


-
The continuing emergence and spread of drug-resistant Mycobacterium tuberculosis complex (MTBC) poses a challenge to global tuberculosis (TB) control programs. Drug resistance in TB is mainly conferred by specific point mutations in the MTBC genome[1]. Multidrug-resistant TB (MDR-TB), which is caused by MTBC strains with resistance to both isoniazid and rifampicin (RIF), the most important first-line medicines, poses the main threat to TB control and elimination. Fluoroquinolones (FQs) and second-line injectable drugs (SLIDs) are core compounds in current MDR-TB treatment regimens[2]; however, data on the prevalence of resistance to FQs and SLIDs among MTBC strains has been lacking. The rapidly increasing number of DR-TB cases further underscores the need for more intensive surveillance of susceptibility to these important second-line drugs, to minimize further increases in the number of cases of preXDR-TB (MDR-TB with additional resistance to any FQ drug or at least one of the three SLIDs) and XDR-TB (MDR-TB with resistance to both FQs and SLIDs).
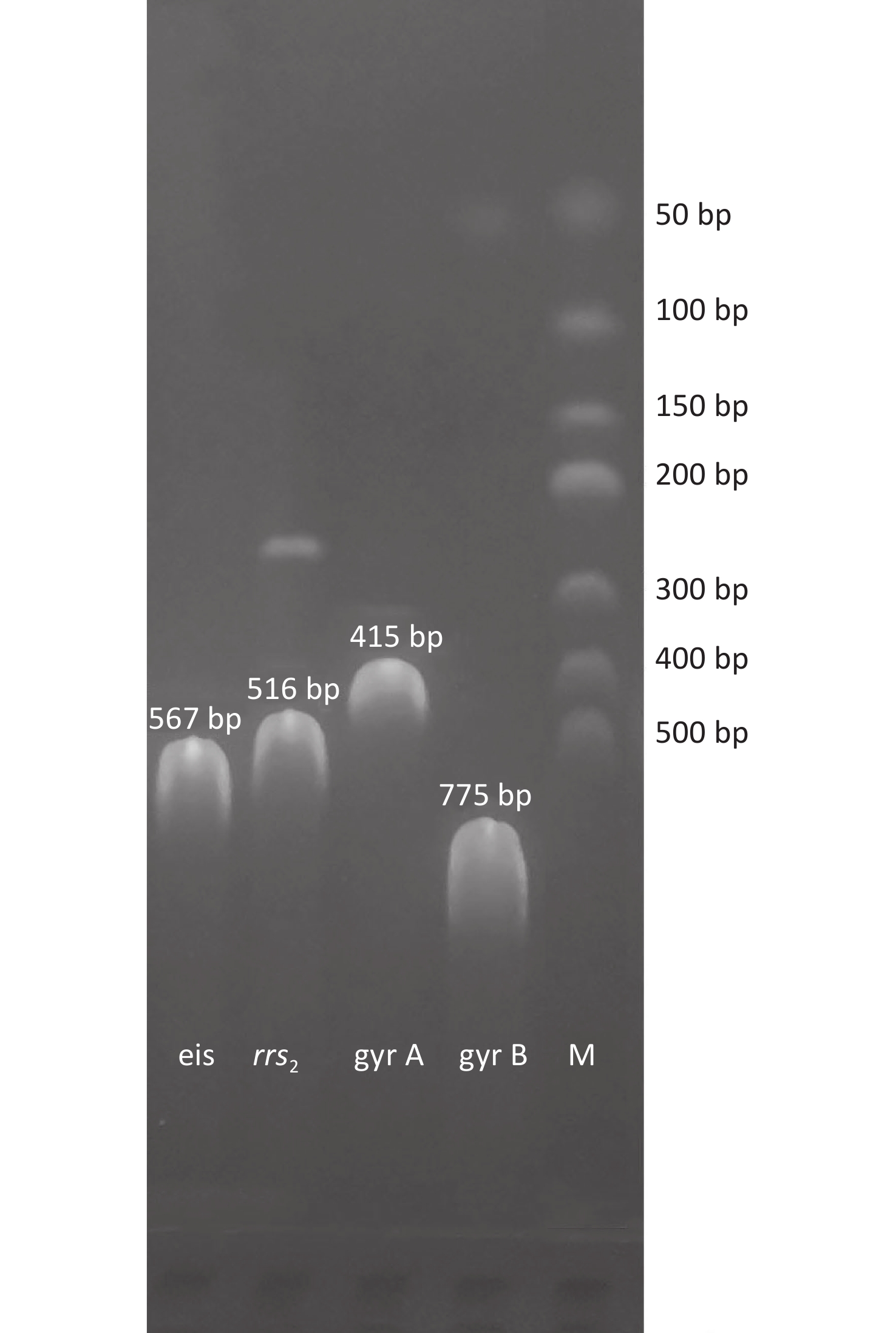
Therefore, in the present study, we investigated the ofloxacin (OFX) and kanamycin (KM) resistance in MDR and non-MDR TB isolates collected from clinical sputum specimens in northwest Zhejiang, China—a rural area with approximately 5,140,000 inhabitants. Mycobacteria were isolated from sputum specimens collected from patients with suspected TB. Sputum smears and GeneXpert MTB/RIF tests were performed simultaneously. Species identification was performed with p-nitrobenzoic acid, and phenotypic drug susceptibility testing to determine the susceptible proportions was performed on Lowenstein–Jensen medium according to the national guidelines[3]. Genomic DNA of inactivated MTBC strains (resistant to OFX or KM) was extracted with a DNA extraction kit (Invitrogen Thermo Fisher Scientific, Waltham, MA, USA). Fragments of the gyrA, gyrB, rrs2, and eis genes were amplified (Supplementary Figure S1, available in www.besjournal.com), and sequencing was performed to identify point mutations in the selected resistant strains as previously reported[4].
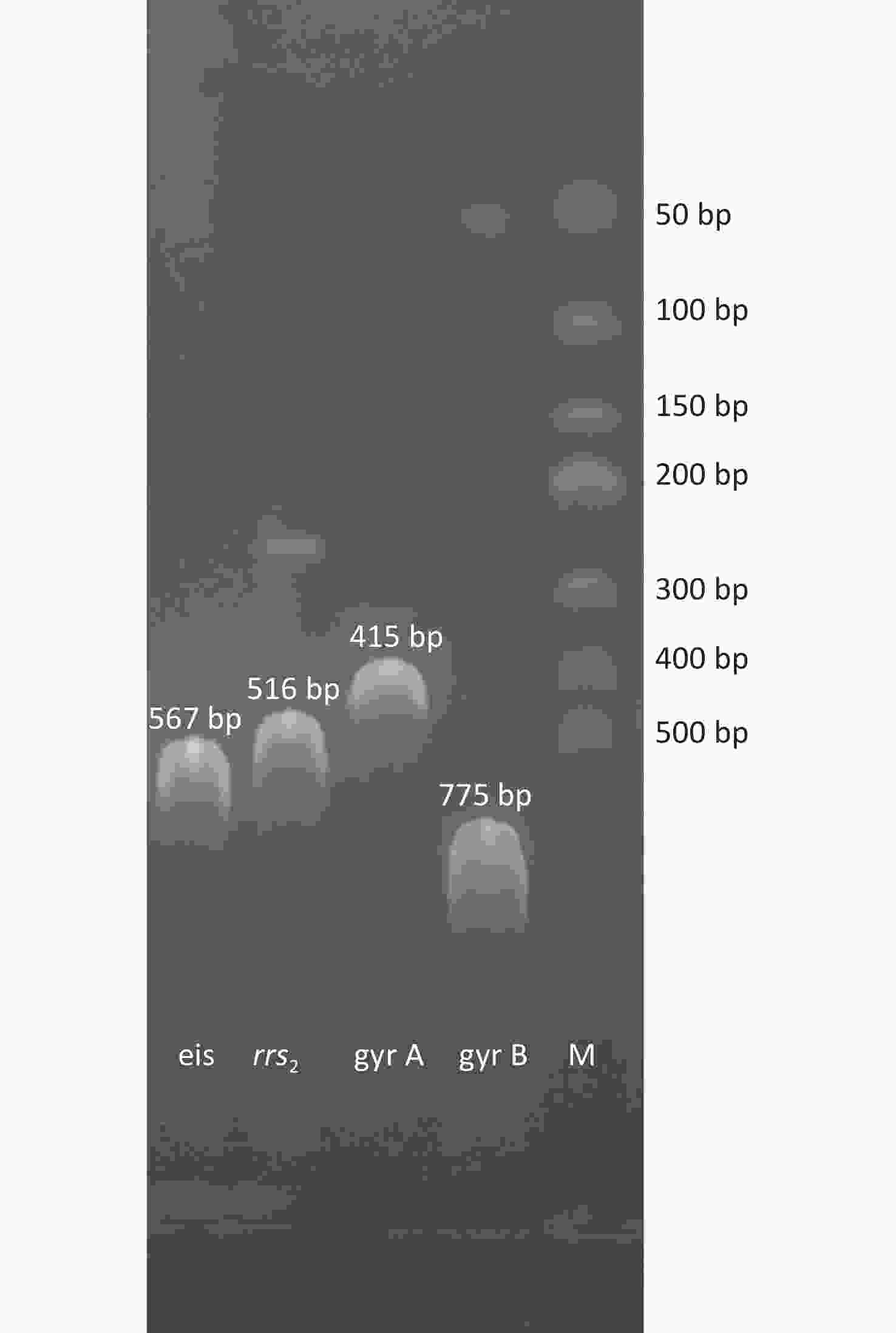
Figure S1. Agarose gel electrophoresis of PCR assays for the identification of eis, rrs2, gyrA, and gyrB genes. M: DL500 DNA Marker (Takara, Code No. 3590A).
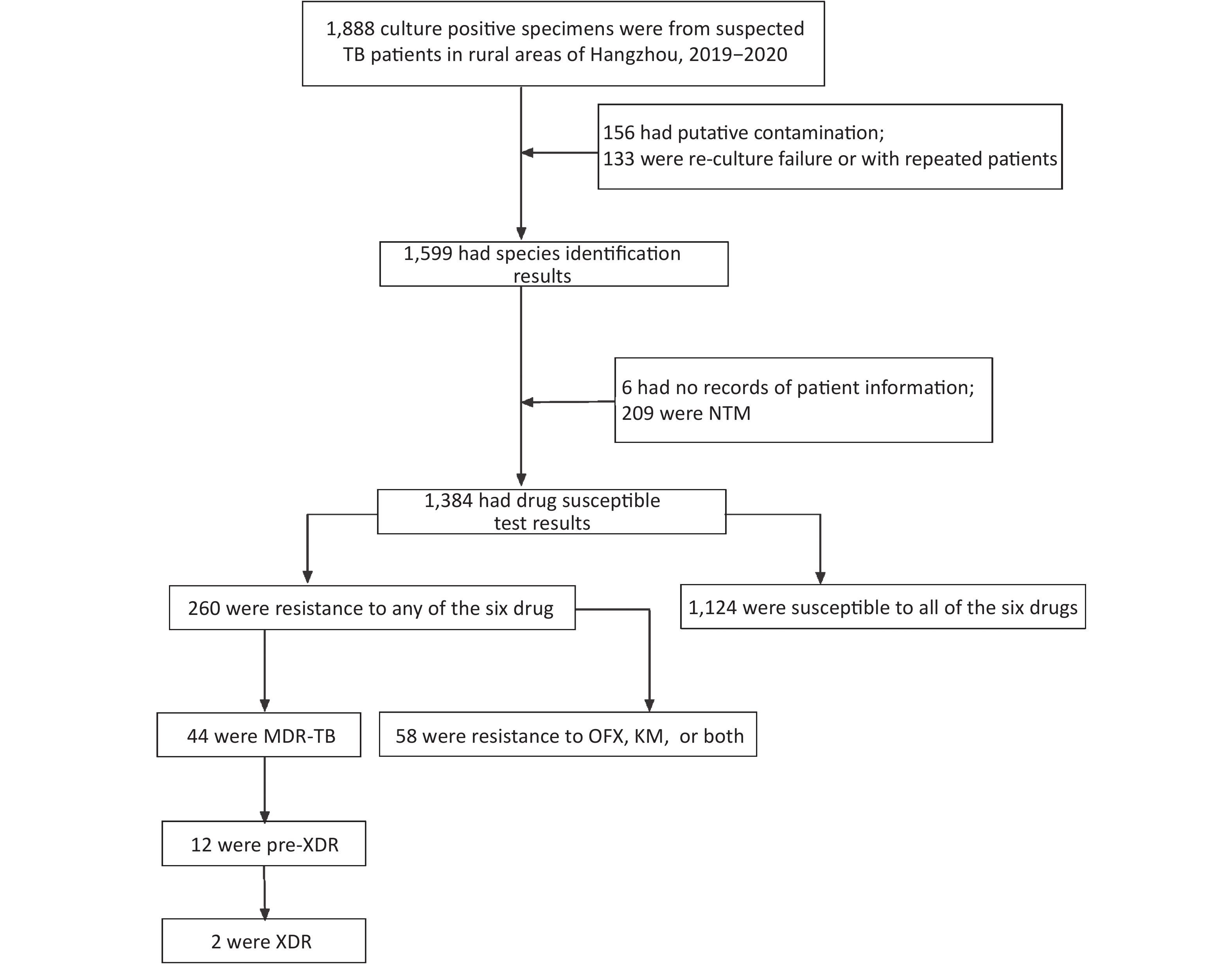
A total of 1,888 sputum culture-positive specimens of suspected TB from ten designated hospitals were collected from 2019 to 2020. Of these, 289 had putative contamination and were either re-culture failures or repeat samples from some patients, and therefore, were excluded from the study (Figure 1). Six specimens had no records of patient information, and 209 were non-tuberculosis Mycobacterium. Of the remaining 1,384 specimens, 1,124 were susceptible to all six drugs, 44 were MDR-TB, and 58 were resistant to OFX, KM, or both.
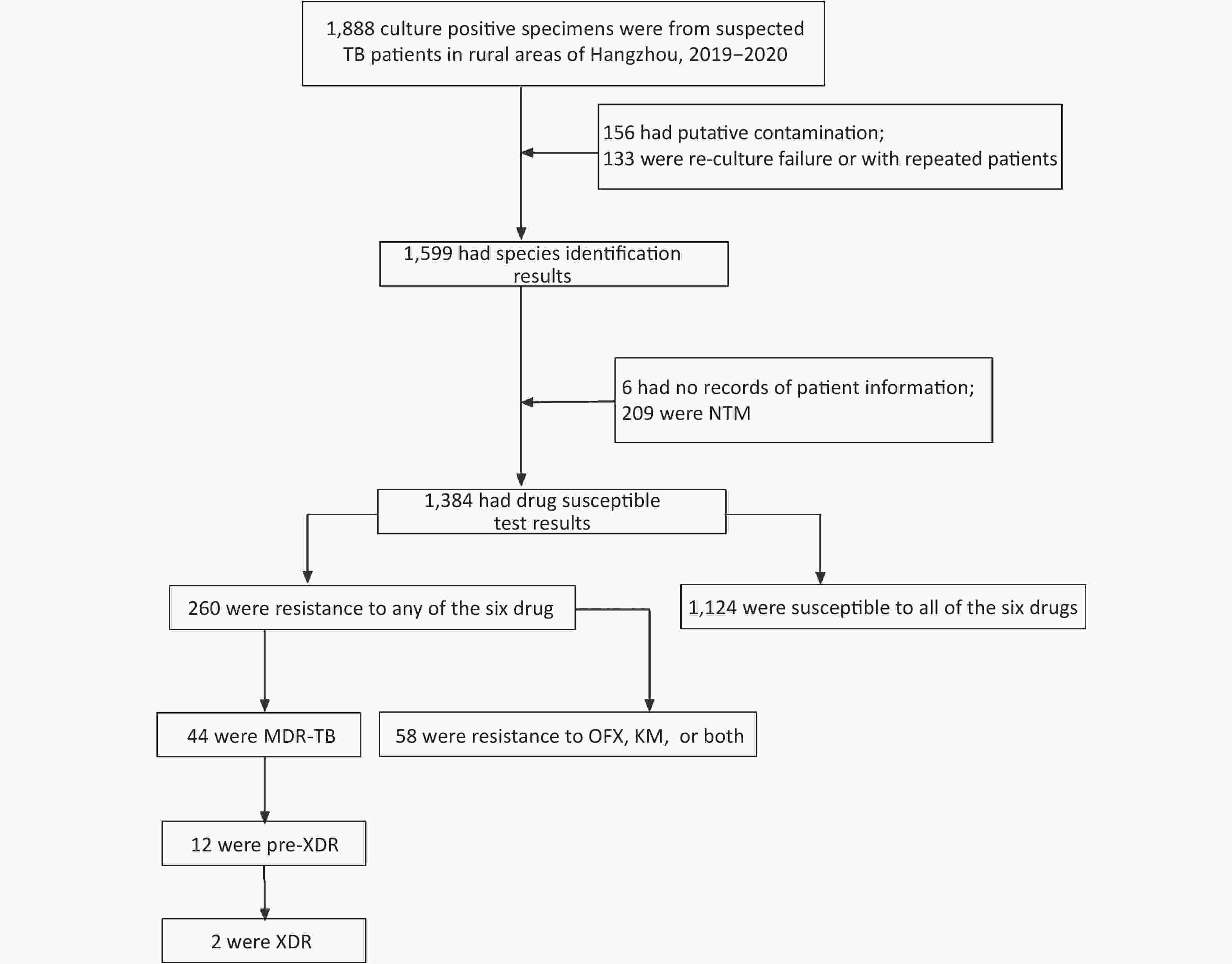
Figure 1. Flow chart of drug resistance MTBC identified from 1,888 culture-positive specimens of suspected TB patients in rural areas of Hangzhou from 2019 to 2020. MTBC: mycobacterium tuberculosis complex, TB: tuberculosis, NTM: nontuberculosis mycobacterium; MDR-TB: multi-drug resistant TB, XDR: extensively-drug resistant TB, OFX: ofloxacin, KM: kanamycin.
Thirty-three specimens were resistant only to OFX, and 11 were resistant to KM; 44 of 58 strains were non-MDR, and 14 were MDR (Table 1). Neither gyrA nor gyrB gene mutations were found in eight OFX resistant strains, and neither eis not rrs2 gene mutations were found in three KM resistant strains (Table 1). The most prevalent mutations were located in gyrA at codon 94 (D→G) (29/50; 58%), followed by gyrA at codon 90 (A→V) (12/50; 24%), as previously reported[5]. We identified a novel mutation in the gyrB gene at codon 499 (N→D) (1/50; 2%) in a non-MDR strain that was phenotypically resistant to both OFX and KM. The mutation at codon 499 in the gyrB gene was also reported previously; however, the amino acid change was different[6]. Therefore, continued efforts should be aimed at clarifying how these mutations confer phenotypic OFX resistance. We detected the presence of a mutation in the rrs2 gene at codon 1401 (A→G) (8/11; 72.73%) in phenotypic KM resistant strains, with a higher frequency than reported in earlier studies[6]. The predominance of the gyrA94 (D→G) and rrs21401 (A→G) mutations indicated that mutations in these two genes play a central role in OFX and KM resistance in Hangzhou, China.
Resistance patterns No. of strains Mutant alleles (detected/not detected) O resistance (n = 50) K resistance (n = 11) gyrA gyrB Not detected eis rrs2 Susceptible to all drugs 1,124 Non-MDR I 62 R 5 S 56 E 3 O 34 A90V (10/34) D94G (21/34) 3 IS 40 IE 4 IO 3 A90V (1/3) D94G (2/3) SE 2 EK 1 A1401G (1/1) OK 1 N499D (1/1) A1401G (1/1) ISO 2 2 ISK 1 A1401G (1/1) IEK 1 1 ISEK 1 A1401G (1/1) MDR IR 11 IRS 8 IRE 2 IRSE 9 IREO 1 D94G (1/1) IRSEO 7 A90V (1/7) D94G (4/7) 2 IRSEK 4 1 A1401G (3/4) IRSEOK 2 D94G (1/2) 1 1 A1401G (1/2) Note. MDR, Multidrug resistant tuberculosis; XDR, extensively drug resistant tuberculosis; I, Isoniazid; R, Rifampicin; S, Streptomycin; E, Ethambutol; O, Ofloxacin; K, Kanamycin. Table 1. Genetic mutations of Ofloxacin and Kanamycin resistantce for MDR and non-MDR strains
In our study, no KM resistant strains had mutations in the eis gene, and we discovered a discordance between the results of phenotypic drug susceptibility testing and genotypic mutations in 18.97% (11/58) of these strains (Table 1)—a proportion much lower than that in previous studies[5]. Nonetheless, our findings may suggest the existence of unexplored resistance mechanisms[7].
As shown in Table 1, in all mono-drug resistant strains, 21.25% (34/160) had OFX resistance. The proportions of OFX and KM resistant strains were 18.52% (40/216) and 2.31% (5/216) in non-MDR, and 22.73% (10/44) and 13.64% (6/44) in MDR. The rapid increase in KM resistance in MDR might be indicative of poor outcomes and survival among these patients. We found no mutations in the eis promoter gene associated with KM resistance, although its mutations have been reported to be highly associated with KM resistance[8]. We were unable to draw a conclusion regarding the frequencies of mutations in the eis gene, because of the small number of KM resistance strains.
In addition, to assess the performance of gene sequencing in predicting OFX and KM resistance, we analyzed the phenotypic and genotypic results of 116 strains (Table 2). With phenotypic drug susceptibility testing, the gold standard method, the sensitivity for detection of OFX resistance according to the gyrA gene was 84.0% (95% CI: 70.89% to 92.83%), similarly to data from other countries[9]. However, the sensitivity of the rrs2 gene for detecting KM resistance was 72.73% (95% CI: 39.03% to 93.98%), a value lower than that reported for Hebei province[6]. Both gyrB and eis had lower sensitivity for phenotypic prediction.
Mutant alleles Drug resistance (n = 58) Drug susceptible (n = 58) Sensitivity (%, 95% CI) Specificity (%, 95% CI) Accuracy (%, 95% CI) O K O K M NM M NM M NM M NM gyrA 42 8 0 58 84.00
(70.89−92.83)100.00
(93.84−100.00)92.59
(85.93−96.75)gyrB 1 49 0 58 2.00
(0.05−10.65)100.00
(93.84−100.00)54.63
(44.76−64.24)eis 0 11 0 58 0.00
(0.00−28.49)100.00
(93.84−100.00)84.06
(73.26−91.76)rrs2 (nt 1158−1674) 8 3 0 58 72.73
(39.03−93.98)100.00
(93.84−100.00)95.65
(87.82−99.09)Note. "M" means "mutations", and "NM" means "no mutations were found"; O, Ofloxacin; K, Kanamycin Table 2. Accuracy analysis of genotypic for Ofloxacin and Kanamycin resistantce
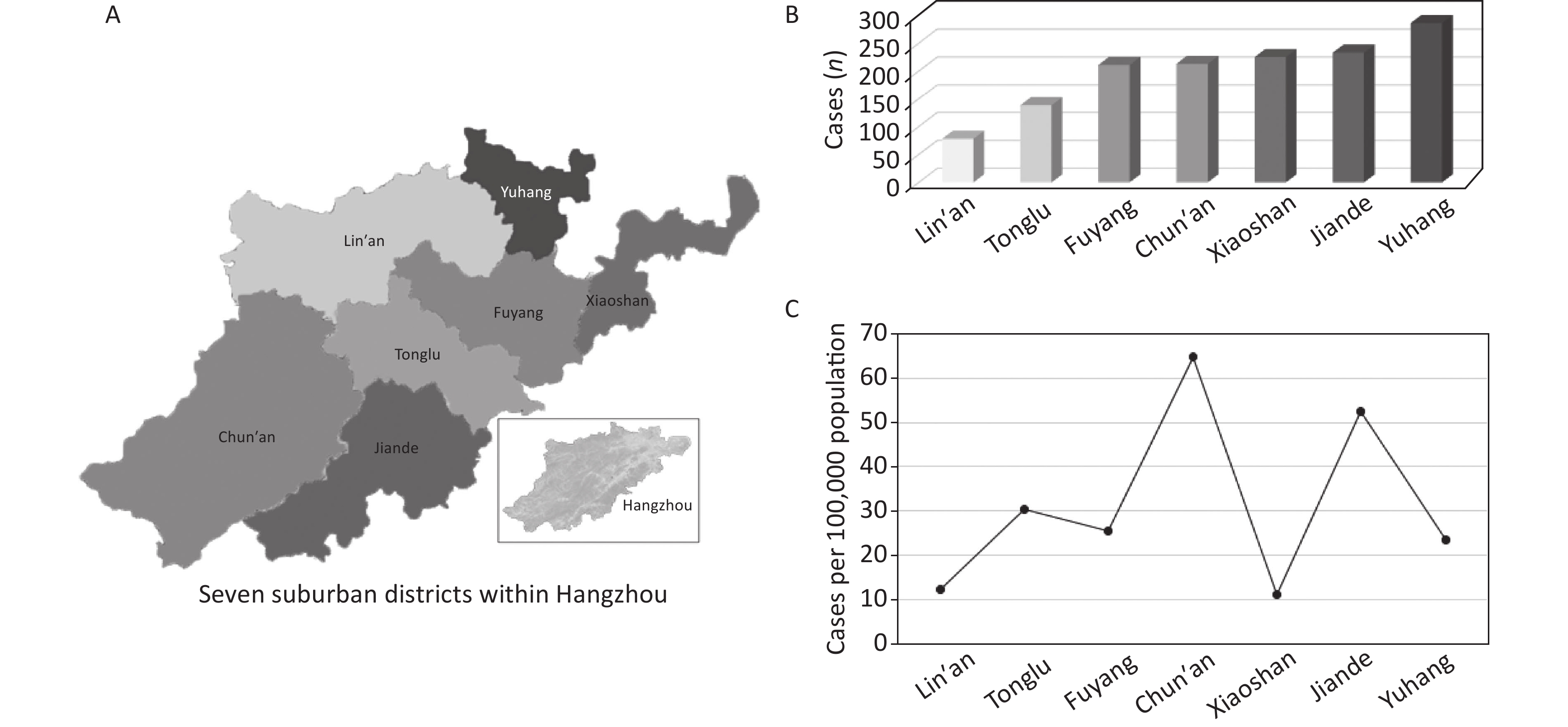
We selected samples from seven suburban counties in Hangzhou for the following reasons: 1) the population in these areas has been growing rapidly in recent years, with many migrants and large population flows; 2) data from drug resistant TB surveillance have indicated a recent increase in OFX resistance in these regions; and 3) some counties are lagging in economic development and have a high incidence of drug-resistant TB. Our results showed that the three regions with the highest numbers of TB cases were Yuhang, Jiande, and Xiaoshan, with case numbers of 286, 233, and 255, respectively. The two districts with the highest and lowest incidence rate per 100,000 people were Chun’an and Xiaoshan according to the most recent census data (
https://tjgb.hongheiku.com/10425.html ), in agreement with the results of our previous studies (Supplementary Figure S2, available in www.besjournal.com)[10].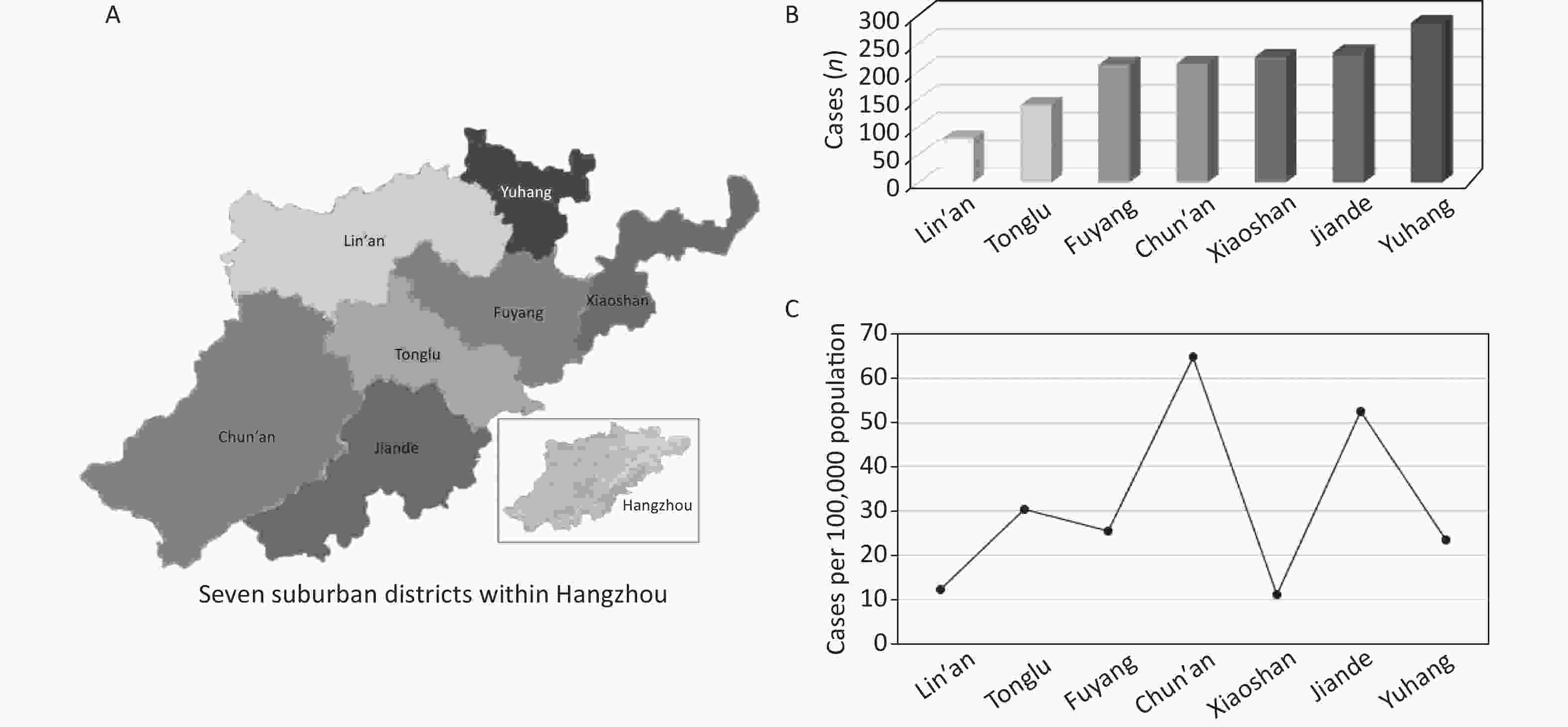
Figure S2. The spatial distributions and TB prevalence rate of seven districts in Hangzhou from 2019 to 2020. Spatial distributions of seven suburban districts within Hangzhou (A); Distributions of TB incidences (n) (B); Incidences of TB cases per 100,000 population by districts (C).
Out results may aid in establishing rapid molecular diagnostic methods for identifying OFX and KM resistance in Hangzhou, China. However, additional studies including a substantial panel of OFX resistant strains are required to further explore the proportions of the novel mutation in the gyrB at codon 499 (N→D) in this region.
On the basis of the high prevalence of OFX resistance in these areas, we identified 58 OFX and/or KM resistant strains from 1,384 MTBC. Because resistance to FQs and SLIDs other than OFX and KM was not analyzed, we found no statistical difference in the proportion of resistance to the two second-line drugs between MDR and non-MDR.
The major conclusions of this study are as follows. First, the most common mutations were single or double amino acid substitutions in gyrA at codon 90 (A→V) and 94 (D→G) for OFX resistance, and mutations in rrs2 at codon 1401 (A→G) for KM resistance. Second, a novel substitution in gyrB at codon 499 (N→D) was also detected. Finally, based on phenotypic drug resistance results, the specificity of genotype for predicting drug resistance was 100.0% (95% CI: 93.84% to 100.0%), the sensitivity of gyrA mutations for predicting OFX resistance was 84.0% (95% CI: 70.89% to 92.83%), and the sensitivity of rrs2 mutations for predicting KM resistance was 72.73% (95% CI: 39.03% to 93.98%).
JIA Qing Jun and ZENG Mei Chun contributed to the study conception, methods, and writing; XIE Li and CHENG Qing Lin designed the study and performed literature research; LI Qing Chun and HUANG Yin Yan performed the data analysis; WU Yi Fei and AI Li Yun performed the experimental studies; LU Min and FANG Zi Jian performed writing, review and editing. All authors read and approved the final version of the manuscript.
HTML
Reference
 22015Supplementary Materials.pdf
22015Supplementary Materials.pdf
|

|

 Quick Links
Quick Links
 DownLoad:
DownLoad: