
-
Rapid population aging has led to an increased focus on age-related conditions such as sarcopenia. causing loss of muscle mass and strength[1,2]. Sarcopenia is associated with adverse outcomes, including falls, functional decline, frailty, and mortality, which can lower the quality of life and shorten lifespan[1,2]. The prevalence of sarcopenia shows considerable variation owing to differences in ethnicity, nationality, country, and diagnostic criteria[2]. Moreover, existing research has primarily concentrated on urban areas, particularly among nursing homes and hospital populations[3]. However, evidence of sarcopenia in rural areas is limited. Therefore, there is an urgent need to explore the epidemiology of sarcopenia and its risk factors even among the rural populations in addition to existing studies in urban areas to provide a comprehensive understanding for its early prevention and treatment.
Environmental pollution is a major risk factor for adverse health outcomes, including sarcopenia[4]. Lai et al. found that outdoor air pollution is associated with probable sarcopenia and its components[5]. In China, from 2013 to 2017, outdoor air pollution was relatively well-controlled owing to the implementation of the clean air policy; however, household air pollution (HAP) has received less attention. The incomplete combustion of solid fuel is a major source of HAP, and indoor ventilation is typically poor in low- and middle-income countries. Thus, HAP exposure is often evaluated based on the cooking fuel type and kitchen ventilation status. Lai et al. also found that solid fuel use was associated with probable sarcopenia, while kitchen ventilation did not exhibit any association. In addition, a recent Chinese study found that solid fuel use was associated with a higher risk of sarcopenia[6]. However, the effect of kitchen ventilation on sarcopenia remains unclear, although it could potentially influence the concentration of air pollutants related to cooking fuel use. Thus, this study aimed to (1) explore the individual and combined associations of cooking fuel type and kitchen ventilation status with sarcopenia and (2) determine whether kitchen ventilation could attenuate the association of solid fuel use with sarcopenia in rural populations, utilizing baseline and first follow-up data from the Henan Rural Cohort Study.
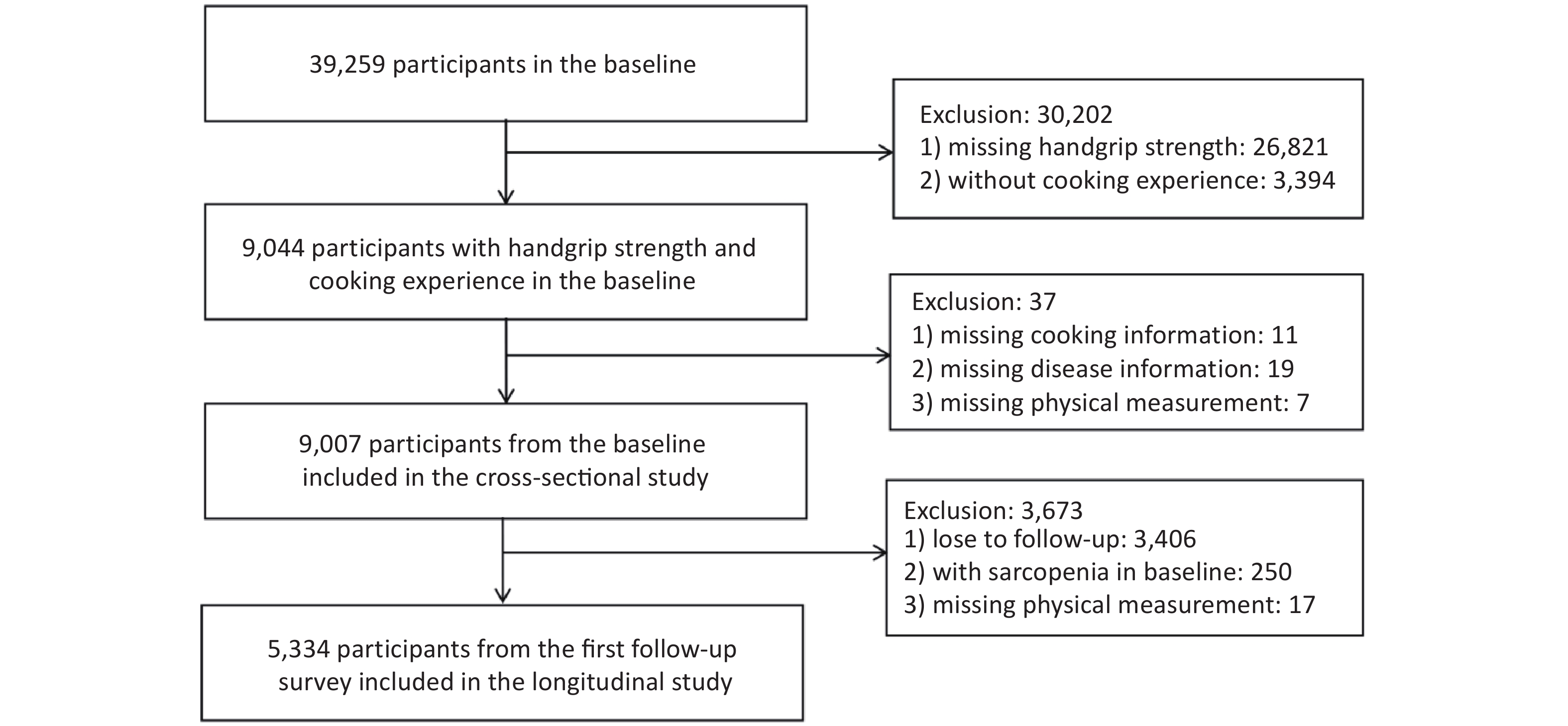
Study participants were recruited from the Henan Rural Cohort Study, which was conducted in five counties in the Henan Province, China. The baseline study was completed between 2015 and 2017, and the first follow-up was completed between 2018 and 2022. Detailed information regarding the study is provided elsewhere[7,8]. In total, 9,007 and 5,334 participants were included in the cross-sectional and longitudinal analyses, respectively. A flow chart illustrating the process of recruitment of participants is shown in Supplementary Figure S1.
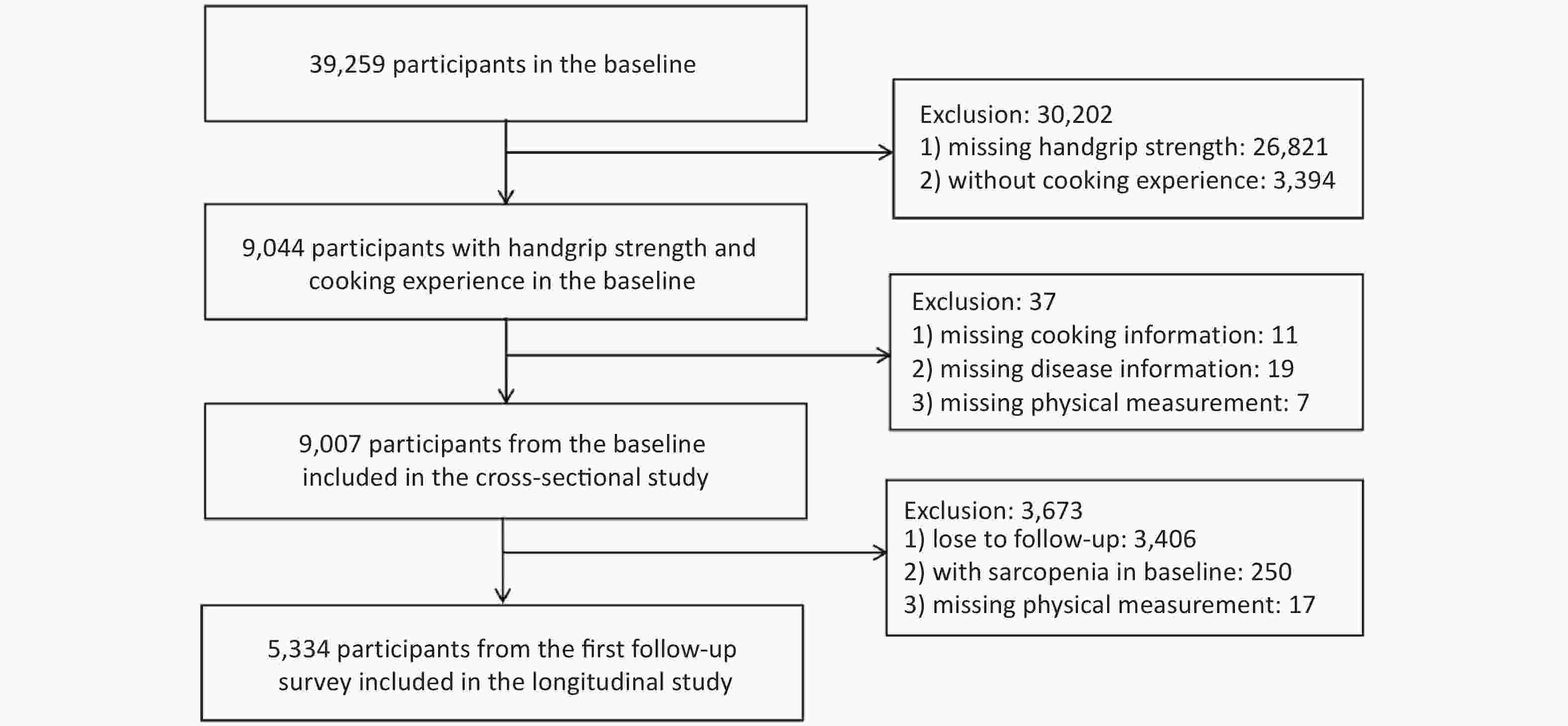
Figure S1. Flow chart of participants including in cross-sectional and longitudinal study.
Household air pollution was defined through questions on cooking fuel type and kitchen ventilation status. Participants responded to “Which type of fuel do you use most often for cooking?” and “Which type of kitchen ventilation do you use most frequently?”. Fuel types were divided into solid and clean fuels. Solid fuel consisted of coal and wood, whereas liquefied gas, natural gas, and electricity were classified as clean fuel. Kitchen ventilation status was classified as natural and mechanical ventilations (including exhaust hoods or fans). Information on daily cooking duration (hours/day) was collected through a questionnaire. According to the updated definition and diagnosis of Asian Working Group for Sarcopenia, sarcopenia is defined as low handgrip strength and muscle mass[1,4]. Sarcopenia was defined as a handgrip strength < 28 kg and skeletal muscle mass index (SMI) < 7.185 kg/m2 for men and handgrip strength < 18 kg and skeletal muscle mass index (SMI) < 5.607 kg/m2 for women (detailed definition of sarcopenia is shown in Supplementary Text 1). Based on the data from this study combined with the 2021 China Cause of Death Surveillance dataset, a life expectancy table was prepared, and healthy life expectancy (HLE) was generated using the Sullivan method[9] (detailed calculation methods are shown in Supplementary Text 2). HLE refers to sarcopenia-free life expectancy. Region of residence, sex, age, educational level, marital status, average monthly income, smoking status, drinking status, high-fat diet, adequate vegetable and fruit intake, physical activity, and history of chronic disease (hypertension, type 2 diabetes mellitus, coronary heart disease, and stroke; categorized as yes or no) were collected by well-trained staff via face-to-face interviews.
Characteristics of the participants were described as numbers (percentages) for categorical variables, and mean ± standard deviation for continuous variables. The differences of characteristics in continuous and categorical variables were tested using t- and Chi-square tests, respectively. Binary logistic regression models were used to examine the individual and combined association of cooking fuel type and kitchen ventilation status with sarcopenia based on odds ratios (ORs) and 95% confidence intervals (CIs). The P for interaction for fuel type and kitchen ventilation were calculated by including the product item of fuel type and kitchen ventilation in the regression model. SPSS 21.0 software package (SPSS Institute, Chicago) and R software version 4.2.2 were used for data analysis, and P values were two-tailed with a statistical significance level of 0.05.
The characteristics of the cross-sectional and longitudinal studies are presented in Supplementary Tables S1 and S2, respectively. A total of 9,007 participants were enrolled in the cross-sectional analysis. The prevalence of sarcopenia was 4.13% (372/9,007). The longitudinal analysis included 5,334 participants. During the 3.7-year follow-up duration, 273 individuals were newly diagnosed with sarcopenia, corresponding to an average annual incidence of 1.38%.
Variables No-sarcopnia (n = 8,635) Sarcopenia (n = 372) P Age (years), mean ± SD 56.3 ± 11.0 68.5 ± 8.3 < 0.001 Women, n (%) 6,781 (78.5) 283 (76.1) 0.260 Region, n (%) < 0.001 Suiping 6,151 (95.1) 317 (4.9) Tongxv and Yima 2,484 (97.8) 55 (2.2) Educational level, n (%) < 0.001 Primary school or below 4,588 (53.2) 287 (77.2) Junior high school or above 4,047 (46.8) 85 (22.8) Married/cohabiting, n (%) 7,667 (88.8) 272 (73.1) < 0.001 Per average monthly income (RMB), n (%) < 0.001 < 500 2,946 (34.1) 190 (51.1) 500– 2,595 (30.1) 89 (23.9) 1,000– 3,094 (35.8) 93 (25.0) Current smoking, n (%) 864 (10.0) 41 (11.0) 0.523 Current drinking, n (%) 863 (10.0) 12 (3.2) < 0.001 High-fat diet, n (%) 1,636 (18.9) 44 (11.8) 0.001 Adequate vegetables and fruits intake, n (%) 4,577 (53.0) 166 (44.6) 0.002 Physical activity, n (%) < 0.001 Light 1,552 (18.0) 99 (26.6) Moderate 4,046 (46.9) 170 (45.7) Vigorous 3,037 (35.1) 103 (27.7) Hypertension, n (%) 2,593 (30.0) 99 (26.6) 0.159 Type 2 diabetes mellitus, n (%) 664 (7.7) 19 (5.1) 0.065 Coronary heart diseases, n (%) 536 (6.2) 33 (8.9) 0.039 Stroke, n (%) 639 (7.4) 37 (9.9) 0.068 Solid fuel, n (%) 1,886 (21.8) 161 (43.3) < 0.001 Natural ventilation, n (%) 5,745 (66.5) 308 (82.8) < 0.001 Daily cooking duration (hour/day), mean ± SD 1.4 ± 0.7 1.4 ± 0.7 0.698 Handgrip strength (kg), mean ± SD 28.1 ± 8.0 17.1 ± 4.5 < 0.001 Skeletal muscle mass index (kg/m2), mean ± SD 6.6 ± 1.0 5.5 ± 0.8 < 0.001 Note. RMB. Renminbi; SD: standard deviation. Table S1. Baseline characteristics of participants in the cross-sectional analysis
Variables No-sarcopenia
(n = 5,061)Sarcopenia
(n = 273)P Age (years), mean ± SD 56.5 ± 10.1 66.8 ± 7.8 < 0.001 Women, n (%) 4,041 (79.8) 206 (75.5) 0.080 Region, n (%) < 0.001 Suiping 4,147 (95.6) 193 (4.4) Tongxv and Yima 914 (92.0) 80 (8.0) Educational level, n (%) < 0.001 Primary school or below 2,669 (52.8) 208 (76.2) Junior high school or above 2,392 (47.2) 65 (23.8) Married/cohabiting, n (%) 4,547 (89.8) 220 (80.6) < 0.001 Per average monthly income (RMB), n (%) < 0.001 < 500 1,782 (35.2) 138 (50.5) 500– 1,546 (30.5) 69 (25.3) 1,000– 1,733 (30.5) 66 (24.2) Current smoking, n (%) 465 (9.2) 28 (10.3) 0.553 Current drinking, n (%) 473 (9.3) 15 (5.5) 0.032 High-fat diet, n (%) 952 (18.8) 34 (12.5) 0.008 Adequate vegetables and fruits intake, n (%) 2,975 (58.8) 114 (41.8) < 0.001 Physical activity, n (%) < 0.001 Light 876 (17.3) 78 (28.6) Moderate 2,605 (51.5) 120 (44.0) Vigorous 1,580 (31.2) 75 (27.4) Hypertension, n (%) 1,423 (28.1) 104 (38.1) < 0.001 Type 2 diabetes mellitus, n (%) 359 (7.1) 23 (8.4) 0.406 Coronary heart diseases, n (%) 322 (6.4) 21 (7.7) 0.383 Stroke, n (%) 376 (7.4) 37 (13.6) < 0.001 Solid fuel, n (%) 1,159 (22.9) 107 (39.2) < 0.001 Natural ventilation, n (%) 3,301 (65.2) 215 (78.8) < 0.001 Daily cooking duration (hour/day), mean ± SD 1.5 ± 0.8 1.5 ± 0.8 0.952 Handgrip strength (kg), mean ± SD 28.2 ± 7.7 23.4 ± 5.7 < 0.001 Skeletal muscle mass index (kg/m2), mean ± SD 6.6 ± 0.9 5.7 ± 0.8 < 0.001 Note. RMB. Renminbi; SD: standard deviation. Table S2. Baseline characteristics of participants in the longitudinal analysis
Previous studies have reported an association between air pollution and sarcopenia[5], but the focus was primarily on outdoor air pollution. Lai et al. found that the odds of probable sarcopenia and its components increased with an increase in particulate matter (PM2.5), coarse particles, PM10, PM2.5 absorbance, nitrogen dioxide (NO2), and nitrogen oxides (NOx) in the UK Biobank[5]. While indoor and outdoor air pollutants were comparable, greater time spent indoors and the higher level of indoor pollutants suggest that HAP may impose a greater health burden that outdoor pollutants. Recently, an association among HAP, sarcopenia, and muscle strength has been reported. A Chinese longitudinal study found that solid fuel use for cooking and heating was positively associated with sarcopenia[6]. Both our cross-sectional and longitudinal studies demonstrate that solid fuel use and natural ventilation are associated with a higher risk of sarcopenia in rural adults. The individual associations between cooking fuel type, kitchen ventilation, and sarcopenia are shown in Table 1. In a cross-sectional study, individuals using solid fuel for cooking had a significantly increased risk of sarcopenia (OR = 1.287; 95% CI: 1.019, 1.625) compared with those using clean fuel. Additionally, participants using natural ventilation when cooking had a significantly higher risk of sarcopenia (OR = 1.491; 95% CI: 1.115, 1.993), compared with those using mechanical ventilation. In a longitudinal study, compared to individuals using clean fuel for cooking, those using solid fuel had a 1.343 (95% CI: 1.013, 1.780) times higher risk of sarcopenia after adjusting for multiple covariates. Furthermore, compared to participants using mechanical ventilation during cooking, those using natural ventilation were at a higher risk of developing sarcopenia (OR = 1.313; 95% CI: 0.951, 1.811). Kitchen ventilation plays an important role in the removal of household air pollutants, yet it has been largely ignored in previous studies. To the best of our knowledge, this is the first study to demonstrate that kitchen ventilation is associated with a higher risk of developing sarcopenia.
Variables Prevalence or incidence %
(case/total)OR (95% CI) Model 1 Model 2 Model 3 Cross-sectional study Fuel type Clean fuel 3.03 (211/6,960) Ref. Ref. Ref. Solid fuel 7.87 (161/2,047) 2.730 (2.210, 3.373) 1.641 (1.316, 2.046) 1.287 (1.019, 1.625) Kitchen ventilation Mechanical ventilation 2.17 (64/2,954) Ref. Ref. Ref. Natural ventilation 5.09 (308/6,063) 2.421 (1.843, 3.181) 1.711 (1.293, 2.265) 1.491 (1.115, 1.993) Longitudinal study Fuel type Clean fuel 4.08 (166/4,068) Ref. Ref. Ref. Solid fuel 8.73 (107/1,226) 2.170 (1.687, 2.791) 1.367 (1.050, 1.780) 1.343 (1.013, 1.780) Kitchen ventilation Mechanical ventilation 3.19 (58/1,818) Ref. Ref. Ref. Natural ventilation 6.11 (215/3,516) 1.976 (1.470, 2.656) 1.454 (1.071, 1.974) 1.313 (0.951, 1.811) Note. CI: confidential interval; OR: odds ratio. Model 1: unadjusted; Model 2: adjusted for age and sex; Model 3: adjusted for age, sex, educational level, marital status, average monthly income, smoking status, drinking status, high-fat diet, adequate vegetable and fruit intake, physical activity, history of chronic diseases (hypertension, type 2 diabetes mellitus, coronary heart disease, and stroke), region, daily cooking duration, cooking fuel type, and kitchen ventilation. Table 1. Individual association of household air pollution with sarcopenia
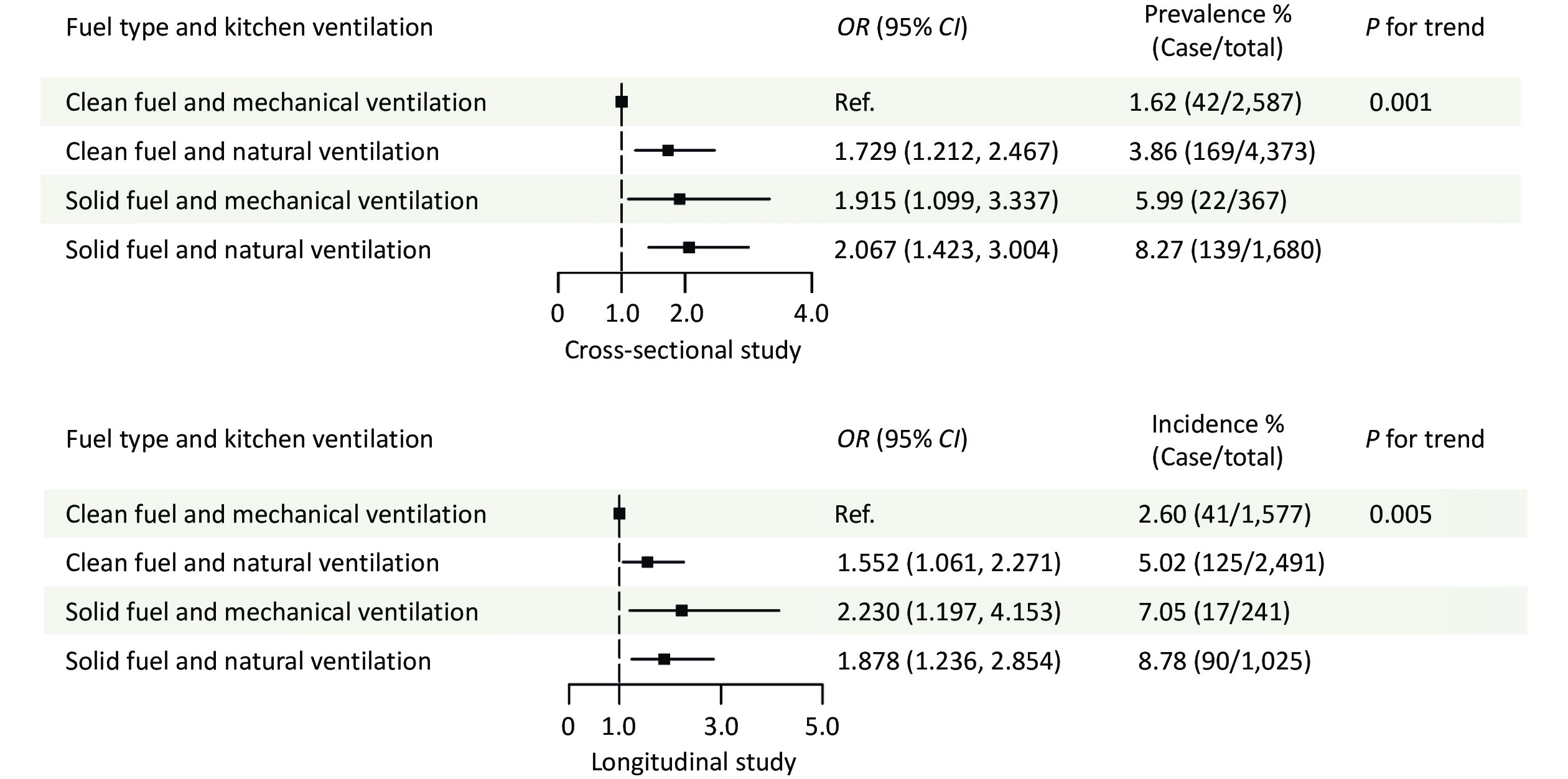
Individuals who used both solid fuel and natural ventilation had a higher risk of sarcopenia than those who used solid fuel or natural ventilation alone. Moreover, this study found that mechanical ventilation could attenuate the association between solid fuel use and sarcopenia, providing an effective method for preventing sarcopenia in resource-limited distractions. In the cross-sectional study, compared with individuals using clean fuel and mechanical ventilation, the ORs (95% CIs) of those using clean fuel and natural ventilation, solid fuel and mechanical ventilation, and solid fuel and natural ventilation were 1.729 (1.212, 2.467), 1.915 (1.099, 3.337), and 2.067 (1.423, 3.004), respectively (Figure 1). Among individuals using solid fuel, those using natural ventilation had a higher risk of sarcopenia (OR = 1.872, 95% CI: 1.314, 2.668) compared with those using mechanical ventilation (Table 2). In the longitudinal study, the estimates and 95% CI of individuals using clean fuel and natural ventilation, solid fuel and mechanical ventilation, and solid fuel and natural ventilation were 1.552 (1.061, 2.271), 2.230 (1.197, 4.153), and 1.878 (1.236, 2.854), compared with those using clean fuel and mechanical ventilation, respectively (Figure 1). Among the participants using mechanical ventilation, those using solid fuel, had a higher risk of sarcopenia (OR = 2.539, 95% CI: 1.292–4.991) than those using clean fuel. Moreover, among individuals using solid fuel individuals using natural ventilation had a higher risk of sarcopenia (OR = 1.608, 95% CI: 1.105–2.339) than those using mechanical ventilation (Table 2). These findings provide an effective method for preventing sarcopenia in resource-limited districts, where changing energy sources is challenging.
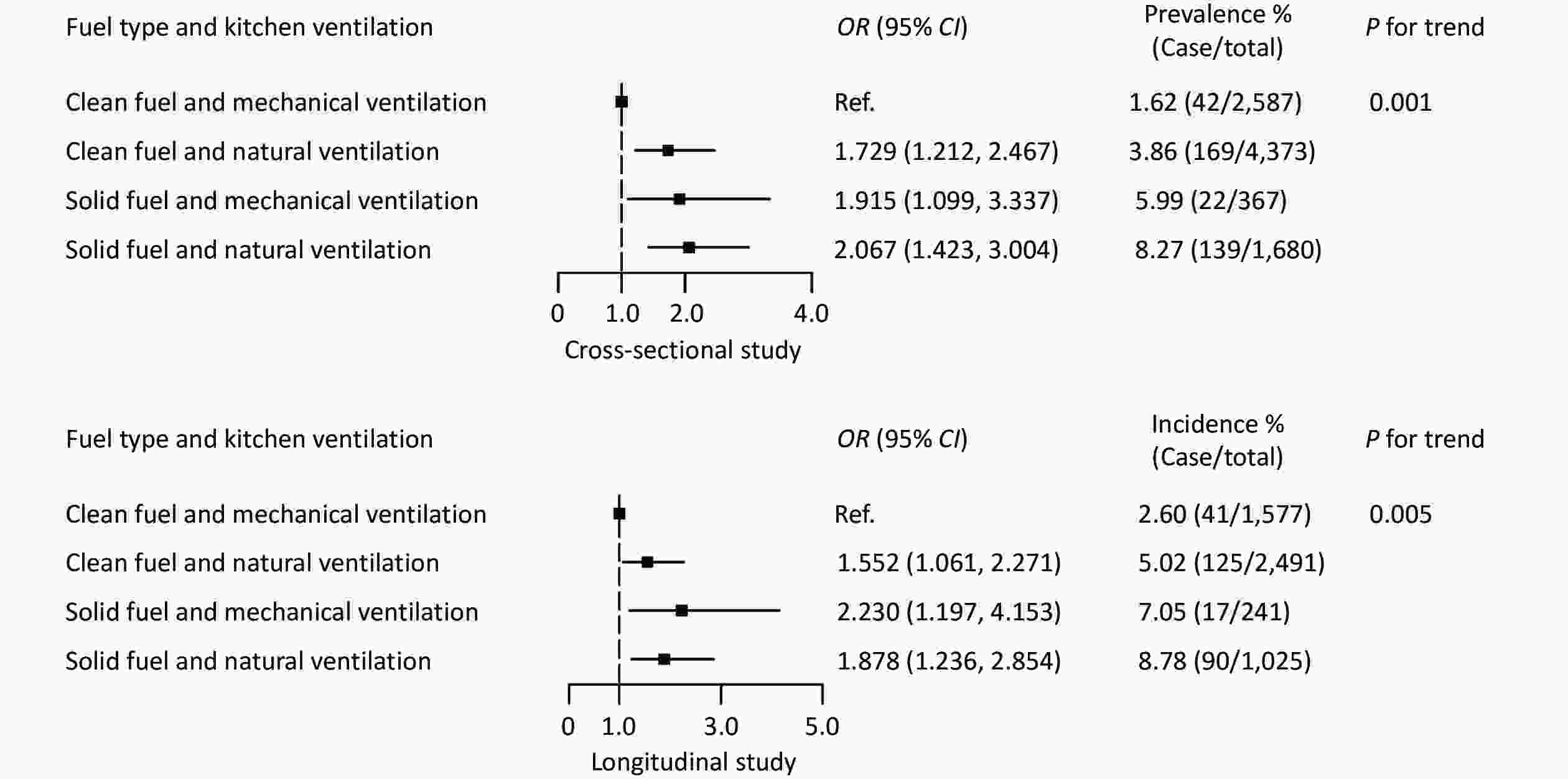
Figure 1. The combined association of household air pollution with sarcopenia. All estimates were adjusted for age, sex, education level, marital status, monthly income, smoking status, drinking status, high-fat diet, adequate vegetable and fruit intake, physical activity, history of chronic diseases (hypertension, type 2 diabetes mellitus, coronary heart disease, and stroke), region of residence, and daily cooking duration.
Fuel type Prevalence or incidence %
(case/total)OR (95% CI) P for interaction Cross-sectional study 0.126 Solid fuel Mechanical ventilation 5.99 (22/367) Ref. Natural ventilation 8.27 (139/1,680) 1.872 (1.314, 2.668) Clean fuel Mechanical ventilation 1.62 (42/2,587) Ref. Natural ventilation 3.86 (169/4,373) 1.126 (0.687, 1.844) Longitudinal study 0.079 Solid fuel Mechanical ventilation 7.05 (17/241) Ref. Natural ventilation 8.78 (90/1,025) 1.608 (1.105, 2.339) Clean fuel Mechanical ventilation 2.60 (41/1,577) Ref. Natural ventilation 5.02 (125/2,491) 0.829 (0.461, 1.491) Note. CI: confidential interval; OR: odds ratio. All estimates were adjusted for age, sex, education level, marital status, monthly income, smoking status, drinking status, high-fat diet, adequate vegetable and fruit intake, physical activity, history of chronic diseases (hypertension, type 2 diabetes mellitus, coronary heart disease, and stroke), region of residence, and daily cooking duration. Table 2. Interaction effect of household air pollution with sarcopenia
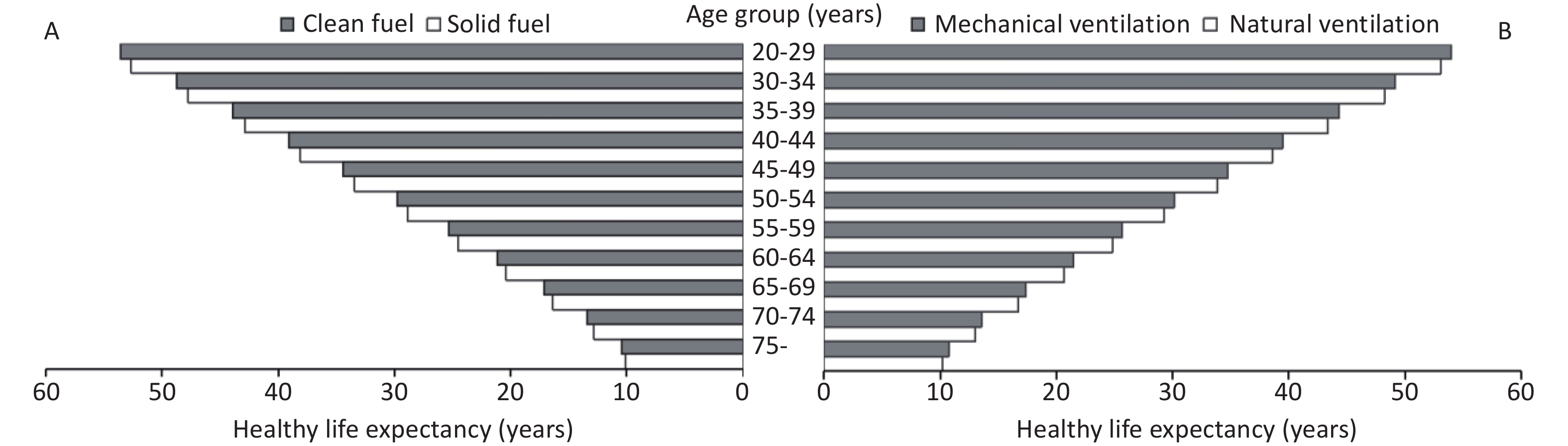
Healthy life expectancy in the context of sarcopenia was lower among participants using solid fuel and natural ventilation than among those using clean fuel and mechanical ventilation. Supplementary Figure S2 shows the HLE of the participants according to the cooking fuel type and kitchen ventilation status. HLE at age 20–29 for individuals using solid fuel vs. clean fuel and natural ventilation vs. mechanical ventilation was 52.64 vs. 53.59 and 53.04 vs. 53.96 years, respectively. Across all age groups, participants using clean fuel or mechanical ventilation had a higher HLE than those using solid fuel or natural ventilation. These results suggest that clean fuel and mechanical ventilation could increase the HLE by reducing the risk of sarcopenia, thereby providing a better quality of life for rural adults.
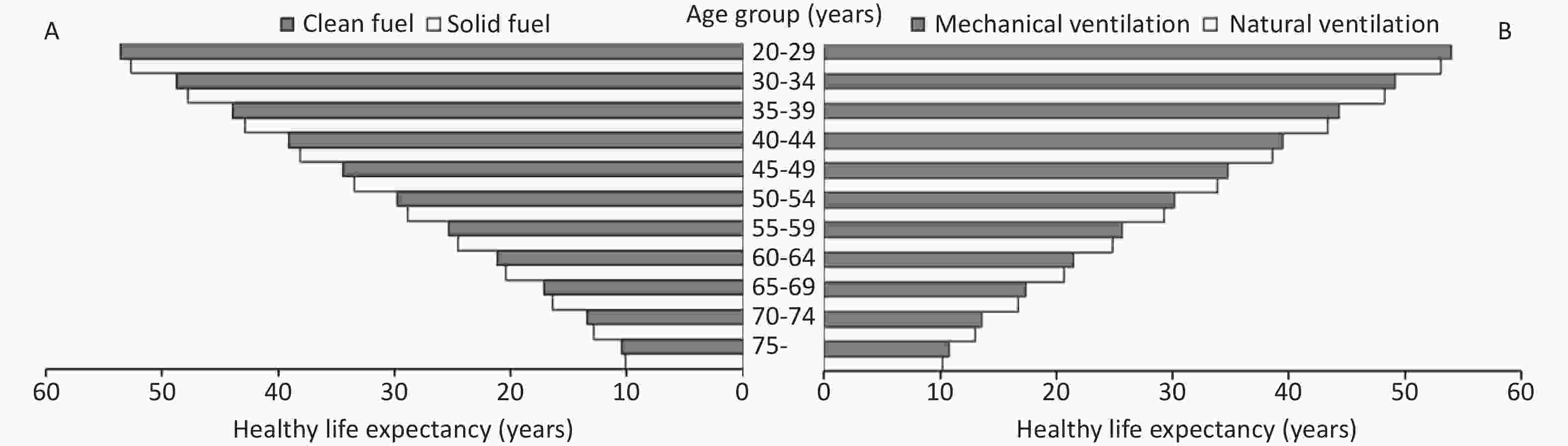
Figure S2. The health life expectancy about sarcopenia by cooking fuel type and kitchen ventilation. (A) The health life expectancy about sarcopenia by cooking fuel type. (B) The health life expectancy about sarcopenia by kitchen ventilation.
The potential biological mechanisms are not fully understood but may include: (1) inflammatory cytokines triggered by the combustion of solid fuels, which could significantly affect muscle function; (2) neuroinflammation and reactive oxygen species induced by fine particulates could cause neuropathology and central nervous system diseases, thereby affecting muscle performance. Further experimental studies are required to elucidate the underlying mechanisms. Mechanical ventilation can facilitate the rapid removal of indoor air pollutants, helping to, reduce the health hazards of fuel use.
This study had four limitations. First, individual exposure to HAP was evaluated based on cooking fuel type and kitchen ventilation status, which may have influenced the accuracy of HAP detection. However, the use of personal air monitoring devices is difficult in large population studies. Previous studies have proven the feasibility of evaluating HAP using a questionnaire[5,6], and a high intraclass correlation coefficient (ICC = 0.841) was recorded for the questionnaire retest test in this study[7]. Because HAP exposure was collected at baseline, exposure stability could not be ensured, and further studies should consider the influence of exposure stability. Second, muscle mass was evaluated using the appendicular skeletal muscle mass equation instead of the actual measurement, which could have led to deviation from the true value. Nevertheless, the equation has been validated in a Chinese population and demonstrated strong agreement with the gold standard dual energy X-ray absorptiometry, where the adjusted R2 of the equation model was 0.90, and the standard error of the estimate was 1.63 kg[10]. This equation has also been used to identify sarcopenia in a large Chinese population[6,10]. In resource-limited districts, the use of this equation could help reduce the cost of identifying at-risk cases while enabling the early prevention and treatment of sarcopenia. Third, the measurement of handgrip strength began in 2021 across Suiping, Tongxu and Yima three regions. However, as these three regions span the south, east, and west of Henan Province, they may not fully represent the rural adults of the province. Finally, although we adjusted for variables including demographic characteristics, lifestyles, and history of common chronic diseases, certain confounding factors exist, including genetic factors and kitchen area.
Solid fuel and/or natural ventilation are associated with a higher risk of sarcopenia and shorter HLE in rural regions. Further results showed that using mechanical ventilation could attenuate the risk of sarcopenia related to solid fuel use, which provides a method for sarcopenia prevention by promoting clean fuel and mechanical ventilation in resource-limited areas.
Kitchen Ventilation Attenuate the Association of Solid Fuel Use with Sarcopenia: A Cross-Sectional and Prospective Study
doi: 10.3967/bes2025.031
- Received Date: 2024-11-22
- Accepted Date: 2025-02-05
The Henan Rural Cohort Study was approved by the Zhengzhou University Life Science Ethics Committee (code: [2015] MEC (S128)) and was conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants or their agents before they enrolled in the study.
| Citation: | 
|

 Quick Links
Quick Links
 DownLoad:
DownLoad: