

-
Chronic obstructive pulmonary disease (COPD), which is characterized by a long-term, irreversible airway limitation and persistent respiratory symptoms, is common and preventable. Several studies have suggested that particulate matter is associated with the prevalence of COPD and the risk of mortality. At the same time, the diurnal temperature range (DTR) has been suggested to be an adverse health factor that is especially associated with an increased risk of hospitalization in patients with COPD[1]. DTR represents temperature variability within 1 day and is considered an important indicator of climate change. A few studies have shown that ambient air pollutants [particulate matter (PM)], such as PM2.5 and PM10, and high or low temperature have a synergistic effect on COPD[1]. Thus, the current study determined the interaction between particulate matter (PM) and the DTR on COPD mortality and identified the vulnerable population in Weifang.
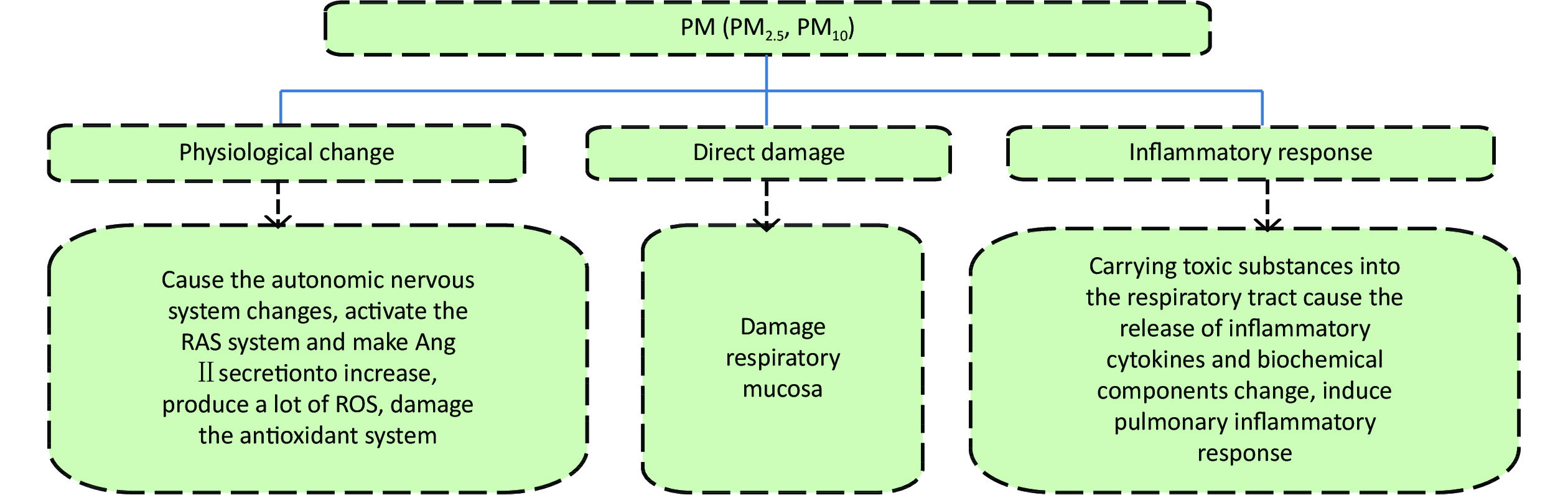
Vulnerability to DTR can be attributed to the following: (1) the DTR increases oxygen uptake, which affects antioxidant activity[2]; (2) sudden temperature changes lead to pathophysiologic responses of respiratory epithelium at the tissue level, which increases respiratory-related mortality or morbidity[3]; and (3) sudden changes in temperature are associated with the release of inflammatory mediators by mast cells, which leads to an increased inflammatory response[3,4]. We suggest that the effect of PM pathways on the body is similar for DTR (Supplementary Figure S1, available in www.besjournal.com). Therefore, our research group speculated that extreme DTR may have a reciprocal action on the body with PM in these pathways, resulting in an increased prevalence of COPD.
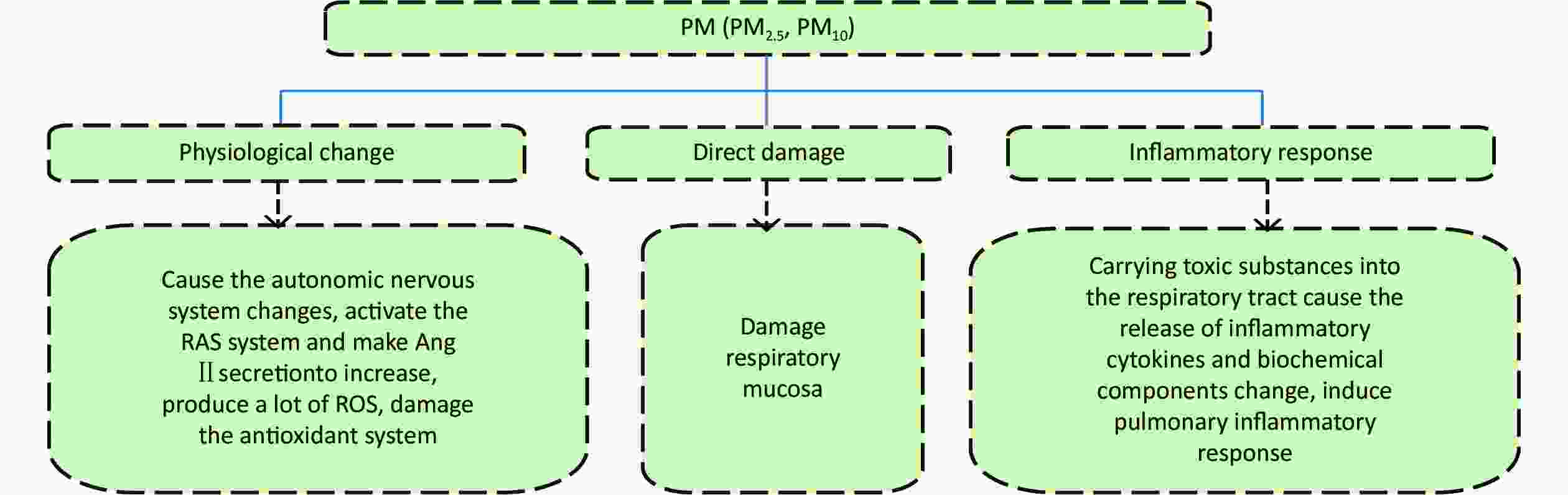
Figure S1. The Influencing Mechanism of PM on COPD. RAS, Renin-angiotensin system; Ang II, Angiotensin II; ROS, Reactive oxygen species.
Daily COPD-related death data from 1 January 2016 to 31 December 2018 were obtained from the Weifang Center for Disease Control and Prevention according to the 10th edition of the International Classification of Diseases (ICD-10). Age, gender, and education were stratified into different categories to identify potentially vulnerable groups. Cases were grouped into three age categories, as follows: young age group (< 39 years); middle age group (39–69 years); and older age group (≥ 70 years). Cases were grouped into two education levels (primary, and secondary and above levels), which are defined as lower and higher education groups, respectively. The Weifang Environmental Monitoring Center provided daily data of air pollutants for particulate matter (PM2.5 and PM10 in μg/m3), ozone (O3 in mg/m3), nitrogen dioxide (NO2 in mg/m3), sulfur dioxide (SO2 in mg/m3), and carbon monoxide (CO in mg/m3) from 10 local air pollution monitoring stations. The daily 24-h average concentration of these air pollutants was obtained by averaging the data from the 10 stations utilized in this study. The 24-h average concentration of PM2.5 was 58.2 μg/m3 (minimum, 5.6 μg/m3; maximum 340.4 μg/m3) and PM10 was 115.1 μg/m3 (minimum, 14.6 μg/m3; maximum, 448.8 μg/m3), both of which exceeded the secondary standards of ambient air quality standard GB 3095-2012. Based on the meteorologic data from 2016−2018 in Weifang city (
http://data.cma.cn ), including the daily mean temperature (Tmean in ℃), daily maximum temperature (Tmax in ℃), daily minimum temperature (Tmin in ℃), daily rainfall in mm, daily mean relative humidity (Rh as a %), daily mean atmospheric pressure (Pmean in hPa), and daily mean wind speed (Wsmean in m/s). The Rh in Weifang was 61.6% (minimum, 18.3%; maximum, 95.0%), the pressure was 1014.7 hPa (minimum, 994.1 hPa; maximum, 1040.4 hPa), and the Ws was 2.0 m/s (minimum, 0.2 m/s; maximum, 5.9 m/s). The DTR is the difference between the daily Tmax and Tmin, i.e., Tmax–Tmin. The mean number of COPD deaths during the study period was 13.8. The ratios of males-to-females, lower-to-higher education level, and the ratio of younger-to-middle-to-older ages were 1:1.1, 66.3:1; and 1:60:372, respectively.A time-series analysis was conducted to evaluate the interaction between daily PM and the DTR on COPD mortality in Weifang, China using data collected from 2016–2018. A distributed lag non-linear model (DLNM) was used to clearly delineate the impact of PM and the DTR on COPD mortality. A two-dimensional smooth response surface was used to demonstrate the interaction between PM and the DTR on COPD.
