

 下载:
下载:

-
Viral hepatitis is an important challenge to public health worldwide. As hepatitis B is well controlled due to vaccination, the disease burden caused by the spread of hepatitis C has become increasingly prominent. Hepatitis C is an infectious disease that is mainly blood-borne. The rate of chronicity ranges from 55% to 85% after people are infected with the hepatitis C virus (HCV)[1-2]. Twenty years after infection in the general population, the incidence of cirrhosis ranges from 5% to 15%[3]. The annual incidence of HCV-associated hepatocellular carcinoma (HCC) in patients with cirrhosis ranges from 2% to 4%[4]. Since 2010, in the United States and other developed countries, there have been breakthroughs in hepatitis C drug treatment, and the vast majority of hepatitis C still in the hepatitis stage can achieve very good therapeutic effect or even cure, which provides a historic opportunity for the elimination of hepatitis C[5-7]. Therefore, starting in 2012, the National Health Commission (NHC) of China established a special department at the National Center for AIDS/STD Control and Prevention (NCAIDS) of the Chinese Center for Disease Control and Prevention (CDC) to coordinate and manage the prevention and treatment of hepatitis C throughout the country. In the literature, the reported number of hepatitis C cases rose slowly from 1997 to 2003 with an average annual increase of 27.89%, and that grew rapidly from 2004 to 2011 with an average annual increase of 48.79%[8]. This study aimed to analyze the epidemiological characteristics of reported hepatitis C cases in China from 2012 to 2016.
Data regarding hepatitis C case information were obtained from the medical case report system of the Chinese CDC, and from the annual report on surveillance of infectious disease in China (2012-2016) published by China National Health and Family Planning Commission. Reportable cases of HCV infection are defined by the diagnostic criteria and principles for the management of viral hepatitis C (WS 213-2008), which include (1) clinically diagnosed case defined as case with positive HCV antibody and epidemiological or clinical criteria, and (2) confirmed case defined as a case with positive HCV-RNA. Epidemiological criteria include patients' reported contact with any blood, blood products or human tissue; history of any invasive medical procedures, hemodialysis, organ transplants, or unsafe injections (including that of illicit drugs); history of commercial blood donation, sexual contact with an HCV-infected person and children born to HCV-infected mothers. Clinical criteria include the clinical symptoms of liver disease, increased levels of liver function parameters (serum aspartate aminotransferase, alanine aminotransferase or bilirubin), B-mode ultrasonography, computed tomography scan or magnetic resonance imaging findings indicative of splenomegaly and hepatomegaly, damage to the liver parenchyma or widening of the portal vein. The reported hepatitis C cases in this report include both clinically diagnosed cases and confirmed cases.
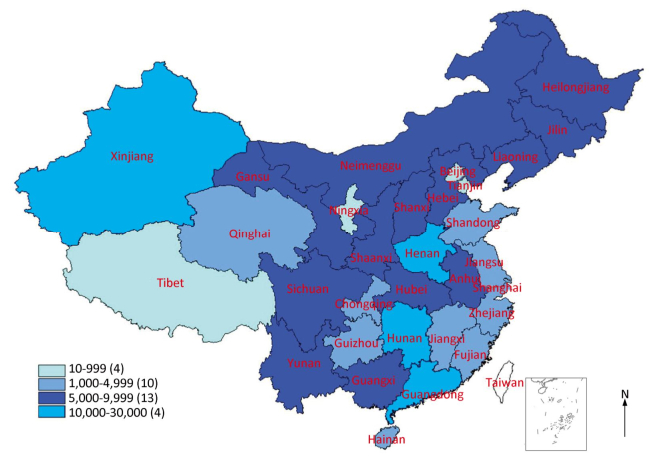
From 2012 to 2016, the number of reported hepatitis C cases per year was relatively stable, with an average of approximately 204, 000 annually. The most prominent change in 2016 was that Guangdong surpassed Henan to become number 1 in the country, and the number of reported cases in Henan Province had decreased year by year. The regional distribution of the number of reported cases was not balanced. The reported hepatitis C cases from the top four provinces with five-year averages of more than 10, 000 cases (Henan, Guangdong, Hunan, and Xinjiang) accounted for 36.6% of the national total, and the last four provinces (Tibet, Tianjin, Ningxia, and Beijing) reported only 1.0% of cases in the country (Figure 1). The top ten provinces with the five-year average number of reported cases were: Henan, Guangdong, Hunan, Xinjiang, Guangxi, Sichuan, Yunnan, Shanxi, Hubei, and Hebei.

Figure 1. Distribution map of reported hepatitis C cases by five-year average in China, 2012-2016.
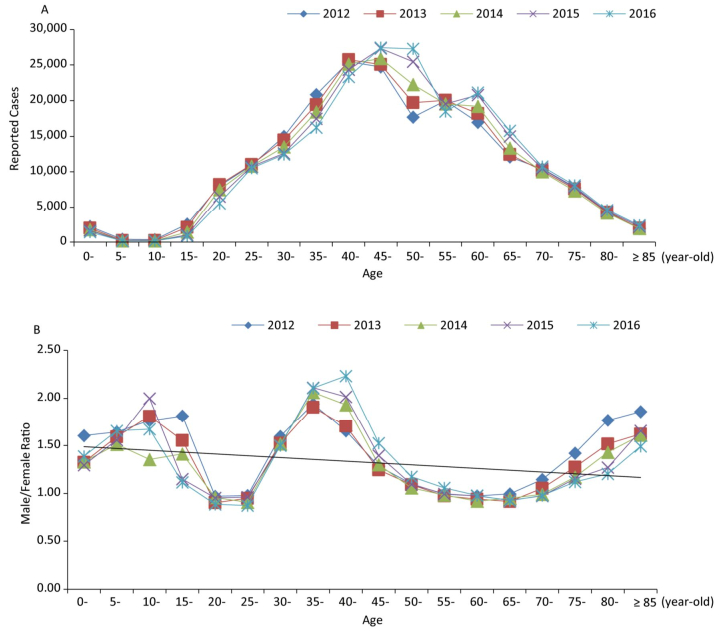
From 2012 to 2016, the age distribution of reported hepatitis C cases overlapped; however, the percentage of cases from 30 to 69 years increased year by year, respectively 75.75%, 76.42%, 77.61%, 78.19%, and 78.39%. The peak age of the most reported cases saw an increasing trend. During the same years, the proportion of child cases under the age of 15 years tended to decrease, accounting for 1.50%, 1.24%, 1.09%, 1.00%, and 0.91%, respectively. Among child cases under the age of 15 years, the number of infant cases aged 0-4 years was significantly higher, which was due to reasons such as postnatal examinations or kindergarten pre-entry examinations. The number of reported cases increased with age from 10 to 39 years, and decreased with age after 60 years. The male/female ratios of reported cases were stable with more males than females: 1.28, 1.23, 1.24, 1.25, and 1.28, respectively, from 2012 to 2016. Interestingly, in the age groups of 20-29 and 55-69 years, the percentages of cases among men were slightly lower than those of women, with sex ratios less than 1 (Figure 2). The proportion of farmers has increased year by year, accounting for 53.49%, 54.55%, 55.39%, 56.80%, and 57.26% of the total reported cases from 2012 to 2016 respectively. During the same years, the proportion of reported student and child cases declined year by year, at 2.42%, 1.96%, 1.65%, 1.41%, and 1.25%, respectively.
Figure 2. Number (A) and male/female ratio (B) of reported hepatitis C cases by age in China, 2012-2016.
The monthly distribution chart of hepatitis C cases from 2012 to 2016 shows that the monthly number reported during the Spring Festival (January or February) was relatively lower, and it rebounded in March and remained relatively stable from April to December. Qin et al. reported that the number of reported hepatitis C cases in China showed a slow growth trend from 1997 to 2003 with an average annual increase of 27.89%, and showed a rapid growth trend from 2004 to 2011 with an average annual increase of 48.79%[8]. Comparing with Qin's report, the number of reported hepatitis C cases was clearly stable and remains at just over 200, 000 per year in China during 2012-2016. Compared with that of the previous year, the number of cases increased (or decreased) at 0.76%, -0.17%, 2.51%, and -0.51%, respectively, from 2013 to 2016.
The Chinese Government established a paper-based reporting system for selected infectious diseases in the 1950s. Since 2003, this system has been web-based. The Chinese CDC is responsible for managing the online reporting system for notifiable infectious diseases. Data are collected by health workers at the county (district), city (prefecture) and provincial level centers for disease prevention and control, which ensure the data availability for 31 provinces in China (except Hongkong, Macao, Taiwan). The 39 notifiable infectious diseases are divided into three classes (A, B, and C). Viral hepatitis, including hepatitis C, is a class B infectious disease. After clinicians diagnose a hepatitis C case, they should complete a standard case report card for infectious diseases and report it through the network within 24 h. As far as hepatitis C was concerned, the number of reported hepatitis C cases in China showed a slow growth trend from 1997 to 2003 and a rapid growth trend from 2004 to 2011. This should be objectively attributed to the network reporting system beginning in 2003 which greatly improved the efficiency and convenience of case reporting. However, the number of reported hepatitis C cases in China from 2012 to 2016 began to stabilize at a steady level with an average annual report of 204, 000 cases. The annual fluctuations are very small. On the one hand, this is because lots of cumulative cases have been discovered and reported in succession, so the fast-growing trend is ending, and the cases naturally being reported to the platform reach a bottleneck after years of network reporting. On the other hand, in October 2012, the NCAIDS of the Chinese CDC set up a special office to implement 'special disease management' which effectively reduced excessive and repeated cases. As a result, it has been clearly stable since 2013.
The special disease management includes two measures: Firstly, to standardize reporting and avoid excessive reporting. According to the diagnostic criteria of viral hepatitis C (WS 213-2008), a clinically diagnosed case is defined as a case with positive HCV antibody and epidemiological or clinical criteria. In practice, many clinicians tend to report 'clinically diagnosed case' with a single positive HCV antibody test. Secondly, to reduce the annual number of repeated reported cases. Hepatitis C is a chronic infectious disease, and there existed annual repeated reported cases in the same hospital and the same region in 2012 and before due to the lack of unified management and standards. A survey revealed that the average annual repeated reporting rate of hepatitis C cases in China was 3.8% during 2009-2011[9]. Since 2013, the NCAIDS of the Chinese CDC has strengthened the training and strict management of hepatitis C case reporting standards throughout the country to avoid excessive and repeated reporting.
The authors have no conflicts of interest to disclose.
doi: 10.3967/bes2018.103
-
-
Figure 1. Distribution map of reported hepatitis C cases by five-year average in China, 2012-2016.
-
[1] Chen SL, Morgan TR. The natural history of hepatitis C virus (HCV) infection. Int J Med Sci, 2006; 3, 47-52. http://d.old.wanfangdata.com.cn/OAPaper/oai_doaj-articles_cca4fe43e3264b66c253643f0f7650bc [2] Chinese Society of Hepatology and Chinese Society of Infectious Diseases, Chinese Medical Association. The guideline of prevention and treatment for hepatitis C:a 2015 update. Chin J Hepatol, 2015; 23, 906-23. (In Chinese) http://en.cnki.com.cn/Article_en/CJFDTotal-CRBX201101003.htm [3] Freeman AJ, Dore GJ, Law MG, et al. Estimating progression to cirrhosis in chronic hepatitis C virus infection. Hepatology, 2001; 34, 809-16. doi: 10.1053/jhep.2001.27831 [4] El-Serag HB, Rudolph KL. HepatocelIular carcinoma:epidemiology and molecular carcinogenesis. Gastroenterology, 2007; 132, 2557-76. doi: 10.1053/j.gastro.2007.04.061 [5] European Association for Study of Liver. EASL recommendations on treatment of hepatitis C 2015. J Hepatol, 2015; 63, 199-236. doi: 10.1016/j.jhep.2015.03.025 [6] John-Baptiste AA, Tomlinson G, Hsu PC, et al. Sustained responders have better quality of life and productivity compared with treatment failures long after antiviral therapy for hepatitis C. Am J Gastroenterol, 2009; 104, 2439-48. doi: 10.1038/ajg.2009.346 [7] Chen XY, Shang J, Yang RF, et al. High sustained virological response to optimized therapy for refractory chronic hepatitis C treatment-naive patients:a multicenter randomized study. Chin J Hepatol, 2015; 23, 412-7. (In Chinese) [8] Qin QQ, Guo W, Wang LY, et al. Epidemiological characteristics of hepatitis C in China, 1997-2011. Chin J Epidemiol, 2013; 34, 548-51. (In Chinese) http://d.old.wanfangdata.com.cn/Periodical/xdyfyx201507008 [9] Chen FF, Wang LY, Qin QQ, et al. Re-reporting and diagnosis of hepatitis C in China. Disease Surveillance, 2014; 29, 578-82. (In Chinese) http://d.old.wanfangdata.com.cn/Periodical/jbjc201407017 -

 点击查看大图
点击查看大图
图(2)
计量
- 文章访问数: 2451
- HTML全文浏览量: 769
- PDF下载量: 138
- 被引次数: 0

 Quick Links
Quick Links