


-
Cardiovascular diseases (CVDs), the leading cause of global mortality and disability, play a crucial role in premature death as well as excessive increases in medical costs, and are becoming one of the largest public health challenges[1]. The burden caused by stroke, a major CVD, has risen steadily since 1990, with a prevalence reaching 101 million cases in 2019[2]. Atrial fibrillation, the most common arrhythmia, has also been estimated to increase over the next 30 years[3]. Current efforts focus on the identification and management of risk factors and etiology to reduce further effects of CVDs.
C-reactive protein (CRP), a clinical marker of systemic inflammation, increases in response to injury, systemic inflammation and other inflammatory stimuli[4]. CRP induces proinflammatory responses and the progression of cardiovascular events[5-8]. In addition, elevated CRP is correlated with an increased risk of other risk factors of CVDs, such as age, sex, metabolic syndrome and dyslipidemia[9-11]. Nevertheless, most relevant studies have been traditional observational studies, thus hindering determination of the causal relationship between CRP and CVDs, owing to possible confounding factors and reverse causation bias.
The Mendelian randomization (MR) method uses genetic variation as instrumental variables (IVs), which assort randomly during gamete formation; thus, MR can effectively avoid the potential bias in traditional epidemiological methods. Therefore, the MR approach is commonly used to make causal inferences from GWAS data[12]. Previous studies have found no evidence of association of CRP levels with CVD risk via MR; however, most of those studies were conducted in European populations[13-15]. The evidence of an association of CRP level with CVD risk in East Asian populations is limited, and sample sizes have also been limited in prior studies[16,17]. Hence, our study used a two-sample MR method to explore the association between CRP and CVDS in a large sample of the Japanese population.
-
Summary statistics of outcomes were obtained from the Japanese Encyclopedia of Genetic association by Riken (JENGER,
http://jenger.riken.jp/en/ ). On the basis of the data available, we selected four CVDs for our study: atrial fibrillation (8,180 cases and 28,612 controls)[18], arrhythmia (17,861 cases and 194,592 controls)[19], ischemic stroke (17,671 cases and 192,383 controls)[19] and congestive heart failure (9,413 cases and 203,040 controls)[19]. The former study evaluated a total of 5,018,049 single-nucleotide polymorphisms (SNPs)[18], whereas the latter tested 8,712,794 autosomal variants and 207,198 X chromosome variants[19]. The case samples in the GWAS studies were collected from the BioBank Japan Project (BBJ), whereas the control samples were from population-based prospective cohorts. The included studies were all approved by relevant ethics committees and obtained participants’ informed consent. -
From the JENGER site, SNPs associated with CRP were used as IVs, which were selected from another GWAS study of 75,391 Japanese participants[20]. The MR analysis was based on the following three assumptions for IVs: 1) the genotype is associated with the exposure; 2) the genotype is not associated with confounding factors that bias the associations between the exposure and outcome; 3) the genotype is associated with the outcome only via its association with the exposure. To meet the requirements of IVs, only SNPs with genome-wide significance (P < 5 × 10−8) were screened out (thus alleviating concerns about violation of assumption 1). Through use of the 1,000 Genomes East Asian ancestry reference panel, linkage disequilibrium was clumped (distance threshold = 10,000 kb; r2 = 0.001) to ensure the independence of SNPs (thus, alleviating concerns about violation of assumption 3). The Cragg–Donald F-statistic was then obtained by using the formula
$F=\dfrac{{R}^{2}}{1-{R}^{2}}\times \dfrac{N-K-1}{K}$ , where K represents the number of IVs[21]. The bias caused by weak instrumental variables was controlled according to the rule of thumb that F < 10 is regarded as a weak instrumental variable[22]. Because of its low minor allele frequency (MAF = 6.44%), rs151233628 was excluded from further study, as was rs814295, which has been shown to be associated with a potential confounder (fasting plasma glucose, P = 0.002) in an East Asian population[23]. Finally, four SNPs were selected as the IVs in our study (Table 1).SNP Chr Positional candidate gene(s) EA OA Beta (SE) P N MAF R2 (%) F rs3093068 1 CRP C G 0.127 (0.007) < 0.001 75,391 0.137 0.384 72.560 rs79802086 7 LOC401312, LOC541472 C T 0.060 (0.007) < 0.001 75,391 0.161 0.098 18.402 rs1169284 12 HNF1A C T −0.058 (0.005) < 0.001 75,391 0.471 0.166 31.278 rs429358 19 APOE C T −0.109 (0.009) < 0.001 75,391 0.104 0.220 41.481 Note. Beta is the estimated effect size. CRP, C-reactive protein; SNP, single-nucleotide polymorphism; Chr, chromosome; EA, effect allele; OA, other allele; SE, standard error of effect size; N, sample size; MAF, minor allele frequency; R2, proportion of variance in C-reactive protein explained by SNP; F, Cragg–Donald F-statistics. Table 1. SNPs associated with CRP
Because some participants in both the exposure and outcome group were from BBJ, sample overlap might have biased MR analysis. As described in previous studies[24,25], the large sample size and small population of case group in this study should alleviate concerns regarding sample overlap bias. In addition, we evaluated the potential bias in a quantitative manner by using the online computing tool (
https://sb452.shinyapps.io/overla p) provided by Burgess et al.[24]. Given that${R}^{2}=0.8{\text{%}}$ , overlap proportion = 0.5 (which is sufficiently conservative), expected F statistic value as well as its lower limit of the one-sided 95% confidence interval > 30, and type I error controlled at 0.05, weak instrument bias caused by sample overlap would not be expected (Supplementary Table S1, available in www.besjournal.com).Outcome Observational estimate Sample size Proportion of cases Overlap proportion Type 1 error rate Bias Ischemic stroke 1.46a 210,054 0.084 0.5 0.050 0.011 Arrhythmia 2.02b 212,453 0.084 0.5 0.050 0.015 Atrial fibrillation 2.02b 36,792 0.222 0.5 0.050 0.015 Congestive heart failure 2.64c 212,453 0.044 0.5 0.050 0.020 Note. aRefer to Zhou Y, Han W, Gong D, et al. Hs-CRP in stroke: A meta-analysis. Clin Chim Acta, 2016; 453, 21–7. bRefer to Kwon CH, Kang JG, Lee HJ, et al. C-reactive protein and risk of atrial fibrillation in East Asians. Europace, 2017; 19, 1643–9. cRefer to Kardys I, Knetsch AM, Bleumink GS, et al. C-reactive protein and risk of heart failure. The Rotterdam Study. American Heart Journal, 2006; 152, 514–20. Table S1. Assessment of bias due to sample overlap
-
Detailed information can be found in the original GWAS studies, including genotyping, imputation and other methods[18-20]. In brief, samples were genotyped with Illumina HumanOmniExpressExome BeadChips, or a combination of Illumina HumanOmniExpress and HumanExome BeadChips. For quality control, these studies excluded samples with: (i) a sample call rate less than 0.98, (ii) closely related individuals identified by identity-by-descent analysis and (iii) outliers from East Asian clusters identified by principal component analysis by using the genotyped samples and the three major reference populations (Africans, Europeans and East Asians) in the International HapMap Project. In quality-control of genotypes, variants meeting the following criteria were excluded: (i) call rate < 99% and (ii) P value for Hardy Weinberg equilibrium < 1.0 × 10−6.
-
In the main analyses, we combined MR estimates for each direction of potential influence by using IVW meta-analysis, a weighted regression of SNP-outcome effects on SNP-exposure effects (the intercept was constrained to 0). IVW, on the basis of traditional MR assumptions, has strict requirements on instrumental variables and is often regarded as a conventional MR method[26]. In addition, we performed other MR methods including the weighted median (WM), penalized weighted median (PWM) and MR-Egger regression, which are relatively robust to horizontal pleiotropy and invalid instruments. These methods are widely used in MR studies to ensure the accuracy of the results[27]. MR-Egger can be used to correct for bias due to directional pleiotropy under a weaker set of assumptions[28]. WM can provide consistent estimates when some IVs in the analysis are not valid. For sensitivity analyses, MR-Egger was used for assessing directional pleiotropy, and leave-one-out analysis was also performed to test the influence of outliers by removing SNPs individually. Cochran’s Q test was used to evaluate heterogeneity.
Statistical tests were all two-tailed. Because of the multiple tests performed in one data set, the Bonferroni-corrected threshold P < 0.0125 (α = 0.05/4 outcomes) was used in our study, whereas associations with P-value between 0.0125 and 0.05 were regarded as suggestive evidence requiring further confirmation.
-
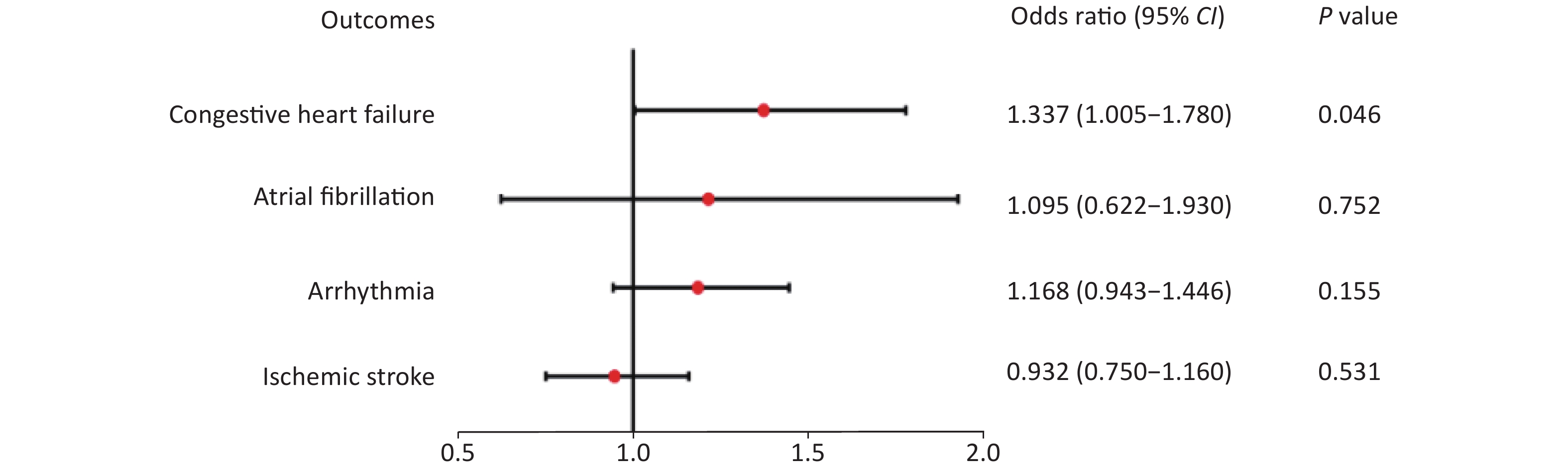
The IVW results of associations between CRP and the risk of four CVDs are shown in Figure 1. In the IVW analysis, genetically predicted CRP levels were not observed to be associated with the risk of ischemic stroke [OR (odds ratio): 0.932, 95% CI (95% confidence interval): 0.750–1.160, P = 0.531], atrial fibrillation (OR: 1.095, 95% CI: 0.622–1.930), P = 0.752) and arrhythmia (OR: 1.168, 95% CI: 0.943–1.446, P = 0.155). The results of the weighted median, penalized weighted median and MR-Egger regression methods were robust (all P values > 0.05). IVW indicated suggestive evidence of an association between CRP and congestive heart failure (OR: 1.337, 95% CI: 1.005–1.780, P = 0.046). However, this result was not consistent in complementary analyses using other MR methods (P > 0.05, Table 2).
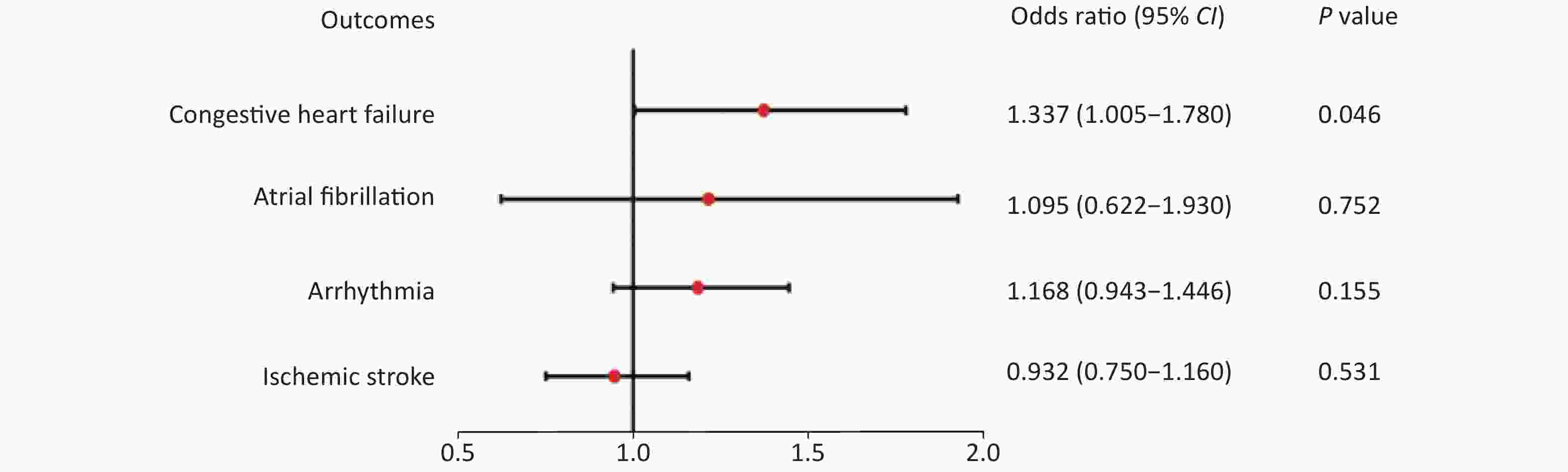
Figure 1. Causal effect estimates of CRP with four cardiovascular outcomes from IVW analysis. Estimates are derived from IVW analysis and are represented as odds ratios (95% CI). A two-sided P value < 0.0125 was considered statistically significant. IVW, inverse-variance weighted; CI, confidence interval.
Outcome Method SNP (N) OR (95% CI) Beta (SE) P Ischemic stroke WM 4 0.936 (0.733–1.194) −0.066 (0.125) 0.594 PWM 4 0.936 (0.736–1.189) −0.066 (0.122) 0.587 MR-Egger 4 1.030 (0.532–1.991) 0.029 (0.336) 0.939 Atrial fibrillation WM 4 1.044 (0.643–1.695) 0.043 (0.247) 0.862 PWM 4 1.044 (0.643–1.683) 0.043 (0.244) 0.860 MR-Egger 4 2.133 (0.336–13.539) 0.758 (0.942) 0.506 Arrhythmia WM 4 1.112 (0.860–1.437) 0.106 (0.131) 0.416 PWM 4 1.112 (0.867–1.427) 0.106 (0.127) 0.403 MR-Egger 4 0.910 (0.479–1.730) −0.094 (0.328) 0.801 Congestive heart failure WM 4 1.299 (0.917–1.839) 0.261 (0.177) 0.140 PWM 4 1.299 (0.934–1.806) 0.261 (0.168) 0.120 MR-Egger 4 0.961 (0.405–2.282) −0.039 (0.441) 0.937 Note. Beta is the estimated effect size. CRP, C-reactive protein; CVDs, Cardiovascular diseases; SNP, single-nucleotide polymorphism; OR, odds ratio; CI, confidence intervals; SE, standard error; WM, weighted median method; PWM, penalized weighted median method; MR-Egger, Egger regression method; MR, Mendelian randomization. Table 2. Other MR method results for CRP on four cardiovascular outcomes
No heterogeneity or evidence of directional pleiotropy was observed, because the P values of MR-Egger intercepts and Cochran’s Q were all greater than 0.05 (Supplementary Table S2, available in www.besjournal.com). Furthermore, the results of leave-one-out sensitivity analysis showed that the associations for ischemic stroke, atrial fibrillation, arrhythmia were not substantially driven by any individual SNP (Supplementary Figures S1–S4, available in www.besjournal.com).
Outcome SNP (N) Intercept Pa Cochran’s Q Q_df Pb Ischemic stroke 4 −0.006 0.785 0.104 3 0.991 Atrial fibrillation 4 −0.044 0.532 6.064 3 0.109 Arrhythmia 4 0.016 0.505 1.924 3 0.588 Congestive heart failure 4 0.022 0.511 1.672 3 0.643 Note. Pa is the value of P for MR-Egger intercept. Pb is the value of P for heterogeneity tests by performing inverse-variance weighted method. CRP, C-reactive protein; CVDs, Cardiovascular diseases; SNP, single-nucleotide polymorphism; MR, Mendelian randomization. Table S2. MR-Egger intercepts and heterogeneity tests of CRP causally linked to four cardiovascular outcomes
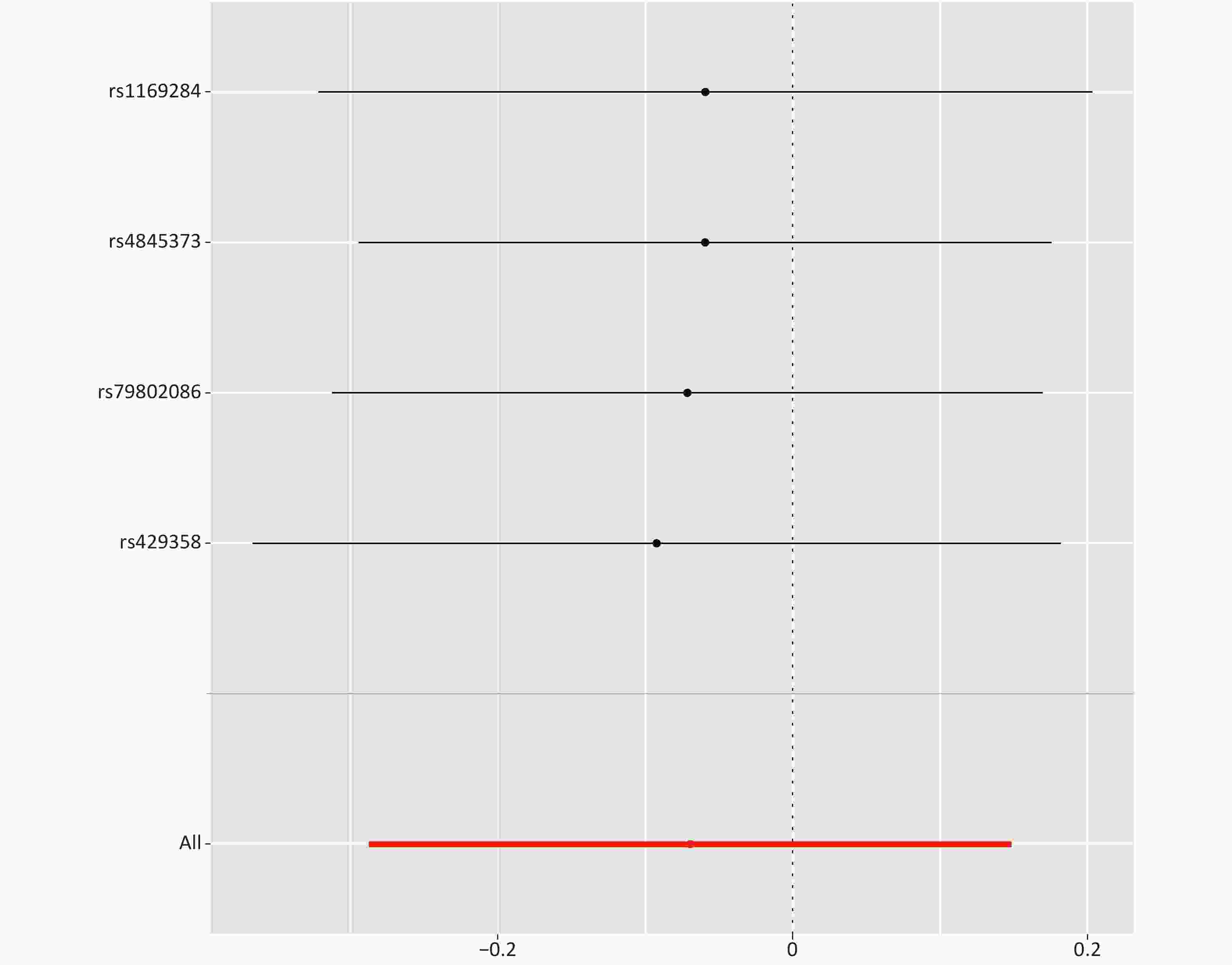
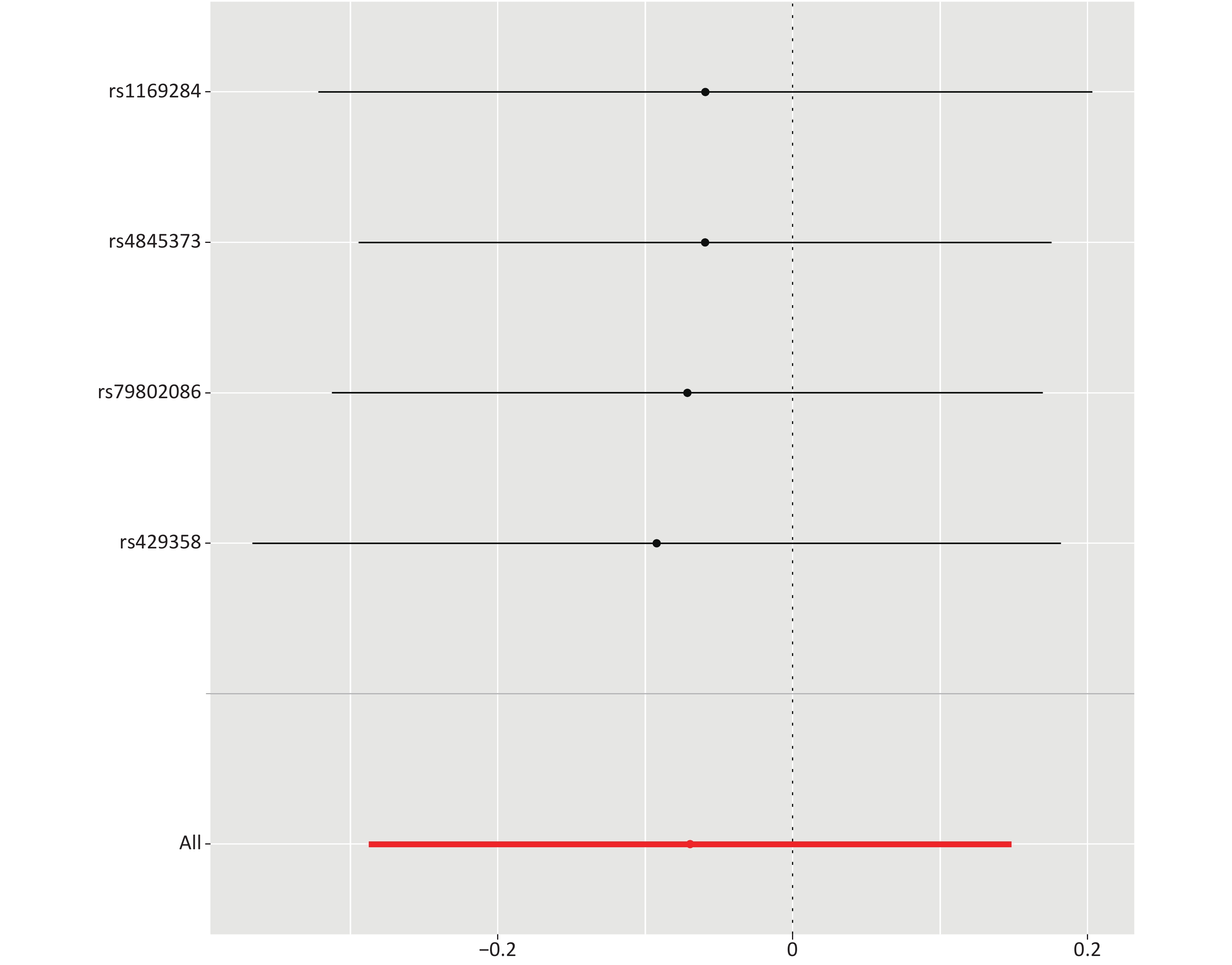
Figure S1. MR leave-one-out sensitivity analysis of the effect of C-reactive protein on ischemic stroke. Leave-one-out analysis: each row represents an MR analysis of the effect of CRP on ischemic stroke, using all instruments except for the SNP associated with CRP listed on the y-axis. The point represents the beta with that SNP removed, and the line represents the 95% confidence interval
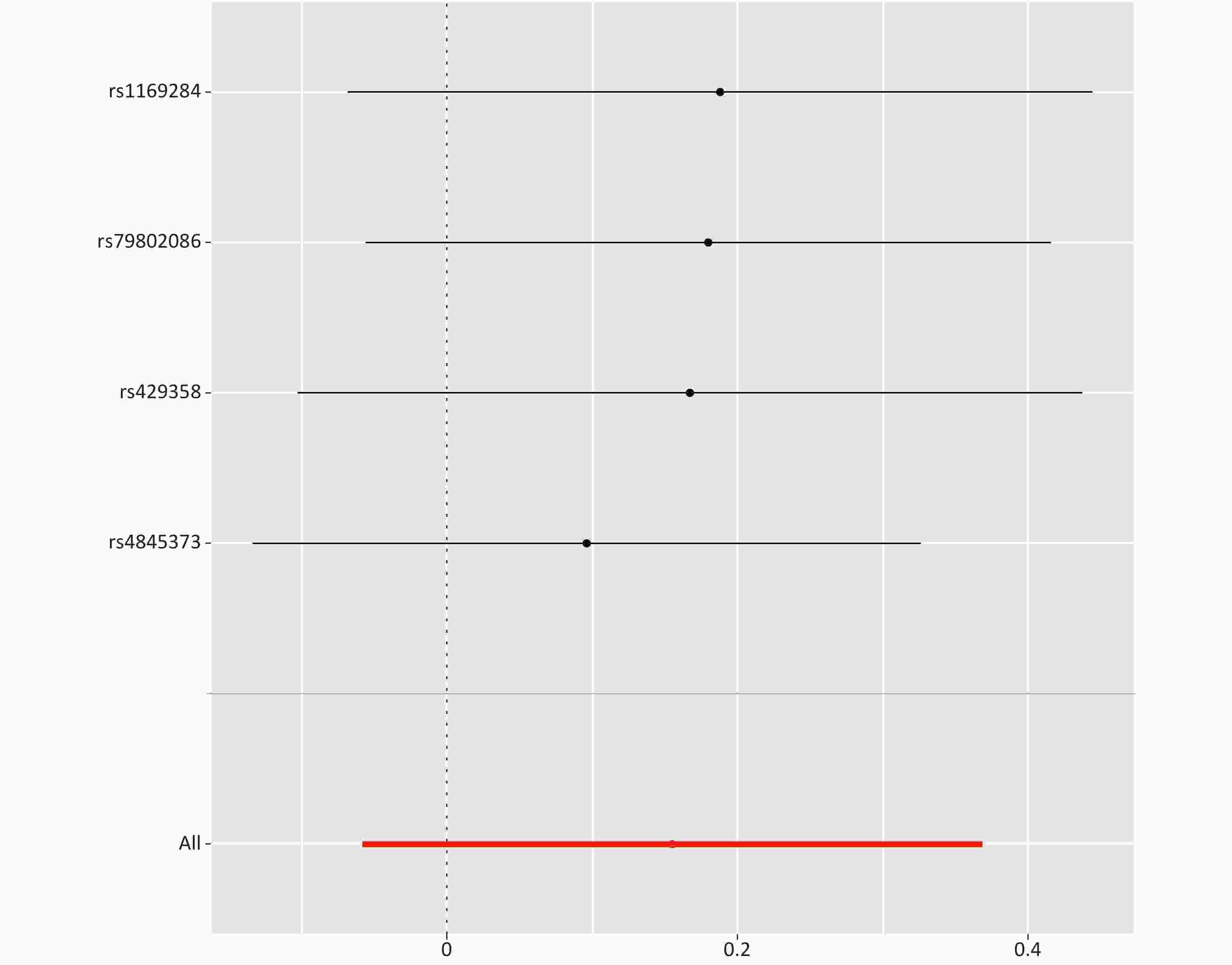
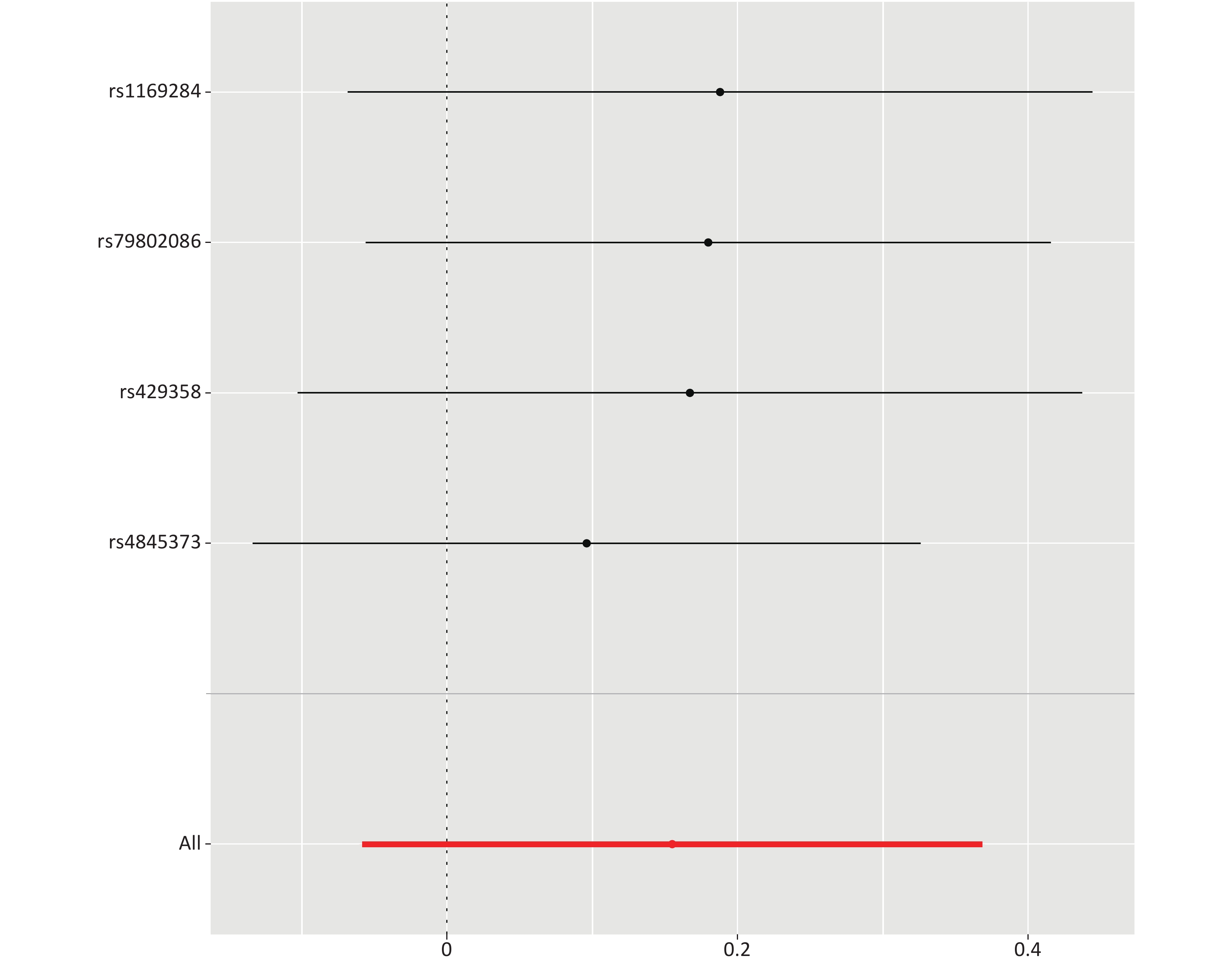
Figure S2. MR leave-one-out sensitivity analysis of the effect of C-reactive protein on arrhythmia. Leave-one-out analysis: each row represents an MR analysis of the effect of CRP on arrhythmia, using all instruments except for the SNP associated with CRP listed on the y-axis. The point represents the beta with that SNP removed, and the line represents the 95% confidence interval
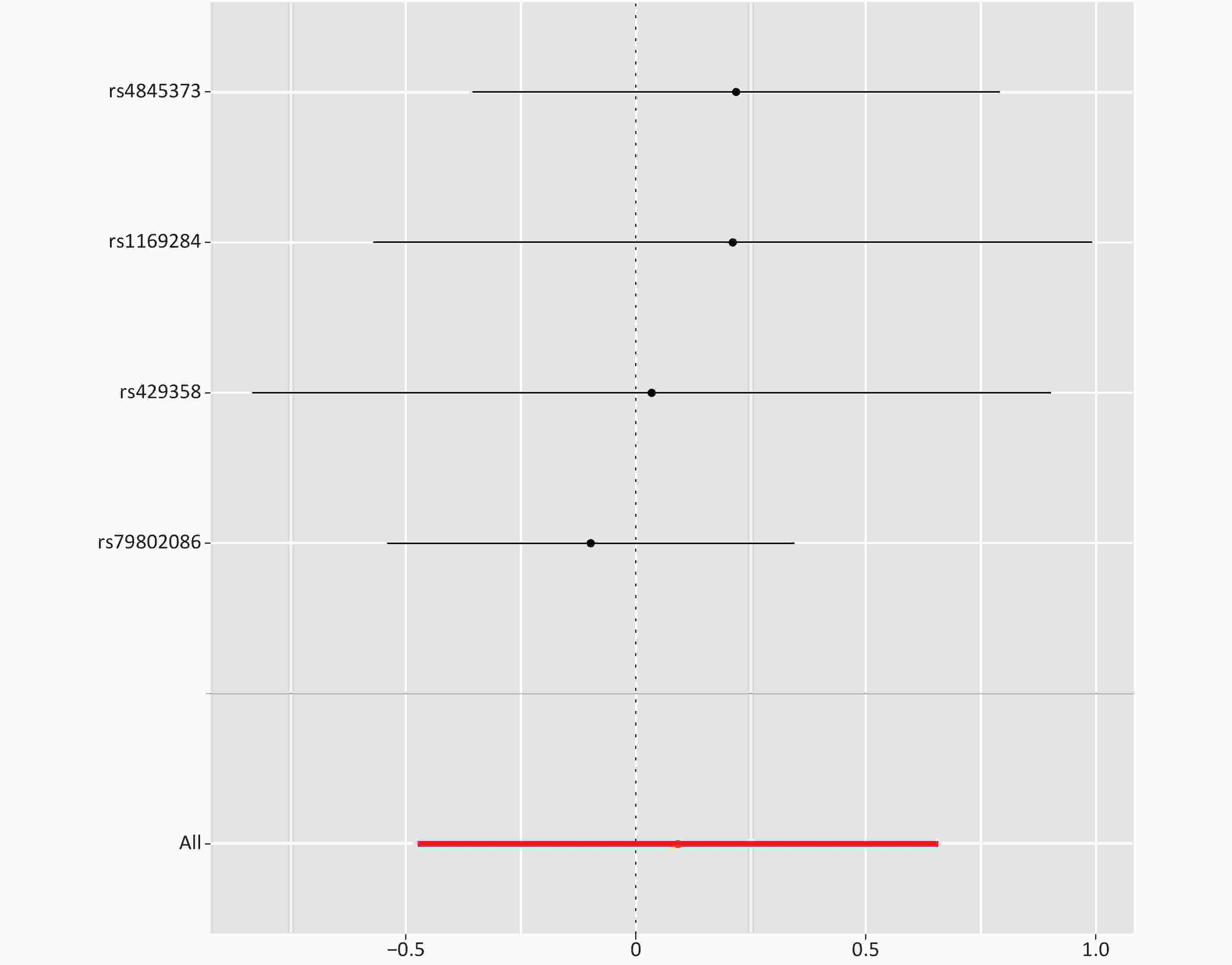
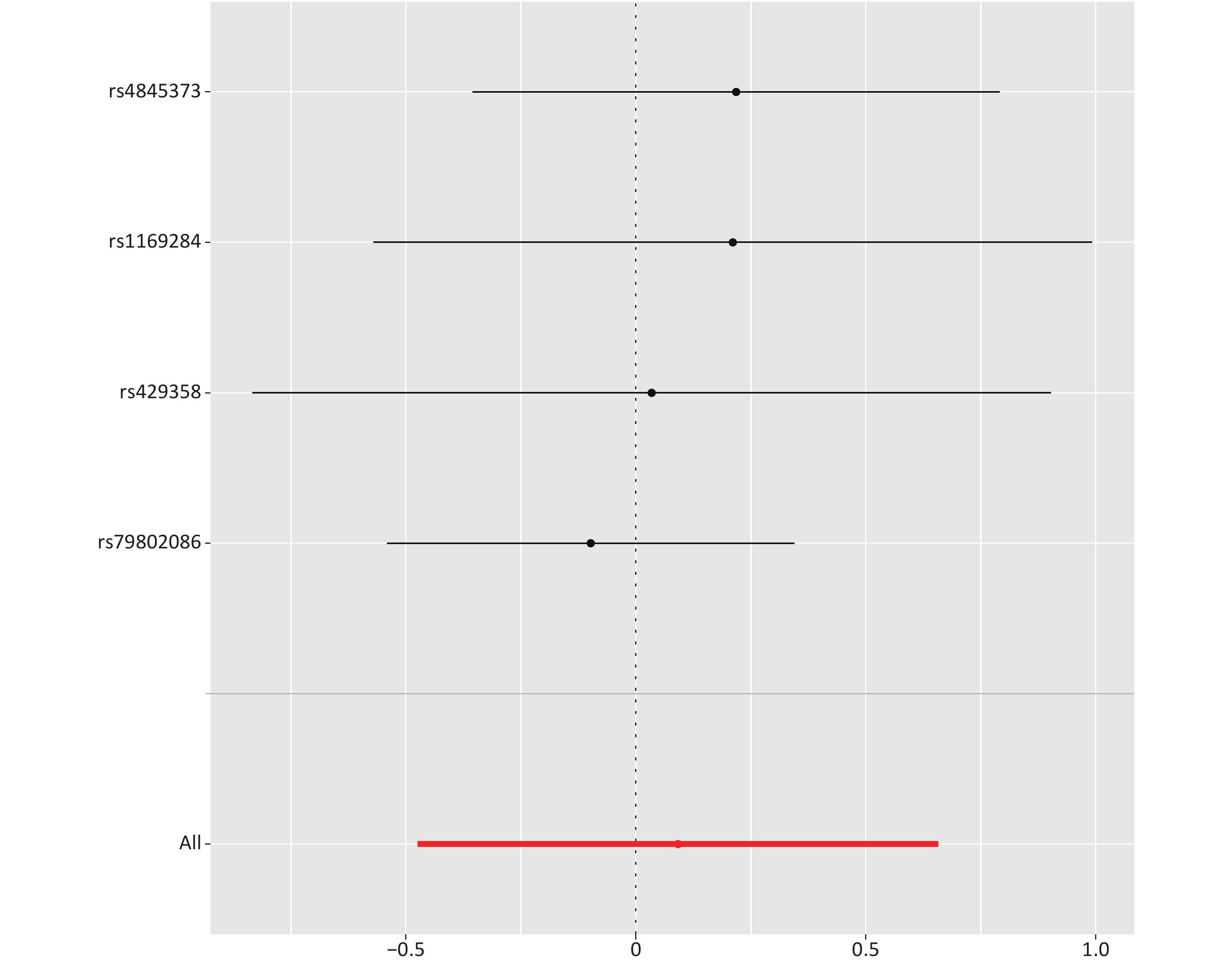
Figure S3. MR leave-one-out sensitivity analysis of the effect of C-reactive protein on atrial fibrillation. Leave-one-out analysis: each row represents an MR analysis of the effect of CRP on atrial fibrillation, using all instruments except for the SNP associated with CRP listed on the y-axis. The point represents the beta with that SNP removed, and the line represents the 95% confidence interval
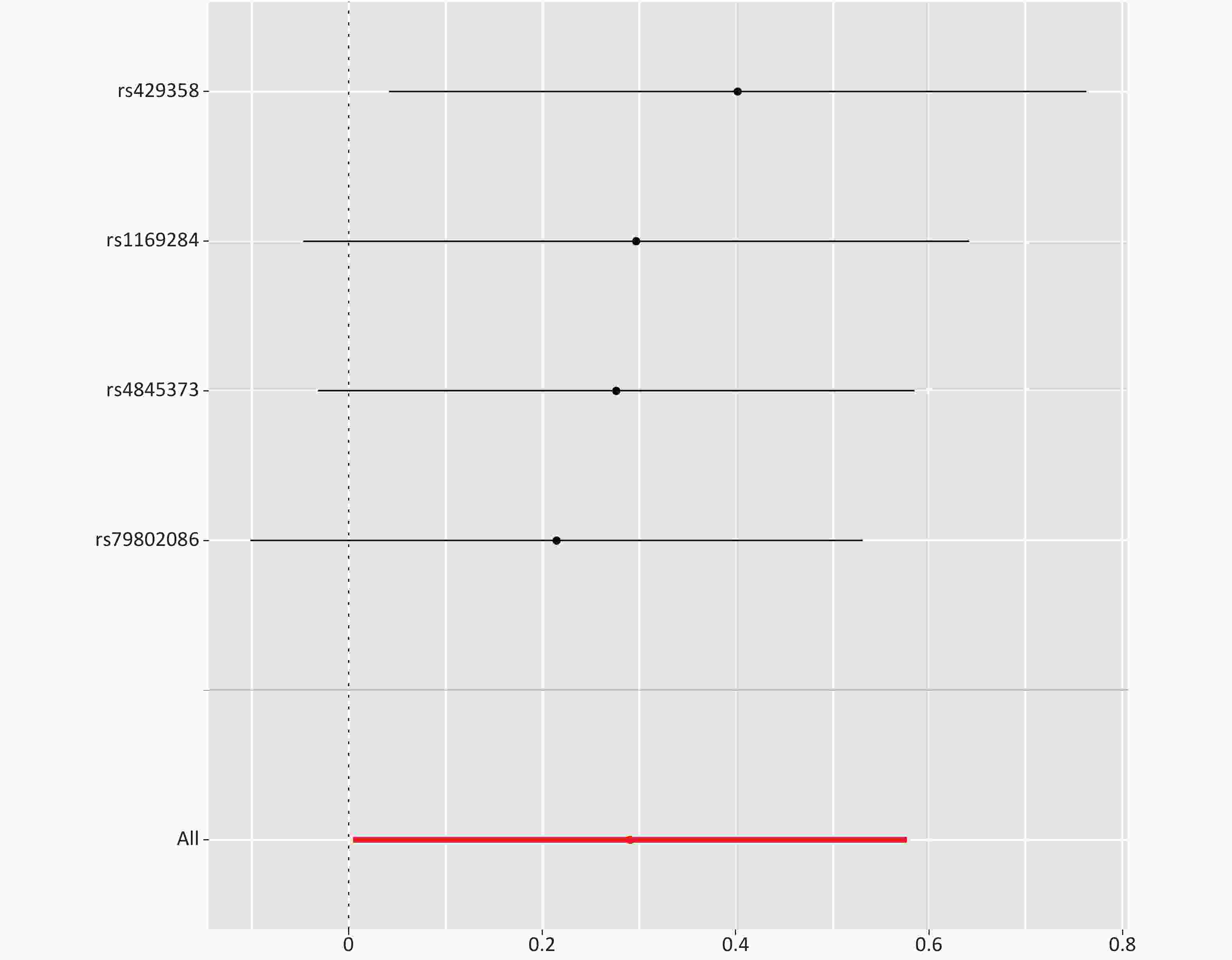
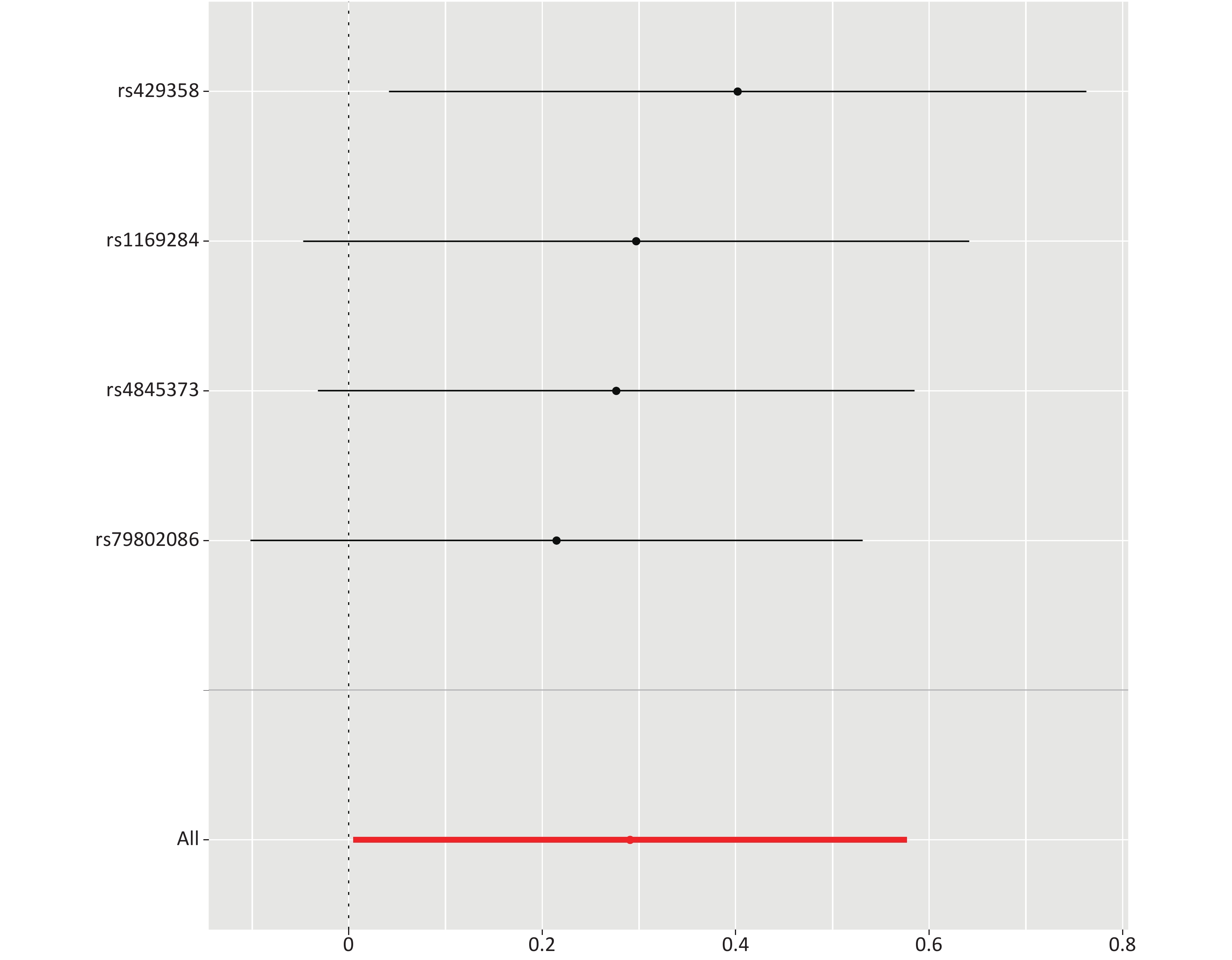
Figure S4. MR leave-one-out sensitivity analysis of the effect of C-reactive protein on congestive heart failure. Leave-one-out analysis: each row represents an MR analysis of the effect of CRP on congestive heart failure, using all instruments except for the SNP associated with CRP listed on the y-axis. The point represents the beta with that SNP removed, and the line represents the 95% confidence interval
In addition, given α = 0.0125, the statistical power of each test was greater than 0.9, according to the online computing platform[29], thus, indicating that type II error was unlikely.
-
In this present study, two-sample MR analysis was performed on public data from a large sample of the Japanese population to assess the causal associations between CRP and four CVDs. A study aim was to address the limitations of confounding and reverse causality in observational studies. Our findings indicated suggestive evidence of a positive association between CRP and congestive heart failure, whereas no associations of CRP with ischemic stroke, atrial fibrillation or arrhythmia were observed. Sensitivity analyses were performed to ensure the accuracy of the results.
Notably, for heart failure, our study revealed suggestive evidence of a causal relationship with CRP. To our knowledge, this is the first exploration of the relationship between CRP and heart failure by MR methods in East Asians. Previous studies have found that CRP is associated not only with the incidence of heart failure in both healthy people[30,31] and patients with other CVDs[32], but also with disease progression[33]. Beyond ventricular remodeling, CRP induces endothelial dysfunction by decreasing nitric oxide and prostacyclin in aortic endothelial cells[34]; this dysfunction is also associated with the pathogenesis of heart failure. Although traditional epidemiological studies have found an association between CRP and the risk of heart failure, this result has not been supported by MR studies. A recent umbrella review has found that most meta-analyses of observational studies have reported a nominally statistically significant result, but substantial evidence of a causal association between CRP and health-related outcomes, including CVDs, has not been observed for any phenotype in MR studies[35]. Therefore, a variety of biases may exist in traditional epidemiological studies, thus leading to the exaggeration of associations. Although our study provides suggestive evidence of a causal association between CRP and heart failure, conclusions regarding its causality should be made as conservatively as possible, because the P value was close to 0.05.
The results of most traditional epidemiological studies have indicated a positive association between CRP and ischemic stroke[36,37]. According to previous research, CRP is believed to contribute to plaque instability through its action on endothelial cells and to cause thrombosis[38]. Thus, CRP is regarded to have an important role in the progression of atherosclerosis, which is closely associated with the incidence of ischemic stroke. However, previous MR studies as well as our study have found no association between CRP and stroke in either European[39,40] or East Asian[17] populations. One possible reason for this inconsistency might be the influence of other confounding factors. For example, previous studies have shown that the association between CRP and ischemic stroke is affected by its relationship with IL-6[41,42]. In addition, elevated inflammatory markers may reflect a high burden of atherosclerosis, or perhaps a highly active form of atherosclerosis[43], thus resulting in false positive results in traditional epidemiological studies, owing to reverse causality. Further studies must combine multiple inflammatory biomarkers to predict ischemic events and evaluate clinical anti-inflammatory interventions.
Atrial fibrillation, the most common sustained arrhythmia, not only increases the burden of disease globally but also is associated with CVDs including stroke and heart failure[44]. Animal experiments and traditional epidemiological studies have suggested that inflammation is involved in structural remodeling, such as the positive relationship between CRP and left atrial diameter[45,46]; moreover, inflammation may increase the inhomogeneity of atrial conduction, which is associated with electrical remodeling[47]. Both types of remodeling are associated with the risk of atrial fibrillation[48]. Prospective cohort studies have found an association between serum high-sensitivity CRP and atrial fibrillation[14,49,50], thereby apparently reinforcing the hypothesis of a cause-and-effect relationship. However, this hypothesis is not supported by an MR study on European populations[14], and the same is true of the results of our study obtained on an East Asian population. Interestingly, another MR study exploring the association between inflammatory markers and atrial fibrillation has yielded a different result, in which genetically predicted circulating IL-6 levels were significantly inversely associated with atrial fibrillation (P = 1.34 × 10−7)[51]. Considering the association between IL-6 and the regulation of CRP, the positive association between CRP and atrial fibrillation in traditional epidemiological studies has been speculated to be caused by IL-6 or other markers, although this possibility remains to be verified in further research.
Our study has several limitations. First, the bias of weak instrumental variables could not be completely excluded. All SNPs included in the study accounted for a low proportion of CRP variation (total
${R}^{2}=0.868{\text{%}}$ ), although the selected genetic variants are strongly associated with exposure. Furthermore, because data on subtypes of disease outcomes were unavailable, we were unable to include more types of CVDs or to further define the disease types. In addition, although our study controlled for possible effects of pleiotropic bias to the maximum extent, such bias, particularly that caused by polymorphisms, could not be completely excluded. Although the potential effect of sample overlap was excluded, the suggestive evidence of congestive heart failure should be validated in large populations in other East Asian countries to ensure the generalizability of the results.Our study based on a large East Asian population examined the causal association between CRP and four CVD outcomes—ischemic stroke, atrial fibrillation, arrhythmia and congestive heart failure—by using two-sample MR methods. Our results indicated suggestive evidence of a causal role of CRP in congestive heart failure, but this role must be verified in further studies. We found no or limited evidence that CRP causally affects the risk of ischemic stroke, atrial fibrillation or arrhythmia.
HTML
Outcome Data Source
Exposure Data Source and Selection of Instrumental Variables


Genotyping and Quality Control
Statistical Analysis

 21264Supplementary Materials.pdf
21264Supplementary Materials.pdf
|

|

 Quick Links
Quick Links
 DownLoad:
DownLoad: