0.87, 1.99)
0.86 (0.63, 1.17)− Case-control 4 1.78 (0.82, 3.86) 58.1 1 2.90 (1.10, 7.67) − 0 − − Stroke type Stroke 0 − − 5 1.78 (1.34, 2.36) 51.2 2 1.31 (0.87, 1.99)
0.86 (0.63, 1.17)− Ischemic stroke 1 2.21 (0.71, 6.88) − 0 − − 0 − − Hemorrhagic stroke 3 1.53 (0.52, 4.53) 1 2.90 (1.10, 7.67) − 0 − − Note. RR: Relative Risk; CI: Confidence Interval. Table 4. Subgroup analysis investigating the association between ever, current, and former smokers and stroke risk in other Asian countries
Sex Group Subgroup Ever smokers Current smokers Former smokers No. of
studyRR (95% CI) I2(%) No. of
studyRR (95% CI) I2(%) No. of
studyRR (95% CI) I2(%) Both Study year −1999 17 1.64 (1.38, 1.94) 94.0 14 1.64 (1.39, 1.93) 98.5 11 1.18 (1.03, 1.35) 75.4 2000− 10 2.24 (1.71, 2.93) 63.7 4 1.27 (0.99, 1.64) 96.2 2 1.28 (0.77, 2.14)
0.98 (0.91, 1.06)— Outcome Morbidity 22 1.92 (1.61, 2.29) 82.2 9 1.81 (1.44, 2.29) 99.1 6 1.01 (0.96, 1.05) 55.2 Mortality 5 1.48 (1.17, 1.88) 95.9 9 1.31 (1.14, 1.51) 87.9 7 1.20 (1.00, 1.44) 73.8 Study type Cohort 7 1.46 (1.18, 1.80) 78.0 16 1.49 (1.28, 1.72) 99.2 12 1.18 (1.03, 1.34) 73.5 Case-control 20 1.99 (1.65, 2.39) 93.9 2 2.70 (1.70,4.20)
2.50 (1.40, 4.50)— 1 0.99 (0.92, 1.06) — Stroke type Stroke 13 1.68 (1.47, 1.93) 91.7 13 1.56 (1.33, 1.83) 98.6 12 1.18 (1.03, 1.34) 73.2 Ischemic stroke 10 2.17 (1.49, 3.18) 86.9 2 1.20 (1.16, 1.24)
1.89 (1.11, 3.22)— 1 0.98 (0.91, 1.06) — Hemorrhagic stroke 4 1.62 (1.00, 2.62) 86.9 3 1.82 (0.94, 3.50) 92.6 0 — — Male Study year −1999 9 1.58 (1.14, 2.19) 92.7 10 1.54 (1.22, 1.95) 95.2 8 0.97 (0.90, 1.04) 40.9 2000− 5 1.34 (1.19, 1.51) 14.7 2 1.37 (1.15, 1.64)
0.57 (0.33, 0.99)— 2 0.98 (0.79, 1.22)
3.24 (1.79, 5.86)— Outcome Morbidity 5 2.35 (1.44, 3.83) 91.6 6 1.38 (0.91, 2.09) — 5 1.32 (0.89, 1.94) 73.8 Mortality 9 1.20 (1.15, 1.26) 36.4 6 1.28 (1.15, 1.41) 55.0 5 0.91 (0.84, 0.99) 17.8 Study type Cohort 6 1.27 (1.14, 1.42) 27.0 10 1.54 (1.24, 1.91) 95.8 9 0.97 (0.91, 1.04) 32.5 Case-control 8 1.84 (1.27, 2.65) 93.6 2 1.10 (0.40, 2.50)
0.57 (0.33, 0.99)— 1 3.24 (1.79, 5.86) — Stroke type Stroke 9 1.20 (1.15, 1.25) 35.8 11 1.44 (1.13, 1.84) — 10 1.05 (0.88, 1.25) 67.2 Ischemic stroke 2 1.32 (1.13, 1.54)
3.43 (1.31, 9.02)— 0 — — 0 — — Hemorrhagic stroke 3 2.43 (1.16, 5.09) 81.6 1 1.10 (0.40, 2.50) — 0 — — Female Study year −1999 7 1.45 (0.96, 2.17) 92.3 8 1.57 (1.46, 1.68) 46.4 6 1.07 (0.88, 1.29) 1.4 2000− 1 2.21 (0.71, 6.88) — 0 — — 0 — — Outcome Morbidity 3 1.81 (0.72, 4.60) 69.1 4 2.25 (1.38, 3.66) 68.0 3 0.96 (0.73, 1.26) 10.9 Mortality 5 1.26 (0.95, 1.66) 88.0 4 1.52 (1.29, 1.80) 15.3 3 1.17 (0.91, 1.51) 0.0 Study type Cohort 2 1.39 (0.97, 1.99)
1.81 (0.31, 10.60)— 7 1.56 (1.46, 1.67) 29.0 6 1.07 (0.88, 1.29) 1.4 Case-control 6 1.49 (0.92, 2.43) 93.5 1 2.90 (1.10, 7.70) — 0 — — Stroke type Stroke 4 1.49 (0.92, 2.43) 93.5 7 1.56 (1.46, 1.67) 29.0 6 1.07 (0.88, 1.29) 1.4 Ischemic stroke 1 2.21 (0.71, 6.88) — 0 — — 0 — — Hemorrhagic stroke 3 1.52 (0.52, 4.54) 71.7 1 2.90 (1.10, 7.70) — 0 — — Note. RR: Relative Risk; CI: Confidence Interval. Table 5. Subgroup analysis investigating the association between ever, current, and former smokers and stroke risk in Asian countries
As for current smokers, the RRs of both sexes in China ranged from 1.20 (1.16, 1,24) to 1.89 (3.22), and those of other Asian countries ranged from 1.30 (1.16, 1.45) to 2.70 (1.70, 4.20), which were approximate as that of the whole of Asia (ranged from 1.20 (1.16, 1.24) to 2.70 (1.70, 4.20)), and they did not reach statistical significance. The RR value for males ranged from 1.32 (0.57, 3.08) to 1.99 (1.18, 3.38) in China, 1.10 (0.42, 2.91) to 1.36 (1.07, 1.71) in other Asia countries, and 1.10 (0.40, 2.50) to 1.54 (1.22, 1.95) in Asia, with no statistical difference. Because of the limited number of studies on females, only two studies were described in China, with 1.55 (1.43, 1.66) and 1.60 (0.90, 2.86), which was smaller than those of other Asian countries (1.52 (1.27, 1.81) to 2.90 (1.10, 7.67)) or the whole of Asia (1.52 (1.29, 1.80) to 2.90 (1.10, 7.70)).
For former smokers, the RRs of the subgroup fluctuated around 1, with ranges in China similar to those of other Asian countries or the entire Asia region, except for some subgroups that did not contain any articles. The RRs of both sexes ranged from 0.98 (0.91, 1.06) to 1.28 (0.77, 2.14) in both China, 0.92 (0.80, 1.06) to 1.48 (0.88, 2.49) in other Asian countries, and 0.98 (1.91, 1.06) to 1.28 (0.77, 2.14) in Asia. And the RRs of males were pretty close, with 0.94 (0.83, 1.05) to 1.43 (0.71, 2.86) in China, and 0.91 (0.84, 0.99) to 1.32 (0.89, 1.94) in Asia, both except 3.24 (1.79, 5.86) for a small sample, and 0.82 (0.65, 1.04) to 1.56 (0.84, 2.90) in other Asian countries. The RRs of females in China were equal to those of other Asian countries (ranged from 0.86 to 1.31), which were also close to those of Asia (0.96 (0.73, 1.26) to 1.17 (0.91, 1.51)).
-
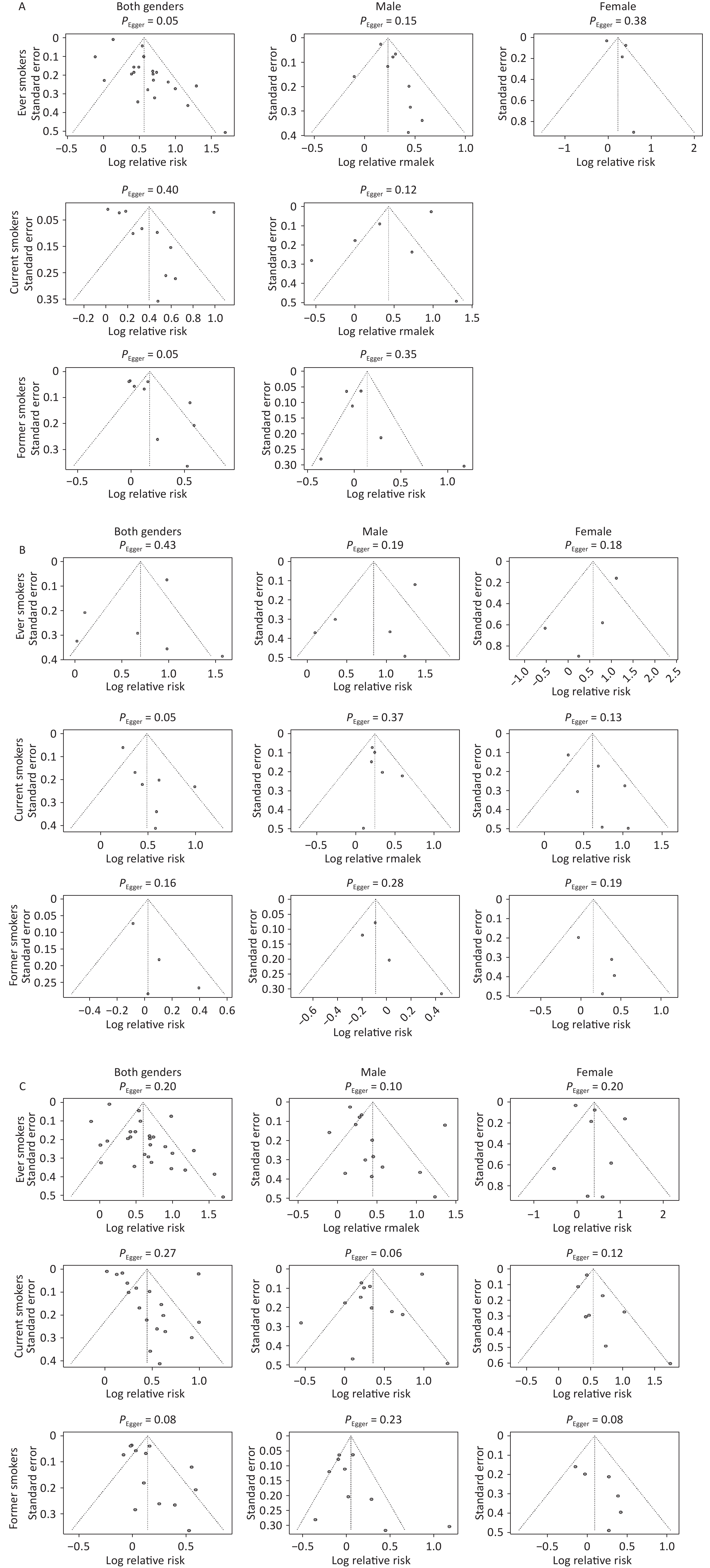
There was no statistically significant evidence of publication bias in China, other Asian countries, or all Asian countries (all Egger’s regression P > 0.05). The funnel plots are shown in Figure 2. The sensitivity analysis is shown in Supplementary Figure S1, which illustrates that the results were steady.
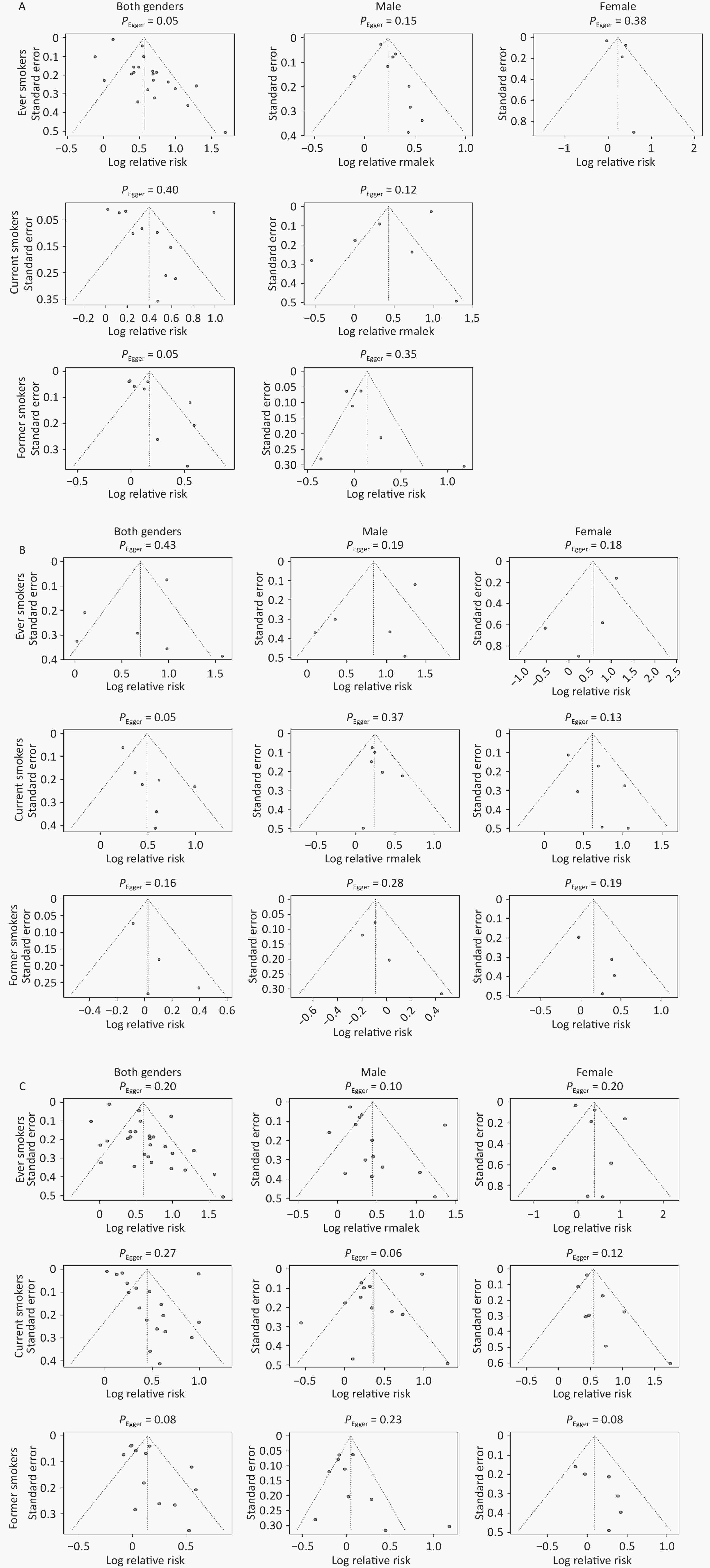
Figure 2. Funnel plots for smoking status and stroke. A: China; B: Other Asian countries; C: All Asian countries
-
This study illustrated that the RRs of ever smokers were similar between China and other Asian countries for both sexes and for females, with no statistical difference. However, the RRs in males were higher in other Asian countries than in China. Overall, neither China nor other Asian countries showed significant statistical differences compared to Asia as a whole. Furthermore, the subgroup analysis demonstrated that the RR of the morbidity group in China was smaller than that of other Asian countries, and the rest of the groups showed no statistical difference with the same subgroup. As for current smokers, the RRs in China were not statistically different from those in other Asian countries or the entire Asian region, in both sexes, males and females, and also among former smokers. Despite the heterogeneity, the RRs of further stratified analyses were stable among the different subgroups. Most studies have shown that long-term tobacco consumption is harmful to health, and quitting smoking can reduce this risk, which is consistent with the results of this study.
The RRs of smoking-related stroke in China were similar to those of other Asian countries in both sexes and females, with no statistical difference between them. However, the RRs of male ever smokers in China were slightly lower than those in other Asian countries, which was statistically different. Further subgroup analyses were conducted, and it was found that the studies from other Asian countries in the morbidity subgroup had a higher RR of 3.76 (3.02, 4.67). The same group from China had only two articles, one of which showed a statistically significant difference. The other had no statistical difference with other Asian countries, which was limited by the number of articles and requires further research in the future. Moreover, the RR of China had no statistical difference with that of the whole of Asia, further reflecting that China and the whole of Asia had relatively similar underlying health threats from smoking-related stroke risk. In this study, most pooled RR analyses indicated heterogeneity, suggesting differences in the research design, sample characteristics, and exposure definitions among the included studies. However, through subgroup analysis, we discovered that despite high I2 values, the direction of RR remained consistent across subgroups, with a relatively limited range of numerical variations, indicating a certain robustness in the association of smoking and stroke.
China and most other Asian countries are in the same tobacco epidemic stage[10], as well as ambient air pollution and indoor coal pollution[16], which have similar risk estimates for smoking-related stroke. Additionally, smoking habits and prevalence in various countries are affected by many factors, including culture, policy, and the level of economic development. In this study, we observe that the risk effects are similar, but there are subtle differences in the above effects. Furthermore, the tobacco epidemic stages in Asia and Western countries are inconsistent[10]. Additionally, ambient[13] and household air pollution[16] in Asia are more severe than those in Western countries, resulting in different accumulation effects. Thus, the RRs for smoking-related diseases differed. A previous study[17] indicated that the RR value of stroke caused by smoking in Western Europe and North America was 3.22 (2.31, 4.50), which is higher than that of China or the whole of Asia in this study. Moreover, some smokers have tried to use e-cigarettes; however, whether e-cigarettes have an impact on human health remains a subject of debate because of the strong effect of prior cigarette use as a risk factor for diseases[18].
Generally, the RRs of smoking-related stroke may be attributed to differences in the study design, sample, smoking status definition, and adjustment for confounders. Moreover, the association between smoking and stroke risk may vary across ethnic populations and be modulated by multiple biological mechanisms. On the one hand, tobacco smoke contains toxic substances that are metabolized by enzymes such as Cytochrome P450 family 2 subfamily A member 6 (CYP2A6)[19]. In Chinese populations, low CYP2A6 activity slows nicotine metabolism, prolonging toxin exposure and possibly worsening vascular injury[20]. By contrast, the Japanese and Korean populations metabolize nicotine faster, but may produce more harmful byproducts, increasing the risk of hemorrhagic stroke[21]. On the other hand, genetic factors also play a role. In Chinese populations, the 5,10-methylenetetrahydrofolate reductase (MTHFR) C677T variant increases homocysteine levels and, when combined with smoking, may increase ischemic stroke risk[22]. Meanwhile, Japanese individuals more commonly carry aldehyde dehydrogenase (ALDH2), which may impair toxin clearance and increase the risk of hemorrhagic stroke[23]. These differences may account for the variations between China and other Asian countries, particularly in terms of morbidity. In this study, Japan accounted for the majority of articles from different Asian countries, and this difference may be attributed to these mechanisms.
In Asia, smoking prevalence has decreased or plateaued among males, but has increased among females[11]. In this study, the risk estimates of smoking-induced stroke were approximately equal in males and females in all Asian countries, with males having a slightly higher risk than females in ever smokers and females having a slightly higher risk than males in current smokers and former smokers in all the Asian countries. In terms of smoking behavior, research has indicated that males typically have a higher smoking rate and intensity, an earlier age of smoking initiation, and longer smoking duration, resulting in greater cumulative tobacco exposure[24]. By contrast, among female smokers, while having a lower average cigarette consumption, the smoking rate is increasing every year[11]. In a previous study, the RR of smoking-related stroke was 1.55 in males, and 1.39 in females in China[25], or 1.36 in males, and 1.51 in females[26]. As for Japan, the RRs were 1.56 in males and 1.31 in females in Japan[27], or 1.40 in males and 1.52 in females[28], which is consistent with our study.
Regarding the biological differences between males and females, research indicates that women may be more sensitive to tobacco toxins, as smoking accelerates estrogen metabolism and weakens its protective effects on the cardiovascular system[29], while also more easily causing vasoconstriction, endothelial dysfunction, and atherosclerosis[19]. Particularly after perimenopause, the stroke risk significantly increases, suggesting that changes in sex hormones may be a key regulatory factor[30]. By comparison, male smokers are more prone to stronger inflammatory responses, such as higher levels of C-reactive protein and tumor necrosis factor-α[31] and more evident activation of coagulation factors, making them more likely to develop a hypercoagulable state[32]. Additionally, studies have found that males show more prominent smoking-induced endothelial dysfunction, increased arterial stiffness, and elevated oxidative stress levels, all of which can accelerate cerebrovascular damage[33]. Testosterone levels may further amplify the adverse effects of smoking on stroke by promoting vascular smooth muscle proliferation and lipid oxidation[34]. In summary, males and females exhibit different physiological responses to smoking exposure, which may serve as an important biological basis for the sex differences in the relative risk observed in this study.
Most Asian countries are developing countries, at critical stages of economic growth and social development. With social development, improvements in living standards, population ageing, and healthcare have shifted the burden of disease more towards Non-Communicable Chronic Diseases (NCDs) such as cancer, cerebrovascular disease, and chronic respiratory diseases. As Asia is in the rising stage of the tobacco epidemic, the burden of the diseases caused by smoking cannot be ignored.
-
This study has several limitations. First, smoking status was defined as dichotomous (ever-smokers or non-smokers), and the smoking dose (PY or CPD) was not considered, which may be more accurate in analyzing the effect. Second, most studies only reported the age range of the participants or mean ± standard deviation without dividing them into age groups; thus, it was impossible to conduct an age-stratified analysis of stroke risk. Third, this study did not include confounding factors such as socioeconomic status because RRs were calculated using multivariate analysis, which adjusted for confounding factors. Fourth, due to the limited literature available, we were unable to conduct further analyses in other specific Asian countries. However, this study has several strengths. First, this was the most integrated and longest-term Asian study on the RRs of stroke attributed by smoking. Second, stratified analyses of smoking status in China, other Asian countries, and the whole of Asia were conducted, which have not been performed in previous studies.
-
The RRs of ever smokers in both sexes combined and females separately in China did not reach statistical significance with other Asian countries, whereas those of males were statistically smaller than those of other Asian countries. Further subgroup analyses showed that the subgroup of morbidity in other Asian countries had a higher RR. The RRs of current and former smokers did not significantly differ between China and other Asian countries. The RRs of ever, current, and former smokers in China and all Asian countries were not statistically significant. Moreover, the risks in current smokers were higher than those in former smokers, illustrating that smoking cessation could reduce the risk of disease.
A Comparison of the Chinese and Asian Population Risk Effect of Active Smoking Associated Stroke
doi: 10.3967/bes2025.146
- Received Date: 2025-03-21
- Accepted Date: 2025-10-13
-
Key words:
- Active smoking /
- Stroke /
- China /
- Asian countries /
- Meta-analysis
Abstract:
The authors declare that they have no competing interests.
| Citation: | Zemin Cai, Xiaojing Guo, Xiao Zhang, Danying Li, Xiaoyue Li, Xia Wan. A Comparison of the Chinese and Asian Population Risk Effect of Active Smoking Associated Stroke[J]. Biomedical and Environmental Sciences. doi: 10.3967/bes2025.146

|

 Quick Links
Quick Links
 DownLoad:
DownLoad: