
-
Metabolic dysfunction-associated steatotic liver disease (MASLD) is the most common chronic liver disease worldwide and a growing public health concern [1]. In addition to established metabolic determinants, environmental metal exposure has been linked to hepatic steatosis and related metabolic abnormalities [2]. However, evidence across metals and populations remains heterogeneous and data on Chinese adults living in rural locations are limited. Dysfunction of lipid metabolism is central to the pathophysiology of MASLD. Triglycerides (TG) reflects hepatic lipid accumulation, whereas the total cholesterol-to-high-density lipoprotein cholesterol ratio (TC/HDL-C) reflects a broader lipid imbalance and cardiometabolic risk [3,4]. We analyzed baseline data from the Guangxi Eco-Environmental Health and Aging Study (GEHAS) to examine the associations between plasma metal concentrations and MASLD and to explore whether TG and TC/HDL-C might partly account for these associations. We hypothesized that the selected plasma metal concentrations would be associated with MASLD, and that lipid-related biomarkers—particularly TG and TC/HDL-C—might be involved in these associations.
This cross-sectional study included data from 3,116 adults aged ≥ 30 years from the 2018 to 2019 baseline survey of the GEHAS—an ongoing population-based study of rural residents in Guangxi, China. Among the 4,356 enrolled participants, we excluded individuals whose questionnaire, examination, biochemical, or plasma metal data were missing, and those with diagnosed major liver or kidney disease, thyroid disorders, cancer, or use of medications affecting liver function (Supplementary Figure S1). We measured the plasma concentrations of ten metals (cadmium (Cd), arsenic (As), barium (Ba), molybdenum (Mo), lead (Pb), iron (Fe), zinc (Zn), copper (Cu), cobalt (Co), and calcium (Ca)) using inductively coupled plasma‒mass spectrometry. Routine laboratory calibration, quality control procedures, and elemental determination were conducted, and the corresponding quality control results are shown in Supplementary Table S2.
Because the concentrations of several essential elements may vary with dietary intake, nutritional status, supplement use, physical activity, and other metabolic or inflammatory conditions, and because detailed information on these factors is unavailable, residual confounding cannot be eliminated. We defined MASLD according to the criteria used for the Chinese population: imaging-confirmed hepatic steatosis, plus at least one metabolic risk criterion; lipid-lowering medication use was considered within the metabolic criteria when applicable. A fibrosis assessment was not included in the primary outcome definition. Detailed analytical procedures and MASLD assessment methods are provided in the Supplementary Methods. All participants fasted for at least 12 hours before blood sampling. We measured TG levels directly and calculated the TC/HDL-C ratio as total cholesterol divided by HDL-C. We used natural log-transformed metal concentrations and a multivariate logistic regression to examine the associations of metals and lipid biomarkers with MASLD; a multivariate linear regression to examine the associations of metals with TG and TC/HDL-C; restricted cubic spline models to assess nonlinearity; and a segmented regression to estimate potential breakpoints, when needed. We further performed exploratory mediation analyses to assess whether TG and TC/HDL-C might statistically account for some of the metal–MASLD associations. The models were adjusted for sex, age, ethnicity, educational attainment, smoking status, alcohol consumption status, obesity status, and diabetes status. We did not adjust for lipid-lowering medication use, as the MASLD definition incorporated this information. Because exposure, lipid biomarkers, and MASLD were measured at the same baseline examination, we interpreted the mediation analyses as hypothesis generating, rather than causal.
Among the 3,116 participants, 454 (14.6%) had MASLD. Compared with those without MASLD, participants with MASLD were more often male (53.7% vs. 35.0%), more likely to be aged < 60 years (61.7% vs. 51.7%), and had a markedly higher prevalence of obesity (25.6% vs. 3.4%) and diabetes (8.8% vs. 3.3%) (all P < 0.001). They also had higher TG levels (1.77 [1.14 – 2.56] vs. 0.98 [0.71 – 1.43] mmol/L) and higher TC/HDL-C ratios (3.73 [3.27 – 4.21] vs. 3.08 [2.65 – 3.61]). Baseline characteristics are presented in Supplementary Table S3. The absolute plasma metal concentrations are shown in Supplementary Table S4; patients with MASLD had lower plasma Co concentrations and higher plasma Fe and Ca concentrations.
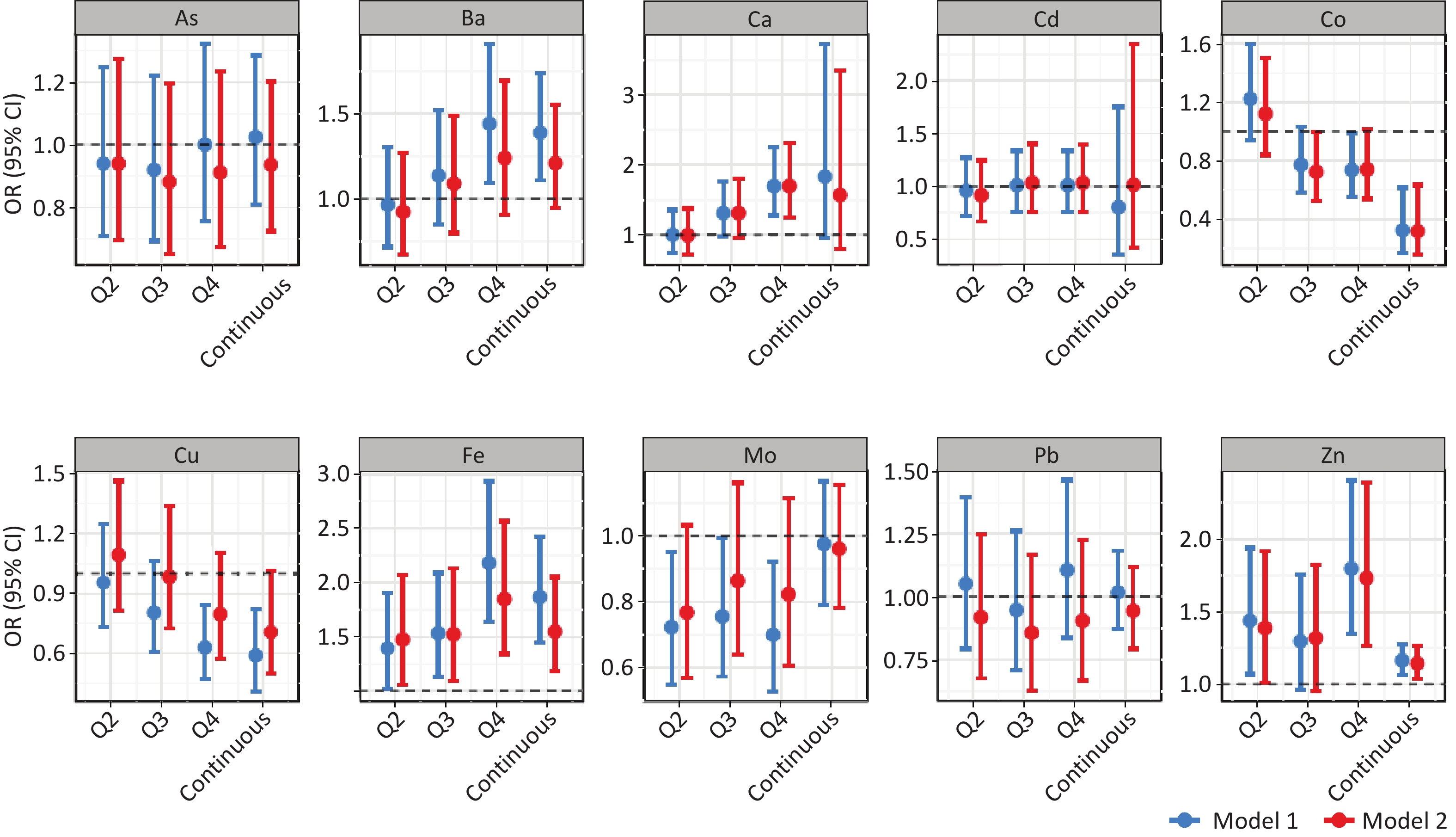
In the multivariate-adjusted models, higher plasma Fe, Zn, and Ca concentrations were associated with higher odds of MASLD, whereas Co showed a modest inverse association (Figure 1; Supplementary Table S5). Compared with the lowest quartile, the highest quartile of Ca was associated with MASLD (OR = 1.684; 95% Confidence Interval )[CI]: 1.245 – 2.289), as were the highest quartiles of Zn (OR = 1.712; 95% CI: 1.248 – 2.361) and Fe (OR = 1.845; 95% CI: 1.338 – 2.561). For Co, only the third quartile had lower odds than the first quartile did (OR = 0.716, 95% CI: 0.520 – 0.984). These findings indicate metal-specific associations with MASLD in this population. The positive associations between Fe and Zn were broadly consistent with the findings of previous studies that linked altered trace element homeostasis to fatty liver and metabolic dysfunction[2,5]. The inverse association observed for cobalt should be interpreted cautiously, although it is directionally consistent with reports suggesting that cobalt-related pathways may influence insulin sensitivity and lipid metabolism[6].
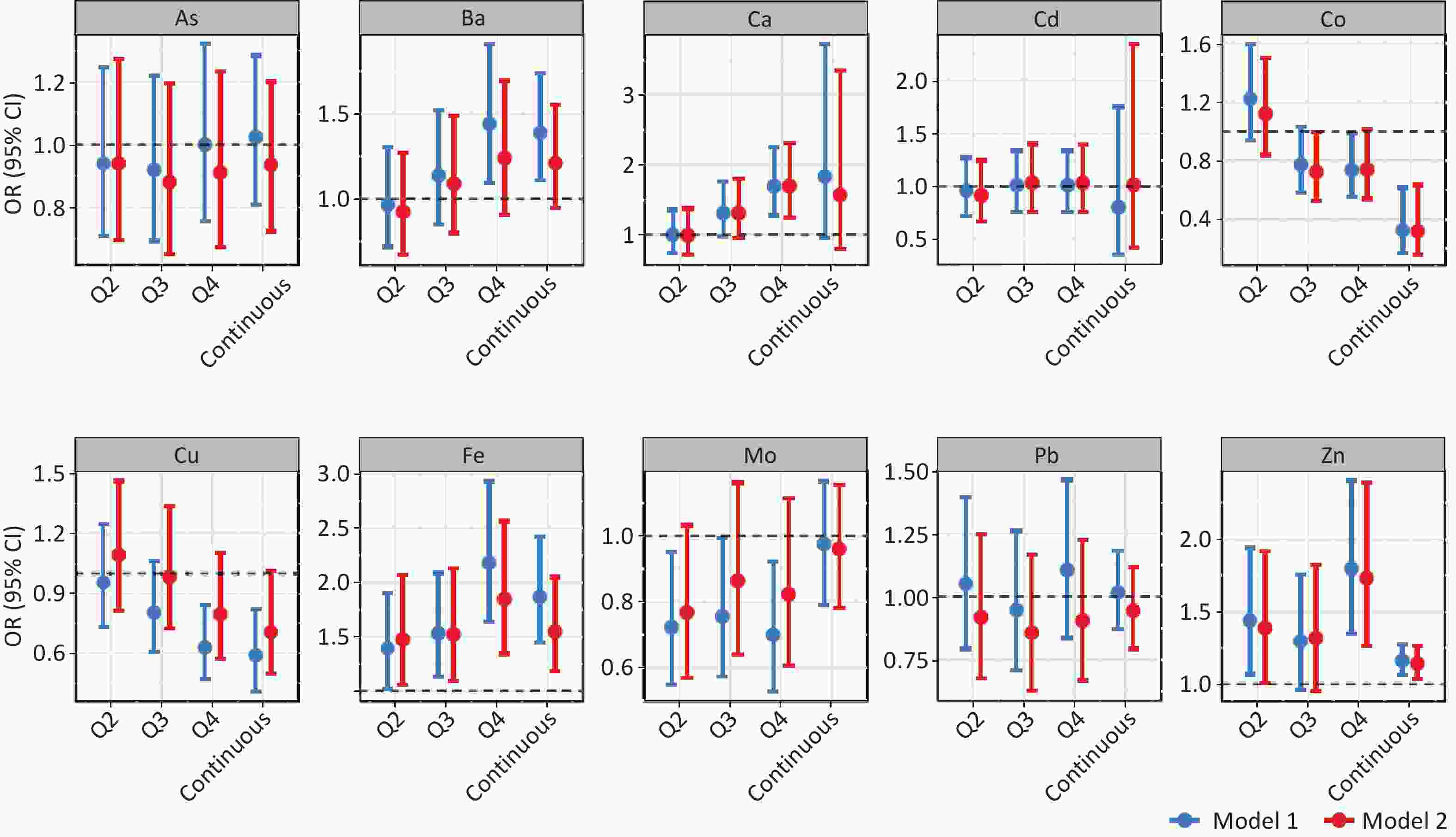
Figure 1. Associations between metal concentrations and the odds of MASLD. Metal levels were analyzed as quartiles (Q2–Q4, with Q1 as the reference) and as continuous variables. Points represent OR, and error bars indicate 95% CI. The horizontal dashed line denotes OR = 1. Model 1 shows unadjusted estimates, and Model 2 shows multivariable-adjusted estimates controlling for sex, age, ethnicity, educational attainment, smoking status, alcohol consumption, obesity, and diabetes. MASLD = metabolic dysfunction-associated steatotic liver disease; OR = odds ratio; CI = confidence interval.
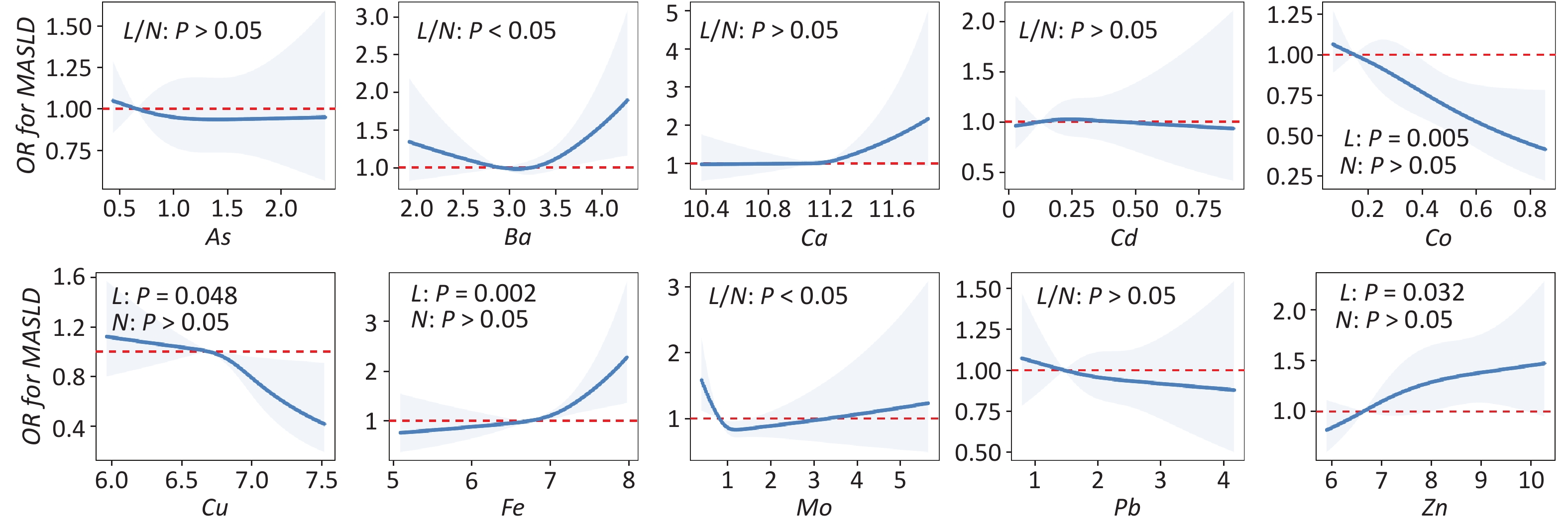
Restricted cubic spline analyses indicated nonlinearity for Mo (P = 0.009) and Ba (P = 0.032) (Figure 2). Because the segmented regression showed clear evidence of a breakpoint for Mo, we focused on Mo in the main text and present detailed results in Supplementary Table S6. The estimated breakpoint for plasma Mo concentration was (0.742 ±0.049) μg/L. Below this value, higher Mo concentrations were associated with lower odds of MASLD (OR = 0.067, 95% CI: 0.006 – 0.768), whereas above it, no significant association was observed (OR = 1.063, 95% CI: 0.867 – 1.279). This pattern is of interest and broadly aligns with previous reports on the nonlinear associations between Mo and metabolic outcomes[7]. However, the breakpoint should be regarded as a model-derived inflection point, rather than a clinically meaningful cutoff. The potential adverse effects of higher Mo concentrations remain uncertain, as the association above the breakpoint was not significant. In addition, the exposure range was limited and the confidence intervals widened at the extremes. Therefore, these findings require cautious interpretation and confirmation through independent cohort studies.
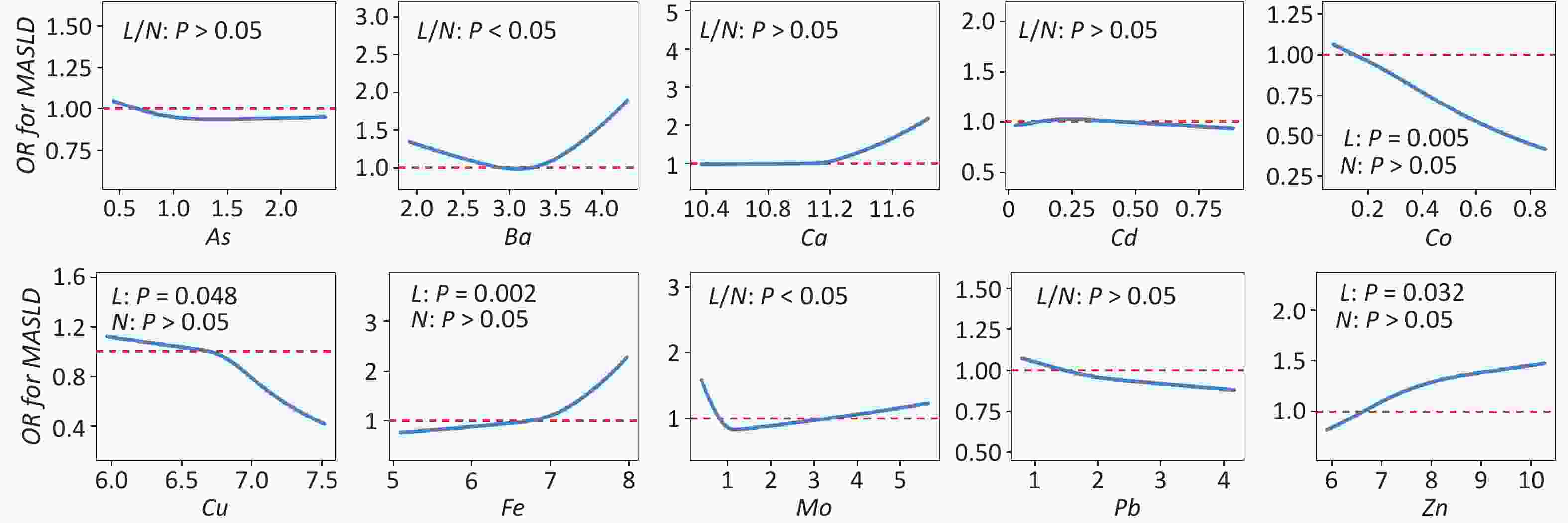
Figure 2. Restricted cubic spline analyses of plasma metal concentrations and the odds of MASLD. Restricted cubic spline models were used to examine potential nonlinear associations between plasma metal concentrations and the odds of MASLD. Solid blue lines represent adjusted OR, and shaded areas indicate 95% CI. The median concentration of each metal was set as the reference value (OR = 1). Models were adjusted for sex, age, ethnicity, educational level, smoking status, alcohol consumption, obesity, and diabetes. “L” denotes a linear relationship, “N” stands for a nonlinear relationship; P < 0.05 is considered statistically significant.
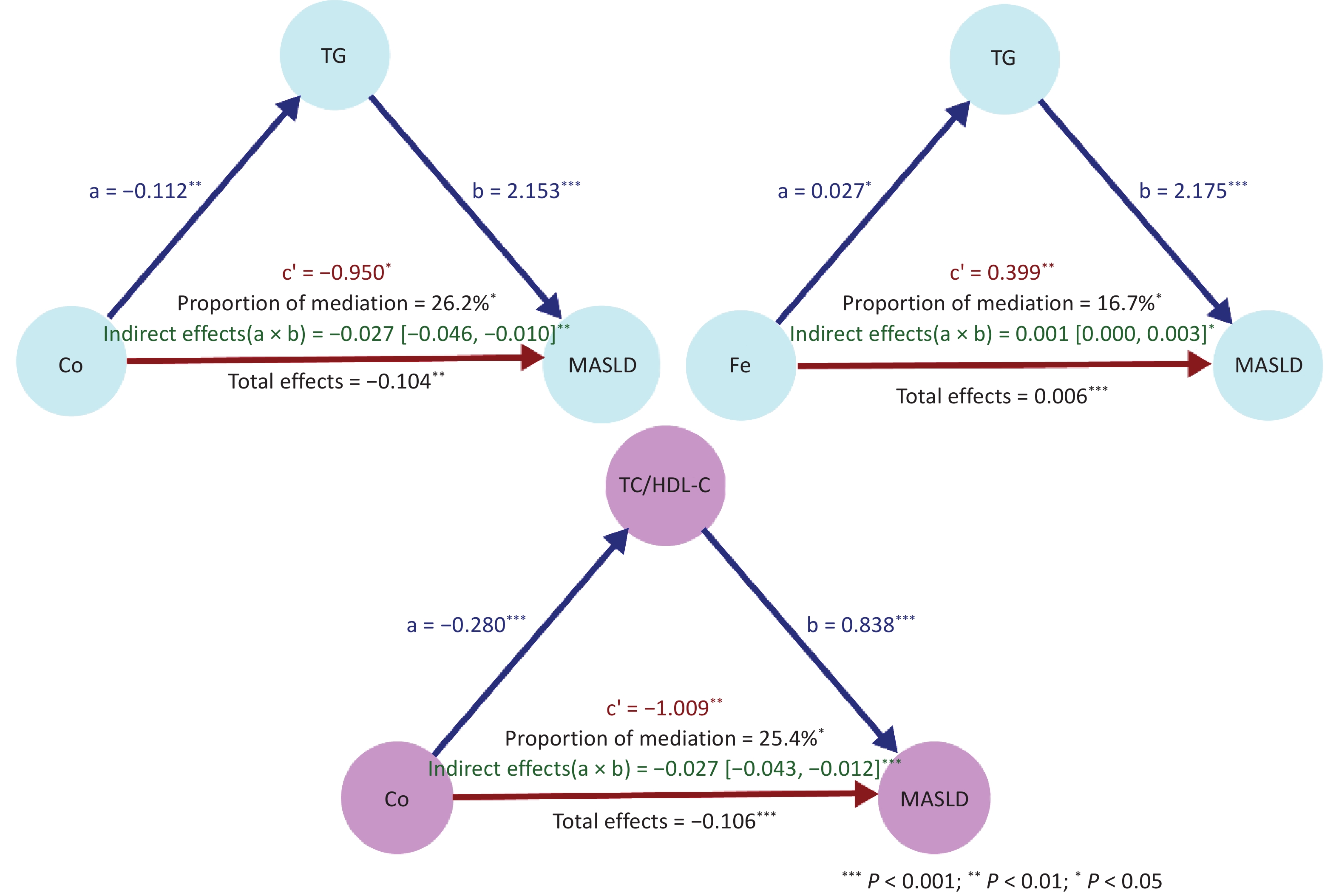
To explore the possible lipid-related pathways, we examined the association of metals with TG and TC/HDL-C. In adjusted linear regression models, plasma Fe (β = 0.026, 95% CI: 0.001 – 0.052), As (β = 0.033, 95% CI: 0.006 – 0.060), and Ca (β = 0.081, 95% CI: 0.016 – 0.146) were positively associated with TG, whereas Co was inversely associated with TG (β = -0.112, 95% CI: -0.183 – -0.041). For TC/HDL-C, Cu (β = 0.191, 95% CI: 0.092 – 0.289), As (β = 0.101, 95% CI: 0.042–0.160), and Ca (β = 0.184, 95% CI: 0.041 – 0.326) were positively associated, whereas Co (β = -0.279, 95% CI: -0.434 – -0.124) and Cd (β = -0.402, 95% CI: -0.602 – -0.201) were inversely associated (Supplementary Table S7). Both lipid biomarkers were strongly associated with MASLD. Compared to the lowest quartile, the highest quartile of TG was associated with substantially higher odds of MASLD (OR = 10.348, 95% CI: 7.040 – 15.680), and the highest quartile of TC/HDL-C was similarly associated with MASLD (OR = 11.466, 95% CI: 7.926 – 17.132) (Supplementary Table S8). These findings suggest that lipid metabolic dysfunction may partially enhance the association between certain metals and MASLD.
Several mechanisms can explain these associations. Iron overload is associated with oxidative stress, insulin resistance, and hepatic lipid accumulation[8]. Calcium imbalance may affect redox signaling and mitochondrial function[9], whereas the association between zinc and fatty liver disease appears to vary according to the population and biomarkers[2]. The inverse association with Co was noteworthy. As a component of vitamin B12, cobalt may influence energy metabolism, insulin-related pathways, and hepatic lipid handling[10]. However, epidemiological findings for Co remain inconsistent, possibly because of differences in the exposure matrix, exposure range and source, nutritional context, and population characteristics. Therefore, the findings should be interpreted with caution. Overall, these results suggest that trace metal homeostasis is associated with MASLD through multiple metabolic pathways, with lipid dysfunction as a plausible component.
This study has several strengths, including a relatively large sample size, simultaneous measurement of multiple plasma metals, and use of flexible modeling approaches to assess both linear and nonlinear associations. However, this study had several limitations. First, exploratory mediation findings require validation in independent populations and prospective cohort studies. Although we adjusted for sex, age, ethnicity, educational attainment, smoking status, alcohol consumption status, obesity status, and diabetes status and excluded participants with major liver disease, residual confounding remained, particularly due to unavailable factors such as diet and physical activity. Second, MASLD was defined by imaging-confirmed steatosis plus metabolic criteria; however, imaging has limited sensitivity for mild steatosis, and fibrosis was not included in the primary outcome definition. Third, TG, HDL-C, and lipid-lowering treatment-related abnormalities are part of the metabolic diagnostic framework of MASLD. As lipid-lowering medication use was incorporated into the outcome definition, we did not adjust for it in the MASLD or mediation models to avoid overadjustment bias. Nevertheless, some conceptual overlap cannot be excluded when the results of the mediation analyses based on TG and TC/HDL-C levels are interpreted. Moreover, assay-specific precision metrics for routine biochemical measurements—including intra- and inter-assay coefficients of variation for TG and HDL-C—are not available in the current database. Therefore, the analytical quality assurance documentation is incomplete and should be considered when interpreting lipid-related findings. Fourth, although internal and external quality control procedures were implemented, the reported QA/QC information was not comprehensive. Plasma concentrations may primarily reflect relatively recent or short- to intermediate-term internal exposure to certain metals, rather than the cumulative long-term burden. Therefore, the temporal variability in plasma levels may have introduced exposure misclassification and affected the stability of the observed associations. Additionally, plasma may not be the optimal matrix for some elements, particularly Cd, Pb, and As. Whole blood is generally preferred for Cd and Pb, whereas urine is more informative for As exposure. Fifth, multiple comparisons were involved and metals were analyzed mainly in single-metal models; thus, chance findings and potential co-exposure effects cannot be excluded. Finally, because the participants—many of whom were ethnic minorities—were predominantly middle-aged and older rural residents of Guangxi, the findings may not be generalizable to urban, younger, or non-Chinese populations.
In summary, in a rural Guangxi population, higher plasma Fe, Zn, and Ca concentrations were associated with higher odds of developing MASLD, whereas Co showed a modest inverse association. Mo also showed a nonlinear association with MASLD; however, this finding requires confirmation in an independent cohort study. Exploratory mediation analyses suggested that TG and TC/HDL-C ratio might partly bring about the association between Fe, Co, and MASLD. These findings provide population-specific epidemiological evidence from an underrepresented rural ethnic minority population in southwestern China, and support further investigation of lipid-related pathways among individuals with metal-associated hepatic abnormalities. From a public health perspective, these results may help inform future risk assessments of environmental metal exposure and metabolic dysfunction in high-risk rural populations.
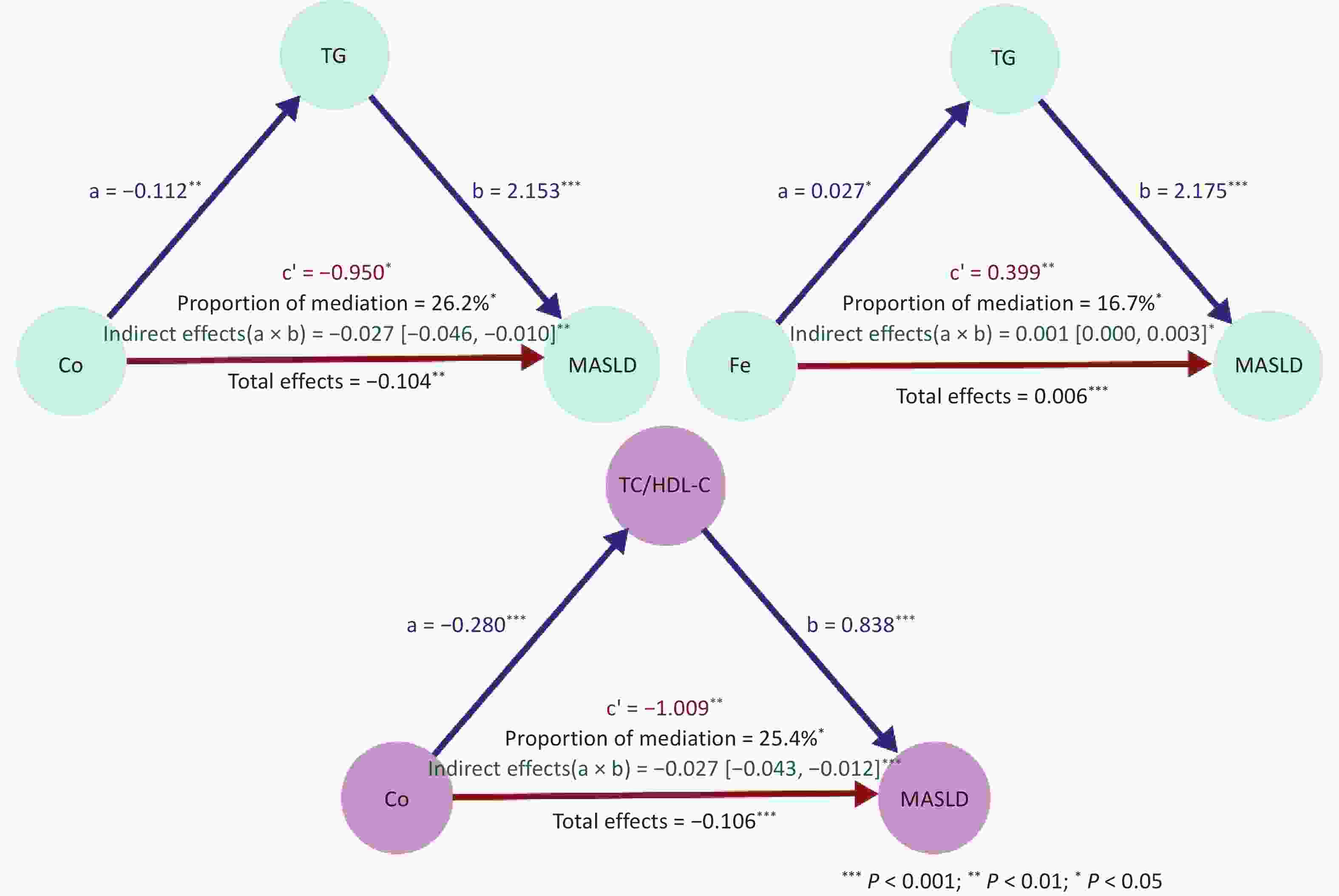
Figure 3. Exploratory indirect-effect models involving TG, the TC/HDL-C ratio, and MASLD. Exploratory indirect effect models involving TG and TC/HDL-C ratio in the association between metal exposure and MASLD. Path diagrams show the standardized coefficients. Path a represents the association between metal exposure and the mediator (TG or TC/HDL-C), Path b represents the association between the mediator and MASLD, and Path c represents the direct association between metal exposure and MASLD, after accounting for the mediator. The indirect effect was calculated as the product of Paths a × b and the mediated proportion was computed as (a × b) / (total effect). All the models were adjusted for sex, age, ethnicity, educational attainment, smoking status, alcohol consumption, obesity, and diabetes. Asterisks indicate statistical significance (P < 0.05, P < 0.01, P < 0.001). MASLD = metabolic dysfunction-associated steatotic liver disease; TG = triglyceride; TC = total cholesterol; HDL-C = high-density lipoprotein cholesterol. Because the data were cross-sectional, these models should be interpreted as exploratory and hypothesis generating, rather than causal.
HTML
Competing Interests The authors declare no competing financial interest.
Ethics The study protocol was approved by the Medical Ethics Committee of Guilin Medical University (approval number 20180702-3), and informed consent was obtained from all participants.
Author Contributions Conceptualization: Yuan Yang; Data curation: Yuan Yang, Moqi Zhang, Chaofan Xie, Hao Wang Shuzhen Liu, Chihua Li; Formal analysis: Yuan Yang; Funding acquisition: Zhiyong Zhang, Xu Gao; Investigation: Yuan Yang, Moqi Zhang, Chaofan Xie, Hao Wang, Shuzhen Liu, Chihua Li; Methodology: Yuan Yang; Project administration: Zhiyong Zhang, Xu Gao, Jiansheng Cai, and You Li; Resources: Zhiyong Zhang, Xu Gao and You Li; Software: Yuan Yang; Supervision: Zhiyong Zhang and Shuzhen Liu; Validation: Yuan Yang; Writing—original draft: Yuan Yang; Writing—review & editing: Zhiyong Zhang, Xu Gao, Yuan Yang.
Data Availability Statement Access to the GEHAS data is available upon reasonable request from Dr. Zhiyong Zhang and Dr. Xu Gao.
Reference

 Quick Links
Quick Links
 DownLoad:
DownLoad: