

 下载:
下载:

-
Stroke is the third-leading cause of disability-adjusted life years (DALYs) and poses a significant public health challenge worldwide[1]. Developing countries, including China, continue to face a substantial burden from stroke. Since 1990, China has reported the highest global stroke burden, with 2.19 million deaths and 45.9 million DALYs recorded in 2019[2].
Air pollution remains a critical contributor to stroke-related mortality. Over the past few decades, global air pollution levels have steadily risen, with stroke mortality attributable to air pollution now estimated to account for approximately 14% of total deaths[3]. Numerous studies have demonstrated that short-term exposure to particulate matter with an aerodynamic diameter of ≤ 2.5 μm (PM2.5)[4] and ≤ 10 μm (PM10)[5], as well as carbon monoxide (CO)[6], sulfur dioxide (SO2)[7], nitrogen dioxide (NO2)[8], and ozone (8-hour average concentration) (O3)[9], is associated with an increased risk of stroke mortality.
Qingdao, located on the east coast of China, features a unique geographical position and climate. This prominent city has experienced rapid development and has transformed into a major urban center with a population exceeding 9 million, largely owing to accelerated urbanization and national policy initiatives. However, this growth has also resulted in greater environmental pollution, driven by urban land expansion, as well as an increase in buildings and vehicles. Several studies have identified traffic exhaust, industrial emissions, and construction dust as the primary sources of pollution in Qingdao[10]. The city exhibits distinctive features, including a pronounced temperate monsoon climate, with dry, cool winters and wet, warm summers. It is essential to recognize that the rising levels of air pollution across different seasons cannot be overlooked. Therefore, incorporating climate characteristics into the analysis of air pollution is crucial.
Data on stroke mortality in Qingdao from 2014 to 2019 were obtained from the Chronic Disease Surveillance Monitoring System, with approval from the Ethics Committee of the Qingdao Municipal Center for Disease Control and Prevention. The committee determined that informed consent was not required for this study. The collected data included variables such as gender, age, date of death, International Classification of Diseases, 10th Revision (ICD-10) codes, cause of death, and cause-of-death diagnosis. Stroke-related mortality was classified based on ICD-10 codes for cerebrovascular diseases: hemorrhagic stroke (I60-I61), ischemic stroke (I63), and unclassified stroke (I64), accompanied by corresponding case summaries. To ensure study accuracy, residents of Qingdao were included, while patients whose cerebrovascular disease resulted from accidents or other unrelated causes were excluded from the analysis.
Daily average concentration data for PM2.5, PM10, SO2, NO2, CO, and O3, as well as daily mean pressure (hPa), temperature (°C), relative humidity (%), and wind speed (m/s), were collected from 10 districts in Qingdao from January 1, 2014, to December 31, 2019. The atmospheric pollutant data were provided by the Qingdao Eco-Environmental Monitoring Center of Shandong Province, while the meteorological data were sourced from the Qingdao Meteorological Observatory.
In this study, a distributed lag nonlinear model (DLNM) was developed to estimate the delayed and nonlinear effects of atmospheric pollutants on stroke mortality risk. The findings aim to inform local initiatives for the effective prevention and control of stroke-related health issues. The model was formulated as follows:
$$ \begin{aligned} Log(E(Yt))= & \alpha +cb(pollutants)+ns(temp,df=3)+\\ & ns(rh,df=3)+ns(pr,df=3)+\\ & ns(wind,df=3) +stratum+holidays \end{aligned} $$ where Yt denotes the daily cases of stroke mortality at time t; α is the intercept; cb (pollutants) is a cross-basis function that fits the lagged effects of daily mean concentrations of PM2.5, PM10, CO, O3, SO2, and NO2 in the single-pollutant model. Natural cubic splines (ns) with 3 degrees of freedom (df) were used to control for daily mean temperature (temp), relative humidity (rh), atmospheric pressure(pr), and wind speed(wind) based on previous literature[5]. Additionally, a stratum was employed to elucidate long-term and seasonal trends. We also adjusted the data to account for the effects of public holidays. The hysteresis effects of the average daily concentrations of PM2.5, PM10, CO, O3, SO2, and NO2 were integrated into the model.
In our study, we utilized single-day lag exposures (ranging from lag 0 to lag 7 days) and moving average lag exposures (spanning from lag 1 to lag 7 days) to examine the acute effects of ambient air pollution on the percentage change in stroke mortality. We identified potentially susceptible subgroups and investigated differences among these groups by incorporating interaction terms and stratifying the data based on various factors. Specifically, we stratified the seasons into warm seasons (May to October) and cold seasons (November to April of the following year) and categorized strokes into hemorrhagic and ischemic types. We then conducted a comprehensive analysis of both ischemic and hemorrhagic strokes to further elucidate variations in risk within these stroke types. We also took into account gender (males and females) and age (N-aging: individuals younger than 75, and aging: individuals aged 75 or older). These subgroup analyses provided insights into specific population segments that may be more susceptible to the effects of air pollutants.
Subsequently, we conducted a sensitivity analysis by adjusting the degrees of freedom for meteorological factors, including mean temperature, relative humidity, air pressure, and wind speed, varying from 3 to between 4 and 6. This adjustment enabled us to observe the impact of different degrees of freedom for these covariates on the association between air pollutants and stroke mortality outcomes. Finally, we employed excess risk to quantify this correlation, which represented the percentage change (PC%) in stroke mortality associated with an interquartile range increase in atmospheric pollutant concentration. This is expressed as PC% =( [e^β - 1]×100%), along with the 95% confidence interval (95% CI). Statistical significance was determined by a P-value of 0.05 for two-tailed tests. All statistical analyses were performed using the “dlnm” package to create the DLNM model in R 4.2.3 (The R project for statistical computing, http://www.r-project.org ).
The distributions of monthly stroke deaths and meteorological factors in Qingdao are summarized in Table 1, which presents the characteristics of stroke-related mortality based on the collected data. A total of 46,263 patients, including 24,947 males and 21,316 females, died from stroke. The number of patients aged 75 or older (29,975 cases) was higher than that of individuals younger than 75 (16,228 cases). Across all demographic groups, including subgroups by sex and age, the number of deaths during the cold season exceeded those observed in the warm season. Additionally, the distributions of pollutants and meteorological factors in Qingdao are summarized in Supplementary Table S1.
Table 1. Characteristics of study participants in Qingdao, China (2014−2019)
Group Total HS IS Unspecified All Warm Cold All Warm Cold All Warm Cold All Warm Cold All 46263 20208 26055 18661 8284 10377 26368 11388 14980 1234 536 698 Sex Male 24947 10969 13978 10491 4685 5806 13806 6004 7802 650 − − Female 21316 9239 12077 8170 3599 4571 12562 5384 7178 584 − − Age Aging 29975 12834 17141 9897 4245 5652 19184 8212 10972 894 − − N-aging 16288 7374 8914 8764 4039 4725 7184 3176 4008 340 − − Notes. Total, Total stroke; HS, Hemorrhagic Stroke; IS, Ischemic Stroke; Unspecified is Stroke, not specifically bleeding or infarction stroke; aging, individuals aged 75 or older; N-aging, individuals younger than 75; Warm season, April to September; Cold season, October to March of the next year. Spearman’s correlation analysis results are presented in Table 2. PM2.5 exhibited significant positive correlations with precipitation (rs = 0.29), while it showed negative correlations with temperature (rs = −0.38), wind speed (rs = −0.24), and relative humidity (rs = −0.03), all with P-values less than 0.01. Similarly, other pollutants displayed weak correlations with meteorological factors. Notably, a positive correlation was also observed between O3 and temperature (rs = 0.66).
Table 2. Spearman Correlation of Air Pollutants in Qingdao, China (2014−2019)
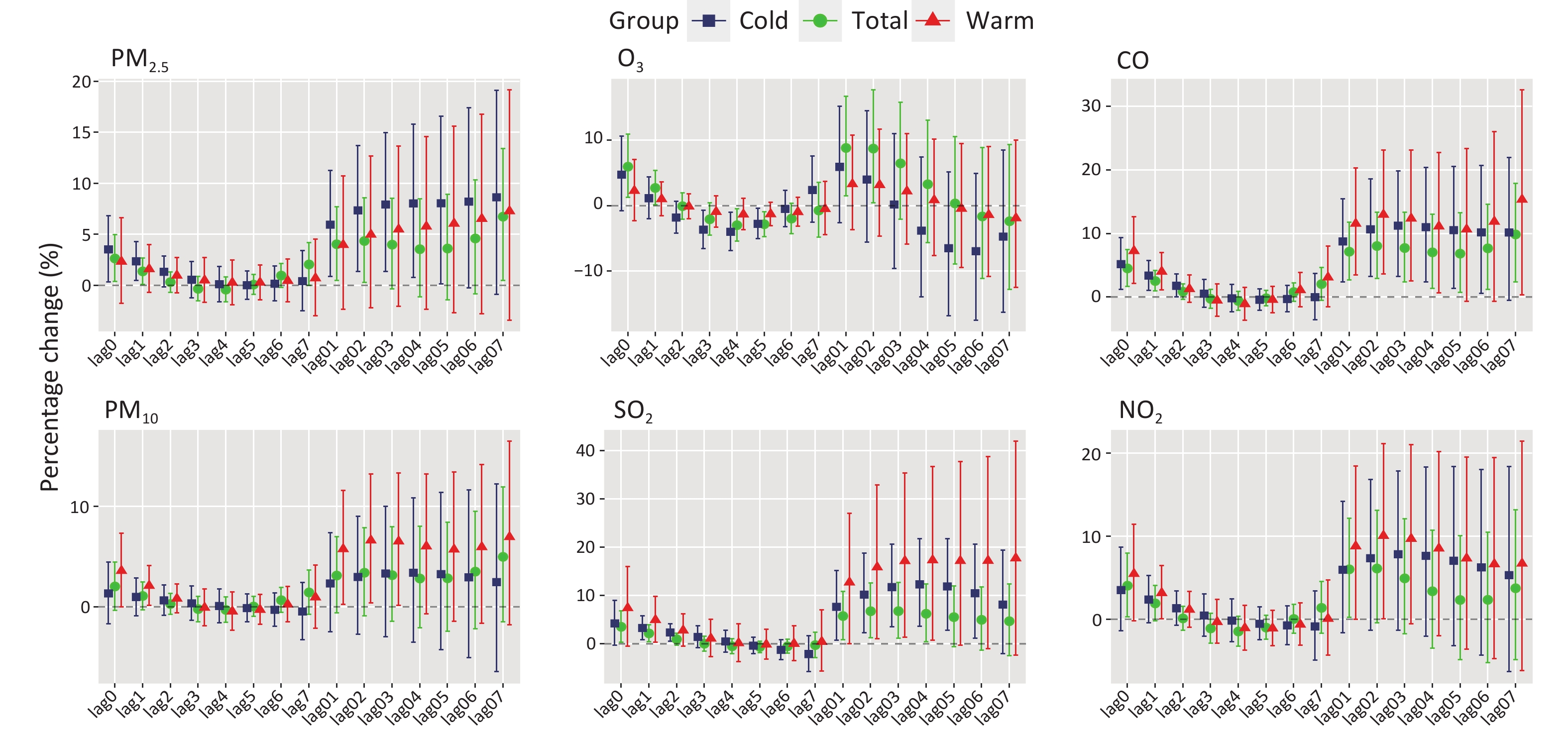
pr temp rh wind PM2.5 PM10 O3 CO SO2 NO2 pr 1.00** temp −0.87** 1.00** rh −0.39** 0.36** 1.00** wind −0.06 −0.10** −0.14** 1.00** PM2.5 0.29** −0.38** −0.03 −0.24** 1.00** PM10 0.26** −0.34** −0.23** −0.15** 0.89** 1.00** O3 −0.58** 0.66** −0.01** −0.10** −0.15** −0.07** 1.00** CO 0.42** −0.52** −0.09** −0.27** 0.91** 0.79** −0.29** 1.00** SO2 0.48** −0.49** −0.27** −0.18** 0.61** 0.56** −0.27** 0.72** 1.00** NO2 0.40** −0.47** −0.34** −0.41** 0.75** 0.73** −0.24** 0.82** 0.66** 1.00** Notes. **P < 0.001; PM2.5, particulate matter with an aerodynamic diameter of ≤ 2.5μm; PM10, particulate matter with an aerodynamic diameter of ≤ 10μm; CO, carbon monoxide; O3, ozone; SO2, sulfur dioxide; NO2, nitrogen dioxide; pr, daily mean pressure; temp, mean temperature; rh, relative humidity; wind, wind speed. Stroke subcategories were stratified to compare mortality risk between two groups exposed to air pollutants. Seasonal stratification was employed to compare the warm and cold seasons with the overall population, as shown in Figure 1. This approach aimed to evaluate the percentage change in stroke mortality risk associated with air pollution exposure. Significant effects on stroke mortality were observed in both the cold and warm seasons. This phenomenon can be attributed to Qingdao’s dry and cold winter climate, which facilitates the retention of air pollutants. Additionally, pollutant concentrations tend to be higher during this time, leading to increased pollution levels and greater exposure of residents to harmful substances[10]. Conversely, under the hot and humid conditions of summer, increased blood flow rates may cause individuals to absorb the harmful effects of pollutants more completely. This phenomenon could explain the increased risk of stroke-related mortality in Qingdao during the warm season.
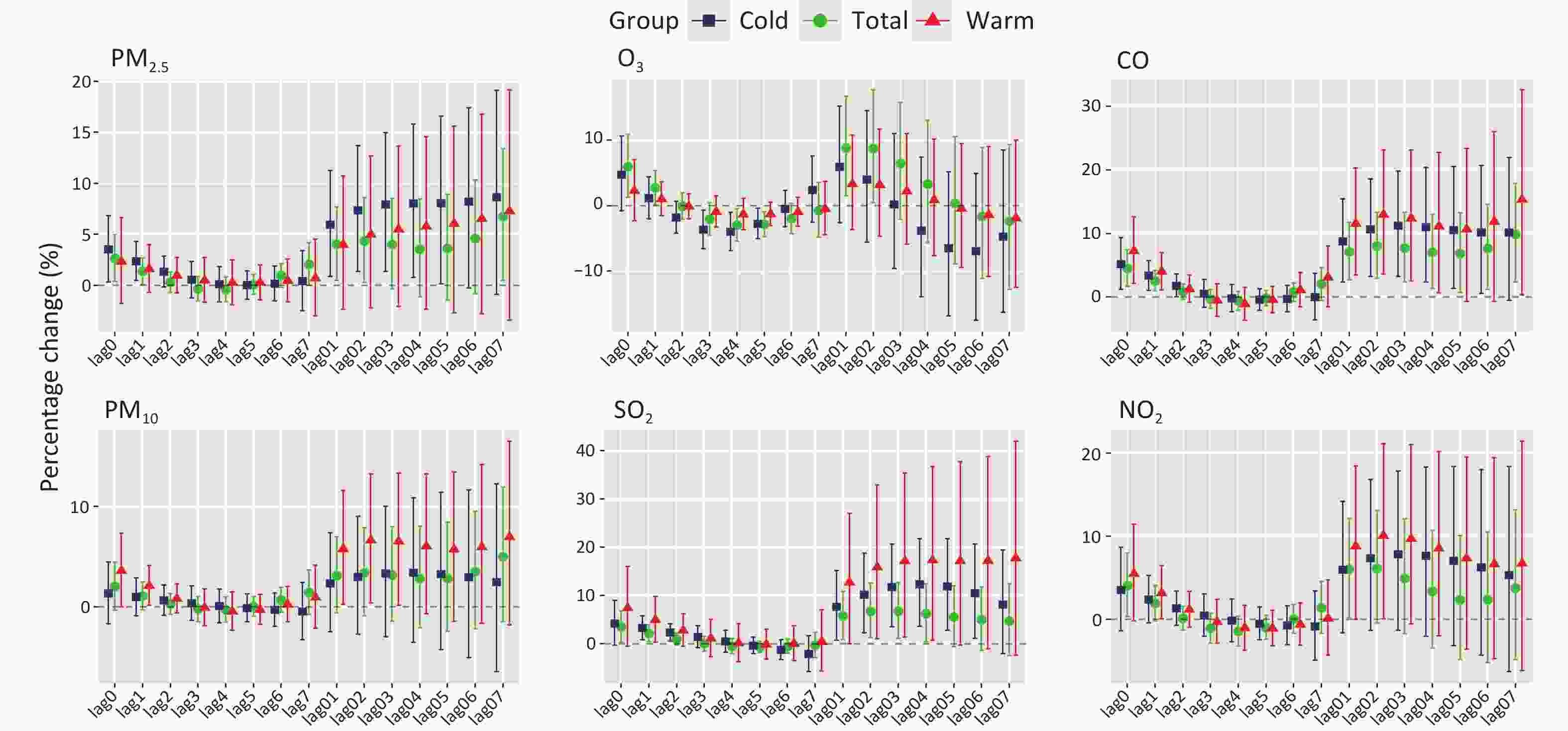
Figure 1. Percentage change (95% confidence interval) in odds of mortality from total stroke associated with an IQR increase of exposure to ambient air pollution during different seasons.
Ischemic stroke exhibited a significantly higher mortality risk and demonstrated increased vulnerability to air pollution (Supplementary Table S2). This aligns with the findings reported by Chen et al., which indicate that short-term exposure to PM2.5, PM10, O3, SO2, and NO2 affects the risk of ischemic stroke[5]. Furthermore, our study did not find a significant association between air pollutants and hemorrhagic stroke.
Supplementary Figure S1 presents an analysis of the Lag 0 lead–lag effect on gender and age subgroups based on all-cause stroke mortality data. The results indicate that women exposed to PM2.5 and CO face a higher risk of death on Lag 0, with a notable risk increase of 3.82% (95% CI: 0.46%, 7.29%) and 4.96% (95% CI: 0.77%, 9.33%). Men are more susceptible to stroke mortality when exposed to SO2 and NO2, with significant effect sizes of 6.02% (95% CI: 1.61%, 10.61%) and 9.84% (95% CI: 4.46%, 15.50%), respectively. Furthermore, the aging group (aged ≥ 75 years) shows a higher risk of stroke mortality due to exposure to PM2.5, CO, and O3, with increases of 2.87% (95% CI: 0.38%, 5.41%), 4.31% (95% CI: 1.20%, 7.51%), and 6.43% (95% CI: 1.26%, 11.85%), respectively. This suggests that older adults, particularly older women, are disproportionately affected by air pollution, resulting in a higher risk of stroke-related mortality. These findings are consistent with previous research[4]. To further explore the long-term effects, we also examined the influence of seasonal factors and their cumulative impact over time, as detailed in Supplementary Table S3 and Figure S2.
Particulate matter, such as PM2.5[4] and PM10[5], along with gaseous pollutants such as CO[6] and O3[9], have been identified as key contributors to stroke mortality in previous studies. However, the impact of seasonal variations on this relationship has not been thoroughly examined. Our study, which accounts for temperature and climatic differences between cold and warm seasons, provides a more nuanced understanding. The stratified analysis in Supplementary Table S3 shows that during the warm season, exposure to PM2.5, PM10, CO, and SO2 is associated with an increased risk of ischemic stroke mortality. The percentage increase in stroke mortality risk associated with these pollutants is 14.37% (95% CI: 2.82%, 27.21%) for PM2.5, 12.32% (95% CI: 2.91%, 22.59%) for PM10, 19.05% (95% CI: 4.46%, 35.68%) for CO, and 35.34% (95% CI: 10.41%, 65.89%) for SO2. Additionally, our findings show that ischemic stroke-related deaths are related to CO and SO2 exposure, with percentage increases of 13.22% (95% CI: 1.79%, 25.94%) and 21.39% (95% CI: 9.11%, 35.06%), respectively.
Supplementary Figure S2 gives a detailed overview of long-term trends The results from the warm season show a clear upward trend in the risk of ischemic stroke mortality associated with exposure to PM2.5, PM10, CO, and SO2. Notably, the risk of ischemic stroke death is higher during the warm season compared with the cold season. In contrast, our study found no significant correlation between air pollution exposure and the risk of hemorrhagic stroke mortality in either season. However, there is a strong link between air pollution exposure and the risk of death from ischemic stroke, which may appear to contradict previous findings. For example, Chen et al. reported that the risk of stroke-related mortality in Chongqing was mainly observed during the cold season[5]. In contrast, our seasonally adjusted analysis indicates that exposure to pollutants during the warm season poses a greater risk for stroke mortality. This discrepancy could be attributed to the hot and humid conditions prevalent in Qingdao during the warm season.
To ensure the reliability of our findings, we conducted a sensitivity analysis by developing a two-pollutant model and adjusting the df from 3 to 4–6 in the single-pollutant model. The two-pollutant model showed a slight reduction in the association between particulate matter exposure and total stroke mortality. However, no significant changes were observed in the relationship between exposure and all-cause stroke mortality (Supplementary Table S4 for details). For example, adjustments for CO on lag 0 days demonstrated minimal variation in the results. When df was set to 3, the percentage change was 4.50% (95% CI: 1.65%, 7.43%). This remained consistent at 4.50% (95% CI: 1.68%, 7.48%) with df = 4, slightly changed to 4.53% (95% CI: 1.66%, 7.47%) with df = 5, and increased to 4.65% (95% CI: 1.78%, 7.60%) with df = 6. Our analysis showed that adjusting the covariate df from 3 to 4–6 in the single-pollutant model had minimal impact on the association between air pollution and stroke mortality, which confirmed the robustness of our model (Supplementary Figure S3).
Our study has several methodological strengths. First, the use of a case-crossover design effectively minimized confounding bias from time-invariant covariates. Second, our analysis included a large sample size, which consisted of 46,263 stroke cases from Qingdao City between 2014 and 2019. This extensive dataset enhanced the statistical power of our study and improved its sensitivity to detect variations in stroke mortality risk across different subpopulations. Finally, the wide range of air pollutant concentrations observed allowed for a more precise examination of exposure–response relationships.
However, our study has some limitations. First, relying on regional average pollutant exposure levels may lead to exposure misclassification, as individual variations in exposure are not fully captured. Second, despite the advantages of the case-crossover design in reducing time-invariant confounding, our study may still be vulnerable to residual confounding from time-varying individual factors, such as changes in medication use or lifestyle. Lastly, the geographical scope of our study is limited to Qingdao City, which may restrict the generalizability of our findings to other coastal regions with different climatic conditions and population characteristics. It is important to emphasize that these limitations do not undermine our primary conclusions. The use of the case-crossover design in this study effectively addresses individual-level variables and potential biases and ensures that the observed associations between air pollution and stroke mortality risk are both robust and credible. While the external validity may be limited, the internal validity of our findings remains strong. In the future, we plan to integrate the latest stroke data from Qingdao with historical data, and subsequently gather the chemical components of PM2.5 to further investigate the factors influencing stroke mortality risk.
doi: 10.3967/bes2025.073
-
Jingkai Zhang: Formal analysis, Writing – original draft, Writing – review & editing; Bingling Wang: Data curation, Writing – review & editing; Lu Pan: Investigation, Writing – review & editing;Ge Nan: Methodology, Formal analysis, Visualization;Xiutao Gao: Data curation, Writing – review & editing; Jingya Yin: Methodology, Visualization;Yuan Fang: Investigation, Data curation; Hua Zhang: Methodology, Data curation; Jianjun Zhang: Data curation, Visualization; Yan Ma: Investigation, Data curation; Li Cheng: Methodology, Data curation; Haiping Duan: Funding acquisition, Writing – review & editing. All authors have reviewed the manuscript and approved the final version for publication.
The authors declare no competing interests in connection with the work submitted.
This study obtained ethical approval from the Ethics Review Committee of Qingdao Municipal Center for Disease Control and Prevention (No.202202). The requirement for patient consent was waived owing to the retrospective study design, and prior to analysis, all data in our study were anonymized.
注释:1) Authors’ contributions: 2) Competing Interests: 3) Ethics: -
Figure 1. Percentage change (95% confidence interval) in odds of mortality from total stroke associated with an IQR increase of exposure to ambient air pollution during different seasons.
Table 1. Characteristics of study participants in Qingdao, China (2014−2019)
Group Total HS IS Unspecified All Warm Cold All Warm Cold All Warm Cold All Warm Cold All 46263 20208 26055 18661 8284 10377 26368 11388 14980 1234 536 698 Sex Male 24947 10969 13978 10491 4685 5806 13806 6004 7802 650 − − Female 21316 9239 12077 8170 3599 4571 12562 5384 7178 584 − − Age Aging 29975 12834 17141 9897 4245 5652 19184 8212 10972 894 − − N-aging 16288 7374 8914 8764 4039 4725 7184 3176 4008 340 − − Notes. Total, Total stroke; HS, Hemorrhagic Stroke; IS, Ischemic Stroke; Unspecified is Stroke, not specifically bleeding or infarction stroke; aging, individuals aged 75 or older; N-aging, individuals younger than 75; Warm season, April to September; Cold season, October to March of the next year.  下载: 导出CSV
下载: 导出CSV
Table 2. Spearman Correlation of Air Pollutants in Qingdao, China (2014−2019)
pr temp rh wind PM2.5 PM10 O3 CO SO2 NO2 pr 1.00** temp −0.87** 1.00** rh −0.39** 0.36** 1.00** wind −0.06 −0.10** −0.14** 1.00** PM2.5 0.29** −0.38** −0.03 −0.24** 1.00** PM10 0.26** −0.34** −0.23** −0.15** 0.89** 1.00** O3 −0.58** 0.66** −0.01** −0.10** −0.15** −0.07** 1.00** CO 0.42** −0.52** −0.09** −0.27** 0.91** 0.79** −0.29** 1.00** SO2 0.48** −0.49** −0.27** −0.18** 0.61** 0.56** −0.27** 0.72** 1.00** NO2 0.40** −0.47** −0.34** −0.41** 0.75** 0.73** −0.24** 0.82** 0.66** 1.00** Notes. **P < 0.001; PM2.5, particulate matter with an aerodynamic diameter of ≤ 2.5μm; PM10, particulate matter with an aerodynamic diameter of ≤ 10μm; CO, carbon monoxide; O3, ozone; SO2, sulfur dioxide; NO2, nitrogen dioxide; pr, daily mean pressure; temp, mean temperature; rh, relative humidity; wind, wind speed.
下载: 导出CSV
-
[1] GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet, 2020; 396, 1204−22. doi: 10.1016/S0140-6736(20)30925-9 [2] Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 study. J Am Coll Cardiol, 2020; 76, 2982−3021. doi: 10.1016/j.jacc.2020.11.010 [3] GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet, 2020; 396, 1223−49. doi: 10.1016/S0140-6736(20)30752-2 [4] Ban J, Wang Q, Ma RM, et al. Associations between short-term exposure to PM2.5 and stroke incidence and mortality in China: a case-crossover study and estimation of the burden. Environ Pollut, 2021; 268, 115743. doi: 10.1016/j.envpol.2020.115743 [5] Chen H, Cheng Z, Li MM, et al. Ambient air pollution and hospitalizations for ischemic stroke: a time series analysis using a distributed lag nonlinear model in Chongqing, China. Front Public Health, 2021; 9, 762597. [6] Liu C, Yin P, Chen RJ, et al. Ambient carbon monoxide and cardiovascular mortality: a nationwide time-series analysis in 272 cities in China. Lancet Planet Health, 2018; 2, e12−8. doi: 10.1016/S2542-5196(17)30181-X [7] Wang LJ, Liu C, Meng X, et al. Associations between short-term exposure to ambient sulfur dioxide and increased cause-specific mortality in 272 Chinese cities. Environ Int, 2018; 117, 33−9. doi: 10.1016/j.envint.2018.04.019 [8] Chen ZS, Wang B, Hu YL, et al. Short-term effects of low-level ambient air NO2 on the risk of incident stroke in Enshi City, China. Int J Environ Res Public Health, 2022; 19, 6683. doi: 10.3390/ijerph19116683 [9] Xue T, Guan TJ, Liu YL, et al. A national case-crossover study on ambient ozone pollution and first-ever stroke among Chinese adults: interpreting a weak association via differential susceptibility. Sci Total Environ, 2019; 654, 135−43. doi: 10.1016/j.scitotenv.2018.11.067 [10] Gao Y, Shan HY, Zhang SQ, et al. Characteristics and sources of PM2.5 with focus on two severe pollution events in a coastal city of Qingdao, China. Chemosphere, 2020; 247, 125861. doi: 10.1016/j.chemosphere.2020.125861 -

 点击查看大图
点击查看大图
图(1) / 表ll (2)
计量
- 文章访问数: 15
- HTML全文浏览量: 5
- PDF下载量: 0
- 被引次数: 0

 Quick Links
Quick Links