


-
Balneatrix alpica is a non-fermentative, oxidase-positive, and gram-negative bacillus with a single polar flagellum. Its optimum growth temperature is 30 ℃, with a range of 20–46 ℃[1,2]. It is transmitted via contact and air-borne spread from hot water. It shows increased susceptibility in the elderly, especially males, and the incubation period ranges from 2 to 17 days. Pneumonia and meningitis were observed in Balneatrix alpica cases, with the earliest symptoms being fever, chills, pleural pain, cough, and hemoptysis[3]. The first case of Balneatrix alpica occurred in France in 1987; however, it has rarely been reported since then. Unfortunately, it was recently reported again in China[4].
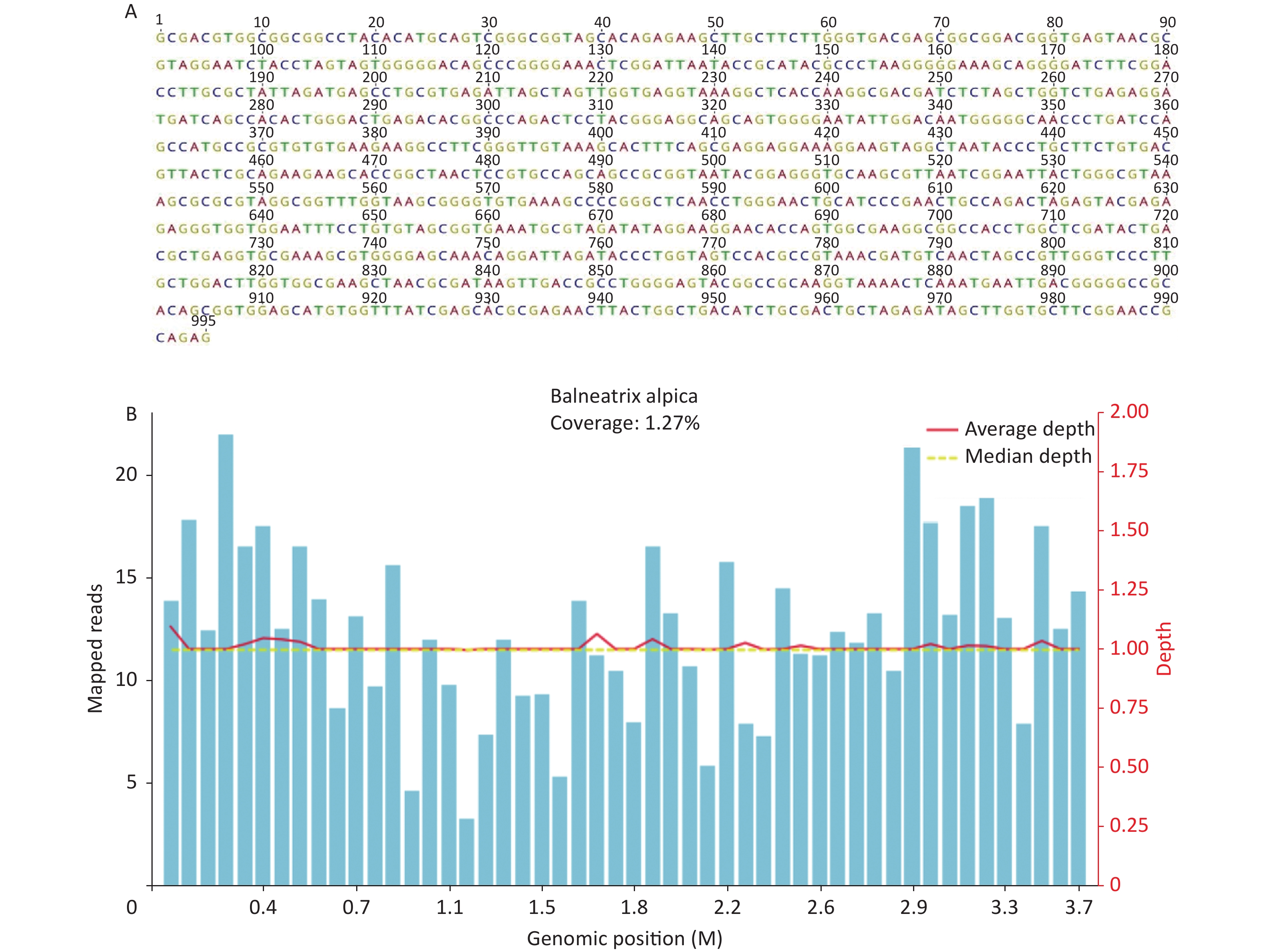
A 62-year-old man with a history of hypertension visited our emergency department in January 2021 with complaints of a 5-day history of intermittent fever and productive cough, followed by a 2-day history of dyspnea (which he treated with azithromycin and acetaminophen but had no improvement). He worked as a security guard, smoked 10 cigarettes a day for 30 years, and had no contact with animals. On arrival, his body temperature was 36.2 ℃, blood pressure was 146/94 mmHg, pulse rate was 123 beats per minute, respiratory rate was 35 breaths per minute, and oxygen saturation was 90% supported by an oxygen face mask with 40% FiO2. The laboratory examination of his blood revealed leukocytosis (white blood cell count, 15.96 × 109/L), inflammatory response (C-reactive protein level, > 200 mg/L), bilirubinemia (bilirubin, 51 umol/L), and metabolic acidosis (pH 7.345 and HCO3− 14.2 mmol/L). Furthermore, the concentration of procalcitonin was 15.05 ng/mL, blood oxygen partial pressure was 60.3 mm Hg, brain natriuretic peptide was 7,384 ng/mL, the serum β-(1,3)-D-glucan was 266.18 pg/mL, and mycobacterium tuberculosis γ-interferon and galactomannan were normal. A chest computed tomography (CT) performed on January 26 (day 1) revealed consolidation in the right upper and lower lobes with air bronchograms and right pleural effusion (Figure 1). The antibiotic therapy was meropenem (Figure 2). On day 2, high-flow oxygen (flow rate 45 L/min and 50% FiO2) was used to improve his hypoxia progression. On day 3, the sputum bacteria and fungi culture were negative. G-bacillus was found in both blood cultures, which we could not identify in our laboratory. Since the pathogen was unknown, the antibiotics were replaced with meropenem and doxycycline, which had a broader antimicrobial spectrum. Targeted Deoxyribonucleic acid (DNA) sequencing was performed on the samples to identify the bacteria (KingMed Diagnostics, Guangzhou, China). On day 6, his body temperature, hypoxia, and inflammatory markers improved, and he was transferred to the general ward. On day 8, amplification of the 16S ribosomal ribonucleic acid (16S rRNA) gene showed a single clear target band, and the Basic Local Alignment Search Tool (BLAST) comparison showed that the sequencing results were similar to Balneatrix alpica (with a similarity of ≥ 99.56%, GenBank No.MN631030) (Figure 3A). Additionally, the pleural effusion metagenomic next-generation sequencing (mNGS) results showed Balneatrix alpica infection, and the sputum mNGS result of DNA was negative (Vision Medicals, Guangzhou, China). A total of 16,628,447 sequences were detected by DNA mNGS, of which 1,083 sequences could be mapped to Balneatrix alpica, with a coverage rate of 1.27%, making up 71.3% of the total microbe sequences (Figure 3B). After identifying the pathogen, we substituted the antibiotic meropenem with cefoperazone-sulbactam. On day 13, chest CT showed less effusion in the right upper lung as well as improved consolidation in the middle and lower lungs. On day 20, the patient had recurrent respiratory symptoms, and the re-examination of inflammatory indicators showed elevated levels. Moreover, the chest CT showed consolidation of the right lower lung again (Figure 1). We adjusted the antibiotics to ceftriaxone and levofloxacin. Subsequently, the patient recovered well and was discharged successfully on day 28. During follow-up visits, the patient’s symptoms did not recur, and a re-examination of his chest CT on day 57 (1 month after discharge) suggested that the lesion in the right lung was absorbed (Figure 1).
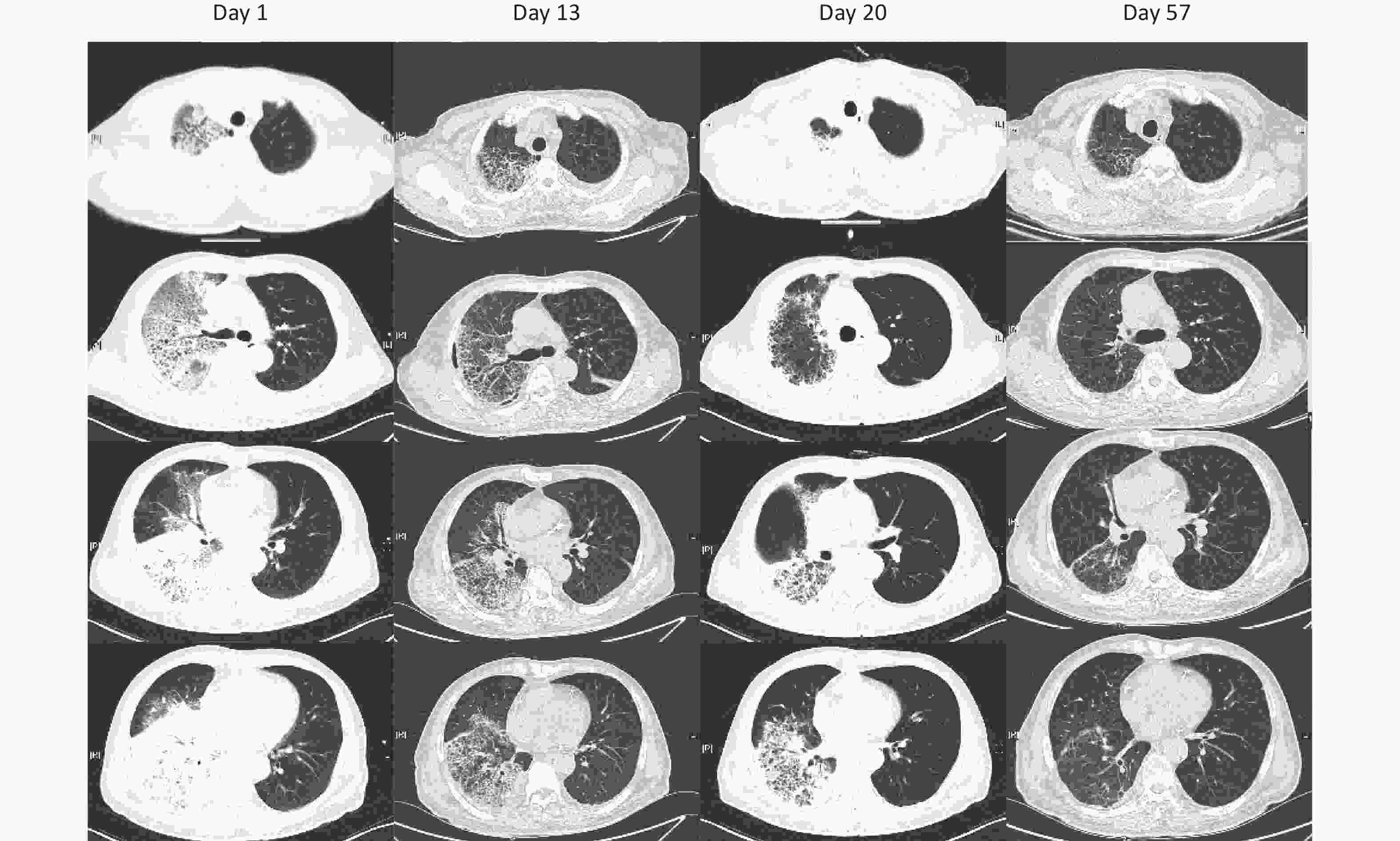
Figure 1. Chest computed tomography of the patient on day 1 (admitted to hospital), 13, 20, and 57 (1 month after discharge).
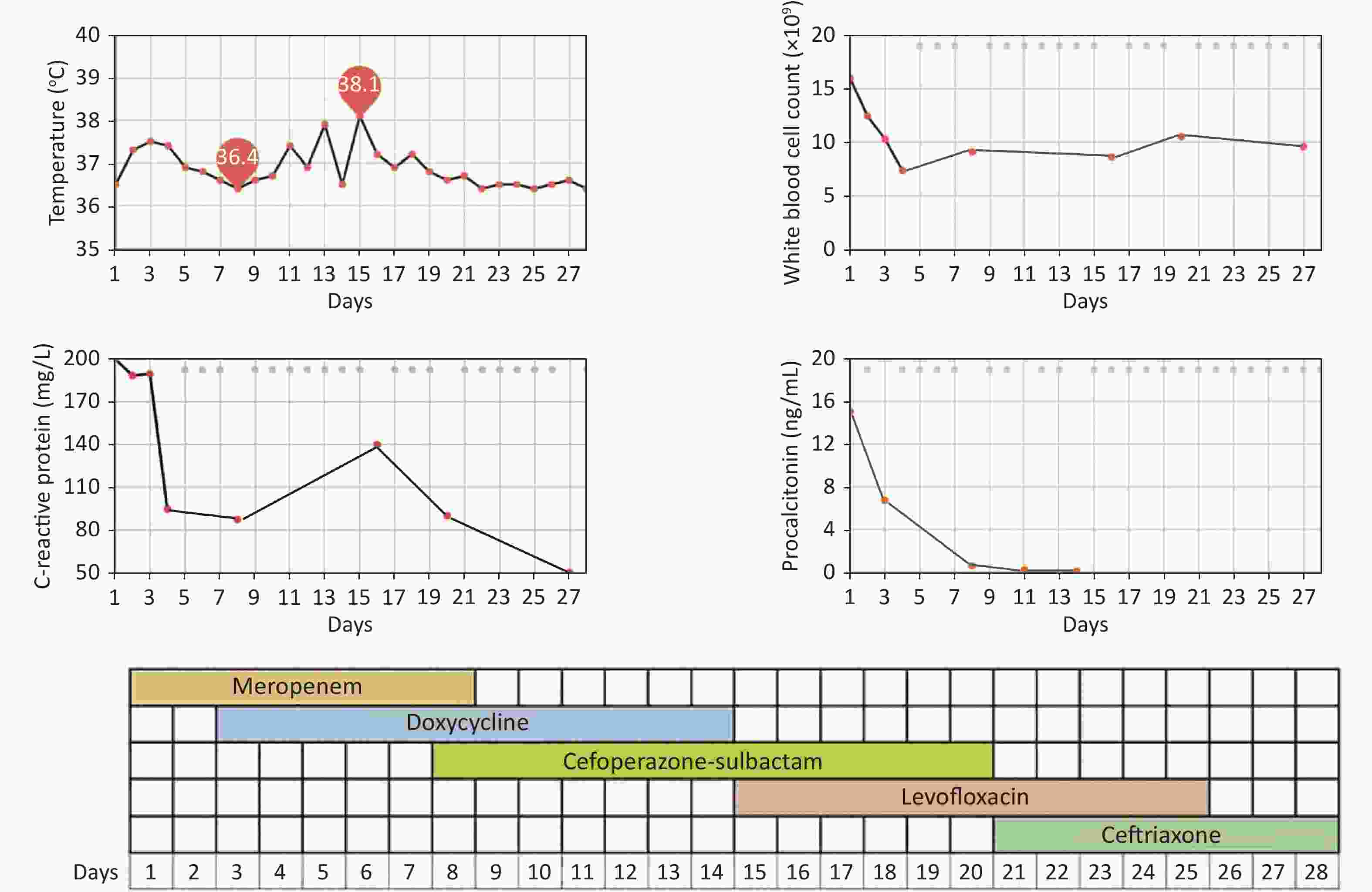
Figure 2. Clinical course of the patient with Balneatrix alpica infection.
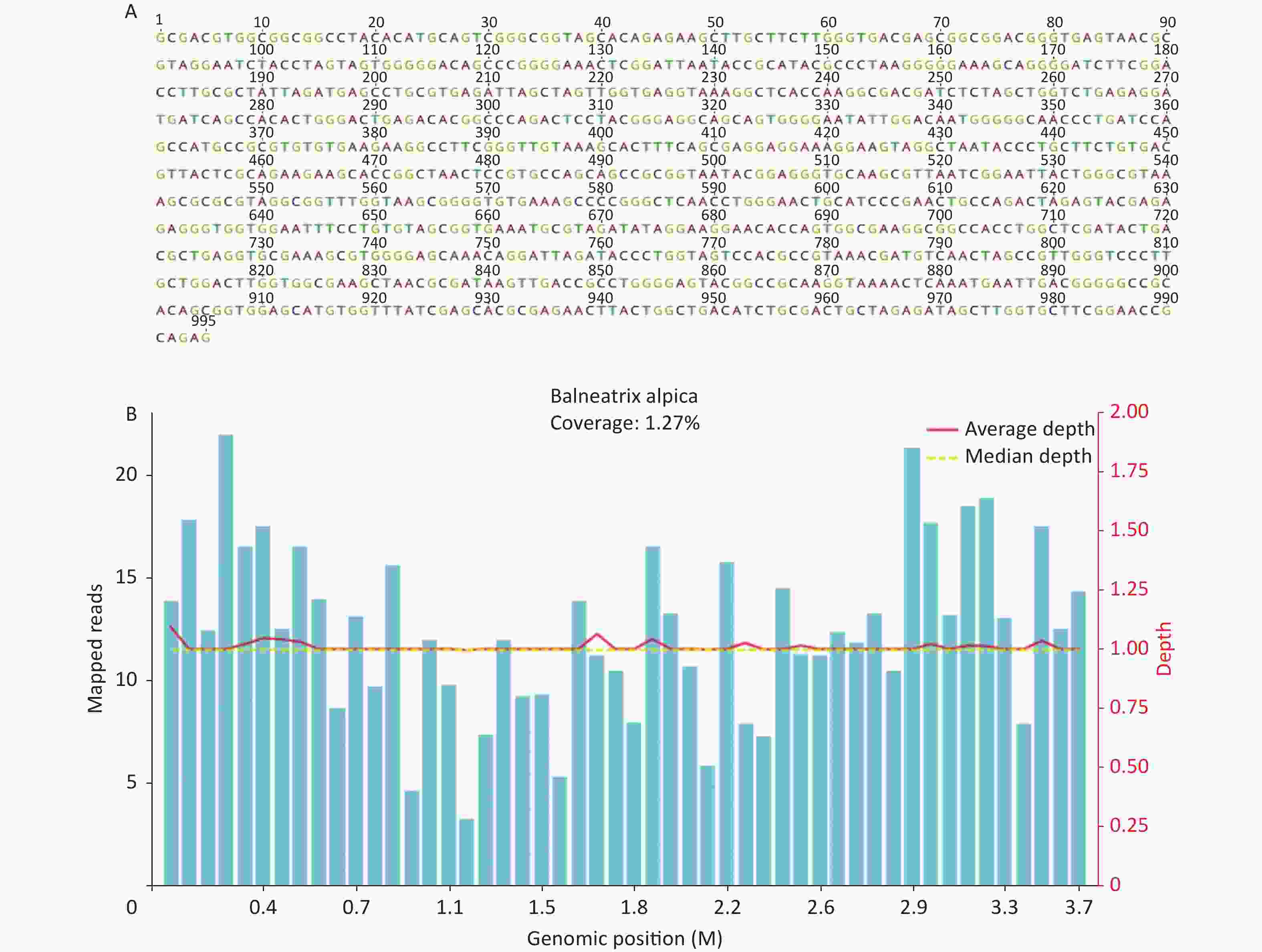
Figure 3. (A) Result of 16S rRNA gene sequence analysis. (B) DNA mNGS results showed that the coverage of Balneatrix alpica was 1.27%.
Balneatrix alpica is a rare pathogen that has not been reported in Pubmed since 1987. After a review of relevant literature [1], we learned that the bacteria’s living environment was related to hot springs. Further examination of the patient’s history revealed that the town he lived in had a spring and that he had a habit of bathing in the spring. Before the onset of the illness, the patient had a history of being exposed to rain. The skin of the patient’s right leg was scratched, and the possible source of the disease may be that the bacteria entered the blood through the skin of the patient’s right leg when he was in the spring. Subsequently, the microbiology staff of our hospital went to the spring for repeated sampling and successfully isolated Balneatrix alpica from the spring water.
A previous report [3] showed that the bacterium caused pneumonia and meningitis; laboratory tests showed elevated inflammatory cells, and chest X-ray showed lobar pneumonia. The drug susceptibility test of Balneatrix strains in vitro indicated that β-lactam, macrolides, aminoglycoside antibiotics, sulfamethoxazole-trimethoprim, chloramphenicol, doxycycline, minocycline, ofloxacin, and nalidixic acid were sensitive, while clindamycin and vancomycin were resistant. In this case, the patient presented with respiratory symptoms, and the course rapidly progressed to severe pneumonia and sepsis (bilirubinemia and hypoxia, SOFA > 2). The chest Computed tomography (CT) result showed consolidation changes in both the upper and lower lobes of the right lung. Unfortunately, our unfamiliarity with the identification of this pathogenic bacteria and the interference of some factors in the treatment process, such as the recurrent respiratory symptoms and the increase of serum β-(1,3)-D-glucan (which later returned to normal), caused a delay in the correct selection of antibiotics. Fortunately, the patient eventually recovered successfully; however, the treatment plan still needs to be summarized and improved. It should be noted that there are many types of spa-associated pathogens, such as Legionella, Enterobacter, and Salmonellae. Legionellae are widely distributed in both natural and artificial water systems, and the fundamental clinical manifestations of Legionella infection are Legionnaires’ disease and Pontiac fever. Legionnaires’ disease is usually characterized by acute pneumonia and a rare extrapulmonary disease; Pontiac fever is a self-limiting flu-like illness that subsides after a few days [5].
The reason for Balneatrix alpica pneumonia is rarely reported, especially for patients who presented to community hospitals and did not have blood, sputum, and other pathogenic microbial examination performed. Balneatrix alpica pneumonia is similar to lobar pneumonia, and there are few reports that treatment with empirical antibacterial is effective. Furthermore, sample culture is the most commonly used method of identifying pathogenic bacteria in clinical practice; thus, laboratory conditions, personnel experience, sample quality, and bacterial species (slow-growing bacteria, rare bacteria, and unculturable bacteria) will affect the results determination. 16S rRNA gene sequence can be performed to complement the traditional culture in identifying rare strains, new pathogens, and uncultured bacteria [6,7]. Moreover, mNGS is a powerful tool for pathogen detection in clinical samples, which enables the detection of organisms associated with the disease in question [8]. In addition, it should be considered that genetic testing is generally not available in hospitals in China; thus, samples need to be sent to genetic testing companies, and the cost is relatively high.
Spa tours or saunas are popular because of the health benefits they offer; however, they also increase the risk of associated bacterial infections. Chemical (e.g., chlorination) or physical (e.g., ultraviolet radiation) disinfection is currently used in recreational water environments. In chemical disinfection, the free chlorine level of the entire pool is 1 mg/L, which ensures adequate routine disinfection. However, the high temperature and pH of springs can reduce the disinfecting effectiveness of free chlorine (volatile, organic complexes), thus suggesting that higher concentrations (up to 2–3 mg/L) may be required [9]. Effective disinfection can reduce potential adverse health consequences, and pre-swim and post-swim baths also help to reduce the risk of bacterium infection.
Our study presented a severe case of Balneatrix alpica pneumonia diagnosed by 16S rRNA gene sequence analysis and mNGS, while the bacterium could not be identified by culture. This bacterium should be suspected in unexplained infection cases following exposure to hot water systems or other artificial water systems.
Ethics Approval and Consent to Participate The patient provided his written informed consent to participate in this study. This case was reviewed and approved by the Biomedical Ethics Committee of Central South University Xiangya School of Medicine Affiliated Haikou Hospital.
Consent for Publication Written informed consent was obtained from the patient for the publication of the case report.
Availability of Data and Materials The datasets used during the study are included in the published articles.
Competing Interests The authors declare no conflicts of interest.
Authors’
Contributions WU Ruo wrote the manuscript. LU Xue Jun and WU Ze collected data and performed the clinical assessment. ZHENG Yong Xian designed the study and conducted the review. All authors reviewed, edited, and approved the final manuscript. Acknowledgments We thank Huang Hui, the chief physician and microbiology staff who successfully isolated the bacterium. We thank Dr. DANG Wen Qiang and colleagues from Guangzhou Kingmed diagnostics for their technical support in the development of this manuscript.
Severe Pneumonia Caused by Balneatrix alpica Associated with Spa
doi: 10.3967/bes2023.021
- Received Date: 2022-09-24
- Accepted Date: 2023-01-12
| Citation: | WU Ruo, LU Xue Jun, WU Ze, ZHENG Yong Xian. Severe Pneumonia Caused by Balneatrix alpica Associated with Spa[J]. Biomedical and Environmental Sciences, 2023, 36(2): 191-195. doi: 10.3967/bes2023.021

|

 Quick Links
Quick Links
 DownLoad:
DownLoad: