

 下载:
下载:



-
Herpes zoster (HZ) is a painful condition resulting from reactivation of dormant varicella-zoster virus (VZV) in a previously VZV-infected person[1]. Typical clinical manifestation of HZ are unilateral radicular pain and a vesicular rash limited to one side of the body in the distribution of a nerve[2]. The most common complication of HZ postherpetic neuralgia (PHN), which occurs in 5% to 30% of HZ patients. PHN presents as severe, persistent pain that remains after the HZ rash has resolved[3]. Domestic studies found anti-VZV antibody seroprevalences of 95%-100% among individuals aged ≥ 30 years in China[4,5], indicating the near-universal, sizable pool of individuals at risk for HZ in China.
HZ is not a nationally notifiable condition in China, challenging population-based studies to estimate incidence of HZ. The availability of hospital-based electronic medical records makes it possible to estimate morbidity and complications through active surveillance studies. We used available electronic medical records to estimate HZ incidence in three cities in China during 2019–2020, extrapolating to the population level and analyzed clinical characteristics in three cities in China from 2019 to 2020 of HZ.
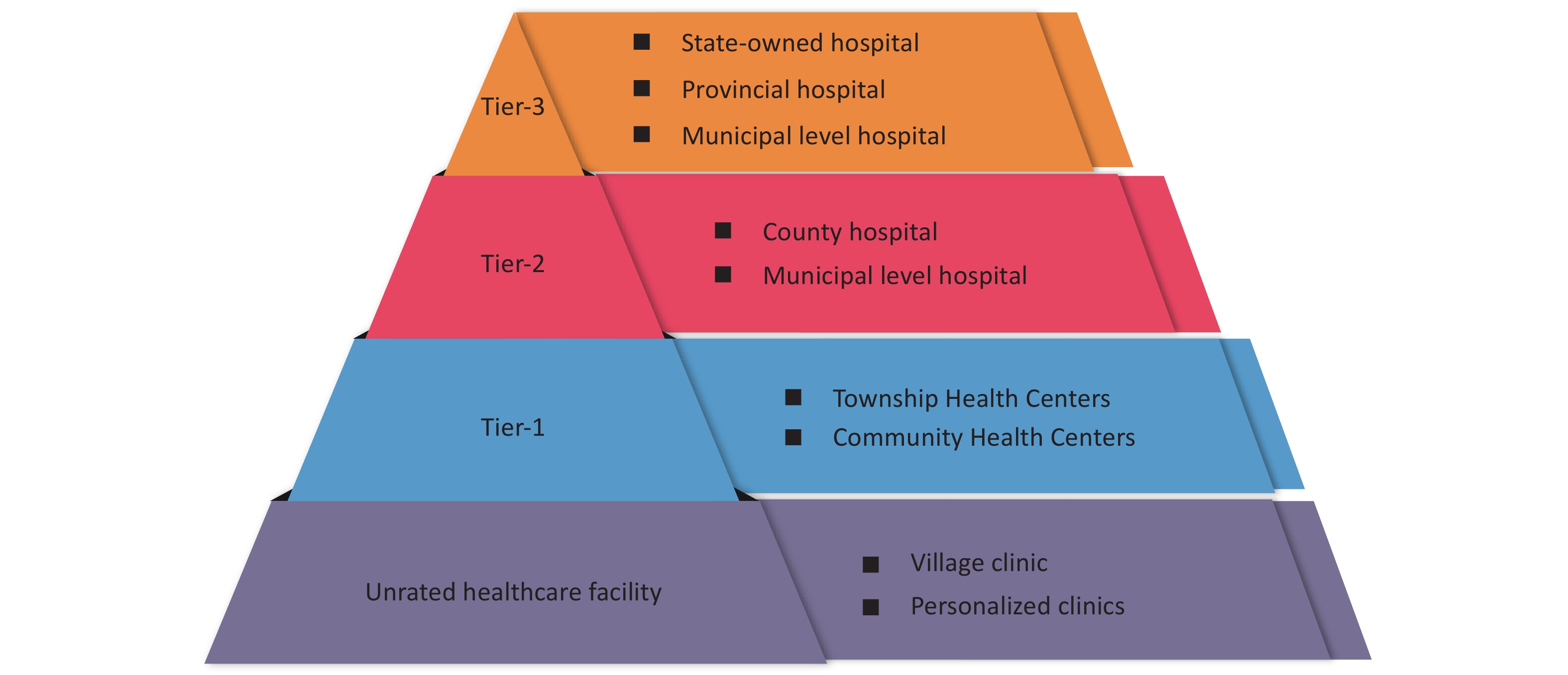
We selected a convenience sample of three non-provincial capital cities (Lu’an, Zibo, and Tongchuan). These cities were selected because they had relatively limited in-and-out population mobility, which could influence stability of incidence estimates. These cities experienced less stringent non-pharmaceutical interventions against COVID-19 during the study period, The population sizes of Lu’an, Zibo, and Tongchuan were 4.4 million, 4.7 million and 0.7 million respectively. We categorized all hospitals in the study setting according to data availability: those with full electronic medical record data, including clinical characteristics (Group A), those with only patient visit volume (Group B), and those for which only hospital type and level were known (Group C). We excluded specialized hospitals that lacked HZ case reports and did not provide care for HZ patients (orthopedic hospitals, stomatological hospitals, Tuberculosis control centers, and mental health centers) and personalized clinics. Supplementary Figure S1 (available in www.besjournal.com) shows hospital types and tiers in China.
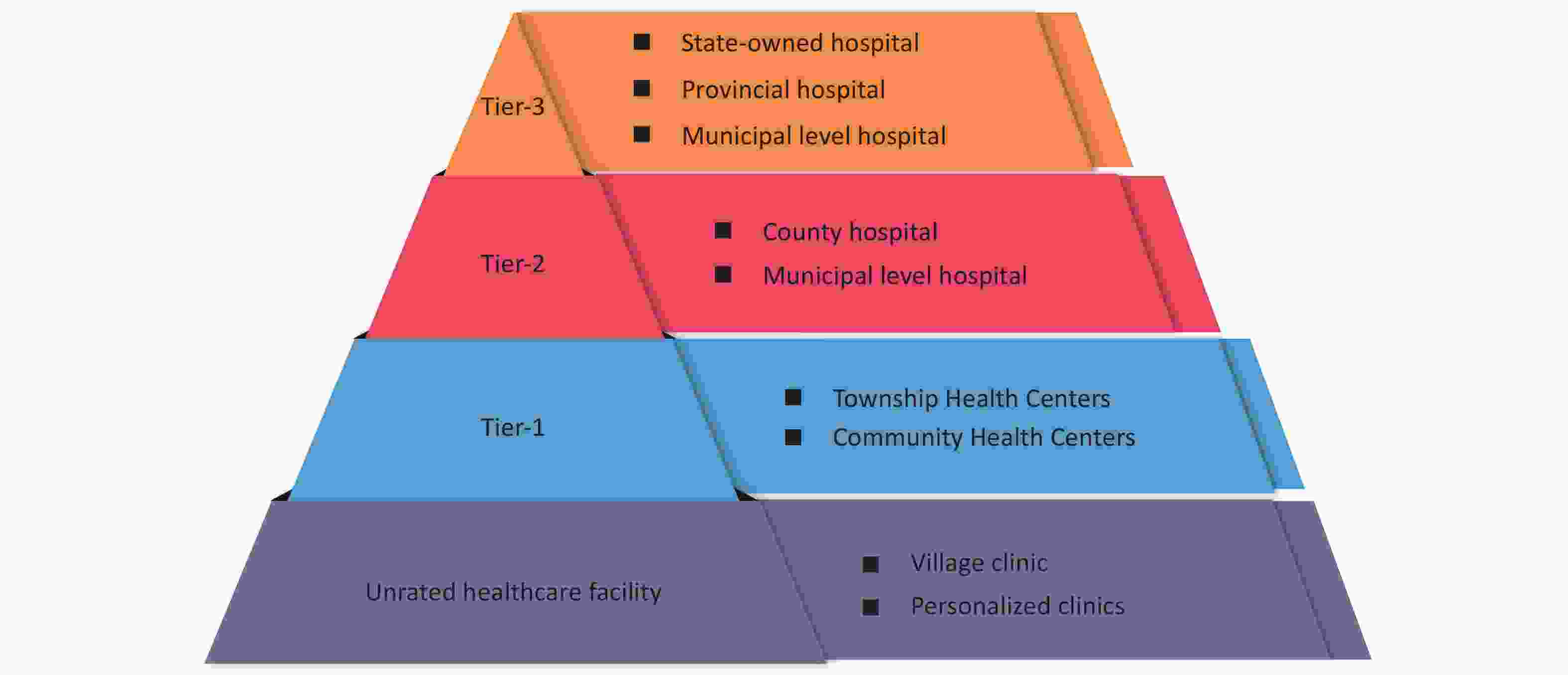
Figure S1. Three-tier system of hospitals in China.
Clinical data in Zibo was obtained from the electronic healthcare record database of the Zibo public health information platform, which integrates electronic medical records of all tier-2 and tier-3 hospitals and some primary hospitals in Zibo. Clinical data in Lu'an and Tongchuan were obtained from independent hospital information systems (HIS). The centers for disease control and prevention (CDCs) in the three cities determined hospital tier and type (
Supplementary Figure S1 ).In group A hospitals, we performed case searches with the terms, “Daizhuangpaozhen” “Daipao” “Daizhuang” “Chuanchuang”, and “HZ” to identify HZ cases seen during the study period of January 1, 2019 to December 31, 2020. All diagnoses related to herpes zoster were included.
From group B hospitals in Zibo and Lu’an, we obtained data on the annual number of visits across the entire facility. The number of HZ cases was estimated by extrapolation of the group A hospital proportion of HZ cases to all patient visits during the same study year and at the same tier and type of hospital using the formula, total visits in group B hospitals × (number of HZ cases in same tier and type group A hospitals / total number of group A hospital visits). The number of HZ cases in Tongchuan group B hospitals was similarly extrapolated, but with the refinement that the number of visits was specific to clinical departments: number of visits in specific departments × (number of HZ cases in the corresponding department of group A hospitals of the same tier and type / the total number of visits in all relevant clinic departments during the same study month) (
Supplementary Tables S1 –S3 , available in www.besjournal.com).For group C hospitals that lacked visit volume data, we estimated HZ case numbers to be the average estimated number of cases in group A and B hospitals of the same tier and type with the formula: estimated number of cases in hospitals group A and B of the same tier and type / the number of hospitals A and B of the same tier and type.
Based on interviews of experts, the number of HZ cases in the village clinic was counted as 2 cases per year. For incidence estimates, population denominators were the resident populations reported in the seventh census.
Descriptive statistics were used to describe clinical characteristics of HZ cases from group A hospitals. We used χ² significance tests to compare categorical variables, and binary logistic regression models were used for multivariate analysis. Data analyses were conducted using Excel software (version Home and Student 2019, Microsoft Office, USA) and SAS software (version 9.4, SAS Institute Inc., Cary, NC, USA).
This study was approved by the China CDC Ethical Review Committee (approval number 202123). Individual informed consent was not required or obtained for this study, which was based on electronic medical records.
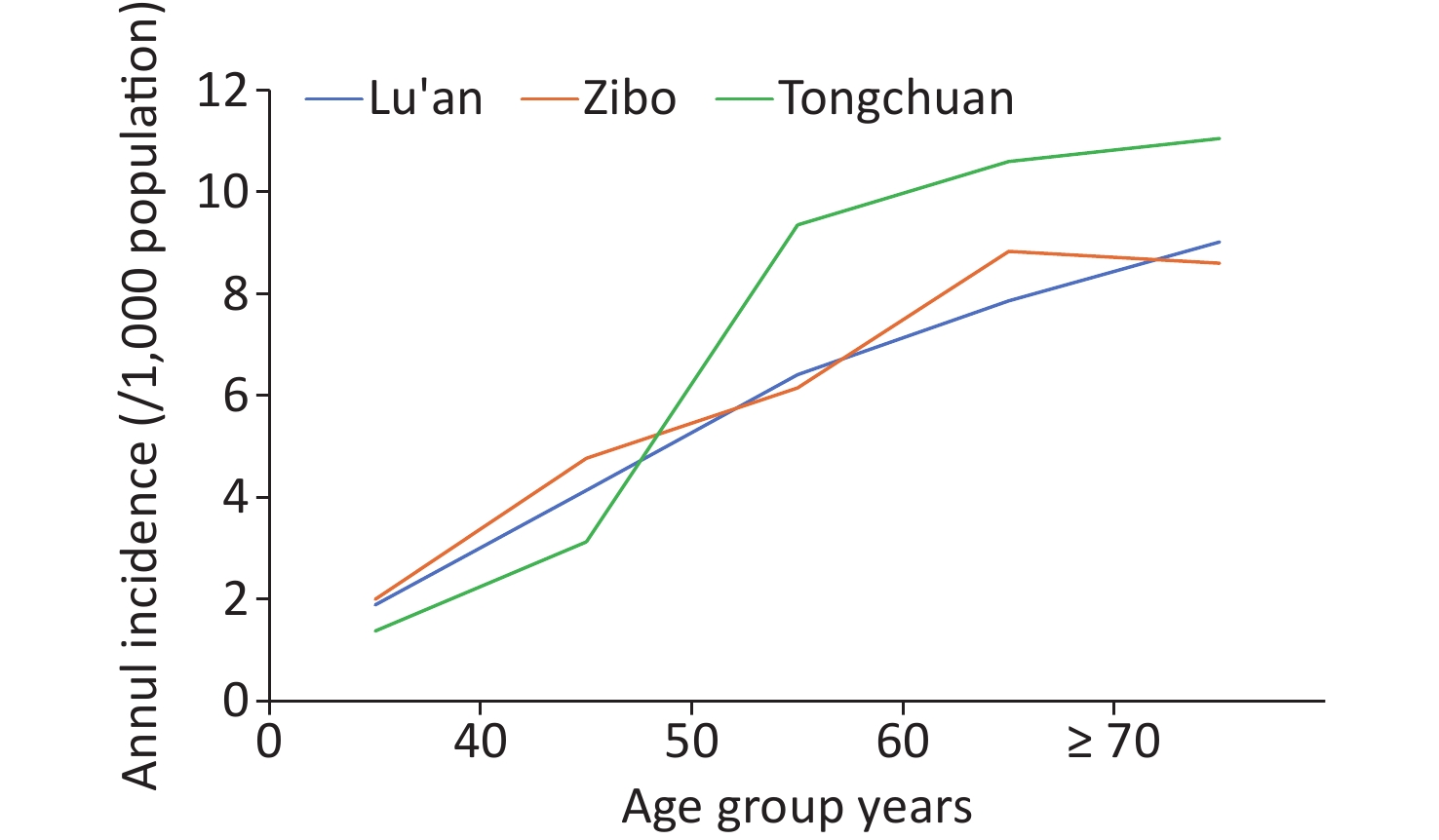
In Lu’an, eight group A hospitals, 17 group B hospitals and 280 group C hospitals were included in the study; In Zibo, 23, 115, 141, respectively, were included. There were nine tier-2 and tier-3 hospitals in Tongchuan, all of which were included as group A hospitals, and Group A also included nine tier-1 hospitals. The remaining 51 tier-1 hospitals were included in group B hospitals. There were no group C hospital in Tongchuan. There were 2,806, 1,785, and 549 village clinics in Lu’an, Zibo, and Tongchuan, respectively. Using hospital system medical records and an incidence estimation method based on hospital type, tier, and data availability, we found that the incidence of herpes zoster in three cities in China was between 4.4 and 4.8 per thousand total population (Table 1). The highest incidence was among the older residents (Figure 1).
