

 下载:
下载:


-
With medical reform in China expanding, both public and private hospitals have undergone significant changes. Health resources and profitability have increased substantially in public hospitals, whereas private hospitals have entered a period of development dividends. Data from the China Health Yearbook show that the number of public hospitals was 13,850 in 2010 and 11,930 in 2019, with an average growth rate of −1.6%. The average revenue growth rate of public hospitals was 13.7%. In contrast, that of private hospitals was 22.7%. However, previous studies have presented different understandings of the stages of development in China’s medical service market.
The degree of competition between public and private hospitals in China remains controversial. Private hospitals in China have undergone more than a decade of development. However, the mainstream view holds that public hospitals have an absolute advantage in the medical market, both in terms of medical resources and technical healthcare personnel, and that private hospitals cannot compete with public hospitals[1]. Public hospitals can profit from drugs through their administrative monopoly, driving up medical expenses[2]. However, to some extent, private hospitals have challenged the absolute monopoly held by public hospitals. First, as the scale of public hospitals has shrunk, the number of private hospitals and patient visits has increased rapidly[3,4]. Second, the clear property rights of private hospitals contribute to their pricing and medical quality advantages. Some researchers believe that the relationship between public and private hospitals is competitive.
The extent of cooperation between public and private hospitals is also controversial. Due to the fragmentation and disconnection of the medical market, providing unified and coordinated medical services to patients is difficult. Some researchers believe that strong competition and poor cooperation among medical institutions have led to an increase in medical expenses and waste of medical resources[5], with suggestions being made to establish integrated medical systems and alliances. The academic community has also begun to focus on observing the cooperation between public and private hospitals[6]. However, research suggests that, due to conflicting interests between medical institutions and flaws in supporting medical insurance policies, the degree of cooperation between medical institutions is low. Furthermore, interest in collaborative decision-making between public and private hospitals is insufficient, making it difficult to improve cooperation between the two[7].
The degree of market competition is usually measured using the Herfindahl–Hirschman Index (HHI), with the formula $\text{HHI} =\sum {{S}_{i}}^{2} $, where $ {S}_{i} $ represents the market share of the i-th institution. Different studies have used different proxy variables for hospital market share, mainly reflecting differences in the number and categories of institutions. The range of HHI values is also influenced by this factor, leading to variations in HHI value ranges across different studies.
The concept of symbiosis, which originally emerged in biology and later expanded to many social fields, refers to the cooperative evolution of two symbiotic units through mutual stimulation rather than mutual exclusion. Currently, symbiotic models are not commonly used in the field of medical services. Both theoretical analyses and model deduction have mainly been used to discuss the prerequisites and development paths of hospital cooperation in China[7]. Since medical reforms were implemented in China, the relationship between private and public hospitals has changed significantly, gradually encouraging both competition and cooperation. Therefore, examining the current status of the medical market in China by measuring the symbiosis between public and private hospitals is feasible.
Data on outpatient visits, inpatient admissions, and provision of surgical services in public and private hospitals in 31 provinces (including autonomous regions and municipalities directly under the central government) of China were sourced from the China Health Yearbook for the years 2011–2016 and 2017–2020. To control for the impact of the coronavirus disease 2019 outbreak on the medical services market, data from 2020 to 2021 were excluded from the analyses. Excel 2019 (Microsoft Corporation, https://office.microsoft.com/excel) and Stata 16.0 (Stata Corp. LLC, College Station, Texas, USA) were used for indicator calculations and model construction. ArcGIS 10.2 (Environmental Systems Research Institute, Inc. (Esri), Redlands, California, USA) was used to visualize the cooperation and competition status between public and private hospitals in the outpatient, inpatient, and surgical service areas (Figure 1), while PyCharm 2022 (JetBrains s.r.o., Prague, Czech Republic)was used to visualize the same information via quadrant diagrams (Figure 2).
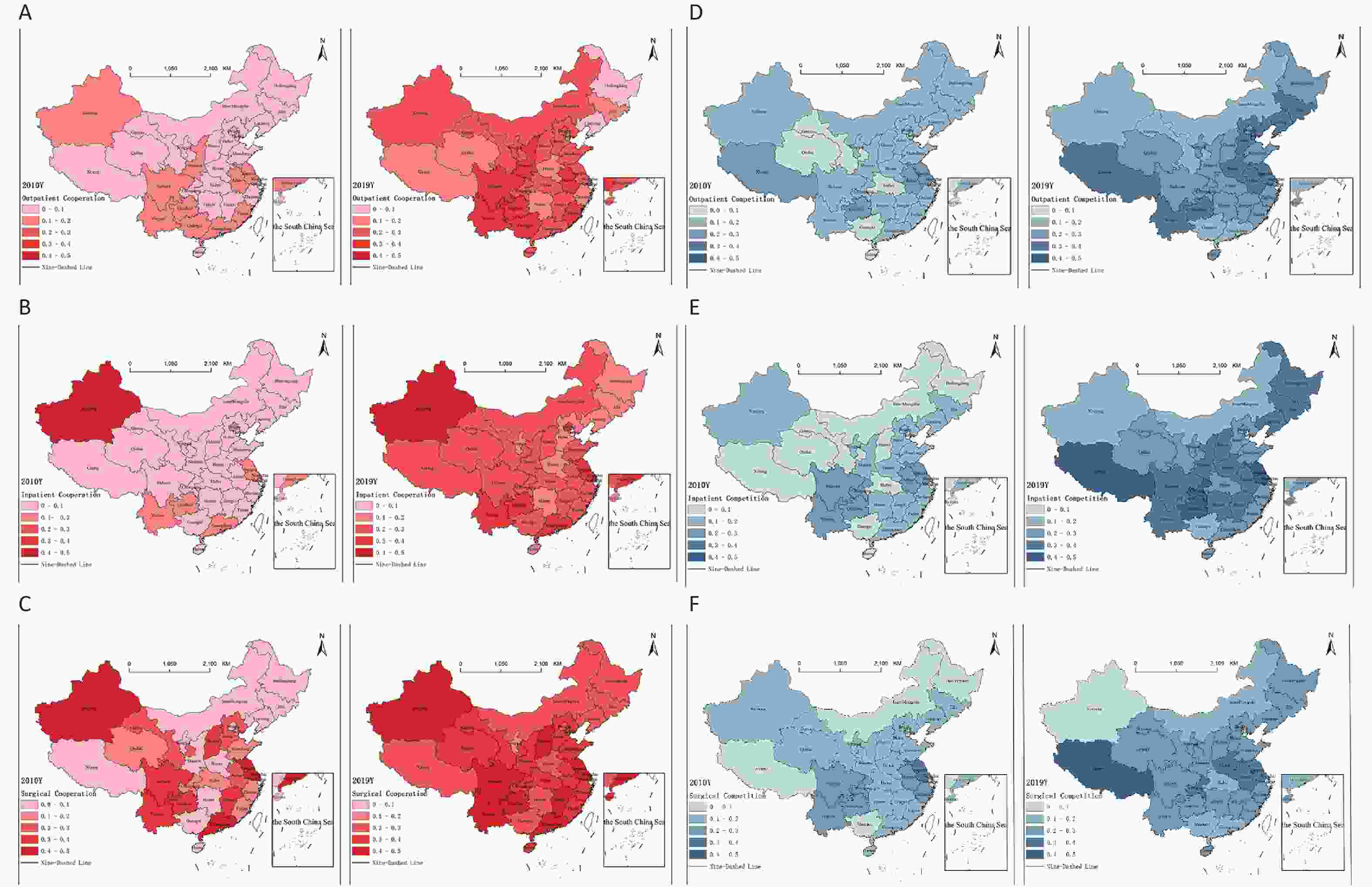
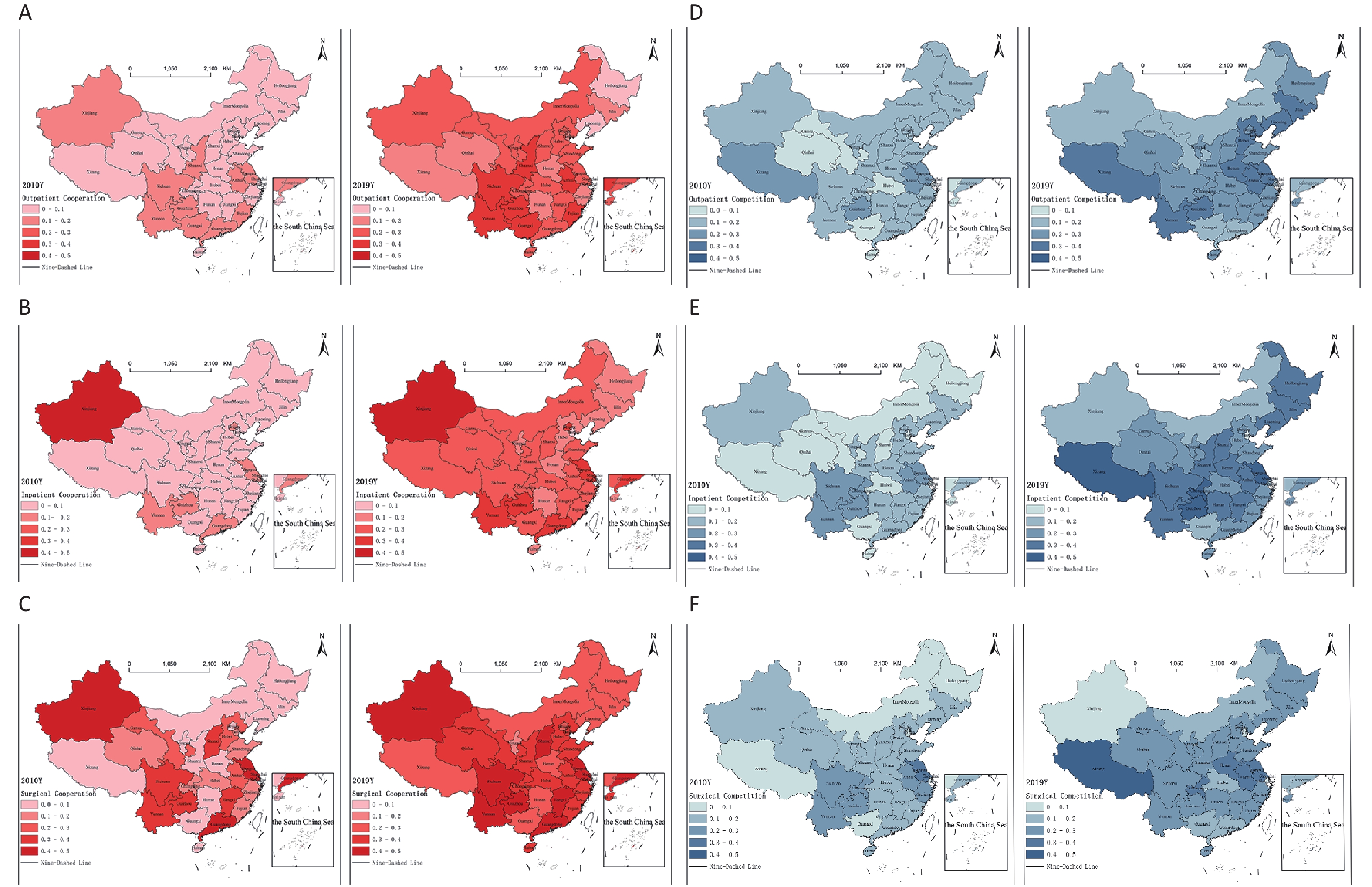
Figure 1. Cooperation and competition between public and private hospitals in various provinces and cities in 2010 and 2019. (A) The degree of cooperation in outpatient services. (B) The degree of cooperation in inpatient services. The linear model fit for inpatient cooperation in Tianjin may have had a lower degree of accuracy, potentially indicating bias. (C) The degree of cooperation in surgical services. (D) The competitiveness in outpatient services. (E) The competitiveness in inpatient services. (F) The competitiveness in surgical services. GS (2020) 4618.
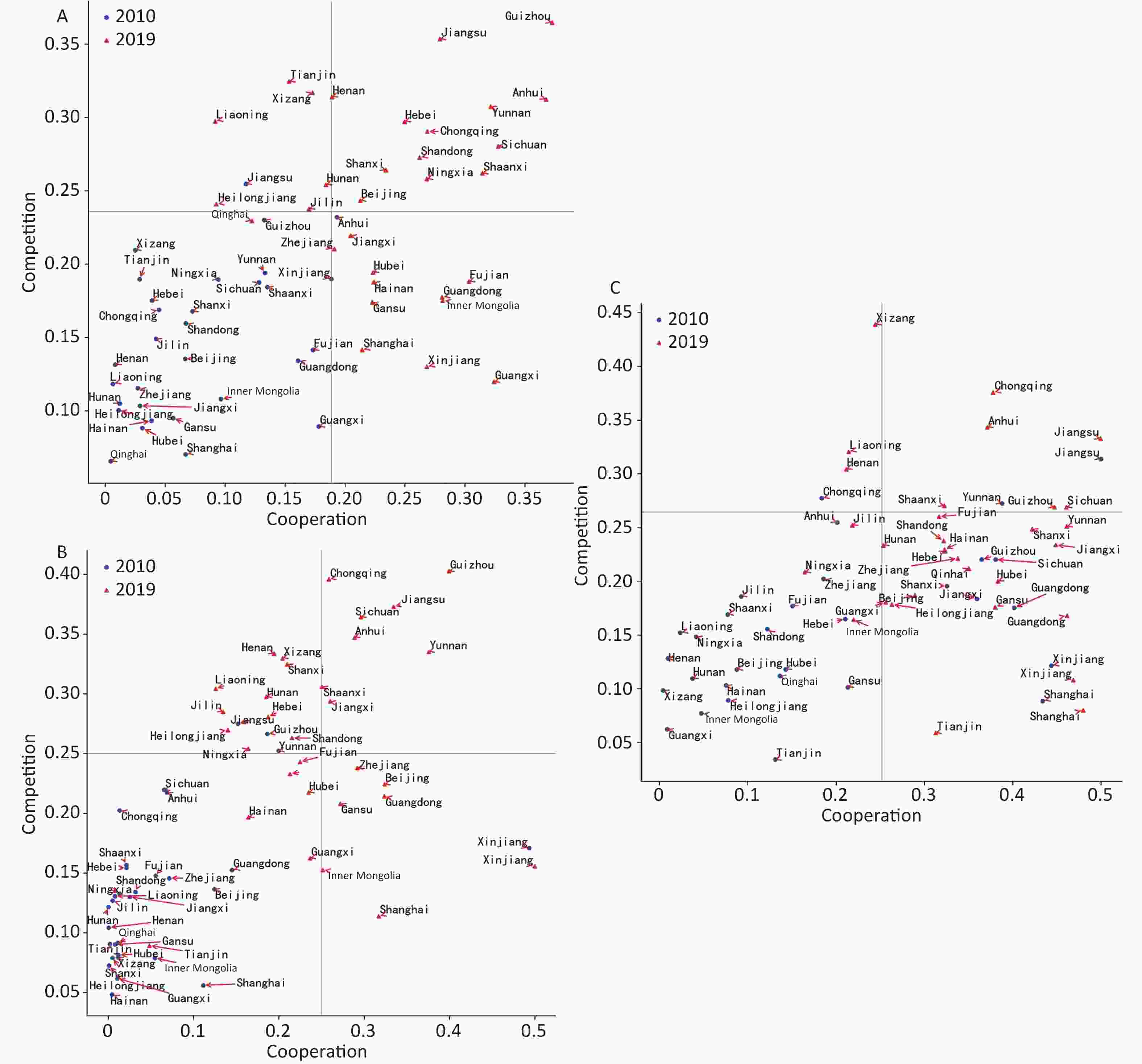
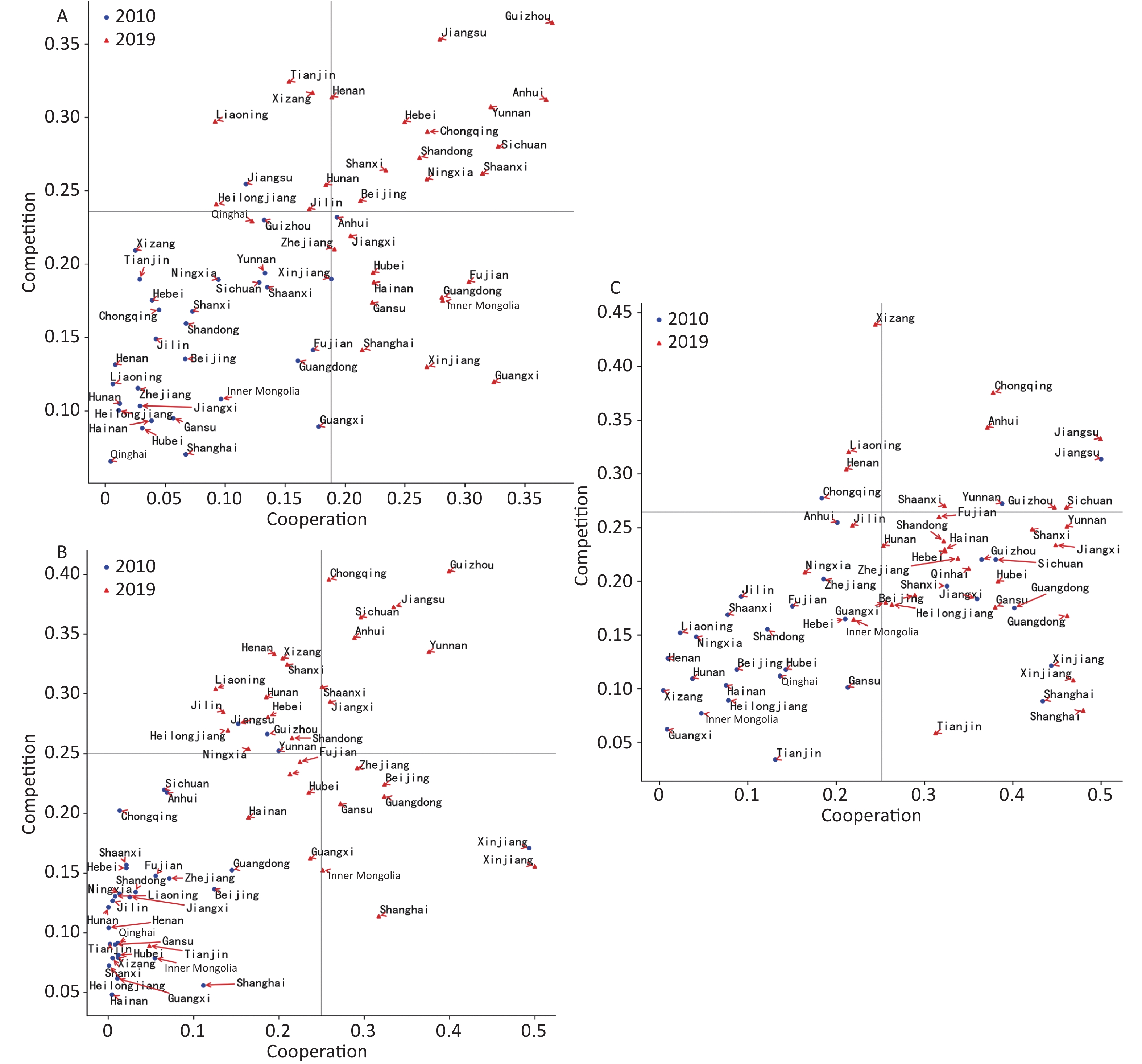
Figure 2. The competition and cooperation between public and private hospitals in various provinces in 2010 and 2019. (A) Outpatient services. (B) Hospitalization services. The linear model fit for the degree of cooperation for hospitalization in Tianjin was relatively low, indicating potential bias. (C) Surgical services. ● represents provincial data for the year 2010; ▲ represents provincial data for the year 2019.
We used the degree of symbiosis to represent the level of cooperation between public and private hospitals in the outpatient, inpatient, and surgical service domains. Cooperative symbiosis refers to the mutually beneficial cooperation achieved between two types of organizations by sharing resources and collaborating. Symbiosis may entail broader and longer-term interactive relationships, whereas cooperation may be temporary, serving as a means to enhance and realize symbiosis[8]. Competition refers to the process by which different individuals or groups in the same market engage in a series of competitive actions to vie for victory or gain more benefits, such as market share, customers, profits, and resources. The calculations for symbiosis and competitive intensity can be found in
Appendices A and B (available in www.besjournal.com).In 1996, Brandenburger and Nalebuff introduced the concept of coopetition into the field of strategic management and established the term. They believed that organizations could achieve a win-win, non-zero-sum game where competition is necessary but does not preclude cooperation. These two researchers argued that competition and cooperation can coexist, with organizations having the option to choose cooperation alongside competition[9].
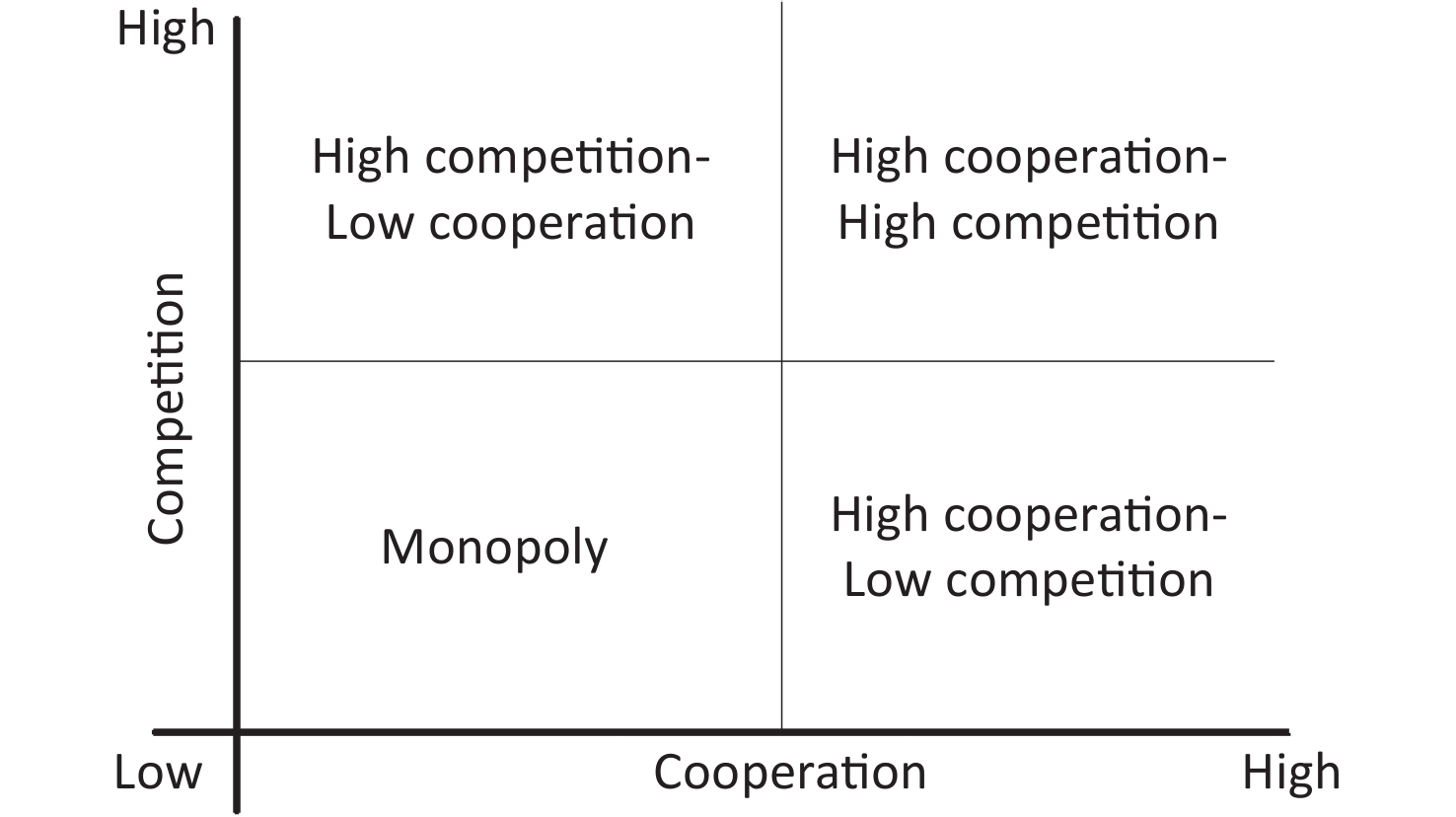
Building on previous research, we constructed a theoretical model of the relationship between public and private hospitals, as shown in Figure 3[10]. Based on the degree of competitive intensity and cooperation, we divided the competitive cooperative relationship into four quadrants: monopoly, high competition-low cooperation, high cooperation-low competition, and high competition-high cooperation.
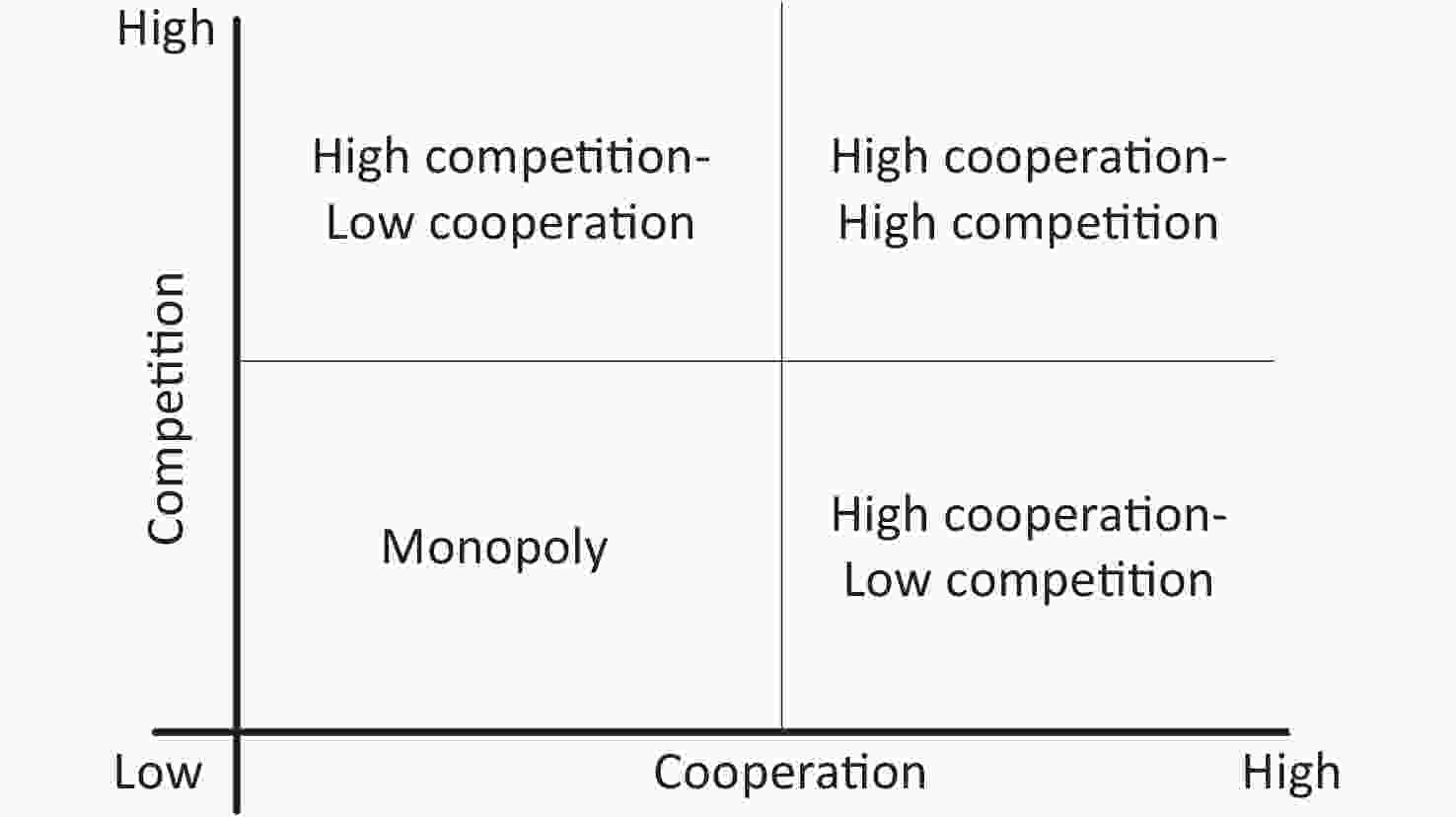
Figure 3. Theoretical model of relationship patterns between public and private hospitals from the perspective of coopetition theory. The four modes in the healthcare service market are as follows. Monopoly: The first scenario is referred to as the monopoly mode. Market monopolies in healthcare services may lead to issues such as inefficient service delivery. High competition-low cooperation: The second scenario is characterized by high competition and low cooperation. This manifests as intense competition among medical institutions, with a lack of cooperation, potentially resulting in the wastage of medical resources due to competitive rivalry. High cooperation-low competition: The third scenario refers to a mode of high cooperation and low competition, where competition among market players is minimal, but the division of labor and cooperation among medical institutions is significant, leading to close ties and collaboration. High competition-high cooperation: In the fourth scenario, the degree of both competition and cooperation among medical institutions is high. Hospitals engage in intense competition, while maintaining close collaborative relationships and exchanges.
From Figures 1 and 2, we can conclude as follows. (1) Outpatient and inpatient services between public and private hospitals have transitioned from partial cooperation to reciprocal cooperation, and the reciprocal cooperation model of surgical services has been further developed. (2) The degree of competition between public and private hospitals for outpatient services has increased, but the competition for inpatient and surgical services has developed unevenly. (3) Outpatient and inpatient services between public and private hospitals changed from a monopoly mode to a high competition-high cooperation mode, and surgical services changed from a monopoly mode to a high cooperation-low competition mode. (4) There are clear regional variations in the relationship model between public and private hospitals. There is a lower degree of competition but a higher degree of cooperation in eastern provinces such as Beijing, Shanghai, and Guangzhou. There is a higher degree of competition and cooperation in western provinces such as Yunnan, Guizhou, and Sichuan.
Due to systemic flaws and low profitability, public and private hospitals lacked the incentive to cooperate, making cooperation difficult to achieve[3]. In our study, we found that from 2010 to 2019, the increase in cooperation between public and private hospitals was more significant than that in competition, indicating that cooperation had become a mainstream trend. However, differences in the level of economic development and geographical location among provinces resulted in significant variations in the evolutionary trends of the relationship patterns between public and private medical institutions.
In the eastern regions of China, the trend was toward high cooperation and low competition, whereas in the western regions, it was toward high cooperation and high competition. We found that from 2010 to 2019, in eastern regions such as Beijing, Shanghai, and Guangzhou, the degree of competition and cooperation between public and private hospitals for outpatient services increased but remained monopolistic. The increase in competition intensity for inpatient and surgical services was relatively slow, whereas the increase in cooperation was rapid, indicating a transition towards high cooperation and low competition. In 2019, western provinces such as Yunnan, Sichuan, and Guizhou had already entered a stage of high competition and high cooperation in outpatient, inpatient, and surgical services.
From 2010 to 2019, the degree of competition and cooperation between public and private hospitals in most provinces and cities in China showed an increasing trend, driven significantly by policy promotion. Numerous local documents consistently proposed providing various preferential policies to foster a social environment conducive to the development of private medical institutions. Preferential policies included relaxing access conditions to the medical market, effectively guaranteeing private medical institutions’ demand for property, implementing various tax reduction policies and fiscal subsidies, and supporting social capital to participate in the reform and restructuring of public hospitals.
Unequal resource allocation is an important factor that causes varying changes in the competition intensity between public and private hospitals. Accessibility and Healthcare Access and Quality Index values in the eastern region are much higher than those in the central and western regions[11]. In our study, we found that the growth in competition intensity between public and private hospitals in the eastern provinces has been slow, mainly because private hospitals find it challenging to compete with the strong public medical system. In contrast, in the central and western provinces, the limitations of the public medical system create development opportunities for private hospitals, leading to a faster increase in competition intensity compared to the eastern regions. Additionally, interest-driven factors play a crucial role in driving changes in cooperation between public and private hospitals. Measures such as talent training, technical guidance, and equipment sharing reduce the operating costs of medical institutions and improve the efficiency of medical resource utilization. Moreover, the circulation of referred patient resources and the interoperability of medical record data increase the number of patients for both parties, generating additional income and complementing resources.
The medical insurance system is an important factor that influences the competition and cooperation between public and private hospitals. In the United Kingdom, internal reform transformed the relationship of responsibility between medical management organizations and medical institutions into contractual relationships, requiring medical institutions to compete for medical insurance contracts. Medical insurance reform in the Netherlands, while promoting market competition, also encouraged the merger and integration of medical service institutions, providing patients with continuous and comprehensive medical services. China’s medical insurance system is undergoing significant changes that will impact the competition and cooperation relationships between public and private hospitals. Given the joint influence of various factors, the relationship between public and private hospitals may undergo new changes.
全文HTML
 24200+.pdf
24200+.pdf
|

|

 Quick Links
Quick Links