
-
Environmental disasters, including hurricanes, air pollution, and wildfires, are increasingly being recognized as significant contributors to cardiovascular morbidity and mortality[1-3]. Earthquakes, in particular, have been linked to sharp increases in acute ischemic events and sudden cardiac death, likely through acute stress responses and disruptions in access to care[4-7]. Despite these associations, their long-term effects on subclinical vascular disease remain poorly understood.
Carotid atherosclerosis constitutes an insidious and disproportionately distributed component of the worldwide cardiovascular disease spectrum, demonstrating significant geographical heterogeneity in both prevalence and clinical manifestations[8,9]. Carotid atherosclerosis persists as a formidable cerebrovascular threat, frequently precipitating devastating ischemic strokes[10]. Compelling epidemiological data have elucidated profound sex-specific divergences in the presentation and management of cerebrovascular disease. Women frequently manifest non-classical stroke symptoms, contributing to delayed recognition, prolonged hospital arrival times, and subsequent treatment delays relative to their male counterparts. These differences also extend to carotid atherosclerotic diseases. Despite these distinctions, women are less likely to receive guideline-directed medical therapy for cardiovascular risk factor modification than men, underscoring a critical gap in sex-equitable care[11].
Seismic events have profound humanitarian consequences, accounting for more than 100,000 annual fatalities[12]. Low-income nations bear a disproportionate burden of this hazard owing to inadequate construction regulations and underdeveloped emergency response systems[13]. Existing research remains notably deficient in rigorous investigations of earthquake-related atherogenesis, particularly regarding carotid atherosclerotic manifestations[14].
To address this, we conducted a prospective study in a cohort of northern Chinese women using serial high-resolution carotid ultrasonography. By adjusting for traditional cardiovascular risk factors, we aimed to examine whether earthquake exposure was associated with accelerated carotid atherosclerosis, offering new insights into disaster-related vascular risk and long-term prevention strategies.
-
This study drew participants from two community-based cohorts in Tangshan, Hebei Province, China: the Jidong and Kailuan cohorts, both of which are situated within the seismically active North China tectonic belt and in proximity to the epicenter of the 1976 Tangshan earthquake (magnitude 7.8), one of the deadliest natural disasters of the twentieth century that claimed over 242,000 lives and destroyed approximately 90% of the city’s infrastructure.
The Jidong cohort study is an ongoing community-based prospective study established in the Caofeidian district of Tangshan, approximately 60 km from the earthquake epicenter. Using a cluster sampling strategy, 9,078 residents were recruited between July 2013 and August 2014. The participants underwent annual physical examinations and provided demographic, behavioral, and clinical data through face-to-face interviews conducted by trained research nurses, supplemented by laboratory assessments.
The Kailuan cohort was originally established among employees and retirees of Kailuan (Group) Co., Ltd., a large state-owned coal mining enterprise in Tangshan. Participants were systematically selected from this cohort using a stratified random sampling approach based on the 2010 Chinese National Census data for age and sex distribution. Between June 2010 and June 2011, 5,440 eligible individuals aged 40 years and older were enrolled after applying pre-specified inclusion criteria.
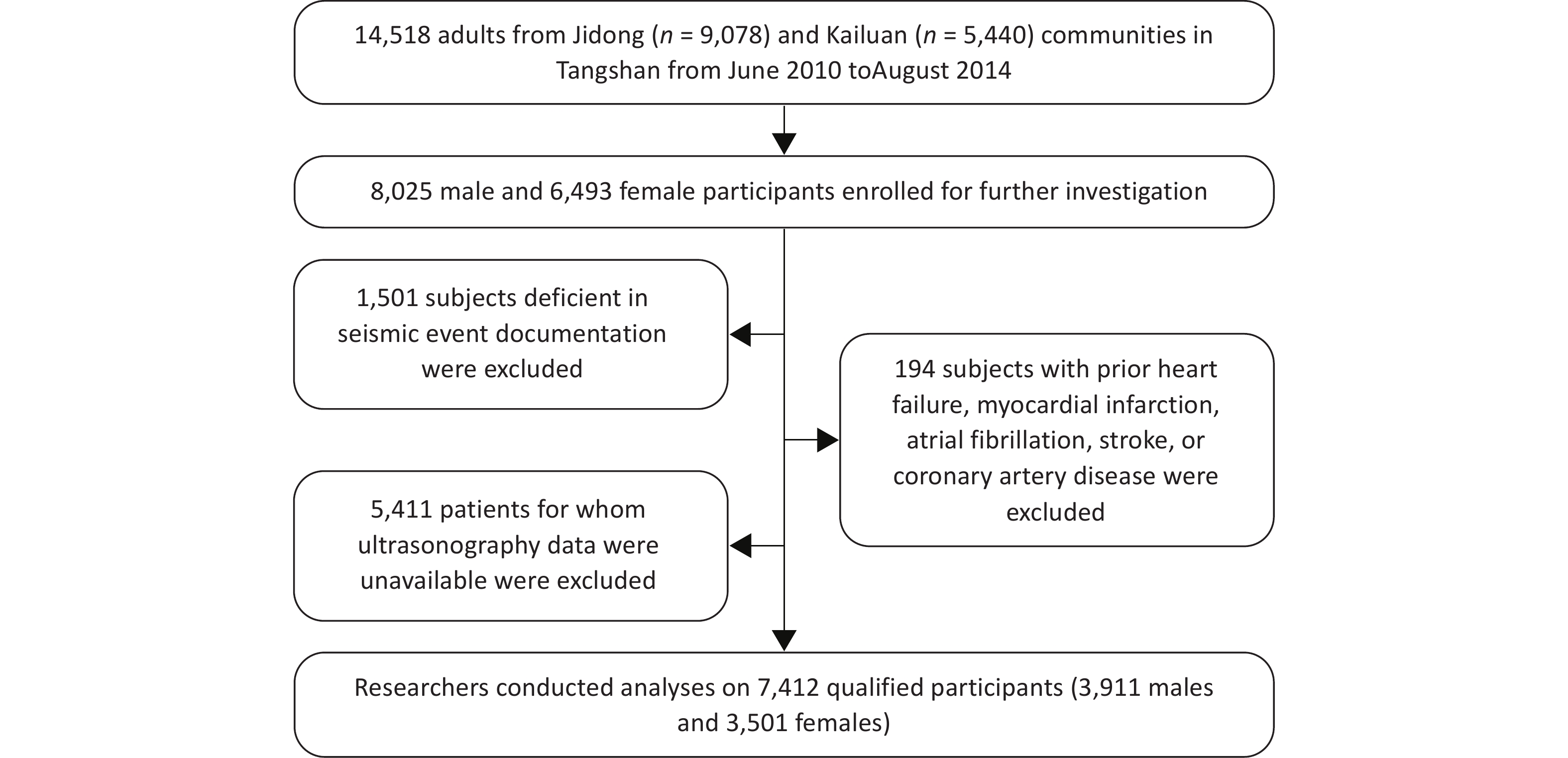
Across both cohorts, a combined total of 14,518 adults (8,025 males and 6,493 females) were initially considered for inclusion. Participants were subsequently excluded for the following reasons: 1,501 individuals lacked sufficient documentation of residential proximity to the earthquake zone; 5,411 had no available carotid ultrasonography data; and 194 had a history of pre-existing cardiovascular conditions, including heart failure, myocardial infarction, atrial fibrillation, stroke, or coronary artery disease. The final analytical cohort comprised 7,412 participants (Figure 1).
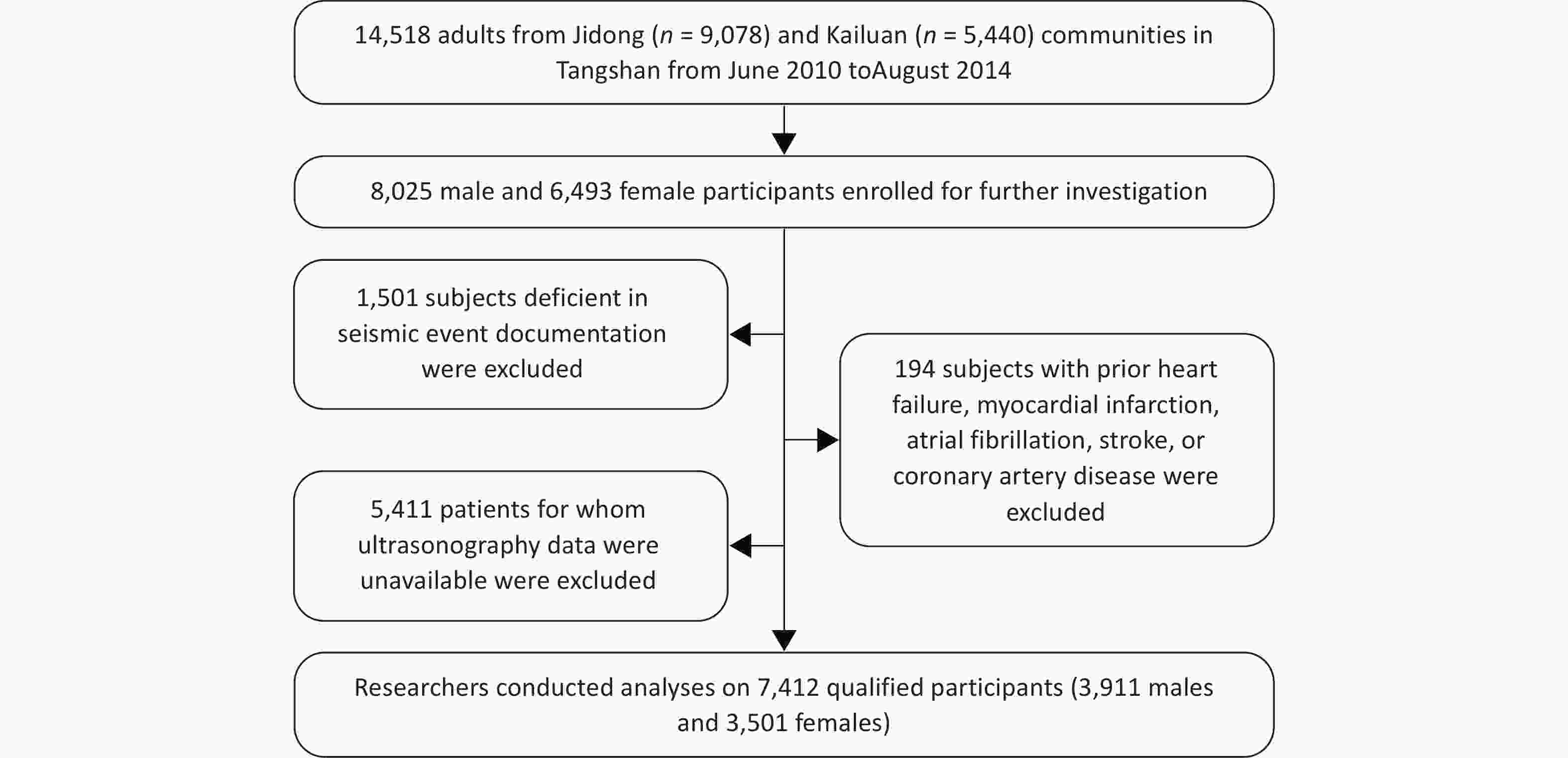
Figure 1. Flow chart of population selection.
This study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Institutional Review Boards of both Jidong Oilfield Staff Hospital and Kailuan General Hospital. Written informed consent was obtained from all participants before enrollment.
-
This study conducted a comparative analysis of two discrete cohorts: individuals with documented exposure to the 1976 Tangshan earthquake and demographically matched controls without prior earthquake-related trauma. Through standardized questionnaires, participants self-reported their 1976 geographic status with the query, “Confirm your presence in the 1976 Tangshan earthquake disaster zone.” Affirmative respondents were further prompted to specify their approximate distance from the epicenter, enabling a binary classification into earthquake and non-earthquake zone cohorts.
-
The primary outcome of this investigation was the incidence of carotid atherosclerotic plaque formation, which was assessed bilaterally in the common carotid arteries. The presence of carotid artery plaques was determined using bilateral duplex ultrasonography (Philips iU-22; Bothell, WA, USA). Two accredited vascular sonographers, blinded to participants’ demographic and clinical data, independently performed assessments to ensure an objective evaluation. The secondary outcome was cardiovascular disease (CVD) risk, including heart failure, myocardial infarction, atrial fibrillation, stroke, and coronary artery disease (Supplementary Table S1).
-
Baseline characteristics, modifiable risk factors, and other relevant data were assessed using standardized questionnaires. The potential confounders included age, sleep duration, menopause, educational level, income, hypertension, diabetes, dyslipidemia, alcohol consumption, smoking, and exercise intensity. The age at the time of the earthquake was quantitatively assessed. Household economic data were collected monthly per capita and dichotomized at the ¥3,000 threshold. Educational attainment was stratified into three categories: elementary education or lower, middle school, and college or higher. Binary classification (present/absent) was applied to smoking and alcohol consumption behaviors as well as menopausal status. Hypertension status was required to be verified by a clinical diagnosis, by systolic blood pressure (SBP) exceeding 140 mmHg, by diastolic blood pressure (DBP) exceeding 90 mmHg, or by current use of antihypertensive medications. Diabetes mellitus classification was based on fasting glucose ≥7.0 mmol/L, use of glucose-lowering medication, or a physician-confirmed diagnosis. Dyslipidemia was identified through prior diagnosis, abnormal lipid levels (total cholesterol [TC] ≥ 5.18 mmol/L, triglycerides [TG] ≥ 1.7 mmol/L, high-density lipoprotein-cholesterol [HDL-C] < 1.04 mmol/L, or low-density lipoprotein-cholesterol [LDL-C] ≥ 3.37 mmol/L), or active lipid-modifying treatment.
-
Descriptive statistics are presented as means with standard deviations (SDs) for continuous variables and frequencies with percentages for categorical variables. The continuous parameters assessed in our study followed a standard normal distribution. Group comparisons between the earthquake-exposed and non-exposed participants were conducted using two independent sample t-tests for continuous variables (age and sleep duration) and the chi-square test or Fisher’s exact test for the remaining categorical variables.
Multivariate logistic regression was used to assess the association between earthquake exposure and carotid atherosclerosis. The initial model was not adjusted for the potential confounding factors. Subsequent models were adjusted for sociodemographic factors (age, education, and income), followed by the incorporation of a comprehensive set of available clinical parameters and behavioral covariates.
Subgroup logistic regression models were also employed to examine the association between earthquake exposure and CVD risk across the pre-specified demographic and clinical subpopulations.
Odds ratios (ORs) with 95% confidence intervals (CIs) are reported. Statistical significance was defined as a two-sided P-value of < 0.05. Data analysis was conducted using the SAS software (version 9.4; SAS Institute Inc., Cary, North Carolina, USA).
-
Table 1 summarizes the baseline demographic, clinical, and behavioral characteristics of the 7,412 study participants stratified by earthquake exposure status. Among them, 52.7% (n = 3,909) were classified as earthquake-exposed and 47.3% (n = 3,503) as unexposed. Compared with the unexposed group, exposed individuals were slightly older (median age: 53.95 vs. 52.83 years; P < 0.001), had shorter average sleep duration (6.61 ± 1.27 vs. 6.73 ± 1.35 hours; P = 0.0005), and included a higher proportion of men (56.35% vs. 48.77%; P < 0.001). Cardiometabolic comorbidities were more common in the exposure group, including higher rates of hypertension (43.47% vs. 24.46%, P < 0.001) and diabetes (10.62% vs. 8.30%, P < 0.001), but not dyslipidemia (47.95% vs. 39.70%, P = 0.38). Socioeconomic characteristics differed markedly between the groups. A lower proportion of the exposed group had attained a college-level education or higher (4.43% vs. 32.33%), whereas a greater percentage reported a higher income status (75.26% vs. 54.68%; P < 0.001). The smoking prevalence was modestly higher in the exposed group (31.70% vs. 28.82%; P = 0.0076), whereas alcohol consumption was substantially lower (3.40% vs. 25.80%; P < 0.001). Differences were also noted in physical activity patterns, with the exposed group being significantly more likely to engage in high-intensity exercise (9.44% vs. 1.51%; P < 0.001). These findings suggest that distinct demographic, clinical, and lifestyle profiles are associated with earthquake exposure, underscoring the need for careful adjustment in subsequent analyses of atherosclerotic risk. Additionally, the sex-specific baseline characteristics of the clinical and socioeconomic risk factors are presented in Supplementary Tables S2 and S3.
Characteristics Total(N = 7,412) EarthquakeYes (n = 3,908) EarthquakeNo (n = 3,504) P-value Age (years ± SD) 53.42 ± 10.03 53.95 ± 10.64 52.83 ± 9.27 < 0.001 Sleep (hours ± SD) 6.68 ± 1.31 6.61 ± 1.27 6.73 ± 1.35 0.0005 Male (n, %) 3,911 (52.77) 2,202 (56.35) 1,709 (48.77) < 0.001 Hypertension (n, %) 2,556 (34.48) 1,699 (43.47) 857 (24.46) < 0.001 Diabetes (n, %) 706 (9.53) 415 (10.62) 291 (8.30) < 0.001 Dyslipidemia (n, %) 3,265 (44.05) 1,874 (47.95) 1,391 (39.70) 0.38 Education (n, %) < 0.001 Illiteracy/Primary 2,339 (31.56) 1,924 (49.23) 415 (11.84) Middle school 3,766 (50.81) 1,810 (46.32) 1,956 (55.82) College or above 1,307 (17.63) 174 (4.45) 1,133 (32.33) Income (n, %) < 0.001 < ¥3000 2,513 (33.90) 963 (24.64) 1,550 (44.24) ≥ ¥3000 4,857 (65.53) 2,941 (75.26) 1,916 (54.68) Smoking (n, %) 2,249 (30.34) 1,239 (31.70) 1,010 (28.82) 0.0076 Drinking (n, %) 1,037 (13.99) 133 (3.40) 904 (25.80) < 0.001 Exercise (n, %) < 0.001 Low intensity 2,457 (33.15) 1,179 (30.17) 1,278 (36.47) Modest intensity 3,874 (52.27) 1,783 (45.62) 2,091 (59.67) High intensity 422 (5.69) 369 (9.44) 53 (1.51) Note. SD = standard deviation. Table 1. Baseline characteristics of participants according to earthquake exposure
To balance covariates between groups and more accurately assess the independent effect of earthquake exposure, while minimizing bias arising from older age and a higher burden of baseline comorbidities in the exposed group, we performed propensity score matching. The baseline characteristics after matching are presented in Supplementary Table S4.
-
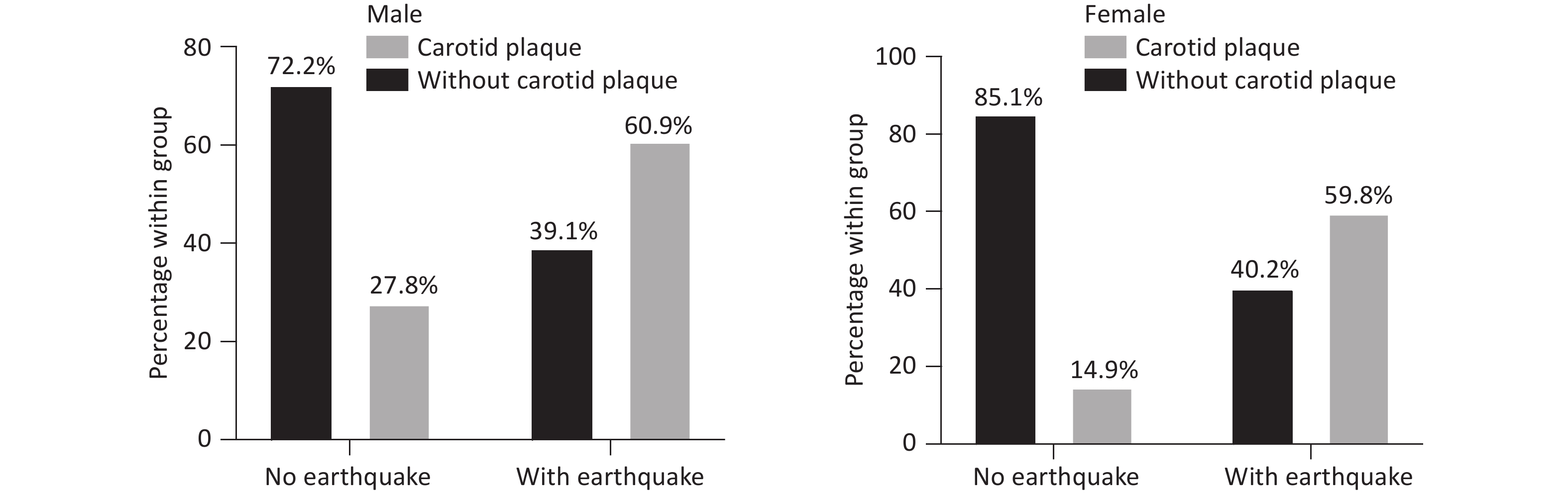
Both male and female participants demonstrated increased carotid plaque prevalence following seismic exposure. As shown in Figure 2, the absolute increase in plaque prevalence associated with earthquake exposure was 33.1% in men and 44.9% in women.
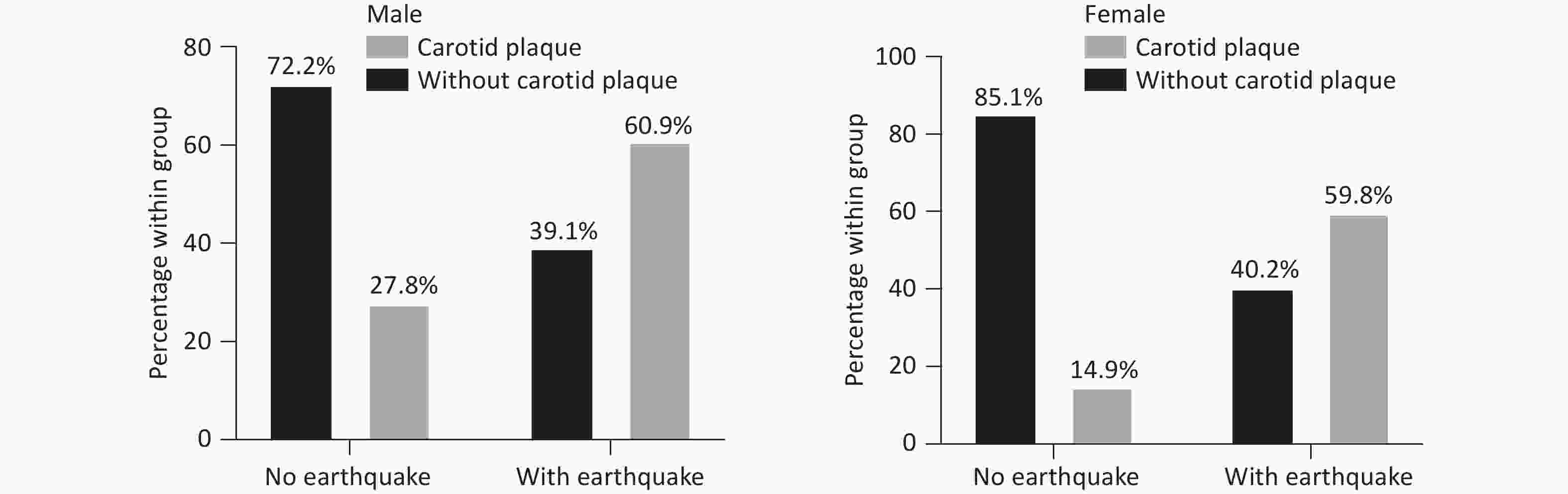
Figure 2. Distribution of carotid atherosclerosis by earthquake exposure. The figure presents a comparative analysis of carotid plaque prevalence by sex, stratified by earthquake exposure status.
-
Logistic regression analysis revealed an association between earthquake exposure and carotid atherosclerosis in both sexes (Table 2). In the general population, the unadjusted model showed substantially higher odds of plaque formation among exposed participants than among unexposed participants (OR = 2.78, 95% CI: 2.34–3.31; P < 0.001). This association remained robust after adjustment for age, education, and income (Model 1: OR = 2.65, 95% CI: 2.13–3.29; P < 0.001) and persisted following further adjustment for cardiometabolic conditions and lifestyle factors (Model 2: OR = 1.66, 95% CI: 1.30–2.13; P < 0.001), although with partial attenuation. Among women, the unadjusted model showed substantially elevated odds of plaque formation in exposed compared to unexposed participants (OR = 2.91, 95% CI: 2.47–3.42; P < 0.001). This association was maintained after adjustment for age, education, and income (Model 1: OR = 3.29, 95% CI: 2.73–3.98; P < 0.001) and remained statistically significant following additional adjustment for cardiometabolic conditions and lifestyle factors (Model 2: OR = 2.32, 95% CI: 1.78–3.02; P < 0.001). Among men, earthquake exposure was similarly associated with increased plaque odds in the unadjusted model (OR = 2.29, 95% CI: 1.75–3.01; P < 0.001). The association attenuated progressively with sequential covariate adjustment (Model 1: OR = 1.60, 95% CI: 1.16–2.21; P = 0.004), and reached borderline significance in the fully adjusted model (Model 2: OR = 1.38, 95% CI: 0.99–1.93; P = 0.060). The results of propensity score matching were consistent with those of the primary analysis (Supplementary Table S5).
Sex Earth
quakeOR (95% CI) Unadjusted P-value Model 1 P-value Model 2 P-value Female No Ref Ref Ref Yes 2.91 (2.47–3.42) < 0.001 3.29 (2.73–3.98) < 0.001 2.32 (1.78–3.02) < 0.001 Male No Ref Ref Ref Yes 2.29 (1.75–3.01) < 0.001 1.60 (1.16–2.21) 0.004 1.38 (0.99–1.93) 0.060 General population No Ref Ref Ref Yes 2.78 (2.34–3.31) < 0.001 2.65 (2.13–3.29) < 0.001 1.66 (1.30–2.13) < 0.001 Note. Model 1 was adjusted for age, education and income. Model 2 was adjusted for age, education, income, hypertension, diabetes, dyslipidemia, drinking, smoking, and exercise. CI = confidence interval; OR = odds ratio; Ref = reference. Table 2. Association between earthquake experience and carotid atherosclerosis formation
To further clarify the association between earthquake exposure and atherosclerotic plaque burden, we analyzed the number of plaques. In both the overall population and sex-stratified analyses, participants exposed to the earthquake had a higher risk of high plaque burden (≥2 plaques) than those without earthquake exposure. This association remained significant after adjusting for potential confounders (Supplementary Table S6).
-
Multivariate Cox regression analysis demonstrated that seismic exposure was a significant independent predictor of incident CVD in the entire cohort (P < 0.001; Table 3). In contrast, after full covariate adjustment, earthquake exposure was not independently associated with CVD risk in male participants (P = 0.500). The results of propensity score matching were consistent with those of the primary analysis (Supplementary Table S7).
Sex Earthquake OR (95% CI) Unadjusted P-value Adjusted P-value Female No Ref Ref Yes 2.29 (1.92–2.76) < 0.001 2.06 (1.66–2.55) < 0.001 Male No Ref Ref Yes 2.17 (1.90–2.47) < 0.001 1.06 (0.89–1.27) 0.500 Note. Adjusted for age, education, income, hypertension, diabetes, dyslipidemia, drinking, smoking, and exercise. CI = confidence interval; OR = odds ratio; Ref = reference. Table 3. CVD risk following earthquake exposure
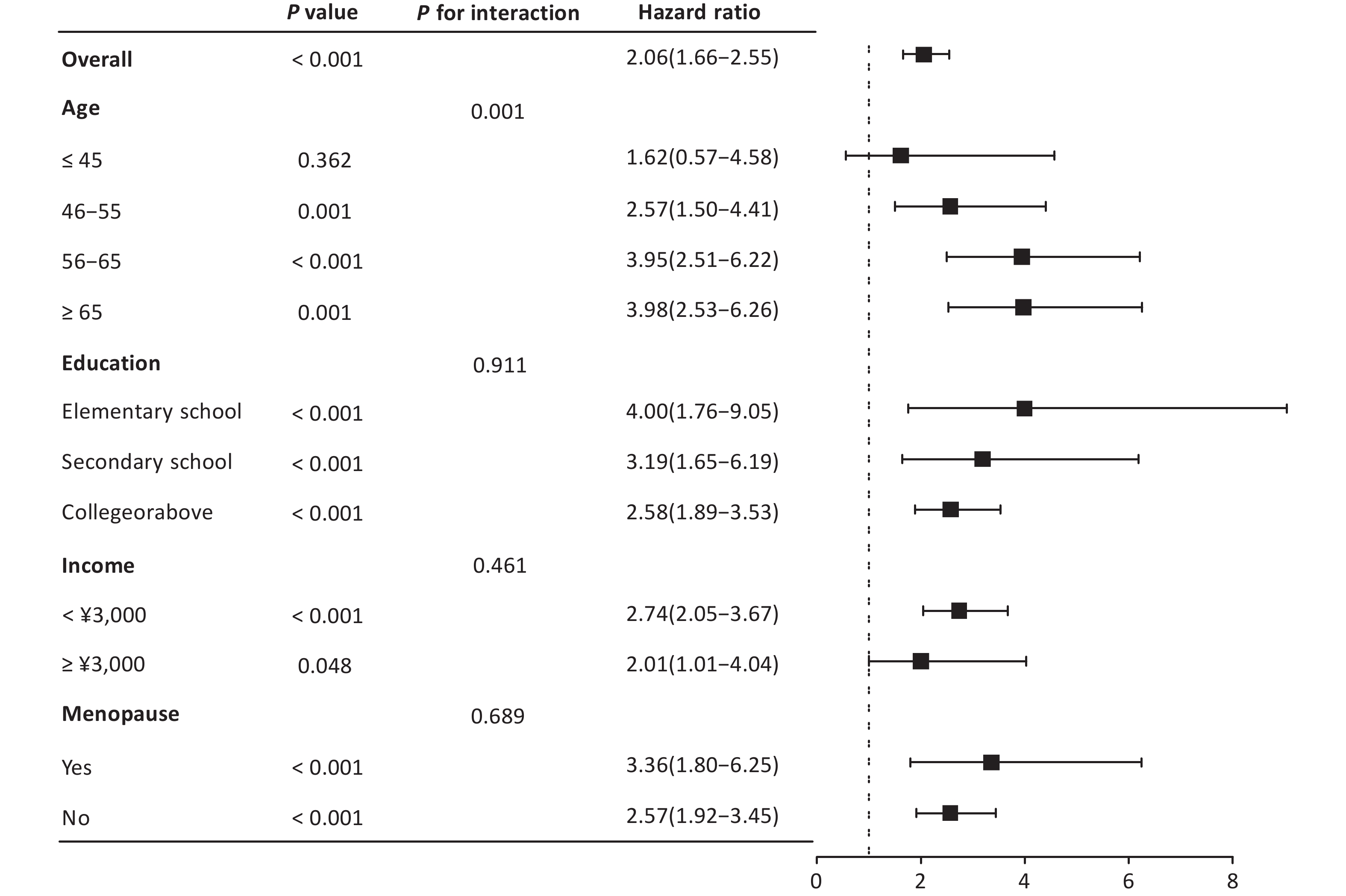
The Cox regression subgroup analysis (Figure 3) in females revealed significant associations between various demographic factors and CVD risk. Overall, the hazard ratio (HR) was 2.06 (95% CI: 1.66–2.55, P < 0.001), indicating a substantially elevated risk. Age stratification revealed a statistically significant monotonic increase in CVD risk across successive age deciles (P = 0.001). The hazard ratios exhibited a progressive escalation, commencing with a non-significant elevation among the youngest cohort (≤45 years: HR = 1.62, 95% CI: 0.57–4.58, P = 0.362), followed by increases in older age strata (46–55 years: HR = 2.57, 95% CI: 1.50–4.41, P = 0.001; 56–65 years: HR = 3.95, 95% CI: 2.51–6.22, P < 0.001). The risk plateaued in the geriatric population (≥ 65 years: HR = 3.98, 95% CI: 2.53–6.26, P = 0.001). Educational attainment showed an inverse relationship with CVD risk (P for interaction = 0.911), with hazard ratios progressively attenuating across ascending educational strata. The most pronounced risk elevation manifested among those with only elementary-level education (HR: 4.00, 95% CI: 1.76–9.05, P < 0.001), followed by secondary education completers (HR: 3.19, 95% CI: 1.65–6.19, P < 0.001). University-educated individuals exhibited the most modest, yet still statistically significant (HR: 2.58, 95% CI: 1.89–3.53, P < 0.001). This socioeconomic stratification was further corroborated by income-based analyses (P for interaction = 0.461), revealing a greater relative hazard among economically disadvantaged individuals (HR: 2.74, 95% CI: 2.05–3.67, P < 0.001) compared to high-income counterparts (HR: 2.01, 95% CI: 1.01–4.04, P = 0.048). Both postmenopausal (HR: 3.36, 95% CI: 1.80–6.25, P < 0.001) and premenopausal women (HR: 2.57, 95% CI: 1.92–3.45, P < 0.001) exhibited elevated risks. These findings underscore the fact that older age, lower educational attainment, lower income, and menopause are associated with a disproportionately higher risk of CVD in the female population.
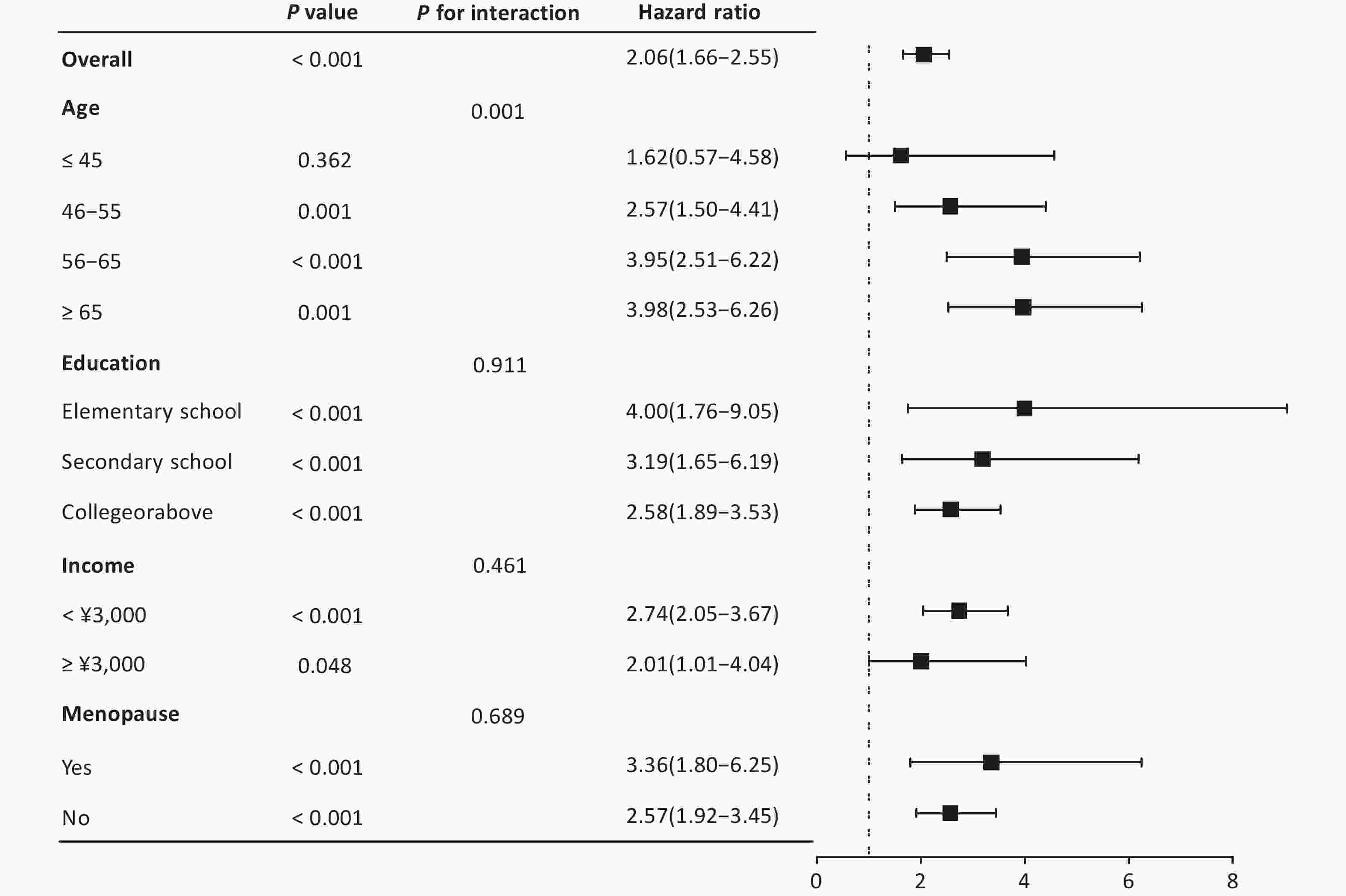
Figure 3. Subgroup analysis of CVD risk factors in women. Hazard ratios for cardiovascular risk factors in the female population, comparing the earthquake-exposed and unexposed cohorts, are shown in the figure.
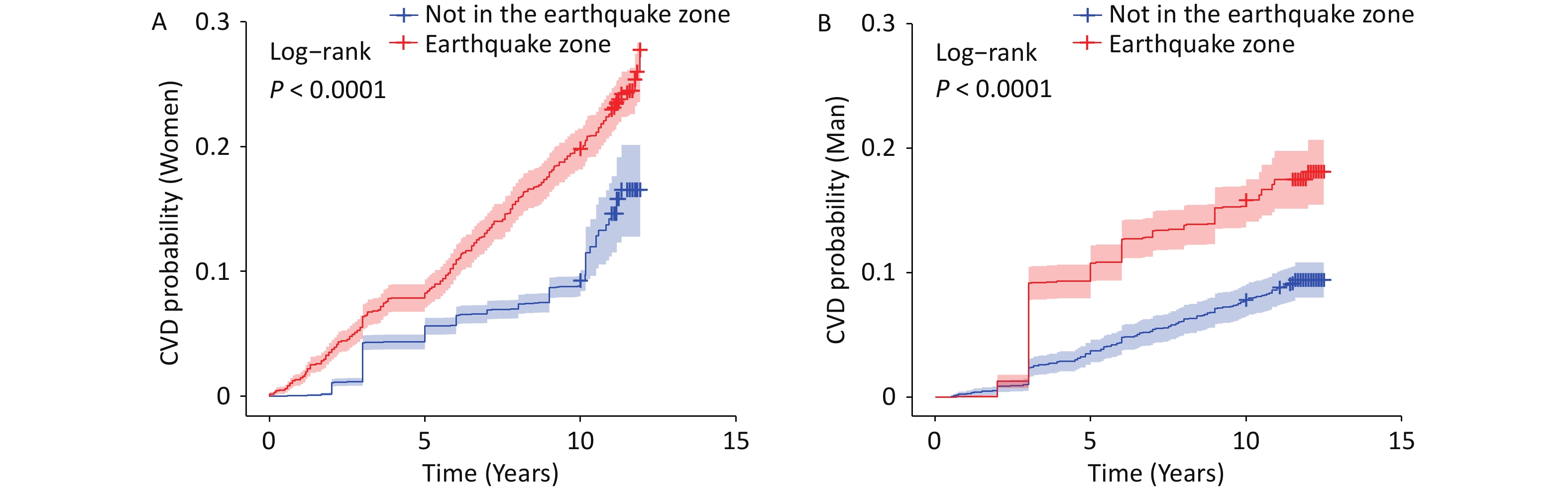
Further analyses demonstrated a significant association between earthquake exposure and the subsequent CVD risk. The Kaplan–Meier curves showed that in both men and women, individuals exposed to the earthquake experienced a progressive increase in CVD incidence over time, with a more pronounced risk among women (Figures 4A and 4B). After propensity score matching, this association was evident in women, whereas the KM curve for men was not statistically significant (Supplementary Figure S1). This divergence suggests that the relationship between earthquake exposure and CVD risk is more robust and independent in women.
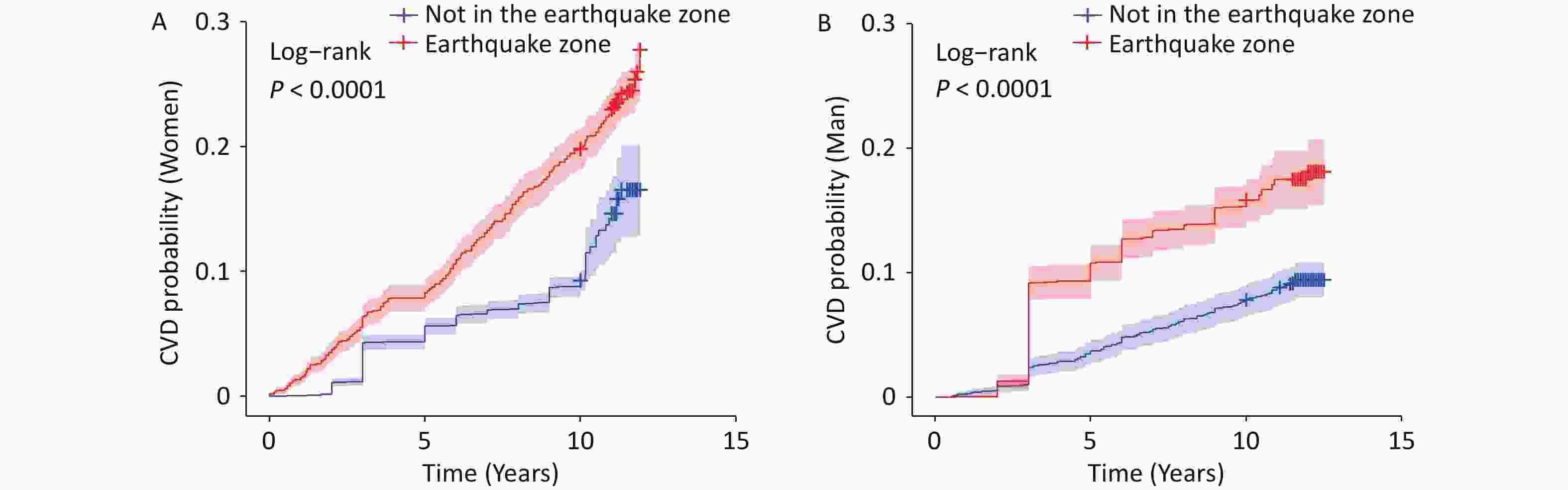
Figure 4. Kaplan–Meier curve of cardiovascular disease risk by earthquake exposure. This figure shows the cumulative incidence of cardiovascular disease (CVD) stratified by earthquake exposure. The x-axis represents the number of years since enrollment. T0 was defined as the baseline examination date (since 2010), and incident CVD events were prospectively ascertained during the follow-up.
-
This study provides evidence of a significant association between exposure to the 1976 Tangshan earthquake and an increased risk of carotid atherosclerosis and incident cardiovascular disease, with a more consistent and independent association observed in women than in men. While the male cohort showed attenuation of the association with atherosclerosis after full covariate adjustment, a robust sex-specific effect was evident for CVD outcomes, with earthquake exposure remaining a significant independent predictor in women but not in men. Subgroup that provided further evidence of the association between seismic events and CVD risk in the female population. These findings corroborate the existing epidemiological evidence demonstrating an association between psychological trauma and adverse cardiovascular sequelae, implying that catastrophe-induced psychological distress may precipitate enduring vascular manifestations[15-18].
Seismic catastrophes may trigger dual pathogenic pathways via distinct mechanisms. Traumatic bereavement may engender profound loneliness and social isolation, whereas direct psychophysiological trauma from a catastrophic exposure is an independent stress vector[19]. Both pathways represent significant psychosocial stressors with well-characterized biological correlates in contemporary populations[17].
Transient stress reactivity, which is typically elicited by natural calamities or major life events, is significantly associated with short-term cardiovascular morbidity. In contrast, prolonged stress responses, including but not limited to traumatic bereavement, may induce endothelial impairment, chronic inflammation, aberrant immunomodulation, hypothalamic-pituitary-adrenal axis dysregulation, and sympathovagal imbalance, which are established contributors to vascular defects such as atherogenesis[17,18].
The emergence of post-traumatic stress disorder (PTSD) after earthquakes requires clinical consideration. Women have been shown to exhibit a higher propensity than men to develop clinically significant PTSD symptoms following seismic events[20]. The durable PTSD symptom profile observed longitudinally after natural disasters was strongly correlated with trauma exposure gradients[21]. Epidemiologic studies have revealed significant geographic heterogeneity in the PTSD burden among seismic survivors, with hyperendemic regions exceeding 60% prevalence compared to more moderate rates documented in populations experiencing single catastrophic earthquake events, such as those observed in Asian cohorts[22]. PTSD independently confers an increased risk of major adverse cardiovascular events (MACE), especially in women[23-26]. Proposed mechanisms include the acceleration of conventional cardiometabolic risk factors (diabetes mellitus, hypertension, and dyslipidemia)[23] as well as neurocardiac pathways involving autonomic dysfunction, neural dysregulation, and systemic inflammation[24-26]. Women exhibit both a higher prevalence of comorbid major depressive disorder and enhanced susceptibility to PTSD following traumatic events, which may partly account for the sex-differential CVD risk observed in the present study[27]. PTSD, particularly when concurrent with depressive disorder, has been associated with premature mortality in women and predisposes them to hypertension, CVD, and diabetes mellitus[28]. Evidence from midlife women further suggests that PTSD may contribute to carotid atherosclerotic pathogenesis and is associated with a substantially elevated cardiovascular risk[29]. However, it should be acknowledged that the present study did not directly measure PTSD or psychological stress levels in participants; therefore, the role of PTSD as a mediating pathway cannot be confirmed and represents an important avenue for future investigation.
However, the clinical implications of these findings require further investigation. Disaster survivors may require cardiovascular monitoring beyond traditional risk factor assessments, particularly women with prolonged trauma exposure. Given that psychological stress appears capable of influencing vascular pathology through pathways that are partially independent of conventional metabolic risk factors, post-disaster clinical protocols may benefit from incorporating psychometric evaluations alongside standard biomarker profiling, including the assessment of neuroinflammatory mediators[17,18] and maladaptive behavioral patterns, such as sleep disturbance and social withdrawal[30].
Regarding atherosclerotic plaque findings, both male and female participants showed increased carotid plaque prevalence associated with earthquake exposure. The point estimates suggested a numerically larger effect in women (44.9% increase) than in men (33.1% increase). However, given the overlapping confidence intervals in the fully adjusted models and the absence of a statistically significant sex-by-exposure interaction, this descriptive difference should be interpreted cautiously. The most compelling evidence for sex specificity in this study lies in the CVD outcome analyses, in which earthquake exposure remained an independent predictor in women across all adjusted models but not in men. This pattern may reflect the greater vulnerability of women to trauma-related psychophysiological stress responses, including PTSD and comorbid depression, which have been shown to exert particularly pronounced effects on cardiovascular health in female populations. Potential explanations for the attenuation of the plaque association in men include greater confounding by cardiometabolic risk factors and the possible healthy-survivor effect, whereby men with more severe vascular consequences of earthquake exposure may have experienced higher early mortality and thus been underrepresented in the analytical cohort.
-
The findings of this study should be interpreted with several constraints. First, the retrospective nature of exposure ascertainment introduces potential recall bias, as the participants’ ability to accurately reconstruct their residential proximity to the 1976 seismic epicenter may have been compromised by a latency of approximately four decades between exposure and enrollment. Second, the exclusion of a substantial number of participants owing to missing seismic exposure documentation or unavailable carotid ultrasonography data may limit the generalizability of the findings to broader populations. Third, baseline comparisons revealed statistically significant differences between the earthquake-exposed and non-exposed groups across several key characteristics, including age, educational attainment, income level, hypertension prevalence, and alcohol consumption. These imbalances indicate that the two groups were not fully comparable at baseline, which may reflect the underlying demographic and geographic differences between the Jidong and Kailuan communities rather than the consequences of a formally matched design. Although exposed individuals had a higher burden of cardiometabolic risk factors at baseline, the association between earthquake exposure and incident CVD persisted after multivariate adjustment, indicating that the increased risk cannot be fully explained by baseline health status alone. To address this, multivariable logistic and Cox regression models were employed with sequential covariate adjustment, incorporating socioeconomic variables (age, education, and income) in Model 1 and additional cardiometabolic and lifestyle factors (hypertension, diabetes, dyslipidemia, smoking, and alcohol use) in Model 2. The persistence of statistically significant associations in the fully adjusted models, particularly among women, suggests that the observed effects are not entirely attributable to the measured confounders.
Nevertheless, residual confounders from unmeasured variables, including dietary patterns, non-seismic psychological stressors, occupational exposure, and genetic predisposition, could not be excluded. Fourth, the substantial time elapsed between the earthquake (1976) and participant enrollment (2010–2014) raises the possibility of a healthy survival effect, whereby individuals who experienced the most severe cardiovascular consequences of seismic exposure, particularly men, may have died before study recruitment, potentially resulting in an underestimation of the true effect sizes and contributing to the attenuated associations observed in the male subgroup. Collectively, these limitations underscore the need for prospective studies to validate and expand our findings.
-
This study demonstrated a substantive independent correlation between catastrophic seismic events and the expedited progression of carotid atherosclerosis and CVD pathology, which persisted after comprehensive adjustment for potential confounders. These findings establish earthquake exposure as a novel and independent risk factor of atherogenesis in women. Future mechanistic investigations should elucidate the long-term pathophysiological pathways that orchestrate vascular pathology induced by seismic trauma, thereby guiding preemptive strategies against atherosclerosis.
HTML
Study Population
Exposure and Controls
Outcome
Covariates
Statistical Analysis
Baseline Characteristics of Participants According to Earthquake Exposure
Unadjusted Association between Carotid Atherosclerosis and Seismic Exposure
Crude and Adjusted Model for Carotid Atherosclerosis Outcome
Subgroup Analysis of Cardiovascular Disease Risk in Women
Limitations
Competing Interests The authors declare that they have no potential competing interests.
Authors’ Contributions JZ, YZ, and BFC participated in the study design, project administration, writing, review, and editing. HX and YW participated in the data collection. KNZ, YHL, and WQW performed statistical analyses. HX and BYG drafted the manuscript. All the authors have read and approved the final manuscript.
Date Sharing The raw data supporting the conclusions of the current study are available from the corresponding author upon request. The supplementary materials will be available in www.besjournal.com.
&These authors contributed equally to this work.

 Quick Links
Quick Links
 DownLoad:
DownLoad: