

 下载:
下载:


-
Pneumoconiosis is a systemic occupational disease that commonly manifests as diffuse fibrosis of the lungs caused by long-term inhalation of silica dust in the production process. The development of pneumoconiosis is a chronic and progressive process; once it occurs, it is irreversible, and gradually develops into lung injury and respiratory failure, and can cause death regardless of exposure to dust. The incidence of pneumoconiosis is the highest in China and the direct and indirect economic loss as a result of pneumoconiosis is approximately 9 billion yuan per year.
The basic pathological changes as a result of silicosis are the formation of silicon nodules and diffuse interstitial fibrosis. The diagnosis of silicosis is based on X-ray imaging, and although computed tomography (CT) scans can detect pulmonary nodules earlier than X-rays, they are not suitable for routine physical examinations due to high costs. The changes in chest films can only be reflected when lesions reach a certain degree. Therefore, there is an urgent need to discover serum markers that can be used to screen for silicosis before it becomes too advanced.
The Clara cell which is located at the terminal bronchioles and the respiratory bronchiolar belongs to a non-ciliated secreting epithelial cell[1]. Clara cell protein 16 (CC16), a 16-kD protein, which is secreted by the Clara cell plays an important role in immune suppression, and it has anti-inflammatory and anti-fibrosis properties. CC16 has been investigated as a potential biomarker related to lung epithelial injury in a variety of diseases, such as idiopathic pulmonary fibrosis (IPF), chronic obstructive pulmonary disease (COPD) and occupational lung injury. CC16 levels in serum differ based on the exposure to toxic occupational lung hazards. The serum CC16 concentration significantly decreased among asbestos-exposed subjects compared to control subjects[2]. Workers exposed to asphalt also had a significant increase in CC16 concentrations[3]. Although it has been reported that exposure to occupational dust may lead to a reduction in CC16[4], there have been few studies focused on silica dust exposure.
The aim of this study was to assess the effect of silica dust exposure on the levels of serum CC16; additionally, we aimed to determine the CC16 levels at silicosis diagnosis in order to distinguish between patients with and without silicosis. All the subjects were treated at the physical examination center of the Nanjing Prevention and Treatment Center for Occupational Diseases in 2017. 239 male workers were divided into three groups as follows: silicosis group (n = 75), dust contact group (n = 75), and control group (n = 89). All the patients in the silicosis group were diagnosed as having phase Ⅰ, Ⅱ, or Ⅲ silicosis using radiography according to the National Diagnostic Standard (GBZ70-2002) for Pneumoconiosis in China. The dust contact group comprised workers with an occupational history of silica exposure, but without abnormal findings based on their radiographs. The control group included healthy male volunteers without a history of silica exposure. Blood samples were obtained by physicians or trained study nurses from all subjects. Serum CC16 was measured using sandwich enzyme-linked immunosorbent assay kits.
Epidata 3.0 software was used to establish a database and enter data. SPSS 19.0 (IBM, Chicago, USA) software was used for statistical analysis. A receiver operating characteristic (ROC) curve was generated to determine the sensitivity threshold (Y axis) and 1-specificity (X axis) of CC16. The area under the curve (AUC) was used to compare and determine the power of discrimination of CC16 to diagnose silicosis. A multivariate linear regression model and Spearman correlation was used to assess the factors significantly related to the serum CC16 levels.
Demographic characteristics for the 239 male workers included in the study, stratified by group are shown in Table 1. Subjects in the silicosis group were older than those in the dust contact and control groups; however, this difference was not significant (P = 0.684). The cumulative exposure (8 h/day, 5 day/week as standard) had no difference between silicosis group and dust contact group (P = 0.549). There were significantly more smokers in the silicosis group than the silica dust contact and control groups (P = 0.005).
Table 1. Demographic Characteristics of the Study Subjects Stratified by Group of Enrollment
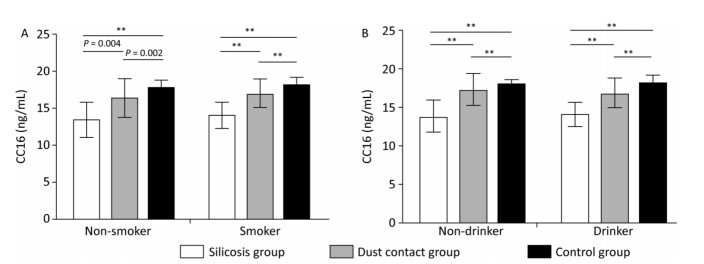
Characteristic Silicosis Group (n = 75) Dust Contact Group (n = 75) Control Group (n = 89) P Value Mean (SD) No. % Mean (SD) No. % Mean (SD) No. % Age (years) 68.08 (7.62) 67.36 (10.15) 66.97 (6.70) 0.684a Length of service (years) 32.01 (5.57) 36.31 (3.72) 41.91 (8.01) < 0.001a Cumulative exposure year 27.47 (5.23) 25.88 (4.97) - 0.549a Smoking status 0.005b Never 5 6.67 14 18.67 23 25.84 Ever 70 93.33 61 81.33 66 74.16 Drink status 0.001b Never 9 22.00 23 30.67 9 10.23 Ever 66 88.00 52 69.33 79 89.77 Note. Abbreviations: SD, standard deviation. aANOVA of the continuous variable differences between the three groups. bχ2 test for the difference in frequencies between the three groups. The subjects were divided into smoking and non-smoking groups. CC16 was significantly lower in silicosis group when compared with dust contact and healthy control groups (Figure 1A). In the non-smokers, serum CC16 levels in the silicosis group were 13.34 ± 2.48 ng/mL vs. 16.32 ± 2.70 ng/mL in the dust contact group and 17.87 ± 0.95 ng/mL in the healthy control group. Serum CC16 levels in the dust contact group were also significantly decreased compared with the controls. In the smokers, serum CC16 levels in the silicosis group were 13.99 ± 1.60 ng/mL vs. 16.99 ± 1.96 ng/mL in the dust contact group and 18.23 ± 1.06 ng/mL in the control group. Serum CC16 levels in the dust contact group were also significantly decreased compared with the controls. In the control group, there are no differences of serum CC16 levels in the drink group and non-drinking group. CC16 was significantly lower in the silicosis group when compared with the dust contact and healthy control groups (Figure 1B). In the non-drinkers, CC16 levels in the silicosis group were 13.80 ± 2.22 ng/mL vs. 17.22 ± 2.17 ng/mL in the dust contact group and 18.04 ± 0.60 ng/mL in healthy control group. Serum CC16 levels in the dust contact group were also significantly decreased compared with the controls. In the drinking group, CC16 levels obtained in silicosis group were 13.97 ± 1.59 ng/mL vs. 16.71 ± 2.09 ng/mL in the dust contact group and 18.13 ± 1.08 ng/mL in the control group. Serum CC16 levels in the dust contact group were also significantly decreased compared with the controls.
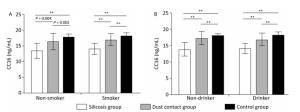
Figure 1. (A) Serum Clara cell protein 16 levels are decreased in the silicosis group both in non-smokers and smokers; (B) Serum Clara cell protein 16 levels are decreased in the silicosis group both in non-drinkers and drinkers. **, P < 0.01; error bars, standard error.
ROC curve analysis was used To determine the potential use of CC16 for silicosis diagnosis (Figure 2). The best cut-off value for CC16 was 16.21 ng/mL and the AUC for the diagnosis of silicosis was 0.919 (P < 0.001), suggesting that CC16 had a higher accuracy for the diagnosis of silicosis (0.9 < AUC < 1.0 suggesting that the diagnosis accuracy was high). The diagnostic sensitivity and specificity of CC16 for silicosis diagnosis was 81.10%, and 92.00%; the Kappa value was 0.731.
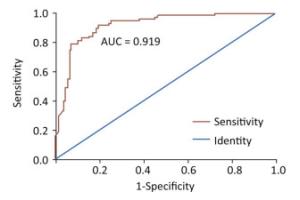
Figure 2. Receiver operating characteristic curves to evaluate serum Clara cell protein 16 as a biomarker for silicosis diagnosis (AUC = 0.919).
Factors that may affect the serum CC16 levels including silicosis group, age, length of service within their current place of employment, dust exposure, and smoking and alcohol intake were included in the linear regression model. The final factors included in the regression equation were silicone grouping and age (Supplementary Table S1, available in www.besjournal.com). Increasing age led to a decrease in the serum CC16 levels (P < 0.001); CC16 levels were the lowest in the silicosis group, followed by the silica dust exposure group; the CC16 levels were the highest in control group (P < 0.001).
Table Supplementary Table S1. Multinomial Linear Regression Model to Assess the Factors Significantly Related to the Serum CC16 Levels
Variable β Standard Error P Value Constant 15.432 0.933 Group 2.045 0.128 < 0.001 Age -0.048 0.013 < 0.001 Silicosis is a fibrotic interstitial lung diseases caused by inhalation of free crystalline silicon dioxide or silica. Phagocytosis of crystalline silica in the lungs causes lysosomal damage, activating the NALP3 inflammasome and triggering the inflammatory cascade with subsequent fibrosis. Impairment of lung function increases with disease progression, even after the patient is no longer exposed[5]. Growing evidence showed that CC16 has anti-inflammatory activities in lung inflammation diseases, such as chronic obstructive pulmonary disease (COPD) and asthma, probably through inhibiting phospholipase A2 (PLA2) and cytokine production[6, 7]. Furthermore, studies of both human COPD cohorts and CC16-gene targeted mice in models of experimental COPD have indicated that reduced CC16 level contributes to the development and progression of COPD[8]. Molecular mechanism research showed that CC16 inhibited LPS-induced TNF-α, IL-6, and IL-8 expression in a concentration-dependent manner and inhibited the increase of nuclear NF-κB and the reduction of cytosolic NF-Κb[9].
Exposure to cigarette smoke has been shown to be associated with a reduction in the numbers of club cells in the bronchial epithelium and serum CC16 concentrations in animal models. The serum CC16 levels were reported to be lower in smokers than in non-smokers[10]. However, in this study, there was no difference in the level of serum CC16 between smoking and non-smoking groups, which may be due to the fact that the toxicity as a result of smoking was not compared with the long-term inhalation of high concentrations of dust.
This study was subject to several limitations. First, we collected serum bio-blood samples from the subjects for this analysis and assessment. We did not collect data on the lung function of the subjects. Therefore, we could not describe the relationship between lung function and CC16 levels. Second, we only included male subjects, because most of the long-term exposure to dust was considered to occur in male workers. Therefore, it was not possible to observe the CC16 levels in serum among female subjects. Further studies on the detailed molecular mechanisms for silica dust exposure resulting in the reduction of CC16 levels in serum are warranted.
In conclusion, long-term exposure to silica dust may result in a reduction in CC16 levels in serum; additionally, CC16 can be used as a blood serum biomarker for higher accuracy in the diagnosis of silicosis.
doi: 10.3967/bes2019.007
The Effect of Silica Dust Exposure on the Serum Clara Cell Protein 16 Levels in Chinese Workers
-
-
Figure 1. (A) Serum Clara cell protein 16 levels are decreased in the silicosis group both in non-smokers and smokers; (B) Serum Clara cell protein 16 levels are decreased in the silicosis group both in non-drinkers and drinkers. **, P < 0.01; error bars, standard error.
Figure 2. Receiver operating characteristic curves to evaluate serum Clara cell protein 16 as a biomarker for silicosis diagnosis (AUC = 0.919).
Table 1. Demographic Characteristics of the Study Subjects Stratified by Group of Enrollment
Characteristic Silicosis Group (n = 75) Dust Contact Group (n = 75) Control Group (n = 89) P Value Mean (SD) No. % Mean (SD) No. % Mean (SD) No. % Age (years) 68.08 (7.62) 67.36 (10.15) 66.97 (6.70) 0.684a Length of service (years) 32.01 (5.57) 36.31 (3.72) 41.91 (8.01) < 0.001a Cumulative exposure year 27.47 (5.23) 25.88 (4.97) - 0.549a Smoking status 0.005b Never 5 6.67 14 18.67 23 25.84 Ever 70 93.33 61 81.33 66 74.16 Drink status 0.001b Never 9 22.00 23 30.67 9 10.23 Ever 66 88.00 52 69.33 79 89.77 Note. Abbreviations: SD, standard deviation. aANOVA of the continuous variable differences between the three groups. bχ2 test for the difference in frequencies between the three groups.  下载: 导出CSV
下载: 导出CSV
Supplementary Table S1. Multinomial Linear Regression Model to Assess the Factors Significantly Related to the Serum CC16 Levels
Variable β Standard Error P Value Constant 15.432 0.933 Group 2.045 0.128 < 0.001 Age -0.048 0.013 < 0.001
下载: 导出CSV
-
[1] Lock-Johansson S, Vestbo J, Sorensen GL. Surfactant protein D, Club cell protein 16, Pulmonary and activation-regulated chemokine, C-reactive protein, and Fibrinogen biomarker variation in chronic obstructive lung disease. Respir Res, 2014; 15, 147. doi: 10.1186/s12931-014-0147-5 [2] Petrek M, Hermans C, Kolek V, et al. Clara cell protein (CC16) in serum and bronchoalveolar lavage fluid of subjects exposed to asbestos. Biomarkers, 2002; 7, 58-67. doi: 10.1080/13547500110086892 [3] Ulvestad B, Randem BG, Andersson L, et al. Clara cell protein as a biomarker for lung epithelial injury in asphalt workers. J Occup Environ Med, 2007; 49, 1073-8. doi: 10.1097/JOM.0b013e3181570726 [4] Kotani K, Kawabata I, Mu H, et al. Urinary protein 1/Clara cell 16 concentrations and lung functions in male subjects with pneumoconiosis. Ann Clin Biochem, 2007; 44, 560-2. doi: 10.1258/000456307782268110 [5] Schoening JM, Corner LAL, Messam LLM, et al. Environmental dust inhalation in the European badger (Meles meles):Systemic distribution of silica-laden macrophages, pathological changes, and association with Mycobacterium bovis infection status. PLoS One, 2018; 13, e0190230. doi: 10.1371/journal.pone.0190230 [6] Laucho-Contreras ME, Polverino F, Tesfaigzi Y, et al. Club Cell Protein 16 (CC16) Augmentation:A Potential Disease-modifying Approach for Chronic Obstructive Pulmonary Disease (COPD). Expert Opin Ther Targets, 2016; 20, 869-83. doi: 10.1517/14728222.2016.1139084 [7] Emmanouil P, Loukides S, Kostikas K, et al. Sputum and BAL Clara cell secretory protein and surfactant protein D levels in asthma. Allergy, 2015; 70, 711-4. doi: 10.1111/all.2015.70.issue-6 [8] Tsoumakidou M, Bouloukaki I, Thimaki K, et al. Innate immunity proteins in chronic obstructive pulmonary disease and idiopathic pulmonary fibrosis. Exp Lung Res, 2010; 36, 373-80. doi: 10.3109/01902141003690389 [9] Pang M, Yuan Y, Wang D, et al. Recombinant CC16 protein inhibits the production of pro-inflammatory cytokines via NF-kappaB and p38 MAPK pathways in LPS-activated RAW264.7 macrophages. Acta Biochim Biophys Sin (Shanghai), 2017; 49, 435-43. doi: 10.1093/abbs/gmx020 [10] Zhu L, Di PY, Wu R, et al. Repression of CC16 by cigarette smoke (CS) exposure. PLoS One, 2015; 10, e0116159. doi: 10.1371/journal.pone.0116159 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 1466
- HTML全文浏览量: 592
- PDF下载量: 100
- 被引次数: 0

 Quick Links
Quick Links