

 下载:
下载:


-
Chronic pharyngitis (CP) is a prevalent medical condition in the field of otorhinolaryngology characterized by persistent inflammation of the pharyngeal mucosa, submucosa, and lymphoid tissue. The etiology of CP is multifactorial, with noninfectious factors such as personal habits (e.g., smoking and drinking), allergic factors, voice overuse, and gastric reflux, as well as infectious agents such as bacteria and viruses playing a significant role[1]. The clinical presentation of CP varies among individuals but commonly includes various uncomfortable symptoms, such as recurrent hoarseness, irritating cough, and sore throat. Despite not being lethal, CP is a stubborn, recurrent, and difficult-to-cure disease that seriously affects the patients’ quality of life.
Atmospheric temperature is an important meteorological factor that plays a critical role in human health. In recent years, a substantial body of literature has emerged, linking ambient temperature to an elevated risk of upper respiratory diseases, including bronchiectasis and allergic rhinitis[2,3]. Our previous study demonstrated a positive correlation between air pollutants, such as SO2 and NO2, and an increase in the number of daily outpatients with CP[4]. However, the effect of ambient temperature on outpatients with CP has yet to be fully understood. Therefore, this study aimed to develop a time-series model to assess the influence of ambient temperature on outpatients with CP in Xinxiang, China. In addition, we assessed the effects of ambient temperature across different subpopulations.
Daily data on outpatient visits for CP were collected from January 1, 2015 to December 31, 2018, at four hospitals in Xinxiang: Xinxiang Central Hospital, Third Affiliated Hospital of Xinxiang Medical University, Xinxiang First People’s Hospital, and Xinxiang Second People’s Hospital. These hospitals are geographically distributed across the four administrative areas of Xinxiang, providing comprehensive coverage of the local population. Hence, the data collected on CP were deemed representative. The diagnosis of CP was made by physicians at these hospitals and was encoded as J31.2 in the electronic medical records, in accordance with the International Classification of Diseases, tenth revision (ICD-10). During the aforementioned timeframe, the China Meteorological Data Sharing Service System (http://data.cma.cn/) was used to obtain the daily mean temperature and relative humidity readings for Xinxiang, and the daily levels of air pollutants (SO2 and NO2) were gathered from four predetermined monitoring stations situated throughout the region. The geographical distribution of the four hospitals, fixed monitoring stations, and detailed data-cleaning procedures have been previously described[4].
To account for the impact of ambient temperature on health outcomes, particularly with respect to its lag and non-linear effects, a distributed lag non-linear model (DLNM) was employed to establish a cross-basis for temperature at varying lag days. This approach has been widely used to study meteorological factors affecting health outcomes[5]. In addition, a generalized additive model (GAM) was employed to evaluate the association between ambient temperature and outpatients with CP. Given the low incidence rate of the disease and the overdispersion of daily outpatient values, we utilized a quasi-Poisson regression. The present study’s model accounts for the influence of long-term trends, the day of the week, and humidity. Additionally, a study by Zhao established a clear association between air pollutants, specifically SO2 and NO2, and an increased outpatient risk of CP[4]. The current study incorporated these pollutants into the model to control for potential confounding effects. The fundamental formula for the model is as follows:
Log[E(Yt)] = α + cb (temperature, 5, lag, 3) + ns (humidity, 3) + ns (time, 7/year) + ns (SO2, 3) + ns (NO2, 3) + DOW + holiday
Yt signifies the total number of CP outpatient visits from the four hospitals at day t and E(Yt) signifies the estimated CP outpatient visits at day t, and α means the intercept. cb represents the cross-basis function for daily ambient temperature and the degree as 5; the degrees of freedom (df) for lag space is 3; ns indicates a natural cubic spline for non-linear variables: humidity and air pollution (SO2, NO2) with the df is 3; 7 df/year was used to control for long-term trends and seasonality. Furthermore, DOW refers to the day of the week, and holiday refers to a public holiday. After establishing the final model, the relative risks and 95% confidence intervals (CIs) were calculated using the P50 temperature as the reference. Additionally, we defined temperatures below the 1st percentile as cold, above the 99th percentile as heat, and the 25th and 75th percentiles as moderate cold and moderate heat, respectively. Previous studies used a maximum lag of 21 days to simultaneously estimate the non-linear and delayed effects of ambient temperature on respiratory diseases[5]. We also selected a maximum lag of 21 days to explore the acute and long-term effects of ambient temperature on CP. Then, the immediate and cumulative lag relative risks (RR) and 95% confidence intervals (CI) of 0–7 days, 0–14 days, and 0–21 days for CP were calculated. Finally, stratified analysis by sex (male, female) and age (< 15, 15–65, and ≥ 65 years) was also performed in our study. In addition, we conducted sensitivity analyses: (1) we selected longer lag times of up to 28 days to evaluate the stability of our model, and (2) for the smoothness of time trends, we chose alternative df values from six to ten per year. All statistical analyses were performed using the R statistical project (‘mgcv’ package for GAMs and ‘dlnm’ package for DLNMs). A two-sided P-value < 0.05 was considered statistically significant.
A total of 62,823 CP hospital outpatient records were collected from January 1, 2015, to December 31, 2018. The statistical descriptions of the daily CP outpatient visits are presented in Supplementary Table S1 (available in www.besjournal.com). The average number of daily CP outpatient visits was 43 (21 males and 22 females). The outpatients were categorized into those aged < 15 (young), 15–64, and ≥ 65 (old) years old, with 15, 32, and 4 cases per day, respectively. Supplementary Table S1 presents the meteorological factors and air pollutants (NO2 and SO2) in Xinxiang during the study period. The daily average temperature and relative humidity were 16 °C and 60%, respectively. The percentiles of temperature, specifically the 1st, 25th, 75th, and 99th percentiles, are denoted as P1, P25, P75, and P99, respectively. These percentiles correspond to temperature values of −2, 7, 25, and 32 °C. The annual average concentrations of NO2 and SO2 were 48 µg/m3 and 33 µg/m3, respectively.
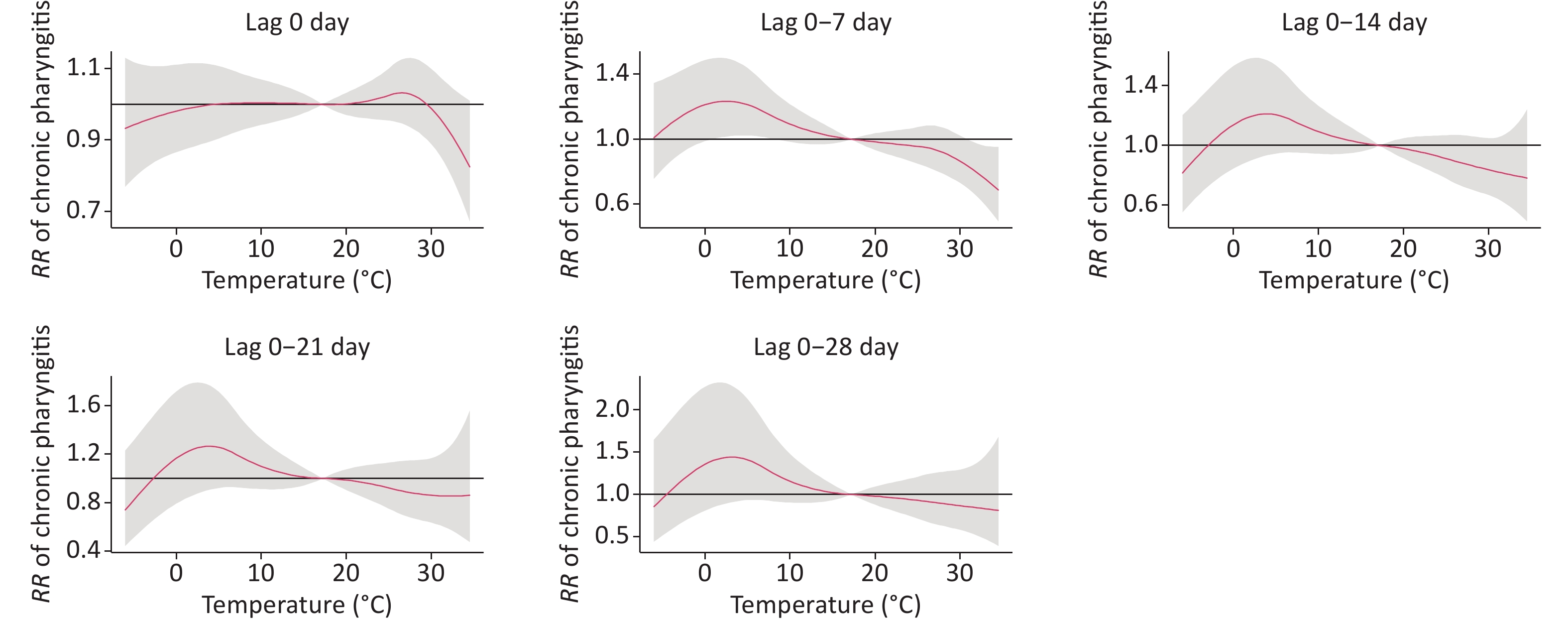
Table 1 shows the relative risks of CP visits corresponding to ambient temperature at different lag times (0, 0–7, 0–14, 0–21, and 0–28 days). Figure 1 presents the exposure-response curves between the temperature and RR of CP visits with different lag times. There was a significant statistical effect of moderate cold (25th percentile, 7 °C) and heat (99th percentile, 32 °C) on outpatient visits for CP with a lag of 0–7 days. In contrast to the median temperature (17 °C), the moderate cold (7 °C) increased the risk of CP visits (RR: 1.17, 95% CI: 1.01–1.34). These results are consistent with those of previous studies. Makinen reported that cold temperatures were associated with increased pharyngitis in Finland[6]. Another study conducted in Shanghai showed that low temperatures increased the incidence of acute pharyngitis[7]. Short-term exposure to low temperatures has also been linked to increased respiratory diseases such as allergic rhinitis and chronic bronchitis[2,3]. However, the mechanisms underlying the influence of low temperatures on chronic pharyngitis remain unclear. One possible reason is that low temperatures are more suitable for bacterial and viral infections. In addition, viral cultivation studies have confirmed that respiratory viruses replicate better at cooler temperatures.
Table 1. Cumulative relative risks of chronic pharyngitis outpatient visits associated with daily mean temperature among selected cutoff points
Lag effects P1 relative to median temperature
RR (95% CI)P25 relative to median temperature
RR (95% CI)P75 relative to median temperature
RR (95% CI)P99 relative to median temperature
RR (95% CI)Lag 0 1.03 (0.97−1.09) 1.01 (0.97−1.05) 1.00 (0.97−1.04) 0.95 (0.90−1.00) Lag 0−7 1.13 (0.91−1.42) 1.17 (1.01−1.34)* 0.96 (0.85−1.07) 0.79 (0.65−0.97)* Lag 0−14 1.00 (0.73−1.37) 1.16 (0.95−1.42) 0.91 (0.78−1.07) 0.81 (0.61−1.08) Lag 0−21 0.98 (0.64−1.49) 1.20 (0.93−1.55) 0.92 (0.75−1.13) 0.86 (0.59−1.25) Lag 0−28 1.14 (0.65−2.00) 1.31 (0.93−1.85) 0.93 (0.72−1.21) 0.84 (0.52−1.38) Note. P1, P25, P50, P75, and P99 refer to 1st, 25th, 50th, 75th, and 99th percentiles of temperature. *P < 0.05. 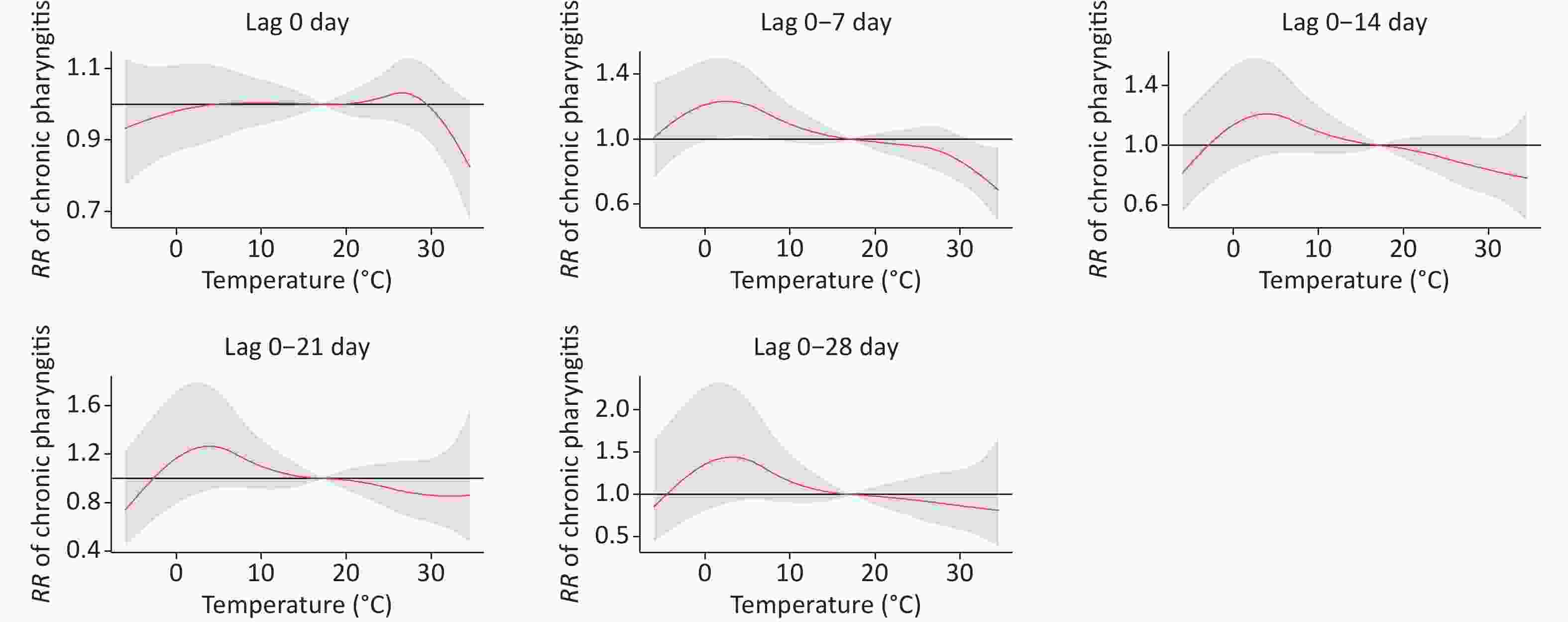
Figure 1. The exposure–response curves between the temperature and the RR of CP visits with different lag 0–28 (reference temperature at 17 °C).
In addition, we also found that the heat (32 °C) had a reduced risk (RR: 0.79, 95% CI: 0.65–0.97) compared to the median temperature (17 °C). However, evidence linking ambient temperature to chronic pharyngitis is scarce, and we compared our findings with those for other respiratory diseases. In studies conducted in Lanzhou, extreme heat has been associated with an increased risk of pneumonia and COPD[5]. However, another study conducted in Shanghai found no positive association between hospital visits for chronic bronchitis and heat[2]. It was difficult to elaborate on the exact reason for this heterogeneity. The most likely reasons for this may be the disease type and age-group composition ratio. Naina et al. reported that the mean age of patients with CP was 34.8 years (range, 18–65 years)[8]; however, it is plausible that older people have a high prevalence of lower respiratory diseases, such as COPD and pneumonia, and are thus more susceptible to extreme temperatures[5]. In addition, the average annual temperature, relative humidity, and socioeconomic status in Xinxiang, which is in the hinterlands of China, were significantly different from those in Shanghai and South India. Further studies are required to investigate the underlying mechanisms.
Figure 2 shows the exposure-response curves stratified by age and sex in a lag of 0–7 days. Females were sensitive to heat; that is, our results demonstrated that females were more protected from heat-associated visits than males. Given that few studies have investigated this relationship, we compared our findings with those of other respiratory diseases. However, these results are inconsistent with our findings. One study in Beijing observed that heat waves introduced an additional risk to respiratory emergency department visits in females (RR = 1.166, 95% CI: 1.007–1.349)[9]. Chai et al. also found that females with respiratory diseases were more susceptible to extreme temperatures than males[5]. Diverse climatic conditions may affect the relationship between temperature and disease. Furthermore, we speculate that geographical conditions may contribute to this variance. In addition, the 15–64 age group had a significant statistical difference according to heat temperature compared to the < 15 and ≥ 65 age groups. Few studies have examined the influence of temperature on CP visit effects based on age group. Thus, we compared our findings with those of other respiratory diseases. However, the study results have been inconsistent. Chai et al. showed that high temperatures displayed significant acute and short-term harmful effects on respiratory diseases in patients aged 15–59 years in Lanzhou[5]. Anderson et al. reported a positive effect of heat on respiratory hospitalization in older individuals in the US[10]. Further research is required to explore these potential differences.

Figure 2. The exposure-response curves between daily ambient temperature and RRs of daily outpatient visits stratified by age and gender.
For the sensitivity analysis, we constructed a model with longer lag times of up to 28 days and examined the effects of various dfs ranging from 6 to 10 each year on the smoothness of seasonality. The results were not substantially changed (data not shown), indicating the robustness of the model.
Our study has several limitations. First, we obtained the records of CP outpatients from four hospitals in Xinxiang; therefore, the CP diagnosis criteria might have been slightly different, and there might have been misdiagnosed records. In addition, climatic data for the CP population exposure were obtained from only one fixed meteorological monitoring station; thus, exposure measurement errors are inevitable. Third, we did not consider etiological data at the individual level, which might have affected the temperature exposure levels and health outcomes. Fourth, the conclusions may only be representative of a single city; hence, more work involving more cities is needed to verify the effect of temperature on CP. Finally, we investigated the correlation between chronic pharyngitis and temperature using the GAM and DLMN models. Further validation of the actual impact of population exposure and animal experimentation is warranted in future research.
In summary, our analysis has demonstrated a significant correlation between moderate cold (7 °C) and an elevated risk of CP outpatient visits, while high temperatures (32 °C) are associated with a reduced risk. These findings have substantial implications for formulating efficient cold risk-management strategies from a public health perspective. To the best of our knowledge, this study represents one of the few investigations that have directly examined the relationship between ambient temperatures and CP outpatient visits. Consequently, our results provide novel evidence of the impact of temperature on human health.
-
LIANG Wen Juan: Investigation, writing the original draft, and funding acquisition; CHAO Ling: Methodology and data Validation; ZHAO Xiang Mei: Methodology, software, and visualization; ZHANG Rong Guang: Writing-review; ZHAO Rui Qing: Investigation, methodology, and validation; WU Wei Dong: Writing-review; SONG Jie: Funding acquisition, supervision writing, editing, and project administration.
doi: 10.3967/bes2023.126
Ambient Temperature and Risk of Outpatient Chronic Pharyngitis Visits: A Time-series Analysis in Xinxiang, China
-
The authors declare no conflict of interest.
This study was an observational study. The Research Ethics Committee of the Xinxiang Medical University confirmed that no ethical approval was required.
注释:1) Competing Interests: 2) Ethics Approval and Consent to Participate: -
Figure 1. The exposure–response curves between the temperature and the RR of CP visits with different lag 0–28 (reference temperature at 17 °C).
Figure 2. The exposure-response curves between daily ambient temperature and RRs of daily outpatient visits stratified by age and gender.
Table 1. Cumulative relative risks of chronic pharyngitis outpatient visits associated with daily mean temperature among selected cutoff points
Lag effects P1 relative to median temperature
RR (95% CI)P25 relative to median temperature
RR (95% CI)P75 relative to median temperature
RR (95% CI)P99 relative to median temperature
RR (95% CI)Lag 0 1.03 (0.97−1.09) 1.01 (0.97−1.05) 1.00 (0.97−1.04) 0.95 (0.90−1.00) Lag 0−7 1.13 (0.91−1.42) 1.17 (1.01−1.34)* 0.96 (0.85−1.07) 0.79 (0.65−0.97)* Lag 0−14 1.00 (0.73−1.37) 1.16 (0.95−1.42) 0.91 (0.78−1.07) 0.81 (0.61−1.08) Lag 0−21 0.98 (0.64−1.49) 1.20 (0.93−1.55) 0.92 (0.75−1.13) 0.86 (0.59−1.25) Lag 0−28 1.14 (0.65−2.00) 1.31 (0.93−1.85) 0.93 (0.72−1.21) 0.84 (0.52−1.38) Note. P1, P25, P50, P75, and P99 refer to 1st, 25th, 50th, 75th, and 99th percentiles of temperature. *P < 0.05.  下载: 导出CSV
下载: 导出CSV
-
[1] Murray RC, Chennupati SK. Chronic streptococcal and non-streptococcal pharyngitis. Infect Disord Drug Targets, 2012; 12, 281−5. doi: 10.2174/187152612801319311 [2] Huang F, Zhao A, Chen RJ, et al. Ambient temperature and outpatient visits for acute exacerbation of chronic bronchitis in Shanghai: a time series analysis. Biomed Environ Sci, 2015; 28, 76−9. [3] Kim H, Kim H, Lee JT. Assessing the cold temperature effect on hospital visit by allergic rhinitis in Seoul, Korea. Sci Total Environ, 2018; 633, 938−45. doi: 10.1016/j.scitotenv.2018.03.166 [4] Zhao XM, Lu MX, An Z, et al. Acute effects of ambient air pollution on hospital outpatients with chronic pharyngitis in Xinxiang, China. Int J Biometeorol, 2020; 64, 1923−31. doi: 10.1007/s00484-020-01980-3 [5] Chai GR, He H, Su YN, et al. Lag effect of air temperature on the incidence of respiratory diseases in Lanzhou, China. Int J Biometeorol, 2020; 64, 83−93. doi: 10.1007/s00484-019-01795-x [6] Mäkinen TM, Juvonen R, Jokelainen J, et al. Cold temperature and low humidity are associated with increased occurrence of respiratory tract infections. Respir Med, 2009; 103, 456−62. doi: 10.1016/j.rmed.2008.09.011 [7] Yu PC, Sun AR, Xue C, et al. Outdoor temperature as an independent risk factor for acute pharyngitis incidence: a preliminary study. Ear Nose Throat J, 2021; 1455613211057637. [8] Naina P, Anandan S, Mathews SS, et al. Chronic pharyngitis: role of atypical organisms: a case control study from South India. Otolaryngol Head Neck Surg, 2012; 147, 894−9. doi: 10.1177/0194599812457344 [9] Song XP, Wang SG, Li TS, et al. The impact of heat waves and cold spells on respiratory emergency department visits in Beijing, China. Sci Total Environ, 2018; 615, 1499−505. doi: 10.1016/j.scitotenv.2017.09.108 [10] Anderson GB, Dominici F, Wang Y, et al. Heat-related emergency hospitalizations for respiratory diseases in the Medicare population. Am J Respir Crit Care Med, 2013; 187, 1098−103. doi: 10.1164/rccm.201211-1969OC -

 点击查看大图
点击查看大图
图(2) / 表ll (1)
计量
- 文章访问数: 172
- HTML全文浏览量: 78
- PDF下载量: 28
- 被引次数: 0

 Quick Links
Quick Links