Table 1. Estimated incidence (per 1,000 population) of HZ by City
Variables Lu’an Zibo Tongchuan Population 2019 2020 Annul Incidence Population 2019 2020 Annul Incidence Population 2019 2020 Annul Incidence cases Incidence (‰) cases Incidence (‰) cases Incidence (‰) cases Incidence (‰) cases Incidence (‰) cases Incidence (‰) Gender Male 2,257,483 8,965 3.97 9,865 4.37 4.17 2,359,559 10,254 4.35 11,598 4.92 4.63 355,376 1,771 4.16 1769 4.85 4.50 Female 2,136,216 9,793 4.58 10,379 4.86 4.72 2,344,579 10,653 4.54 12,068 5.15 4.85 342,946 1,477 5.16 1723 5.16 5.16 Age group 0– 2,025,518 3,920 1.94 3,746 1.85 1.89 2,038,421 3,973 1.95 4,184 2.05 2.00 315,680 419 1.33 452 1.43 1.38 40– 620,657 2,758 4.44 2,383 3.84 4.14 723,119 3,261 4.51 3,638 5.03 4.77 138,547 448 3.24 420 3.03 3.13 50– 81,487 4,783 5.88 5,645 6.94 6.41 849,441 4,710 5.55 5,736 6.75 6.15 93,016 844 9.08 895 9.62 9.35 60– 468,134 3,668 7.84 3,689 7.88 7.86 604,802 5,173 8.55 5,505 9.10 8.83 86,394 924 10.70 908 10.51 10.60 ≥ 70 465,903 3,628 7.79 4,779 10.26 9.02 488,355 3,790 7.76 4,604 9.43 8.60 64,684 613 9.47 817 12.63 11.05 Total 4,393,699 18,758 4.27 20,244 4.61 4.44 4,704,138 20,907 4.44 23,666 5.03 4.74 698,322 3,248 4.65 3492 5.00 4.83 Note. HZ, Herpes Zoster; Population is the resident populations reported in the seventh census. 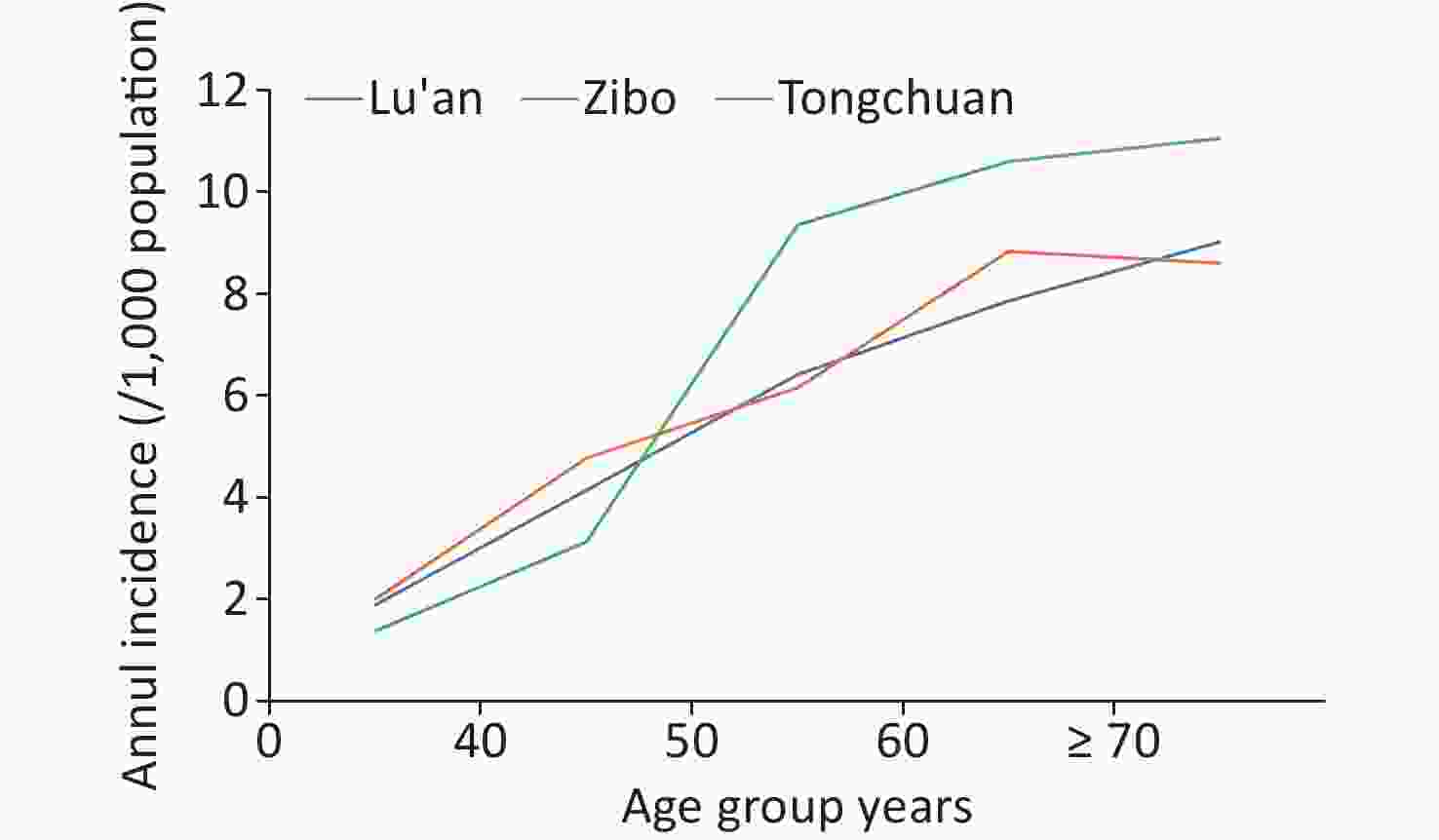
Figure 1. Annual incidence of HZ by city and age group during 2019–2020. HZ, herpes zoster.
We found that the estimated incidence in Tongchuan was slight higher than that in the other two study cities. Because we were able to obtain diagnostic data of all HZ cases from January 2019 to December 2020 in all tier-2 and tier-3 hospitals in Tongchuan, the Tongchuan estimate may be the most accurate of the three estimates. Similar to our incidence estimates, two retrospective studies that used the Big Data Platform for Health Management in Yichang City, Hubei Province during 2016–2017 found an HZ incidence of 5.06 per 1,000 among urban residents. They also found that among > 50-year-olds and > 60-year-olds, incidences were 8 and 10 per 1,000 respectively[6]. A community-based retrospective study in Laiwu district, Jinan city, Shandong Province reported HZ incidence of 14 per 1,000 population among > 60-year-olds in 2018[7]. Differences in study design and data sources likely contributed to differences in the incidence estimates of these domestic studies.
We obtained diagnostic data of 19,196 HZ cases in the 49 group A hospitals (Supplementary Table S4, available in www.besjournal.com). The median (interquartile range, IQR) age was 55 (42, 66) years. 6.66% (1,279) cases had PHN. Among patients ≥ 50 years old, 8.03% had PNH. A retrospective study in 34 districts / counties in Guangdong Province found that 40.2% of the HZ cases among ≥ 50-year-olds had pain for more than one month after the onset of HZ rash[8]. In Yinzhou District (Zhejiang Province), 7.26% of HZ cases among ≥ 50-year-olds had pain more than 90 days after HZ onset[9]. PHN estimates in domestic studies vary significantly by study design, target population, and definition of PHN[9]. It is generally acknowledged that risk of developing PHN increases with age (Supplementary Table S5, available in www.besjournal.com).
Table S4. Characteristics of HZ cases seen in Group A hospitals
Variables Lu’an Zibo Tongchuan Overall Gender Male 3,361 (49.34) 4,493 (48.71) 1,537 (48.64) 9,391 (48.92) Female 3,451 (50.66) 4,731 (51.29) 1,623 (51.36) 9,805 (51.08) Age group 0– 1,521 (22.33) 2,259 (24.49) 502 (15.89) 4,282 (22.31) 40– 937 (13.76) 1,400 (15.18) 440 (13.92) 2,777 (14.47) 50– 1,637 (24.03) 2,012 (21.81) 900 (28.48) 4,549 (23.70) 60– 1,285 (18.86) 2,009 (21.78) 712 (22.53) 4,006 (20.86) ≥ 70 1,432 (21.02) 1,544 (16.74) 606 (19.18) 3,582 (18.66) Complications Yes 2,556 (37.52) 2,385 (25.86) 345 (10.92) 5,286 (27.54) No 4,256 (62.48) 6,839 (74.14) 2,815 (89.08) 13,907 (72.46) PHN Yes 133 (1.95) 833 (9.03) 313 (9.91) 1279 (6.66) No 6,679 (98.05) 8,391 (90.97) 2,847 (90.09) 17,917 (93.34) Hospitalization Yes 618 (9.07) 758 (8.22) 13 (0.41) 1,389 (7.24) No 6,194 (90.93) 8,466 (91.78) 3,147 (99.59) 17,807 (92.76) Grade of hospitals Tier-1 123 (1.81) 990 (10.73) 282 (8.92) 1,395 (7.27) Tier-2 223 (3.27) 4,238 (45.95) 628 (19.87) 5,089 (26.51) Tier-3 6,466 (94.92) 3,996 (43.22) 2,250 (71.21) 12,712 (66.22) Total 6,812 (35.49) 9,224 (48.05) 3,160 (16.46) 19,196 (100.00) Note. Shown as n (%). Table S5. Postherpetic neuralgia in Group A hospital cases
Variables PHN cases Proportion of PHN cases (%) Univariate analysis Binary logistic regression χ2 P OR 95% CI Gender Male 650 6.92 1.98 0.160 Female 629 6.42 Age group 0– 146 3.49 168.09 < 0.001 1.00 40– 158 5.69 1.78 1.41−2.24 50– 273 6.00 1.92 1.56−2.36 60– 344 8.59 2.82 2.31−3.44 ≥ 70 358 9.99 3.35 2.75−4.08 Tier of hospitals Tier-1 21 1.51 75.56 < 0.001 1.00 Tier-2 410 8.06 6.49 4.17−10.11 Tier-3 848 6.67 5.16 3.33−7.98 Note. All tests were 2-sided and P values < 0.05 were considered statistically significant. Our study found around 22% HZ cases were under the age of 40 years, representing a relatively underappreciated burden of disease. Given the profound impact of HZ and its complications on physical and mental well-being and productivity, it is important to consider prioritizing prevention and management of HZ and associated complications in these younger adults. We also found that 52 infants had HZ. However, we did not investigate history of varicella during pregnancy in these 52 mothers, which should be a topic for further study to understand the pathogenic mechanisms underlying such occurrences (Supplementary Table S4). Most likely, these represent reactivation of dormant VZV from intrauterine fetal infections.
A strength of our study is that we developed a method to estimate population incidence of a non-notifiable condition. We categorized all hospitals in the study setting into three groups. Estimates for hospitals without full clinical data were extrapolated from estimates from hospitals with full clinical data based on visit volume and adjusted for level and type of hospital to obtain population-based estimates of incidence. Our study certainly has several limitations. Group A hospitals were not a random sample of hospitals, and the method we used for weighting the estimated the number of cases in hospitals group B and hospitals group C may introduce bias. Second, we did not make estimates of HZ case numbers in personal health clinics and among individuals who did not seek medical attention, and this will lead to underestimating the incidence of mild HZ cases. Thus, our results can only represent medically-attended HZ. However, these cases are most severe and are policy-relevant. The phenomenon of finding only the medically-attended cases is similar to a novel surveillance strategy for bacterial meningitis that was also hospital-based[10]. Third, the three cities we studied were a convenience sample and cannot be considered as representative of all of China. Although the age-based incidence may vary across China, the similarity of our incidence estimates in the three cities provides some reassurance that all-China results would likely be similar to our findings. Future studies could use the methodology we developed to estimate age-based incidences in other areas to assess generalizability of incidence rates.
In conclusion, our study showed that there is a significant burden of medically-attended HZ in China, with an overall incidence of about 4.5 cases per 1,000 total population. Elderly people are at greatest risk of HZ and PHN. Our study provide a methodology to estimate population incidence of non-notifiable conditions.
-
Table S1. Group A hospital proportions of HZ cases to all patient visits during 2019 to 2020 at the same tier and type of hospital in Lu’an
Group A hospitals 2019 2020 Visit volume Cases Weights Visit volume Cases Weights Community Health Center 49,303 99 0.002008 87,576 110 0.001256 Township Health Centers 61,582 113 0.001835 57,437 120 0.002089 Tier-2 general hospitals 221,958 171 0.000770 206,848 191 0.000923 Tier-3 general hospitals 2,441,415 3214 0.001316 2,495,374 3,258 0.001306 Maternal and child health care hospital 399,142 93 0.000223 349,359 109 0.000312 Traditional Chinese medicine hospital 59,854 119 0.001988 6,2501 139 0.002224 Note. Weights is weighting factor; for the Group A hospital proportion of HZ cases to all patient visits during the same study year and at the same tier and type of hospital. Table S2. Group A hospital proportions of HZ cases to all patient visits during 2019 to 2020 at the same tier and type of hospital in Zibo
Group A hospitals 2019 2020 Visit volume Cases Weights Visit volume Cases Weights Community health center 7611 23 0.003022 18,033 52 0.002884 Township health centers 63,564 42 0.000661 69,503 47 0.000676 Tier-2 general hospitals 373,756 258 0.000690 288,900 240 0.000831 Tier-3 general hospitals 3,838,054 2345 0.000611 4,428,006 3,206 0.000724 Maternal and child health care hospital 74,145 13 0.000175 406,175 110 0.000271 Traditional Chinese medicine hospital 766,273 291 0.000380 623,130 363 0.000583 Note. Weights is weighting factor; for the Group A hospital proportion of HZ cases to all patient visits during the same study year and at the same tier and type of hospital. Table S3. Group A hospital proportions of HZ cases to all patient visits during 2019 to 2020 at the same type of hospital in Tongchuan
Month Group A community health center Group A township health centers 2019 2020 2019 2020 Visit volume Cases Weights Visit volume Cases Weights Visit volume Cases Weights Visit volume Cases Weights 1 3,519 21 0.005968 1,600 3 0.001875 1,595 5 0.003135 1,470 3 0.002041 2 2,106 17 0.008072 955 7 0.007330 1,570 3 0.001911 1,494 3 0.002008 3 3,175 18 0.005669 1,006 8 0.007952 2,753 3 0.001090 1,674 3 0.001792 4 2,981 18 0.006038 1,269 21 0.016548 2,535 4 0.001578 1,884 3 0.001592 5 3,366 24 0.007130 1,667 26 0.015597 2,254 3 0.001331 1,965 3 0.001527 6 3,689 20 0.005422 1,946 18 0.009250 2,247 3 0.001335 1,977 3 0.001517 7 3,503 21 0.005995 1,898 21 0.011064 2,416 5 0.002070 2,353 2 0.000850 8 3,586 20 0.005577 2,104 22 0.010456 2,139 3 0.001403 2,015 5 0.002481 9 2,525 21 0.008317 2,344 17 0.007253 1,975 4 0.002025 2,058 4 0.001944 10 2,942 18 0.006118 2,091 24 0.011478 2,199 3 0.001364 2,065 3 0.001453 11 3,042 21 0.006903 2,316 22 0.009499 3,024 3 0.000992 2,783 2 0.000719 12 3,123 19 0.006084 2,157 29 0.013445 3,457 3 0.000868 2,939 2 0.000681 Note. Weights is weighting factor; for the Group A hospital proportion of HZ cases to all patient visits during the same study month and at the same type of hospital.
doi: 10.3967/bes2024.115
-
-
Figure 1. Annual incidence of HZ by city and age group during 2019–2020. HZ, herpes zoster.
Table 1. Estimated incidence (per 1,000 population) of HZ by City
Variables Lu’an Zibo Tongchuan Population 2019 2020 Annul Incidence Population 2019 2020 Annul Incidence Population 2019 2020 Annul Incidence cases Incidence (‰) cases Incidence (‰) cases Incidence (‰) cases Incidence (‰) cases Incidence (‰) cases Incidence (‰) Gender Male 2,257,483 8,965 3.97 9,865 4.37 4.17 2,359,559 10,254 4.35 11,598 4.92 4.63 355,376 1,771 4.16 1769 4.85 4.50 Female 2,136,216 9,793 4.58 10,379 4.86 4.72 2,344,579 10,653 4.54 12,068 5.15 4.85 342,946 1,477 5.16 1723 5.16 5.16 Age group 0– 2,025,518 3,920 1.94 3,746 1.85 1.89 2,038,421 3,973 1.95 4,184 2.05 2.00 315,680 419 1.33 452 1.43 1.38 40– 620,657 2,758 4.44 2,383 3.84 4.14 723,119 3,261 4.51 3,638 5.03 4.77 138,547 448 3.24 420 3.03 3.13 50– 81,487 4,783 5.88 5,645 6.94 6.41 849,441 4,710 5.55 5,736 6.75 6.15 93,016 844 9.08 895 9.62 9.35 60– 468,134 3,668 7.84 3,689 7.88 7.86 604,802 5,173 8.55 5,505 9.10 8.83 86,394 924 10.70 908 10.51 10.60 ≥ 70 465,903 3,628 7.79 4,779 10.26 9.02 488,355 3,790 7.76 4,604 9.43 8.60 64,684 613 9.47 817 12.63 11.05 Total 4,393,699 18,758 4.27 20,244 4.61 4.44 4,704,138 20,907 4.44 23,666 5.03 4.74 698,322 3,248 4.65 3492 5.00 4.83 Note. HZ, Herpes Zoster; Population is the resident populations reported in the seventh census.  下载: 导出CSV
下载: 导出CSV
S4. Characteristics of HZ cases seen in Group A hospitals
Variables Lu’an Zibo Tongchuan Overall Gender Male 3,361 (49.34) 4,493 (48.71) 1,537 (48.64) 9,391 (48.92) Female 3,451 (50.66) 4,731 (51.29) 1,623 (51.36) 9,805 (51.08) Age group 0– 1,521 (22.33) 2,259 (24.49) 502 (15.89) 4,282 (22.31) 40– 937 (13.76) 1,400 (15.18) 440 (13.92) 2,777 (14.47) 50– 1,637 (24.03) 2,012 (21.81) 900 (28.48) 4,549 (23.70) 60– 1,285 (18.86) 2,009 (21.78) 712 (22.53) 4,006 (20.86) ≥ 70 1,432 (21.02) 1,544 (16.74) 606 (19.18) 3,582 (18.66) Complications Yes 2,556 (37.52) 2,385 (25.86) 345 (10.92) 5,286 (27.54) No 4,256 (62.48) 6,839 (74.14) 2,815 (89.08) 13,907 (72.46) PHN Yes 133 (1.95) 833 (9.03) 313 (9.91) 1279 (6.66) No 6,679 (98.05) 8,391 (90.97) 2,847 (90.09) 17,917 (93.34) Hospitalization Yes 618 (9.07) 758 (8.22) 13 (0.41) 1,389 (7.24) No 6,194 (90.93) 8,466 (91.78) 3,147 (99.59) 17,807 (92.76) Grade of hospitals Tier-1 123 (1.81) 990 (10.73) 282 (8.92) 1,395 (7.27) Tier-2 223 (3.27) 4,238 (45.95) 628 (19.87) 5,089 (26.51) Tier-3 6,466 (94.92) 3,996 (43.22) 2,250 (71.21) 12,712 (66.22) Total 6,812 (35.49) 9,224 (48.05) 3,160 (16.46) 19,196 (100.00) Note. Shown as n (%).
下载: 导出CSV
S5. Postherpetic neuralgia in Group A hospital cases
Variables PHN cases Proportion of PHN cases (%) Univariate analysis Binary logistic regression χ2 P OR 95% CI Gender Male 650 6.92 1.98 0.160 Female 629 6.42 Age group 0– 146 3.49 168.09 < 0.001 1.00 40– 158 5.69 1.78 1.41−2.24 50– 273 6.00 1.92 1.56−2.36 60– 344 8.59 2.82 2.31−3.44 ≥ 70 358 9.99 3.35 2.75−4.08 Tier of hospitals Tier-1 21 1.51 75.56 < 0.001 1.00 Tier-2 410 8.06 6.49 4.17−10.11 Tier-3 848 6.67 5.16 3.33−7.98 Note. All tests were 2-sided and P values < 0.05 were considered statistically significant.
下载: 导出CSV
S1. Group A hospital proportions of HZ cases to all patient visits during 2019 to 2020 at the same tier and type of hospital in Lu’an
Group A hospitals 2019 2020 Visit volume Cases Weights Visit volume Cases Weights Community Health Center 49,303 99 0.002008 87,576 110 0.001256 Township Health Centers 61,582 113 0.001835 57,437 120 0.002089 Tier-2 general hospitals 221,958 171 0.000770 206,848 191 0.000923 Tier-3 general hospitals 2,441,415 3214 0.001316 2,495,374 3,258 0.001306 Maternal and child health care hospital 399,142 93 0.000223 349,359 109 0.000312 Traditional Chinese medicine hospital 59,854 119 0.001988 6,2501 139 0.002224 Note. Weights is weighting factor; for the Group A hospital proportion of HZ cases to all patient visits during the same study year and at the same tier and type of hospital.
下载: 导出CSV
S2. Group A hospital proportions of HZ cases to all patient visits during 2019 to 2020 at the same tier and type of hospital in Zibo
Group A hospitals 2019 2020 Visit volume Cases Weights Visit volume Cases Weights Community health center 7611 23 0.003022 18,033 52 0.002884 Township health centers 63,564 42 0.000661 69,503 47 0.000676 Tier-2 general hospitals 373,756 258 0.000690 288,900 240 0.000831 Tier-3 general hospitals 3,838,054 2345 0.000611 4,428,006 3,206 0.000724 Maternal and child health care hospital 74,145 13 0.000175 406,175 110 0.000271 Traditional Chinese medicine hospital 766,273 291 0.000380 623,130 363 0.000583 Note. Weights is weighting factor; for the Group A hospital proportion of HZ cases to all patient visits during the same study year and at the same tier and type of hospital.
下载: 导出CSV
S3. Group A hospital proportions of HZ cases to all patient visits during 2019 to 2020 at the same type of hospital in Tongchuan
Month Group A community health center Group A township health centers 2019 2020 2019 2020 Visit volume Cases Weights Visit volume Cases Weights Visit volume Cases Weights Visit volume Cases Weights 1 3,519 21 0.005968 1,600 3 0.001875 1,595 5 0.003135 1,470 3 0.002041 2 2,106 17 0.008072 955 7 0.007330 1,570 3 0.001911 1,494 3 0.002008 3 3,175 18 0.005669 1,006 8 0.007952 2,753 3 0.001090 1,674 3 0.001792 4 2,981 18 0.006038 1,269 21 0.016548 2,535 4 0.001578 1,884 3 0.001592 5 3,366 24 0.007130 1,667 26 0.015597 2,254 3 0.001331 1,965 3 0.001527 6 3,689 20 0.005422 1,946 18 0.009250 2,247 3 0.001335 1,977 3 0.001517 7 3,503 21 0.005995 1,898 21 0.011064 2,416 5 0.002070 2,353 2 0.000850 8 3,586 20 0.005577 2,104 22 0.010456 2,139 3 0.001403 2,015 5 0.002481 9 2,525 21 0.008317 2,344 17 0.007253 1,975 4 0.002025 2,058 4 0.001944 10 2,942 18 0.006118 2,091 24 0.011478 2,199 3 0.001364 2,065 3 0.001453 11 3,042 21 0.006903 2,316 22 0.009499 3,024 3 0.000992 2,783 2 0.000719 12 3,123 19 0.006084 2,157 29 0.013445 3,457 3 0.000868 2,939 2 0.000681 Note. Weights is weighting factor; for the Group A hospital proportion of HZ cases to all patient visits during the same study month and at the same type of hospital.
下载: 导出CSV
-
[1] Min XY, Xu ST, Xu WB. Advance in epidemiological researches and related vaccines of herpes zoster. Chin J Virol, 2020; 36, 109−14. (In Chinese) [2] Gater A, Abetz-Webb L, Carroll S, et al. Burden of herpes zoster in the UK: findings from the zoster quality of life (ZQOL) study. BMC Infect Dis, 2014; 14, 402. doi: 10.1186/1471-2334-14-402 [3] Kawai K, Gebremeskel BG, Acosta CJ. Systematic review of incidence and complications of herpes zoster: towards a global perspective. BMJ Open, 2014; 4, e004833. doi: 10.1136/bmjopen-2014-004833 [4] Zhou H, Wang SQ, Chu Y, et al. Survey of seroprevalence of varicella zoster virus in healthy population in Shanghai. Chin J Vaccines Immun, 2006; 12, 137−9. (In Chinese) [5] Suo LD, Zhao D, Chen M, et al. An investigation on serum antibody level of varicella-zoster virus in healthy population in Beijing. Chin J Vaccines Immun, 2022; 56, 108−13. (In Chinese) [6] Jiang W, Li GW, Xu Y, et al. Epidemiological characteristics of herpes zoster in urban areas of Yichang city during 2016-2017 based on the Yichang Big Data Platform for Health Management. Chin J Vaccines Immun, 2019; 25, 432−5. (In Chinese) [7] Zhang WY, Liu SN, Sun HY, et al. Study of incidence and economic burden of herpes zoster based on community investigation among the aged in Laiwu district, Jinan city, Shandong Province of China. Chin J Prev Med, 2022; 56, 119−24. (In Chinese) [8] Zhu Q, Zheng HZ, Qu HY, et al. Epidemiology of herpes zoster among adults aged 50 and above in Guangdong, China. Hum Vaccin Immunother, 2015; 11, 2113−8. doi: 10.1080/21645515.2015.1016672 [9] Sun XH, Wei Z, Lin HB, et al. Incidence and disease burden of herpes zoster in the population aged ≥ 50 years in China: data from an integrated health care network. J Infect, 2021; 82, 253−60. [10] Li YX, Yin ZD, Shao ZJ, et al. Population-based surveillance for bacterial meningitis in China, September 2006-December 2009. Emerg Infect Dis, 2014; 20, 61−9. -
 24213+Supplementary Materials.pdf
24213+Supplementary Materials.pdf

-

 点击查看大图
点击查看大图
计量
- 文章访问数: 331
- HTML全文浏览量: 145
- PDF下载量: 34
- 被引次数: 0

 Quick Links
Quick Links