
-
Cardiorespiratory fitness (CRF) is defined as the ability of the circulatory, respiratory, and muscular systems to deliver oxygen during prolonged, sustained, and dynamic exercises of moderate to vigorous intensity[1]. Previous studies have shown that, compared with traditional risk factors, such as hyperlipidemia, obesity, hypertension, and insulin resistance, CRF has not been routinely used in clinical practice, although it is a stronger predictor of cardiovascular disease (CVD) and all-cause mortality. Moreover, the associations between CRF and mortality risk are inverse, independent, and graded across age ranges, including individuals in their 70s and 80s, men, women, and all races. Higher CRF is associated with lower all-cause mortality and CVD risk[2]. However, whether CRF ultimately influences all-cause mortality and life expectancy by mediating these chronic diseases and the causal relationship between CRF and longevity remain unclear. Therefore, it is crucial to investigate the association between CRF and all-cause mortality. Furthermore, previous studies did not consider the causal relationship between CRF and all-cause mortality.
Accordingly, the present study investigated the association between different CRF levels and genetic susceptibility to all-cause mortality and life expectancy. We used a two-sample Mendelian randomization (MR) approach with genetically predicted fitness from the UK Biobank (UKB) as an instrumental variable[3], supplemented by genetic case-control data from collaborative research projects targeting the same health status. Our main analyses were performed using data from the UKB and the National Health and Nutrition Examination Survey (NHANES). We aimed to strengthen the basis for inferring causal relationships by combining observational epidemiological findings with MR methods.
The UKB was a large-scale prospective cohort study. From an initial enrollment of 502,486 participants between 2006 and 2010, data from 424,544 were excluded due to missing CRF-related information, along with an additional 6,160 lacking essential baseline covariates. As such, the final analytical UKB cohort comprised 71,782 eligible participants. NHANES is a nationally representative survey that used a complex, multistage, and stratified design. Data extracted from the 1999 to 2004 cycle included 36,483 participants. Following the exclusion of 32,059 individuals with insufficient data to estimate maximal oxygen consumption (VO2max) for CRF evaluation and 1,033 with missing mortality records or covariates, data from 3,391 individuals were ultimately retained for analysis.
CRF was defined as the estimated VO2max. In the UKB, CRF is assessed using a submaximal bicycle power test[4]; in NHANES, a submaximal treadmill exercise protocol was used[5]. VO2max was estimated as VO2max = 7+10.8 × (workload)/weight[6] and expressed as VO2maxtbm and VO2maxffm. Covariates included age, sex, race, socioeconomic indicators (Townsend Deprivation Index [TDI]/Poverty Income Ratio [PIR]), education, smoking status, alcohol consumption, diabetes, hypertension, body mass index (BMI), and fat mass.
In the present study, the genetic determinants of CRF were analyzed using genome-wide association study (GWAS) data from participants of European descent in the UKB (n = 69,416). Given that resting heart rate can serve as a proxy for fitness in genetic analyses, GWAS data were leveraged for resting heart rate from the full UKB cohort (n = 452,941), excluding individuals using beta-blockers and selected variants at genome-wide significance (P < 5 × 10-8). After removing heterogeneity outliers using a radial plot approach, 149 variants associated with the fitness proxy were retained (P < 0.05). Together with the 14 CRF-associated variants, 160 independent variants were included after accounting for overlap and applying linkage disequilibrium (r2 < 0.01) to form a composite genetic instrument for fitness.
The primary outcome measure was all-cause mortality. Mortality data were ascertained through linkage to the national registries in the UKB, with follow-up through November 30, 2022, and via the National Death Index for the NHANES, with follow-up through December 31, 2019. Due to the absence of GWAS mortality data, longevity was adopted as a surrogate outcome, consistent with previous research[7].
Kaplan–Meier survival curves and log-rank tests were used to visualize and compare survival differences across different CRF categories. Cox proportional hazards models were used to estimate hazard ratio (HR) and corresponding 95% confidence interval (CI). Restricted cubic splines (RCS) with 3 knots was also used to flexibly model and visualize the potential nonlinear association between CRF and all-cause mortality. Multistate life tables were constructed using a continuous-time model that included absence of CVD, presence of CVD, and mortality. CVD was selected as the intermediate state due to its strong association with CRF and mortality[8]. Subgroup, sensitivity, and meta-analyses were performed.
R version 4.3.3 (R Core Team; R Foundation for Statistical Computing, Vienna, Austria) STATA\MP Release 17.0 (StataCorp LLC, College Station, TX, USA), and SPSS version 25.0 (IBM Corp., Armonk, NY, USA) were used for the data cleaning and analysis. MR analysis was performed using the two-sample MR package in R version 4.3.3 (https://mrcieu.github.io/TwoSampleMR/index.html). All statistical tests were two-sided, and differences with P < 0.05 were considered to be significant.
Among participants in the UKB, 3,489 died, whereas 36 all-cause deaths occurred among NHANES participants. Baseline characteristics according to CRF levels are summarized in Supplementary Table S1. The mean age (standard deviation [SD]) of the UKB participants at high baseline CRF was 56.49 (8.13) years, and 45.40% of participants were men. The mean age of the NHANES study participants with higher baseline CRF levels was 31.74 (SD = 9.64), and 54.90% were male. Detailed characteristics of the participants are reported in Supplementary Tables S1 and S2. Total body weight and fat-free body mass were included in the calculation of CRF in the low, medium, and high tiers.
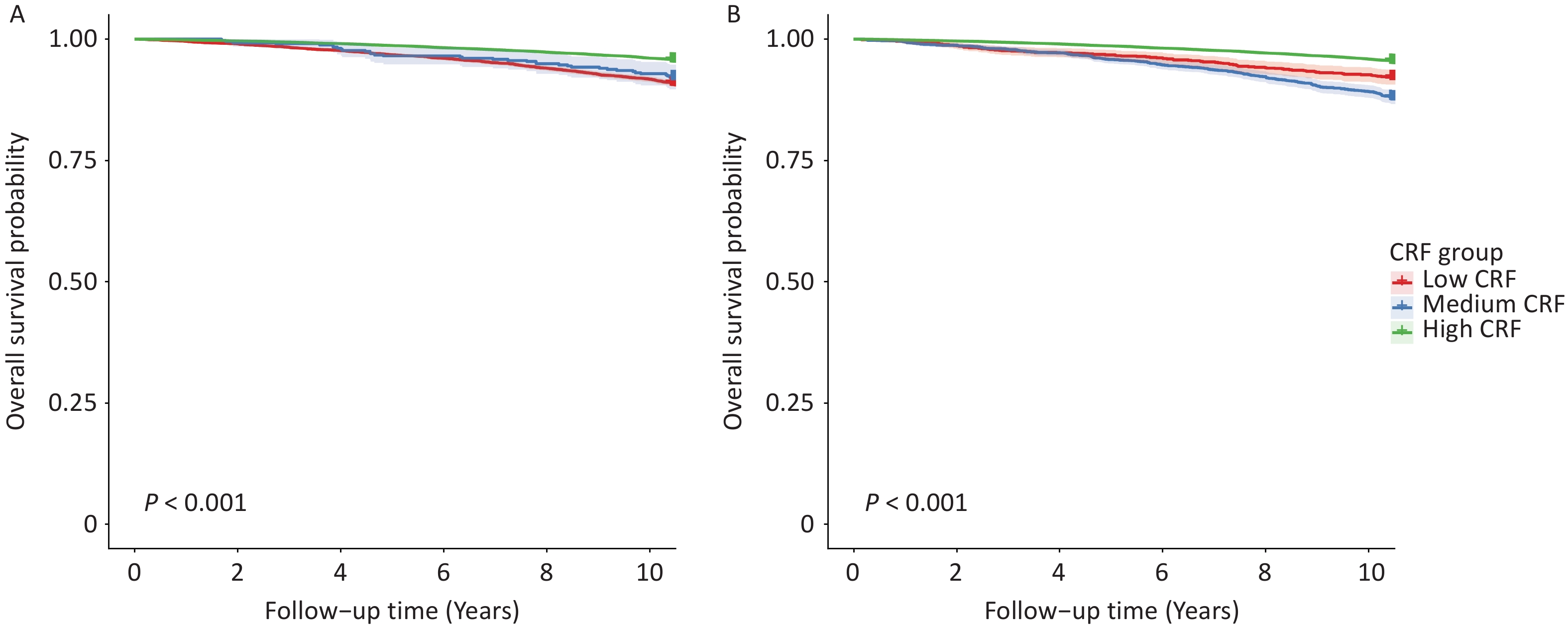
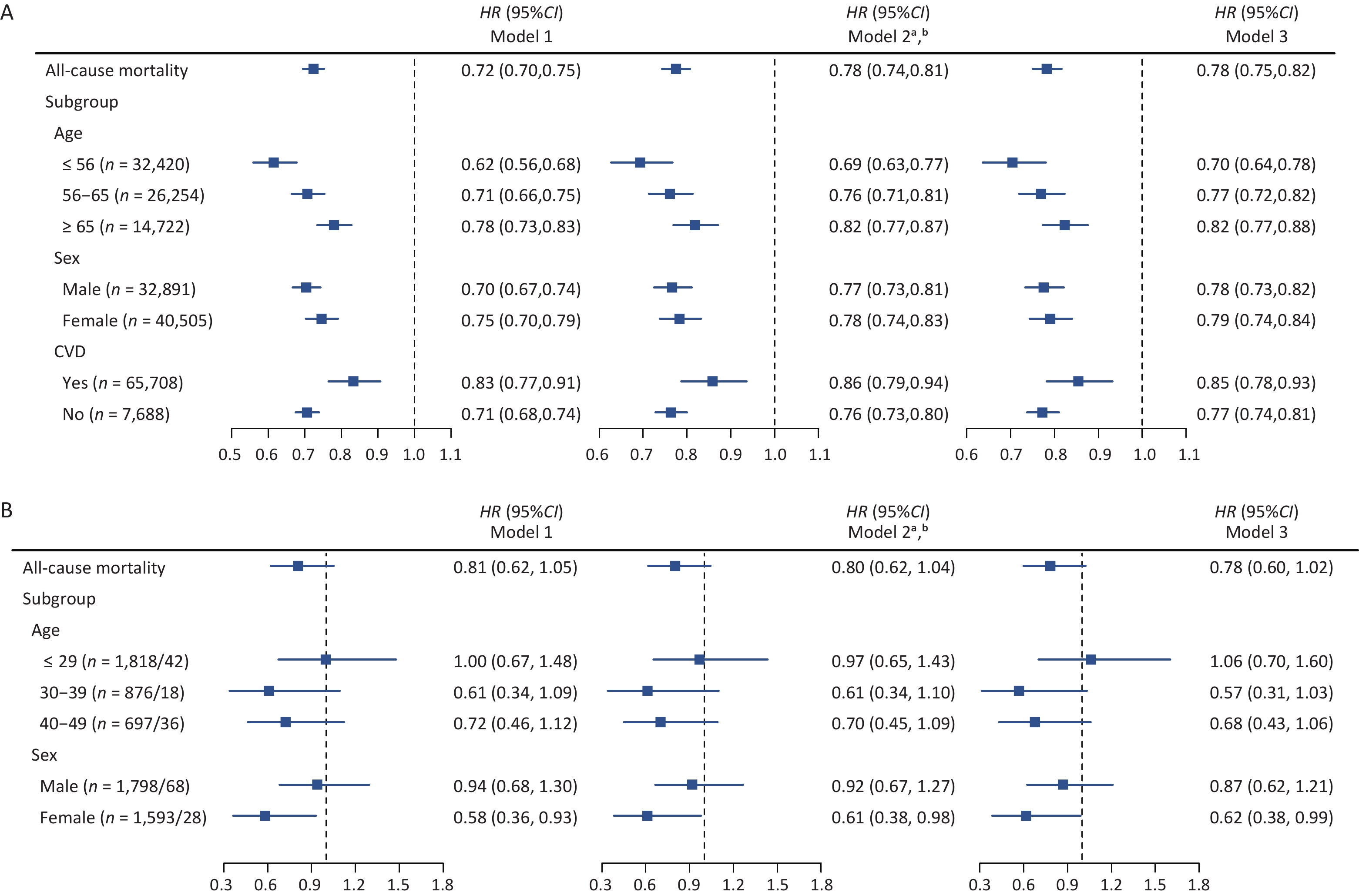
In the observational analyses, only the UKB cohort demonstrated a significant inverse association between higher CRF and all-cause mortality, both before (Model 2: HR = 0.78, 95% CI, 0.74, 0.81) and after BMI adjustment (Model 3: HR = 0.78; 95% CI: 0.75, 0.82). No significant overall association was observed in the NHANES data (Figure 1 and Supplementary Table S3). These divergent outcomes were visually corroborated using Kaplan–Meier survival analyses. In the UKB study, participants in the high-CRF group exhibited significantly higher overall survival probabilities at the 10-year follow-up than those in the medium- and low-CRF groups (both P < 0.001) (Figure 2A, B). Conversely, the survival curves for the NHANES cohort demonstrated no significant differences over the 20-year follow-up (P = 0.774 and P = 0.764) (Supplementary Figure 1A, B). Sensitivity and subgroup analyses revealed that the inverse association in UKB remained robust after excluding deaths within the first 2 years (Supplementary Table S4). Furthermore, when standardized according to fat-free mass, each increase in VO2max was associated with a 30.2% lower mortality risk in the UKB group (Supplementary Table S3). Subgroup analyses of the UKB revealed consistent benefits across sex- and age-stratified models (Figure 1 and Supplementary Table S3). Importantly, this inverse association remained robust regardless of baseline CVD status, with HRs consistently indicating a protective effect. For NHANES, statistical significance was observed only among women (Model 3: HR = 0.62; 95% CI: 0.38, 0.99), and CVD-stratified analyses were not feasible because of stringent VO2max inclusion criteria excluding patients with preexisting CVD.
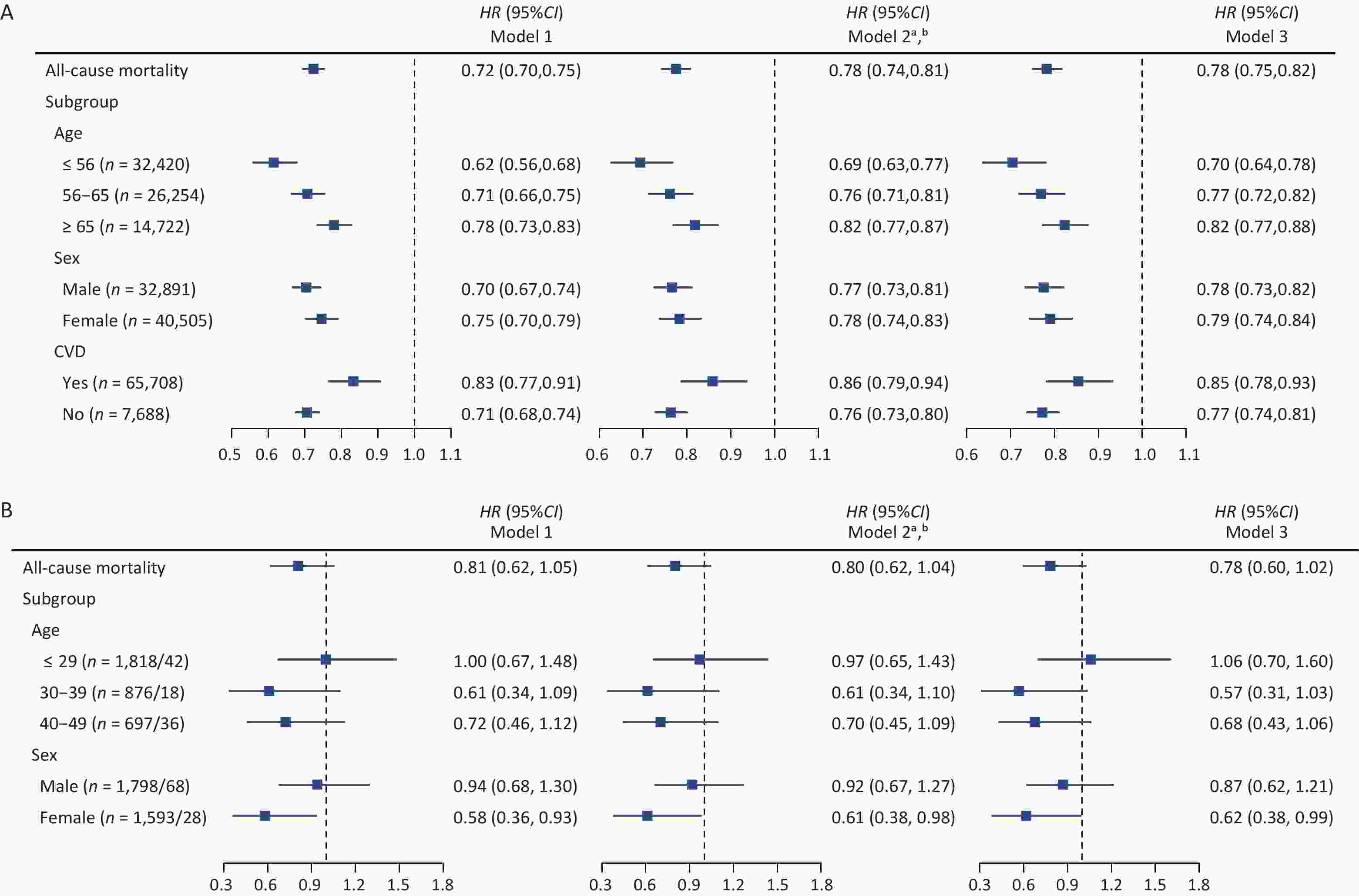
Figure 1. Associations between CRF (VO2maxtbm) and all-cause mortality in the UKB (A) and NHANES (B).
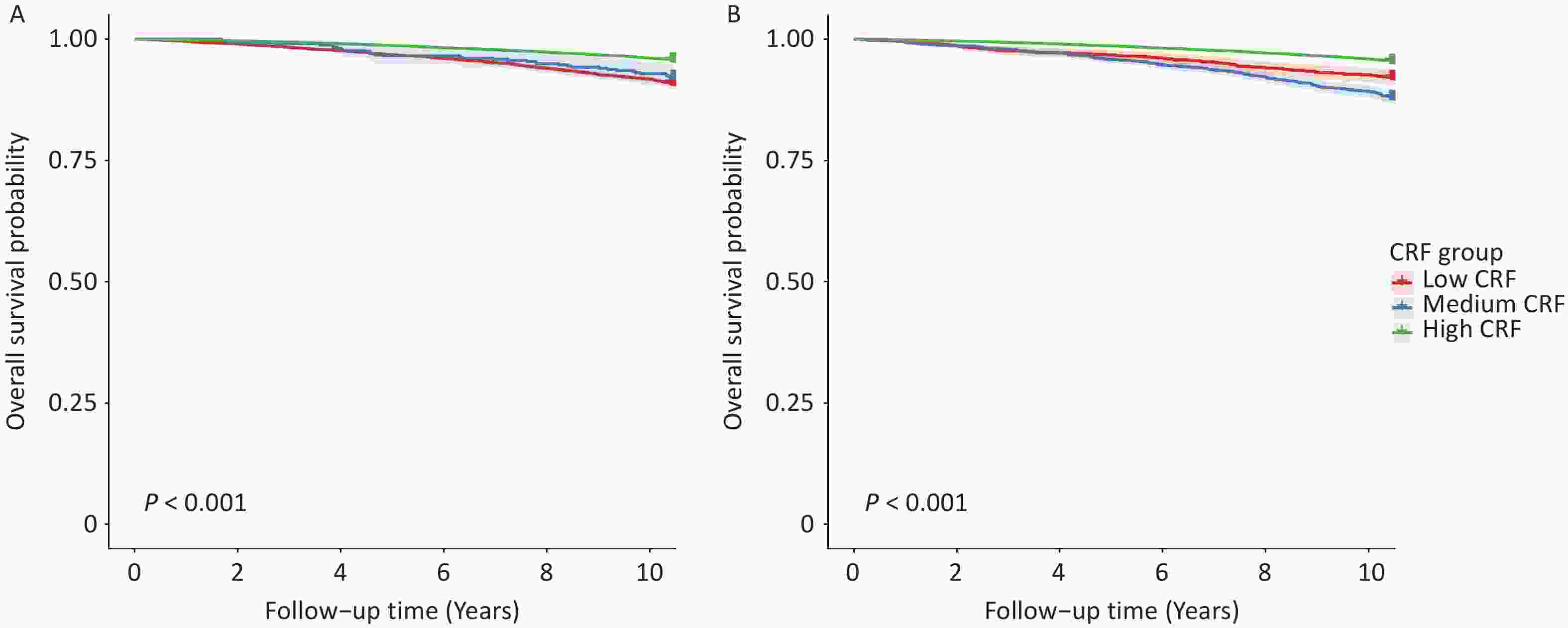
Figure 2. Kaplan‒Meier survival curves for the association between CRF and all-cause mortality in the UKB cohort based on (A) VO2maxtbm and (B) VO2maxffm.
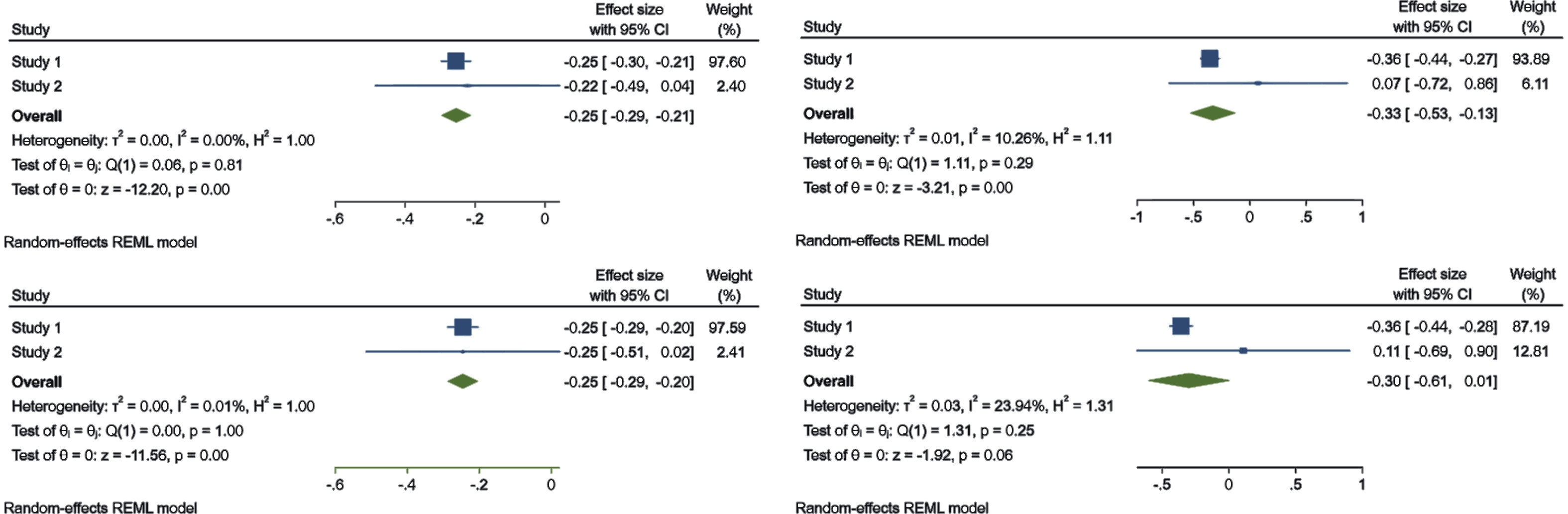
A meta-analysis combining data from both cohorts confirmed the overall protective effect of CRF (VO2maxtbm) without significant heterogeneity, although this was primarily driven by UKB data (97.60% weight) (Figure 3, Supplementary Figures S2 and S3). Finally, RCS analyses revealed significant nonlinear dose–response relationships in both cohorts (P < 0.001). The UKB cohort exhibited a continuous inverse trajectory, whereas the NHANES cohort exhibited a U-shaped association (Supplementary Figures S4 and S5). Life-table analyses revealed that higher CRF was associated with longer total life expectancy and longer life expectancy, both free of CVD and with CVD. With regard to CRF (VO2maxtbm), total life expectancy in the 40–49 years’ age group increased from 32.17 to 36.61 years for women, and from 27.69 to 32.44 years for men from the lower to the higher CRF group. In the higher CRF group, CVD-free life expectancy was 33.45 years for women and 27.34 years for men (Supplementary Tables S5 and S6). For CRF (VO2maxffm), total life expectancy increased from 29.55 to 35.63 years in women, and from 25.71 to 32.13 years in men, whereas CVD-free life expectancy increased by 5.97 years in women and 5.96 years in men in the higher versus lower CRF groups (Supplementary Tables S7 and S8). However, MR analyses did not support the causal effect of genetically predicted CRF on longevity. Specifically, the IVW method revealed no association with survival to the 90th percentile (OR = 1.003, 95% CI: 0.971, 1.037; P = 0.857) or 99th percentile (OR = 0.999, 95% CI: 0.947, 1.053; P = 0.965). Similar null results were obtained using the weighted median and penalized weighted median methods (Supplementary Table S9). Although significant heterogeneity was detected (Supplementary Table S10), the MR-Egger intercept tests did not indicate horizontal pleiotropy.
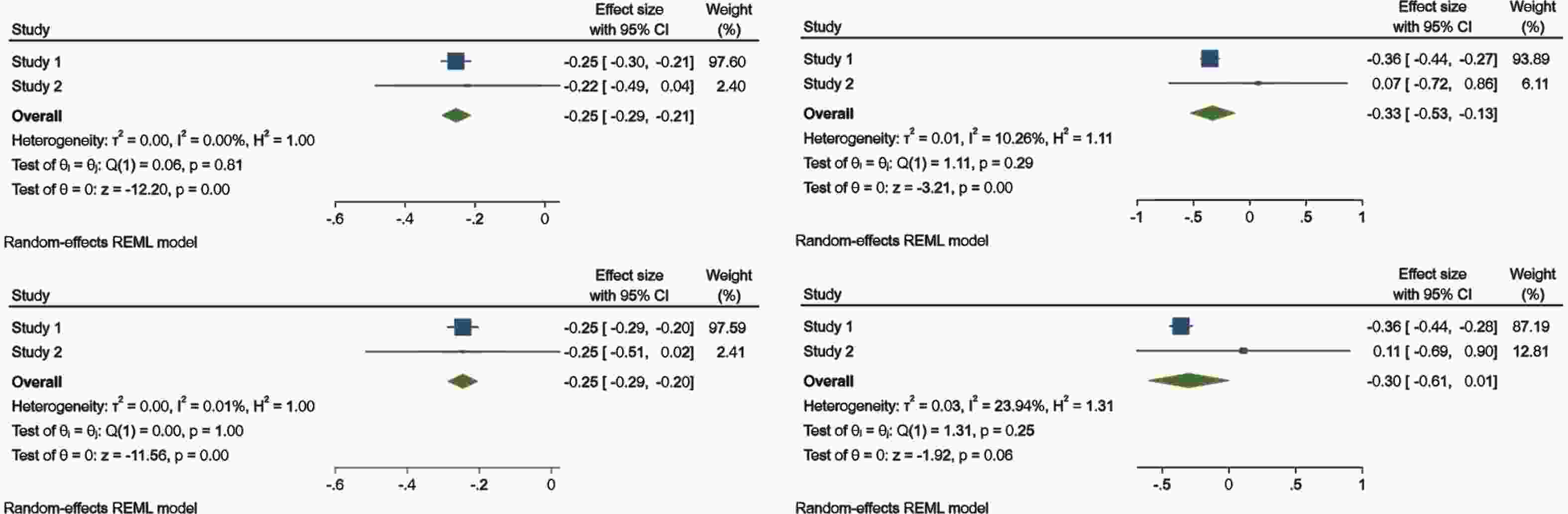
Figure 3. Meta-analysis forest plot of the association between CRF (VO2maxtbm or VO2maxffm) and all-cause mortality. Study 1: All-cause mortality from the UKB database; Study 2: All-cause mortality outcomes from the NHANES database. (a) Model was adjusted for age, sex, smoking status, history of diabetes, history of hypertension, and TDI/PIR. (b) Further adjusted for BMI. (c) Model adjusted for age, sex, smoking status, history of diabetes, history of hypertension, and PIR. Adjustment for fat mass.
In these 2 large prospective cohort studies, it was consistently observed that a higher CRF was associated with a lower risk for all-cause mortality and longer life expectancy, including both CVD-free and CVD-related survival. Individuals with high CRF exhibited the greatest survival advantage, suggesting that optimal physical fitness may substantially offset baseline mortality risk. These findings are consistent with previous large-scale studies reporting a robust and inverse association between CRF and mortality risk[2]. However, MR analyses did not support a causal effect of genetically predicted CRF on longevity, indicating that the observed benefits were more likely mediated through downstream behavioral and cardiometabolic pathways rather than direct genetic mechanisms.
The inverse association between CRF and mortality was primarily driven by the UKB cohort, whereas no significant overall trend was observed in the NHANES cohort, likely due to its smaller sample size and limited statistical power. In addition, the U-shaped relationship observed in the NHANES cohort suggests heterogeneity across CRF levels. This pattern may be partly explained by the “physical activity paradox[9]”, in which high CRF in some individuals reflects strenuous occupational activity rather than health-promoting leisure-time exercise, potentially attenuating the expected protective effect of high CRF.
Importantly, our findings highlighted the role of body composition in CRF-related risk stratification. When the CRF was normalized to the VO2maxtbm, a clear graded association with survival was observed. In contrast, normalization according to VO2maxffm disrupted this gradient, with the moderate CRF group exhibiting poorer survival rates than those in the low CRF group. This discrepancy likely reflects the underlying metabolic heterogeneity within CRF categories. Specifically, fat-free mass adjustment may reclassify individuals with higher adiposity but relatively preserved muscle mass into the moderate CRF group, introducing “metabolically unhealthy but physically capable[10]” phenotypes that reduce the discriminatory ability of CRF.
By translating relative risks into life table estimates, the present study provides a time-based and intuitive interpretation of CRF-associated survival benefits. More than one-half of the increase in life expectancy was attributable to prolonged CVD-free survival, suggesting that CRF may extend lifespan primarily by reducing cardiovascular risk. Furthermore, the persistence of the associations after adjusting for BMI and fat mass supported the independent and joint contributions of CRF and body composition. Although women have a higher overall life expectancy, the relative contribution of CRF to longevity was greater in men, possibly reflecting a higher burden of modifiable cardiometabolic risk factors.
The present study had several limitations. Differences between the UKB and NHANES in fitness assessment methods and population characteristics may have affected comparability. In addition, CRF was assessed only at baseline, limiting its ability to account for longitudinal changes. Finally, although MR analysis reduces confounding factors, the lack of causal evidence may reflect the limitations of genetic instruments or residual pleiotropy.
In conclusion, results of the present study revealed that individuals with higher CRF levels exhibited a lower risk for all-cause mortality. In addition, a higher CRF was associated with a longer total life expectancy and longer lifetime free of CVD. However, the causal relationship between CRF and longevity remains unclear and requires further exploration and verification.
HTML
-
The authors declare that they have no competing interests.
-
Not applicable.
Consent for publication Not applicable
Ethics The study was conducted in accordance with the principles of the Declaration of Helsinki. The UK Biobank was constructed with ethical approval from the North West Multicenter Research Ethics Committee (REC reference: 11/NW/03820), and each participant provided written informed consent prior to participation. The current analyses were carried out under application number 362917.
Approval from the relevant ethical review committees was obtained for all studies included in the GWASs, and all participants provided written informed consent. This study used only publicly accessible summary-level data, obviating the need for an additional ethical review.
Author Contributions Youxin Wang contributed to the conception and design of the study; Tong Guo, Haotian Wang, and Meiling Cao participated in the acquisition and analysis of the data; Tong Guo, Huimin Lu, and Meiling Cao participated in the interpretation of the data; Tong Guo and Huimin Lu were involved in writing and critiquing the drafts of the manuscript; Youxin Wang and Jingyu Wang approved the final manuscript for submission.
&These authors contributed equally to this work.
Reference

 Quick Links
Quick Links
 DownLoad:
DownLoad: