
-
Oocytes play a critical and irreplaceable role in female reproduction, and their maturity and functional integrity directly determine fertilization capacity, early embryonic development, and pregnancy success[1,2]. The development of oocytes depends not only on the maternal endocrine and metabolic milieu but is also highly susceptible to environmental exposures[3-5]. Among various environmental stressors, fine particulate matter (PM2.5) has drawn considerable attention owing to its ubiquity and well-documented biological toxicity[6-8]. Growing experimental and epidemiological evidence suggests that PM2.5 may disrupt folliculogenesis and oocyte developmental competence through oxidative stress, mitochondrial dysfunction, inflammatory responses, and hormonal dysregulation, ultimately impairing female fertility[9-11].
However, the health effects of PM2.5 are shaped not only by its mass concentration but also by its chemical composition, including major constituents such as sulfate (SO42-), nitrate (NO3-), ammonium (NH4+), organic matter (OM), and black carbon (BC)[12]. These components differ markedly in their emission sources, oxidative potential, inflammatory activity, and ability to penetrate biological barriers, highlighting the importance of component-specific analyses for elucidating the reproductive toxicity of PM2.5[13,14]. Folliculogenesis is a continuous, month-long dynamic process from primordial follicle recruitment to ovulation, with potentially varying susceptibilities to environmental exposures at different stages[15,16]. Although recent research suggests that both short- and long-term PM2.5 exposure may adversely impact reproductive outcomes, the sensitive exposure windows of distinct chemical components remain poorly understood.
Assisted reproductive technology (ART) offers a unique opportunity to investigate the effects of environmental exposure on oocyte development. Through controlled ovarian hyperstimulation and oocyte retrieval, ART provides precise, quantifiable indicators of oocyte count and maturity, thereby minimizing confounding factors inherent in natural reproductive processes[17]. By leveraging a large ART cohort from southwestern China, this study systematically evaluated both the independent and combined effects of PM2.5 and its major chemical components on oocyte quantity and maturity across multiple exposure windows, considering both proximal exposures (near oocyte retrieval) and distal exposures (early folliculogenesis). By identifying sensitive exposure windows and characterizing component-specific toxicity patterns, this study advances mechanistic understanding of PM2.5-related reproductive toxicity. It provides important evidence to guide fertility preservation, clinical decision-making, and environmental health policies in ART populations.
-
This study used data from a prospectively established ART cohort at the Assisted Reproductive Center of Jinxin Xinan Women and Children’s Hospital, Sichuan Province, China. We retrospectively analyzed data from women who underwent in vitro fertilization (IVF) or intracytoplasmic sperm injection (ICSI) between January 2018 and December 2023 (n = 69,443)[18]. Demographic characteristics, residential addresses, and oocyte-related outcomes were obtained from the hospital's electronic medical records. Cycles with non-local residential addresses or missing address information were excluede (n = 9,291). Among the remaining cycles, exclusion criteria included age > 45 years, incomplete treatment records, donor oocyte use, chromosomal abnormalities, and polycystic ovary syndrome (PCOS)[19]. After applying these criteria, 51,122 cycles constituted the final analytic cohort (Supplementary Figure S1).
-
During assisted reproductive treatment, women underwent controlled ovarian stimulation (COS) to promote synchronous growth of multiple follicles, followed by transvaginal oocyte retrieval at a clinically optimal time[20,21]. The retrieved oocytes were classified into germinal vesicle (GV), metaphase I (MI), metaphase II (MII), and degenerated stages[22]. Total oocyte yield was defined as the number of oocytes retrieved regardless of maturity, whereas mature oocytes were identified as those at the MII stage[23]. Depending on clinical indications, fertilization was performed using conventional IVF or ICSI. Fertilization outcomes were assessed microscopically 17–20 h post insemination, with the presence of two pronuclei indicating normal fertilization[24].
-
Daily average concentrations of PM2.5 and its major components (SO42-, NO3-, NH4+, OM, and BC) were obtained from the Tracking Air Pollution in China (TAP) database (http://tapdata.org.cn). The TAP system integrates ground-based monitoring data, satellite-derived aerosol optical depth, chemical transport model outputs, and auxiliary variables (e.g., meteorology, land use, population density, and elevation) to estimate pollutant levels nationwide at a spatial resolution of approximately 10 km using a two-stage machine learning framework[25,26]. Validation against ground measurements yielded daily correlation coefficients of 0.67–0.80 for 2013–2020, demonstrating good accuracy and reliability[26]. The TAP dataset has been widely used in epidemiological studies of air pollution and health[27,28]. Daily temperature and relative humidity data were retrieved from the National Oceanic and Atmospheric Administration (NOAA, https://www.ncei.noaa.gov/data/global-summary-of-the-day/archive/). The participants’ residential addresses were geocoded in latitude and longitude coordinates, which were used to assign daily exposure estimates for pollutants and meteorological factors.
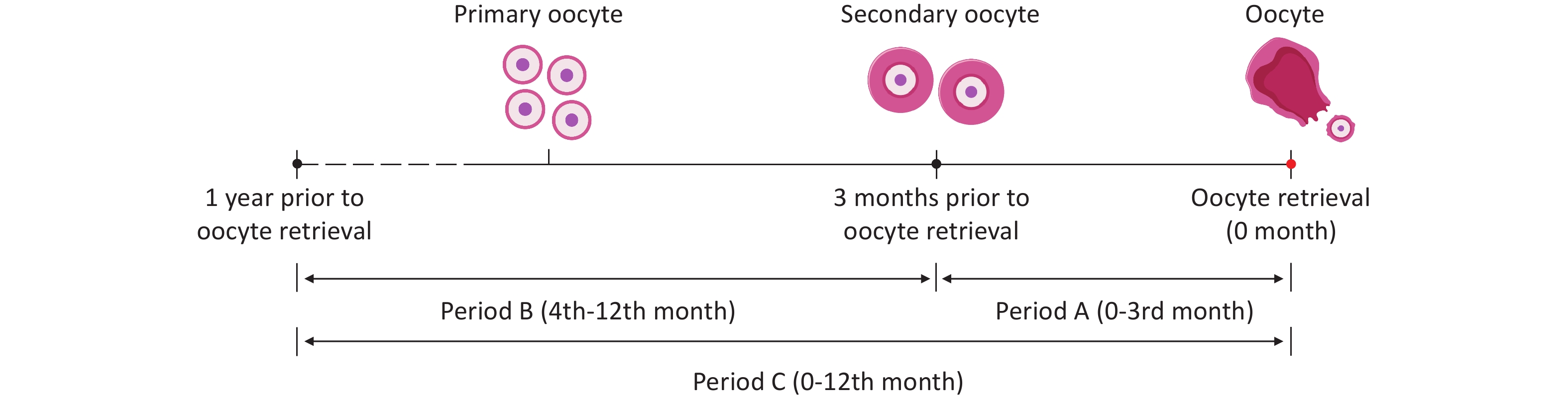
To comprehensively evaluate the effects of air pollution on follicular development and oocyte-related outcomes, three exposure windows were defined (Figure 1): Period A, the first 3 months before oocyte retrieval, covering the critical phase of follicle development from secondary follicles to mature follicles[29]; Period B, from the 4th to the 12th month before oocyte retrieval (9 months), focusing on the early stages of follicular development and evaluating the impact of early exposure on follicle quality and developmental potential; and Period C, one year before oocyte retrieval, examining the potential effects of long-term continuous pollutant exposure on follicular development. By defining multiple temporal windows, this study aimed to assess the impact of air pollution on oocyte-related outcomes from different temporal perspectives, thereby providing a comprehensive understanding of its reproductive toxicity.
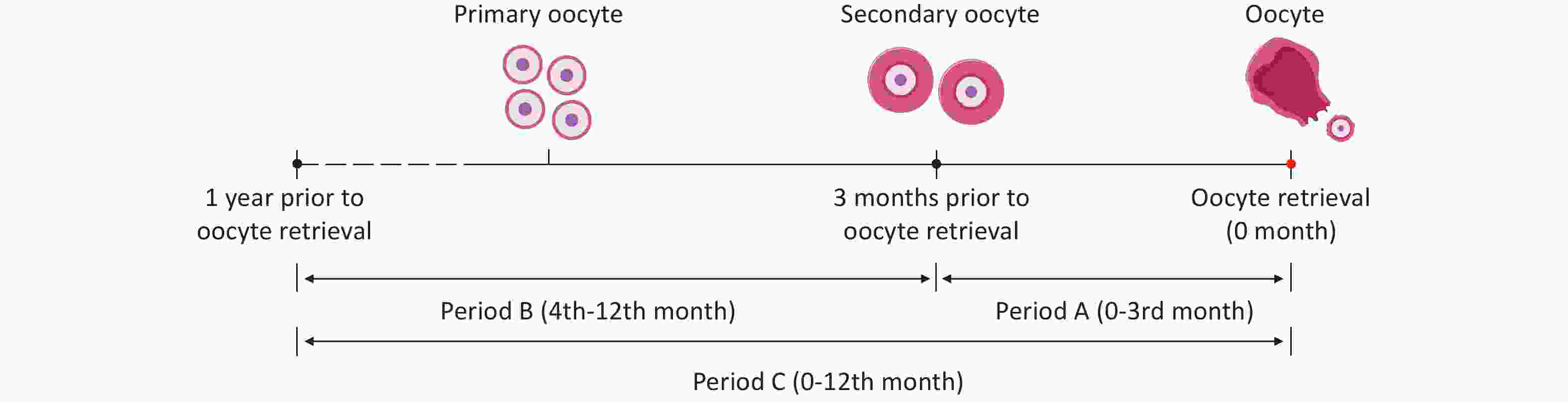
Figure 1. The schematic diagram of three exposure windows at different time scales during follicular development. Period A: The first 3 months before oocyte retrieval; Period B:From the 4th to the 12th month before oocyte retrieval (9 months); Period C:One year before oocyte retrieval.
-
Baseline characteristics were summarized descriptively, with categorical variables presented as counts and percentages and continuous variables as means (SD) or medians (IQRs), depending on the distribution. Air pollutants and meteorological variables are described for all exposure windows. Correlations between PM2.5 and its major components were assessed using Spearman’s rank coefficients. Associations among PM2.5 exposure and oocyte-related outcomes were estimated using negative binomial regression models. Results are expressed as relative risks (RRs) and 95% confidence intervals (CIs) for each interquartile range increase in pollutant concentrations. To further investigate the potential temporal windows of air pollution effects on oocyte-related outcomes, we applied distributed lag non-linear models (DLNM) to estimate the non-linear, lagged associations between monthly PM2.5 and its major components and oocyte quantity and maturity. Both prior literature-guided covariate selection and a directed acyclic graph (DAG) were used to identify the minimal sufficient adjustment set for estimating the total effect of PM2.5 exposure on oocyte outcomes (Supplementary Figure S2)[9,15]. The final set included maternal age, body mass index (BMI), infertility type, stimulation protocol, and relative humidity. To account for seasonal variation, the oocyte retrieval season was modeled as a categorical variable.
Additionally, to capture the potential non-linear effects of ambient temperature, a natural cubic spline term was introduced to model the relationship between temperature and oocyte outcomes. Model node selection was optimized using the Akaike Information Criterion (AIC)[18]. All the models were adjusted for pre-defined covariates. Comparisons between exposure periods (A vs. B) were evaluated using Wald χ2 tests based on linear hypotheses testing the equality of regression coefficients derived from the negative binomial regression models. Subgroup analyses were conducted by age and BMI, and multiplicative interaction terms were tested for effect modification.
To assess the combined effects of PM2.5, quantile-based G-computation (Qgcomp) and weighted quantile sum (WQS) regression models were applied using Poisson distributions to estimate the mixture effects and component weights, adjusting for the same covariates as in the main models. To ensure the robustness of our findings, several sensitivity analyses were performed: (1) modeling exposure quartiles (Q1–Q4 and Q1 as reference) to test for linear trends and visualize marginal means, and (2) restricting analyses to IVF cycles to account for sperm quality and procedural differences.
To control for multiple testing, P values were adjusted using the Benjamini–Hochberg false discovery rate (FDR) method. All analyses were performed in R (version 4.3.1), with two-sided P < 0.05 considered statistically significant.
-
In total, 51,122 women were included in this study, and each participant provided data from a single ART treatment cycle. The baseline characteristics of the study population are summarized in Table 1. The mean age of the participants was 31.74 years, and 74.1% were younger than 35 years. Secondary infertility was observed in 52.09% of participants. Among the COS protocols, the gonadotropin-releasing hormone antagonist (GnRH-ant) regimen was most commonly used, accounting for 55.19% of the cycles. During the oocyte retrieval season, the highest proportion was observed in summer (30.85%). As for oocyte-related outcomes, the median number of total oocytes retrieved, mature oocytes, and normally fertilized oocytes was 10.00, 9.00, and 6.00, respectively.
Characteristic Age (years),mean ± SD 31.74 (4.61) Age (years),n (%) < 35 37,871 (74.08) ≥ 35 13,251 (25.92) BMI (kg/m2),mean ± SD 22.10 (3.11) BMI (kg/m2),n (%) < 18.5 4,889 (9.56) 18.5−23.9 33,619 (65.76) ≥ 24 12,614 (24.67) Infertility type,n (%) Primary 24,492 (47.90) Secondary 26,630 (52.09) COS protocol,n (%) GnRH agonist 14,589 (28.53) GnRH antagonist 28,216 (55.19) Others 8,317 (16.27) Season of oocyte retrieval,n (%) Spring (March-May) 14,377 (28.12) Summer (June-August) 15,771 (30.85) Autumn (September-November) 11,769 (23.02) Winter (December-February) 9,205 (18.01) Total oocyte yield,median (IQR) 10.00 (6.00,15.00) Mature oocyte yield,median (IQR) 9.00 (5.00,13.00) Normally fertilized oocyte,median (IQR) 6.00 (3.00,10.00) Note. SD,standard deviation; IQR,interquartile range; BMI,body mass index; COS,controlled ovarian stimulation; GnRH,gonadotropin-releasing hormone. Table 1. Demographic and clinical characteristics of study subjects
The exposure levels to PM2.5, its five components, temperature, and relative humidity across the different exposure periods are presented in Supplementary Table S1. During the one year before oocyte retrieval, the median ambient PM2.5 concentration was 41.21 µg/m3 (IQR: 33.74–45.57 µg/m3). Among the five PM2.5 components analyzed, OM had the highest concentration, followed by NO3-, SO42-, NH4+, and BC. Spearman’s rank correlation analysis indicated strong correlations between PM2.5 and its components, with correlation coefficients (rs) ranging from 0.80 to 0.99, all statistically significant (P < 0.001; Supplementary Figure S3).
-
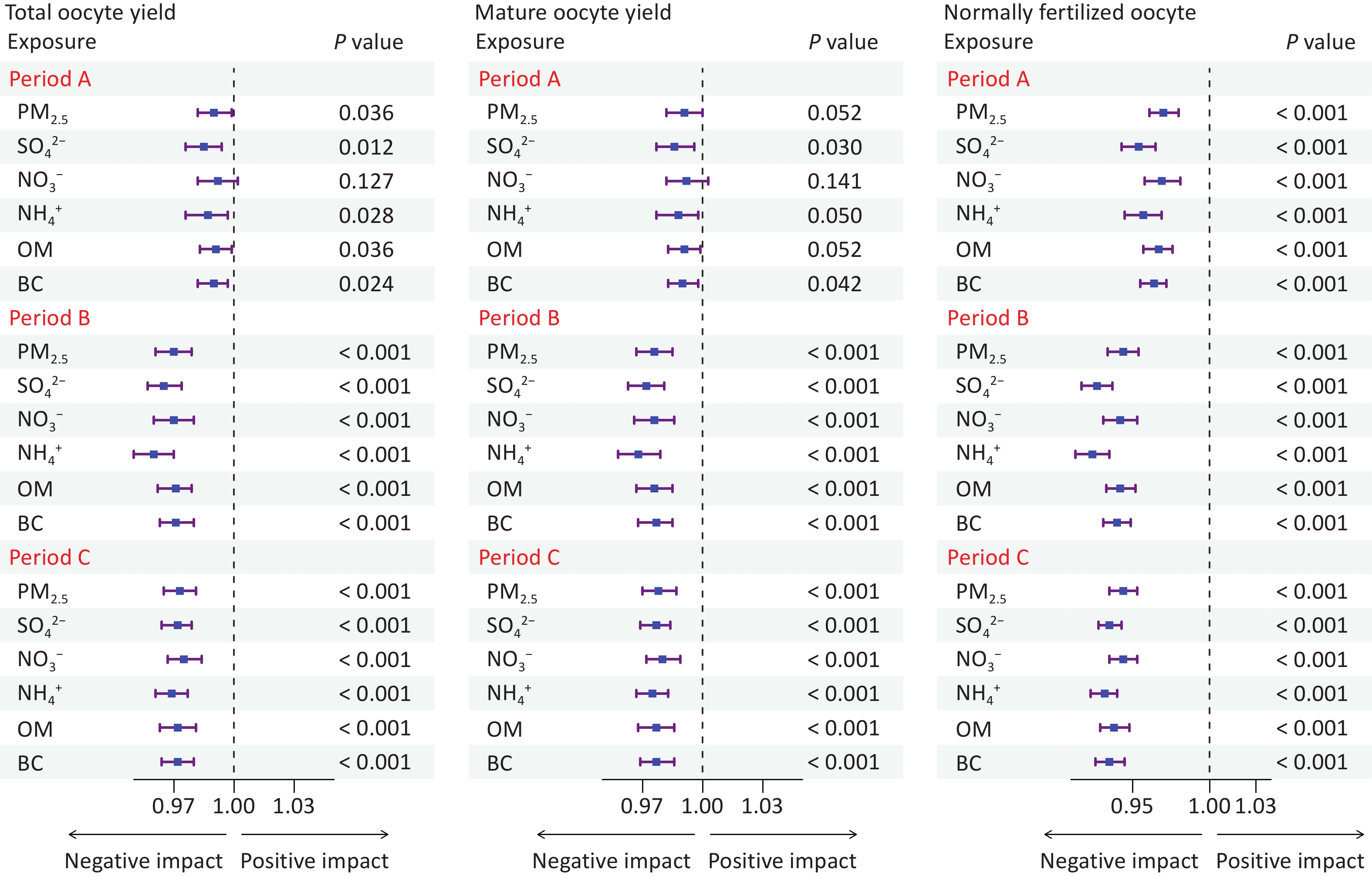
We evaluated the association between the increase in the IQR of air pollutant concentrations across different exposure periods and oocyte-related outcomes using fully adjusted negative binomial regression models (Figure 2, Supplementary Table S2). In exposure Period A, exposures to PM2.5 and its components, except NO3-, showed significant negative associations with the total number of oocytes retrieved (adjusted P-values < 0.05). Regarding the number of mature oocytes, significant negative associations were observed only with SO42-, NH4+, and BC. Although exposure to PM2.5, NO3-, and OM was not significantly associated with the number of mature oocytes (adjusted P-values > 0.05), their estimated effects remained negative, for the number of normally fertilized oocytes, exposure to PM2.5 and all its components were significantly negatively associated with the outcome (all adjusted P-values < 0.05). During exposure Periods B and C, higher air pollutant levels were consistently associated with significantly reduced counts across all three oocyte-related outcomes (all adjusted P-values < 0.05). Wald χ2 tests indicated that the effect estimates in Period B were significantly stronger than those in Period A, suggesting greater sensitivity of oocyte-related outcomes to pollutant exposure during Period B (all P-values < 0.05).
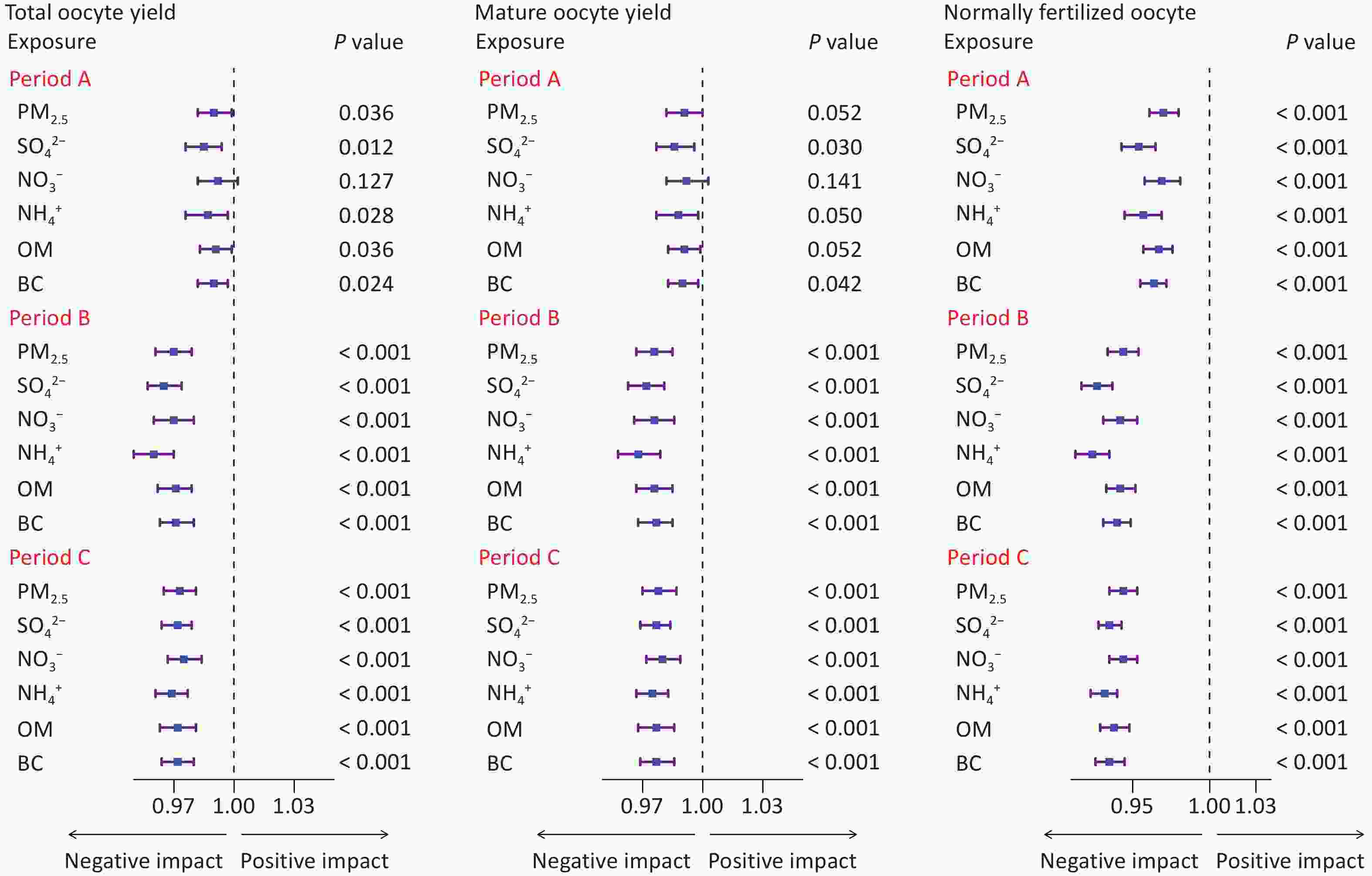
Figure 2. Association between ambient PM2.5 and its components exposure and oocyte-related outcomes during different exposure Periods. Models were adjusted for age,body mass index,infertility types,COS protocols,season of oocyte retrieval,temperature,and relative humidity.The reported P-values are adjusted using the Benjamini & Hochberg (BH) procedure.All Wald χ2 tests comparing effect estimates for windows A vs.B were significant (P < 0.05).Period A:The first 3 months before oocyte retrieval; Period B:From the 4th to the 12th month before oocyte retrieval (9 months); Period C:One year before oocyte retrieval.:SO42:-,sulfate; NO3:-,nitrate; NH4:+,ammonium; OM:,organic matter; BC:,black carbon.
-
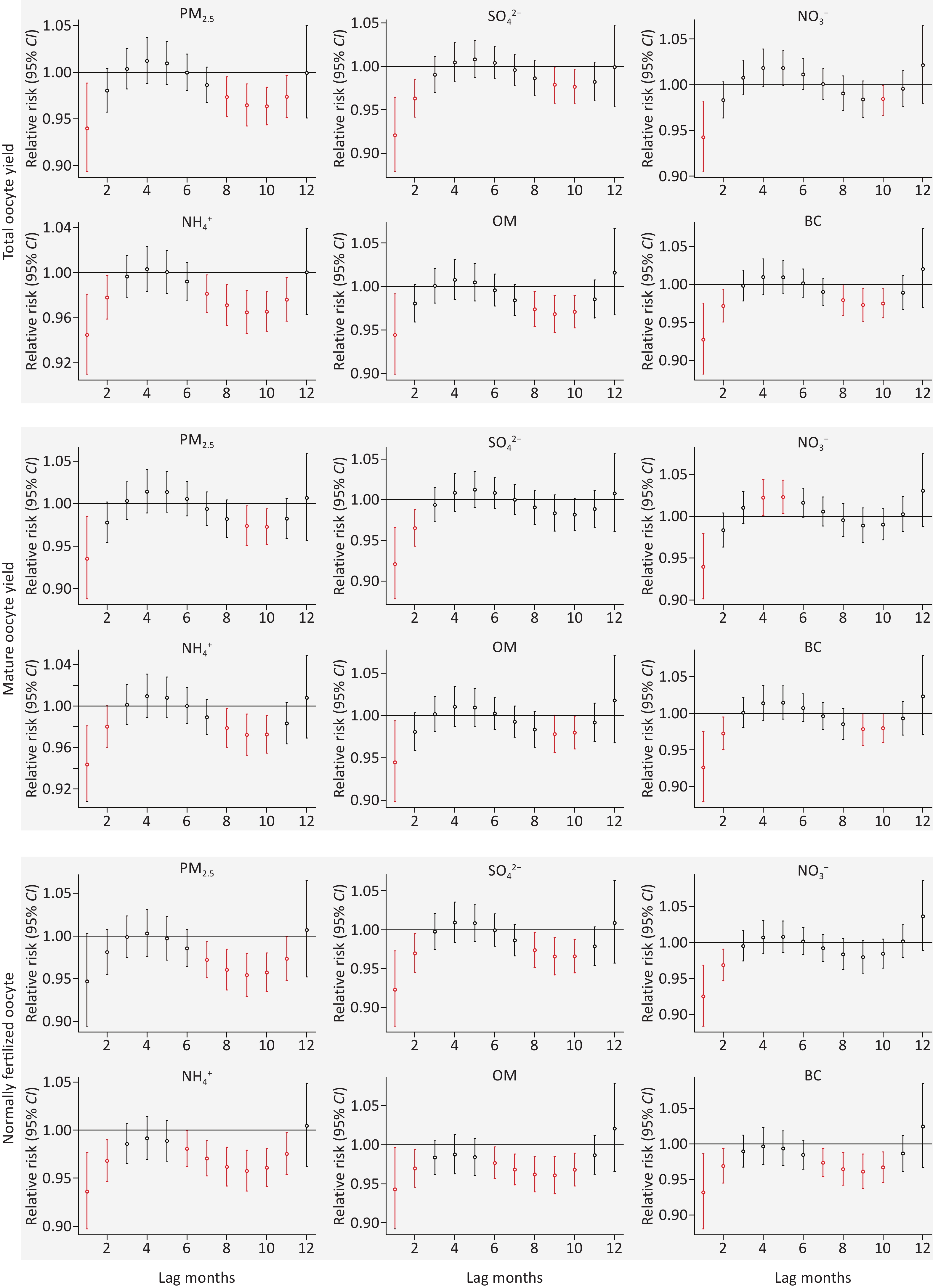
To identify potentially sensitive windows, we applied a DLNM within a negative binomial regression framework to assess the monthly lagged associations between ambient PM2.5 exposure and oocyte-related outcomes over the 12 months preceding oocyte retrieval. Figure 3 illustrates the RRs associated with an interquartile range increase in PM2.5 and its components at each monthly lag (lag 1–lag 12). We observed that exposure to PM2.5, at lag 1 and lags 7–11, was significantly associated with an increased risk of adverse oocyte-related outcomes. For PM2.5, significant lag-specific effects were concentrated mainly at lags 1–2 and 6–11, indicating the presence of both proximal- and distal-sensitive exposure windows.
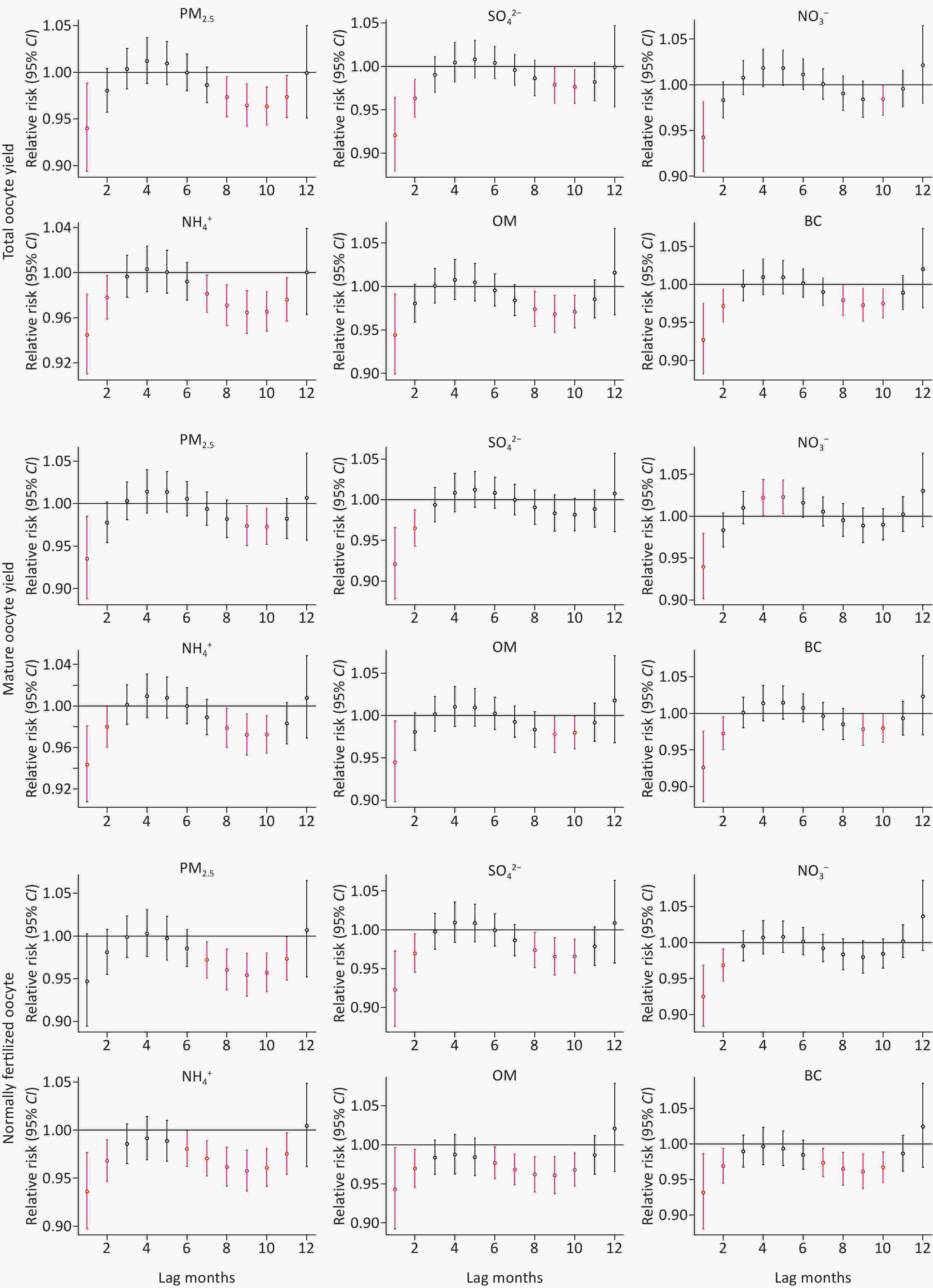
Figure 3. Lagged effects of monthly average exposure to PM2.5 and its major chemical components within one year before oocyte retrieval on the risk of adverse oocyte-related outcomes. The model was adjusted for age,body mass index,infertility types,COS protocols,season of oocyte retrieval,temperature,and relative humidity.The x-axis represents lag months (with 0 indicating the day of retrieval),and the y-axis depicts relative risks.Hollow circles denote the estimated relative risks,and the error bars show the corresponding 95% confidence intervals.Error bars are highlighted in red when the confidence interval does not include 1,indicating potentially sensitive exposure windows.
-
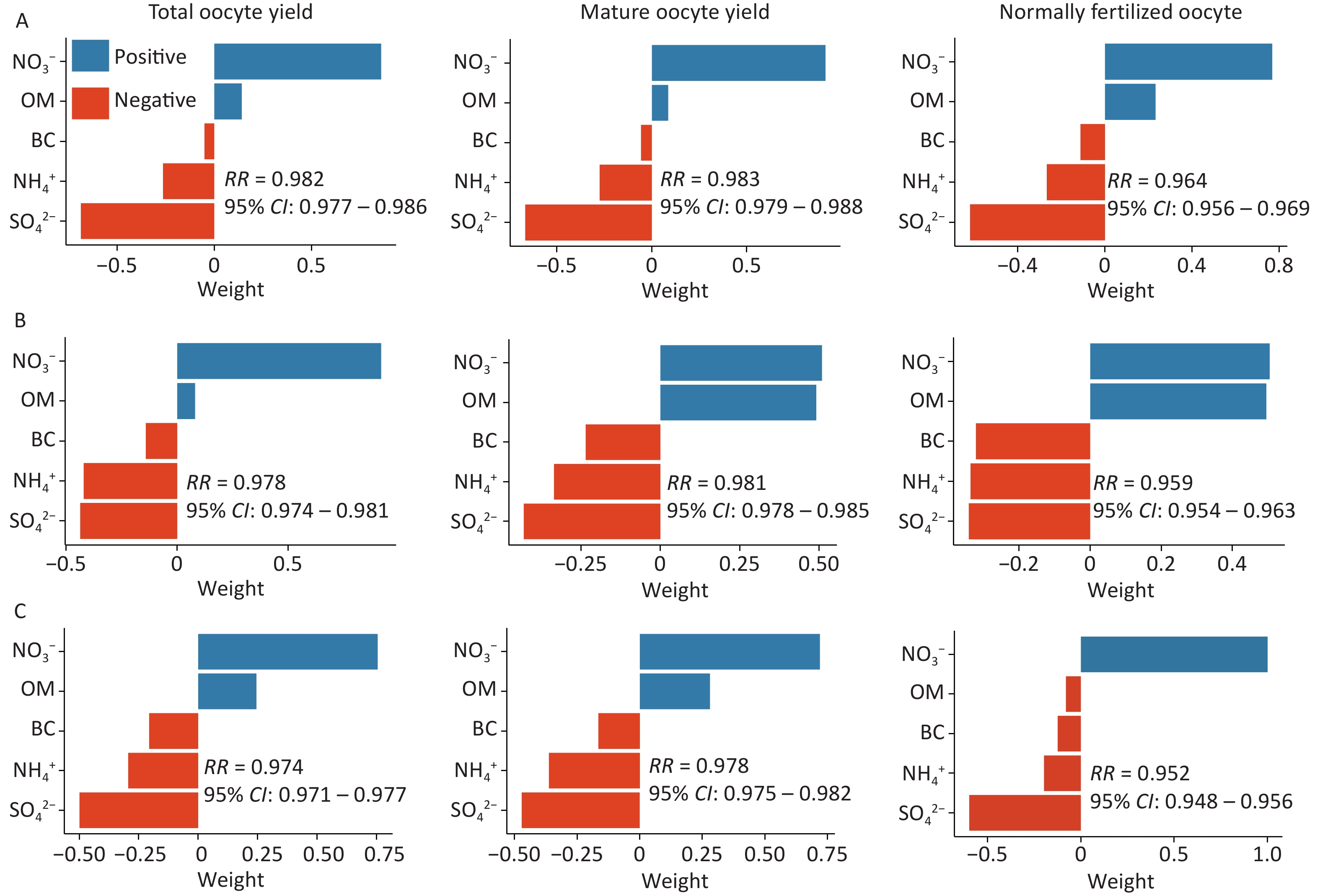
Table 2 summarizes the results of the mixed-pollutant analysis using the Qgcomp and WQS regression models. The Qgcomp model demonstrated that across different exposure periods, each 1-quartile increase in the air pollutant mixture was significantly associated with a decrease in the number of oocytes (adjusted P-values < 0.05). Specifically, in exposure Period A, total oocyte yield decreased by 1.85% (95% CI: –2.26%, –1.43%), mature oocyte yield decreased by 1.68% (95% CI: –2.13%, –1.24%), and the number of normally fertilized oocytes decreased by 3.61% (95% CI: –4.10%, –3.11%). Across most exposure periods, SO42- and NH4+ had the most significant negative effects on oocyte-related outcomes and the largest negative weights (Figure 4). WQS analysis also showed a significant negative correlation between mixed pollutants and oocyte-related outcomes across the three exposure periods. During exposure Periods A and C, SO42- and NH4+ contributed the most to the overall mixed effect, which is consistent with the results of the Qgcomp model. During exposure Period B, SO42- and BC made the largest contributions to the mixed effect (Supplementary Figure S4).
Outcomes RR (95% CI) Index weight SO42- NO3- NH4+ OM BC Qgcomp Total oocyte yield Period A 0.982 (0.977,0.986) −0.686 0.859 −0.263 0.141 −0.051 Period B 0.978 (0.974,0.981) −0.421 0.919 −0.437 0.081 −0.142 Period C 0.974 (0.971,0.977) −0.206 0.755 −0.499 −0.294 0.245 Mature oocyte yield Period A 0.983 (0.979,0.988) −0.667 0.914 −0.275 0.086 −0.058 Period B 0.981 (0.978,0.985) −0.335 0.509 −0.430 0.491 −0.235 Period C 0.978 (0.975,0.982) −0.166 0.720 −0.471 −0.363 0.280 Normally fertilized oocyte Period A 0.964 (0.959,0.969) −0.620 0.768 −0.267 0.232 −0.113 Period B 0.959 (0.954,0.963) −0.322 0.495 −0.337 0.505 −0.342 Period C 0.952 (0.948,0.956) −0.198 1.000 −0.598 −0.124 −0.080 WQS regression a Total oocyte yield Period A 0.980 (0.975,0.984) 0.342 0.165 0.165 0.164 0.164 Period B 0.980 (0.975,0.984) 0.276 0.154 0.160 0.159 0.251 Period C 0.976 (0.972,0.980) 0.294 0.146 0.241 0.167 0.151 Mature oocyte yield Period A 0.980 (0.975,0.986) 0.336 0.164 0.172 0.163 0.164 Period B 0.983 (0.979,0.988) 0.227 0.190 0.176 0.147 0.260 Period C 0.981 (0.976,0.985) 0.284 0.158 0.228 0.171 0.160 Normally fertilized oocyte Period A 0.961 (0.955,0.967) 0.615 0.089 0.111 0.091 0.094 Period B 0.959 (0.954,0.964) 0.324 0.109 0.215 0.110 0.242 Period C 0.953 (0.948,0.957) 0.333 0.088 0.374 0.105 0.100 Note. The models were adjusted for age,body mass index,infertility type,COS protocol,season of oocyte retrieval,temperature,and relative humidity.:RR:,relative risk; 95%CI,:95% confidence interval; SO42-,:sulfate; NO3-,:nitrate; NH4+,:ammonium; OM,:organic matter; BC,:black carbon; Period A:the first 3 months before oocyte retrieval; Period B,:from the 4th to the 12th month before oocyte retrieval (9 months); Period C,:one year before oocyte retrieval.Negative mixed weights were obtained using the Qgcomp model,which assesses the relationship between a mixture of air pollutants and the outcomes. aIn the WQS regression,we constrained each mixture component effect to be negative based on findings from the individual model. Table 2. Estimated joint associations and weights of PM2.5 component exposures on oocyte-related outcomes based on the Qgcomp and WQS regression
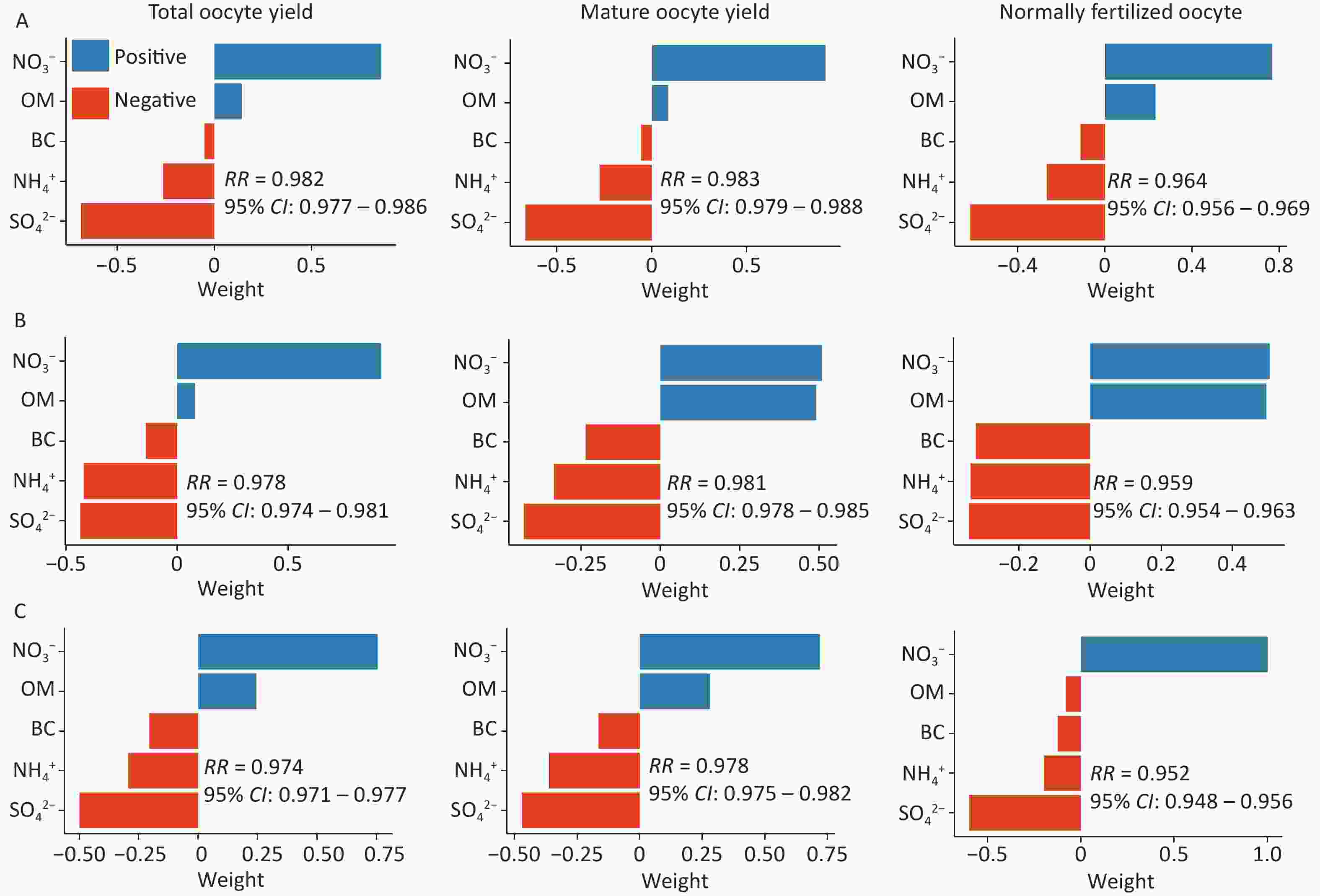
Figure 4. Qgcomp model regression weights of PM2.5 component mixture on oocyte-related outcomes during different exposure periods. Models were adjusted for age,body mass index,infertility types,COS protocols,season of oocyte retrieval,temperature,and relative humidity.Period A:The first 3 months before oocyte retrieval; Period B:From the 4th to the 12th month before oocyte retrieval (9 months); Period C:One year before oocyte retrieval.:SO42:,sulfate; NO3-,:nitrate; NH4+,:ammonium; OM,:organic matter; BC,:black carbon.
-
In the subgroup analysis (Supplementary Figures S5–S7), we found that during exposure Periods B and C, PM2.5 and its components were significantly associated with a reduction in the number of oocytes across age subgroups. However, during exposure Period A, only a significant negative correlation was observed between pollutants and the number of normally fertilized oocytes. For total oocyte yield and mature oocyte yield, although the direction of the association was consistent with pollutant exposure, neither reached statistical significance. In the normal BMI group (18.5–23.9 kg/m2), exposure to PM2.5 and its components during Periods B and C was significantly associated with a decrease in oocyte yield. In contrast, in the group with BMI ≥ 24 kg/m2, this association was even more pronounced. Interaction tests indicated that BMI significantly moderated this association (interaction P-value < 0.05). This suggests that BMI may influence the relationships among PM2.5, its components, and oocyte-related outcomes across different exposure periods. Detailed data can be found in Supplementary Tables S3–S4.
-
The results of the sensitivity analyses supported the findings of this study. Using a fully adjusted negative binomial regression model, we calculated the marginal means of PM2.5 and its components at quartiles of exposure during different exposure periods (Supplementary Figure S8; detailed data in Supplementary Tables S5–S7). The results indicated that increased exposure to PM2.5 and its components significantly reduced oocyte count across all exposure periods. Furthermore, when the study population was limited to women undergoing IVF treatment, the results remained consistent, further demonstrating the robustness of the association between PM2.5 and its components and oocyte-related outcomes (Supplementary Table S8).
-
This study included 51,122 women undergoing ART and systematically evaluated the independent and joint effects of PM2.5 and its major chemical components across different exposure windows on oocyte-related outcomes. The results demonstrated that both short-term critical exposure and long-term cumulative exposure to PM2.5 and its components were significantly associated with reductions in oocyte quantity and quality. Our findings further suggest that the early stages of follicular development are particularly susceptible to environmental pollution. Mixture analysis identified sulfate and ammonium as the primary harmful contributors, indicating an important role of secondary inorganic aerosols in PM2.5-related reproductive toxicity.
We observed that higher exposure to PM2.5 and its components was significantly associated with decreased oocyte yield. As one of the most direct and sensitive indicators of ART, oocyte yield not only reflects the number of recruited follicles but also partially represents overall ovarian function and oocyte developmental competence. Clinically, poor ovarian response (POR) is typically characterized by a marked reduction in oocyte yield[30]. However, POR is a composite phenotype involving impaired ovarian responsiveness, disrupted follicular development, and reduced oocyte quality, which complicates precise identification of the stages at which pollutants exert their effects. In contrast, oocyte yield, a more direct quantitative measure, facilitates detection of progressive functional impairments before they reach the diagnostic threshold for POR. Previous studies have reported an association between air pollution exposure and increased POR risk[18,31], and epidemiological evidence indicates that environmental pollution can reduce antral follicle count (AFC)[32]. AFC is a key indicator of ovarian reserve and early follicle recruitment capacity, reflecting the size of the pool of recruitable follicles.
In contrast, oocyte yield represents the final output of follicles that reach the ovulatory stage. These two metrics are biologically continuous[29]. Therefore, the observed reduction in oocyte yield in this study, in conjunction with previously reported declines in AFC, supports the notion that environmental exposure may negatively affect follicle number early in folliculogenesis.
Furthermore, exposure to PM2.5 and its components was also significantly associated with reductions in mature oocyte count and the number of normally fertilized oocytes, suggesting that pollutants may impair both follicle recruitment and oocyte maturation/fertilization potential. The mature oocyte count reflects follicular development and oocyte maturation quality, whereas the normally fertilized oocyte count represents fertilization capacity; together, they indicate overall follicular health and embryonic developmental potential[2]. Pollutant-induced oxidative stress, inflammatory responses, and mitochondrial dysfunction may disrupt chromosomal segregation, cytoplasmic maturation, and fertilization preparation processes, thereby reducing oocyte quantity and impairing functionality[33,34]. These results indicate that air pollution cumulatively and in a stage-specific manner affects ovarian function, affecting not only oocyte yield but also oocyte maturation and embryonic developmental potential.
Our findings indicate that folliculogenesis exhibits a stage-specific sensitivity to environmental stressors. A comparison across exposure windows showed that recent exposure (0–3 months before oocyte retrieval, Period A) corresponds to the rapid growth phase of follicles, during which oocytes exhibit high metabolic activity and immature antioxidant defenses, making them susceptible to environmental stress[1,35]. Exposure during Period A was consistently and negatively associated with oocyte quantity and developmental potential, consistent with a large-scale cohort study reporting reduced oocyte yield following approximately three months of pre-retrieval exposure[36]. In contrast, distant exposure (4–12 months before retrieval, Period B) corresponds to the early stage of the primordial-to-primary/secondary follicle transition, which is highly dependent on homeostasis of the ovarian microenvironment[1]. In this study, the pollutant effects during Period B were generally stronger than those during Period A, suggesting that cumulative interference during early follicular development may be particularly critical. Potential mechanisms may include persistent oxidative stress and chronic inflammation, which can impair ovarian microvascular function, disrupt stromal microcirculation, compromise the nutrient and signaling environment required for follicle development, and perturb endocrine homeostasis and follicle recruitment, ultimately affecting early oocyte developmental trajectories[37-40]. Additionally, human tissue studies have shown that particulate matter can accumulate in ovarian tissue, providing direct evidence of long-term disruption of the early follicular microenvironment[41].
DLNM further characterized the time-dependent associations between PM2.5 exposure and oocyte outcomes, identifying multiple relatively independent sensitive periods. While lag effects varied across outcomes, the most sensitive windows were observed at 1–2 and 6–11 months before oocyte retrieval, indicating stage-specific temporal responses. The DLNM results were highly consistent with the regression analyses based on pre-defined exposure windows, both showing stable negative associations between pollutant exposure and oocyte outcomes across temporal scales. Collectively, these analyses support a coherent time-dependent susceptibility framework, in which PM2.5 can cause proximal damage during rapid follicular growth and induce long-term cumulative effects during early follicular stages, resulting in additive reproductive toxicity across multiple stages of folliculogenesis. These findings enhance our understanding of multi-stage PM2.5 reproductive toxicity and highlight the importance of considering short-, long-, and lag-specific exposures when assessing environmental risk in women undergoing ART.
Although stable negative associations between PM2.5 exposure and oocyte outcomes were observed across multiple models in this study, previous findings have been inconsistent[42,43]. Such discrepancies may reflect differences in regional pollution sources and particulate chemical composition, suggesting that analyses based solely on PM2.5 may inadequately capture reproductive toxicity[44]. Therefore, this study further analyzed the chemical components to identify key risk factors. Sulfate, ammonium, and black carbon have been identified as the primary contributors to adverse oocyte outcomes. Toxicological evidence indicates that sulfate and ammonium, as major secondary inorganic aerosol components, can impair the follicular microenvironment through oxidative stress, endocrine disruption, and inflammatory responses, thereby interfering with follicle recruitment and development[45,46]. Although OM and NO3− accounted for relatively larger proportions of PM2.5 mass in the study area, the mixture models consistently identified SO42− and NH4+ as the dominant toxic contributors. This finding suggests that the toxic contribution may not necessarily correspond to the mass proportion. Still, it may instead reflect the relatively stronger intrinsic biological toxicity and oxidative potential of sulfate- and ammonium-related secondary inorganic aerosols. Previous studies have shown that these components may have an enhanced capacity to induce reactive oxygen species generation and inflammatory responses, thereby contributing to oxidative stress-related reproductive damage[47,48]. Black carbon, due to its high adsorption and pollutant-carrying capacities, may facilitate the translocation of organic pollutants and heavy metals across biological barriers and their accumulation in ovarian tissue, thereby causing persistent damage to oocyte maturation and fertilization potential[41].
Comparisons across studies have revealed regional differences in the dominant harmful components, with some emphasizing nitrate, traffic-related particles, or organic components[15,49]. Such inconsistencies likely reflect genuine differences in regional pollution source profiles rather than statistical fluctuations or model selection biases[50]. For example, the Sichuan Basin, influenced by its energy structure and meteorology, has a higher proportion of secondary inorganic salts in PM2.5[51-53]. In contrast, regions dominated by industrial and traffic emissions show PM2.5 compositions enriched in nitrate and organic carbon[54]. Variations in pollution source composition can alter the physicochemical properties and bioavailability of particulates, thereby modulating the intensity and pathways of reproductive toxicity.
Subgroup analyses suggested that individual characteristics may modify PM2.5-related reproductive effects. No significant differences were observed across age groups; however, adverse effects were more pronounced in women with normal or elevated BMI. This may be related to the differences in metabolism, baseline inflammation, and endocrine regulation. Obesity is often accompanied by chronic low-grade inflammation and heightened oxidative stress, which may reduce ovarian resilience to external insults[55]. Adipose tissue may also serve as a reservoir for lipophilic or particle-bound pollutants, thereby prolonging systemic retention and amplifying long-term toxicity[56]. Furthermore, obesity-related disruptions in estrogen metabolism and insulin signaling may perturb the follicular microenvironment, exacerbating pollutant-induced reproductive impairment[57].
This study has several methodological and contextual strengths. First, the inclusion of over 50,000 ART cycles provided substantial statistical power and minimized random variation and selection bias, enabling precise assessment of associations between PM2.5 components and oocyte outcomes. Second, the use of both single-pollutant and mixture models allowed for the identification of component-specific contributions and enhanced robustness. Third, multiple exposure windows combined with DLNM enabled evaluation of both lagged and non-linear exposure–response relationships, facilitating accurate identification of sensitive periods and temporal characterization of reproductive effects. Finally, the coverage of major cities in the Sichuan Basin, an area with persistent air pollution but limited prior studies, extends its geographic relevance and provides empirical data for regional public health assessments.
This study has some limitations. Participants were recruited from a single reproductive center in Southwest China, which ensures consistency in data and treatment but may limit generalizability. Lifestyle data, such as smoking, alcohol intake, diet, and occupational exposure, were partially unavailable. Additionally, information on indoor air pollution sources, including cooking oil fumes and secondhand smoke, could not be assessed comprehensively due to the retrospective nature of the ART clinical database. However, given the relatively low prevalence and exposure intensity of these factors among women undergoing ART, their impact on effect estimates is likely to be limited. Any incomplete assessment is more likely to introduce non-differential bias, potentially attenuating rather than exaggerating the observed associations[58,59]. Exposure assessment based on environmental monitoring data may not fully capture personal activity patterns or indoor exposures, potentially introducing a nondifferential bias that generally underestimates the true effects[60]. Differences in the physicochemical properties of pollutants may affect how environmental concentrations represent individual exposures; however, these factors are unlikely to create spurious stable associations. Minor residential mobility could also have biased the results. However, most participants were undergoing their first ART cycle and were long-term residents, making any misclassification more likely to attenuate the associations.
In conclusion, this study expands the framework for PM2.5 reproductive toxicity research by integrating continuous phenotypic characterization, fine-scale exposure windows, and chemical component analysis. Our findings emphasize the cumulative, multistage impact of air pollution on folliculogenesis and provide new epidemiological evidence to inform targeted environmental interventions and reproductive risk assessments for women undergoing ART.
-
This study systematically evaluated the effects of PM2.5 and its components on oocyte-related outcomes in ART across different exposure periods and identified key harmful constituents. These results emphasize the importance of reducing exposure during both critical and cumulative periods, highlighting the role of air quality management in protecting female reproductive health and improving ART outcomes, with implications for clinical practice and public health policies.
HTML
Study Population
Outcomes Assessment
Exposure Assessment and Window Setting
Statistical Analysis
Study Population Characteristics and Environmental Exposure
Relationship between Air Pollution and Oocyte-related Outcomes
Critical Sensitive Windows
Mixed Effects of Air Pollution Exposure on Outcomes
Subgroup Analysis
Sensitivity Analysis
Competing Interests The authors have no relevant financial or non-financial interests to disclose.
Ethics This study was approved by the Ethics Committees of Sichuan Jinxin Xinan Women and Children's Hospital (approval no. 2023001) and Chongqing Medical University (approval no. 2022133). All the procedures were performed in strict accordance with the ethical principles of the Declaration of Helsinki. As a secondary analysis of the previously collected data, all datasets were de-identified to protect patient privacy. The requirement for written informed consent was waived by the ethics committee following review.
Author Contributions Zhilei Xu: Conceptualization, Formal analysis, Methodology, Software, Visualization, Writing of the original draft. Ruiling Liu: Conceptualization, Formal analysis, Investigation, Software, Validation, Writing the original draft. Yuling Hu: Data curation, Investigation, Methodology, Project administration, Resources, Writing, review, and editing. Quanzi Yao: Data curation, Investigation, Software, Validation. Xin Luo: Funding acquisition, project administration, and supervision. Jialiang He: Data curation, Investigation, Methodology, Software, Validation. Lihong Geng: Funding acquisition, Methodology, Project administration, and supervision. Lijuan Fu: Funding acquisition, project administration, and supervision. Zhaohui Zhong: Methodology, Supervision, Writing, review, and editing. Yubin Ding: conceptualization, funding acquisition, Methodology, Project administration, Resources, Writing, review, and editing. Xingyu Lv: Funding acquisition, project administration, Supervision, Writing, review, and editing.
Data Sharing The supplementary materials will be available in www.besjournal.com.
&These authors contributed equally to this work.

 Quick Links
Quick Links
 DownLoad:
DownLoad: