
-
Cerebral small vessel disease (CSVD) encompasses a spectrum of pathological processes that affect the small arteries, capillaries, and venules of the brain. The neuroimaging features include white matter hyperintensities (WMH), lacunar infarcts, cerebral microbleeds, and enlarged perivascular spaces. Ischemic leukoaraiosis (ILA) represents the most common and characteristic imaging phenotype of CSVD, typically appearing as patchy or diffuse hyperintensities in the periventricular or deep white matter on T2-weighted or fluid-attenuated inversion recovery (FLAIR) sequences[1]. ILA is the main cerebrovascular pathological basis that causes CSVD-related cognitive impairment and vascular dementia. Its lesion burden is significantly correlated with specific cognitive domain impairments such as information processing speed (IPS) and executive function[2]. However, the underlying pathophysiological mechanism remains unclear. Given the rapidly aging global population, it is increasingly necessary to investigate the pathogenesis of ILA-related cognitive impairment to delay the onset or progression of dementia.
Multiple neuroimaging studies have shown that ILA is associated with extensive damage to both gray and white matter, primarily within the cortico-cortical and cortico-subcortical circuits[3]. Considering that the brain is a complex network of interconnected regions, accumulating evidence from brain connectome-based studies on CSVD supports the idea that cerebral vascular lesions (e.g., WMH, lacunes, and microbleeds) are linked to the topological disorganization of structural networks (SN) and functional networks (FN). This network disruption, in turn, facilitates the correlation between vascular lesions and cognitive impairment[4]. These studies strongly suggest that "brain network dysfunction" is the most compelling interpretive model for understanding the neurobiological processes that drive cognitive impairments in ILA. SN-FN coupling, derived from multimodal neuroimaging, provides a unique and comprehensive measure of brain organization. Compared to any single modality, it enables more sensitive detection of subtle cerebral changes and has thus been recognized as a clinically meaningful metric for investigating brain disorders[5]. There has been a growing focus on the connection between the SN and FN in neuroscience. Emerging evidence indicates that FN patterns are constrained by an anatomical underpinning, the structural connectome[6]. Therefore, mapping the relationship between structural and functional connectivity at the network level may provide deeper insights into the mechanisms underlying cognitive impairment in ILA.
In this study, we enrolled 36 patients with ILA (ILA group; Fazekas sum score ≥ 3 for deep and periventricular WMH on FLAIR sequences) and 34 healthy controls (HCs; Fazekas score = 0). Detailed inclusion and exclusion criteria are provided in the Supplementary Materials. All participants underwent comprehensive neuropsychological assessments of general cognitive function, episodic memory, visuospatial function, IPS, executive function, and multimodal magnetic resonance imaging (MRI) scans, including three-dimensional T1-weighted imaging, diffusion tensor imaging (DTI), and resting-state functional MRI (R-fMRI). Further details on the neuropsychological testing and MRI acquisition are available in the Supplementary Materials. This study (2019ZDSYLL189-P01) was approved by the Research Ethics Committee of Zhongda Hospital, Southeast University, and written informed consent was obtained from all participants.
The DTI data were preprocessed and analyzed using FSL (http://www.fmrib.ox.ac.uk/fsl/). The R-fMRI data were preprocessed using SPM8 (http://www.fil.ion.ucl.ac.uk/spm) and DPARSFA (http://www.restfmri.net/forum/dparsf). Four patients with ILA were excluded because of incomplete brain coverage or excessive head motion (translation > 3 mm or rotation > 3°), leaving 32 patients with ILA and 34 healthy controls for the SN-FN coupling analysis.
Whole-brain structural networks were reconstructed using DTI-based deterministic tractography, with 90 cortical and subcortical regions defined as nodes and connection weights based on streamline density. Functional networks were constructed by calculating Pearson correlation coefficients of the resting-state time series between the same 90 regions. To avoid ambiguous biological interpretations of negative correlations, only positive connections were retained for analysis, and negative correlation values were set to zero. SN-FN coupling was evaluated at three levels: at the whole-brain connection level, coupling was quantified as the correlation between structural and functional connection strengths across all edges; at the small-world property level, global graph-theoretical metrics (including clustering coefficient Cp, characteristic path length Lp, normalized clustering coefficient γ, normalized characteristic path length λ, small-worldness σ, local efficiency Eloc, and global efficiency Eglob) and the nodal property (i.e., degree) were computed for both structural and functional networks, and Pearson correlations between each pair of corresponding metrics were calculated across participants; at the nodal level, coupling was defined as the number of connections shared between structural and functional networks for each brain region. Network analyses were performed using a fixed-density threshold of 30% to ensure the comparability of network topology across participants and to maintain the small-world properties of the networks.
Statistical analyses were performed using SPSS (version 17.0; SPSS Inc., Chicago, IL, USA). Demographic variables were compared between groups using independent two-sample t-tests or chi-square tests. Group differences in cognitive domain z-scores were examined using analysis of covariance (ANCOVA) models with age, sex, and education as covariates, and the significance threshold was set at P < 0.0125 (0.05/4) after Bonferroni correction. To investigate whether the identified cognitive deficits were independent of or mediated by core impairments, we conducted a series of follow-up ANCOVA. Specifically, we tested whether group differences in one cognitive domain remained significant after statistically controlling for performance in other domains by sequentially adding z-scores of the relevant domains as covariates. Group differences in network coupling measures were tested using nonparametric permutation tests, controlling for age, sex, and education, and comparisons of small-world property coupling were performed using Z statistics. Multiple comparisons in the nodal-level coupling analysis were corrected using the false discovery rate (FDR) method. Finally, multiple linear regression models adjusted for age, sex, and education were used to examine the association between alterations in SN-FN coupling and cognitive decline.
The demographic information and neuropsychological performance of all participants are shown in Table 1. Compared with HCs, the ILA group was younger (P = 0.017) and had a higher proportion of males (P = 0.019). There was no significant difference in education between the two groups (P = 0.141). To eliminate the interference from these potential confounding factors, age, sex, and education were included as covariates in all subsequent neuropsychological and SN-FN coupling analyses.
Measures HCs (n = 34) ILA group (n = 36) P values Demographics Age (years) 71.0 ± 8.0 65.2 ± 10.1 0.017 a Education (years) 12.3 ± 3.5 11.0 ± 3.4 0.141 a Gender (male/female) 7/27 17/19 0.019 b General Cognitive Function MMSE 28.3 ± 1.6 26.4 ± 3.7 0.040 c Composite Z-scores for each cognitive domain Episodic Memory (z-score) 0.34 ± 0.63 −0.32 ± 0.74 0.009 c AVLT-DR (raw score) 6.4 ± 2.3 3.4 ± 3.1 0.003 c LMT-DR (raw score) 5.1 ± 2.7 3.8 ± 2.9 0.143 c CFT-DR (raw score) 13.1 ± 7.2 9.1 ± 7.1 0.132 c Executive Function (z-score) 0.33 ± 0.56 −0.31 ± 0.70 0.003 c VFT (raw score) 18.3 ± 4.4 14.6 ± 4.6 0.007 c DST (raw score) 4.8 ± 1.4 3.9 ± 1.5 0.075 c TMT-B (raw score, second) 153.1 ± 74.3 251.4 ± 118.2 0.007 c Stroop C (raw score, second) 80.8 ± 27.8 125.6 ± 60.4 0.008 c Similarity (raw score) 14.9 ± 4.5 15.8 ± 4.5 0.805 c IPS (z-score) 0.43 ± 0.70 −0.41 ± 0.72 0.003 c DSST (raw score) 37.5 ± 13.8 28.1 ± 18.6 0.525 c TMT-A (raw score, second) 66.4 ± 23.3 99.0 ± 59.3 0.119 c Stroop A (raw score, second) 26.9 ± 5.7 37.3 ± 10.8 < 0.001 c Stroop B (raw score, second) 39.1 ± 8.9 56.7 ± 18.9 0.001 c Visuospatial Function (z-score) 0.08 ± 0.56 −0.07 ± 1.09 0.635 c CDT (raw score) 7.8 ± 1.5 7.6 ± 2.5 0.636 c CFT (raw score) 33.1 ± 3.9 31.8 ± 7.5 0.727 c Note. Data are presented as mean ± standard deviation. The performance of each neuropsychological test is expressed as raw scores. The level of each cognitive domain is denoted by the composite z-scores. AVLT-DR, auditory verbal learning test-20 min delayed recall; CDT, clock drawing test; CFT, Rey-Osterrieth complex figure test; CFT-DR, Rey-Osterrieth complex figure test delayed recall; DSST, digital symbol substitution test; DST, digit span test; HCs, healthy controls; ILA, ischemic leukoaraiosis; IPS, information processing speed; LMT-DR, the logical memory test with a 20 min delayed recall; MMSE, mini-mental state examination; Similarity, semantic similarity test; Stroop A, B, and C, Stroop color-word test A, B, and C; TMT-A, trail making tests A; TMT-B, trail making tests B; VFT, verbal fluency test. a Independent two-sample t-test. b Chi-square test. c Analysis of covariance (ANCOVA). Table 1. Demographic and neuropsychological data for all participants
Our analyses confirmed the characteristic cognitive profiles of the ILA. The ILA group had lower Mini-Mental State Examination scores than the HCs group (P = 0.040). Furthermore, the ILA group performed significantly worse than HCs in terms of episodic memory (P = 0.009), executive function (P = 0.003), and IPS (P = 0.003). For each neuropsychological test, compared with the HCs, the ILA group performed worse in AVLT-DR, VFT, TMT-B, Stroop A, Stroop B and Stroop C (all P < 0.05; Table 1). Although ILA can affect various aspects of cognitive function, the most relevant aspects of WMH progression are attention and executive function[7]. After identifying significant group differences in episodic memory, IPS, and executive function, we conducted further analyses to determine whether these cognitive deficits were interdependent. When comparing episodic memory, we found that once IPS and executive function were controlled for as confounding factors, the difference in episodic memory between the two groups was eliminated. To further explore domain specificity, we performed reciprocal control analyses. When IPS scores were included as covariates, the group difference in executive function was no longer significant (P = 0.307). Conversely, the trend of poorer IPS (P = 0.093) in the ILA group persisted even after including executive function scores as a covariate. This suggests that IPS impairment may be a primary driving cognitive deficit in ILA, potentially contributing to the deficits observed in other domains, a finding consistent with the frontal-subcortical circuit dysfunction hypothesis in CSVD.
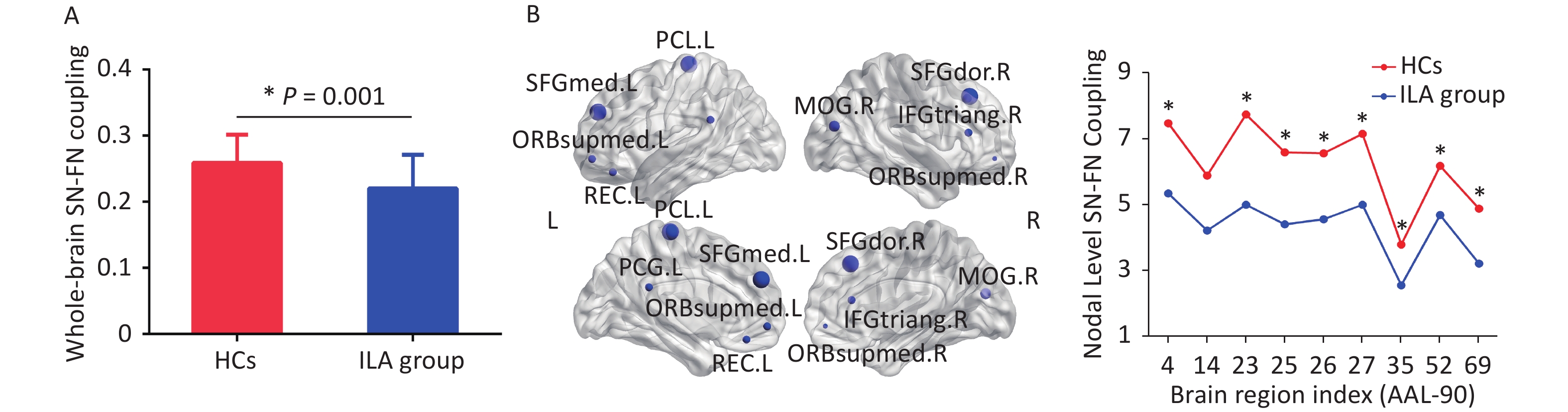
At the neuroimaging level, we found compelling evidence of widespread SN-FN decoupling in ILA. At the whole-brain connectivity level, while both groups showed significant positive structure-function correlations, the coupling strength was significantly weaker in the ILA group compared with HCs (HCs vs. ILA group: 0.259 ± 0.04 vs. 0.220 ± 0.05, P = 0.001, 10,000 permutations; Figure 1A). This global decoupling indicated that the consistency of brain structure and function in the ILA was disrupted. This could be due to the weakened correlation between functional interactions and potential anatomical structures, or to the asynchronous nature of destructive brain activity and morphological structure. At the small-worldness level, there were no significant correlations of the topological measures across participants for each group (all P > 0.05) and no significant between-group differences in Fisher’s r-to-z transformed correlation coefficients (all P > 0.05). At the nodal level, this decoupling was not diffuse, but targeted specific hub regions. The ILA group exhibited a significantly reduced degree of coupling in the right dorsolateral superior frontal gyrus (SFGdor), right triangular part of the inferior frontal gyrus (IFGtriang), left medial superior frontal gyrus (SFGmed), bilateral medial orbital superior frontal gyrus (ORBsupmed), left gyrus rectus, left posterior cingulate gyrus, right middle occipital gyrus, and left paracentral lobule (all P < 0.05, 10,000 permutations, FDR corrected; Figure 1B, C). These regions are primarily located within the hubs of the frontoparietal control network and the default mode network (DMN), which are critical for executive control, attention, and internally directed cognition. The selective vulnerability of these high-level cognitive hubs aligns with the "disconnection" hypothesis, where white matter lesions disrupt the efficient integration of information between distributed but functionally specialized cortical regions[8]. The observed decoupling may reflect maladaptive reorganization in which functional connectivity patterns can no longer be fully supported by the underlying damaged structural scaffold.
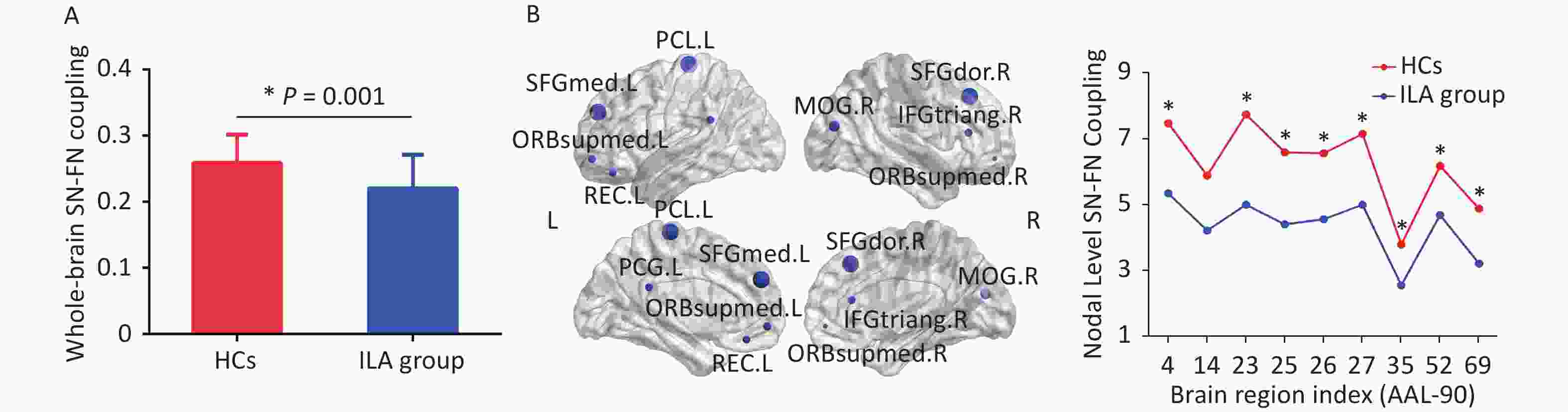
Figure 1. Brain SN-FN Decoupling in patients with ILA. (A) ILA group showed significantly decreased whole-brain SN-FN coupling strength compared with the HCs. The data are expressed as the mean ± standard error. (B) ILA group exhibited significantly decreased coupling degree in the right SFGdor, right IFGtriang, left SFGmed, bilateral ORBsupmed, left gyrus rectus, left posterior cingulate gyrus, right middle occipital gyrus, and left paracentral lobule at the nodal level. (C) At the node level, compared with the HCs, ILA group had reduced SN-FN coupling in nine brain regions. AAL, Automated Anatomical Labeling; HCs, healthy controls; IFGtriang.R, Triangular part of inferior frontal gyrus_right; ILA, ischemic leukoaraiosis; MOG.R, Middle occipital gyrus_right; ORBsupmed.L: Medial orbital superior frontal gyrus_left; ORBsupmed.R: Medial orbital superior frontal gyrus_right; PCL.L, Paracentral lobule_left; PCG.L, Posterior cingulate gyrus_left; REC.L, Gyrus rectus_left; SFGdor.R, dorsolateral superior frontal gyrus_right; SFGmed.L, medial superior frontal gyrus_left.
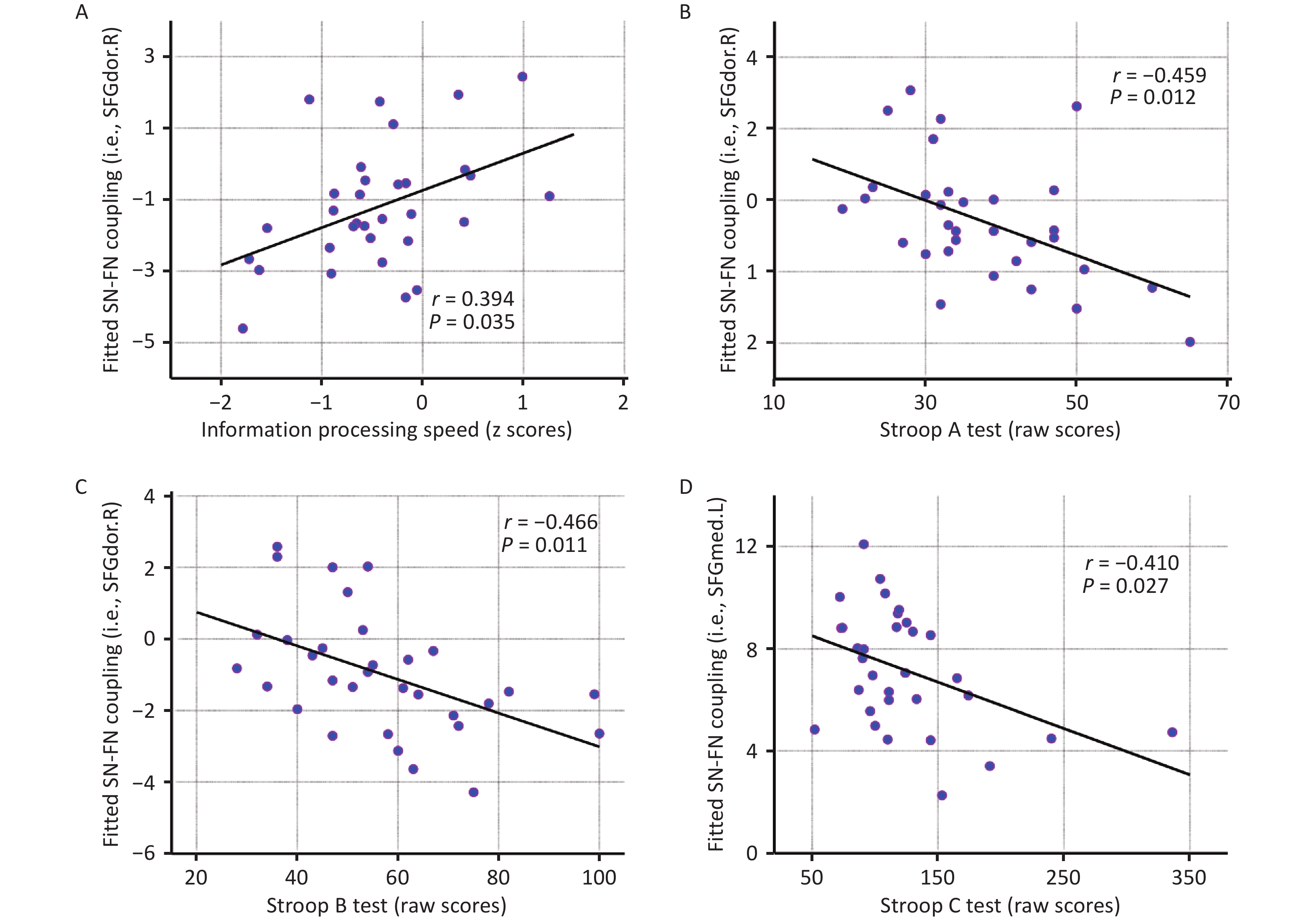
The observed association between SN-FN coupling and cognitive impairment in the ILA group offers important insights into the mechanisms underlying cognitive changes during ILA progression. Specifically, in the ILA group, the coupling strength of the right SFGdor positively correlated with the IPS (r = 0.394, P = 0.035; Figure 2A). Moreover, coupling of the right SFGdor showed negative correlations with both Stroop A (r = –0.459, P = 0.012) and Stroop B scores (r = –0.466, P = 0.011; Figure 2, C). As a key node in the DMN and frontal-parietal control network, the SFGdor is an important brain area for improving focus ability and achieving effective attention allocation[9]. These results all support that the SFGdor is a key brain region for the speed of information processing in patients with ILA, and SN-FN coupling may provide evidence for further exploration of cognitive changes in ILA. Interventions in the most-affected cognitive domains may benefit patients with ILA more significantly. Coupling of the left SFGmed was negatively correlated with Stroop C scores (r = –0.410, P = 0.027; Figure 2D). The SFGmed has been widely recognized as being related to task execution and plays an important role in cognitive processes[10]. This supports our finding that the degree of coupling of the left SFGmed was negatively correlated with Stroop C scores (a part of the execution function test). Our research findings provide evidence of cognitive impairment in patients with ILA, which may help understand the neuropsychological dysfunction of ILA and develop corresponding treatment interventions.
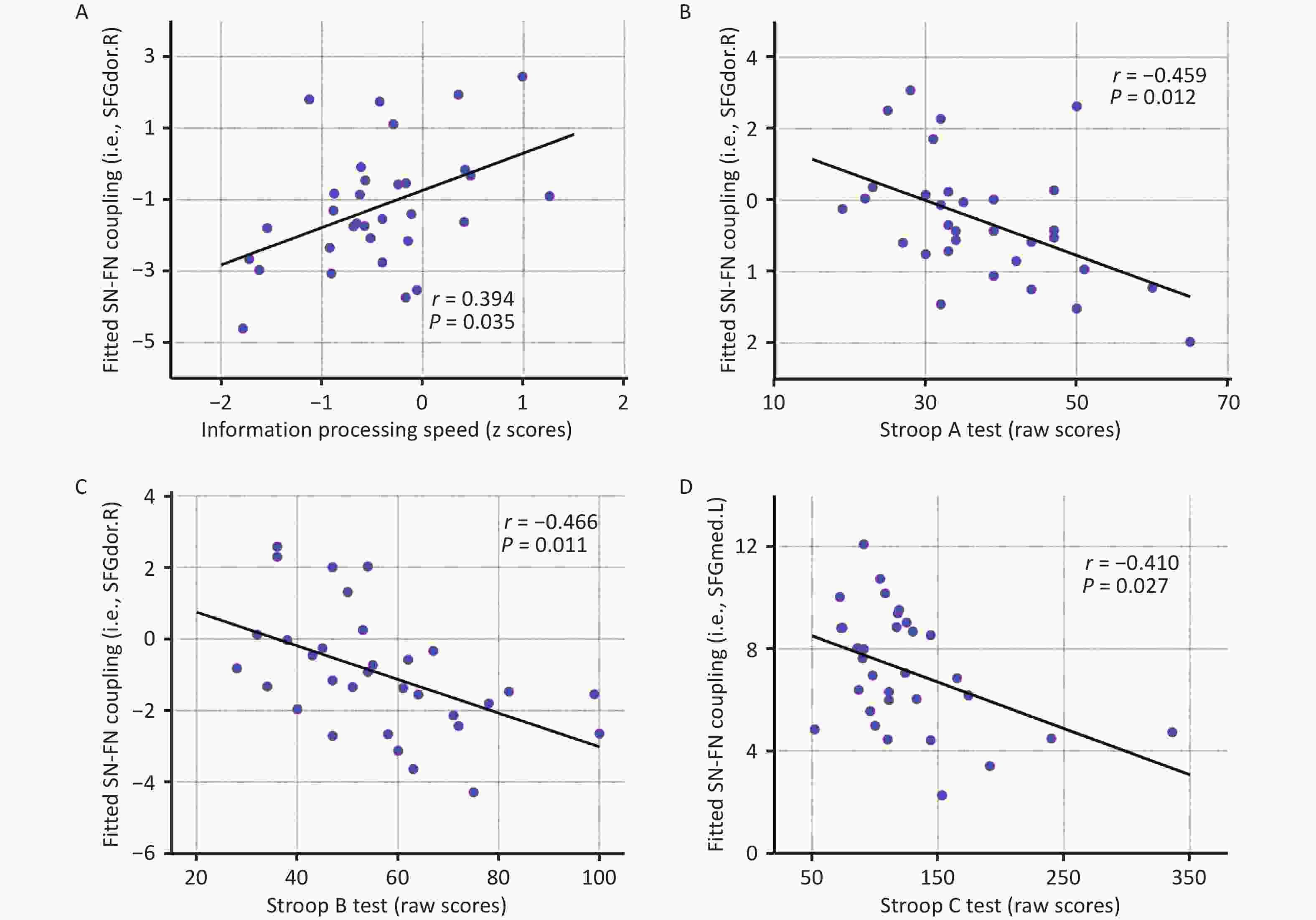
Figure 2. Association Between Brain SN-FN Coupling and Cognitive Performance. The scatter plots show positive correlation between the coupling degree of the right SFGdor and the information processing speed (A). The coupling degree of the right SFGdor is negatively correlated with Stroop A (B) and B (C) scores. (D) The coupling degree of the left SFGmed is negatively correlated with Stroop C scores. SFGdor.R, dorsolateral superior frontal gyrus_right; SFGmed.L, medial superior frontal gyrus_left; Stroop A, B, and C, Stroop color-word test A, B, and C.
Although our study provides insights into SN-FN coupling in ILA, several limitations should be acknowledged. First, the cross-sectional design and relatively small sample size limit the ability to infer longitudinal changes or establish generalizability. Future longitudinal studies with larger sample sizes are required to examine the progression of brain pathophysiology and cognitive function in patients with ILA. Second, our measure of SN-FN coupling was based on correlations between structural and functional connectivity derived only from connections with nonzero values in both modalities. Since strong functional connections can exist between regions without direct structural links, our approach does not capture interactions mediated by indirect structural pathways, a methodological constraint inherent to current coupling analyses. Third, the cognitive impact of WMH is likely to be influenced by their spatial distribution. Future studies should investigate SN-FN coupling in patients with ILA at different lesion locations.
In summary, this study advances our understanding of the topological properties of brain networks in patients with ILA. We demonstrated that ILA were associated with reduced SN-FN coupling across multiscale network levels, suggesting that ILA may break the hierarchical structure of brain networks, leading to the disruption of consistency between functional and structural networks. Critically, the degree of coupling of the right SFGdor was significantly related to the IPS, indicating that this region is a key area for core cognitive dysfunction in ILA. Collectively, alterations in SN-FN coupling enhance our understanding of the neurophysiological mechanisms underlying ILA-related cognitive impairment and provide a valuable framework for further investigation of its pathophysiology.
HTML
Competing Interests All authors report no conflicts of interest.
Ethics This study (2019ZDSYLL189-P01) was authorized by the Research Ethics Committee of Zhongda Hospital, Southeast University. Written informed consent was obtained from all participants.
Authors’ Contributions Conceptualization, Data Curation, Formal analysis, methodology, visualization, and writing of the original draft: Mengxue Wang. Investigation, validation, writing, review, and editing: Wenjuan Huang. Methodology and software: Yixin Zhu. Data Curation, Investigation: Tong Lu. Writing, review, and Editing: Zhengsheng Zhang. Resources, writing-review, and editing: Chunming Xie. Conceptualization, writing–review and editing, funding acquisition: Zan Wang. Conceptualization, Project administration, Supervision, Funding acquisition: Qingguo Ren.
&These authors contributed equally to this work.
Reference

 Quick Links
Quick Links
 DownLoad:
DownLoad: