

 下载:
下载:



-
A causal relationship has been reported between the average population salt (sodium chloride) intake and the increased risk of stroke and cardiovascular and cerebrovascular diseases in some epidemiological and clinical studies. The World Health Organization has recommended that a sodium intake of < 2 g/day is preventive against cardiovascular disease, although the current intake is in excess in most countries. Among the various methods for evaluating dietary salt intake, 24 h urinary sodium and potassium excretion are considered the gold standard biomarkers for use as surrogates of salt intake[1]. However, it encounters problems such as high participant burden, high analysis cost, and susceptibility to insufficient or excessive urine collection. Additionally, the dietary composition of an individual often changes. Therefore, it is more reasonable to estimate habitual intake using urine data collected over several days. Therefore, there is an urgent need to develop and validate innovative dietary assessment methods.
Wastewater analysis has received a lot of credit in recent years as an efficient method of measuring the consumption of illicit drugs and pharmaceuticals worldwide. Its general principle is as follows[2]: after drugs are metabolized in the human body, their metabolites are excreted in urine or feces and enter domestic wastewater treatment plants (WWTPs). The per capita use of drugs can be deduced by analyzing the concentrations of metabolites in raw wastewater.
Urine is an important source of potassium in domestic wastewater. Friedler et al. indicated that urine, feces, and greywater accounted for 71%, 22%, and 7% of the proportional potassium loads in domestic wastewater, respectively[3]. In addition to dietary sources, sodium is found in laundry detergents, tap water, and mouth cleansers. However, data on the proportion of dietary sodium to total sodium in domestic wastewater are not available. Assuming that the dietary intake of sodium and potassium can be assessed based on their excretion in urine, the wastewater analysis method may provide a feasible way to evaluate their use. Theoretically, the dietary consumption of sodium and potassium can be evaluated by eliminating the contribution of non-dietary sources. The population served by municipal WWTPs can be estimated using the concentration of biomarkers in raw wastewater, such as ammonia nitrogen (NH4-N)[2]. Sampling was convenient and inexpensive. Continuous sampling can be performed for days, weeks, months, or even years to reflect changes in eating habits over time.
This study was a preliminary attempt to apply a wastewater analysis method to estimate dietary sodium and potassium use. By measuring their concentrations in influent wastewater from 24 WWTPs in 20 Chinese cities, the spatial consumption trends of sodium and potassium and their association with socioeconomics were determined.
Influent wastewater was collected between August 2018 and March 2019 from 24 WWTPs in Beijing, Yinchuan, Shenyang, Xi’an, Changzhou, Chengdu, Kunming, Baoding, Hefei, Guiyang, Harbin, Huhhot, Zhengzhou, Guangzhou, Qingdao, Weihai, Jinan, Dalian, Changchun, and Jinzhou. In Guiyang, Dalian, and Changchun, two or three WWTPs were selected, while one WWTP was selected from the other cities. Automated 24 h continuous sampling was performed with two replicates per WWTP. After collection, the samples were acidified to pH 2 using hydrochloric acid, immediately transported to the laboratory and stored at –20 °C until analysis. There was no rain or snow two days before sample collection to avoid the influence of rain or snow-melting agents. The details of the sampling information are provided in Supplementary Table S1 (available in www.besjournal.com). Tap water from residential areas was collected simultaneously without further processing. Flame atomic absorption spectrometry was used to detect sodium and potassium concentrations according to the National Standard (GB/T 11904-1989). Blank water was analyzed using the aforementioned method. The anionic surfactant concentration was measured using the methylene blue spectrophotometric method (GB 7494-37).
Table S1. Concentration of sodium and potassium in wastewater and tap water, concentration of NH4-N and parameters of each WWTP
WWTPs CNH4-N, mean ±
SDa (mg L−1)Populationb
(× 104)
Flow rate
(× 104 m3 day−1)Concentration in wastewater
mean ± SDc (mg L−1)Concentration in tap water
mean ± SD (mg L−1)Sodium Potassium Sodium Potassium QD 21.7 ± 0.3 50.6 14.0 126.2 ± 10.1 31.6 ± 1.9 20.2 ± 1.1 6.2 ± 0.2 JN 51.2 ± 1.0 21.3 2.5 102.4 ± 8.5 35.6 ± 1.1 11.0 ± 0.3 5.3 ± 0.4 WH 63.6 ± 1.1 42.4 4.0 128.3 ± 9.3 49.0 ± 3.2 33.1 ± 1.7 16.3 ± 0.9 HF 26.1 ± 0.6 130.0 30.0 89.4 ± 7.6 24.1 ± 1.1 8.6 ± 0.6 7.7 ± 0.2 CD 21.4 ± 0.2 17.8 5.0 81.4 ± 3.4 22.1 ± 2.0 < LOD 4.3 ± 0.1 HAR 9.5 ± 0.2 4.8 3.0 97.6 ± 2.9 62.9 ± 5.8 1.7 ± 0.1 5.9 ± 0.3 XA 40.2 ± 1.3 133.0 20.0 84.6 ± 3.6 30.8 ± 2.0 10.2 ± 0.6 3.9 ± 0.2 BJ 50.6 ± 0.3 337.0 40.0 86.5 ± 4.5 28.8 ± 3.2 12.1 ± 0.4 6.2 ± 0.3 ZZ 26.7 ± 0.1 88.9 20.0 104.3 ± 9.9 31.6 ± 1.5 24.3 ± 1.0 6.5 ± 0.2 HUH 22.3 ± 0.2 14.8 4.0 146.0 ± 10.2 14.7 ± 1.3 8.8 ± 0.6 9.5 ± 0.6 CZ 29.9 ± 0.8 80.3 16.1 82.0 ± 4.6 21.6 ± 0.2 < LOD 3.9 ± 0.1 GY-1 8.9 ± 0.01 9.0 6.1 44.0 ± 1.3 19.3 ± 0.3 0.2 ± 0.02 7.0 ± 0.4 GY-2 12.3 ± 0.2 16.4 8.0 28.0 ± 3.5 13.3 ± 0.6 0.2 ± 0.02 7.0 ± 0.4 GZ 26.1 ± 0.8 217.0 50.0 69.6 ± 7.1 17.5 ± 0.2 2.1 ± 0.1 6.5 ± 0.5 YC 23.9 ± 0.1 39.9 10.0 151.6 ± 9.0 25.2 ± 0.9 20.4 ± 0.7 3.7 ± 0.1 BD 8.3 ± 0.02 4.1 3.0 136.3 ± 8.5 14.8 ± 0.4 76.6 ± 1.2 10.5 ± 0.7 CC-1 19.6 ± 2.0 127.3 39.0 65.9 ± 3.6 21.9 ± 0.7 2.4 ± 0.9 6.4 ± 0.1 CC-2 9.5 ± 0.9 14.3 9.0 71.9 ± 4.0 21.3 ± 0.7 2.4 ± 0.9 6.4 ± 0.1 SY 34.4 ± 1.4 229.1 40.0 37.3 ± 1.3 8.1 ± 0.5 18.3 ± 1.6 6.7 ± 0.2 DL-1 32.8 ± 7.6 64.8 12.0 98.2 ± 5.2 23.8 ± 1.1 13.4 ± 1.0 10.8 ± 0.3 DL-2 28.3 ± 9.1 38.5 8.2 95.1 ± 6.7 19.9 ± 0.9 13.4 ± 1.0 10.8 ± 0.3 DL-3 35.5 ± 11.7 17.7 3.0 95.1 ± 3.4 25.9 ± 1.0 13.4 ± 1.0 10.8 ± 0.3 JZ 32.1 ± 1.3 158.0 26.0 149.5 ± 9.8 27.9 ± 1.2 15.0 ± 0.8 10.9 ± 0.4 KM 15.3 ± 0.02 77.8 30.5 39.6 ± 1.1 16.0 ± 0.8 < LOD 7.9 ± 0.2 Note. a: CNH4-N: concentration of NH4−N in wastewater, mg L−1; SD: standard deviation. b: Population was calculated from equation (3) based on the concentration of NH4−N. c: Concentration of sodium and potassium in wastewater from all sources. WWTPs, wastewater treatment plants; Beijing (BJ), Yinchuan (YC), Shenyang (SY), Xi’an (XA), Changzhou (CZ), Chengdu (CD), Kunming (KM), Baoding (BD), Hefei (HF), Guiyang (GY), Harbin (HRB), Huhhot (HUH), Zhengzhou (ZZ), Guangzhou (GZ), Qingdao (QD), Weihai (WH), Jinan (JN), Dalian (DL), Changchun (CC), and Jinzhou (JZ). Based on the wastewater analysis methodology, the consumption of sodium and potassium can be calculated using Equations (1) and (2), respectively.
$$ {{m}}_{{N}{a}\left({K}\right)}=\frac{{{C}}_{{N}{a}\left({K}\right),{ }{i}{ }\times {{F}}_{{i}}\times {{f}}_{{N}{a}\left({K}\right)}}}{{{P}}_{{i}}} $$ (1) $$ {L}{o}{a}{d}=\frac{{{{C}}_{{N}{a}\left({K}\right),{ }{i}}\times {F}}_{{i}}}{{{P}}_{{i}}}$$ (2) where mNa(K), i is the consumption, CNa(K), i is the concentration of sodium or potassium in WWTPi, Fi is the flow rate of raw wastewater for WWTPi. fNa(K) is the correction factor and a value of 1 for fNa(K) is used in this equation. The population (Pi) served by WWTPi was estimated using the method described in our previous study[2].
The Kolmogorov−Smirnov algorithm was used to determine whether the data had a normal distribution. If applicable, a one-way analysis of variance was used for multiple comparisons. All calculations and statistical tests were performed using SPSS statistics and Origin 8.0 software, and a P-value < 0.05 was considered statistically significant.
Sodium and potassium presented in wastewater with concentrations of 28.0−151.6 mg/L and 8.1−62.9 mg/L, respectively (Supplementary Table S1). They are a collection of sodium and potassium consumed by humans from all sources, including both dietary and non-dietary sources. Dietary sources include the consumption of food, drinks, and additives containing sodium or potassium in cooking and dishes. According to an epidemiological study in 2014, the three main contributors to the dietary sources of sodium intake in the US population were added during the production and preparation of commercial foods (71%), naturally occurring in foods (14%), and during the preparation of meals at home (11%)[4]. Other sources such as dietary supplements, home tap water, and non-prescription antacids contributed the least to sodium intake (< 0.5% each). Non-dietary sources were primarily referred to as the contribution of domestic water, such as tap water and anionic surfactants, which were the largest and most widely used classes of surfactants. Therefore, the sodium and potassium concentrations in tap water around each WWTP and anionic surfactant content were measured.
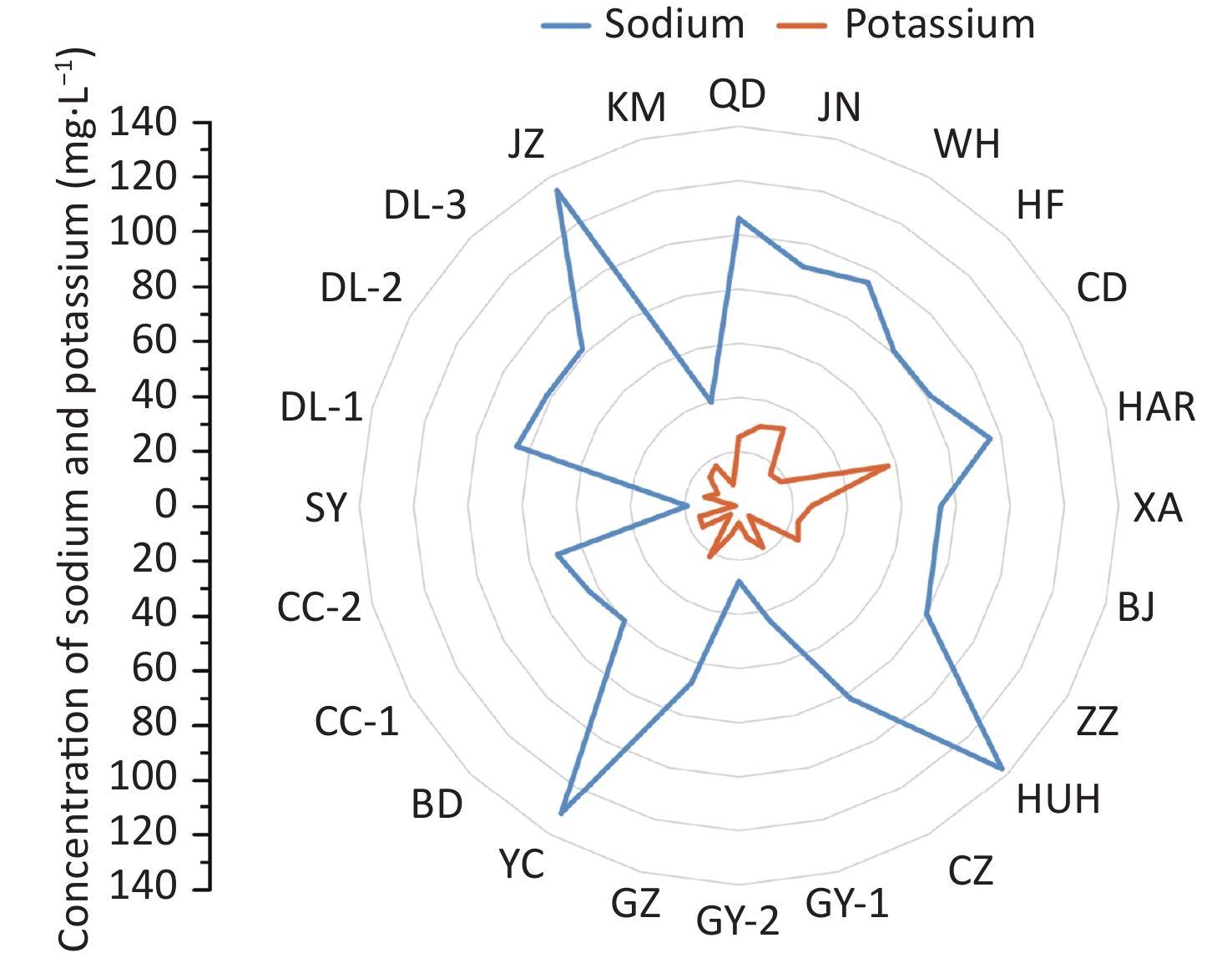
The sodium and potassium in the wastewater originating from anionic surfactants ranged from below limit of detection (LOD) to 1.67 mg/L, accounting for 0%–1.3% of total concentrations. Therefore, the contribution of surfactants was negligible. Sodium and potassium were detected in tap water with concentrations of < LOD−76.6 mg/L and 3.6−16.3 mg/L, accounting for 0%–56% and 0%–83% of the total concentration in the wastewater, respectively. Therefore, the content of sodium and potassium in the wastewater after excluding the sources of tap water and surfactants were in a range of 18.9−137.1 mg/L and 1.4−56.9 mg/L, respectively (Figure 1).
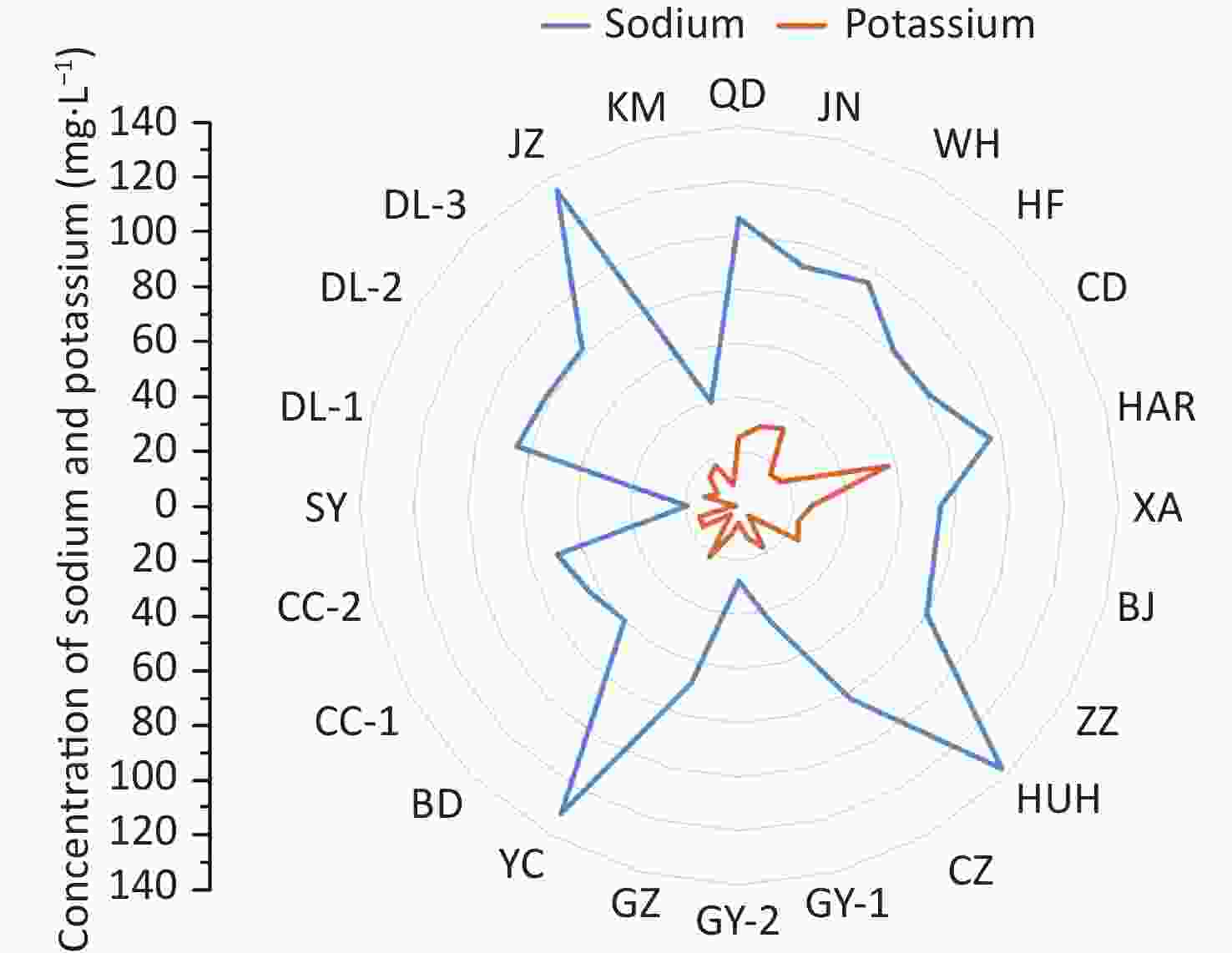
Figure 1. Concentrations of sodium and potassium in wastewater from dietary sources in 24 wastewater treatment plants. Beijing (BJ), Yinchuan (YC), Shenyang (SY), Xi’an (XA), Changzhou (CZ), Chengdu (CD), Kunming (KM), Baoding (BD), Hefei (HF), Guiyang (GY), Harbin (HRB), Huhhot (HUH), Zhengzhou (ZZ), Guangzhou (GZ), Qingdao (QD), Weihai (WH), Jinan (JN), Dalian (DL), Changchun (CC) and Jinzhou (JZ).
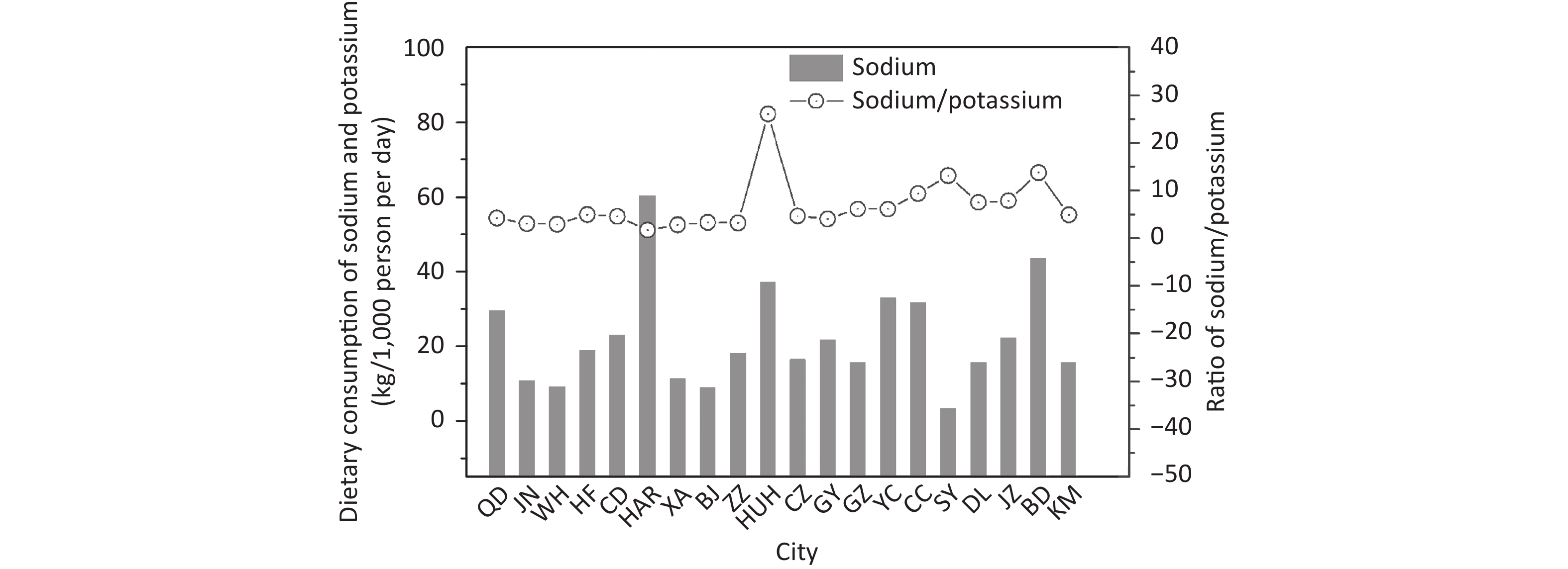
NH4-N has been reported to be a reliable biomarker for this population. Therefore, its concentration was used to estimate the population served by WWTPs, and it was found in a range of 8.3−63.6 (median, 26.1) mg/L in 24 WWTPs (Supplementary Table S1). The population served by WWTPs ranged from 0.04 million in Baoding to 3.37 million in Beijing. Dietary sodium uses in 20 cities ranged from 3.3−60.3 (median, 18.3; mean, 22.2) kg/1,000 person per day, the minimum and maximum appeared in Shenyang and Harbin, respectively (Figure 2). Furthermore, notable positive associations were observed between sodium and potassium consumption (unadjusted r = 0.639, P < 0.001), consistent with a previous prospective epidemiological cohort study[5]. Meanwhile, the gram-to-gram ratio (sodium vs. potassium) was 1.7−26.0 with a median value of 4.7. Sodium consumption was much higher than potassium consumption, which may be because modern diets often contain excessive sodium and relatively low potassium.
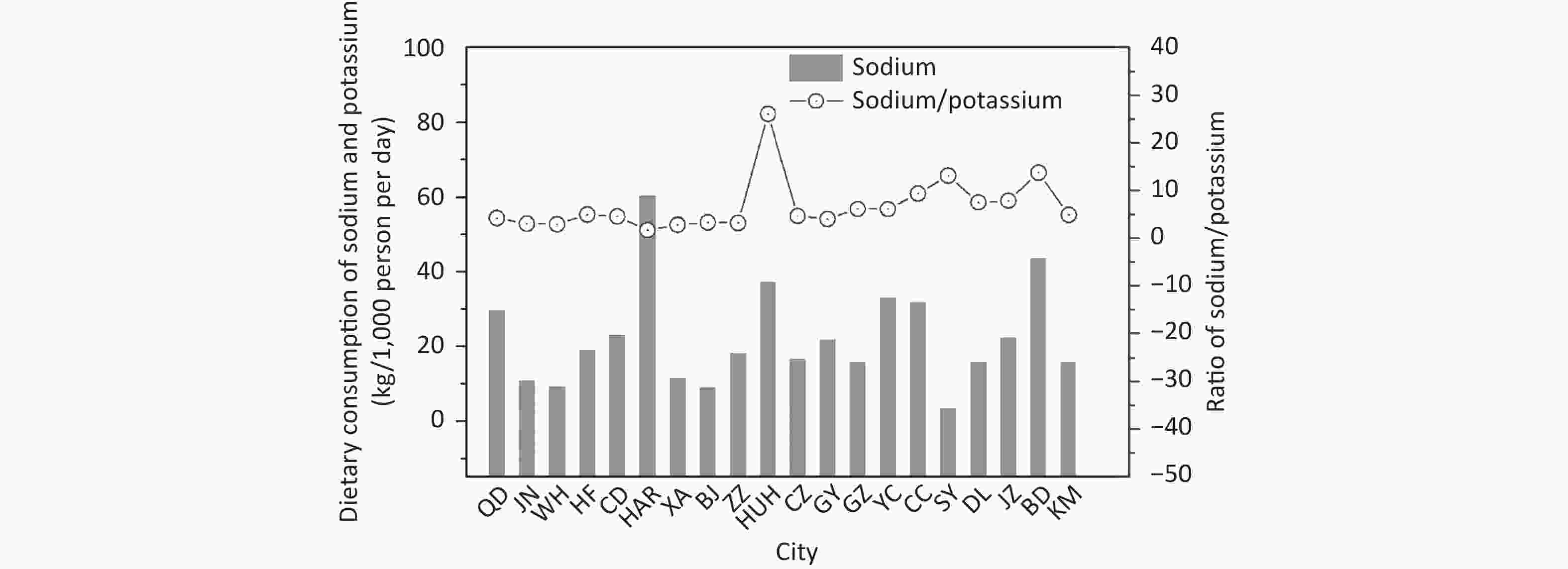
Figure 2. Dietary consumption of sodium and potassium in 20 Chinese cities. Beijing (BJ), Yinchuan (YC), Shenyang (SY), Xi’an (XA), Changzhou (CZ), Chengdu (CD), Kunming (KM), Baoding (BD), Hefei (HF), Guiyang (GY), Harbin (HRB), Huhhot (HUH), Zhengzhou (ZZ), Guangzhou (GZ), Qingdao (QD), Weihai (WH), Jinan (JN), Dalian (DL), Changchun (CC), and Jinzhou (JZ).
High sodium consumption (> 30 kg/1,000 person per day) was found in Harbin (60.3 kg/1,000 person per day), followed by Baoding (43.4 kg/1,000 person per day), Huhhot (37.1 kg/1,000 person per day), Yinchuan (32.9 kg/1,000 person per day) and Changchun (31.2 kg/1,000 person per day). Meanwhile, the cities of Weihai, Beijing, and Shenyang had a low sodium consumption (< 10 kg/1,000 persons per day). It should be noted that the sodium consumption estimated by the wastewater analysis approach was a summary of all dietary sources, containing a portion of the ingested and excreted sodium, as well as a portion that was directly discarded in the sewer through leftover disposal and dishes. According to national surveys in China, the average daily sodium intake in 2012 was estimated as 3.8 g (3.5−4.3 g in urban areas, 4.0−4.9 g in rural areas)[6]. This intake may have been largely underestimated due to the high subjectivity and uncertainty of the dietary questionnaires[7].
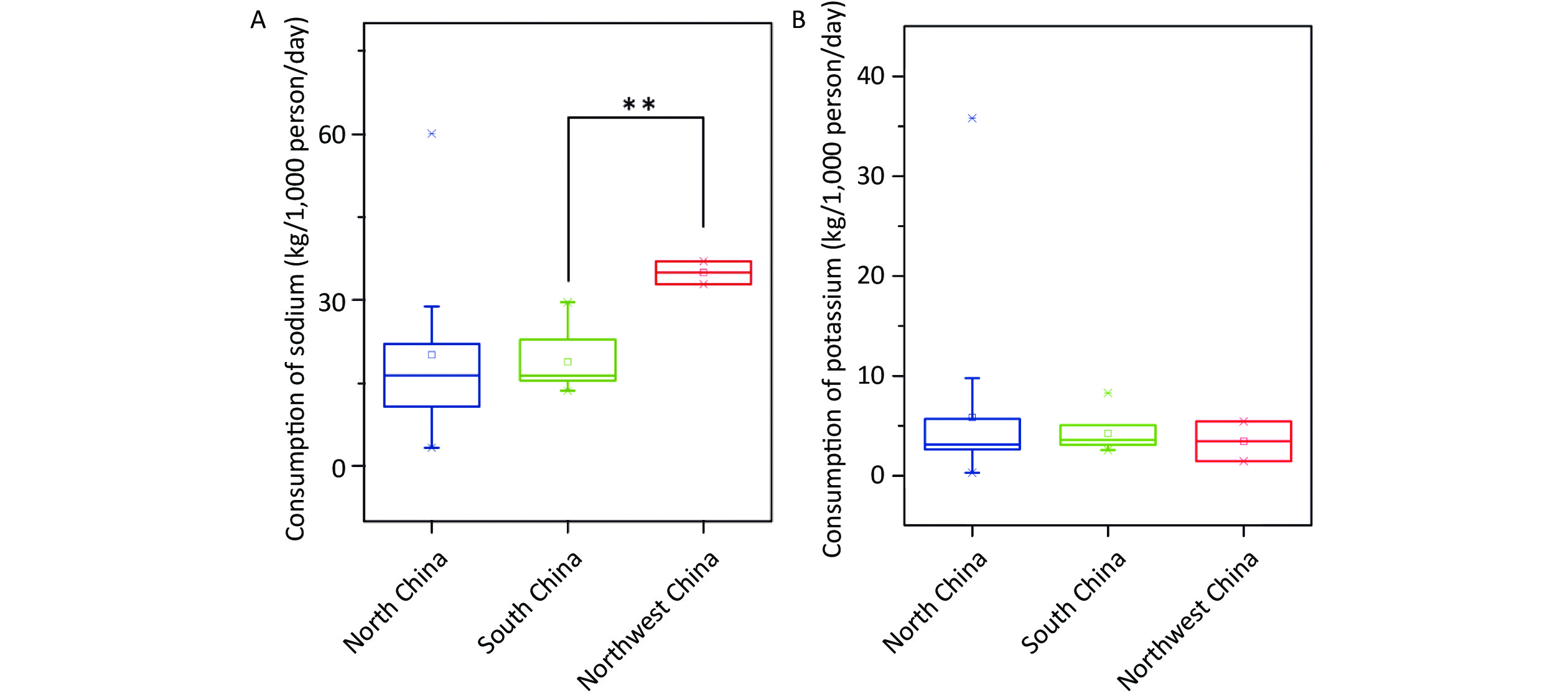
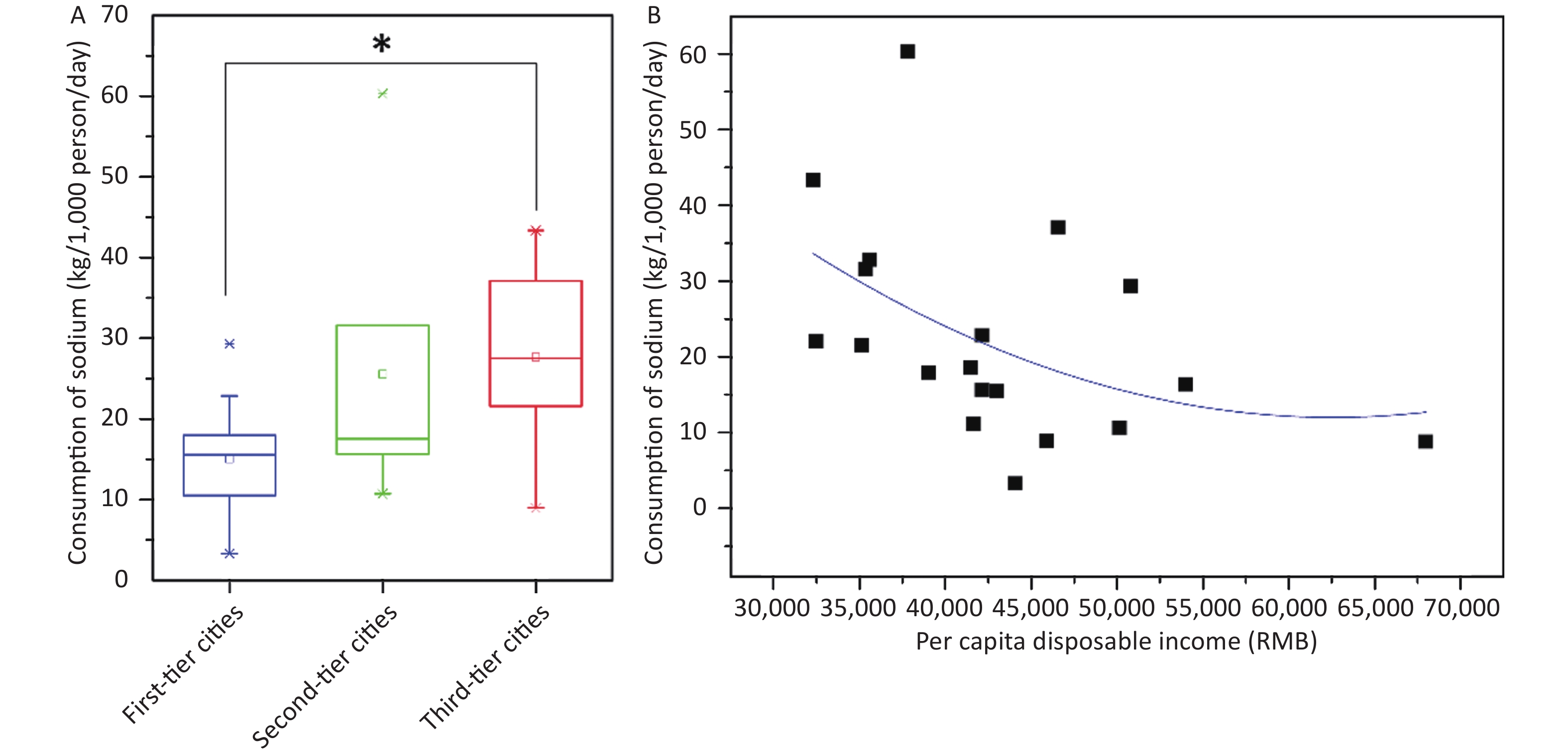
Dietary sodium and potassium consumption were predicted in three regions (North China, Northwest China, and South China). Sodium consumption in Northwest China (mean, 35.0 kg/1,000 person per day) was significantly higher than in the southern region (mean, 18.9 kg/1,000 person per day) (t-test, P < 0.01) (Figure 3A). In terms of potassium consumption, no significant differences were observed between the regions (Figure 3B). The association between dietary sodium consumption and socioeconomic status was also investigated. Considering the level of economic development and the size of the city, Beijing, Guangzhou, Chengdu, Xi’an, Shenyang, Qingdao, Zhengzhou, and Kunming are first-tier cities. Dalian, Hefei, Harbin, Jinan, Changchun, and Changzhou were included as second-tier cities. Guiyang, Huhhot, Yinchuan, Weihai, Baoding, and Jinzhou are classified as third (or more)-tier cities[8]. As shown in Supplementary Figure S1 (available in www.besjournal.com), sodium consumption showed a clear association with the city grade. The third (or more)-tier cities had a higher sodium consumption (range, 9.0−43.3; mean, 28.9 kg/1,000 person per day) than the first-tier cities (range, 3.3−29.3; mean, 15.6 kg/1,000 person/day) (t-test, P < 0.05). Additionally, there was a negative correlation between sodium consumption per capita and disposable income per capita in 20 cities (unadjusted r = −0.449, P < 0.05).
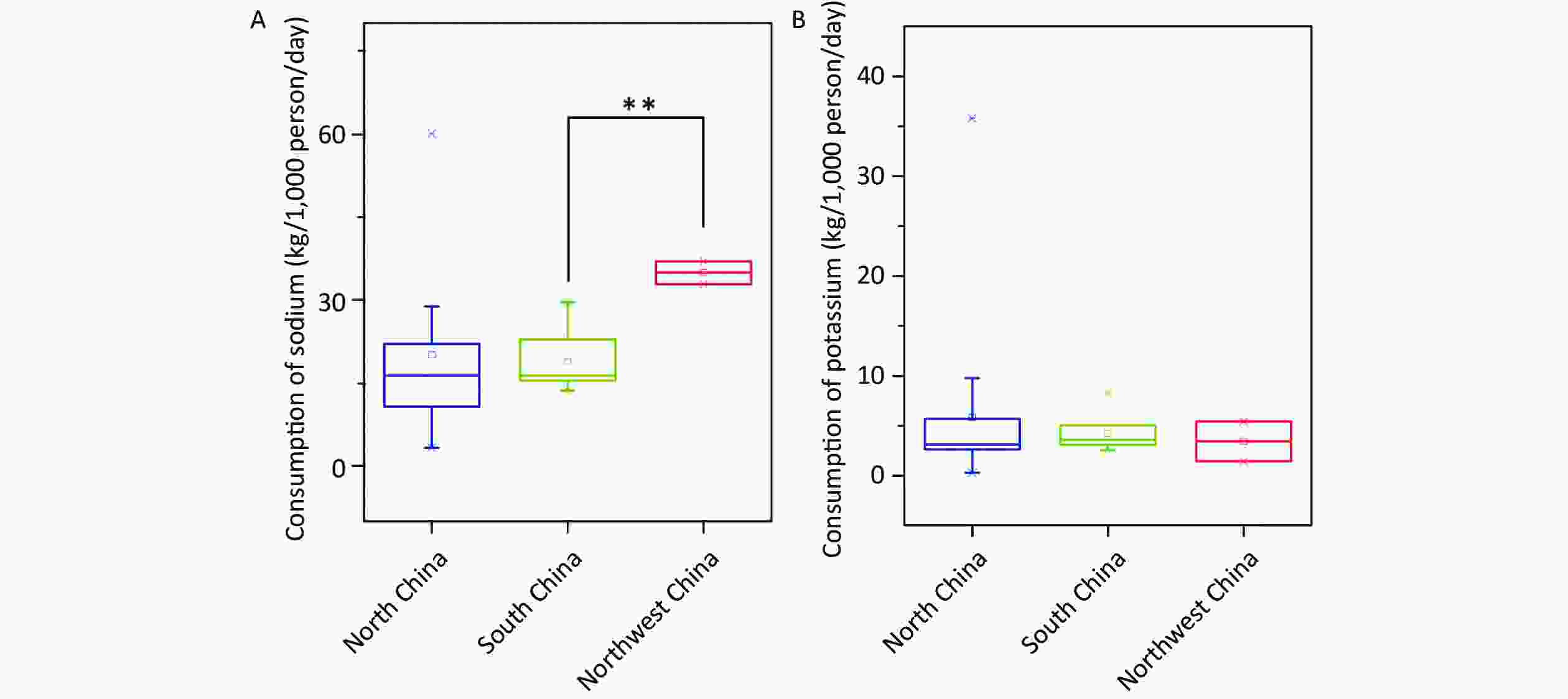
Figure 3. Distribution of spatial variation in the dietary consumption of sodium (A) and potassium (B) in China. **Indicates a significant difference (P < 0.01).
The higher sodium consumption in Northwest China and developed cities in China could be due to differences in socioeconomic status and food culture. Socioeconomic differences can affect eating habits, which, in turn, leads to unequal health. According to food habits surveys between 1985 and 1999 in 15 European countries, a higher socioeconomic status was positively related to higher consumption of fruits and vegetables[9]. In China, dietary habits, cooking methods, and food types vary significantly between regions. The southern region has a balanced diet pattern with a high intake of rice, vegetables, eggs, fish, and meat[10]. Meanwhile, in Northwest China, people are accustomed to eating diets rich in meat, especially bacon, dried meat, dairy products, and lacking fresh fruits and vegetables. Similarly, compared to less developed cities, people in developed cities were more likely to contact health information and optimize their eating habits.
This study preliminarily explored the feasibility of estimating dietary sodium and potassium consumption using wastewater analysis. Compared to traditional methods (questionnaires or biological fluid analysis), this approach has the advantage of convenient sampling and providing data in near real-time. Additionally, it can show spatial and temporal variations at the community or country level. Combining population health or disease information has the potential to aid in evaluating correlations (or hypotheses) between salt consumption and public health in future studies. There are some limitations to this study. First, the small sample size. Therefore, it is necessary to increase the number of wastewater samples to reflect the actual consumption level accurately. Second, the results only reflected the total amount of dietary sodium, including the parts that were ingested and those that were not ingested by the human body. To obtain the intake values, it may be necessary to build models based on large amounts of data. Furthermore, the discharge of industrial wastewater may increase the sodium content of domestic wastewater, and this interference must be eliminated.
The authors have no conflicts of interest to declare.
-
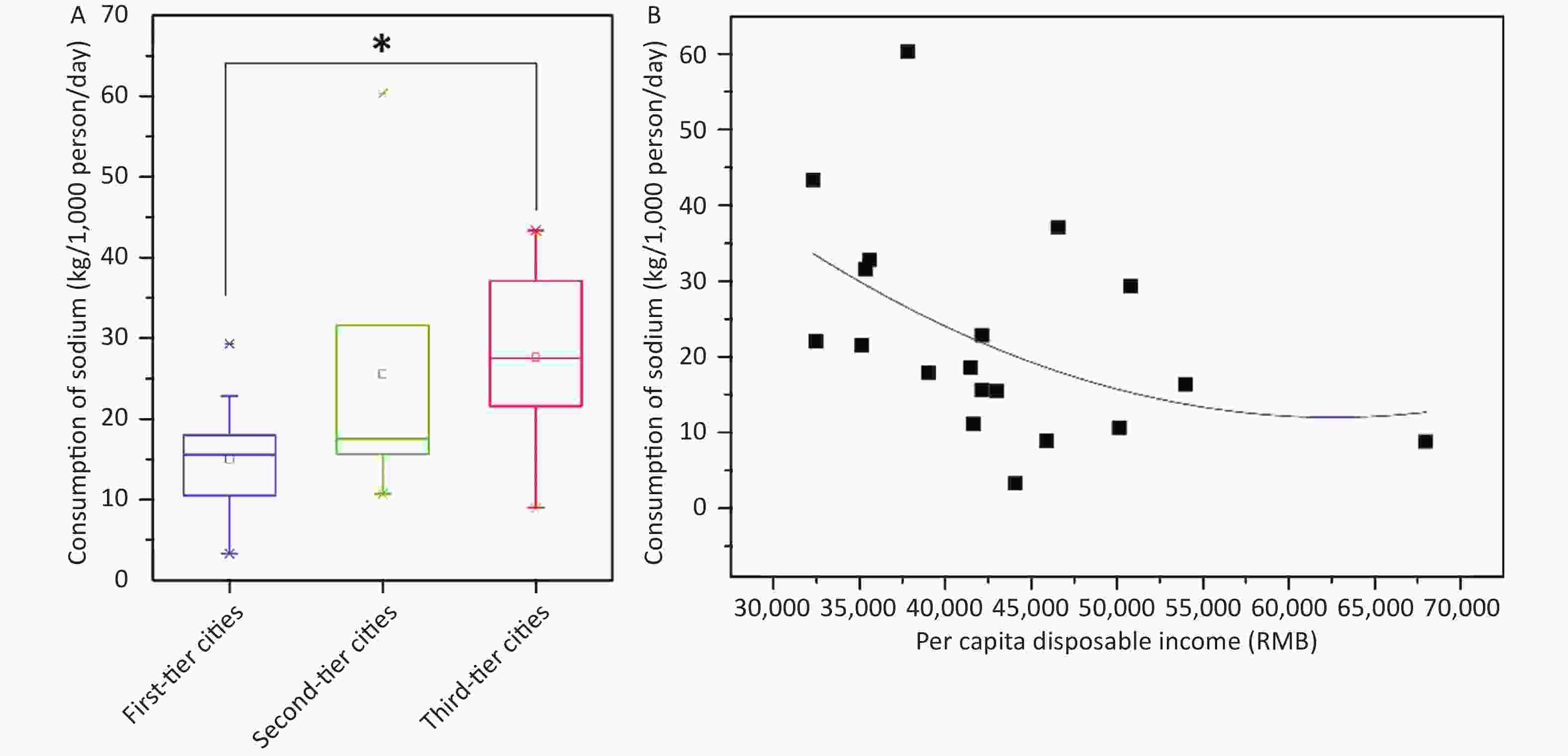
Figure S1. The association of daily consumption of sodium with city grades (A) and per capita disposable income (B). *Indicates a significant difference (P < 0.05).
doi: 10.3967/bes2024.013
Assessing Dietary Consumption of Sodium and Potassium in China through Wastewater Analysis
-
-
Figure 1. Concentrations of sodium and potassium in wastewater from dietary sources in 24 wastewater treatment plants. Beijing (BJ), Yinchuan (YC), Shenyang (SY), Xi’an (XA), Changzhou (CZ), Chengdu (CD), Kunming (KM), Baoding (BD), Hefei (HF), Guiyang (GY), Harbin (HRB), Huhhot (HUH), Zhengzhou (ZZ), Guangzhou (GZ), Qingdao (QD), Weihai (WH), Jinan (JN), Dalian (DL), Changchun (CC) and Jinzhou (JZ).
Figure 2. Dietary consumption of sodium and potassium in 20 Chinese cities. Beijing (BJ), Yinchuan (YC), Shenyang (SY), Xi’an (XA), Changzhou (CZ), Chengdu (CD), Kunming (KM), Baoding (BD), Hefei (HF), Guiyang (GY), Harbin (HRB), Huhhot (HUH), Zhengzhou (ZZ), Guangzhou (GZ), Qingdao (QD), Weihai (WH), Jinan (JN), Dalian (DL), Changchun (CC), and Jinzhou (JZ).
Figure 3. Distribution of spatial variation in the dietary consumption of sodium (A) and potassium (B) in China. **Indicates a significant difference (P < 0.01).
S1. The association of daily consumption of sodium with city grades (A) and per capita disposable income (B). *Indicates a significant difference (P < 0.05).
S1. Concentration of sodium and potassium in wastewater and tap water, concentration of NH4-N and parameters of each WWTP
WWTPs CNH4-N, mean ±
SDa (mg L−1)Populationb
(× 104)
Flow rate
(× 104 m3 day−1)Concentration in wastewater
mean ± SDc (mg L−1)Concentration in tap water
mean ± SD (mg L−1)Sodium Potassium Sodium Potassium QD 21.7 ± 0.3 50.6 14.0 126.2 ± 10.1 31.6 ± 1.9 20.2 ± 1.1 6.2 ± 0.2 JN 51.2 ± 1.0 21.3 2.5 102.4 ± 8.5 35.6 ± 1.1 11.0 ± 0.3 5.3 ± 0.4 WH 63.6 ± 1.1 42.4 4.0 128.3 ± 9.3 49.0 ± 3.2 33.1 ± 1.7 16.3 ± 0.9 HF 26.1 ± 0.6 130.0 30.0 89.4 ± 7.6 24.1 ± 1.1 8.6 ± 0.6 7.7 ± 0.2 CD 21.4 ± 0.2 17.8 5.0 81.4 ± 3.4 22.1 ± 2.0 < LOD 4.3 ± 0.1 HAR 9.5 ± 0.2 4.8 3.0 97.6 ± 2.9 62.9 ± 5.8 1.7 ± 0.1 5.9 ± 0.3 XA 40.2 ± 1.3 133.0 20.0 84.6 ± 3.6 30.8 ± 2.0 10.2 ± 0.6 3.9 ± 0.2 BJ 50.6 ± 0.3 337.0 40.0 86.5 ± 4.5 28.8 ± 3.2 12.1 ± 0.4 6.2 ± 0.3 ZZ 26.7 ± 0.1 88.9 20.0 104.3 ± 9.9 31.6 ± 1.5 24.3 ± 1.0 6.5 ± 0.2 HUH 22.3 ± 0.2 14.8 4.0 146.0 ± 10.2 14.7 ± 1.3 8.8 ± 0.6 9.5 ± 0.6 CZ 29.9 ± 0.8 80.3 16.1 82.0 ± 4.6 21.6 ± 0.2 < LOD 3.9 ± 0.1 GY-1 8.9 ± 0.01 9.0 6.1 44.0 ± 1.3 19.3 ± 0.3 0.2 ± 0.02 7.0 ± 0.4 GY-2 12.3 ± 0.2 16.4 8.0 28.0 ± 3.5 13.3 ± 0.6 0.2 ± 0.02 7.0 ± 0.4 GZ 26.1 ± 0.8 217.0 50.0 69.6 ± 7.1 17.5 ± 0.2 2.1 ± 0.1 6.5 ± 0.5 YC 23.9 ± 0.1 39.9 10.0 151.6 ± 9.0 25.2 ± 0.9 20.4 ± 0.7 3.7 ± 0.1 BD 8.3 ± 0.02 4.1 3.0 136.3 ± 8.5 14.8 ± 0.4 76.6 ± 1.2 10.5 ± 0.7 CC-1 19.6 ± 2.0 127.3 39.0 65.9 ± 3.6 21.9 ± 0.7 2.4 ± 0.9 6.4 ± 0.1 CC-2 9.5 ± 0.9 14.3 9.0 71.9 ± 4.0 21.3 ± 0.7 2.4 ± 0.9 6.4 ± 0.1 SY 34.4 ± 1.4 229.1 40.0 37.3 ± 1.3 8.1 ± 0.5 18.3 ± 1.6 6.7 ± 0.2 DL-1 32.8 ± 7.6 64.8 12.0 98.2 ± 5.2 23.8 ± 1.1 13.4 ± 1.0 10.8 ± 0.3 DL-2 28.3 ± 9.1 38.5 8.2 95.1 ± 6.7 19.9 ± 0.9 13.4 ± 1.0 10.8 ± 0.3 DL-3 35.5 ± 11.7 17.7 3.0 95.1 ± 3.4 25.9 ± 1.0 13.4 ± 1.0 10.8 ± 0.3 JZ 32.1 ± 1.3 158.0 26.0 149.5 ± 9.8 27.9 ± 1.2 15.0 ± 0.8 10.9 ± 0.4 KM 15.3 ± 0.02 77.8 30.5 39.6 ± 1.1 16.0 ± 0.8 < LOD 7.9 ± 0.2 Note. a: CNH4-N: concentration of NH4−N in wastewater, mg L−1; SD: standard deviation. b: Population was calculated from equation (3) based on the concentration of NH4−N. c: Concentration of sodium and potassium in wastewater from all sources. WWTPs, wastewater treatment plants; Beijing (BJ), Yinchuan (YC), Shenyang (SY), Xi’an (XA), Changzhou (CZ), Chengdu (CD), Kunming (KM), Baoding (BD), Hefei (HF), Guiyang (GY), Harbin (HRB), Huhhot (HUH), Zhengzhou (ZZ), Guangzhou (GZ), Qingdao (QD), Weihai (WH), Jinan (JN), Dalian (DL), Changchun (CC), and Jinzhou (JZ).  下载: 导出CSV
下载: 导出CSV
-
[1] GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet, 2019; 393, 1958−72. doi: 10.1016/S0140-6736(19)30041-8 [2] Zheng QD, Lin JG, Pei W, et al. Estimating nicotine consumption in eight cities using sewage epidemiology based on ammonia nitrogen equivalent population. Sci Total Environ, 2017; 590-591, 226-32. [3] Friedler E, Butler D, Alfiya Y. Wastewater composition. In: Larsen T, Udert K, Linert J. Source Separation and Decentralization for Wastewater Management. IWA Publishing. 2013. [4] Harnack LJ, Cogswell ME, Shikany JM, et al. Sources of sodium in US adults from 3 geographic regions. Circulation, 2017; 135, 1775−83. doi: 10.1161/CIRCULATIONAHA.116.024446 [5] O'Donnell M, Mente A, Rangarajan S, et al. Joint association of urinary sodium and potassium excretion with cardiovascular events and mortality: prospective cohort study. BMJ, 2019; 364, l772. [6] Yu DM, He YN, Fang HY, et al. Salt intake among Chinese adults in 2010-2012. Chin J Prev Med, 2016; 50, 217−20. (In Chinese) [7] Leiba A, Vald A, Peleg E, et al. Does dietary recall adequately assess sodium, potassium, and calcium intake in hypertensive patients? Nutrition, 2005; 21, 462-6. [8] Ranking of Cities's Business Attractiveness 2019. Archicreation, 2019; 106-11. (In Chinese) [9] De Irala-Estévez J, Groth M, Johansson L, et al. A systematic review of socio-economic differences in food habits in Europe: consumption of fruit and vegetables. Eur J Clin Nutr, 2000; 54, 706−14. doi: 10.1038/sj.ejcn.1601080 [10] Song FF, Cho MS. Geography of food consumption patterns between south and North China. Foods, 2017; 6, 34. doi: 10.3390/foods6050034 -
 23103+Supplementary Materials.pdf
23103+Supplementary Materials.pdf

-

 点击查看大图
点击查看大图
计量
- 文章访问数: 625
- HTML全文浏览量: 219
- PDF下载量: 27
- 被引次数: 0

 Quick Links
Quick Links