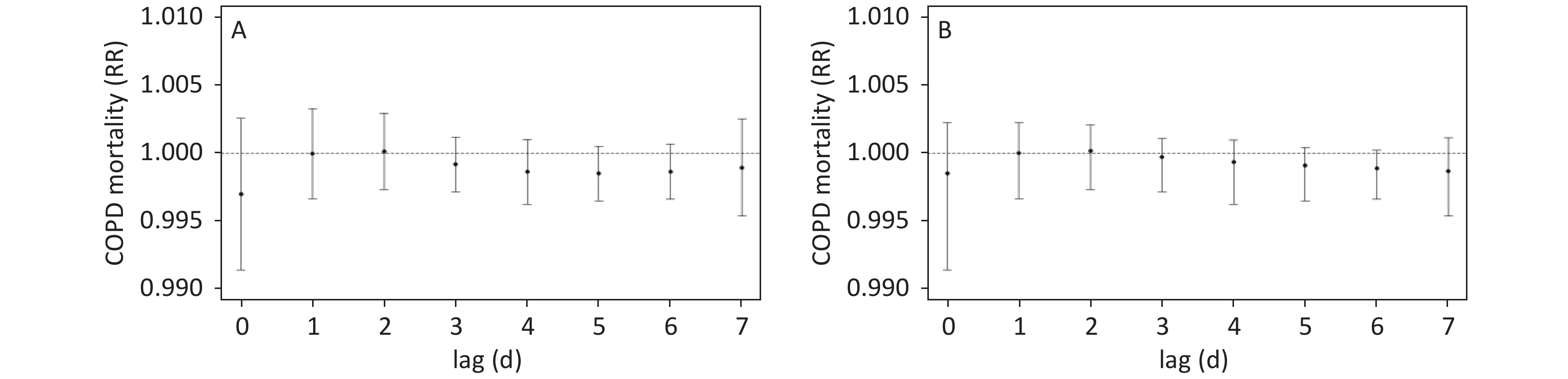
The RR and 95% CI of COPD mortality were obtained by DLNM for every 10 μg/m3 increase of PM with a lag of 0–7 days. This study showed that the effects of PM on COPD were not statistically significant during the lag days. Moreover, lag1 and lag2 days had RRs > 1.000 (Supplementary Figure S2, available in www.besjournal.com). Based on the stratified analyses, the cumulative female and male death rates during lag0–2 days for every 10 μg/m3 increase in PM2.5 were 0.998 and 1.001, respectively, and the cumulative mortality rate varied among different categories of the study population (Supplementary Table S1, available in www.besjournal.com). In agreement with European[5] and German studies[6], the research conducted by our group demonstrated no significant associations between PM and COPD; however, some studies in Asia showed the opposite results, indicating that the number of COPD patients increased with the increase in PM2.5 concentration [7]. Regional differences and PM composition may lead to differences in the adverse effects and toxicity of air pollution, which in turn contribute to inconsistent study results. Changes in the composition of air pollutant mixtures over time could also impose different effects on health. Kunzli[8] reported that PM constituents and correlations vary across regions. In recent years, reports of the atmospheric PM composition spectrum, which consists of hundreds of chemical substances, were ever-growing. Based on a cohort study of COPD patients, the organic carbon, elemental carbon, nitrate, and ammonium salts in PM had the strongest effect on DNA methylation of genes encoding airway inflammatory factors[9].
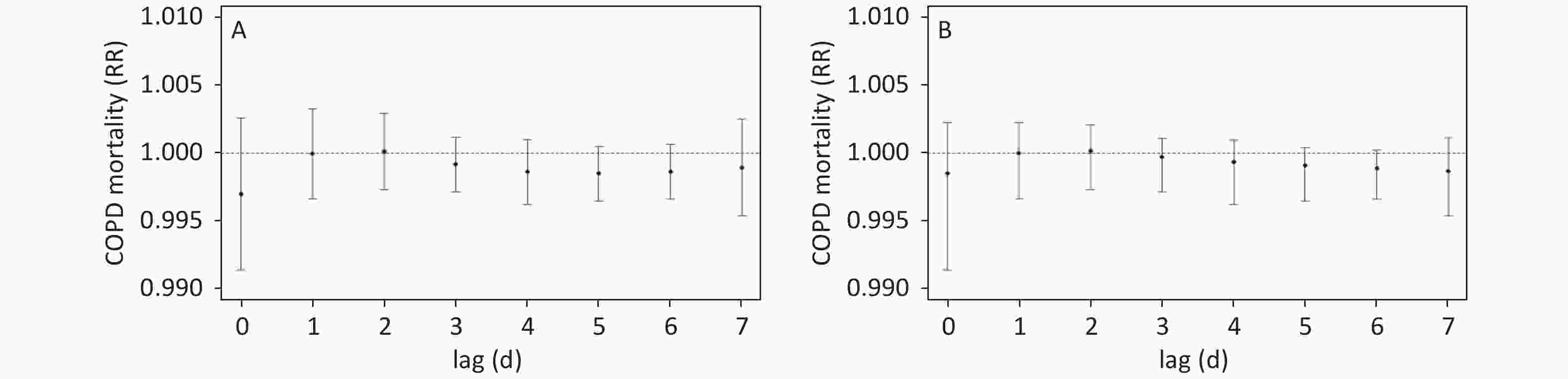
Figure S2. From 2016 to 2018, RR and 95% CI of PM2.5(A)/PM10(B) of COPD mortality in Weifang with lagged 0–7 days.
Groups PM2.5 PM10 Lag0-1 Lag0–2 Lag0–1 Lag0–2 RR 95% CI RR 95% CI RR 95% CI RR 95% CI All cases 0.999 0.996–1.003 1.000 0.997–1.002 1.000 0.996–1.002 1.000 0.997–1.002 Sex Female 0.997 0.992–1.001 0.998 0.994–1.002 0.998 0.996–1.001 0.999 0.997–1.002 Male 1.003 0.998–1.007 1.001 0.998–1.005 1.001 0.996–1.004 1.000 0.997–1.003 Education Lower 1.000 0.996–1.003 1.000 0.997–1.002 1.000 0.996–1.002 1.000 0.997–1.002 Higher 0.993 0.970–1.018 1.000 0.979–1.021 0.998 0.996–1.015 1.003 0.997–1.017 Age 39–70 0.996 0.988–1.004 0.995 0.988–1.002 0.998 0.996–1.003 0.998 0.997–1.002 70+ 1.000 0.997–1.003 1.001 0.997–1.003 1.000 0.996–1.002 1.000 0.997–1.002 Table S1. Association between the concentration of PM and COPD mortality based on lag0–2
This study compared the effects of single factors and single factor interactions on COPD. The higher education group RRs were 1.000 and 0.997 for the PM2.5-single and PM2.5-DTR-cross effects, respectively. The RRs for the population 39–70 years of age for the PM2.5-single and PM2.5-DTR-cross effects were 0.995 and 0.993, respectively, while the corresponding RRs for those > 70 years of age were 1.002 and 1.003, respectively. The male group RRs for the PM10-single and PM10-DTR-cross effects were 1.001 and 1.000, and the corresponding RRs for the higher education group were 0.998 and 1.003, respectively. None of the RRs were statistically significant (Supplementary Table S2, available in www.besjournal.com).
Groups PM2.5 PM2.5 and DTR PM10 PM10 and DTR RR 95% CI RR 95% CI RR 95% CI RR 95% CI All cases 1.000 0.997–1.002 1.000 0.997–1.003 0.999 0.992–1.002 0.999 0.998–1.001 Sex Female 0.998 0.994–1.002 0.998 0.994–1.003 0.998 0.997–1.001 0.998 0.998–1.001 Male 1.001 0.998–1.005 1.002 0.998–1.006 1.001 0.997–1.004 1.000 0.998–1.003 Education Lower 1.000 0.997–1.002 1.000 0.997–1.003 0.999 0.997–1.002 0.999 0.998–1.001 Higher 1.000 0.979–1.021 0.997 0.974–1.020 0.998 0.997–1.015 1.003 0.998–1.018 Age 39–70 0.995 0.988–1.002 0.993 0.986–1.001 0.997 0.997–1.003 0.997 0.998–1.002 70+ 1.001 0.997–1.003 1.002 0.998–1.004 1.000 0.997–1.002 1.000 0.998–1.002 Table S2. Comparison of the effects of single and interactive on COPD
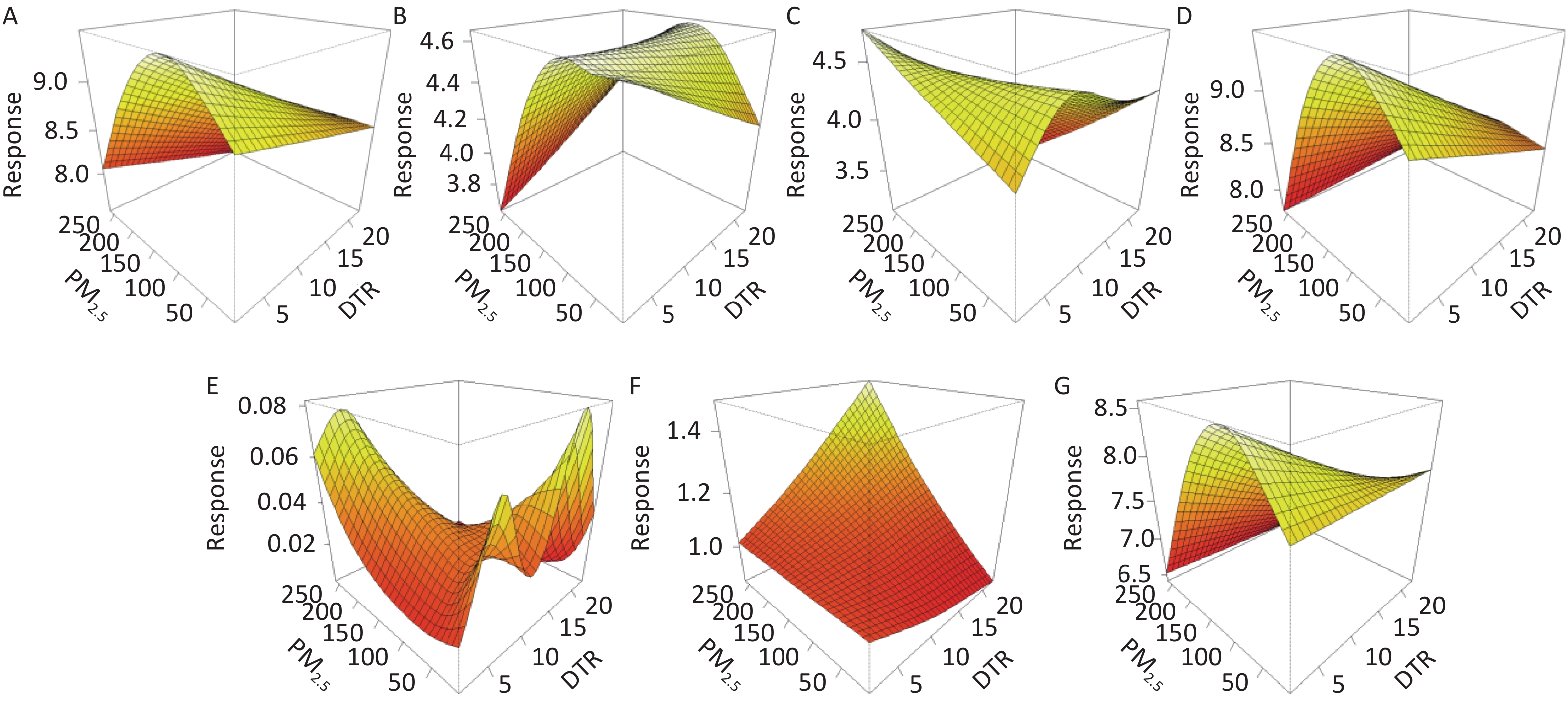
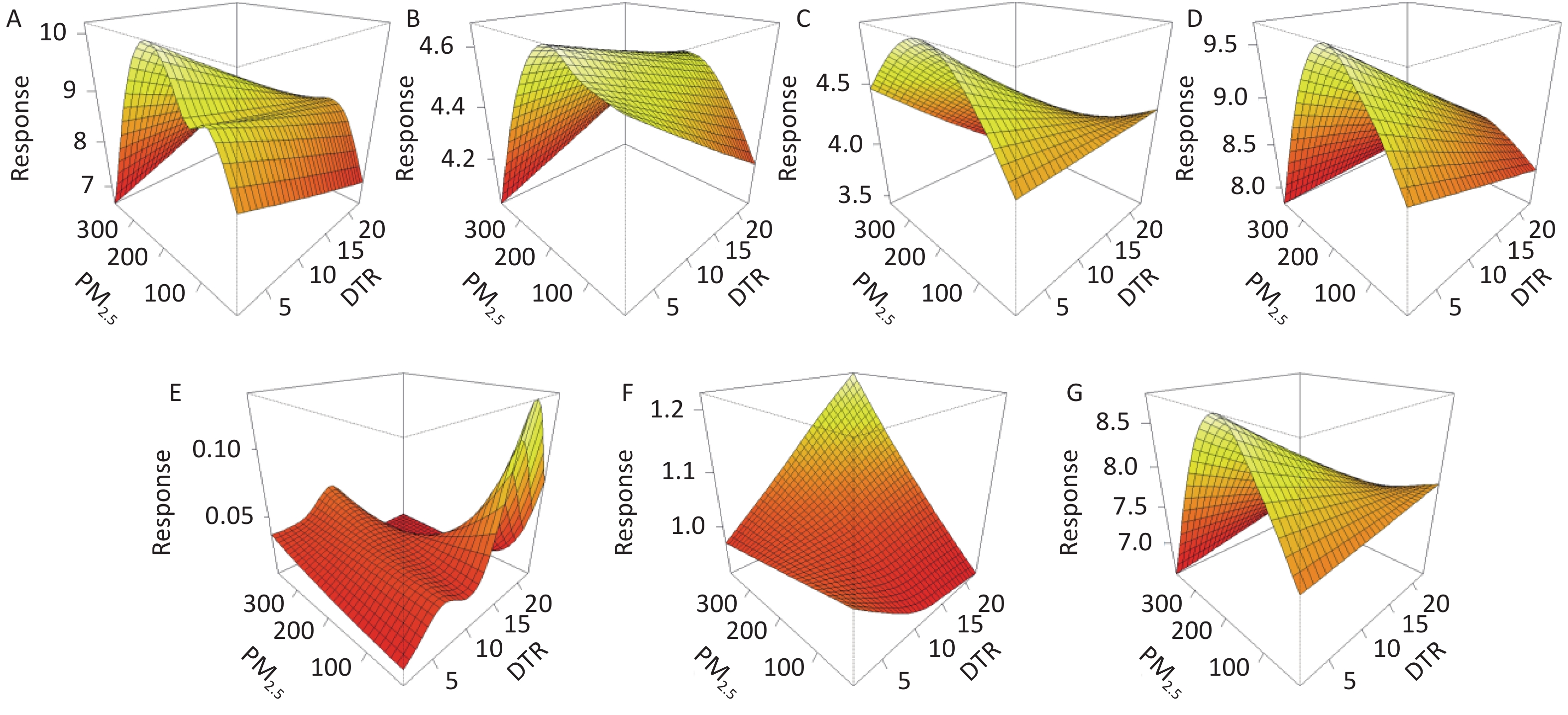
As shown in Figures 1 and 2, the COPD-associated mortality rate increased as the DTR decreased and the PM increased, especially the higher education group and the middle age group (aged 39–70).
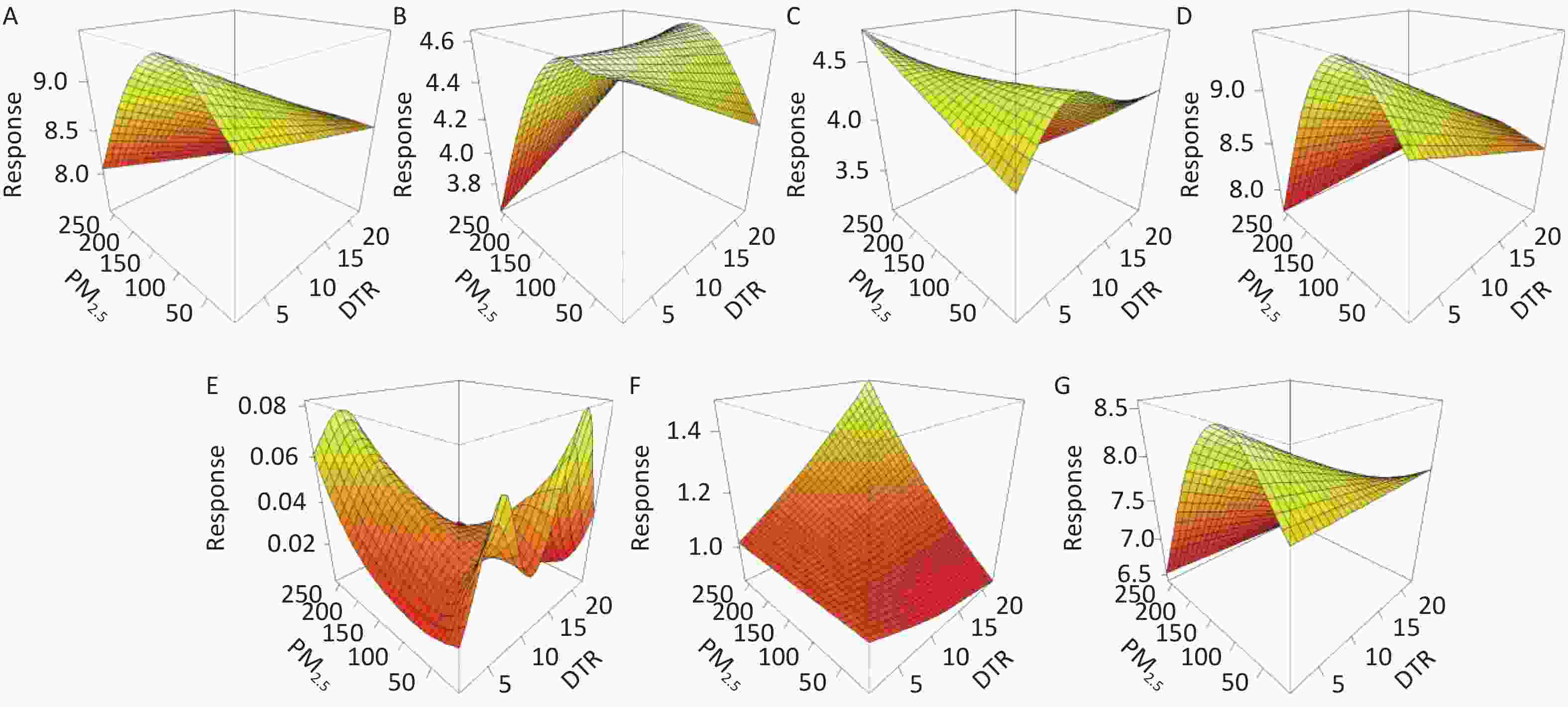
Figure 1. PM2.5-DTR response surface plots for COPD in different Weifang populations, 2016–2018.
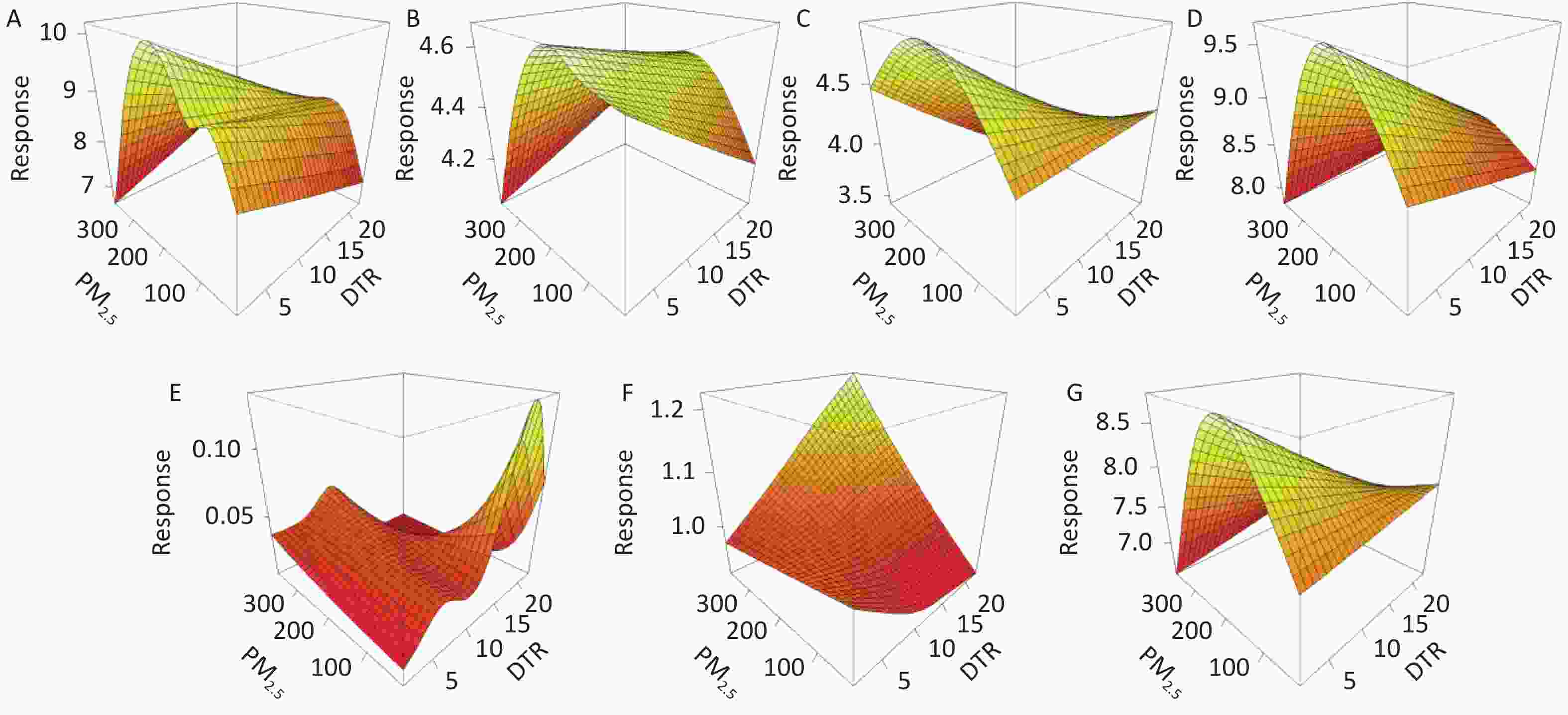
Figure 2. PM10-DTR response surface plots for COPD in different Weifang populations, 2016–2018.
We divided the DTR into three levels to determine the effect of PM in different DTR strata, and reported the interaction effect of PM and the DTR on COPD mortality. When the DTR was divided into 3 levels at the 5th and 95th percentiles, the independent effect of DTR at different levels or PM on COPD was not statistically significant. The interaction between PM and low extreme DTR led to a significant increase in COPD mortality (Table 1). The cross-effect of PM2.5 and low-DTR was associated with increased COPD mortality; the RRs and 95% CIs of the male and higher age groups were 1.002 (1.000, 1.005) and 1.002 (1.000, 1.005), respectively. The cross-effect of PM10 and low-DTR was also associated with increased COPD mortality; the RRs and 95% CIs for male, lower education, and older age groups were 1.002 (1.000, 1.004), 1.001 (1.000, 1.003), and 1.002 (1.000, 1.003), respectively. The interaction between high-DTR and PM on COPD was mostly non-significant. Only the higher education group had a protective effect; the RR and 95% CI was 0.934 (0.877, 0.995). With extreme low-DTR as a covariate for PM, the prevalence of COPD was higher compared with the DTR (three levels) and PM as independent factors. Based on this result, it is possible that the extreme low-DTR had a synergistic effect with PM when PM had an influence on COPD. Luo[10] showed that the effects of extreme high- or low-DTR on health events were more severe than moderate-DTR, and extreme low-DTR had a greater immediate influence than extreme high-DTR. The relatively higher risk of death from COPD in males, the less educated, and the elderly may be due to a greater sensitivity to environmental changes. Moreover, males were more likely to be exposed to PM in the workplace and were more likely to smoke cigarettes than females, which also increased the risk. The elderly were more susceptible to PM due to decreased immune and respiratory functions. Compared with the members of the population with a higher education level, those with a lower education level may be involved in a working environment associated with more PM and less protective measures.
Groups All cases Male Female Low-education High-education 39–70 70+ PM2.5 0.999 0.999 0.999 0.999 0.999 1.000 0.999 0.998 0.998 0.998 0.998 0.993 0.999 0.998 1.000 1.000 1.000 1.000 1.004 1.002 1.000 PM10 0.999 0.999 0.999 0.999 0.999 1.000 0.999 0.999 0.999 0.999 0.999 0.996 0.999 0.999 1.000 1.000 1.000 1.000 1.003 1.001 1.000 Low-DTR 0.874 0.887 0.859 0.881 0.520 1.144 0.835 0.751 0.726 0.691 0.756 0.152 0.790 0.712 1.016 1.084 1.068 1.026 1.774 1.654 0.980 High-DTR 0.902 0.832 0.995 0.898 24.457 1.109 0.872 0.737 0.641 0.738 0.733 0.924 0.666 0.706 1.103 1.079 1.342 1.099 647.045 1.847 1.079 PM2.5: Low-DTR 1.002 1.002 1.001 1.002 1.002 0.997 1.002 0.999 1.000 0.997 0.999 0.985 0.991 1.000 1.004 1.005 1.004 1.004 1.018 1.003 1.005 PM2.5: High-DTR 1.001 1.002 0.999 1.001 0.934 0.998 1.001 0.998 0.999 0.995 0.998 0.877 0.991 0.998 1.003 1.005 1.003 1.003 0.995 1.005 1.004 PM10: Low-DTR 1.001 1.002 1.000 1.001 1.001 0.998 1.002 1.000 1.000 0.998 1.000 0.989 0.993 1.000 1.003 1.004 1.003 1.003 1.013 1.002 1.003 PM10: High-DTR 1.000 1.001 1.000 1.000 0.956 0.999 1.000 0.998 0.998 0.997 0.998 0.918 0.994 0.999 1.002 1.003 1.002 1.002 9.961 1.003 1.002 Table 1. The interactive effect of PM and different DTR levels on COPD mortality [RR (first row of each group), lower bound of 95% CI (second row), and higher bound of 95% CI (third row)]
In conclusion, we have reported novel findings involving the interaction between PM and low-DTR, which increased the COPD mortality risk in Weifang, China. Only one city was studied, which might limit the generalizability of our results; however, the findings of this research may encourage large-scale, multi-center studies in the future.
Author Contributions DIAO Li Jie, GAO Zhi Hao, XU Xin, JIANG Yi Chen, and LI Jing conceived and designed the study; CHEN Zuo Sen, LI Ning, MENG Xian Feng, and LI Jing collected the data; GAO Zhi Hao and XU Xin analyzed the data; and DIAO Li Jie, GAO Zhi Hao, and JIANG Yi Chen wrote the paper.
Conflict of Interest Disclosures The authors declare that they have no competing interests.
Linear and Interactive Effects of Air Pollution and Diurnal Temperature Range on COPD Mortality in Weifang, China: A Time Series Analysis
doi: 10.3967/bes2021.093
Funds:
This study was supported by the Key Research and Development Plan of Shandong Province [No.2019GSF111067]; the Shandong Provincial Social Science Planning Research Project [No.18CQXJ18]; the Shandong Medical and Health Technology Development Plan [No.2017WS703]; the Teaching Reform and Research Project of Weifang Medical College [No.2018YB013]; the National Steering Committee of Medical Professional Degree Postgraduate Education Project [No.C-YX20190301-04]; and the Medical Education Research Project of Medical Education Branch of Chinese Medical Association and Medical Education Professional Committee of Chinese Association of Higher Education [No.2018A-N02079]
- Received Date: 2020-11-13
- Accepted Date: 2021-05-06
| Citation: | DIAO Li Jie, GAO Zhi Hao, JIANG Yi Chen, CHEN Zuo Sen, LI Ning, MENG Xian Feng, XU Xin, LI Jing. Linear and Interactive Effects of Air Pollution and Diurnal Temperature Range on COPD Mortality in Weifang, China: A Time Series Analysis[J]. Biomedical and Environmental Sciences, 2021, 34(8): 662-666. doi: 10.3967/bes2021.093

|

 Quick Links
Quick Links
 DownLoad:
DownLoad: