

 下载:
下载:



-
Gynecological cancer is the most prevalent malignancy among women worldwide. It disrupts the functioning of the female reproductive system and seriously affects their quality of life[1]. Cervical, uterine, and ovarian cancers are the three primary types of gynecological cancers. According to the Global Cancer Statistics 2022, cervical cancer ranks fourth in terms of incidence (6.8%) and mortality (8.1%) in women, and is the most frequently diagnosed cancer and the leading cause of cancer death in low and medium Human Development Index (HDI) regions and in India[2]. Uterine corpus cancer (endometrial cancer) is the sixth most common cancer in women, accounting for 420,242 cases worldwide. The incidence rate of endometrial cancer in the high/very high HDI group was 3.4-fold higher than that in the low/medium HDI[2]. Ovarian cancer is the eighth most diagnosed cancer among women in 2022 and has the highest lethality, accounting for nearly half of all gynecological malignancy deaths[2,3].
In addition to incidence and mortality, survival is an important indicator for cancer burden. Population-based cancer survival statistics provide indicators for the effectiveness of screening, early diagnosis, and treatment, as well as reflect the overall effectiveness of health services[4]. Accurate survival rates not only have broad population-based implications, but also provide patients with a better understanding of the nature and course of the disease, as well as guide clinicians in counseling and management[5]. However, the availability of cancer survival data may be limited in countries or regions with systematic reports of cancer incidence or mortality because of the time gaps that often exist in survival.
Little attention has been paid to the characteristics and long-term trends of gynecological cancer survival in different countries and regions. This systematic review extracted the survival rates of population-based cancer registrations for common gynecological cancers from published articles. The primary aim was to provide a comprehensive analysis of global trends and temporal variations in the survival outcomes of patients with gynecological cancer across different populations or regions between the 1980s and the 2020s.
-
This review was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement (
Supplementary Table S1 , available in www.besjournal.com). A comprehensive search of the PubMed, Web of Science, EMBASE, SinoMed, and Surveillance, Epidemiology, and End Results (SEER) databases was conducted for retrieving related studies published between January 1980 and November 2022. The keywords were as follows: “cervical cancer,” “uterine corpus cancer,” “ovarian cancer,” “survival rate,” “cancer registry”, and “population-based survival analysis” (Appendix S1 , available in www.besjournal.com). The cancer site and histological type were coded according to the International Classification of Diseases or the International Classification of Diseases for Oncology (Supplementary Table S2 , available in www.besjournal.com).A total of 5,055 articles were identified using the search strategy and examined independently by two authors (Xiaohui Zhou and Danni Yang). Studies were included as follows: (a) a population-based survival analysis or from cancer registries, (b) survival rate as outcome, and (c) not assessing overlapping periods and incomplete or unavailable articles. After reviewing the titles and abstracts of the publications, 501 full-text articles were identified. After full-text evaluation, 132 articles were included in the final analysis (Figure 1).
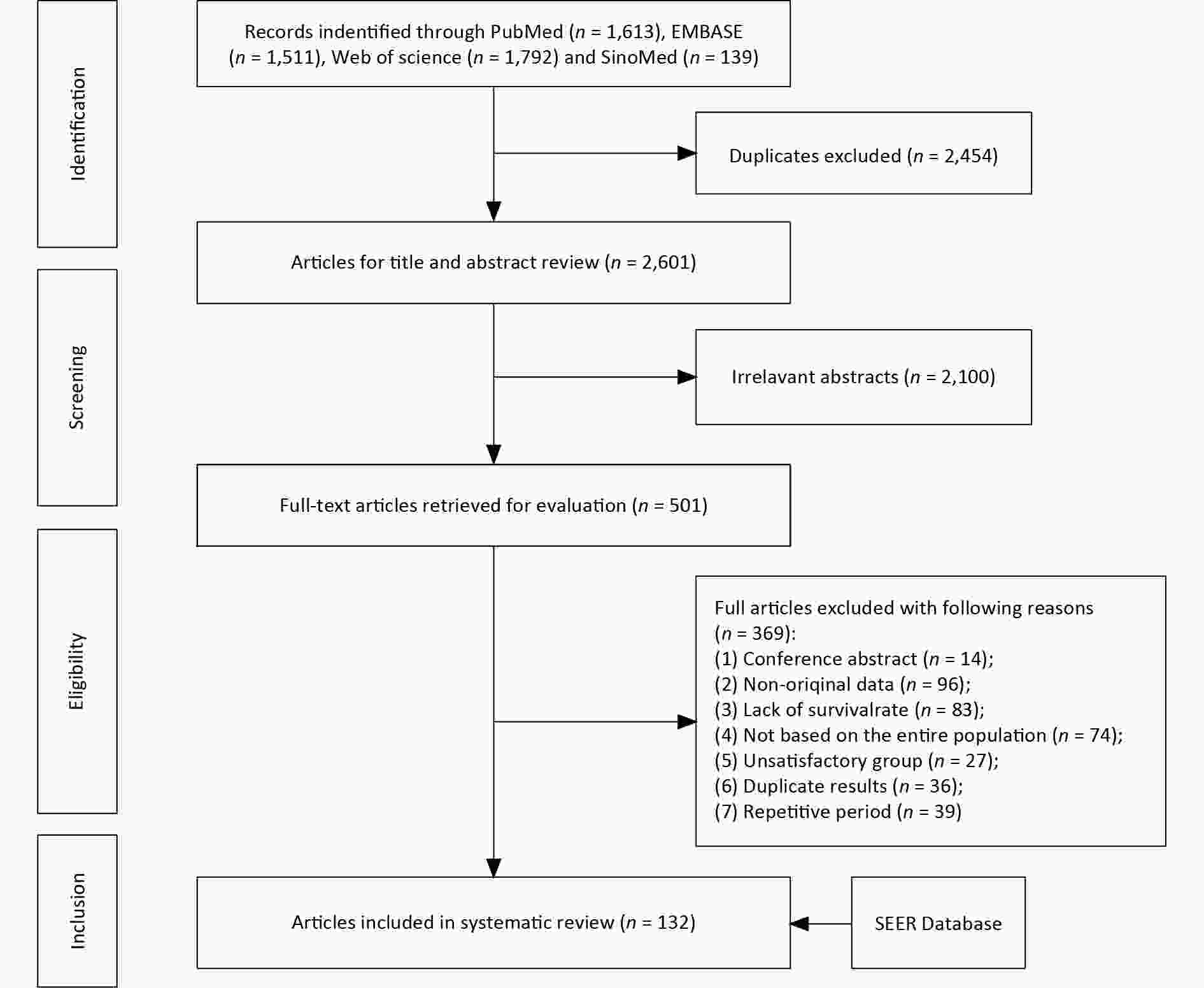
Figure 1. Study selection process.
-
Estimates of observed survival rates (OSR), relative survival rates (RSR), and net survival rates were extracted from published studies. OSR estimates the chance of remaining alive for some years after diagnosis and uses death from all causes as the endpoint. RSR is the ratio of the overall survival of cancer patients to the expected survival of a comparable group of cancer-free individuals[5]. Expected survival, which uses life tables from the general population covered by the cancer registry, can be calculated using the Ederer I, Ederer II, Hakulinen, and Pohar-Perme. The net survival rate is an estimate of the net effect of cancer diagnosis after eliminating the influence of competing causes of death as a cancer prognosis indicator[5]. Both RSR and net survival refer to the cumulative survival probabilities in a given period after excluding other causes of death. Therefore, these two indicators were combined in the present study. The observed relative or net survival rates were primarily utilized and compared across various countries or regions, as well as across different age and sex groups. Age-standardized survival rate was used to compare survival rates between different populations or time periods by adjusting for differences in age distribution. We extracted age-standardized RSRs from each article to further eliminate the impact of age structure on international comparisons. The RSR estimates were age-standardized using weights from different standard populations, including the World, SEER, European, and country-specific Standard Populations. In addition, we collected the results of the statistical tests of all survival trends at different time periods and subgroup-specific 5-year survival rates. EndNote X20 was employed for literature management, while Microsoft Excel 2016 was used for data analysis and graph creation.
-
Table 1 shows the overall 1-, 3-, 5-, and 10-year OSRs of cervical cancer in 20 countries[6-39]. The 5-year OSR was the highest in Anshan, Liaoning, China (2008–2017)[11] at 76.5%, whereas it was the lowest in Uganda, Kampala (1993–1997)[38] at 15.9%. Among the collected countries and regions[9,11,13,14,18,22,27,30,31,33-36,40,41], the 5-year OSRs for endometrial cancer were highest in Finland (1995–1999)[34] and lowest in Sihui, Guangdong, China (1987–1996)[9], at 82.5% and 7.4%, respectively (Table 2). For ovarian cancer[7,8,11,13,14,18,20-22,30,31,33-36,40,42-52], the highest 5-year OSR was observed in Singapore (1988–1992)[18] at 64.0%; in Kampala, Uganda (1988–1997)[51] and Ragusa, Sicily, Italy (1992)[31], the 5-year OSRs were poor, only at 14.1% and 18.1%, respectively (Table 3).
Table 1. Overall observed survival rates (%) of cervical cancer in selected countries and regions during 1980–2017
Continent Country Region Period 1-year 3-year 5-year 10-year Asia China Qidong, Jiangsu[6]* 1982−1986 57.4 37.4 33.0 27.0 1987−1991 57.9 39.0 26.3 20.0 1992−1996 42.4 35.3 29.4 27.1 1997−2001 55.8 41.9 33.7 25.6 2002−2006 65.3 51.5 49.1 45.2 2007−2011 79.3 66.2 62.8 58.2 2012−2016 90.9 77.9 73.6 − Jiulongpo, Chongqing[7] 2008−2013 69.8 42.6 35.3 − Zhejiang[8] 2005−2010 86.9 75.4 70.8 − Sihui, Guangdong[9]* 1987−1996 − − 18.8 − 1997−2006 − − 47.1 − 2007−2009 − − 49.8 − Guizhoua[10] 2013−2015 81.6 66.4 − − Anshan, Liaoningb[11] 2008−2017 91.5 81.0 76.5 − Yangpu, Shanghai[12] 2002−2012 91.2 79.1 75.5 − Shanghai[13] 1988−1991 73.3 53.6 45.4 − Tianjin[14] 1981−1985 55.0 42.0 38.0 − Korea Kangwha[15] 1983−1987 − − 67.1 − Malaysia[16] 2000−2005 94.1 79.3 71.1 − Thailand Khon Kaen[17] 1985−1990 − − 56.8 − Singapore[18] 1983−1987 − − 56.0 − 1988−1992 − − 63.0 − India Bangalore[19] 1982−1989 − − 34.4 − Mumbai[20] 1990−1994 77.0 55.9 44.0 − Dindigul Ambilikkai[21] 2003−2006 − − 35.0 − America Costa Rica[22] 2011−2015 − − 68.0 − Colombia Manizales[23] 2003−2007 80.7 62.1 51.4 − Canada Ontario[24] [25]* 1995−1998 − 71.1 − − 1999−2001 − 75.9 − − 2003−2007 − − 71.0 − Canada British Columbia[26] 1980−1989 89.0 − 73.0 − 1990−1999 91.0 − 73.0 − 2000−2002 90.0 − − − Cuba[27] 1982 − − 44.0 − 1988−1998 74.0 57.0 52.0 − Europe total[28] 1995−1999 84.9 68.0 62.0 − France Martinique[29] 2002−2011 84.1 62.6 55.1 43.3 Switzerland Vaud[30] 1984−1988 − − 55.0 − 1989−1993 − − 62.0 − Italy Sicily, Ragusa[31] 1992 − − 55.8 − Lithuanian[32] 2001−2009 − − 64.1 − Sweden[33] 2011−2015 − − 74.0 − Finland[34] 1995−1999 − − 63.4 − Bulgaria[35]* 1993−1997 − − 49.7 − 2005−2009 − − 54.7 − Germany[36] 2002−2006 − − 65.0 − Australiac [37] 2003−2007 − − 70.3 − 2008−2012 − − 72.1 − Africa Uganda Kampala[38,39] 1995−1997 79.7 52.4 − − 1993−1997 − − 15.9 − Note. −, No report or unavailable in the original article. *Long−term change in survival rates was statistically significant. aOnly three counties in the Guizhou Province are included. bOnly four districts in Anshan, Liaoning Province are included. cSix Australian states/territories (New South Wales, Victoria, Queensland, South Australia, Western Australia, and the Northern Territory) were included in the original article. Table 2. Overall observed survival rates (%) of uterine corpus cancer in selected countries and regions during 1981–2017
Continent County Region Period 1-year 3-year 5-year Asia China Sihui, Guangdong[9]* 1987−1996 − − 7.4 1997−2006 − − 40.0 2007−2009 − − 78.1 Anshan, Liaoningb[11] 2008−2017 94.1 86.9 82.2 Shanghai[13] 1988−1991 89.3 77.6 72.6 Tianjin[14] 1981−1985 65.0 55.0 54.0 Jiulongpo, Chongqing[7] 2008−2013 69.4 48.4 37.6 Singapore[18] 1983−1987 − − 71.0 1988−1992 − − 72.0 Europe[28] 1995−1999 88.3 76.1 69.4 Denmark[91] 2005−2009 − − 73.5 Germany[36] 2002−2006 − − 70.0 Bulgaria[35]* 1993−1997 − − 66.6 2005−2009 − − 69.0 Finland[34] 1995−1999 − − 82.5 Switzerland Vaud[30] 1984−1988 − − 69.0 1989−1993 − − 74.0 Italy Sicily, Ragusa[31] 1992 − − 68.5 America Costa Rica[22] 2011−2015 − − 74.0 Cuba[27] 1982 − − 56.0 1988−1998 77.0 59.0 52.0 Note. *The long-term change trend of survival rate was statistically significant. bOnly four districts in Anshan, Liaoning Province are included. −, No report or unavailable in the original article. Table 3. Overall observed survival rates (%) of ovarian cancer in selected countries and regions during 1981–2017
Continent County Region Period 1−year 3−year 5−year Asia China Qidong, Jiangsu[42] 1982−1986 − − 46.8 1987−1991 − − 30.3 1992−1996 − − 32.7 1997−2000 − − 43.1 Tianjin[14] 1981−1985 47.0 35.0 33.0 Shanghai[13] 1988−1991 65.0 47.2 41.6 Sihui, Guangdong[43] 2003−2005 64.7 58.8 58.8 Zhejiang[8] 2005−2010 76.7 61.0 52.6 Anshan, Liaoningb[11] 2008−2017 80.7 60.7 50.2 Jiulongpo, Chongqing[7] 2008−2013 65.8 44.7 37.5 Singapore[18] 1983−1987 − − 56.0 1988−1992 − − 64.0 India Mumbai[20] 1990−1994 51.0 27.5 23.3 Dindigul Ambilikkai[21] 2003−2006 − − 30.0 Iran[44, 105] 2000−2004
2009-2014−
84.0−
66.061.0
55.0Africa Egypt Alexandria[49] 1988−1997 − − 46.0 Uganda Kampala[38] 1993−1997 − − 14.1 America Costa Rica[22] 2011−2015 − − 52.0 Europe[28,47] 1995−1999 69.1 46.5 37.1 1999−2001 − − 34.8 2002−2004 − − 34.3 2005−2007 − − 35.5 Central Europe[47] 1999−2001 − − 38.7 2002−2004 − − 37.9 2005−2007 − − 37.7 Southern Europe[47] 1999−2001 − − 35.7 2002−2004 − − 33.7 2005−2007 − − 36.7 Eastern Europe[47] 1999−2001 − − 28.9 2002−2004 − − 30.1 2005−2007 − − 32.2 Northern Europe[47] 1999−2001 − − 36.8 2002−2004 − − 37.6 2005−2007 − − 38.8 UK and Ireland[47] 1999−2001 − − 27.8 2002−2004 − − 28.5 2005−2007 − − 29.7 Denmark[48,91] 2000−2002 73.0 − 37.0 2003−2005 69.0 − 36.0 2005−2009 − − 37.7 2009−2011 69.0 − − Italy Sicily, Ragusa[31] 1992 − − 18.1 Bulgaria[35]* 1993−1997 − − 35.4 2005−2009 − − 40.3 France[52] 1989−2010 74.0 − 40.0 Finland[34] 1995−1999 − − 44.6 Germany[36] 2002−2006 − − 37.0 Saarland[45] 1981−1985 − − 29.9 1986−1990 − − 32.4 1991−1995 − − 37.2 Switzerland Vaud[30] 1984−1988 − − 28.0 1989−1993 − − 32.0 Note. *The long-term change trend of survival rate was statistically significant. bOnly four districts in Anshan, Liaoning Province are included. −, No report or unavailable in the original article. Tables 4–6 show the overall relative or net survival rates of the common gynecological cancers worldwide. For cervical cancer[6,8-10,13,14,18-20,22,27,28,30,33,37-39,53-86], the 5-year survival rates were higher in Haining and Jiashan, Zhejiang, China (2011–2014)[54] and in Finland (1995–1999)[66], with 85.8% and 82.3%, respectively; differences remained very wide, with levels as low as 18.2% in Kampala, Uganda (1993–1997)[38]. The highest 10-year survival rate (78.3%) was observed in Korea (1996–2000, 2001–2005)[60]; the lowest rate (28.4%) was observed in Qidong, Jiangsu, China (1987–1991)[6]. For endometrial cancer[9, 13, 14, 18, 22, 27, 28, 30, 36, 53, 54, 57, 59, 64, 65, 67-69, 71, 72, 75-77, 82-84, 86-94], 5-year survival rates were very high in Korea (2015–2019; 89.0%)[59]. Conversely, Tianjin (1981–1985)[14] had the lowest 5-year survival rate (39.3%) (Table 5). For ovarian cancer[8,13,14,18,20,22,30,34,36,38,42, 46,52-54,57,59,62-64,67-69,71,72,75-77,82-84,86,88,91,93,95-105], Korea (2011–2015) ranked first, with a 5-year relative and net survival rate of 64.8%[59]. In Kampala, Uganda (1993–1997)[38], the 5-year rate was low (16.2 %). The range of survival in Asia was wider than that in Europe. In Asia, the 5-year survival rate ranges from 64.5%[59] to 25.4%[20]; in Europe, 5-year survival ranges from 49.0%[100] –32.0%[30].
Table 4. Overall relative/net survival rates (%) of cervical cancer in selected countries and regions during 1980−2019
Continent Country Region Period 1−year 3−year 5−year 10−year Asia China Qidong, Jiangsu[6]* 1982−1986 59.3 41.4 39.2 38.0 1987−1991 59.8 43.0 31.1 28.4 1992−1996 43.6 38.5 34.2 37.9 1997−2001 57.3 45.4 38.6 33.6 2002−2006 66.2 53.8 53.0 52.6 2007−2011 80.2 68.5 66.4 65.0 2012−2016 91.6 79.8 76.8 − Zhejiang[8] 2005−2010 87.5 77.2 73.9 − Guizhoua[10] 2013−2015 84.7 74.3 − − Sihui, Guangdong[9] 2007−2009 − − 50.5 − Shanghai [13] 1988−1991 75.2 57.9 52.1 − Tianjin[14] 1981−1985 56.8 46.6 45.8 − Fujian[53] 2012−2014 − − 68.6 − Haining and Jiashan, Zhejiang[54] 2003−2006 − − 65.6 − 2007−2010 − − 81.7 − 2011−2014 − − 85.8 − Hong Kong[55] 1997−2006 90.6 76.6 71.3 − Taiwan[56] 2004−2008 − − 75.1 − Japand[57] 1993−1996 − − 73.4 − 1997−1999 − − 71.5 − Osaka[58]* 1987−1994 − − 58.6 54.0 1995−2002 − − 56.8 52.7 2003−2010 − − 64.3 59.6 Korea[59,60] 1993−1995 − − 78.3 − 1996−2000 − − 80.3 77.2 2001−2005 − − 81.5 78.3 2006−2010 − − 80.7 77.1 2011−2015 − − 80.3 − 2015−2019 − − 80.5 − Singapore[18] 1983−1987 − − 57.0 − 1988−1992 − − 65.0 − Thailande[61] 1997−2001 78.8 − 55.4 − 2002−2006 80.9 55.5 2008−2012 81.5 − 59.5 − Bangkok[61] 1997−2001 52.5 33.9 2002−2006 75.5 49.0 2008−2012 79.9 56.5 Chiang Mai[61] 1997−2001 83.7 60.8 2002−2006 86.9 61.9 2008−2012 85.3 67.0 Khon Kaen[61] 1997−2001 83.1 57.4 2002−2006 81.0 57.2 2008−2012 79.2 56.1 Lampang[61] 1997−2001 81.7 46.1 2002−2006 83.5 55.0 2008−2012 83.8 64.5 Songkhla[61] 1997−2001 88.8 59.0 2002−2006 79.6 55.3 2008−2012 80.6 55.6 Philippines Metro Manila and Rizal province[62] 1998−2002 − − 45.4 − India Bangalore[19] 1982−1989 − − 38.8 − Mumbai[20] 1990−1994 78.2 58.7 47.7 − Kuwait[63] 2000−2004 84.4 − 57.8 − 2005−2009 88.7 − 73.8 − 2010−2013 86.3 − 71.8 − Turkey[64] 2009 62.0 − Europe[28,65,66] 1981−1983 − − 60.0 − 1983−1985 − − 61.0 1986−1988 − − 62.0 − 1989−1991 − − 64.0 − 1992−1994 − − 63.0 − 1995−1999 86.0 71.0 66.7 − Denmark[66,67] 1983−1985 − − 62.0 − 1986−1988 − − 66.0 − 1989−1991 − − 67.0 − 1992−1994 − − 66.0 − 1994−2003 89.0 − 71.0 − Finland[66,68] 1980−1982 − − 57.5 − 1983−1985 − − 65.0 − 1986−1988 − − 60.0 − 1989−1991 − − 62.0 − 1992−1994 − − 69.0 − 1995−1999 − − 82.3 − Iceland[66] 1983−1985 − − 69.0 − 1986−1988 − − 75.0 − 1989−1991 − − 67.0 − 1992−1994 − − 75.0 − Norway[66] 1983−1985 − − 67.0 − 1986−1988 − − 65.0 − 1989−1991 − − 66.0 − 1992−1994 − − 71.0 − Sweden[33,66,69] 1983−1985 − − 68.0 − 1986−1988 − − 67.0 − 1989−1991 − − 71.0 − 1992−1994 − − 68.0 − 2000−2002 − − 70.9 − 2011−2015 − − 76.0 − England[66,70] 1983−1985 − − 59.0 − 1986−1988 − − 61.0 − 1989−1991 − − 65.0 − 1992−1994 − − 62.0 − 2006−2008 80.4 − 62.2 − 2007−2009 80.8 − − − 2008−2010 80.9 − − − Scotland[66] 1983−1985 − − 54.0 − 1986−1988 − − 58.0 − 1989−1991 − − 61.0 − 1992−1994 − − 60.0 − Wales[66] 1983−1985 − − 62.0 − 1986−1988 − − 59.0 − 1989−1991 − − 59.0 − 1992−1994 − − 58.0 − France[66] 1983−1985 − − 70.0 − 1986−1988 − − 64.0 − 1989−1991 − − 71.0 − 1992−1994 − − 67.0 − Germany[66] 1983−1985 − − 63.0 − 1986−1988 − − 63.0 − 1989−1991 − − 61.0 − 1992−1994 − − 66.0 − Augsburg, Swabia[71] 2005−2011 − 71.4 67.2 − 2005–2007 − 72.1 − − 2008–2010 − 72.2 − − 2011–2013 − 72.3 − − Saarland[72] 1990−1992 − − 61.0 56.6 2000−2002 − − 60.4 55.2 Switzerland[66] 1983−1985 − − 66.0 − 1986−1988 − − 62.0 − 1989−1991 − − 70.0 − 1992−1994 − − 61.0 − Vaud[30,73] 1980−1982 − − 59.0 − 1983−1985 − − 59.0 − 1984−1988 − − 61.0 − 1989−1993 − − 70.0 − Netherlands[66,74]* 1983−1985 − − 66.0 − 1986−1988 − − 69.0 − 1989−1991 − − 72.0 − 1992−1994 − − 66.0 − 2009−2013 − − 73.0 − 2014−2018 − − 74.0 − 1989−2018* − − 71.0 − Eindhoven[75] 1980−2002 − − 70.4 65.1 Italy[66] 1983−1985 − − 60.0 − 1986−1988 − − 62.0 − 1989−1991 − − 63.0 − 1992−1994 − − 67.0 − Umbria[76] 1994−1998 85.0 69.0 64.0 − Slovenia[66] 1983−1985 − − 56.0 − 1986−1988 − − 61.0 − 1989−1991 − − 60.0 − 1992−1994 − − 59.0 − Spain[66] 1983−1985 − − 59.0 − 1986−1988 − − 59.0 − 1989−1991 − − 70.0 − 1992−1994 − − 70.0 − The Czech Republic[77]* 2000−2004 − − 62.1 − 2005−2008 − − 64.2 − Estonia[66,78]* 1983−1985 − − 51.0 − 1986−1988 − − 58.0 − 1989−1991 − − 59.0 − 1992−1994 − − 49.0 − 1995−1999 80.0 − 59.0 − 2000−2004 84.0 − 64.0 − 2005−2009 86.0 − 69.0 − 2010−2014 84.0 − 67.0 − Lithuania[79]* 1990−1994 − − 46.9 − 1995−1999 − − 51.5 − 2000−2004 − − 55.3 − Poland[66] 1983−1985 − − 49.0 − 1986−1988 − − 52.0 − 1989−1991 − − 48.0 − 1992−1994 − − 49.0 − Slovakia[66] 1983−1985 − − 56.0 − 1986−1988 − − 60.0 − 1989−1991 − − 57.0 − 1992−1994 − − 58.0 − America Columbia Cali[80] 1995−1999 77.0 58.0 50.0 47.0 2000−2004 82.0 63.0 60.0 − Cuba[27] 1982 − − 47.0 − 1988−1998 76.0 59.0 56.0 − Costa Rica[22] 2011−2015 − − 69.0 − Canada Manitoba[81] 1985−1989 − − 68.0 − 1990−1994 − − 65.0 − 1995−1999 − − 72.0 − United States[82−84] 1985−1989 − − 66.0 − 2006−2012 − − 68.8 − 2013−2019 − − 67.2 − Oceania Australia New South Wales[85,86] 1982−1986 − − 68.0 − 1987−1991 − − 72.0 − 1993−1996 − − 73.1 − Australiac[37] 2003−2007 − − 75.6 − 2008−2012 − − 76.3 − Africa Uganda Kampala[38,39] 1993−1997 − − 18.2 − 1995−1997 84.1 59.9 − − Note. *The survival rate trend was statistically significant in the original article. aOnly three counties in the Guizhou Province were included in the original article. cSix Australian states/territories (New South Wales, Victoria, Queensland, South Australia,Western Australia, and the Northern Territory) were included in the original article. dSix registries (Miyagi, Yamagata, Niigata, Fukui, Osaka, and Nagasaki) were included in the original article. eFive Thai provinces (Bangkok, Chiang Mai, Khon Kaen, Lampang, and Songkhla) were included in the original article. −, No report or unavailable in the original article. Table 5. Overall relative/net survival rates (%) of uterine corpus cancer in selected countries and regions during 1980−2019
Continent County Regions Period 1−year 3−year 5−year 10−year Asia China Fujian[53] 2012−2014 − − 68.3 − Haining, Jiashan, Zhejiang[54] 2003−2006 − − 75.4 − 2007−2010 − − 85.2 − 2011−2014 − − 87.2 − Shanghai[13] 1988−1991 90.2 80.2 77.0 − Tianjin[14] 1981−1985 66.3 60.5 58.6 − Sihui,Guangdong [9] 2007−2009 − − 79.6 − Japan b [57,87]* 1993−1996 − − 79.5 − 1997−1999 − − 76.8 − 1993−2000 90.4 − 77.7 − 2001−2006 91.8 − 80.2 − Osaka[88,89] 1982−1989 − − 70.7 − 1990−1997 − − 68.5 − 1989−2000 − − − 71.2 Korea[59,90] 1999−2017 − − 88.1 − 1993−1995 − − 82.9 − 1996−2000 − − 82.0 − 2001−2005 − − 84.7 − 2006−2010 − − 86.5 − 2011−2015 − − 87.7 − 2015−2019 − − 89.0 − Singapore[18] 1983−1987 − − 68.0 − 1988−1992 − − 64.0 − Turkey[64] 2009 − − 85.0 − America United States[82−84] 1985−1989 − − 83.0 − 2006−2012 − − 83.4 − 2013−2019 81.0 Costa Rica[22] 2011−2015 − − 78.0 − Cuba[27] 1982 − − 69.0 − 1988−1998 81.0 66.0 62.0 − Oceania Australia New South Wales[86] 1993−1996 − − 79.2 − Europe[28] 1995−1999 90.3 81.7 78.6 − Czech[77] 2000−2004 − − 76.6 − 2005−2008 − − 78.9 − Denmark[67,91] 1994−2003 94.0 − 80.0 − 2005−2009 − − 83.0 − Estonia[92] 1996−2002 − − 75.0 − 2003−2009 − − 73.0 − 2010−2016 − − 79.0 − Finland[68,93] 1985−1994 92.0 − 82.0 82.0 1980−1982 − − 75.9 − 1985−1987 − − 75.1 − 1990−1992 − − 80.3 − Germany[36] 2002−2006 − − 79.0 − Augsburg, Swabia[71] 2005−2011 − 85.4 82.5 − 2005−2007 − 82.7 − − 2008−2010 − 87.3 − − 2011–2013 − 88.0 − − Saarland[72] 1990−1992 − − 81.8 80.8 2000−2002 − − 82.8 81.9 Italy Umbria[76] 1994−1998 92.0 81.0 79.0 − Netherlands[83,94] 1985−1989 − − 75.2 − 1989−1993 − − 77.0 − 1994−1998 − − 78.0 − 1999−2003 − − 79.0 − 2004−2008 − − 80.0 − Eindhoven[75] 1980−2002 − − 81.2 79.1 Sweden[65,69] 1981−1983 − − 75.0 − 1984−1986 − − 75.0 − 1987−1989 − − 73.0 − 2000−2002 − − 85.3 − Switzerland Vaud[30] 1984−1988 − − 78.0 − 1989−1993 − − 84.0 − Note. *The survival rate trend was statistically significant in the original article. −, No report or unavailable in the original article. Table 6. Overall relative/net survival rates(%) of ovarian cancer in selected countries and regions during 1980–2019
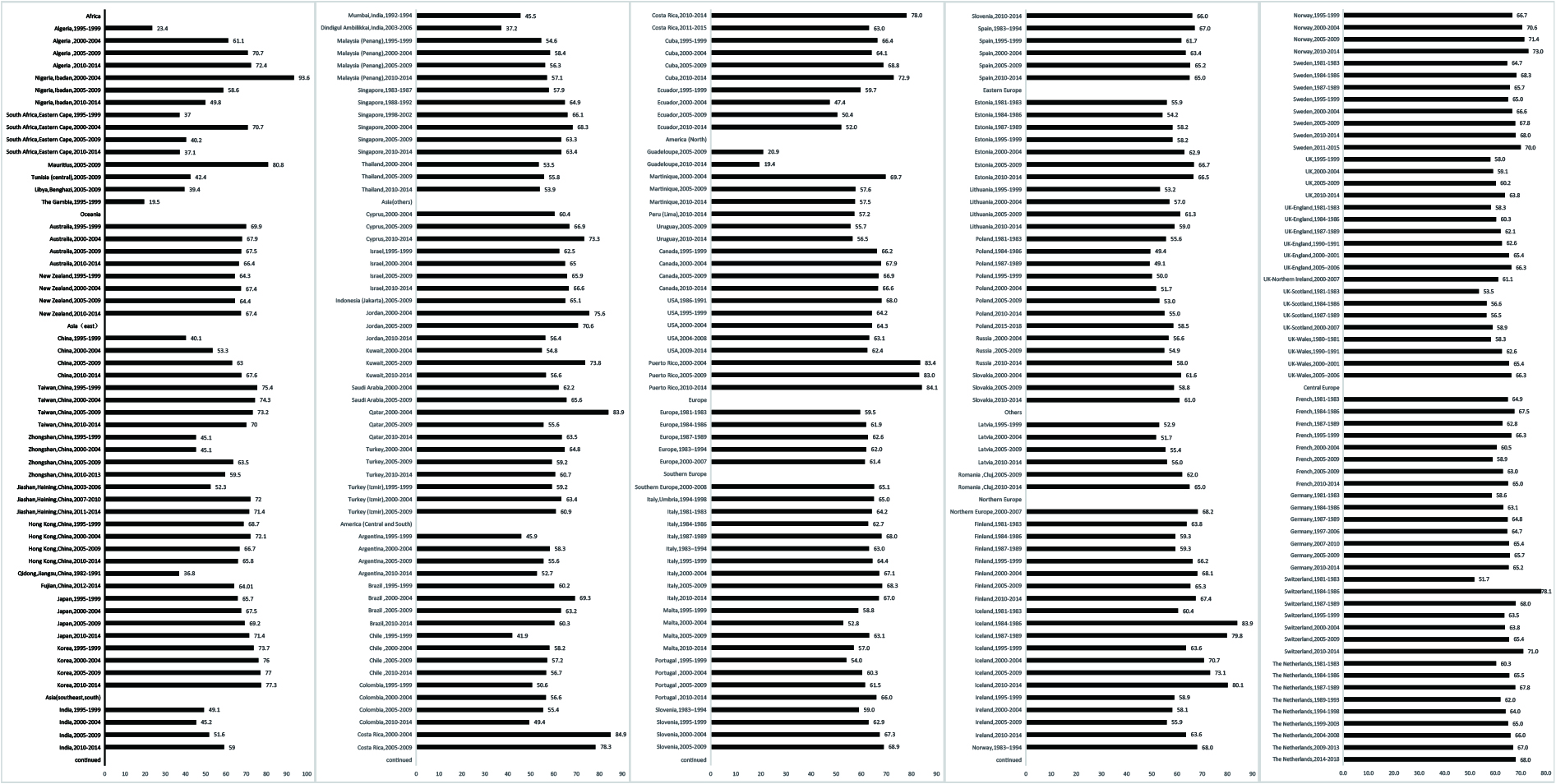
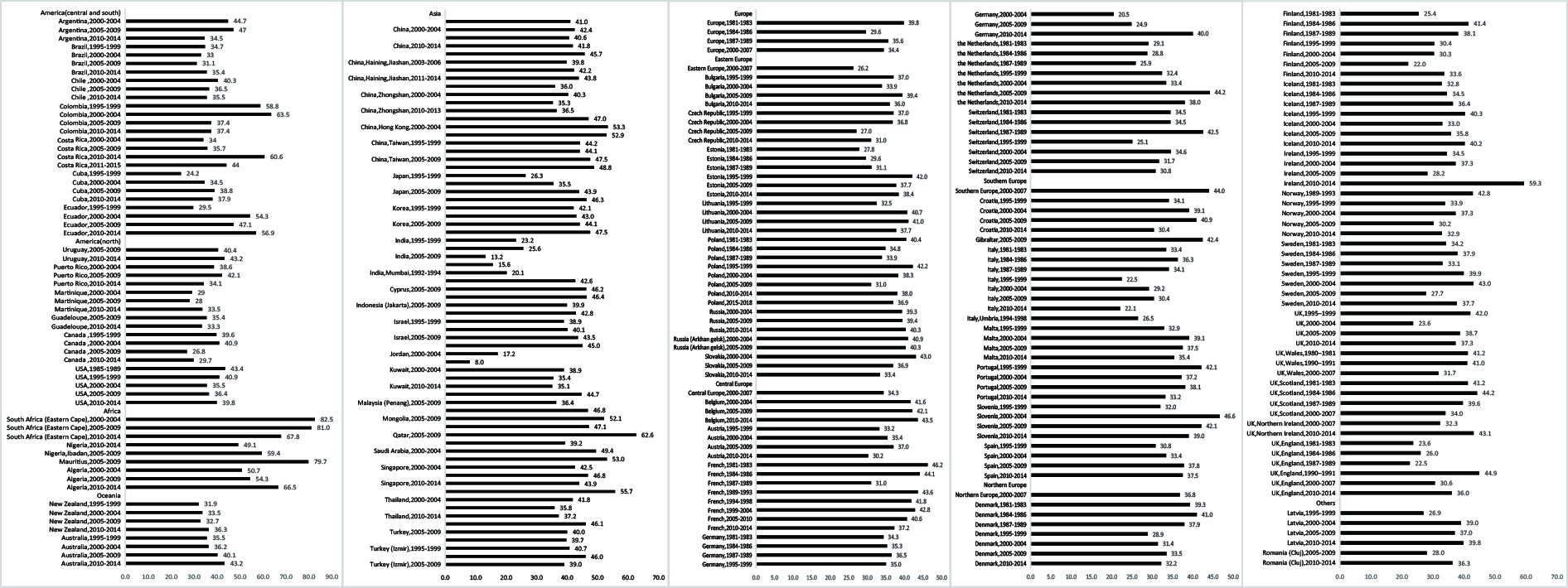
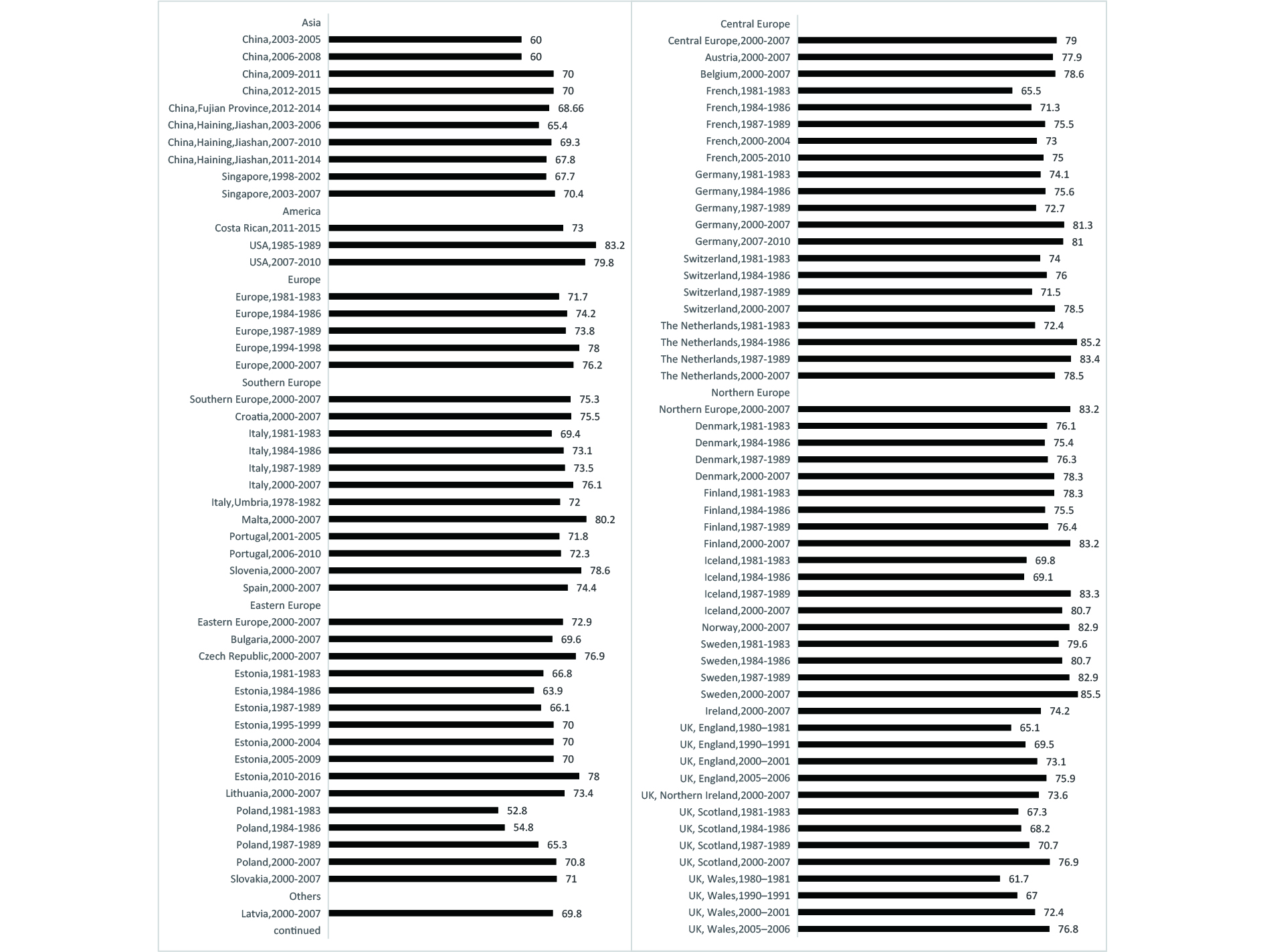
Continent County Regions Period 1−year 3−year 5−year Asia China Fujian[53] 2012−2014 − − 51.5 Haining, Jiashan, Zhejiang[54] 2003−2006 − − 51.1 2007−2010 − − 47.2 2011−2014 − − 53.1 Zhejiang[8] 2005−2010 77.3 62.6 55.2 Qidong, Jiangsu[42,95] 1982−1986 − − 48.7 1987−1991 − − 31.7 1992−1996 − − 34.3 1997−2000 − − 44.6 2002-2006 68.0 47.3 45.2 2007-2011 75.7 50.9 41.9 2012-2016 78.8 57.9 49.5 Shanghai[13] 1988−1991 65.7 48.9 44.3 Tianjin[14] 1981−1985 47.8 37.0 36.3 Japand [57] 1993−1996 − − 49.4 1997−1999 − − 52.0 Osaka[88,96] 1985−1994 − − 40.9 1982−1989 − − 27.7 1990−1997 − − 33.2 Korea[59] 1993−1995 − − 60.1 1996−2000 − − 59.4 2001−2005 − − 61.7 2006−2010 − − 61.3 2011−2015 − − 64.8 2015−2019 − − 64.5 Kuwait[63] 2000−2004 73.4 − 38.9 2005−2009 79.0 − 42.6 2010−2013 78.3 − 40.3 Turkey[64] 2009 − − 50.0 Philippines Metro Manila and Rizal[62] 1998−2002 − − 49.5 India Mumbai[20] 1990−1994 51.9 29.0 25.4 Singapore[18] 1983−1987 − − 51.0 1988−1992 − − 62.0 Africa Uganda Kampala[38] 1993−1997 − − 16.2 America United States[82,84,97] 1981−1987 69.6 − 36.9 2006−2012 − − 46.4 2013−2019 − − 50.8 Canada[98] 2010−2014 71.7 50.1 − Canada Manitoba[99] 1992–1995 64.9 37.2 − 1996–1999 71.0 44.4 − 2000–2003 72.1 49.1 − 2004–2007 66.6 43.3 − 2008–2011 69.6 46.7 − 1992−2011 68.8 44.4 − Costa Rica[22] 2011−2015 − − 54.0 Oceania Australia[98] 2010−2014 78.2 56.4 − New South Wales[86] 1993−1996 − − 37.3 New Zealand[98] 2010−2014 71.4 45.5 − Europe[28,65,100] 1981−1983 − − 33.0 1984−1986 − − 35.0 1987−1989 − − 33.0 1990−1994 36.7 1995−1999 70.7 49.9 41.8 Austria[83] 1985−1989 − − 44.0 Czech[77]* [100] 1995–1999 − − 45.0 2000−2004 − − 37.0 2005−2008 − − 38.4 Denmark[67,91,98] 1994−2003 77.0 − 37.0 2005−2009 − − 41.5 2010−2014 77.6 53.6 − Finland[34,68,93,100] 1980−1982 − − 44.8 1985−1994 68.0 37.0 35.0 1985−1987 − − 42.9 1990−1992 − − 45.7 1995−1999 − − 40.4 2003–2005 − − 49.0 France [101]* 1982−2005 81.0 55.0 44.0 1982−1989 82.0 49.0 41.0 1990−1997 74.0 50.0 39.0 1998−2005 87.0 64.0 49.0 France[52] 1989−2010 76.0 − 42.0 Germany[36] 2002−2006 − − 40.0 Saarland[45, 72, 102] 1981−1985 − − 32.0 1986−1990 − − 34.4 1991−1995 − − 39.4 1999-2003 − − 45.2 2000−2002 − − 45.7 Augsburg, Swabia [71] 2005−2011 − 48.0 40.2 2005–2007 − 41.7 − 2008–2010 − 52.4 − 2011–2013 − 66.3 − Ireland[98] 2010−2014 69.2 44.8 − Italy[100] 1995–1999 − − 41.0 Umbria[76] 1994−1998 73.0 48.0 42.0 Modena[100]* 1990–1997 − − 41.0 1998–2005 − − 36.0 Norway[98] [100]* 1991−1995 − − 39.9 1996–2000 − − 44.1 2010−2014 77.7 57.2 − Slovenia[100]* 1993–1997 − − 37.0 1998–2002 − − 46.0 Spain[83] 1985−1989 − − 41.0 Sweden[46,69,83] 1985−1989 − − 45.0 2000−2002 − − 47.5 2009−2013 − − 37.0 Switzerland[83] 1985−1989 − − 40.0 Vaud[30] 1984−1988 − − 32.0 1989−1993 − − 37.0 Geneva[100]* 1990–1994 − − 39.0 1994–1998 − − 48.0 UK[98] 2010−2014 70.4 − 47.3 UK−Northern Ireland[100]* 1993−1996 − − 41.6 2001–2004 − − 43.6 UK−Scotland[100]* 1992–1996 − − 32.8 1997–2001 − − 40.6 The Netherlands[103] 1989−1991 − − 36.0 2007−2009 − − 41.0 Eindhoven[75,104] 1980−2002 − − 40.3 1981−1985 − 48.0 42.0 Amsterdam[100]* 1993–1996 − − 37.0 2001–2005 − − 40.0 Note. *The survival rate trend was statistically significant in the original article. dSix registries (Miyagi, Yamagata, Niigata, Fukui, Osaka, and Nagasaki) were included in the original article. −, No report or unavailable in the original article. Figures 2–4 demonstrate the age-standardized 5-year relative or net survival rates for cervical, endometrial, and ovarian cancer from to 1980–2015. The age-standardized 5-year relative or net survival rates for cervical cancer varied widely around the world[21,106-111]. The highest was 93.6% in Nigeria and Ibadan (2000–2004), while the lowest was 19.4% in Guadeloupe (2010–2014). Survival was in the range of 50%–70% in most countries and regions (Figure 2). For endometrial cancer, the rates ranged from 60% to 80% in most countries[65,92,112-119], with the highest 5-year rate in the United States (1985–1989) at 83.2%, and the poorest in Poland (1981–1983) at 52.8% (Figure 3). The prognosis of ovarian cancer is typically worse than that of cervical and endometrial cancers, with a rate of less than 50%, regardless of the economic status of the country[47,65,76,108,109,112,120-124] (Figure 4).
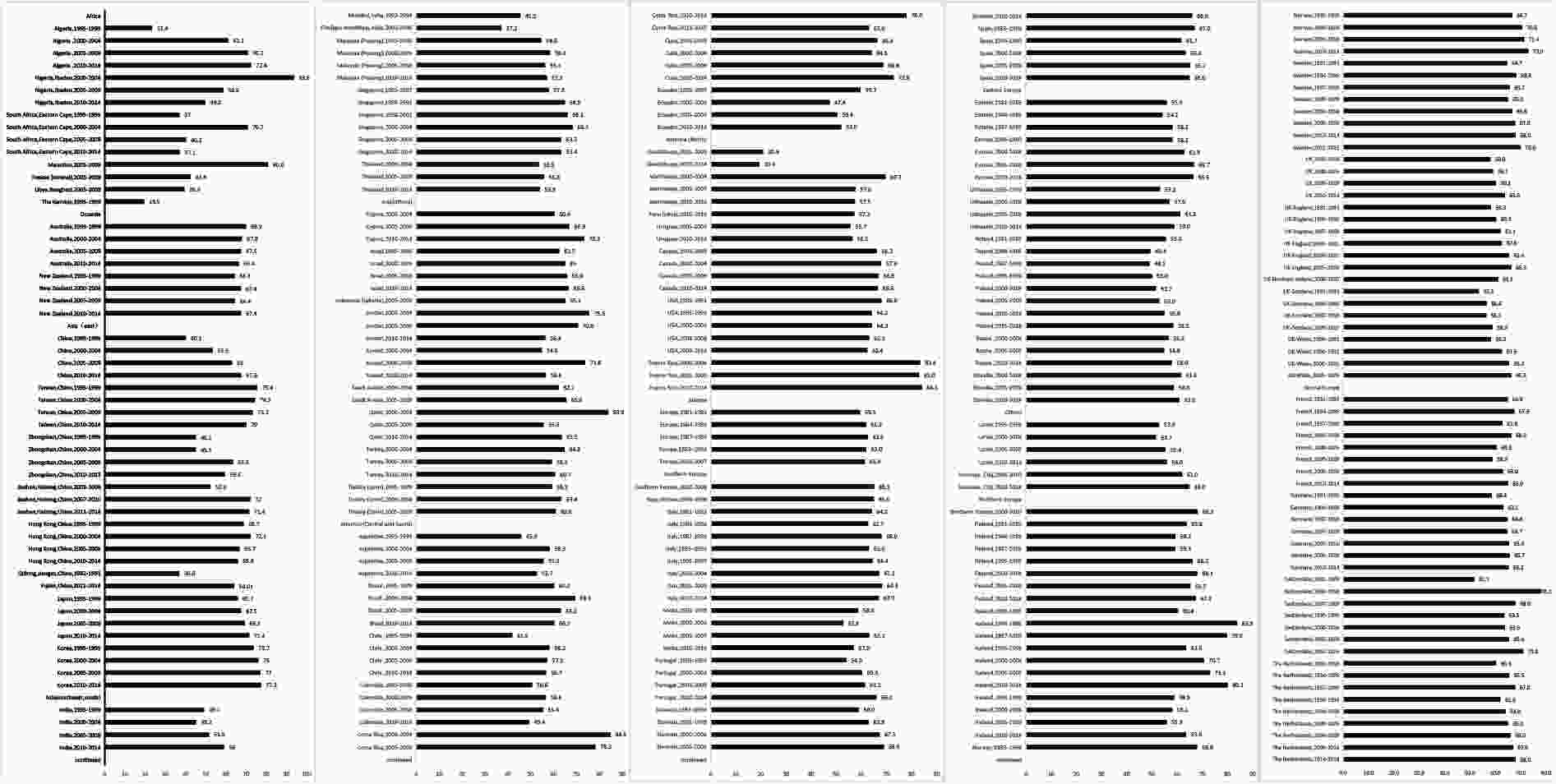
Figure 2. Age-standardized 5-year relative/net survival rates (%) of cervical cancer in selected countries and regions, 1980–2015.
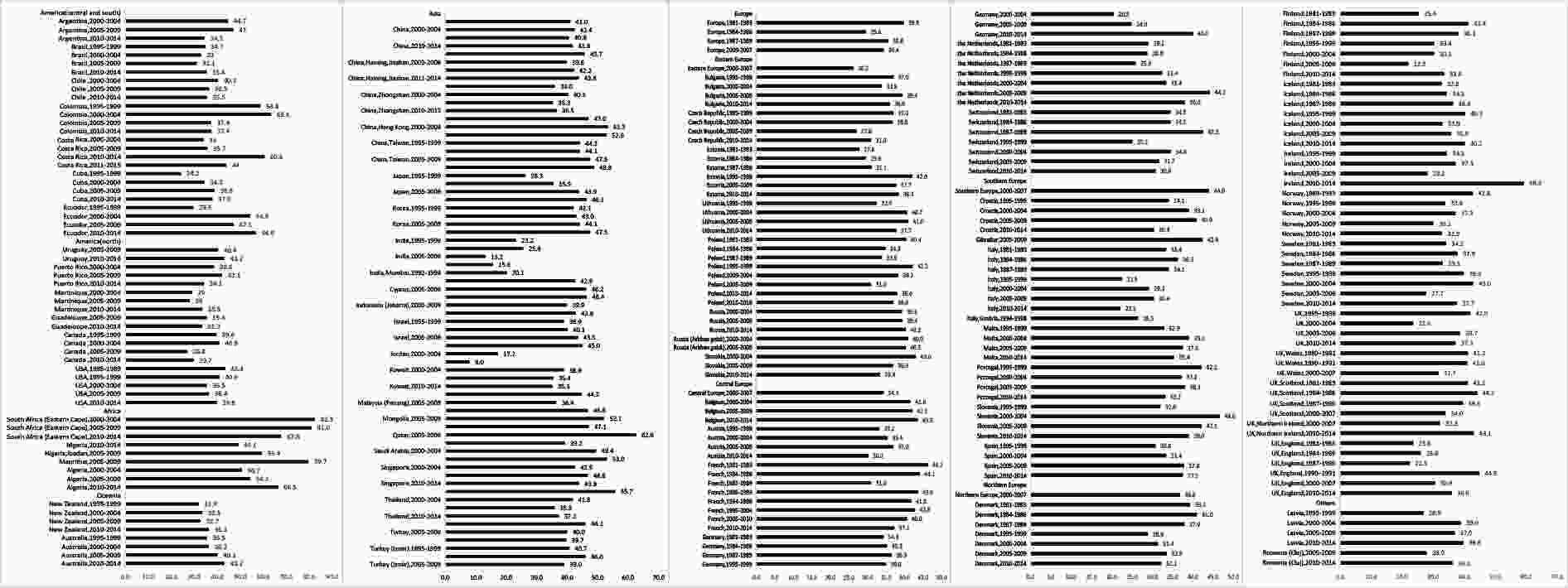
Figure 4. Age-standardized 5-year relative/net survival rates (%) of ovarian cancer in selected countries and regions, 1980–2015.
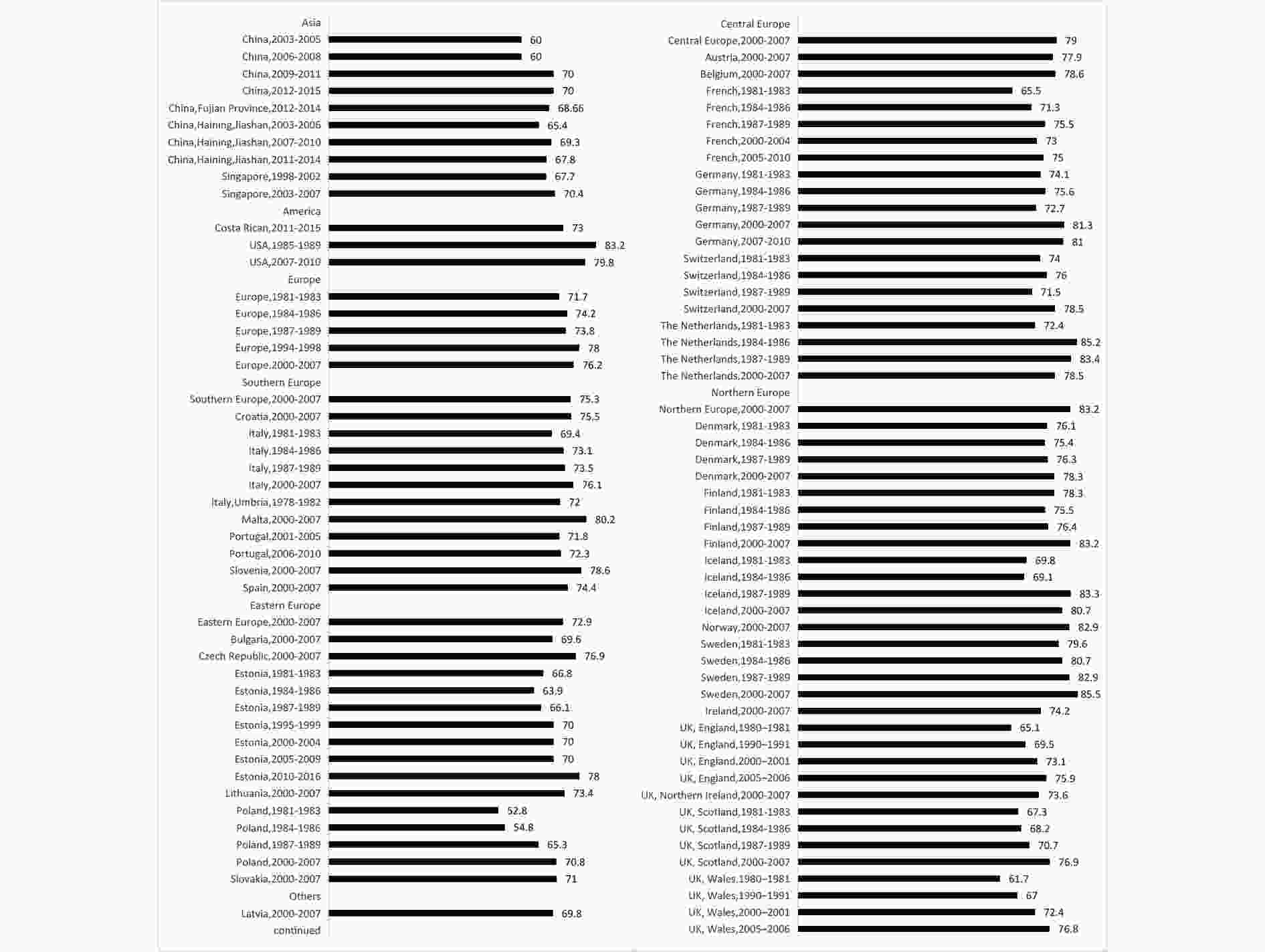
Figure 3. Age-standardized 5-year relative/net survival rates (%) of uterine corpus cancer in selected countries and regions, 1980–2015.
-
The 5-year OSR trends of cervical cancer have increased by 20%–40% in Qidong, Jiangsu, China[6] and in Sihui, Guangdong Province, China [9,43], and by 5%–10% in Singapore[18], Vaud, Switzerland [30,125], Bulgaria[35] and Cuba[27] (Table 1). For women diagnosed with endometrial cancer between 2007-2009, the 5-year OSR was 78.1% in Sihui, Guangdong, China, a significant increase from 7.4% for women diagnosed 20 years ago[9] (Table 2). The 5-year OSR improvements of more than 5.0% in ovarian cancer were found in Singapore (from 56.0% in 1983–1987 to 64.0% in 1988–1992)[18] and Saarland, Germany (from 29.9% in 1981–1985 to 37.2% in 1991–1995)[45] (Table 3).
The 5-year relative or net survival rate trends of cervical cancer from the 1980s to the 2010s increased by 20%–40% in Qidong, Jiangsu, China[6], in Haining, Zhejiang, China[54], in Bangkok, Thailand[61], and in Finland[66,68]. Survival increased by 5%–20% in Osaka, Japan[58], Singapore[18], Chiang Mai, Thailand[61], Lampang, Thailand[61], Kuwait[63], Cuba[27], Cali, Columbia[80], and nine European countries (Denmark[66,67], Iceland[66], Sweden[33,66,69], Scotland[66], Netherlands[66,74], Italy[66], Spain[66], Estonia[66,78] and Lithuania[79]) (Table 4). For endometrial cancer, the 5-year survival trends were rather flat in the United States[83,84] and Sweden[28, 41,65], but increased in Haining, Jiashan, Zhejiang, China [54], Korea[59,126], and the Netherlands[83,94] (Table 5). From the 1980s to the 2010s, the 5-year survival trends of ovarian cancer increased by 5%–10% in Osaka, Japan[88,96], Singapore[18], the United States[82,84,97], Saarland, Germany[45, 72,102], Slovenia[100], Geneva[100], and Switzerland[83] (Table 6).
For the time changes, the age-standardized 5-year relative or net survival rates for cervical cancer increased over time in many countries and regions, including those in a few countries such as Australia, Nigeria, Ibadan, Costa Rica, and the United States (Figure 2). The 5-year survival rates of endometrial cancer continued to increase until 2015 in Asian and European countries, with an increase of more than 10% in China, Estonia, Poland, England, and Wales (Figure 3). In most countries and regions, the 5-year survival rate for ovarian cancer has increased or fluctuated from 1980 to 2015. These rates increased by more than 10% in Japan, Ecuador, Algeria, Cuba, Latvia, Estonia, Ireland, England, and Costa Rica (Figure 4). In addition, in Argentina, Colombia, South Africa (Eastern Cape), Thailand, France, and Italy, this rate fell by more than 10%.
-
Supplementary Tables S3–S5 (available in www.besjournal.com) compare the age-specific relative or net survival rates for gynecological cancer. Generally, survival rates gradually decrease with increasing age, wherein patients aged ≥ 75 years have the worst prognoses. However, there are exceptions in some regions. For cervical cancer, the lowest rate was in the 65–74-year age group in Qidong, Jiangsu, China (2001–2007)[127]. The worst prognosis for ovarian cancer was in the 65–74-year age group in Mumbai and Europe (1981–1983). As compared with other countries and regions, Taizhou, Zhejiang, China (2014–2018)[128] had a better prognosis for cervical cancer in each age group. Besides, the survival rates of endometrial cancer demonstrated a consistent improvement over time, particularly among patients aged ≥ 75 years in Europe[28, 41,65,114].
-
Supplementary Tables S6–S8 (available in www.besjournal.com) illustrates the 5-year relative or net survival rates for gynecological cancers by country and stage, respectively. Cases registered as localized or stage I-II exhibited better 5-year survival rates than those in other stages. The 5-year survival rates of patients in the early stages are usually between 80% and 90%; as the disease progresses to advanced stages, the rates drop significantly to below 20%. Furthermore, the rates of cervical cancer for each clinical stage showed significant improvements in Osaka, Japan (from to 1987–1994 to 2003–2010)[58] and Lithuania (from to 1990–1994 to 2000–2004)[79]. The 5-year survival rates remained flat in Korea (from to 1996–2015 to 2015–2019)[59,60].
-
Supplementary Tables S9–S11 (available in www.besjournal.com) show the pathology-specific 5-year relative/net survival rates of gynecological cancers. The prognosis of patients with squamous cell carcinoma (SCC) was similar to that of patients with adenocarcinoma (ADC) and adenosquamous carcinoma (ASC) in most countries and regions (Supplementary Table S8). SCC shows slightly better survival than non-SCC histology[55,60,64,73,74,78]. For endometrial cancer, the 5-year rates were higher in patients with endometrial carcinoma and mucinous adenocarcinoma than in those with other histological subtypes (Supplementary Table S9). For ovarian cancer, the 5-year rates of germ cell and sex cord-stromal tumors were higher than those of epithelial ovarian cancers (Supplementary Table S10). Among the different histological types of epithelial ovarian cancer, endometrioid, mucinous, and clear cell ovarian cancers have a higher 5-year relative/net survival than serous, not otherwise specified (NOS), and other epithelial cancers.
-
In this study, we systematically collected and summarized the global survival features and long-term trends among common gynecological cancers. We also compared the survival rates by region, diagnostic period, stage, histological type, and age group. The overall survival rate in developed countries was generally higher than that in developing countries. The 5-year survival rates for cervical and endometrial cancers have increased in several Asian and European countries and regions. The magnitude of this increase was greater in developing than in developed countries. However, the trend for ovarian cancer fluctuated in most countries but increased in a few countries.
Survival rates of cervical and endometrial cancers were lower in low-HDI countries. For instance, the survival rate in Africa was poorer than that in other continents; Eastern Europe was poorer than that in other parts of Europe. A global study showed that cancer outcomes were significantly correlated with economic indicators[129]. Countries with high HDI usually have more sophisticated health systems, wider medical security, and higher levels of medical services. There was more than a 10-fold difference in median physician densities between the lowest and highest HDI quintiles[130]. Compared with the number of patients with cancer in Latin American countries, there are fewer oncologists, radiotherapists, cancer surgeons, and palliative care professionals in the Caribbean region[131,132]. Areas with low HDI often experience limited access to medical resources, inadequate healthcare facilities, and unequal distribution of medical services, thus resulting in lower rates of early cancer screening and diagnosis as well as inaccurate detection of cancer. Denny discussed the challenges in cancer survival data from Africa and pointed out that limitations in detection and diagnostic technologies significantly affect the accuracy of the data collected from these areas[133].
The 5-year survival rates for cervical cancer have improved in Asia and Europe, but remain stagnant in other countries across North America and Oceania. This discrepancy can be attributed to the implementation of more comprehensive screening programs in these regions, aimed at the early detection of precancerous cells and localized tumors that can be effectively treated using a range of simple techniques, thereby reducing the overall incidence of cancer. However, screening may have limited efficacy in detecting aggressive tumor types[108]. Human papillomavirus (HPV) infections are also associated with cervical cancer. Cervical cytology (i.e., liquid-based cytology) and HPV DNA testing are important for its prevention and early diagnosis[134,135]. The early detection and treatment of precancerous cervical lesions can significantly improve survival rates.
In the past 40 years, the survival rate of patients with endometrial cancer has increased, probably due to improvements in treatment methods and precision. With the continuous increase in medical research, the treatment methods for endometrial cancer have improved, thereby leading to an increase in patient survival rates. With the development of genetic testing and molecular targeted therapy, doctors can more accurately formulate treatment plans according to an individual’s condition, thus improving treatment effectiveness and survival rate[136]. Molecularly targeted therapies, such as hormonal drugs[137], immune checkpoint inhibitors[138], drugs targeting ERBB2/HER2[139], poly-ADP-ribose polymerase (PARP) inhibitors[140] and others molecularly targeted therapies[141,142], have become a promising therapeutic modality to improve the prognosis of endometrial cancer.
Ovarian cancer is associated with a low survival rate, partly because of difficulties in early diagnosis and the development of metastases. In addition, low survival is related to the evasion of immune system function[143]. Surgery and chemotherapy are the mainstay treatments for ovarian cancer; however, patients often relapse within a few years after initial treatment because of chemotherapy resistance[144]. Immunotherapy has evolved rapidly over the last two decades, revolutionizing the treatment of a wide range of cancers. New treatment technologies, such as therapeutic targets, neoadjuvant immunotherapy, and nanomedicine, have the potential to prolong patient survival[145].
Our findings suggest that the survival rates for gynecological cancers have increased in China over the past four decades; however, there are still large differences in 5-year survival rates between cities over the same period. For example, in the late 1980s, the 5-year relative/net survival rates for cervical cancer were 52.1% in Shanghai and 31.1% in Qidong. Some of the main reasons for this disparity are as follows. There are significant differences in medical resources between cities, including the distribution of hospital facilities, medical technology levels, and medical talent. Some large cities usually have more advanced medical equipment, more aggressive early screening activities, and higher levels of healthcare teams, thus allowing for better and more advanced treatment services for gynecological cancers[146]. Song et al. suggested that HPV vaccination rates in the Chinese female population of an appropriate age group were affected by the varying economic, health, and educational levels of each region[147].
Survival rates for cervical, endometrial, and ovarian cancers vary significantly across different stages. The cervical cancer results were similar to those of a previous retrospective cohort study[148]. Advanced cancer often entails a heavy tumor burden accompanied by distant metastasis or organ invasion, thus increasing treatment complexity and risk for recurrence[149-152]. Advanced cancers require more invasive treatments, such as radiation therapy, chemotherapy, or surgery. Consequently, these interventions can result in adverse effects and complications[153].
There are differences in survival rates among the various histological types of gynecological cancers. Different histological types of cancer have different biological characteristics, including growth patterns, cell morphology, and degree of differentiation, which may affect the tumor growth rate, degree of invasion, and sensitivity to treatment[154,155]. Cancers of different histological types tend to occur in different patient populations, depending on age, sex, genetic background, and living environment, which may affect a patient's response to treatment and survival[156,157]. Therefore, it is necessary to implement individualized treatments for gynecological tumors of different histological types to improve the therapeutic effect and survival rate.
Age characteristics of the survival of patients with gynecological cancers are also summarized in our review. Survival rates decline with age in most countries and regions, with the lowest survival rates observed in individuals aged ≥ 75 years. Poor prognosis in the elderly may be attributed to several factors, including physiological changes[158], psychological factors[159], health status, treatment tolerance and compliance[160,161], and nutritional status. Older individuals often develop multiple chronic diseases. Conditions such as cardiovascular disease, diabetes, and renal dysfunction can affect the efficacy of cancer treatments and overall tolerability[159]. Even after adjusting for frailty, comorbidities, and socioeconomic status, elderly patients remain under-treated[162]. A population-based study shows that patients aged ≥ 70 years were significantly less likely to be seen by a gynecologic oncologist in their course of treatment[163]. Finally, some older adults may experience malnutrition or physical depletion due to dietary changes or reduced absorption capacity[164,165], thus hurting their treatment tolerance and recovery efficacy.
Several factors must be considered when comparing the survival rates across countries and over time. First, we collected only OSRs and relative/net survival rates. However, other indicators, such as disease-specific survival rates, were not assessed. Second, the survival rates were considered either too high or low in some countries. The reliability of survival estimates is compromised due to the significant loss of follow-up within 5 years after diagnosis, limited registration based solely on death certificates or autopsy reports, and cases with unknown vital status or incomplete registration dates in some countries and regions, such as Africa (Algeria, Nigeria, South Africa), America (Colombia, Costa Rica, Guadeloupe), and Asia (Cyprus, Malaysia, Qatar, Thailand). Third, some studies excluded patients aged ≤ 18 years in this review.
In conclusion, we summarized the 1-, 3-, 5-, and 10-year survival rates for common gynecological cancers over the past four decades globally, which showed significant differences among countries and regions. To improve the survival rate of gynecological cancers, especially ovarian cancer, there is a need to strengthen international cooperation, share the latest research results and treatment experiences, and promote treatment improvement globally. Developing countries should invest more resources in the development and promotion of screening campaigns for early stage cancers, and raise awareness of early symptoms among medical personnel and the public, so that more patients can be diagnosed and treated at an early stage.
-
Yongbing Xiang designed the research and obtained funding; Xiaohui Zhou, Danni Yang, Qun Xu, and Yongbing Xiang conducted the study; Xiaohui Zhou and Danni Yang collected publications and abstract data; Xiaohui Zhou, Qun Xu, and Yongbing Xiang prepared and wrote the first draft; Xiaohui Zhou, Danni Yang, Yixin Zou, Dandan Tang, Jun Chen, Zhuoying Li, Qiuming Shen, Qun Xu, and Yongbing Xiang reviewed and approved the final version of the manuscript; Yongbing Xiang had primary responsibility for the final content.
-
All authors declare no conflicts of interest.
-
Not applicable.
-
Not applicable.
doi: 10.3967/bes2024.133
Long-Term Survival Trend of Gynecological Cancer: A Systematic Review of Population-Based Cancer Registration Data
-
Abstract: Gynecological cancer significantly affect the health of women. This review aimed to describe the global patterns and trends in the survival of patients with gynecological cancers. We searched PubMed, Embase, Web of Science, SinoMed, and SEER for survival analyses of cancer registration data of cervical, endometrial, and ovarian cancers published between 1980 and 2022. Globally, the highest 5-year observed survival rate for cervical cancer was 76.5% in Anshan, Liaoning, China (2008–2017). The 5-year observed survival rates of endometrial and ovarian cancers were higher in Finland (1995–1999, 82.5%) and Singapore (1988–1992, 62.0%). The 5-year relative survival rate of cervical cancer patients was higher in Haining, Zhejiang, China (2011–2014, 85.8%). Korea ranked first at 89.0% and 64.5% for endometrial and ovarian cancers, respectively. Survival rates have improved for cervical, endometrial, and ovarian cancers. Patients aged ≥ 75 years and those with advanced-stage disease had the worst 5-year survival rates. Survival rates were better for squamous cell carcinoma in cervical cancer, for endometrial carcinoma and mucinous adenocarcinoma in endometrial cancer, and for germ cell and sex-cord stromal tumors in ovarian cancer. Over the past four decades, the survival rates of gynecological cancers have increased globally, with notable increases in cervical and endometrial cancers. Survival rates are higher in developed countries, with a slow-growing trend. Future studies should focus on improving survival, especially in ovarian cancer patients.
-
Key words:
- Gynecology cancer /
- Relative survival rate /
- Observed survival study /
- Cancer registry /
- Time trend
-
Figure 2. Age-standardized 5-year relative/net survival rates (%) of cervical cancer in selected countries and regions, 1980–2015.
Figure 4. Age-standardized 5-year relative/net survival rates (%) of ovarian cancer in selected countries and regions, 1980–2015.
Figure 3. Age-standardized 5-year relative/net survival rates (%) of uterine corpus cancer in selected countries and regions, 1980–2015.
Table 1. Overall observed survival rates (%) of cervical cancer in selected countries and regions during 1980–2017
Continent Country Region Period 1-year 3-year 5-year 10-year Asia China Qidong, Jiangsu[6]* 1982−1986 57.4 37.4 33.0 27.0 1987−1991 57.9 39.0 26.3 20.0 1992−1996 42.4 35.3 29.4 27.1 1997−2001 55.8 41.9 33.7 25.6 2002−2006 65.3 51.5 49.1 45.2 2007−2011 79.3 66.2 62.8 58.2 2012−2016 90.9 77.9 73.6 − Jiulongpo, Chongqing[7] 2008−2013 69.8 42.6 35.3 − Zhejiang[8] 2005−2010 86.9 75.4 70.8 − Sihui, Guangdong[9]* 1987−1996 − − 18.8 − 1997−2006 − − 47.1 − 2007−2009 − − 49.8 − Guizhoua[10] 2013−2015 81.6 66.4 − − Anshan, Liaoningb[11] 2008−2017 91.5 81.0 76.5 − Yangpu, Shanghai[12] 2002−2012 91.2 79.1 75.5 − Shanghai[13] 1988−1991 73.3 53.6 45.4 − Tianjin[14] 1981−1985 55.0 42.0 38.0 − Korea Kangwha[15] 1983−1987 − − 67.1 − Malaysia[16] 2000−2005 94.1 79.3 71.1 − Thailand Khon Kaen[17] 1985−1990 − − 56.8 − Singapore[18] 1983−1987 − − 56.0 − 1988−1992 − − 63.0 − India Bangalore[19] 1982−1989 − − 34.4 − Mumbai[20] 1990−1994 77.0 55.9 44.0 − Dindigul Ambilikkai[21] 2003−2006 − − 35.0 − America Costa Rica[22] 2011−2015 − − 68.0 − Colombia Manizales[23] 2003−2007 80.7 62.1 51.4 − Canada Ontario[24] [25]* 1995−1998 − 71.1 − − 1999−2001 − 75.9 − − 2003−2007 − − 71.0 − Canada British Columbia[26] 1980−1989 89.0 − 73.0 − 1990−1999 91.0 − 73.0 − 2000−2002 90.0 − − − Cuba[27] 1982 − − 44.0 − 1988−1998 74.0 57.0 52.0 − Europe total[28] 1995−1999 84.9 68.0 62.0 − France Martinique[29] 2002−2011 84.1 62.6 55.1 43.3 Switzerland Vaud[30] 1984−1988 − − 55.0 − 1989−1993 − − 62.0 − Italy Sicily, Ragusa[31] 1992 − − 55.8 − Lithuanian[32] 2001−2009 − − 64.1 − Sweden[33] 2011−2015 − − 74.0 − Finland[34] 1995−1999 − − 63.4 − Bulgaria[35]* 1993−1997 − − 49.7 − 2005−2009 − − 54.7 − Germany[36] 2002−2006 − − 65.0 − Australiac [37] 2003−2007 − − 70.3 − 2008−2012 − − 72.1 − Africa Uganda Kampala[38,39] 1995−1997 79.7 52.4 − − 1993−1997 − − 15.9 − Note. −, No report or unavailable in the original article. *Long−term change in survival rates was statistically significant. aOnly three counties in the Guizhou Province are included. bOnly four districts in Anshan, Liaoning Province are included. cSix Australian states/territories (New South Wales, Victoria, Queensland, South Australia, Western Australia, and the Northern Territory) were included in the original article.  下载: 导出CSV
下载: 导出CSV
Table 2. Overall observed survival rates (%) of uterine corpus cancer in selected countries and regions during 1981–2017
Continent County Region Period 1-year 3-year 5-year Asia China Sihui, Guangdong[9]* 1987−1996 − − 7.4 1997−2006 − − 40.0 2007−2009 − − 78.1 Anshan, Liaoningb[11] 2008−2017 94.1 86.9 82.2 Shanghai[13] 1988−1991 89.3 77.6 72.6 Tianjin[14] 1981−1985 65.0 55.0 54.0 Jiulongpo, Chongqing[7] 2008−2013 69.4 48.4 37.6 Singapore[18] 1983−1987 − − 71.0 1988−1992 − − 72.0 Europe[28] 1995−1999 88.3 76.1 69.4 Denmark[91] 2005−2009 − − 73.5 Germany[36] 2002−2006 − − 70.0 Bulgaria[35]* 1993−1997 − − 66.6 2005−2009 − − 69.0 Finland[34] 1995−1999 − − 82.5 Switzerland Vaud[30] 1984−1988 − − 69.0 1989−1993 − − 74.0 Italy Sicily, Ragusa[31] 1992 − − 68.5 America Costa Rica[22] 2011−2015 − − 74.0 Cuba[27] 1982 − − 56.0 1988−1998 77.0 59.0 52.0 Note. *The long-term change trend of survival rate was statistically significant. bOnly four districts in Anshan, Liaoning Province are included. −, No report or unavailable in the original article.
下载: 导出CSV
Table 3. Overall observed survival rates (%) of ovarian cancer in selected countries and regions during 1981–2017
Continent County Region Period 1−year 3−year 5−year Asia China Qidong, Jiangsu[42] 1982−1986 − − 46.8 1987−1991 − − 30.3 1992−1996 − − 32.7 1997−2000 − − 43.1 Tianjin[14] 1981−1985 47.0 35.0 33.0 Shanghai[13] 1988−1991 65.0 47.2 41.6 Sihui, Guangdong[43] 2003−2005 64.7 58.8 58.8 Zhejiang[8] 2005−2010 76.7 61.0 52.6 Anshan, Liaoningb[11] 2008−2017 80.7 60.7 50.2 Jiulongpo, Chongqing[7] 2008−2013 65.8 44.7 37.5 Singapore[18] 1983−1987 − − 56.0 1988−1992 − − 64.0 India Mumbai[20] 1990−1994 51.0 27.5 23.3 Dindigul Ambilikkai[21] 2003−2006 − − 30.0 Iran[44, 105] 2000−2004
2009-2014−
84.0−
66.061.0
55.0Africa Egypt Alexandria[49] 1988−1997 − − 46.0 Uganda Kampala[38] 1993−1997 − − 14.1 America Costa Rica[22] 2011−2015 − − 52.0 Europe[28,47] 1995−1999 69.1 46.5 37.1 1999−2001 − − 34.8 2002−2004 − − 34.3 2005−2007 − − 35.5 Central Europe[47] 1999−2001 − − 38.7 2002−2004 − − 37.9 2005−2007 − − 37.7 Southern Europe[47] 1999−2001 − − 35.7 2002−2004 − − 33.7 2005−2007 − − 36.7 Eastern Europe[47] 1999−2001 − − 28.9 2002−2004 − − 30.1 2005−2007 − − 32.2 Northern Europe[47] 1999−2001 − − 36.8 2002−2004 − − 37.6 2005−2007 − − 38.8 UK and Ireland[47] 1999−2001 − − 27.8 2002−2004 − − 28.5 2005−2007 − − 29.7 Denmark[48,91] 2000−2002 73.0 − 37.0 2003−2005 69.0 − 36.0 2005−2009 − − 37.7 2009−2011 69.0 − − Italy Sicily, Ragusa[31] 1992 − − 18.1 Bulgaria[35]* 1993−1997 − − 35.4 2005−2009 − − 40.3 France[52] 1989−2010 74.0 − 40.0 Finland[34] 1995−1999 − − 44.6 Germany[36] 2002−2006 − − 37.0 Saarland[45] 1981−1985 − − 29.9 1986−1990 − − 32.4 1991−1995 − − 37.2 Switzerland Vaud[30] 1984−1988 − − 28.0 1989−1993 − − 32.0 Note. *The long-term change trend of survival rate was statistically significant. bOnly four districts in Anshan, Liaoning Province are included. −, No report or unavailable in the original article.
下载: 导出CSV
Table 4. Overall relative/net survival rates (%) of cervical cancer in selected countries and regions during 1980−2019
Continent Country Region Period 1−year 3−year 5−year 10−year Asia China Qidong, Jiangsu[6]* 1982−1986 59.3 41.4 39.2 38.0 1987−1991 59.8 43.0 31.1 28.4 1992−1996 43.6 38.5 34.2 37.9 1997−2001 57.3 45.4 38.6 33.6 2002−2006 66.2 53.8 53.0 52.6 2007−2011 80.2 68.5 66.4 65.0 2012−2016 91.6 79.8 76.8 − Zhejiang[8] 2005−2010 87.5 77.2 73.9 − Guizhoua[10] 2013−2015 84.7 74.3 − − Sihui, Guangdong[9] 2007−2009 − − 50.5 − Shanghai [13] 1988−1991 75.2 57.9 52.1 − Tianjin[14] 1981−1985 56.8 46.6 45.8 − Fujian[53] 2012−2014 − − 68.6 − Haining and Jiashan, Zhejiang[54] 2003−2006 − − 65.6 − 2007−2010 − − 81.7 − 2011−2014 − − 85.8 − Hong Kong[55] 1997−2006 90.6 76.6 71.3 − Taiwan[56] 2004−2008 − − 75.1 − Japand[57] 1993−1996 − − 73.4 − 1997−1999 − − 71.5 − Osaka[58]* 1987−1994 − − 58.6 54.0 1995−2002 − − 56.8 52.7 2003−2010 − − 64.3 59.6 Korea[59,60] 1993−1995 − − 78.3 − 1996−2000 − − 80.3 77.2 2001−2005 − − 81.5 78.3 2006−2010 − − 80.7 77.1 2011−2015 − − 80.3 − 2015−2019 − − 80.5 − Singapore[18] 1983−1987 − − 57.0 − 1988−1992 − − 65.0 − Thailande[61] 1997−2001 78.8 − 55.4 − 2002−2006 80.9 55.5 2008−2012 81.5 − 59.5 − Bangkok[61] 1997−2001 52.5 33.9 2002−2006 75.5 49.0 2008−2012 79.9 56.5 Chiang Mai[61] 1997−2001 83.7 60.8 2002−2006 86.9 61.9 2008−2012 85.3 67.0 Khon Kaen[61] 1997−2001 83.1 57.4 2002−2006 81.0 57.2 2008−2012 79.2 56.1 Lampang[61] 1997−2001 81.7 46.1 2002−2006 83.5 55.0 2008−2012 83.8 64.5 Songkhla[61] 1997−2001 88.8 59.0 2002−2006 79.6 55.3 2008−2012 80.6 55.6 Philippines Metro Manila and Rizal province[62] 1998−2002 − − 45.4 − India Bangalore[19] 1982−1989 − − 38.8 − Mumbai[20] 1990−1994 78.2 58.7 47.7 − Kuwait[63] 2000−2004 84.4 − 57.8 − 2005−2009 88.7 − 73.8 − 2010−2013 86.3 − 71.8 − Turkey[64] 2009 62.0 − Europe[28,65,66] 1981−1983 − − 60.0 − 1983−1985 − − 61.0 1986−1988 − − 62.0 − 1989−1991 − − 64.0 − 1992−1994 − − 63.0 − 1995−1999 86.0 71.0 66.7 − Denmark[66,67] 1983−1985 − − 62.0 − 1986−1988 − − 66.0 − 1989−1991 − − 67.0 − 1992−1994 − − 66.0 − 1994−2003 89.0 − 71.0 − Finland[66,68] 1980−1982 − − 57.5 − 1983−1985 − − 65.0 − 1986−1988 − − 60.0 − 1989−1991 − − 62.0 − 1992−1994 − − 69.0 − 1995−1999 − − 82.3 − Iceland[66] 1983−1985 − − 69.0 − 1986−1988 − − 75.0 − 1989−1991 − − 67.0 − 1992−1994 − − 75.0 − Norway[66] 1983−1985 − − 67.0 − 1986−1988 − − 65.0 − 1989−1991 − − 66.0 − 1992−1994 − − 71.0 − Sweden[33,66,69] 1983−1985 − − 68.0 − 1986−1988 − − 67.0 − 1989−1991 − − 71.0 − 1992−1994 − − 68.0 − 2000−2002 − − 70.9 − 2011−2015 − − 76.0 − England[66,70] 1983−1985 − − 59.0 − 1986−1988 − − 61.0 − 1989−1991 − − 65.0 − 1992−1994 − − 62.0 − 2006−2008 80.4 − 62.2 − 2007−2009 80.8 − − − 2008−2010 80.9 − − − Scotland[66] 1983−1985 − − 54.0 − 1986−1988 − − 58.0 − 1989−1991 − − 61.0 − 1992−1994 − − 60.0 − Wales[66] 1983−1985 − − 62.0 − 1986−1988 − − 59.0 − 1989−1991 − − 59.0 − 1992−1994 − − 58.0 − France[66] 1983−1985 − − 70.0 − 1986−1988 − − 64.0 − 1989−1991 − − 71.0 − 1992−1994 − − 67.0 − Germany[66] 1983−1985 − − 63.0 − 1986−1988 − − 63.0 − 1989−1991 − − 61.0 − 1992−1994 − − 66.0 − Augsburg, Swabia[71] 2005−2011 − 71.4 67.2 − 2005–2007 − 72.1 − − 2008–2010 − 72.2 − − 2011–2013 − 72.3 − − Saarland[72] 1990−1992 − − 61.0 56.6 2000−2002 − − 60.4 55.2 Switzerland[66] 1983−1985 − − 66.0 − 1986−1988 − − 62.0 − 1989−1991 − − 70.0 − 1992−1994 − − 61.0 − Vaud[30,73] 1980−1982 − − 59.0 − 1983−1985 − − 59.0 − 1984−1988 − − 61.0 − 1989−1993 − − 70.0 − Netherlands[66,74]* 1983−1985 − − 66.0 − 1986−1988 − − 69.0 − 1989−1991 − − 72.0 − 1992−1994 − − 66.0 − 2009−2013 − − 73.0 − 2014−2018 − − 74.0 − 1989−2018* − − 71.0 − Eindhoven[75] 1980−2002 − − 70.4 65.1 Italy[66] 1983−1985 − − 60.0 − 1986−1988 − − 62.0 − 1989−1991 − − 63.0 − 1992−1994 − − 67.0 − Umbria[76] 1994−1998 85.0 69.0 64.0 − Slovenia[66] 1983−1985 − − 56.0 − 1986−1988 − − 61.0 − 1989−1991 − − 60.0 − 1992−1994 − − 59.0 − Spain[66] 1983−1985 − − 59.0 − 1986−1988 − − 59.0 − 1989−1991 − − 70.0 − 1992−1994 − − 70.0 − The Czech Republic[77]* 2000−2004 − − 62.1 − 2005−2008 − − 64.2 − Estonia[66,78]* 1983−1985 − − 51.0 − 1986−1988 − − 58.0 − 1989−1991 − − 59.0 − 1992−1994 − − 49.0 − 1995−1999 80.0 − 59.0 − 2000−2004 84.0 − 64.0 − 2005−2009 86.0 − 69.0 − 2010−2014 84.0 − 67.0 − Lithuania[79]* 1990−1994 − − 46.9 − 1995−1999 − − 51.5 − 2000−2004 − − 55.3 − Poland[66] 1983−1985 − − 49.0 − 1986−1988 − − 52.0 − 1989−1991 − − 48.0 − 1992−1994 − − 49.0 − Slovakia[66] 1983−1985 − − 56.0 − 1986−1988 − − 60.0 − 1989−1991 − − 57.0 − 1992−1994 − − 58.0 − America Columbia Cali[80] 1995−1999 77.0 58.0 50.0 47.0 2000−2004 82.0 63.0 60.0 − Cuba[27] 1982 − − 47.0 − 1988−1998 76.0 59.0 56.0 − Costa Rica[22] 2011−2015 − − 69.0 − Canada Manitoba[81] 1985−1989 − − 68.0 − 1990−1994 − − 65.0 − 1995−1999 − − 72.0 − United States[82−84] 1985−1989 − − 66.0 − 2006−2012 − − 68.8 − 2013−2019 − − 67.2 − Oceania Australia New South Wales[85,86] 1982−1986 − − 68.0 − 1987−1991 − − 72.0 − 1993−1996 − − 73.1 − Australiac[37] 2003−2007 − − 75.6 − 2008−2012 − − 76.3 − Africa Uganda Kampala[38,39] 1993−1997 − − 18.2 − 1995−1997 84.1 59.9 − − Note. *The survival rate trend was statistically significant in the original article. aOnly three counties in the Guizhou Province were included in the original article. cSix Australian states/territories (New South Wales, Victoria, Queensland, South Australia,Western Australia, and the Northern Territory) were included in the original article. dSix registries (Miyagi, Yamagata, Niigata, Fukui, Osaka, and Nagasaki) were included in the original article. eFive Thai provinces (Bangkok, Chiang Mai, Khon Kaen, Lampang, and Songkhla) were included in the original article. −, No report or unavailable in the original article.
下载: 导出CSV
Table 5. Overall relative/net survival rates (%) of uterine corpus cancer in selected countries and regions during 1980−2019
Continent County Regions Period 1−year 3−year 5−year 10−year Asia China Fujian[53] 2012−2014 − − 68.3 − Haining, Jiashan, Zhejiang[54] 2003−2006 − − 75.4 − 2007−2010 − − 85.2 − 2011−2014 − − 87.2 − Shanghai[13] 1988−1991 90.2 80.2 77.0 − Tianjin[14] 1981−1985 66.3 60.5 58.6 − Sihui,Guangdong [9] 2007−2009 − − 79.6 − Japan b [57,87]* 1993−1996 − − 79.5 − 1997−1999 − − 76.8 − 1993−2000 90.4 − 77.7 − 2001−2006 91.8 − 80.2 − Osaka[88,89] 1982−1989 − − 70.7 − 1990−1997 − − 68.5 − 1989−2000 − − − 71.2 Korea[59,90] 1999−2017 − − 88.1 − 1993−1995 − − 82.9 − 1996−2000 − − 82.0 − 2001−2005 − − 84.7 − 2006−2010 − − 86.5 − 2011−2015 − − 87.7 − 2015−2019 − − 89.0 − Singapore[18] 1983−1987 − − 68.0 − 1988−1992 − − 64.0 − Turkey[64] 2009 − − 85.0 − America United States[82−84] 1985−1989 − − 83.0 − 2006−2012 − − 83.4 − 2013−2019 81.0 Costa Rica[22] 2011−2015 − − 78.0 − Cuba[27] 1982 − − 69.0 − 1988−1998 81.0 66.0 62.0 − Oceania Australia New South Wales[86] 1993−1996 − − 79.2 − Europe[28] 1995−1999 90.3 81.7 78.6 − Czech[77] 2000−2004 − − 76.6 − 2005−2008 − − 78.9 − Denmark[67,91] 1994−2003 94.0 − 80.0 − 2005−2009 − − 83.0 − Estonia[92] 1996−2002 − − 75.0 − 2003−2009 − − 73.0 − 2010−2016 − − 79.0 − Finland[68,93] 1985−1994 92.0 − 82.0 82.0 1980−1982 − − 75.9 − 1985−1987 − − 75.1 − 1990−1992 − − 80.3 − Germany[36] 2002−2006 − − 79.0 − Augsburg, Swabia[71] 2005−2011 − 85.4 82.5 − 2005−2007 − 82.7 − − 2008−2010 − 87.3 − − 2011–2013 − 88.0 − − Saarland[72] 1990−1992 − − 81.8 80.8 2000−2002 − − 82.8 81.9 Italy Umbria[76] 1994−1998 92.0 81.0 79.0 − Netherlands[83,94] 1985−1989 − − 75.2 − 1989−1993 − − 77.0 − 1994−1998 − − 78.0 − 1999−2003 − − 79.0 − 2004−2008 − − 80.0 − Eindhoven[75] 1980−2002 − − 81.2 79.1 Sweden[65,69] 1981−1983 − − 75.0 − 1984−1986 − − 75.0 − 1987−1989 − − 73.0 − 2000−2002 − − 85.3 − Switzerland Vaud[30] 1984−1988 − − 78.0 − 1989−1993 − − 84.0 − Note. *The survival rate trend was statistically significant in the original article. −, No report or unavailable in the original article.
下载: 导出CSV
Table 6. Overall relative/net survival rates(%) of ovarian cancer in selected countries and regions during 1980–2019
Continent County Regions Period 1−year 3−year 5−year Asia China Fujian[53] 2012−2014 − − 51.5 Haining, Jiashan, Zhejiang[54] 2003−2006 − − 51.1 2007−2010 − − 47.2 2011−2014 − − 53.1 Zhejiang[8] 2005−2010 77.3 62.6 55.2 Qidong, Jiangsu[42,95] 1982−1986 − − 48.7 1987−1991 − − 31.7 1992−1996 − − 34.3 1997−2000 − − 44.6 2002-2006 68.0 47.3 45.2 2007-2011 75.7 50.9 41.9 2012-2016 78.8 57.9 49.5 Shanghai[13] 1988−1991 65.7 48.9 44.3 Tianjin[14] 1981−1985 47.8 37.0 36.3 Japand [57] 1993−1996 − − 49.4 1997−1999 − − 52.0 Osaka[88,96] 1985−1994 − − 40.9 1982−1989 − − 27.7 1990−1997 − − 33.2 Korea[59] 1993−1995 − − 60.1 1996−2000 − − 59.4 2001−2005 − − 61.7 2006−2010 − − 61.3 2011−2015 − − 64.8 2015−2019 − − 64.5 Kuwait[63] 2000−2004 73.4 − 38.9 2005−2009 79.0 − 42.6 2010−2013 78.3 − 40.3 Turkey[64] 2009 − − 50.0 Philippines Metro Manila and Rizal[62] 1998−2002 − − 49.5 India Mumbai[20] 1990−1994 51.9 29.0 25.4 Singapore[18] 1983−1987 − − 51.0 1988−1992 − − 62.0 Africa Uganda Kampala[38] 1993−1997 − − 16.2 America United States[82,84,97] 1981−1987 69.6 − 36.9 2006−2012 − − 46.4 2013−2019 − − 50.8 Canada[98] 2010−2014 71.7 50.1 − Canada Manitoba[99] 1992–1995 64.9 37.2 − 1996–1999 71.0 44.4 − 2000–2003 72.1 49.1 − 2004–2007 66.6 43.3 − 2008–2011 69.6 46.7 − 1992−2011 68.8 44.4 − Costa Rica[22] 2011−2015 − − 54.0 Oceania Australia[98] 2010−2014 78.2 56.4 − New South Wales[86] 1993−1996 − − 37.3 New Zealand[98] 2010−2014 71.4 45.5 − Europe[28,65,100] 1981−1983 − − 33.0 1984−1986 − − 35.0 1987−1989 − − 33.0 1990−1994 36.7 1995−1999 70.7 49.9 41.8 Austria[83] 1985−1989 − − 44.0 Czech[77]* [100] 1995–1999 − − 45.0 2000−2004 − − 37.0 2005−2008 − − 38.4 Denmark[67,91,98] 1994−2003 77.0 − 37.0 2005−2009 − − 41.5 2010−2014 77.6 53.6 − Finland[34,68,93,100] 1980−1982 − − 44.8 1985−1994 68.0 37.0 35.0 1985−1987 − − 42.9 1990−1992 − − 45.7 1995−1999 − − 40.4 2003–2005 − − 49.0 France [101]* 1982−2005 81.0 55.0 44.0 1982−1989 82.0 49.0 41.0 1990−1997 74.0 50.0 39.0 1998−2005 87.0 64.0 49.0 France[52] 1989−2010 76.0 − 42.0 Germany[36] 2002−2006 − − 40.0 Saarland[45, 72, 102] 1981−1985 − − 32.0 1986−1990 − − 34.4 1991−1995 − − 39.4 1999-2003 − − 45.2 2000−2002 − − 45.7 Augsburg, Swabia [71] 2005−2011 − 48.0 40.2 2005–2007 − 41.7 − 2008–2010 − 52.4 − 2011–2013 − 66.3 − Ireland[98] 2010−2014 69.2 44.8 − Italy[100] 1995–1999 − − 41.0 Umbria[76] 1994−1998 73.0 48.0 42.0 Modena[100]* 1990–1997 − − 41.0 1998–2005 − − 36.0 Norway[98] [100]* 1991−1995 − − 39.9 1996–2000 − − 44.1 2010−2014 77.7 57.2 − Slovenia[100]* 1993–1997 − − 37.0 1998–2002 − − 46.0 Spain[83] 1985−1989 − − 41.0 Sweden[46,69,83] 1985−1989 − − 45.0 2000−2002 − − 47.5 2009−2013 − − 37.0 Switzerland[83] 1985−1989 − − 40.0 Vaud[30] 1984−1988 − − 32.0 1989−1993 − − 37.0 Geneva[100]* 1990–1994 − − 39.0 1994–1998 − − 48.0 UK[98] 2010−2014 70.4 − 47.3 UK−Northern Ireland[100]* 1993−1996 − − 41.6 2001–2004 − − 43.6 UK−Scotland[100]* 1992–1996 − − 32.8 1997–2001 − − 40.6 The Netherlands[103] 1989−1991 − − 36.0 2007−2009 − − 41.0 Eindhoven[75,104] 1980−2002 − − 40.3 1981−1985 − 48.0 42.0 Amsterdam[100]* 1993–1996 − − 37.0 2001–2005 − − 40.0 Note. *The survival rate trend was statistically significant in the original article. dSix registries (Miyagi, Yamagata, Niigata, Fukui, Osaka, and Nagasaki) were included in the original article. −, No report or unavailable in the original article.
下载: 导出CSV
-
[1] Keyvani V, Kheradmand N, Navaei ZN, et al. Epidemiological trends and risk factors of gynecological cancers: an update. Med Oncol, 2023; 40, 93. doi: 10.1007/s12032-023-01957-3 [2] Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin, 2024; 74, 229−63. doi: 10.3322/caac.21834 [3] Ino K. Indoleamine 2, 3-dioxygenase and immune tolerance in ovarian cancer. Curr Opin Obstet Gynecol, 2011; 23, 13−8. doi: 10.1097/GCO.0b013e3283409c79 [4] Yoshida Y, Schmaltz CL, Jackson-Thompson J, et al. Ovarian cancer survival in Missouri, 1996-2014. Mo Med, 2018; 115, 542−7. [5] Baldwin LA, Huang B, Miller RW, et al. Ten-year relative survival for epithelial ovarian cancer. Obstet Gynecol, 2012; 120, 612−8. doi: 10.1097/AOG.0b013e318264f794 [6] Wang Y, Wang J, Xu YY, et al. Survival trend of cervical cancer in Qidong city of Jiangsu province from 1977 to 2016. China Cancer, 2022; 31, 782−6. (In Chinese [7] Deng SM, Li N, Liang Y, et al. Analysis of survival in major malignances during 2008-2013 in Jiulongpo avea of Chongqing. Chin J Cancer Prev Treat, 2014; 21, 1223−6. (In Chinese [8] Gong WW, Luo SL, Hu RY, et al. Analysis of survival rate of breast, cervical, and ovarian cancer patients during 2005-2010 in Zhejiang province, China. Chin J Prev Med, 2014; 48, 366−9. (In Chinese [9] Li YH, Lu YQ, Ling W, et al. Survival analysis of patients with malignant tumors in Sihui city between 1987 and 2009. China Cancer, 2017; 26, 596−600. (In Chinese [10] Zhou J, Su X, Li L, et al. Survival rate among the main cancer patients in three countys of GuiZhou province, 2013~2015. Studies Trace Elem Health, 2020; 37, 54−6. (In Chinese [11] Zhang WW, Wang LJ. Analysis of cancer incidence and survival in Anshan City from 2008 to 2017. J Community Med, 2021; 19, 530−5. (In Chinese [12] Han X, Huang CX, Zhao J, et al. Incidence and survival analysis of cervical cancer patients among permanent residents in Yangpu district of Shanghai during 2002-2012. Acad J Second Military Med Univ, 2014; 35, 26−9. (In Chinese doi: 10.3724/SP.J.1008.2014.00026 [13] Xiang YB, Jin F, Chen HQ, et al. An analysis of survival rate of patients with malignancy in urban district of Shanghai from 1988 to 1991. China Cancer, 1996; 5, 6-8. (In Chinese [14] Wang QS, Lin XP, Li RT, et al. An analysis of relative survival rate in patients with malignancy in Tianjin. China Cancer, 2001; 10, 276−7. (In Chinese [15] Kim IS, Suh I, Oh HC, et al. Incidence and survival of cancer in Kangwha County (1983-1987). Yonsei Med J, 1989; 30, 256−68. doi: 10.3349/ymj.1989.30.3.256 [16] Muhamad NA, Kamaluddin MA, Adon MY, et al. cia. Asian Pac J Cancer Prev, 2015; 16, 3067−72. doi: 10.7314/APJCP.2015.16.7.3067 [17] Sriamporn S, Swaminathan R, Parkin DM, et al. Loss-adjusted survival of cervix cancer in Khon Kaen, Northeast Thailand. Br J Cancer, 2004; 91, 106−10. doi: 10.1038/sj.bjc.6601959 [18] Chia KS, Du WB, Sankaranarayanan R, et al. Population-based cancer survival in Singapore, 1968 to 1992: an overview. Int J Cancer, 2001; 93, 142−7. doi: 10.1002/ijc.1293 [19] Nandakumar A, Anantha N, Venugopal TC. Incidence, mortality and survival in cancer of the cervix in Bangalore, India. Br J Cancer, 1995; 71, 1348−52. doi: 10.1038/bjc.1995.262 [20] Yeole BB, Kumar AVR, Kurkure A, et al. Population-based survival from cancers of breast, cervix and ovary in women in Mumbai, India. Asian Pac J Cancer Prev, 2004; 5, 308−15. [21] Swaminathan R, Selvakumaran R, Esmy PO, et al. Cancer pattern and survival in a rural district in South India. Cancer Epidemiol, 2009; 33, 325−31. doi: 10.1016/j.canep.2009.09.008 [22] Fantin R, Santamaría-Ulloa C, Barboza-Solís C. Social inequalities in cancer survival: A population-based study using the Costa Rican Cancer Registry. Cancer Epidemiol, 2020; 65, 101695. doi: 10.1016/j.canep.2020.101695 [23] Arias-Ortiz NE, de Vries E. Health inequities and cancer survival in Manizales, Colombia: a population-based study. Colomb Med (Cali), 2018; 49, 63−72. doi: 10.25100/cm.v49i1.3629 [24] Booth CM, Li G, Zhang-Salomons J, et al. The impact of socioeconomic status on stage of cancer at diagnosis and survival: a population-based study in Ontario, Canada. Cancer, 2010; 116, 4160−7. doi: 10.1002/cncr.25427 [25] Pearcey R, Miao Q, Kong WD, et al. Impact of adoption of chemoradiotherapy on the outcome of cervical cancer in Ontario: results of a population-based cohort study. J Clin Oncol, 2007; 25, 2383−8. doi: 10.1200/JCO.2006.09.1926 [26] Hislop GT, Bajdik CD, Regier MD, et al. Ethnic differences in survival for female cancers of the breast, cervix and colorectum in British Columbia, Canada. Asian Pac J Cancer Prev, 2007; 8, 209−14. [27] Boschmonar MCG, Chaviano PJJ, García AAM, et al. Trends in survival rates of cancer in Cuba. Eur J Epidemiol, 1999; 15, 521−8. doi: 10.1023/A:1007587507460 [28] Sant M, Allemani C, Santaquilani M, et al. EUROCARE-4. Survival of cancer patients diagnosed in 1995-1999. Results and commentary. Eur J Cancer, 2009; 45, 931−91. doi: 10.1016/j.ejca.2008.11.018 [29] Melan K, Janky E, Macni J, et al. Epidemiology and survival of cervical cancer in the French West-Indies: data from the Martinique Cancer Registry (2002-2011). Glob Health Action, 2017; 10, 1337341. doi: 10.1080/16549716.2017.1337341 [30] Levi F, Randimbison L, Te VC, et al. Trends in survival for patients diagnosed with cancer in Vaud, Switzerland, between 1974 and 1993. Ann Oncol, 2000; 11, 957−63. doi: 10.1023/A:1008339623847 [31] Gafà L, Amendola P, Dardanoni G, et al. Cancers of the female genital tract in Ragusa, Sicily. Eur J Epidemiol, 1995; 11, 443−6. doi: 10.1007/BF01721230 [32] Vincerževskienė I, Jasilionis D, Austys D, et al. Education predicts cervical cancer survival: a Lithuanian cohort study. Eur J Public Health, 2017; 27, 421−4. [33] Bjurberg M, Holmberg E, Borgfeldt C, et al. Primary treatment patterns and survival of cervical cancer in Sweden: A population-based Swedish Gynecologic Cancer Group Study. Gynecol Oncol, 2019; 155, 229−36. doi: 10.1016/j.ygyno.2019.08.022 [34] Brenner H, Hakulinen T. Period versus cohort modeling of up-to-date cancer survival. Int J Cancer, 2008; 122, 898−904. doi: 10.1002/ijc.23087 [35] Chakalova G, Dimitrova N, Gavrilov I, et al. Cancer burden of breast and gynecological cancers in Bulgaria: epidemiology and clinical aspects. J BUON, 2013; 18, 1038−44. [36] Waldmann A, Eisemann N, Katalinic A. Epidemiology of malignant cervical, corpus uteri and ovarian tumours - current data and epidemiological trends. Geburtshilfe Frauenheilkd, 2013; 73, 123−9. doi: 10.1055/s-0032-1328266 [37] Diaz A, Baade PD, Valery PC, et al. Comorbidity and cervical cancer survival of Indigenous and non-Indigenous Australian women: A semi-national registry-based cohort study (2003-2012). PLoS One, 2018; 13, e0196764. doi: 10.1371/journal.pone.0196764 [38] Gondos A, Brenner H, Wabinga H, et al. Cancer survival in Kampala, Uganda. Br J Cancer, 2005; 92, 1808−12. doi: 10.1038/sj.bjc.6602540 [39] Wabinga H, Ramanakumar AV, Banura C, et al. Survival of cervix cancer patients in Kampala, Uganda: 1995-1997. Br J Cancer, 2003; 89, 65−9. doi: 10.1038/sj.bjc.6601034 [40] Gultekin M, Dundar S, Kucukyildiz I. Survival of gynecological cancers in Turkey: where are we at? J Gynecol Oncol. 2017; 28:e85. [41] Berrino F, De Angelis R, Sant M. Survival for eight major cancers and all cancers combined for European adults diagnosed in 1995-99: results of the EUROCARE-4 study. Lancet Oncol. 2007; 8:773-83 . [42] Chen JG, Zhu J, Zhang YH. An analysis of survival in major malignancies during 1972-2000 in Qidong, China. China Cancer, 2006; 15, 575−8. (In Chinese [43] Li YH, Huang QH, Lin X, et al. Survival rates of malignancies and nasopharyngeal carcinoma during 2003-2005 in Sihui city. Chin J Cancer Prev Treat, 2013; 20, 734−6. (In Chinese [44] Arab M, Khayamzadeh M, Mohit M, et al. Survival of ovarian cancer in Iran: 2000-2004. Asian Pac J Cancer Prev, 2009; 10, 555−8. [45] Brenner H, Stegmaier C, Ziegler H. Trends in survival of patients with ovarian cancer in Saarland, Germany, 1976-1995. J Cancer Res Clin Oncol, 1999; 125, 109−13. doi: 10.1007/s004320050250 [46] Dahm-Kähler P, Borgfeldt C, Holmberg E, et al. Population-based study of survival for women with serous cancer of the ovary, fallopian tube, peritoneum or undesignated origin - on behalf of the Swedish Gynecological Cancer Group (SweGCG). Gynecol Oncol, 2017; 144, 167−73. doi: 10.1016/j.ygyno.2016.10.039 [47] De Angelis R, Sant M, Coleman MP, et al. Cancer survival in Europe 1999-2007 by country and age: results of EUROCARE-5-a population-based study. Lancet Oncol, 2014; 15, 23−34. doi: 10.1016/S1470-2045(13)70546-1 [48] Grann AF, Thomsen RW, Jacobsen JB, et al. Comorbidity and survival of Danish ovarian cancer patients from 2000-2011: a population-based cohort study. Clin Epidemiol, 2013; 5, 57−63. [49] Mahdy NH, Abdel-Fattah M, Ghanem H. Ovarian cancer in Alexandria from 1988 to 1997: trends and survival. East Mediterr Health J, 1999; 5, 727−39. doi: 10.26719/1999.5.4.727 [50] Nilsson B, Gustavson-Kadaka E, Hakulinen T, et al. Cancer survival in Estonian migrants to Sweden. J Epidemiol Community Health, 1997; 51, 418−23. doi: 10.1136/jech.51.4.418 [51] Okongo F, Ogwang DM, Liu BY, et al. Cancer incidence in Northern Uganda (2013–2016). Int J Cancer, 2019; 144, 2985−91. doi: 10.1002/ijc.32053 [52] Trétarre B, Molinié F, Woronoff AS, et al. Ovarian cancer in France: trends in incidence, mortality and survival, 1980-2012. Gynecol Oncol, 2015; 139, 324−9. doi: 10.1016/j.ygyno.2015.09.013 [53] Zhou Y, Xiang ZS, Ma JY, et al. Survival of cancer patients in Fujian, Southeast China: a population-based cancer registry study. Neoplasma, 2021; 68, 892−8. doi: 10.4149/neo_2021_210203N168 [54] Li HZ, Du LB, Li QL, et al. Cancer survival in Haining and Jiashan cancer registry areas of Zhejiang province. China Cancer, 2020; 29, 14−21. (In Chinese [55] Cheung FY, Mang OWK, Law SCK. A population-based analysis of incidence, mortality, and stage-specific survival of cervical cancer patients in Hong Kong: 1997-2006. Hong Kong Med J, 2011; 17, 89−95. [56] Chiang CJ, Lo WC, Yang YW, et al. Incidence and survival of adult cancer patients in Taiwan, 2002-2012. J Formos Med Assoc, 2016; 115, 1076−88. doi: 10.1016/j.jfma.2015.10.011 [57] Matsuda T, Ajiki W, Marugame T, et al. Population-based survival of cancer patients diagnosed between 1993 and 1999 in Japan: a chronological and international comparative study. Jpn J Clin Oncol, 2011; 41, 40−51. doi: 10.1093/jjco/hyq167 [58] Yagi A, Ueda Y, Kakuda M, et al. Epidemiologic and clinical analysis of cervical cancer using data from the population-based Osaka Cancer Registry. Cancer Res, 2019; 79, 1252−9. [59] Kang MJ, Won YJ, Lee JJ, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2019. Cancer Res Treat, 2022; 54, 330−44. doi: 10.4143/crt.2022.128 [60] Shin DW, Bae J, Ha J, et al. Conditional relative survival of cervical cancer: a Korean National Cancer Registry Study. J Gynecol Oncol, 2021; 32, e5. doi: 10.3802/jgo.2021.32.e5 [61] Maláková K, Cabasag CJ, Bardot A, et al. Cancer survival in Thailand from 1997 to 2012: assessing the impact of universal health coverage. J Cancer Policy, 2022; 34, 100353. doi: 10.1016/j.jcpo.2022.100353 [62] Laudico AV, Mirasol-Lumague MR, Mapua CA, et al. Cancer incidence and survival in Metro Manila and Rizal province, Philippines. Jpn J Clin Oncol, 2010; 40, 603−12. doi: 10.1093/jjco/hyq034 [63] Alawadhi E, Al-Awadi A, Elbasmi A, et al. Cancer survival by stage at diagnosis in Kuwait: a population-based study. J Oncol, 2019; 2019, 8463195. [64] Gultekin M, Dundar S, Kucukyildiz I, et al. Survival of gynecological cancers in Turkey: where are we at?. J Gynecol Oncol, 2017; 28, e85. doi: 10.3802/jgo.2017.28.e85 [65] Gatta G, Lasota MB, Verdecchia A. Survival of European women with gynaecological tumours, during the period 1978-1989. Eur J Cancer, 1998; 34, 2218−25. doi: 10.1016/S0959-8049(98)00326-8 [66] Bielska-Lasota M, Inghelmann R, van de Poll-Franse L, et al. Trends in cervical cancer survival in Europe, 1983-1994: a population-based study. Gynecol Oncol, 2007; 105, 609−19. doi: 10.1016/j.ygyno.2007.01.048 [67] Jensen KE, Hannibal CG, Nielsen A, et al. Social inequality and incidence of and survival from cancer of the female genital organs in a population-based study in Denmark, 1994-2003. Eur J Cancer, 2008; 44, 2003−17. doi: 10.1016/j.ejca.2008.06.014 [68] Brenner H, Hakulinen T. Long-term cancer patient survival achieved by the end of the 20th century: most up-to-date estimates from the nationwide Finnish cancer registry. Br J Cancer, 2001; 85, 367−71. doi: 10.1054/bjoc.2001.1905 [69] Talbäck M, Dickman PW. Predicting the survival of cancer patients recently diagnosed in Sweden and an evaluation of predictions published in 2004. Acta Oncol, 2012; 51, 17−27. doi: 10.3109/0284186X.2011.626444 [70] Emmett M, Gildea C, Nordin A, et al. Cervical cancer - does the morphological subtype affect survival rates?. J Obstet Gynaecol, 2018; 38, 548−55. doi: 10.1080/01443615.2017.1379062 [71] Grundmann N, Meisinger C, Trepel M, et al. Trends in cancer incidence and survival in the Augsburg study region: results from the Augsburg cancer registry. BMJ Open, 2020; 10, e036176. doi: 10.1136/bmjopen-2019-036176 [72] Brenner H, Stegmaier C, Ziegler H. Long-term survival of cancer patients in Germany achieved by the beginning of the third millenium. Ann Oncol, 2005; 16, 981−6. doi: 10.1093/annonc/mdi186 [73] Levi F, La Vecchia C, Randimbison L, et al. Incidence, mortality and survival from invasive cervical cancer in Vaud, Switzerland, 1974-1991. Ann Oncol, 1994; 5, 747−52. doi: 10.1093/oxfordjournals.annonc.a058980 [74] Wenzel HHB, Bekkers RLM, Lemmens VEPP, et al. No improvement in survival of older women with cervical cancer—a nationwide study. Eur J Cancer, 2021; 151, 159−67. doi: 10.1016/j.ejca.2021.04.014 [75] Houterman S, Janssen-Heijnen MLG, van de Poll-Franse LV, et al. Higher long-term cancer survival rates in southeastern Netherlands using up-to-date period analysis. Ann Oncol, 2006; 17, 709−12. doi: 10.1093/annonc/mdj139 [76] Minelli L, Stracci F, Prandini S, et al. Gynaecological cancers in Umbria (Italy): trends of incidence, mortality and survival, 1978-1998. Eur J Obstet Gynecol Reprod Biol, 2004; 115, 59−65. doi: 10.1016/j.ejogrb.2003.11.026 [77] Pavlík T, Májek O, Büchler T, et al. Trends in stage-specific population-based survival of cancer patients in the Czech Republic in the period 2000-2008. Cancer Epidemiol, 2014; 38, 28−34. doi: 10.1016/j.canep.2013.11.002 [78] Ojamaa K, Innos K, Baburin A, et al. Trends in cervical cancer incidence and survival in Estonia from 1995 to 2014. BMC Cancer, 2018; 18, 1075. doi: 10.1186/s12885-018-5006-1 [79] Ulinskas K, Aleknaviciene B, Smailyte G. Demographic differences in cervical cancer survival in Lithuania. Open Med, 2013; 8, 16−21. doi: 10.2478/s11536-012-0051-7 [80] Bravo LE, García LS, Collazos PA. Cancer survival in Cali, Colombia: a population-based study, 1995-2004. Colomb Med (Cali), 2014; 45, 110−6. doi: 10.25100/cm.v45i3.1525 [81] Gari A, Lotocki R, Krepart G, et al. Cervical cancer in the province of Manitoba: a 30-year experience. J Obstet Gynaecol Can, 2008; 30, 788−95. doi: 10.1016/S1701-2163(16)32943-7 [82] Jemal A, Ward EM, Johnson CJ, et al. Annual report to the nation on the status of cancer, 1975-2014, featuring survival. J Natl Cancer Inst, 2017; 109, djx030. [83] Gatta G, Capocaccia R, Coleman MP, et al. Toward a comparison of survival in American and European cancer patients. Cancer, 2000; 89, 893−900. doi: 10.1002/1097-0142(20000815)89:4<893::AID-CNCR24>3.0.CO;2-9 [84] Surveillance Research Program NCI. SEER*Explorer: An interactive website for SEER cancer statistics. https://seer.cancer.gov/statistics-network/explorer/application.html?site=1&data_type=1&graph_type=2&compareBy=sex&chk_sex_3=3&chk_sex_2=2&rate_type=2&race=1&age_range=1&hdn_stage=101&advopt_precision=1&advopt_show_ci=on&hdn_view=0&advopt_show_apc=on&advopt_display=2#resultsRegion0. [2023-06-07]. [85] Taylor R, Bell J, Coates M, et al. Cervical cancer in New South Wales women: five-year survival, 1972 to 1991. Aust N Z J Public Health, 1996; 20, 413−20. doi: 10.1111/j.1467-842X.1996.tb01055.x [86] Yu XQ, O'Connell DL, Gibberd RW, et al. Trends in survival and excess risk of death after diagnosis of cancer in 1980-1996 in New South Wales, Australia. Int J Cancer, 2006; 119, 894−900. doi: 10.1002/ijc.21909 [87] Inoue S, Hosono S, Ito H, et al. Improvement in 5-year relative survival in cancer of the corpus uteri from 1993-2000 to 2001-2006 in Japan. J Epidemiol, 2018; 28, 75−80. doi: 10.2188/jea.JE20170008 [88] Ioka A, Tsukuma H, Ajiki W, et al. Influence of hospital procedure volume on uterine cancer survival in Osaka, Japan. Cancer Sci, 2005; 96, 689−94. doi: 10.1111/j.1349-7006.2005.00094.x [89] Yagi A, Ueda Y, Ikeda S, et al. Improved long-term survival of corpus cancer in Japan: a 40-year population-based analysis. Int J Cancer, 2022; 150, 232−42. doi: 10.1002/ijc.33799 [90] Ha HI, Chang HK, Park SJ, et al. The incidence and survival of cervical, ovarian, and endometrial cancer in Korea, 1999-2017: Korea Central Cancer Registry. Obstet Gynecol Sci, 2021; 64, 444−53. doi: 10.5468/ogs.21116 [91] Dalton SO, Olsen MH, Johansen C, et al. Socioeconomic inequality in cancer survival - changes over time. A population-based study, Denmark, 1987-2013. Acta Oncol, 2019; 58, 737−44. doi: 10.1080/0284186X.2019.1566772 [92] Ojamaa K, Veerus P, Baburin A, et al. Increasing incidence and survival of corpus uteri cancer in Estonia over the past two decades. Cancer Epidemiol, 2019; 62, 101566. doi: 10.1016/j.canep.2019.101566 [93] Dickman PW, Hakulinen T, Luostarinen T, et al. Survival of cancer patients in Finland 1955-1994. Acta Oncol, 1999; 38 Suppl 12, 1-103. [94] Boll D, Verhoeven RHA, van der Aa MA, et al. Incidence and survival trends of uncommon corpus uteri malignancies in the Netherlands, 1989-2008. Int J Gynecol Cancer, 2012; 22, 599−606. doi: 10.1097/IGC.0b013e318244cedc [95] Zhu J, Xu YY, Zhang YH, et al. Analysis of the survival trend of ovary cancer in Qidong City, Jiangsu Province from 1977 to 2016. Journal of Modern Oncology,2023; 31:1731-5. (In Chinese) [96] Loka A, Tsukuma H, Ajiki W, et al. Ovarian cancer incidence and survival by histologic type in Osaka, Japan. Cancer Sci, 2003; 94, 292−6. doi: 10.1111/j.1349-7006.2003.tb01435.x [97] Ries LAG. Ovarian cancer: Survival and treatment differences by age. Cancer, 1993; 71, 524−9. [98] Cabasag CJ, Butler J, Arnold M, et al. Exploring variations in ovarian cancer survival by age and stage (ICBP SurvMark-2): a population-based study. Gynecol Oncol, 2020; 157, 234−44. doi: 10.1016/j.ygyno.2019.12.047 [99] Lambert P, Galloway K, Altman A, et al. Ovarian cancer in Manitoba: trends in incidence and survival, 1992-2011. Curr Oncol, 2017; 24, 78−84. doi: 10.3747/co.24.3312 [100] Karim-Kos HE, de Vries E, Soerjomataram I, et al. Recent trends of cancer in Europe: a combined approach of incidence, survival and mortality for 17 cancer sites since the 1990s. Eur J Cancer, 2008; 44, 1345−89. doi: 10.1016/j.ejca.2007.12.015 [101] Hamidou Z, Causeret S, Dabakuyo TS, et al. Population-based study of ovarian cancer in Côte d'Or: prognostic factors and trends in relative survival rates over the last 20 years. BMC Cancer, 2010; 10, 622. doi: 10.1186/1471-2407-10-622 [102] Gondos A, Holleczek B, Arndt V, et al. Trends in population-based cancer survival in Germany: to what extent does progress reach older patients? Ann Oncol. 2007; 18:1253-9. ) [103] Karim-Kos HE, Kiemeney LALM, Louwman MWJ, et al. Progress against cancer in the Netherlands since the late 1980s: An epidemiological evaluation. Int J Cancer, 2012; 130, 2981−9. doi: 10.1002/ijc.26315 [104] Balvert-Locht HR, Coebergh JWW, Hop WCJ, et al. Improved prognosis of ovarian cancer in The Netherlands during the period 1975-1985: a registry-based study. Gynecol Oncol, 1991; 42, 3−8. doi: 10.1016/0090-8258(91)90222-Q [105] Akbari A, Azizmohammad Looha M, Moradi A, Akbari ME. Ovarian Cancer in Iran: National Based Study. Iran J Public Health. 2023; 52:797-808. [106] Wei KR, Liang ZH, Cen HS. Net survival of cancers in Zhongshan city, Guangdong province, 1995-2009. China Cancer, 2016; 25, 747−51. (In Chinese [107] Wei KR, Liang ZH, Li ZM. Net survival of major cancers in Zhongshan city of Guangdong province from 2003 to 2013. China Cancer, 2020; 29, 103−7. (In Chinese [108] Allemani C, Matsuda T, Di Carlo V, et al. Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet, 2018; 391, 1023−75. doi: 10.1016/S0140-6736(17)33326-3 [109] Allemani C, Weir HK, Carreira H, et al. Global surveillance of cancer survival 1995-2009: analysis of individual data for 25 676 887 patients from 279 population-based registries in 67 countries (CONCORD-2). Lancet, 2015; 385, 977−1010. doi: 10.1016/S0140-6736(14)62038-9 [110] Lim GH, Wong CS, Chow KY, et al. Trends in long-term cancer survival in Singapore: 1968-2002. Ann Acad Med Singap, 2009; 38, 99−105. doi: 10.47102/annals-acadmedsg.V38N2p99 [111] Zeng HM, Chen WQ, Zheng RS, et al. Changing cancer survival in China during 2003–15: a pooled analysis of 17 population-based cancer registries. Lancet Glob Health, 2018; 6, e555−67. doi: 10.1016/S2214-109X(18)30127-X [112] Quaresma M, Coleman MP, Rachet B. 40-year trends in an index of survival for all cancers combined and survival adjusted for age and sex for each cancer in England and Wales, 1971-2011: A population-based study. Lancet, 2015; 385, 1206−18. doi: 10.1016/S0140-6736(14)61396-9 [113] Sant M, Lopez MDC, Agresti R, et al. Survival of women with cancers of breast and genital organs in Europe 1999-2007: Results of the EUROCARE-5 study. Eur J Cancer, 2015; 51, 2191−205. doi: 10.1016/j.ejca.2015.07.022 [114] Antunes L, Roche L, José BM. Trends in net survival from corpus uteri cancer in six European Latin countries: results from the SUDCAN population-based study. Eur J Cancer Prev, 2017; 26, S100−6. doi: 10.1097/CEJ.0000000000000294 [115] Antunes L, Santos LL, Bento MJ. Survival from cancer in the north region of Portugal: results from the first decade of the millennium. Eur J Cancer Prev, 2017; 26, S170−5. doi: 10.1097/CEJ.0000000000000378 [116] Chen TH, Jansen L, Gondos A, et al. Survival of endometrial cancer patients in Germany in the early 21st century: a period analysis by age, histology, and stage. BMC Cancer, 2012; 12, 128. doi: 10.1186/1471-2407-12-128 [117] Jansen L, Castro FA, Gondos A, et al. Recent cancer survival in Germany: an analysis of common and less common cancers. Int J Cancer, 2015; 136, 2649−58. doi: 10.1002/ijc.29316 [118] Cowppli-Bony A, Uhry Z, Remontet L, et al. Survival of solid cancer patients in France, 1989-2013: a population-based study. Eur J Cancer Prev, 2017; 26, 461−8. doi: 10.1097/CEJ.0000000000000372 [119] Innos K, Baburin A, Aareleid T. Cancer patient survival in Estonia 1995-2009: Time trends and data quality. Cancer Epidemiol, 2014; 38, 253−8. doi: 10.1016/j.canep.2014.03.008 [120] Arnold M, Rutherford MJ, Bardot A, et al. Progress in cancer survival, mortality, and incidence in seven high-income countries 1995-2014 (ICBP SURVMARK-2): a population-based study. Lancet Oncol, 2019; 20, 1493−505. doi: 10.1016/S1470-2045(19)30456-5 [121] dos Santos FLC, Wojciechowska U, Michalek IM, et al. Progress in cancer survival across last two decades: a nationwide study of over 1.2 million Polish patients diagnosed with the most common cancers. Cancer Epidemiol, 2022; 78, 102147. doi: 10.1016/j.canep.2022.102147 [122] Myklebust TÅ, Andersson T, Bardot A, et al. Can different definitions of date of cancer incidence explain observed international variation in cancer survival? An ICBP SURVMARK-2 study. Cancer Epidemiol, 2020; 67, 101759. doi: 10.1016/j.canep.2020.101759 [123] Ojamaa K, Veerus P, Baburin A, et al. Time trends in ovarian cancer survival in Estonia by age and stage. Int J Gynecol Cancer, 2017; 27, 44−9. doi: 10.1097/IGC.0000000000000858 [124] Walters S, Benitez-Majano S, Muller P, et al. Is England closing the international gap in cancer survival?. Br J Cancer, 2015; 113, 848−60. doi: 10.1038/bjc.2015.265 [125] Levi F, Randimbison L, Te VC, et al. Trends in cancer survival in Vaud, Switzerland. Eur J Cancer, 1992; 28, 1490−5. doi: 10.1016/0959-8049(92)90551-C [126] Ha HI, Chang HK, Park SJ, et al. Correction of Funding information: The incidence and survival of cervical, ovarian, and endometrial cancer in Korea, 1999-2017: Korea Central Cancer Registry. Obstet Gynecol Sci, 2022; 65, 384. doi: 10.5468/ogs.21116.e1 [127] Jun J, Zhang YH, Chen YS, et al. Analysis of survival rate of cervical cancer patients during 2001-2007 in Qidong City. Chin J Clin Oncol Rehab, 2011; 18, 193−6. (In Chinese [128] Lu HS, Li L, Cheng YR, et al. Timely estimates of 5-year relative survival for patients with cervical cancer: a period analysis using cancer registry data from Taizhou, Eastern China. Front Public Health, 2022; 10, 926058. doi: 10.3389/fpubh.2022.926058 [129] Choi HCW, Lam KO, Pang HHM, et al. Global comparison of cancer outcomes: standardization and correlation with healthcare expenditures. BMC Public Health, 2019; 19, 1065. doi: 10.1186/s12889-019-7384-y [130] GBD 2019 Human Resources for Health Collaborators. Measuring the availability of human resources for health and its relationship to universal health coverage for 204 countries and territories from 1990 to 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet, 2022; 399, 2129−54. doi: 10.1016/S0140-6736(22)00532-3 [131] Riano I, Contreras-Chavez P, Pabon CM, et al. An overview of cervical cancer prevention and control in Latin America and the Caribbean countries. Hematol Oncol Clin North Am, 2024; 38, 13−33. doi: 10.1016/j.hoc.2023.05.012 [132] Goss PE, Lee BL, Badovinac-Crnjevic T, et al. Planning cancer control in Latin America and the Caribbean. Lancet Oncol, 2013; 14, 391−436. doi: 10.1016/S1470-2045(13)70048-2 [133] Denny L. Control of cancer of the cervix in low- and middle-income countries. Ann Surg Oncol, 2015; 22, 728−33. [134] Bouvard V, Wentzensen N, Mackie A, et al. The IARC perspective on cervical cancer screening. N Engl J Med, 2021; 385, 1908−18. doi: 10.1056/NEJMsr2030640 [135] Arbyn M, Ronco G, Anttila A, et al. Evidence regarding human papillomavirus testing in secondary prevention of cervical cancer. Vaccine, 2012; 30 Suppl 5, F88-99. [136] Lee SY. Tailored therapy based on molecular characteristics in endometrial cancer. BioMed Res Int, 2021; 2021, 2068023. [137] van Weelden WJ, Massuger LFAG, ENITEC, et al. Anti-estrogen treatment in endometrial cancer: a systematic review. Front Oncol, 2019; 9, 359. doi: 10.3389/fonc.2019.00359 [138] Urick ME, Bell DW. Clinical actionability of molecular targets in endometrial cancer. Nat Rev Cancer, 2019; 19, 510−21. doi: 10.1038/s41568-019-0177-x [139] Fader AN, Roque DM, Siegel E, et al. Randomized phase II trial of carboplatin-paclitaxel versus carboplatin-paclitaxel-trastuzumab in uterine serous carcinomas that overexpress human epidermal growth factor receptor 2/neu. J Clin Oncol, 2018; 36, 2044−51. doi: 10.1200/JCO.2017.76.5966 [140] Levine DA, The Cancer Genome Atlas Research Network. Integrated genomic characterization of endometrial carcinoma. Nature, 2013; 497, 67−73. doi: 10.1038/nature12113 [141] Aghajanian C, Filiaci V, Dizon DS, et al. A phase II study of frontline paclitaxel/carboplatin/bevacizumab, paclitaxel/carboplatin/temsirolimus, or ixabepilone/carboplatin/bevacizumab in advanced/recurrent endometrial cancer. Gynecol Oncol, 2018; 150, 274−81. doi: 10.1016/j.ygyno.2018.05.018 [142] Lorusso D, Ferrandina G, Colombo N, et al. Carboplatin-paclitaxel compared to carboplatin-paclitaxel-bevacizumab in advanced or recurrent endometrial cancer: MITO END-2 - a randomized phase II trial. Gynecol Oncol, 2019; 155, 406−12. doi: 10.1016/j.ygyno.2019.10.013 [143] Latha TS, Panati K, Gowd DSK, et al. Ovarian cancer biology and immunotherapy. Int Rev Immunol, 2014; 33, 428−40. doi: 10.3109/08830185.2014.921161 [144] Torre LA, Trabert B, DeSantis CE, et al. Ovarian cancer statistics, 2018. CA Cancer J Clin, 2018; 68, 284−96. doi: 10.3322/caac.21456 [145] Yang C, Xia BR, Zhang ZC, et al. Immunotherapy for ovarian cancer: adjuvant, combination, and neoadjuvant. Front Immunol, 2020; 11, 577869. doi: 10.3389/fimmu.2020.577869 [146] Zhang H, Liu XY, Penn-Kekana L, et al. A systematic review of the profile and density of the maternal and child health workforce in China. Hum Resour Health, 2021; 19, 125. doi: 10.1186/s12960-021-00662-4 [147] Song YF, Liu XX, Yin ZD, et al. Human papillomavirus vaccine coverage among the 9-45-year-old female population of China in 2018-2020. Chin J Vaccines Immunization, 2021; 27, 570−5. (In Chinese [148] Tabatabaei FS, Saeedian A, Azimi A, et al. Evaluation of survival rate and associated factors in patients with cervical cancer: a retrospective cohort study. J Res Health Sci, 2022; 22, e00552. doi: 10.34172/jrhs.2022.87 [149] Moore DH. Cervical cancer. Obstet Gynecol, 2006; 107, 1152−61. doi: 10.1097/01.AOG.0000215986.48590.79 [150] Solmaz U, Mat E, Dereli ML, et al. Stage-III and -IV endometrial cancer: A single oncology centre review of 104 cases. J Obstet Gynaecol, 2016; 36, 81−6. doi: 10.3109/01443615.2015.1041890 [151] Guarneri V, Barbieri E, Dieci MV, et al. Timing for starting second-line therapy in recurrent ovarian cancer. Expert Rev Anticancer Ther, 2011; 11, 49−55. doi: 10.1586/era.10.204 [152] Schorge JO, Garrett LA, Goodman A. Cytoreductive surgery for advanced ovarian cancer: quo vadis?. Oncology (Williston Park), 2011; 25, 928−34. [153] Lea JS, Lin KY. Cervical cancer. Obstet Gynecol Clin North Am, 2012; 39, 233−53. doi: 10.1016/j.ogc.2012.02.008 [154] Meng YF, Chu T, Lin ST, et al. Clinicopathological characteristics and prognosis of cervical cancer with different histological types: A population-based cohort study. Gynecol Oncol, 2021; 163, 545−51. doi: 10.1016/j.ygyno.2021.10.007 [155] Amant F, Moerman P, Neven P, et al. Endometrial cancer. Lancet, 2005; 366, 491−505. doi: 10.1016/S0140-6736(05)67063-8 [156] Tai YJ, Chiang CJ, Chiang YC, et al. Age-specific trend and birth cohort effect on different histologic types of uterine corpus cancers. Sci Rep, 2023; 13, 1019. doi: 10.1038/s41598-022-21669-4 [157] Mori S, Gotoh O, Kiyotani K, et al. Genomic alterations in gynecological malignancies: histotype-associated driver mutations, molecular subtyping schemes, and tumorigenic mechanisms. J Hum Genet, 2021; 66, 853−68. doi: 10.1038/s10038-021-00940-y [158] Granier C, Gey A, Roncelin S, et al. Immunotherapy in older patients with cancer. Biomed J, 2021; 44, 260−271. doi: 10.1016/j.bj.2020.07.009 [159] Vitale SG, Capriglione S, Zito G, et al. Management of endometrial, ovarian and cervical cancer in the elderly: current approach to a challenging condition. Arch Gynecol Obstet, 2019; 299, 299−315. doi: 10.1007/s00404-018-5006-z [160] Fentiman IS. Are the elderly receiving appropriate treatment for cancer?. Ann Oncol, 1996; 7, 657−8. doi: 10.1093/oxfordjournals.annonc.a010712 [161] Yamamoto M, Yoshida Y, Itani Y, et al. How do doctors choose treatment for older gynecological cancer patients? A Japanese Gynecologic Oncology Group survey of gynecologic oncologists. Int J Clin Oncol, 2020; 25, 741−5. doi: 10.1007/s10147-019-01574-z [162] Goodwin JS, Hunt WC, Samet JM. Determinants of cancer therapy in elderly patients. Cancer, 1993; 72, 594−601. doi: 10.1002/1097-0142(19930715)72:2<594::AID-CNCR2820720243>3.0.CO;2-# [163] Carney ME, Lancaster JM, Ford C, et al. A population-based study of patterns of care for ovarian cancer: who is seen by a gynecologic oncologist and who is not?. Gynecol Oncol, 2002; 84, 36−42. doi: 10.1006/gyno.2001.6460 [164] Liu Z, Zhao LY, Man QQ, et al. Dietary micronutrients intake status among Chinese elderly people living at home: data from CNNHS 2010-2012. Nutrients, 2019; 11, 1787. doi: 10.3390/nu11081787 [165] Ongan D, Rakıcıoğlu N. Nutritional status and dietary intake of institutionalized elderly in Turkey: a cross-sectional, multi-center, country representative study. Arch Gerontol Geriatr, 2015; 61, 271−6. doi: 10.1016/j.archger.2015.05.004 -
 Supplementary_Information-revised 24145 放网站.docx
Supplementary_Information-revised 24145 放网站.docx
 24145+Supplementary Materials.pdf
24145+Supplementary Materials.pdf
-

 点击查看大图
点击查看大图
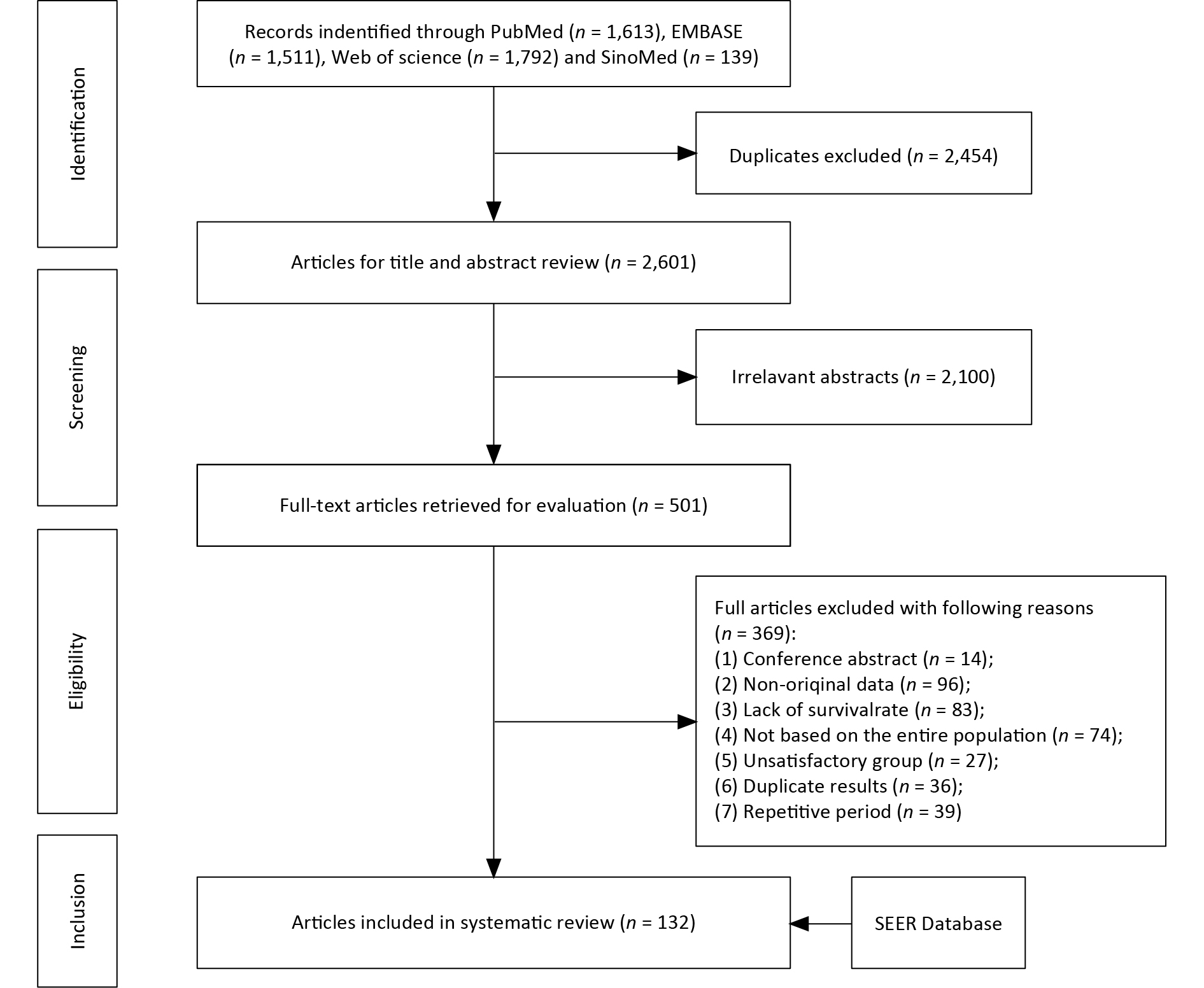
计量
- 文章访问数: 941
- HTML全文浏览量: 381
- PDF下载量: 37
- 被引次数: 0

 Quick Links
Quick Links