

 下载:
下载:

-
Three-vessel disease (TVD), characterized by significant stenosis in three main epicardial coronary arteries, is found in 20%-30% of patients with obstructive coronary artery disease (CAD)[1, 2] and 15%-20% of patients with acute myocardial infarction (MI)[3, 4]. It is well established that TVD increases the risk of mortality compared with singlevessel disease[3, 5]. Therefore, risk stratification in patients with TVD is important for improving management and prognosis. The Synergy between PCI with Taxus and Cardiac Surgery (SYNTAX) score characterizes the extent and severity of CAD and is tightly related to the outcomes in patients with TVD[6].
As the prominent cation and anion in extracellular fluid, serum sodium, and chloride levels are directly correlated with each other to preserve electroneutrality[7]. Both are commonly assessed as a part of routine biochemical testing in clinical practice. The significance of serum sodium level has been studied in diverse cardiovascular conditions. For example, low serum sodium level at admission was associated with worse prognosis and increased mortality in patients with acute coronary syndrome[8-12] and heart failure (HF)[13, 14]. By contrast, the role of serum chloride in cardiovascular diseases was largely overlooked until recent studies indicated that low serum chloride level was an independent predictor of mortality in patients with HF[7, 15, 16] and acute MI accompanied by systolic dysfunction[17]. However, the application of serum sodium and chloride levels in high-risk CAD patients with advanced coronary atheroma burden remains unclear. Therefore, this study aimed to evaluate the long-term prognostic value of serum chloride and sodium levels in patients with TVD.
-
This prospective cohort study enrolled 8, 943 consecutive patients with TVD at Fuwai Hospital, Chinese Academy of Medical Sciences from April 2004 to February 2011[18]. Patients were eligible for inclusion in the study if they had TVD, defined as angiographically confirmed stenosis of ≥ 50% in all three main epicardial coronary arteries (i.e., left anterior descending, left circumflex and right coronary arteries), with or without involvement of the left main artery, and were willing to receive follow-up. There was no pre-specified exclusion criterion. Patients received medical therapy (MT) alone, percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) according to clinical and anatomical factors, contemporary treatment guidelines[19, 20], and their preferences. After enrollment, the patients were followed up as study protocol defined. Baseline and procedural data for all the participants were collected in a database by independent clinical research coordinators. Outcome data were obtained through telephone interview, follow-up letter, or clinic visit. The last follow-up was completed in 2016, with a response rate of 80.6%. All events were carefully checked and verified by an independent group of clinical physicians. Investigator training, blinded questionnaire survey, and telephone recording were performed to obtain results with high-quality.
The study conformed to the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Fuwai Hospital. Written informed consents were obtained from all the participants.
-
Baseline serum chloride and sodium levels were measured by using blood samples which were taken from the patients by direct venipuncture after admission for coronary angiography. The SYNTAX score[6] was calculated by a dedicated research group blinded to the clinical data using an online calculator (http://www.syntaxscore.com). Creatinine clearance was calculated by using the Cockcroft and Gault formula[21].
-
The primary endpoint was all-cause death. Secondary endpoints included cardiac death, major adverse cardiac and cerebrovascular events (MACCE), a composite of all-cause death, myocardial infarction, stroke or unplanned revascularization, and the individual components of the composite endpoint. All deaths were considered as cardiac ones unless an unequivocal non-cardiac cause could be established.
-
Continuous variables are presented as mean ± standard deviation, while categorical variables are presented as numbers of patients and proportions (%). One-way ANOVA was used to compare continuous variables, and χ2 test or Fisher's exact test was used for the comparisons among the categorical variables.
The study population was stratified into tertiles by each of the following two variables: serum chloride levels ≤ 102.0 mmol/L, > 102.0 to ≤ 105.1 mmol/L, and > 105.1 mmol/L; and serum sodium levels ≤ 139.0 mmol/L, > 139.0 to ≤ 141.0 mmol/L, and > 141.0 mmol/L. Spearman correlation coefficient was used to assess the correlation between serum chloride level and serum sodium level. Survival curves were constructed with the Kaplan-Meier method and log-rank tests were used to compare the curves of different groups based on tertiles of serum chloride and sodium levels. Univariable and multivariable Cox proportional hazard models were used to calculate hazard ratio (HR) and 95% confidence interval (CI) to analyze the relationship of serum chloride and sodium levels with long-term outcomes. In multivariable analyses, covariates were selected based on their prognostic relevance, potential confounding effect and clinical significance. A base model was constructed with the following covariates: age, sex, body mass index, medical history and risk factor (hypertension, diabetes mellitus, previous MI, hyperlipidemia, stroke, peripheral artery disease, and chronic kidney disease), presentation [stable angina pectoris (SAP), unstable angina pectoris (UAP), or acute myocardial infarction (AMI)], left ventricular ejection fraction (LVEF), left main coronary artery involvement, creatinine clearance, SYNTAX score (0-22, 23-32, or ≥ 33) and procedure (MT, PCI, or CABG).
The interaction between serum chloride and sodium levels with outcomes was tested by using the multivariable Cox regression hazard model. Subgroup analyses were performed based on the following covariates: age (≥ 65 or < 65 years), sex (male or female), diabetes (yes or no), presentation (SAP, UAP, or AMI), LVEF (≥ 40% vs. < 40%), left main disease (yes or no), SYNTAX score (0-22, 23-32, or ≥ 32), and procedure (MT, PCI, or CABG). Interactions between chloride or sodium levels and these covariates on outcomes were tested to interpret possible subgroup differences.
Comparisons of area under the receiver operating characteristic curves (AUC) were performed to assess differences between predictability of the SYNTAX score with and without serum chloride or sodium levels as an additional variable. Two-sided P-values < 0.05 were considered statistically significant. Statistical analyses were performed with SPSS software version 22.0 (IBM, Armonk, NY, USA).
-
A total of 8, 318 (93%) participants with available serum chloride and sodium values were included in the present analysis. The mean levels of serum chloride and sodium were 103.5 ± 3.5 mmol/L and 139.9 ± 3.1 mmol/L, respectively. The correlation between serum chloride level and serum sodium level was modest (r = 0.41, P < 0.001).
Baseline characteristics of the participants grouped by tertiles of serum chloride and sodium levels are presented in Table 1. Patients in the low chloride tertiles group (≤ 102.0 mmol/L) were younger, had higher rates of diabetes and MI, lower LVEF and serum sodium level, higher creatinine clearance, and received MT more frequently. Patients in the low sodium tertiles group (≤ 139.0 mmol/L) showed a higher prevalence of diabetes, chronic kidney disease and MI, with lower LVEF and serum chloride level, and were more likely to receive MT.
Table 1. Baseline Characteristics of the Study Population

-
During the median follow-up of 7.5 years, deaths from any cause were observed in 1, 249 patients (15.0%), including 643 deaths from cardiac causes (7.7%). Most all-cause deaths, cardiac deaths and MACCE occurred in patients in the low tertiles group of serum chloride or sodium level (Table 2).
Table 2. Long-Term Clinical Outcomes of the Study Population

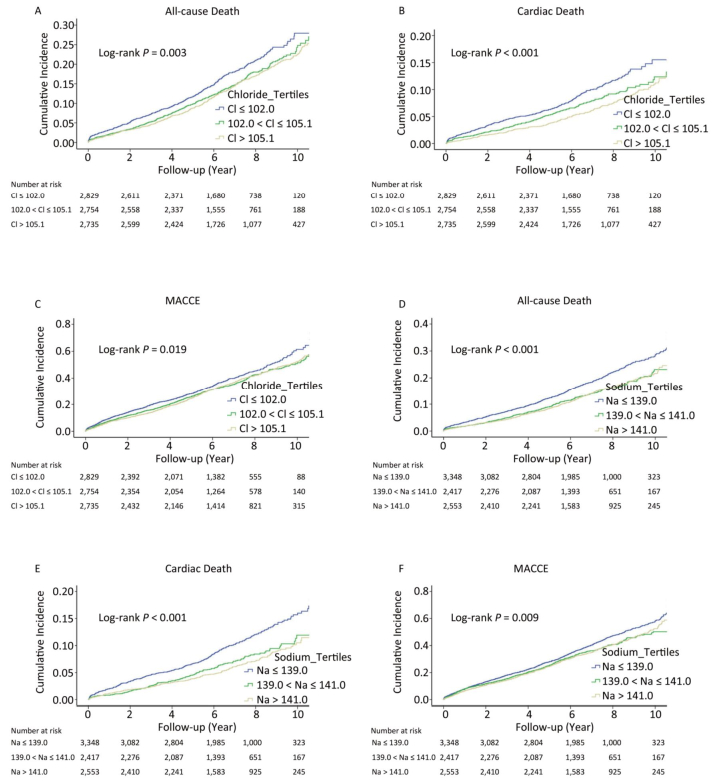
In univariate analyses, patients in the low tertiles group of serum chloride level had a higher risk for all-cause death (HR: 1.25, 95% CI: 1.09-1.43, P = 0.001), cardiac death (HR: 1.52, 95% CI: 1.26-1.84, P < 0.001), and MACCE (HR: 1.13, 95% CI: 1.03-1.24, P = 0.012), but not for MI, stroke or unplanned revascularization, compared with those in the high tertiles group (Table 3 and Supplementary Table S1 available in www.besjournal.com). Comparable findings were also observed in patients in the low tertiles group of serum sodium level (Table 3 and Supplementary Table S1). Kaplan-Meier estimates of all-cause death, cardiac death and MACCE were significantly different across tertiles groups of serum chloride and sodium levels (log-rank P < 0.05 for all) (Figure 1A-F).
Table Supplementary Table S1. Univariable Analysis for Other Secondary Endpoints
Variable Myocardial Infarction Stroke Unplanned Revascularization HR (95% CI) P-value HR (95% CI) P-value HR (95% CI) P-value Chloride ≤ 102.0 mmol/L 0.92 (0.74-1.15) 0.451 1.03 (0.85-1.25) 0.752 1.03 (0.86-1.23) 0.780 Chloride > 102.0 to ≤ 105.1 mmol/L 0.99 (0.80-1.23) 0.944 0.86 (0.70-1.05) 0.127 1.00 (0.84-1.20) 0.977 Chloride > 105.1 mmol/L Reference Reference Reference Sodium ≤ 139.0 mmol/L 0.94 (0.76-1.16) 0.550 1.01 (0.83-1.22) 0.940 0.88 (0.74-1.06) 0.173 Sodium > 139.0 to ≤ 141.0 mmol/L 0.93 (0.74-1.17) 0.520 1.00 (0.81-1.23) 0.994 1.00 (0.83-1.20) 0.989 Sodium > 141.0 mmol/L Reference Reference Reference Note. CI, confidence interval; HR indicates hazard ratio. Table 3. Univariable and Multivariable Analysis for Mortality and MACCE


Figure 1. Kaplan-Meier curves for all-cause death (A, D), cardiac death (B, E) and major adverse cardiac and cerebrovascular events (MACCE; C, F) across tertiles of chloride and sodium. Cl, serum chloride level, mmol/L; Na, serum sodium level, mmol/L.
When both chloride and sodium were simultaneously integrated into the base model, low sodium level (≤ 139.0 mmol/L) remained significantly associated with an increased risk for all-cause death (HR: 1.16, 95% CI: 1.01-1.34, P = 0.041) and cardiac death (HR: 1.26, 95% CI: 1.03-1.55, P = 0.027), while serum chloride level was no longer significantly associated with the outcomes (Table 3). There was no interaction of serum chloride and sodium levels with all-cause or cardiac death (P = 0.705 and 0.618, respectively).
-
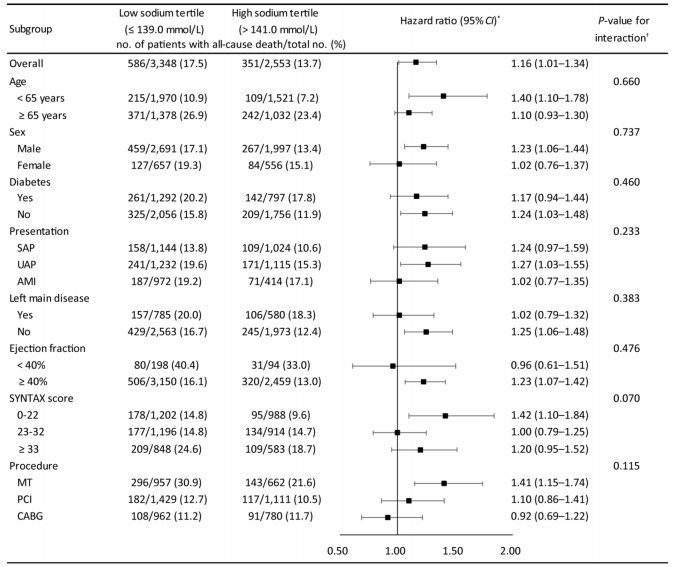
The relationship of serum sodium level with all-cause death was relatively consistent across the subgroups of age, sex, diabetes, presentation, left main disease, LVEF, SYNTAX score or procedure (Figure 2). There was no significant interaction of tertiles of sodium and these covariates (interaction P-value > 0.05 for all subgroups).
Figure 2. Associations of tertiles of serum sodium with risk of all-cause death across subgroups. AMI, acute myocardial infarction; CABG, coronary artery bypass grafting; MT, medical therapy; PCI, percutaneous coronary intervention; SAP, stable angina pectoris; UAP, unstable angina pectoris. *Multivariable Cox regression was used to determine mortality risk of patients in low sodium tertile (≤ 139.0 mmol/L) compared with patients in high sodium tertile (> 141.0 mmol/L). †The interaction between sodium tertiles and each covariate was tested using multivariable Cox regression hazard model.
-
Since serum sodium level was more strongly associated with outcomes compared with serum chloride, tertiles of serum sodium level were combined with SYNTAX score for prediction of mortality to evaluate its incremental information. There was a modest but significant improvement for AUC values between the two prediction sets [SYNTAX score: 0.570 (0.552-0.588) vs. SYNTAX score with serum sodium level 0.586 (0.568-0.603), P = 0.011].
-
In a large prospective cohort of patients with three-vessel coronary artery disease, we found that both serum chloride level and serum sodium level were prognostically similar in univariate analysis. However, when incorporated into the base model, only low sodium level remained to be associated with increased risks for all-cause and cardiac death. Although serum chloride level and serum sodium level were modestly correlated, there was no significant interaction for mortality prediction. Subgroup analysis revealed that the relationship of serum sodium level with all-cause death was relatively consistent across the subgroups. There was no significant interaction of serum sodium level with those covariates, suggesting that there was no true subgroup difference. Taken together, these findings indicate that low serum sodium level, rather than serum chloride level, is an independent predictor of mortality in patients with TVD.
TVD is common in patients with obstructive CAD[1, 2], with an almost 2-fold risk of mortality compared with single-vessel CAD[5]. SYNTAX Score is widely used to assess risk of adverse cardiac events in patients with TVD, but it showed only a modest predictability in previous studies as well as in our study[22, 23]. In this regard, SYNTAX score Ⅱ, in which clinical factors were included, has been developed to provide improved prognostic information[24]. But it showed only a moderate discrimination ability for long-term mortality prediction in patients with multivessel disease[25, 26]. Additional prognosis-associated clinical markers may add important information to SYNTAX score.
Previous studies reported that low serum sodium level was associated with mortality in patients with acute coronary syndromes[8-12], and was an independent predictor of adverse outcomes in diverse cardiovascular diseases[8, 13]. In the present study, we extended this finding to the setting of TVD. In addition, sodium level provided modest but significant prognostic information on top of SYNTAX score for prediction of mortality. This is of great importance because risk stratification can add in treatment decision and improve prognosis of patients.
A recent epidemiologic study suggested that mild hyponatremia even within the normal range of serum sodium level was associated with an increased risk for cardiovascular death[27]. Indeed, a more conservative definition of hyponatremia (< 139.0 mmol/L) has been suggested[28]. In support, we found that patients in the low tertiles group of serum sodium level (≤ 139.0 mmol/L) had significantly increased risk of mortality compared with those in the high tertiles group. Thus, low serum sodium level, even within the normal range, increases risk for mortality and requires prompt correction in patients with TVD.
A J or U curve was reported with respect to the association of serum sodium level with mortality[14, 27]. For example, hypernatremia was also associated with an increased risk for mortality compared with normal sodium level[29]. However, we found that patients in the high tertiles group of serum sodium level (> 141.0 mmol/L) had the lowest risk for mortality, with no evidence of a J or U curve. This might be related to the low numbers of patients (276; 12.6%) with serum sodium level > 145.0 mmol/L (hypernatremia), and only one patient with serum sodium level > 155 mmol/L (severe hypernatremia) in this high tertiles group.
The levels of serum sodium and chloride are tightly related with each other. High level of serum sodium is typically accompanied by high level of serum chloride, and vice versa. However, consistent with previous studies[16, 17], we found only a modest correlation of serum chloride level with serum sodium level (r < 0.5), suggesting that serum chloride and sodium levels might provide distinct predictive information. Assessment of serum chloride level was largely ignored until recent studies suggesting a stronger prognostic value than serum sodium level in HF patients and in MI patients complicated by systolic dysfunction[7, 15-17]. Thus, we evaluated the relationship of both serum chloride and sodium levels with long-term outcomes in patients with TVD. The prognostic value of serum chloride level diminished when serum sodium level was added into the multivariable model for all-cause death, suggesting that serum sodium level has a stronger association with long-term outcomes in patients with TVD compared with serum chloride level. Both low chloride level and low sodium level were associated with complex neurohormonal activation, including activation of the renin-angiotensin system[30, 31], which was associated with increased mortality in both HF patients and CAD patients[32-34]. Moreover, low serum chloride level was strongly associated with diuretic resistance[31, 35], a marker of poor decongestion and related to an increased risk for mortality in HF[36]. In the setting of TVD, however, diuretics were not used as often as that in HF[37]. This might partly explain why serum chloride level provided less prognostic information in TVD than that in HF.
The present study has several limitations. First, this was a registry-based observational study, with potential for selection bias that cannot be balanced with multivariable analysis. Second, all the patients in the study were recruited from a single specialized center for cardiovascular disease. Therefore, our findings might be population specific, especially the cut-off values among serum chloride and/or sodium level tertiles might differ in various populations. Third, medication information on diuretics, which could influence serum chloride and sodium levels, was not recorded in the database. Fourth, despite the strong association of low serum sodium level with mortality, the definite pathophysiology underlying this association still needs to be fully elucidated and further functional studies are required.
-
In patients with TVD, serum sodium level had a stronger association with long-term outcomes compared with serum chloride level, which was different from the setting of heart failure. Low serum sodium level (≤ 139.0 mmol/L) was an independent risk factor for mortality. Serum sodium level could provide modest improvement in discrimination for mortality prediction after adding it to SYNTAX score.
-
We thank all staff members for data collection, data entry, and monitoring as part of this study.
doi: 10.3967/bes2019.035
Prognostic Values of Serum Chloride and Sodium Levels in Patients with Three-vessel Disease
-
Abstract:
Objective Identification of new risk factors is needed to improve prediction of adverse outcomes in patients with three-vessel disease (TVD). The present study aimed to evaluate the prognostic values of serum chloride and sodium levels in patients with TVD. Methods We used data from a prospective cohort of consecutive patients with angiographically confirmed TVD. The primary endpoint was all-cause death. Cox proportional hazard regression was used to analyze the relationship of serum chloride and sodium levels with long-term outcomes of TVD patients. Results A total of 8, 318 participants with available serum chloride and sodium data were included in this analysis. At baseline, patients in the low tertiles group of serum chloride level (≤ 102.0 mmol/L) or serum sodium level (≤ 139.0 mmol/L) had more severe disease conditions. During a median follow-up of 7.5-year, both low serum chloride level and low serum sodium level were found to be associated with an increased risk for mortality in univariate analysis. However, when both parameters were incorporated into a multivariate model, only low serum sodium level remained to be an independent predictor of all-cause death (hazard ratio:1.16, 95% confidence interval:1.01-1.34, P=0.041). Modest but significant improvement of discrimination was observed after incorporating serum sodium level into the Synergy between percutaneous coronary intervention (PCI) with Taxus and Cardiac Surgery score. Conclusion Serum sodium level is more strongly associated with long-term outcomes of TVD patients compared with serum chloride level. Low serum sodium level is an independent risk factor for mortality, but only provides modest prognostic information beyond an established risk model. -
Key words:
- Coronary disease /
- Prognosis /
- Biomarkers
-
Figure 1. Kaplan-Meier curves for all-cause death (A, D), cardiac death (B, E) and major adverse cardiac and cerebrovascular events (MACCE; C, F) across tertiles of chloride and sodium. Cl, serum chloride level, mmol/L; Na, serum sodium level, mmol/L.
Figure 2. Associations of tertiles of serum sodium with risk of all-cause death across subgroups. AMI, acute myocardial infarction; CABG, coronary artery bypass grafting; MT, medical therapy; PCI, percutaneous coronary intervention; SAP, stable angina pectoris; UAP, unstable angina pectoris. *Multivariable Cox regression was used to determine mortality risk of patients in low sodium tertile (≤ 139.0 mmol/L) compared with patients in high sodium tertile (> 141.0 mmol/L). †The interaction between sodium tertiles and each covariate was tested using multivariable Cox regression hazard model.
Table 1. Baseline Characteristics of the Study Population
Table 2. Long-Term Clinical Outcomes of the Study Population
Supplementary Table S1. Univariable Analysis for Other Secondary Endpoints
Variable Myocardial Infarction Stroke Unplanned Revascularization HR (95% CI) P-value HR (95% CI) P-value HR (95% CI) P-value Chloride ≤ 102.0 mmol/L 0.92 (0.74-1.15) 0.451 1.03 (0.85-1.25) 0.752 1.03 (0.86-1.23) 0.780 Chloride > 102.0 to ≤ 105.1 mmol/L 0.99 (0.80-1.23) 0.944 0.86 (0.70-1.05) 0.127 1.00 (0.84-1.20) 0.977 Chloride > 105.1 mmol/L Reference Reference Reference Sodium ≤ 139.0 mmol/L 0.94 (0.76-1.16) 0.550 1.01 (0.83-1.22) 0.940 0.88 (0.74-1.06) 0.173 Sodium > 139.0 to ≤ 141.0 mmol/L 0.93 (0.74-1.17) 0.520 1.00 (0.81-1.23) 0.994 1.00 (0.83-1.20) 0.989 Sodium > 141.0 mmol/L Reference Reference Reference Note. CI, confidence interval; HR indicates hazard ratio.  下载: 导出CSV
下载: 导出CSV
Table 3. Univariable and Multivariable Analysis for Mortality and MACCE
-
[1] Patel MR, Peterson ED, Dai D, et al. Low diagnostic yield of elective coronary angiography. N Engl J Med, 2010; 362, 886-95. doi: 10.1056/NEJMoa0907272 [2] Bradley SM, Spertus JA, Kennedy KF, et al. Patient selection for diagnostic coronary angiography and hospital-level percutaneous coronary intervention appropriateness:insights from the National Cardiovascular Data Registry. JAMA Intern Med, 2014; 174, 1630-9. doi: 10.1001/jamainternmed.2014.3904 [3] Sorajja P, Gersh BJ, Cox DA, et al. Impact of multivessel disease on reperfusion success and clinical outcomes in patients undergoing primary percutaneous coronary intervention for acute myocardial infarction. Eur Heart J, 2007; 28, 1709-16. doi: 10.1093/eurheartj/ehm184 [4] Park DW, Clare RM, Schulte PJ, et al. Extent, location, and clinical significance of non-infarct-related coronary artery disease among patients with ST-elevation myocardial infarction. JAMA, 2014; 312, 2019-27. doi: 10.1001/jama.2014.15095 [5] Min JK, Dunning A, Lin FY, et al. Age-and sex-related differences in all-cause mortality risk based on coronary computed tomography angiography findings results from the International Multicenter CONFIRM (Coronary CT Angiography Evaluation for Clinical Outcomes:An International Multicenter Registry) of 23, 854 patients without known coronary artery disease. J Am Coll Cardiol, 2011; 58, 849-60. doi: 10.1016/j.jacc.2011.02.074 [6] Serruys PW, Morice MC, Kappetein AP, et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med, 2009; 360, 961-72. doi: 10.1056/NEJMoa0804626 [7] Grodin JL, Simon J, Hachamovitch R, et al. Prognostic Role of Serum Chloride Levels in Acute Decompensated Heart Failure. J Am Coll Cardiol, 2015; 66, 659-66. doi: 10.1016/j.jacc.2015.06.007 [8] Goldberg A, Hammerman H, Petcherski S, et al. Prognostic importance of hyponatremia in acute ST-elevation myocardial infarction. Am J Med, 2004; 117, 242-8. doi: 10.1016/j.amjmed.2004.03.022 [9] Goldberg A, Hammerman H, Petcherski S, et al. Hyponatremia and long-term mortality in survivors of acute ST-elevation myocardial infarction. Arch Intern Med, 2006; 166, 781-6. doi: 10.1001/archinte.166.7.781 [10] Singla I, Zahid M, Good CB, et al. Effect of hyponatremia (< 135 mEq/L) on outcome in patients with non-ST-elevation acute coronary syndrome. Am J Cardiol, 2007; 100, 406-8. doi: 10.1016/j.amjcard.2007.03.039 [11] Burkhardt K, Kirchberger I, Heier M, et al. Hyponatraemia on admission to hospital is associated with increased long-term risk of mortality in survivors of myocardial infarction. Eur J Prev Cardiol, 2015; 22, 1419-26. doi: 10.1177/2047487314557963 [12] Choi JS, Kim CS, Bae EH, et al. Prognostic impact of hyponatremia occurring at various time points during hospitalization on mortality in patients with acute myocardial infarction. Medicine (Baltimore), 2017; 96, e7023. doi: 10.1097/MD.0000000000007023 [13] Klein L, O'Connor CM, Leimberger JD, et al. Lower serum sodium is associated with increased short-term mortality in hospitalized patients with worsening heart failure:results from the Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure (OPTIME-CHF) study. Circulation, 2005; 111, 2454-60. doi: 10.1161/01.CIR.0000165065.82609.3D [14] Gheorghiade M, Abraham WT, Albert NM, et al. Relationship between admission serum sodium concentration and clinical outcomes in patients hospitalized for heart failure:an analysis from the OPTIMIZE-HF registry. Eur Heart J, 2007; 28, 980-8. doi: 10.1093/eurheartj/ehl542 [15] Grodin JL, Verbrugge FH, Ellis SG, et al. Importance of Abnormal Chloride Homeostasis in Stable Chronic Heart Failure. Circ Heart Fail, 2016; 9, e2453. http://cn.bing.com/academic/profile?id=7d2d69c5e36a7608ff5e524fcf09e038&encoded=0&v=paper_preview&mkt=zh-cn [16] Testani JM, Hanberg JS, Arroyo JP, et al. Hypochloraemia is strongly and independently associated with mortality in patients with chronic heart failure. Eur J Heart Fail, 2016; 18, 660-8. doi: 10.1002/ejhf.2016.18.issue-6 [17] Ferreira JP, Girerd N, Duarte K, et al. Serum Chloride and Sodium Interplay in Patients With Acute Myocardial Infarction and Heart Failure With Reduced Ejection Fraction:An Analysis From the High-Risk Myocardial Infarction Database Initiative. Circ Heart Fail, 2017; 10, e003500. http://cn.bing.com/academic/profile?id=e29c57fe7f8427f0ad12f88140fadca5&encoded=0&v=paper_preview&mkt=zh-cn [18] Xu JJ, Jiang L, Xu LJ, et al. Association of CDKN2B-AS1 Polymorphisms with Premature Triple-vessel Coronary Disease and Their Sex Specificity in the Chinese Population. Biomed Environ Sci, 2018; 31, 787-96. http://d.old.wanfangdata.com.cn/Periodical/bes201811001 [19] Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol, 2011; 58, e44-122. doi: 10.1016/j.jacc.2011.08.007 [20] Hillis LD, Smith PK, Anderson JL, et al. 2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Developed in collaboration with the American Association for Thoracic Surgery, Society of Cardiovascular Anesthesiologists, and Society of Thoracic Surgeons. J Am Coll Cardiol, 2011; 58, e123-210. doi: 10.1016/j.jacc.2011.08.009 [21] Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron, 1976; 16, 31-41. doi: 10.1159/000180580 [22] Girasis C, Garg S, Raber L, et al. SYNTAX score and Clinical SYNTAX score as predictors of very long-term clinical outcomes in patients undergoing percutaneous coronary interventions:a substudy of SIRolimus-eluting stent compared with pacliTAXel-eluting stent for coronary revascularization (SIRTAX) trial. Eur Heart J, 2011; 32, 3115-27. doi: 10.1093/eurheartj/ehr369 [23] Zhang YJ, Iqbal J, Campos CM, et al. Prognostic value of site SYNTAX score and rationale for combining anatomic and clinical factors in decision making:insights from the SYNTAX trial. J Am Coll Cardiol, 2014; 64, 423-32. doi: 10.1016/j.jacc.2014.05.022 [24] Farooq V, van Klaveren D, Steyerberg EW, et al. Anatomical and clinical characteristics to guide decision making between coronary artery bypass surgery and percutaneous coronary intervention for individual patients:development and validation of SYNTAX score Ⅱ. Lancet, 2013; 381, 639-50. doi: 10.1016/S0140-6736(13)60108-7 [25] Sotomi Y, Cavalcante R, van Klaveren D, et al. Individual Long-Term Mortality Prediction Following Either Coronary Stenting or Bypass Surgery in Patients With Multivessel and/or Unprotected Left Main Disease:An External Validation of the SYNTAX Score Ⅱ Model in the 1, 480 Patients of the BEST and PRECOMBAT Randomized Controlled Trials. JACC Cardiovasc Interv, 2016; 9, 1564-72. doi: 10.1016/j.jcin.2016.04.023 [26] Cavalcante R, Sotomi Y, Mancone M, et al. Impact of the SYNTAX scores Ⅰ and Ⅱ in patients with diabetes and multivessel coronary disease:a pooled analysis of patient level data from the SYNTAX, PRECOMBAT, and BEST trials. Eur Heart J, 2017; 38, 1969-77. doi: 10.1093/eurheartj/ehx138 [27] Wannamethee SG, Shaper AG, Lennon L, et al. Mild hyponatremia, hypernatremia and incident cardiovascular disease and mortality in older men:A population-based cohort study. Nutr Metab Cardiovasc Dis, 2016; 26, 12-9. doi: 10.1016/j.numecd.2015.07.008 [28] Kumar S, Berl T. Sodium. Lancet, 1998; 352, 220-8. doi: 10.1016/S0140-6736(97)12169-9 [29] Palevsky PM, Bhagrath R, Greenberg A. Hypernatremia in hospitalized patients. Ann Intern Med, 1996; 124, 197-203. doi: 10.7326/0003-4819-124-2-199601150-00002 [30] Lilly LS, Dzau VJ, Williams GH, et al. Hyponatremia in congestive heart failure:implications for neurohumoral activation and responses to orthostasis. J Clin Endocrinol Metab, 1984; 59, 924-30. doi: 10.1210/jcem-59-5-924 [31] Hanberg JS, Rao V, Ter Maaten JM, et al. Hypochloremia and Diuretic Resistance in Heart Failure:Mechanistic Insights. Circ Heart Fail, 2016; 9, e003180. http://cn.bing.com/academic/profile?id=6b7bfa7aefa45530707f4a8d0cebe553&encoded=0&v=paper_preview&mkt=zh-cn [32] Palmer BR, Pilbrow AP, Frampton CM, et al. Plasma aldosterone levels during hospitalization are predictive of survival post-myocardial infarction. Eur Heart J, 2008; 29, 2489-96. [33] Ivanes F, Susen S, Mouquet F, et al. Aldosterone, mortality, and acute ischaemic events in coronary artery disease patients outside the setting of acute myocardial infarction or heart failure. Eur Heart J, 2012; 33, 191-202. doi: 10.1093/eurheartj/ehr176 [34] Swedberg K, Eneroth P, Kjekshus J, et al. Hormones regulating cardiovascular function in patients with severe congestive heart failure and their relation to mortality. CONSENSUS Trial Study Group. Circulation, 1990; 82, 1730-6. doi: 10.1161/01.CIR.82.5.1730 [35] Ter Maaten JM, Damman K, Hanberg JS, et al. Hypochloremia, Diuretic Resistance, and Outcome in Patients With Acute Heart Failure. Circ Heart Fail, 2016; 9, e003109. http://cn.bing.com/academic/profile?id=b6e57a3d3e8286fa7fbc4462d42b01b3&encoded=0&v=paper_preview&mkt=zh-cn [36] Neuberg GW, Miller AB, O'Connor CM, et al. Diuretic resistance predicts mortality in patients with advanced heart failure. Am Heart J, 2002; 144, 31-8. doi: 10.1067/mhj.2002.123144 [37] Fihn SD, Gardin JM, Abrams J, et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the diagnosis and management of patients with stable ischemic heart disease:a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol, 2012; 60, e44-164. doi: 10.1016/j.jacc.2012.07.013 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 2059
- HTML全文浏览量: 553
- PDF下载量: 108
- 被引次数: 0

 Quick Links
Quick Links