


-
Knee pain and discomfort appear at the early stages of normal aging, which lead to impaired mobility and reduced quality of life (QOL). Among age-related conditions, osteoarthritis (OA) is considered the most significant cause of disability. The acceleration of the aging process in China has troubled the middle-aged and elderly with a relatively high prevalence of OA, as recently reported in a meta-analysis pooling and analyzing epidemiological publications on OA in the middle-aged and elderly Chinese published from 2000 to 2018 [1].
The underlying mechanisms of the onset of OA with aging are not entirely elucidated; however, evidence is growing that a combination of local and systemic factors is involved with a complex interaction of mechanical, biochemical, and pro-inflammatory mediators.
Current interventions are focused on managing symptoms in individuals with OA but are largely inadequate, which results in incomplete pain reduction and, usually, without improved function or modified disease progression [2].
Resistance exercise showed to be effective for pain relief, pain and stiffness alleviation, and physical function improvement. Interestingly, a first, recent systematic review/meta-analysis on the effects of Traditional Chinese Exercise (TCE), which combines low-level aerobic exercise, strength, balance, and coordination, showed beneficial effects on reducing pain, improving physical function, and alleviating stiffness and symptoms in patients with OA after TCE interventions of average 12 weeks [3]. These conclusions are consistent with previous reviews on the benefits of Tai Chi on knee OA.
Other non-pharmacological approaches involve the use of dietary supplements, with the most widely studied glucosamine and chondroitin. The feasibility single-arm baseline trial of Ng et al. (2010) [4] showed that combining a progressive walking program (at least 3,000 steps, 3 days/week) and daily supplementation with glucosamine sulfate (1,500 mg/day) helped to alleviate OA symptoms of the hip and knee in OA participants over 6–12 weeks of intervention. In a Japanese population, Kanzaki et al. [5] demonstrated that supplements containing a mixture of nutrients, including 1,200 mg of glucosamine, were effective in improving locomotor function. However, very few studies have been conducted on individuals at risk but not yet diagnosed with OA.
Due to the multifactorial nature of OA, the increasing incidence in the adult population at earlier ages (linked to the obesity epidemic), and the inadequacy of a single treatment approach, interest is growing in the implementation of more holistic lifestyle approaches.
This study aimed to test the feasibility of combined nutrition and exercise approach in healthy older adults who are experiencing joint pain and discomfort but not yet diagnosed as OA and test if such interventions would alleviate symptoms and improve the QOL.
This study employed a single-center, single-arm, and open-design format with a single treatment group, where each participant acted as their control. A total of 54 healthy participants [mean age 55.8 ± 5.09 years, mean body mass index (BMI) 24.1 ± 2.61 kg/m2] were recruited and included in the present study (Supplementary Table S1, available in www.besjournal.com). All participants were non-diagnosed for OA.
Parameter Baseline
Mean ± SEM
(range)6 months
Mean ± SEM
(range)Age (years) 55.8 ± 2.26 (47–65) N/A Sex 7
47N/A Weight (Kg) 62.5 ± 3.05 (43–86) 62.2 ± 10.15 (42–89) Height (cm) 161.8 ± 2.60 (141–178) N/A BMI (kg/m2) 23.8 ± 1.59 (20–28) 23.9 ± 1.71 (19–30) Calcium intake (mg/d) 672 ± 15.7 (317–1,255) 520 ± 13.7 (279–1,053) Proteins intake (g/d) 76.7 ± 5.2 (54.5–138.7) 74.1 ± 4.8 (32.5–146.5) Note. Values are expressed as mean ± SEM. Table S1. Subject (n = 54) characteristics at baseline and 6 months
The study protocol was approved by the Medical Ethics Committee of the Peking University Third Hospital (medical ethics trial 2015-004). All participants in the trial provided their written and signed informed consent. Trial registration: NCT02276183 (
https://clinicaltrials.gov ).The intervention consisted of a progressive physical activity program combined with nutritional supplementation for a total duration of 24 consecutive weeks. For the first 8 weeks, all participants consumed the nutritional supplement in the absence of the physical activity program while monitoring the total daily step count with a pedometer (Garmin SA). The recorded baseline daily step count was
$\cong $ 8,200 on average. At 3 months, the physical activity program was introduced while maintaining the nutritional supplement consumption (Supplementary Figure S1, available in www.besjournal.com). All participants consumed the oral supplement reconstituted in 180 mL of warm water twice per day for the duration of the study. Total daily intake was 50 g of a milk powder supplemented with key nutrients (levels are expressed /100 g of product): glucosamine sulfate at 2,500 mg (2,500–3,200), calcium at 1,350 mg (1,350–2,000), vitamin D3 at 12 μg (12.0–26.0), Zinc at 10.4 mg (10.4–16.2), and vitamin C at 56 mg (56–105) (produced by NESTLÉ SHUANGCHENG LIMITED). No additional dairy product and dietary supplements (including calcium, vitamin D, Glucosamine Sulfate, or any supplement or traditional Chinese medicine that affects tendons, bone, and joints) were permitted to be consumed within the 2 weeks preceding the intake of the first dose of investigational product and during the entire intervention period. Compliance for product intake was 98% for participants who completed the study. Daily calcium and protein intake at baseline was recorded (Mean ± SEM) 672.0 ± 15.7 g/day and 76.7 ± 5.2 g/day, respectively, and were not significantly different at 6 months. (Supplementary Table S1).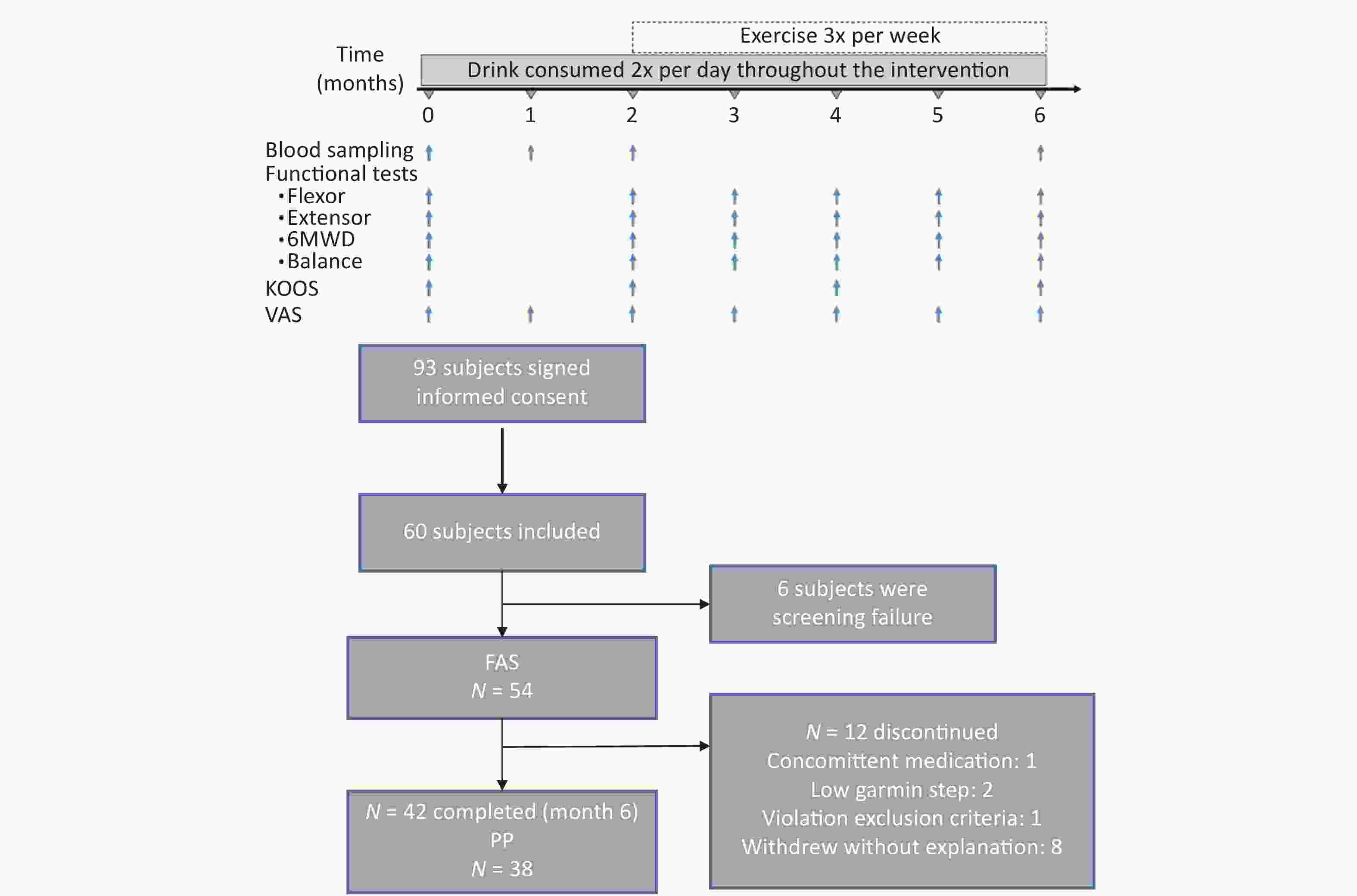
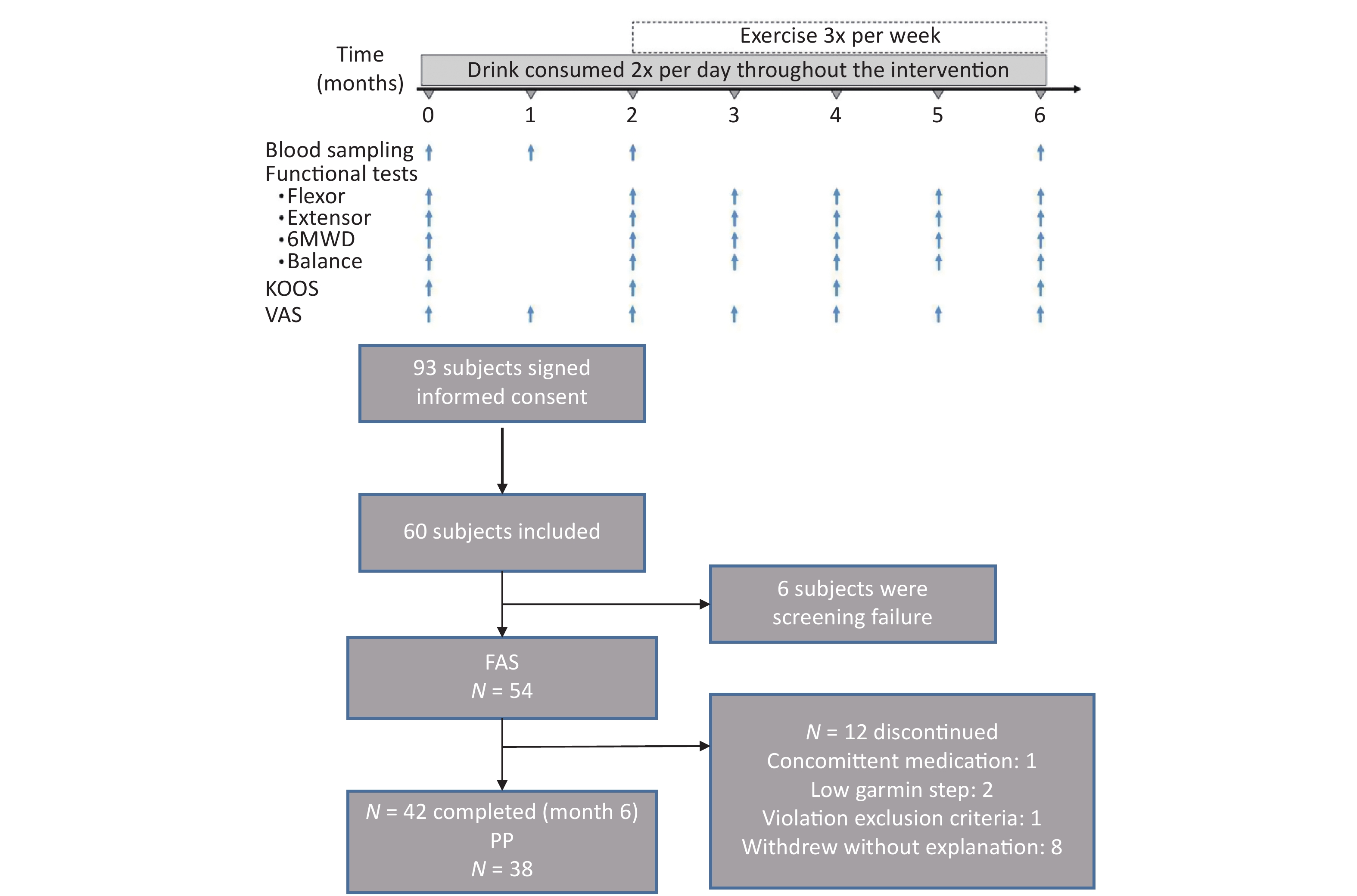
Figure S1. Outline of study highlighting the collection of blood samples and performance of functional tests (isokinetic knee flexor and extensor, 6-minute walking distance test, balance), visual analogue scale for knee pain (VAS score) and osteoarthritis outcomes score (KOOS) and disposition of subjects.
The exercise intervention program was a progressive incremental exercise program that included muscle strength training, balance training, daily aerobic exercises, and Tai Chi. Specifically, muscle strength training was performed 2 days per week for 30 min per day, whereas Tai Chi once per week for 20 min. Balance training was performed at home, twice per week for 10 min per session. A 10-min warm-up and cool-down were performed before and after each exercise session. As the exercise program was progressing over time, the amount of exercise increased by 10%–15% per month based on the previous month’s physical activity level. For muscle strength training, this meant an increased load, and for aerobic exercise an increased target number of steps. The average of daily steps recorded (Garmin) increased as follow: ≈ 8,200 (month 2); ≈ 11,400 (month 3); ≈ 11,900 (month 4), and ≈ 12,200 (month 6).
During the trial period, a total of seven visits were performed, including baseline (V0), month 1 (V1), month 2 (V2), month 3 (V3), month 4 (V4), month 5 (V5), and month 6 (V6) visits. Co-primary outcomes included the 6-Minute Walking Test and isokinetic strength. Secondary outcomes included the balance test, serum biomarkers of bone, joint, and inflammation, Vitamin D, and patient-reported questionnaires such as Visual Analog Scale (VAS) and Knee injury and OA Outcome Score (KOOS).
The primary analysis focused on the change from baseline at 6 months for combined nutrition and exercise. Therefore, the analysis of covariance model correction for baseline was used with compliance to the physical program as a factor (Average daily Garmin step counts).
No significant difference was found in the results between the two population sets [Intent-to-treat analysis (ITT) and per-protocol]; thus, only ITT results are listed.
Physical activity has been outlined in several international guidelines, including the Osteoarthritis Research Society International and European Alliance of Associations for Rheumatology, as a recommended non-pharmacological approach aimed to improve functional outcomes in individuals with early-stage OA. Participants in our present study were not overweight or obese (BMI: 24.1 ± 2.61 kg/m2); thus, the low-intensity physical activity component was chosen to improve functional outcomes through increased leg strength and balance and not weight loss per se, which previously showed functional improvement in patients with OA [6].
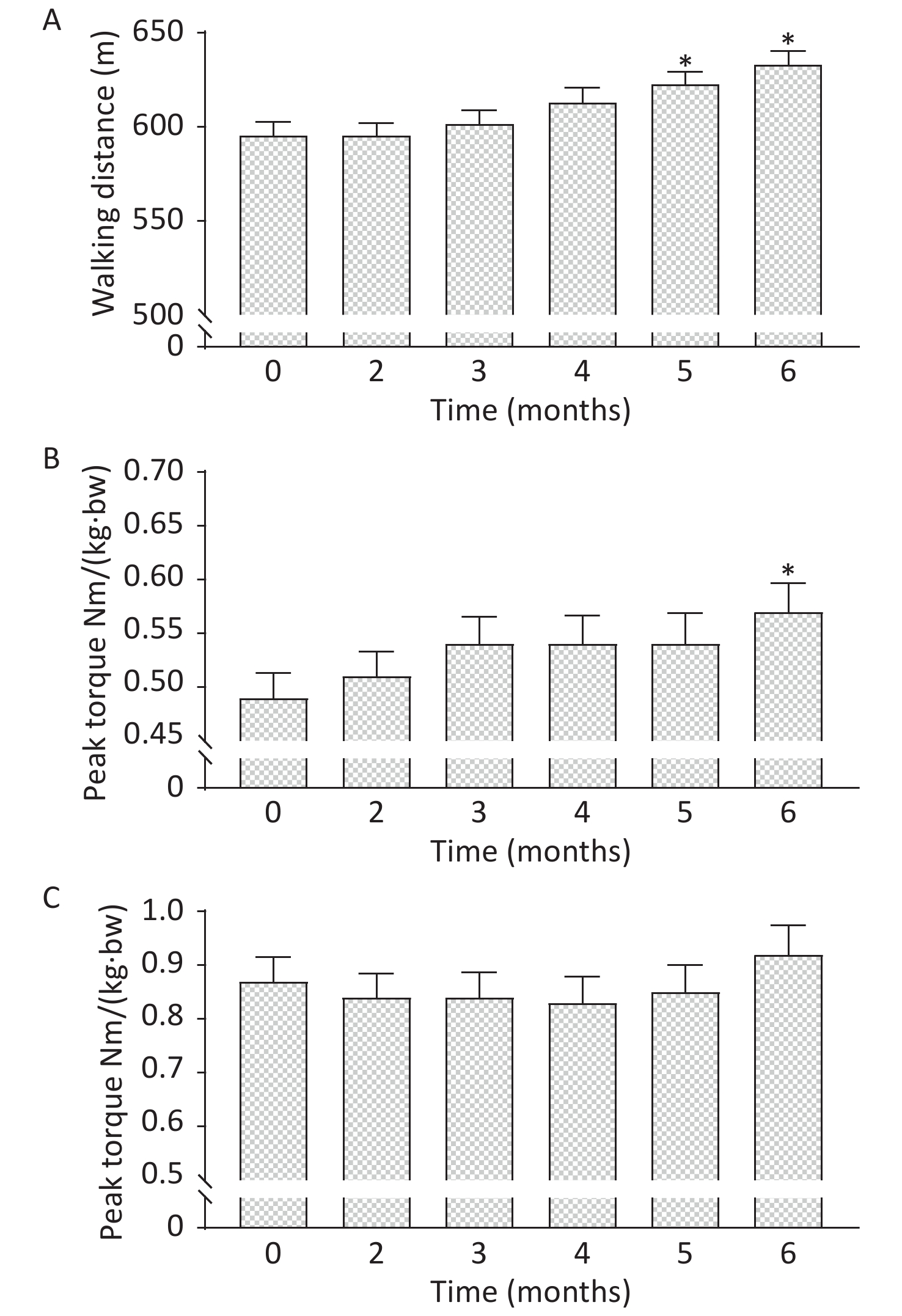
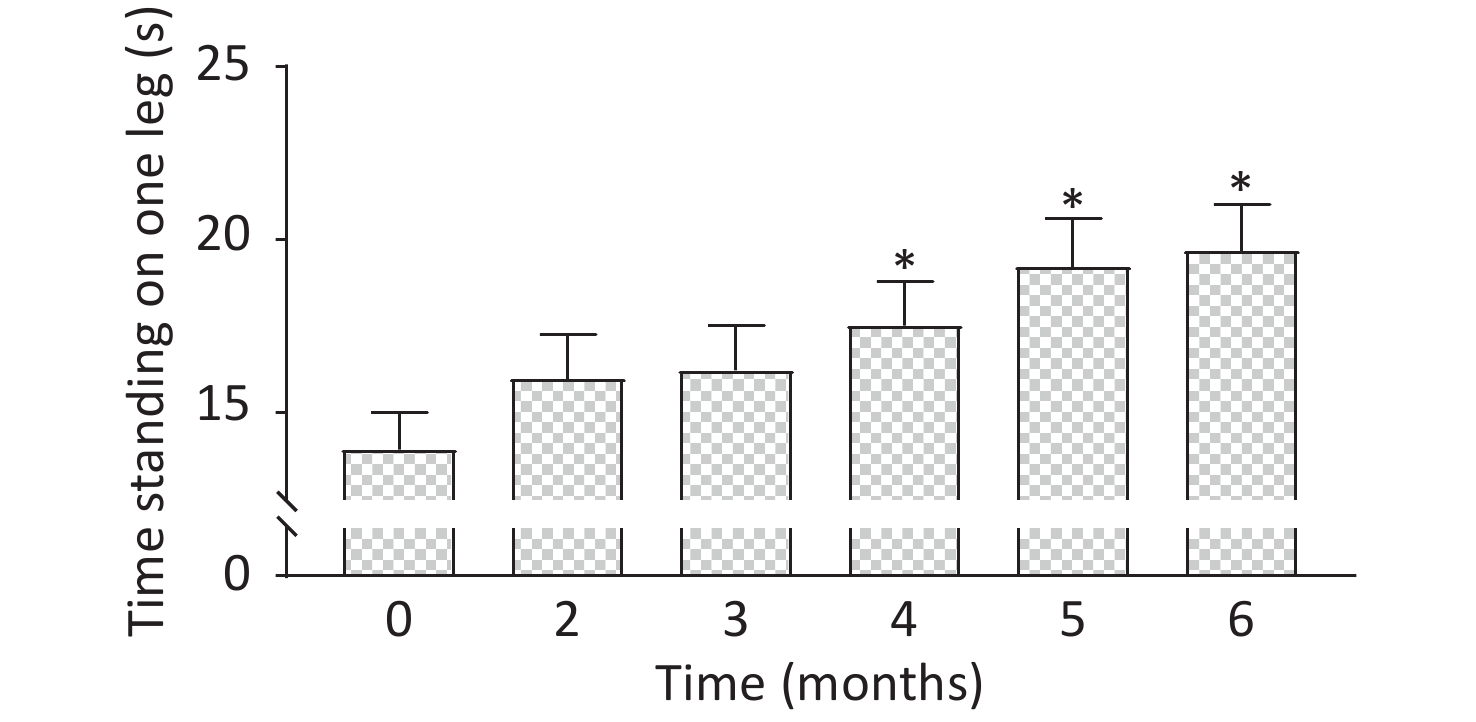
A significant difference was found in the walking distance during the 6-minute walking distance test. Specifically, an increase of 27 and 38 meters at months 5 and 6 was noted, respectively (P < 0.05) compared to baseline (Figure 1). The isokinetic peak torque assessment showed a statistically significant increase in peak knee flexor torque at 6 months compared to baseline (P < 0.05) (Figure 1), a finding in line with previous reports [7]. Contrary to our trial, these studies were conducted in patients with OA. Of note is the fact that we observed a significantly increased time for participants to stand on one leg from month’s 4–6 inclusive (Figure 2).
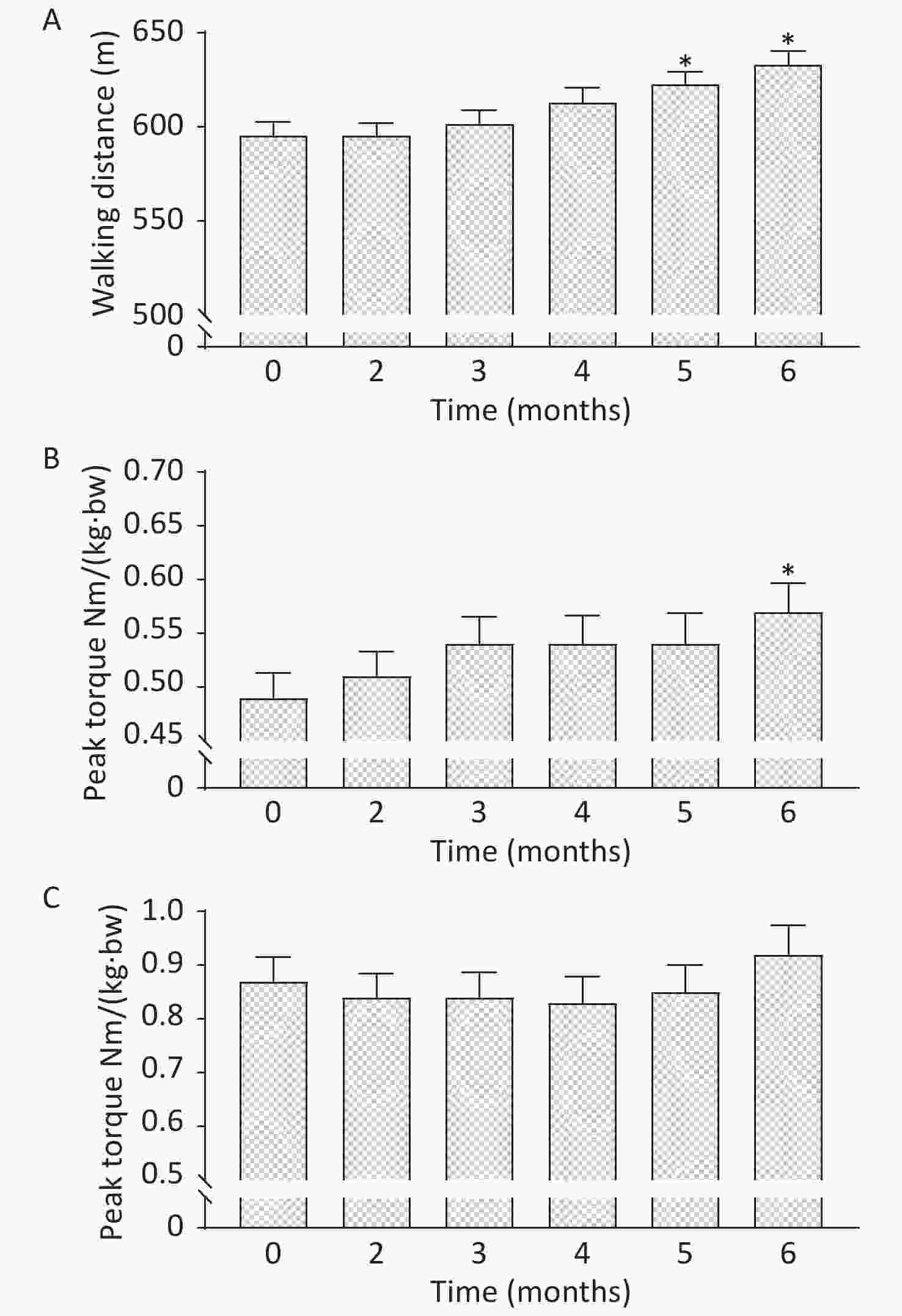
Figure 1. Data showing A) the distance covered during the 6- minute walking distance (6MWD) test, isokinetic B) flexor and C) extensor peak torque corrected for body weight, throughout the duration of the trial. *P < 0.05 relative to baseline (0 months). Values are expressed as mean ± SEM.
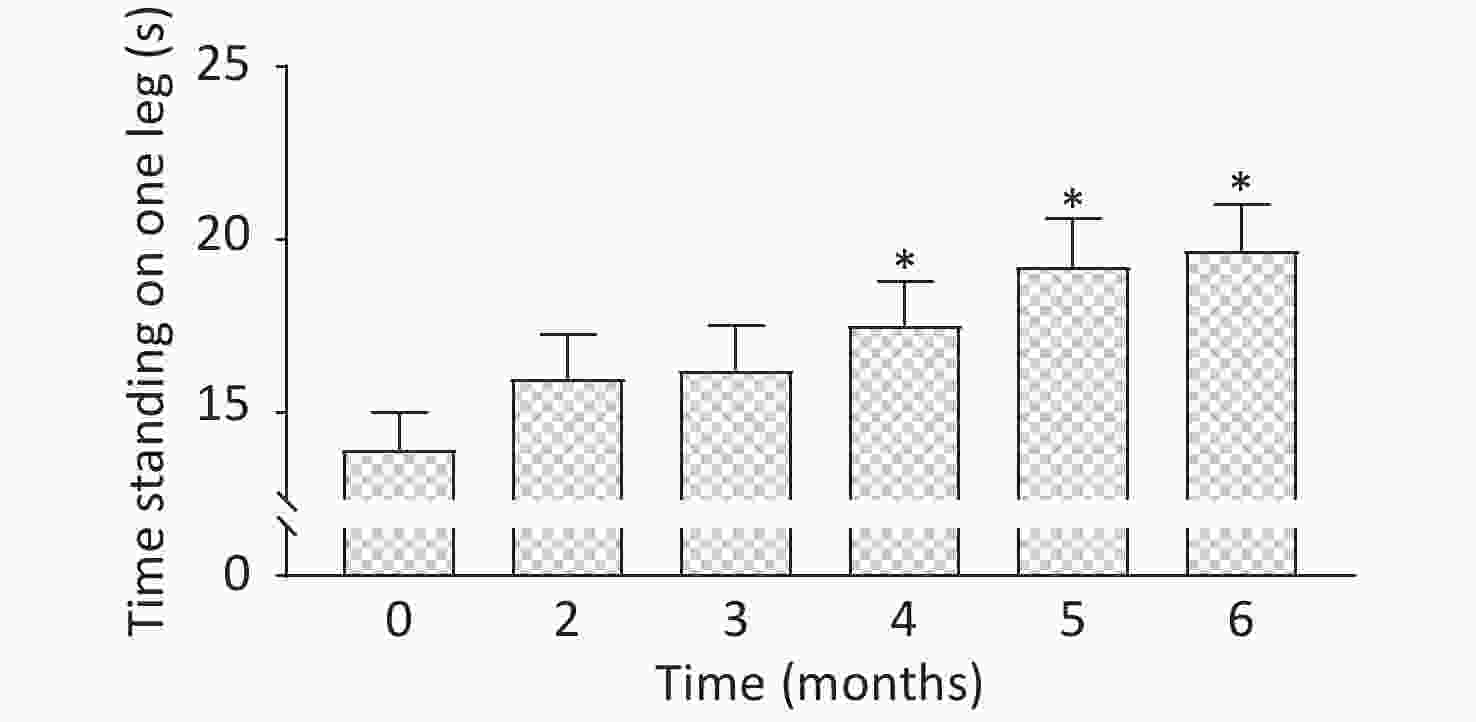
Figure 2. Balance test data showing the time standing on one leg throughout the duration of the trial. *P < 0.05 relative to baseline (0 months). Values are expressed as mean ± SEM.
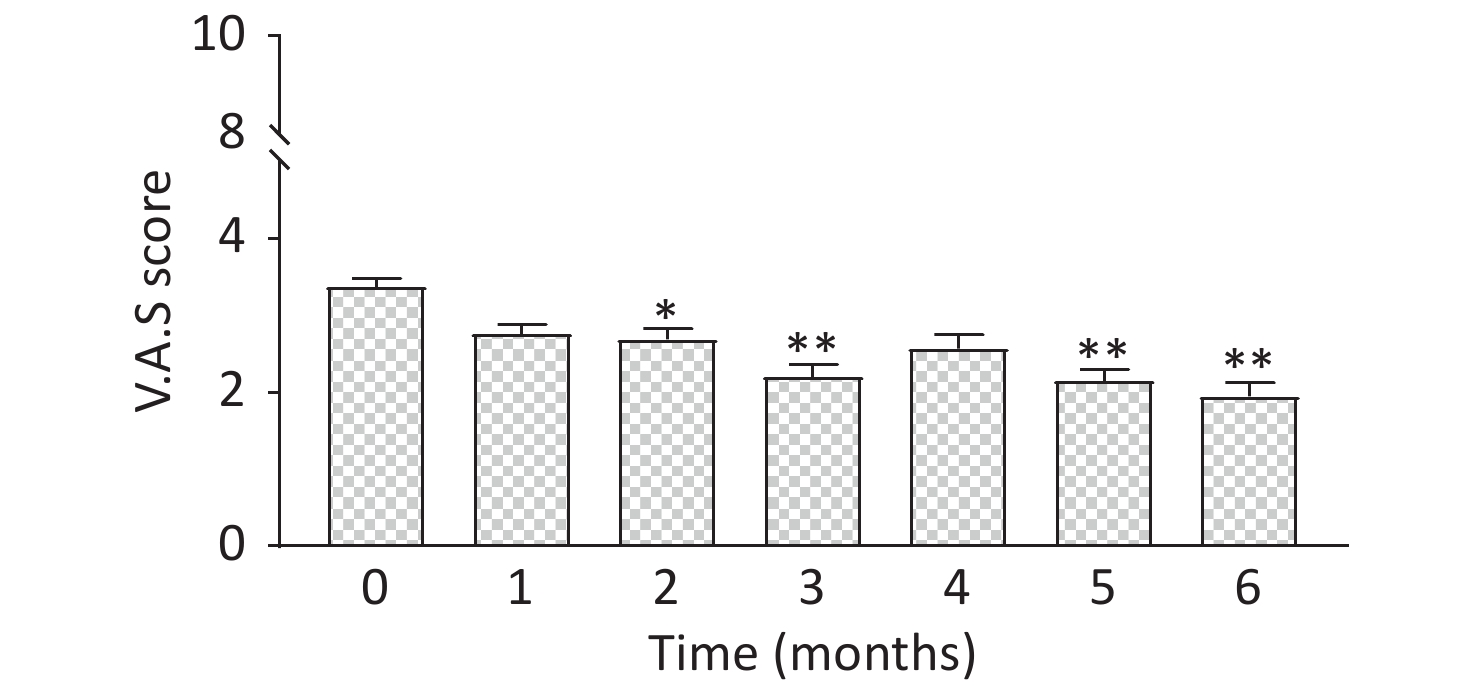
In addition, our program (nutritional blend combined with physical activity) resulted in improvement of self-reported joint discomfort and mild knee pain of participants at 6 months relative to baseline. Indeed, the pain VAS score decreased by 42% (P < 0.001) at 6 months of intervention (Figure 3). Furthermore, KOOS-Pain (5.5%, P < 0.05), activity (4%, P < 0.05), and sport (5.5%, P < 0.05) scores significantly improved at the end of the intervention. This might partly explain the reported KOOS-QoL score that was significantly improved at 4 (28.5%, P < 0.05) and 6 months (51%, P < 0.01) (Supplementary Table S2, available in www.besjournal.com). Ng et al. [4] also showed that combining a progressive walking program and daily oral supplement with glucosamine sulfate (1,500 mg) helped to alleviate OA symptoms of the hip and knee in their OA diagnosed participants by 6–12 weeks of intervention, using the WOMAC questionnaire.
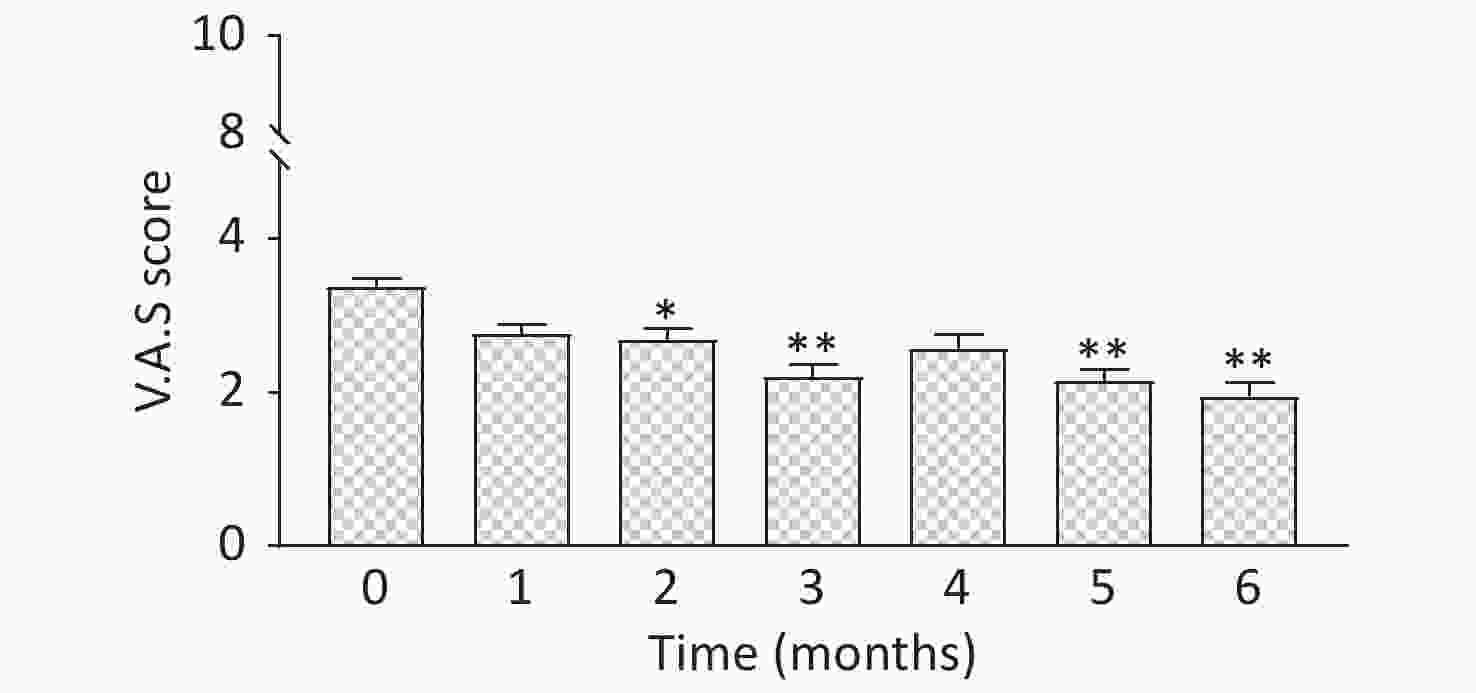
Figure 3. VAS score data showing the knee pain evolution throughout the duration of the trial. *P < 0.05; **P < 0.001 relative to baseline (0 months). Values are expressed as mean ± SEM.
A significant decrease (20%, P < 0.001) was observed in bone resorption markers CTX1 and cartilage breakdown (22%, P < 0.001) at the end of the combined nutrition and exercise phase (Supplementary Table S3, available in www.besjournal.com). This indicates that our lifestyle intervention program may exhibit an osteo-chondroprotective action. Indeed, the biomarkers measured in this study increased in progressive knee OA early stages compared to non-progressive OA and controls [8].
Parameter Month Mean ± SEM CTX-2 0 0.91 ± 0.029 2 0.87 ± 0.043 6 0.71 ± 0.0230** CTX-1 0 0.42 ± 0.030 2 0.36 ± 0.026** 6 0.34 ± 0.025** P1NP 0 49.33 ± 3.02 2 45.28 ± 2.37* 6 43.26 ± 2.54* IL-6 0 2.74 ± 1.56 2 2.85 ± 1.69 6 3.51 ± 2.26 Note. *P < 0.05; **P < 0.001 relative to baseline (0 months). Values are expressed as mean ± SEM. Table S3. Data showing serum levels of biomarkers, i.e. bone resorption (CTX-1, ng/mL), bone formation (P1NP, µg/L), cartilage breakdown (CTX-2, µg/L) and inflammation (IL-6, pg/mL) throughout the duration of the trial
Following the nutritional period alone, biomarkers of bone turnover were altered in response to the nutritional supplement period alone. The bone resorption marker CTX1 was reduced by an average of 15% (P < 0.01). Bone resorption markers were extensively reported to respond rapidly and effectively to milk/Ca-based supplements, which may be supposed that a similar effect is seen here. More surprising was the finding that CTX-2 (a marker of cartilage breakdown) decreased by 5%, although this effect size did not reach significance at 2 months (Supplementary Table S3). Whether this response is due to any single component of the nutritional supplement or the mix interventions remains to be verified. Concerning self-reported knee pain, a 20% decreased knee pain (VAS score, Figure 3, P < 0.001) was shown to be significant after 2 months of intervention. We may speculate that this early effect on the alleviation of pain could be due to an effect of glucosamine, as the results of the previous meta-analysis of the effects of glucosamine formulations on knee pain in OA populations conclude that glucosamine sulfate alone is effective in pain reduction, whereas glucosamine hydrochloride is not [9]. Contrarily, Ng et al. [4] reported improved WOMAC score for symptoms, such as stiffness and physical function but not for pain, at 6 weeks intervention (glucosamine sulfate alone, 1,500 mg/day).
Our study showed some limitations. The main one is that a randomized controlled trial was not performed. However, this single-arm study aimed to monitor the evolution of mobility function outcomes, as well as self-reported outcomes on knee pain and function over 6 months in response to nutrition and physical activity, with each participant being their control. Like previous studies of this kind in diagnosed hip or knee OA participants [4, 10], our study was designed as a pilot, single treatment arm, baseline controlled, open-label trial but in the non-OA diagnosed population. Indeed, translation of findings from clinical studies performed using participants with OA to healthy aging participants has been strongly challenged with the argument that the cellular metabolism may be different between normal and diseased cartilage cells. Therefore, in normal-weight individuals with joint discomfort and pain, the responses may be different from those observed in individuals diagnosed with OA.
Another limitation in this study is the characterization of the population. Even though no radiographic assessment of the knee was performed at recruitment, these baseline characteristics, e.g., BMI, low knee pain, and baseline daily step count (≈ 8,200 average), are representative of healthy/normal aging participants. Furthermore, the mechanical strain exerted on the joints in overweight individuals is recognized as a risk factor for the development and progression of OA and a strong contributor to pain, but participants’ body weight in our study remained unchanged (Supplementary Table S1). Nevertheless, one cannot strongly affirm that all participants were healthy because no diagnosis of any disease has been performed (participants with already an OA diagnosis were excluded). This study tried to include participants that are the targeted participants of the nutritional supplement and the physical activity program and, thus, also check the feasibility for participants. A substantial proportion of our study population may have probably symptomatic OA, as in the general population.
In conclusion, our study revealed that a combined nutrition and exercise program provided a measurable benefit on mobility and QOL in healthy aging who are individuals experiencing mild knee pain and joint discomfort. Despite the limitations of a single-arm trial, which does not allow us to distinguish the relative contribution of nutrition or physical activity, we can nevertheless speculate that the nutritional supplement did contribute to the overall effects. Indeed, some early effects of nutrition alone were observed in the first 2 months of the study (biomarkers of bone and cartilage breakdown and pain scoring). No improvement was seen in the physical function tests after the nutrition period alone; however, functional improvements at 6 months were reported, underlining the importance of the physical activity component. To this end, we cannot exclude that the nutritional intervention may have also indirectly impacted the functional performance over time.
Acknowledgments The authors thank D. Breuille and K. Mace for the critical reading of the manuscript and W. Sauret for setting up and managing the Medidata data capture system. Thank for the Nestlé SA (Switzerland) funded for this study.
Conflicts of Interest The authors declare that there are no conflicts of interest.
Parameter Month Mean ± SEM KOOS- Pain 0 57.46 ± 2.95 2 59.72 ± 2.99 6 60.67 ± 2.15* KOOS- Symptoms 0 59.85 ± 3.62 2 63.01 ± 3.37 6 63.16 ± 3.48 KOOS-ADL 0 64.03 ± 2.69 2 65.81 ± 2.77 6 66.56 ± 3.01* KOOS- Sport 0 49.44 ± 3.92 2 50.54 ± 4.21 6 54.21 ± 4.27* KOOS-QoL 0 35.53 ± 4.17 2 37.28 ± 3.93 6 53.95 ± 4.19** Note. *P < 0.05; **P < 0.001 relative to baseline (0 months). Values are expressed as mean ± SEM. Table S2. Data showing 5-KOOS Scores [i.e. Pain, Symptoms, function in daily leaving (ADL), function in sport and recreation (Sport) and knee-related quality of life (QOL)] throughout the duration of the trial
HTML

 20469Supplementary Materials.pdf
20469Supplementary Materials.pdf
|

|

 Quick Links
Quick Links
 DownLoad:
DownLoad: