


-
Polycystic ovary syndrome (PCOS) is one of the most common causes of infertility in women of childbearing age, affecting 5%–20% of women worldwide and representing a substantial health burden[1]. Some essential microelements, such as copper (Cu) and zinc (Zn), are implicated in several physiological functions. A deficiency or excess of these elements adversely affects female reproductive health[2]. Heavy metals such as mercury (Hg), lead (Pb), and cadmium (Cd), which are commonly present in the environment, can adversely affect female health even at the relatively low levels[3]. Associations between metal(loid) exposure and PCOS risk have been previously reported. The joint effects of Pb, Hg, Cd, arsenic (As), and barium (Ba) on PCOS risk were observed in a Chinese population, of which major contributions may be attributed to As and Pb exposure[4]. In a female rat model, Hg exposure (approximately 8 ng/mL in the serum) induced reproductive and metabolic abnormalities similar to a PCOS-like phenotype[5]. Given that the evidence demonstrating the associations between metal(loid) exposure and PCOS risk is limited and inconsistent, comprehensive research on more metal(loid)s is warranted.
The pathogenesis of PCOS remains unclear; however, disturbances in the hypothalamic-pituitary-ovarian (HPO) axis may contribute to its development[6]. Elevated circulating levels of luteinizing hormone (LH), low-to-normal levels of follicle-stimulating hormone (FSH), and increased androgen levels are often observed in PCOS patients, serving as potential clinical indicators for investigating its pathogenesis[6,7]. Some heavy metals (e.g., Pb, Cd, and Hg) may act as endocrine-disrupting agents, altering hormone homeostasis, including reproductive hormone levels[4,8,9]. In premenopausal women, a negative association between circulating Cd and FSH levels, and a positive association between circulating Pb and progesterone levels were observed[10]. Elevated serum FSH levels were also observed along with higher blood Pb levels in both premenopausal and postmenopausal women[11]. Changes in circulating hormone levels may be important indicators for investigating the associations between metal(loid) exposure and PCOS risk.
Among several hormones, the anti-Müllerian hormone (AMH), a member of the transforming growth factor-β superfamily, has gained considerable attention regarding its potential involvement in PCOS pathogenesis[12]. Serum levels of AMH, LH, and FSH were identified as potential diagnostic markers of PCOS in previous studies, with AMH showing the highest association[13]. It has been considered that AMH levels can be listed as one of the important diagnostic criteria for PCOS, although a consensus on cutoff values has not yet been reached[13,14].
In epidemiological studies, serum samples are typically used to determine internal metal(loid) exposure levels of a population. However, the entry of metal(loid)s into the follicular microenvironment may be affected by the selective permeability of the blood-follicle barrier. Follicular fluid (FF) is considered a better medium than serum to represent ovarian metal(loid) exposure levels. This study aimed to explore the relationship and possible pathways between metal(loid) exposure and PCOS risk. FF samples from a large population of women of childbearing age (25–37 years, with or without PCOS) were analyzed to obtain a better characterization of ovarian exposure profiles. In addition, several clinical indicators were evaluated, and an exploratory mediation analysis was performed to evaluate the possible roles of these indicators in the relationship between metal(loid) exposure and PCOS risk.
-
This retrospective case-control study, conducted between 2018 and 2021, included women who had undergone in vitro fertilization-embryo transfer or intracytoplasmic sperm injection-embryo transfer treatments at Yantai Yuhuangding Hospital (Shandong Province, China). In total, 200 participants with PCOS (cases) and 896 non-PCOS controls (total, 1,096) were loosely matched to increase the sample size. Women aged 25–37 years with a body mass index (BMI) of 18.5–28 kg/m2 were included. PCOS was diagnosed according to the Rotterdam criteria. Details of the study design are provided in
Section S1 (available in www.besjournal.com) of Supporting Information. For each participant, FF collected from the first large follicle was used for metal(loid) analysis. The demographic information of the study participants was extracted from their clinical diagnosis records using their unique medical record numbers. -
FF was collected during oocyte retrieval and stored at –80 °C prior to analysis. In total, 29 metal(loid)s in FF were analyzed using inductively coupled plasma mass spectrometry (ICP-MS). The detailed analysis method was described previously[15]. Briefly, 100 μL of FF was spiked with 100 μL of mixed internal standards [i.e., rhodium (Rh), indium (In), and rhenium (Re)], digested with 1.8 mL of 1% nitric acid, and then thoroughly mixed. Titanium (Ti), manganese (Mn), selenium (Se), chromium (Cr), and As were analyzed using an Agilent 7700x ICP-MS instrument (Agilent Technologies, Santa Clara, CA, USA). Aluminum (Al), germanium (Ge), strontium (Sr), lithium (Li), cobalt (Co), nickel (Ni), molybdenum (Mo), silver (Ag), tin (Sn), antimony (Sb), cesium (Cs), uranium (U), rubidium (Rb), lanthanum (La), cerium (Ce), praseodymium (Pr), neodymium (Nd), yttrium (Y), Zn, Pb, Ba, Cd, Hg, and Cu were analyzed using an Elan DRC II ICP-MS instrument (Perkin-Elmer Sciex, Waltham, MA, USA). Concentrations below the limit of detection (LOD) were replaced with a value equal to LOD divided by the square root of 2 (LOD/√2).
-
Baseline blood samples were collected on the 2nd or 3rd day of the menstrual cycle or vaginal bleeding after drug withdrawal and centrifuged for analysis of clinical indicators. Determination of 14 clinical indicators in serum was performed at Yantai Yuhuangding Hospital, including AMH, LH, FSH, progesterone, estradiol (E2), testosterone (T), prolactin (PRL), thyroid-stimulating hormone (TSH), free thyroxine (FT4), free triiodothyronine (FT3), anti-thyroglobulin antibody (TG-Ab), anti-thyroid peroxidase antibody (A-TPO), thyrotropin receptor antibody (TRAb), and 25-hydroxyvitamin D (25(OH)D). The chemiluminescence immunoassay was used to measure 25(OH)D levels, whereas other indicators were measured using the electrochemiluminescence immunoassay.
-
Chi-squared test, Student's t-test, or Mann-Whitney U test was used to compare the population characteristics, metal(loid) levels, and clinical indicator levels between the case and control groups. Population characteristics that were unevenly distributed between the groups, namely age and BMI, were considered as covariates when investigating the associations between metal(loid) exposure and PCOS risk and in the mediation analysis. Unconditional logistic regression was used to investigate the associations between metal (loid) levels in the FF and PCOS risk. The mediation analysis was conducted using the R package “mediation.” Spearman’s correlation analysis was used for correlation analysis. A P value < 0.05 indicated statistical significance. All statistical analyses were performed using the R software (ver. 4.2.1).
-
The basic population characteristics are presented in Table 1. Information on the participants’ age, BMI, occupation, residence, and education was collected. No significant differences were observed in occupation, residence, or educational level between the PCOS and non-PCOS groups. Most participants were from Shandong Province, China, with only four exceptions, and approximately 80% had an educational level above junior high school. Compared with the non-PCOS group, participants in the PCOS group were younger (90% aged 25–34 years) with a higher BMI (23.7 ± 2.6 kg/m2).
Variables N Controls, n = 896 Cases, n = 200 Pa Age (25–37 years), n (%) 1,096 < 0.001* < 35 710 (79) 181 (90) ≥ 35 186 (21) 19 (10) BMI (kg/m2), mean ± SD 1,096 22.7 ± 2.4 23.7 ± 2.6 < 0.001* Occupation, n (%) 1,096 0.065 Non-workers 756 (84) 158 (79) Workers 140 (16) 42 (21) Residence, n (%) 1,096 > 0.9 Shandong 892 (99.6) 200 (100) Others 4 (0.4) 0 (0) Education, n (%) 1,096 0.664 Bachelor’s degree or above 272 (30) 61 (30) High school, technical secondary school, college, and junior college 450 (50) 108 (54) Junior high school 166 (19) 30 (15) Primary school 8 (1) 1 (1) Note. PCOS, polycystic ovary syndrome; BMI, body mass index; *P < 0.05. aPearson’s chi-squared test or Fisher’s exact test for categorical variables; Student’s t-test for continuous variables. Table 1. Population characteristics of women (with) cases and without PCOS (controls)
-
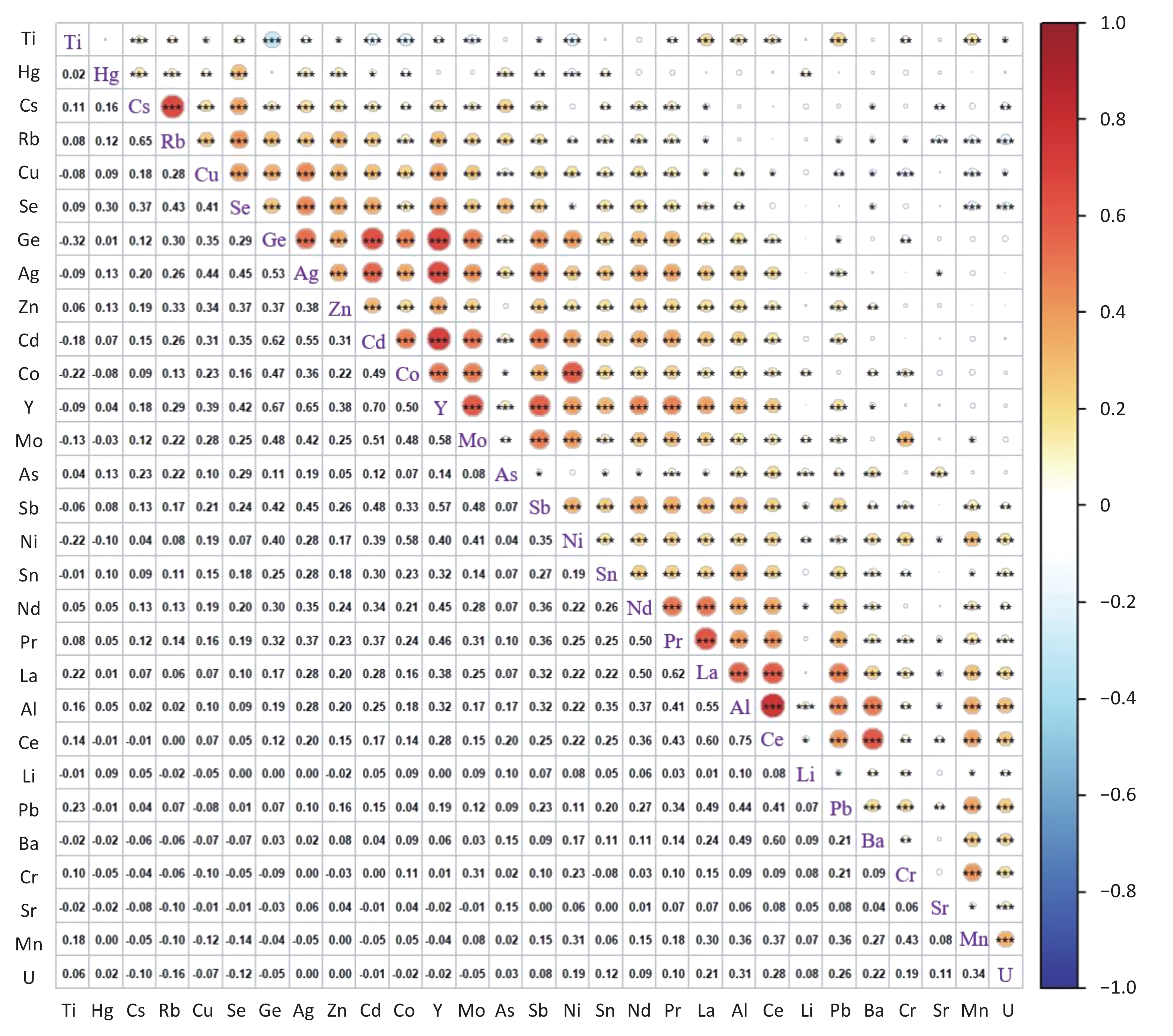
Table 2 lists the FF concentrations of the 29 measured metal(loid)s in the PCOS and non-PCOS groups, and their inter-correlations are depicted in Figure 1 and Supplementary Table S1 (available in www.besjournal.com). The detection rates of most metal(loid)s were approximately 100%, except for As and Li, which were below 80%. Strong positive correlations were observed among the rare earth elements La, Ce, Pr, Nd, and Y, and among the essential trace elements Cu, Zn, and Se, as well as Co, Ni, and Mo. Compared with the non-PCOS group, the PCOS group had higher Cu and Zn, and lower As concentrations.
Metal(loid)sa Detection rate (%) Control, n = 896 (ng/mL) PCOS cases, n = 200 (ng/mL) Pc As 73 1.70 (0.71, 3.03)b 1.52 (0.71, 2.47)b 0.033* Cu 100 789 (678, 905) 904 (764, 1,076) < 0.001* Zn 100 454 (398, 519) 481 (422, 543) < 0.001* Pb 82 0.43 (0.28, 0.73) 0.43 (0.27, 0.68) 0.694 Cd 99 0.40 (0.28, 0.55) 0.42 (0.25, 0.57) 0.817 Hg 82 0.23 (0.16, 0.32) 0.25 (0.16, 0.34) 0.282 Sb 97 0.17 (0.12, 0.22) 0.17 (0.12, 0.22) 0.578 Cr 100 0.79 (0.55, 1.82) 0.71 (0.53, 1.56) 0.133 Mn 100 1.41 (0.98, 2.13) 1.41 (0.98, 2.06) 0.677 Co 100 0.50 (0.35, 0.67) 0.47 (0.33, 0.63) 0.061 Mo 100 2.09 (1.65, 2.59) 2.01 (1.58, 2.54) 0.149 Se 100 54 (46, 63) 55 (47, 64) 0.326 Ge 100 4.18 (3.32, 5.74) 4.18 (3.28, 5.86) 0.624 Ni 100 3.64 (2.70, 5.14) 3.65 (2.68, 4.87) 0.842 Sn 96 0.39 (0.28, 0.54) 0.41 (0.27, 0.55) 0.635 Al 100 25 (19, 32) 25 (18, 32) 0.618 Ti 99 3.31 (2.39, 4.27) 3.21 (2.17, 4.40) 0.295 Li 68 0.67 (0.38, 0.90) 0.66 (0.38, 0.89) 0.601 Cs 100 0.66 (0.52, 0.82) 0.64 (0.53, 0.77) 0.348 Rb 100 140 (122, 156) 137 (120, 154) 0.275 Ag 99 0.27 (0.20, 0.35) 0.27 (0.20, 0.36) 0.739 U 85 0.008 (0.005, 0.012) 0.008 (0.005, 0.012) 0.244 Sr 100 41 (35, 47) 40 (35, 47) 0.691 Ba 100 4.54 (2.49, 7.12) 4.93 (2.47, 7.16) 0.980 La 96 0.04 (0.03, 0.06) 0.04 (0.03, 0.06) 0.786 Ce 100 0.09 (0.06, 0.12) 0.09 (0.06, 0.12) 0.662 Pr 100 0.02 (0.01, 0.03) 0.02 (0.01, 0.03) 0.665 Nd 82 0.11 (0.07, 0.15) 0.11 (0.08, 0.16) 0.348 Y 99 0.20 (0.13, 0.29) 0.21 (0.12, 0.28) 0.613 Note. Data were represented as median (Q25, Q75). PCOS, polycystic ovary syndrome; *P < 0.05. aAs, arsenic; Cu, copper; Zn, zinc; Pb, lead; Cd, cadmium; Hg, mercury; Sb, antimony; Cr, chromium; Mn, manganese; Co, cobalt; Mo, molybdenum; Se, selenium; Ge, germanium; Ni, nickel; Sn, tin; Al, aluminum; Ti, titanium; Li, lithium; Cs, cesium; Rb, rubidium; Ag, silver; U, uranium; Sr, strontium; Ba, barium; La, lanthanum; Ce, cerium; Pr, praseodymium; Nd, neodymium; Y, yttrium. bMedian (interquartile range). cMann-Whitney U test. Table 2. Metal(loid) levels in follicular fluid of PCOS case and non-PCOS control groups
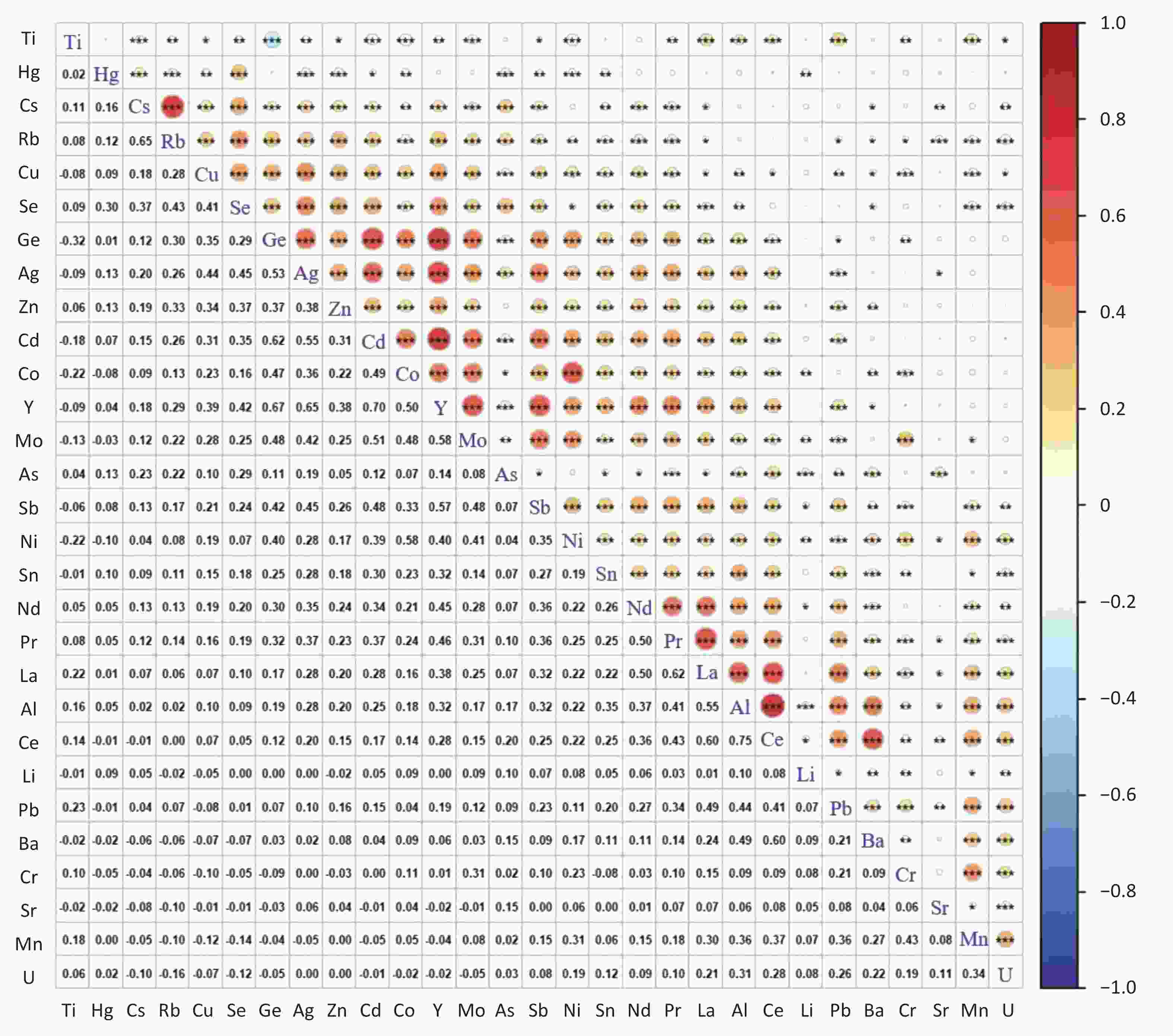
Figure 1. Correlation coefficients among 29 metal(loid)s analyzed in the follicular fluid. ***P < 0.001; **P < 0.01; *P < 0.05; Ti, titanium; Hg, mercury; Cs, cesium; Rb, rubidium; Cu, copper; Se, selenium; Ge, germanium; Ag, silver; Zn, zinc; Cd, cadmium; Co, cobalt; Y, yttrium; Mo, molybdenum; As, arsenic; Sb, antimony; Ni, nickel; Sn, tin; Nd, neodymium; Pr, praseodymium; La, lanthanum; Al, aluminum; Ce, cerium; Li, lithium; Pb, lead; Ba, barium; Cr, chromium; Sr, strontium; Mn, manganese; U, uranium.
-
The serum levels of clinical indicators in the PCOS and non-PCOS groups were also analyzed, including basic sex hormones, thyroid-related indicators, 25(OH)D, and AMH (Table 3). The median serum AMH concentration was approximately two-fold higher in the PCOS group than in the non-PCOS group. Higher serum concentrations of LH, T, and E2 and lower serum concentrations of progesterone, FSH, and PRL were detected in PCOS patients. In terms of thyroid-related indicator and 25(OH)D levels, only TSH levels differed significantly between the PCOS and non-PCOS groups.
Clinical indicatorsa Control PCOS cases Pb Median (IQR) n Median (IQR) n AMH (ng/mL) 3.4 (2.2, 4.9) 892 8.0 (5.5, 13.4) 199 < 0.001* E2 (pg/mL) 35 (27, 45) 896 37 (30, 47) 200 0.035* LH (mIU/mL) 5.1 (3.9, 6.5) 896 7.9 (5.7, 11.9) 200 < 0.001* FSH (mIU/mL) 6.7 (5.8, 7.8) 896 5.9 (5.2, 6.9) 200 < 0.001* T (ng/mL) 0.24 (0.17, 0.33) 894 0.39 (0.26, 0.50) 199 < 0.001* P (ng/mL) 0.39 (0.28, 0.52) 895 0.33 (0.23, 0.43) 200 < 0.001* PRL (ng/mL) 18 (14, 24) 893 16 (13, 21) 199 0.004* TSH (mIU/L) 2.0 (1.5, 2.7) 895 2.2 (1.7, 3.0) 200 0.006* FT4 (pmol/L) 16 (15, 18) 896 17 (15, 18) 200 0.869 FT3 (pmol/L) 4.9 (4.5, 5.2) 895 4.9 (4.5, 5.3) 200 0.151 TG-Ab (IU/mL) 12 (7, 19) 873 11 (7, 16) 196 0.398 A-TPO (IU/mL) 15 (10, 21) 875 14 (10, 19) 195 0.175 TRAb (IU/L) 0.21 (0.21, 0.58) 861 0.32 (0.21, 0.61) 191 0.120 25(OH)D (ng/mL) 14 (11, 19) 887 15 (11, 19) 197 0.683 Note. PCOS, polycystic ovary syndrome; IQR, interquartile range; *P < 0.05. aAMH, anti-Müllerian hormone; E2, estradiol; LH, luteinizing hormone; FSH, follicle-stimulating hormone; T, testosterone; P, progesterone; PRL, prolactin; TSH, thyroid-stimulating hormone; FT4, free thyroxine; FT3, free triiodothyronine; TG-Ab, anti-thyroglobulin antibody; A-TPO, anti-thyroid peroxidase antibody; TRAb, thyrotropin receptor antibody; 25(OH)D, 25-hydroxyvitamin D. bMann-Whitney U test. Table 3. Serum levels of clinical indicators in the PCOS case and non-PCOS control groups
-
Table 4 presents the associations between FF metal(loid) concentrations and PCOS risk. When the FF metal(loid) concentrations were classified into two levels, Cu concentrations [adjusted odds ratio (aOR) = 2.17, 95% confidence interval (CI): 1.53–3.07] and Zn concentrations [aOR = 1.51 (95% CI: 1.09–2.08)] had significant associations with PCOS risk after adjusting for age and BMI. When further classified into four levels, significant positive associations were still observed between Cu levels and PCOS risk, and between Zn levels and PCOS risk. Compared with women in the lowest quartile of the Cu group, the PCOS risk increased among women in the highest quartile [Q4 vs. Q1, aOR = 2.94 (95% CI: 1.83–4.72)]. Higher likelihoods of PCOS were also observed among women in high exposure group of Zn, and the aORs were 1.72 (Q3 vs. Q1, 95% CI: 1.07–2.76) and 1.89 (Q4 vs. Q1, 95% CI: 1.18–3.03). A negative association was observed between PCOS risk and As concentrations at the highest quartile [Q4 vs. Q1, aOR = 0.55 (95% CI: 0.34–0.89)]. The association of PCOS risk with Cu (two-level classification) and the association of PCOS risk with Cu and As (four-level classification) were still observed in the multi-metal(loid) logistic regression models.
Metal(loid)s Model 1c Model 2d Model 3e aOR (95% CI) P aOR (95% CI) P aOR (95% CI) P Cua Low Ref Ref Ref Ref Ref Ref High 2.17 (1.53–3.07) < 0.001* 2.04 (1.42–2.91) < 0.001* 2.17 (1.53–3.07) < 0.001* Zna Low Ref Ref Ref Ref High 1.51 (1.09–2.08) 0.013* 1.28 (0.91–1.78) 0.152 Cub Q1 Ref Ref Ref Ref Ref Ref Q2 1.04 (0.59–1.81) 0.901 1.01 (0.57–1.77) 0.976 1.09 (0.62–1.90) 0.764 Q3 1.45 (0.86–2.44) 0.163 1.43 (0.83-2.45) 0.195 1.55 (0.92-2.62) 0.103 Q4 2.94 (1.83–4.72) < 0.001* 2.86 (1.73–4.73) < 0.001* 3.14 (1.95–5.08) < 0.001* Znb Q1 Ref Ref Ref Ref Q2 1.40 (0.85–2.30) 0.188 1.26 (0.75–2.11) 0.377 Q3 1.72 (1.07–2.76) 0.026* 1.38 (0.83–2.28) 0.212 Q4 1.89 (1.18–3.03) 0.008* 1.47 (0.88–2.45) 0.138 As b Q1 Ref Ref Ref Ref Ref Ref Q2 0.76 (0.50–1.18) 0.225 0.70 (0.45–1.10) 0.118 0.71 (0.45–1.10) 0.125 Q3 0.99 (0.66–1.48) 0.955 0.91 (0.60–1.39) 0.667 0.87 (0.57–1.32) 0.514 Q4 0.55 (0.34–0.89) 0.014* 0.49 (0.30–0.80) 0.005* 0.49 (0.30–0.80) 0.004* Tib Q1 Ref Ref Ref Ref Q2 0.71 (0.46–1.10) 0.128 0.83 (0.53–1.30) 0.408 Q3 0.61 (0.39–0.95) 0.029* 0.72 (0.45–1.15) 0.164 Q4 0.85 (0.56–1.29) 0.457 1.01 (0.65–1.58) 0.959 Lab Q1 Ref Ref Ref Ref Q2 0.62 (0.39–0.97) 0.037* 0.51 (0.32–0.82) 0.005* Q3 0.76 (0.49–1.17) 0.209 0.66 (0.42–1.04) 0.070 Q4 0.79 (0.52–1.21) 0.281 0.70 (0.44–1.11) 0.135 Note. PCOS, polycystic ovary syndrome; Cu, copper; Zn, zinc; As, arsenic; Ti, titanium; La, lanthanum; aOR, adjusted odds ratio; CI, confidence interval; BMI, body mass index; *P < 0.05. aMetal(loid)s were divided into two levels (low and high) based on the medians of the control group. bMetal(loid)s were divided into four levels (Q1, Q2, Q3, and Q4) based on the quartiles of the control group. cModel 1: single-metal(loid) logistic regression model, adjusted for age and BMI. dModel 2: multi-metal(loid) logistic regression model, adjusted for age and BMI; 1) two-level, Cu and Zn were included; 2) four-level, Cu, Zn, As, Ti, and La were included. eModel 3: multi-metal(loid) logistic regression model with the stepwise method; 1) two -level, Cu and Zn were included, with Cu kept in the model, adjusted for age and BMI; 2) four-level, Cu, Zn, As, Ti, and La were included, with Cu and As kept in the model, adjusted for age and BMI. Table 4. Associations between metal(loid) levels and PCOS risk
-
Supplementary Table S2 (available in www.besjournal.com) presents the correlations between the clinical indicators and FF Cu levels. Serum levels of AMH, LH, and T, which were higher in the PCOS group, also showed significant (P < 0.001) positive correlations with FF Cu levels. A significant (P < 0.001) negative correlation was observed between serum FSH and FF Cu levels, with serum FSH levels also lower in the PCOS group, as previously noted. These findings suggest the possible roles of AMH, LH, FSH, and T in the association between Cu exposure and PCOS risk.
Clinical indicators r P N AMH 0.211 < 0.001 1,091 LH 0.119 < 0.001 1,096 FSH −0.133 < 0.001 1,096 T 0.131 < 0.001 1,093 FT3 0.063 0.038 1,095 Note. AMH, anti-Müllerian hormone; LH, luteinizing hormone; FSH, follicle-stimulating hormone; T, testosterone; FT3, free triiodothyronine; r, correlation coefficient; P, P-value; N, sample size. Table S2. Spearman correlations between copper levels in follicular fluid and clinical indicators
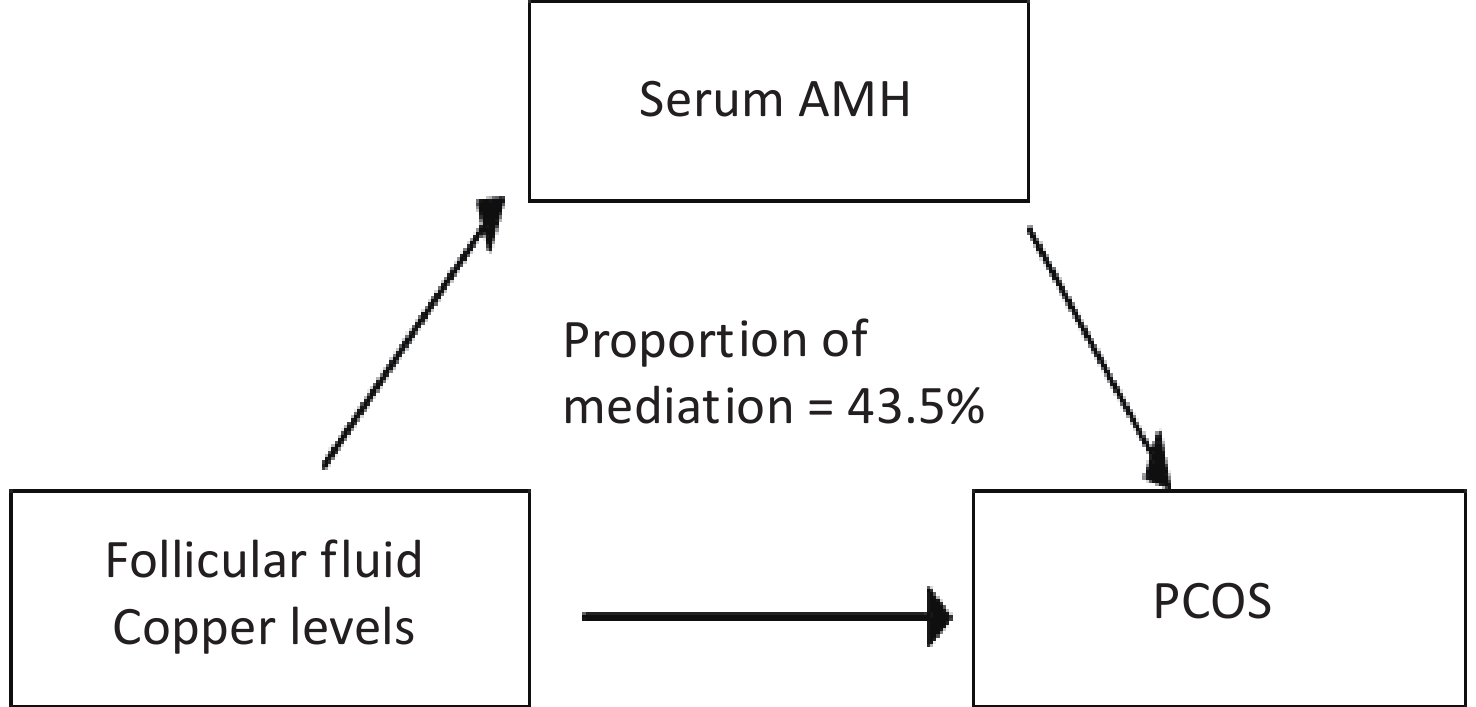
Serum AMH levels were negatively correlated (r = –0.268, P < 0.001) with FSH levels and positively correlated (P < 0.001) with LH (r = 0.390) and T (r = 0.329) levels. Mediation analysis indicated that AMH may act as a mediator in the relationship between Cu exposure and PCOS risk (Figure 2 and Supplementary Table S3, available in www.besjournal.com).
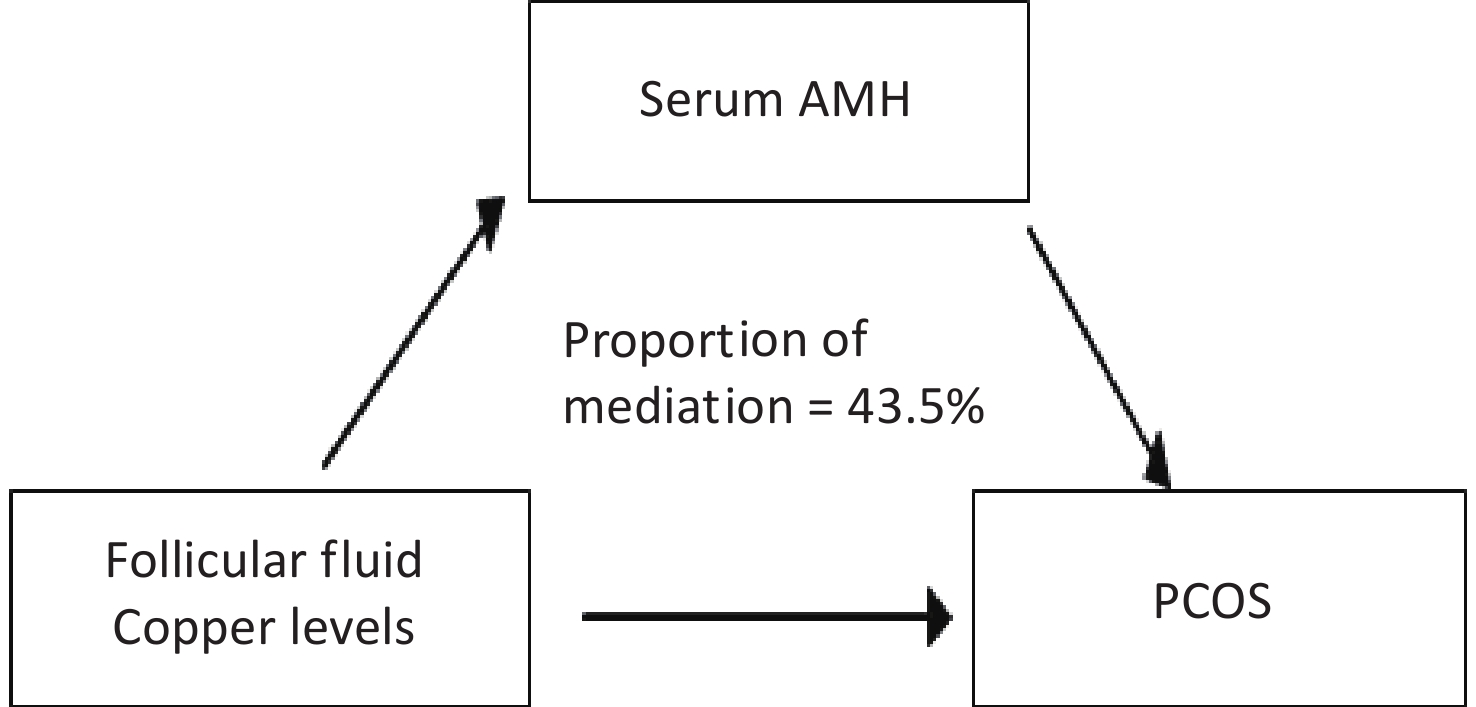
Figure 2. Mediation effect of anti-Müllerian hormone (AMH) in the association between copper levels in follicular fluid and polycystic ovary syndrome (PCOS) risk, adjusted by age and body mass index.
-
Several studies have analyzed the concentrations of metal(loid)s, particularly Cu and Zn, in the serum or FF of PCOS patients and controls (Supplementary Table S4, available in www.besjournal.com). Serum concentrations were included in this comparison, as limited information is available regarding metal(loid) levels in the FF of PCOS patients. The FF metal(loid) levels measured in the present study were generally consistent with those observed in previous studies; however, the As, Ti, and Cr levels varied among studies[16]. For example, the median FF Cu level in PCOS patients in the present study was 904 ng/mL, comparable to 1,065 ± 244 ng/mL in a southeastern Chinese population. In addition, the median FF As level in PCOS patients in the present study was 1.52 ng/mL, which is lower than the levels observed in the southeastern Chinese population (36 ± 9 ng/mL). The serum metal(loid) concentrations of other populations are in the same order of magnitude, although slightly higher than those in FF of the present study[17,18]. For instance, serum Cu levels in PCOS patients from Beijing and Iran were 1,480 ± 55 ng/mL and 2,060 ng/mL, respectively.
References Regions Mediaa Groupsb Metal(loid)sc, ng/mL Cu Cr Se Zn Mn Pb Hg As Ti Li Sr Mo (Sun et al., 2019)[3] Fujian
ChinaFF Control 920.91 ±
305.89124.09 ±
86.7685.98 ± 22.34 479.69 ±
218.9237.64 ±
9.39200.07 ±
84.852.78 ±
0.6732.15 ±
13.051.10 ±
1.05PCOS 1,064.53 ±
243.75133.37 ±
41.9091.27 ± 20.75 527.77 ±
236.7035.98 ±
9.36164.83 ±
49.772.75 ±
0.5234.01 ±
12.381.71 ±
3.13FTO 877.98 ±
239.7397.75 ±
53.0980.13 ± 19.70 506.83 ±
278.3033.72 ±
9.50216.99 ±
101.992.24 ±
0.5628.05 ±
9.761.22 ±
1.94(Schmalbrock
et al., 2021) [4]Dobl
AustriaFF 1 Subfertile 555 ± 191 23 ± 10 474 ± 118 PCOS 518 ± 267 19 ± 11 402 ± 164 2 Subfertile 683 ± 289 31 ± 26 569 ± 144 PCOS 682 ± 381 24 ± 11 572 ± 231 3 Subfertile 516 ± 185 24 ± 14 571 ± 111 PCOS 479 ± 179 22 ± 5 419 ± 142 4 Subfertile 619 ± 176 26 ± 11 536 ± 170 PCOS 652 ± 276 24 ± 11 467 ± 174 5 Subfertile 507 ± 190 22 ± 11 503 ± 167 PCOS 742 ± 318 27 ± 12 591 ± 220 (Li et al., 2017) [5] Guangxi
ChinaSerum Control 1,152 (992−
1,400)PCOS 1,273 (1,078−
1,536)(Zhang et al., 2022)[6] Beijing
ChinaSerum Control 1,320 ± 40 1.19 (0.708−
2.07)80.06 ± 2.52 860
(750−1,010)3.45
(2.37−
5.64)2.49
(1.30−
6.20)0.104
(0.104−
0.104)PCOS 1,480 ± 55 2.58 (1.01−
9.31)77.31 ± 2.01 805
(665−1,120)3.31
(2.10−
7.82)2.31
(1.14−
8.47)0.350
(0.104−
0.633)(Kanafchian
et al., 2020) [7]Babol
IranSerum Control 1,870 (1,540−
2,140)PCOS 2,060 (1,790−
2,480)Note. Data was presented as mean ± standard deviation or median (interquartile range). a FF, follicular fluid. b PCOS, polycystic ovary syndrome; FTO, fallopian tube obstruction. c Cu, copper; Cr, chromium; Se, selenium; Zn, zinc; Mn, manganese; Pb, lead; Hg, mercury; As, arsenic; Ti, titanium; Li, lithium; Sr, strontium; Mo, molybdenum. Table S4. Metal(loid) levels in follicular fluid or serum of women from other populations
Consistent with the present study, previous studies also observed higher Cu levels in the FF or serum of PCOS patients than in controls[16,18]. For example, serum levels of Cr, Hg, and Cu were higher in PCOS patients (N = 40) than in controls (N = 40) in a study carried out in Beijing, China[18]. In addition, among 22 trace elements measured in the FF of 89 PCOS patients and 114 controls from southeastern China, Cu levels were relatively high in the PCOS group[16]. Regarding Zn levels, Kurdoglu et al. also reported higher serum Zn levels in PCOS patients than in controls, consistent with the present study[19]. However, similar or lower Zn levels in the serum of PCOS patients were also observed in other studies[18,20].
Higher serum AMH concentrations were observed in the PCOS group in this study, which is consistent with previous studies[21,22]. Regarding E2, LH, FSH, T, PRL, and progesterone, the trends were mostly consistent with a study conducted among Chinese women in a reproductive center in eastern China, except that the previous study found no difference in serum PRL levels between the PCOS and control groups[4].
It is difficult to explain the protective role of As exposure currently, and more research into the association is needed. Therefore, the present study focused on the association between Cu exposure and PCOS risk. Logistic regression analysis indicated high exposure to Cu as a potential risk factor for PCOS, which is consistent with the findings from a meta-analysis[23]. Cu is a cofactor for several enzymes and an electron transporter, and is involved in biological redox reactions. Both the deficiency and excess of Cu may induce the deregulation of oxidative stress, which may be an inducing factor in the pathogenesis of PCOS[23-25]. Additionally, Cu overexposure may negatively affect follicular maturation. In yellow catfish (Pelteobagrus fulvidraco), the development of the ovary and secretion of related hormones were affected by Cu exposure[26]. Long-term and higher waterborne Cu exposure induced inhibitory effects both on the expression of proteins involved in ovarian development and the secretion of reproductive hormones.
Several clinical indicators (i.e., hormone levels) were measured, and their potential involvement in the relationship between Cu exposure and PCOS risk was investigated in the present study to elucidate the underlying mechanisms. In this study, positive correlations of serum LH and T levels, and a negative correlation of serum FSH levels with FF Cu levels were observed. Cu can act directly on the pituitary, affecting LH release, and indirectly impact the release of LH and FSH by influencing the release of gonadotropin-releasing hormone (GnRH) in the hypothalamus[27,28]. In addition, the Cu-GnRH complex can bind to GnRH receptors, stimulating the release of FSH and LH in the pituitary. Compared with native GnRH, the Cu-GnRH complex is even a more potent stimulator of FSH and LH[28]. As demonstrated in in vivo experiments, increased release of LH and FSH was induced by complexes of Cu with GnRH[27,29]. However, higher Cu levels in FF correlated with lower serum FSH levels in the present study. This suggests that other pathways may be involved in the action of Cu on the HPO axis.
Serum AMH levels were positively correlated with FF Cu levels and PCOS risk. Mediation analysis indicated that AMH may mediate the relationship between Cu exposure and PCOS risk. Circulating AMH levels in women fluctuate slightly but not significantly during the menstrual cycle[30]. AMH may regulate the HPO axis by acting on GnRH neurons and further increasing LH pulsatility and secretion[31]. Androgens may accumulate because of the inhibition of aromatase expression and activity by elevated AMH levels, which can block the conversion of androgens to estrogens[1,12]. In addition, follicular sensitivity to FSH may be inhibited by elevated AMH levels[32]. The possible enhancement of the circulating LH/FSH ratio, androgen excess, and decreased FSH sensitivity induced by AMH elevation cause disturbances in follicular development and anovulation, promoting the development of PCOS[1,33]. Therefore, higher Cu exposure may induce an increase in the LH/FSH ratio and T levels via elevated AMH levels, thereby enhancing the risk of PCOS.
This study had certain limitations. First, genetic factors were not included in this study, which should be considered in future. In addition, this study did not investigate Cu exposure routes in participants, and substances co-exposed with Cu might have contributed to potential bias. Despite these limitations, the study had several advantages. First, the inclusion of a large sample size made it possible to demonstrate the relatively weak association between Cu exposure and PCOS risk. Second, the metal(loid) concentrations in this study were measured using FF samples, which is more representative of the ovarian exposure levels in women of childbearing age. Third, AMH mediated the relationship between Cu exposure and PCOS risk, providing a new perspective for understanding the pathogenesis of PCOS. The results of this study highlight elevated Cu levels as a possible risk factor for PCOS and the potential role of AMH in contributing to PCOS. Therefore, simultaneous monitoring of internal levels of Cu and AMH in women of childbearing age may facilitate early detection of PCOS, especially among susceptible populations.
-
The authors have no actual or potential competing financial interests to declare.
HTML
Study Population
Metal(loid) Analysis
Clinical Indicator Analysis
Statistical Analysis
Population Characteristics
Metal(loid) Levels in FF
Clinical Indicator Levels in Serum
Associations between FF Metal(loid) Levels and PCOS Risk
Correlations between FF Cu and Clinical Indicator Levels
 24005+Supplementary Materials.pdf
24005+Supplementary Materials.pdf
|

|

 Quick Links
Quick Links
 DownLoad:
DownLoad: