

 下载:
下载:


-
Respiratory diseases (RD) such as bronchitis, emphysema, and asthma significantly affect global public health and result in a substantial socioeconomic burden on individuals and society[1]. In 2019, RD affected an estimated 454.6 million individuals worldwide and caused 4 million deaths, making it the third leading cause of mortality globally[2]. In China, in 2017, RD was observed in 27.8 million individuals (41.4%) aged 65 years and older[3]. Because the older adult population is increasing, the incidence of RD is expected to continue to increase[4], and these diseases can significantly impair individuals' quality of life and increase mortality risk[5]. Thus, identifying preventable risk factors for RD has become a critical priority in the effort to reduce the global burden of this disease.
Studies have consistently confirmed outdoor air pollution as a significant risk factor for RD[6-8]. Research has demonstrated that individuals spend a large portion of their time indoors, particularly older adults who tend to engage in reduced outdoor activities, increasing their risk of exposure to indoor air pollutants[9]. Household chemicals have been identified as significant contributors to indoor air pollution[10]. These chemicals, including insecticides, repellents, anti-caries agents, and cleaning products, are often volatile and can enter the body through the respiratory tract, irritating the respiratory mucosa[11]. The use of household chemicals such as insecticides has been linked to increased indoor concentrations of PM2.5[12]. Collectively, these factors suggest a potential association between household chemicals, which are key sources of indoor air pollution, and RD.
Extensive research has examined the harmful effects of chemical exposure on respiratory health in occupational settings. For example, the association between exposure to harsh cleaning products and RD among occupational household cleaners has been investigated, demonstrating an increased risk of asthma and RD[13-16]. Moreover, Orianne Dumas et al. revealed that the population-attributable fraction of weekly use of disinfectants on chronic obstructive pulmonary disease risk among female nurses was 12%[17]. However, research on nonprofessional individuals is limited. In a longitudinal study, Zock et al. explored the relationship between the use of household cleaning sprays and asthma in adults and observed a dose-response relationship between the frequency of spray use and the risk of asthma[18]. Several studies have investigated the association between household chemical usage and RD among children[19,20], and the findings highlighted a negative effect on the respiratory outcomes of children under 5 years of age. A study of young people in Germany reported that heavy use of disinfectants more than tripled the risk of asthma compared with not using disinfectants[21]. However, these studies have limitations in that they overlook other important household chemicals, such as repellents and insecticides; do not simultaneously consider the effects of single chemical exposure and multiple chemical exposures. Additionally, the current research is mostly focused on Western countries, with limited studies on household chemical exposure and RD among the older population in China. Thus, further research is required to delve into this crucial issue.
We examined the relationship between eight major household chemicals and RD risk in an older population (aged ≥ 65 years) in China. These chemicals include insecticides, repellents, anti-caries agents, air fresheners, air purifiers, disinfectants, toilet cleaners, and oil removers. Additionally, we developed a total score to evaluate the frequency and quantity of household chemical usage and its potential dose-response relationship with RD risk.
-
The data for this study were obtained from the 2018 wave of the China Longitudinal Health and Longevity Survey (CLHLS)[22], which is a nationwide health and aging survey that aims to investigate the effect of various health-related factors on health outcomes. The survey included demographic information; lifestyle habits; educational attainment; indoor air quality factors; and the prevalence of bronchitis, emphysema, asthma, and pneumonia. Comprehensive information regarding the CLHLS has been published[23].
The 2018 CLHLS gathered data from 15,874 participants, with 12,411 individuals as the original interviewees for that year. We excluded participants aged < 65 years and those with missing information regarding household chemical use and whether they had a diagnosis of RD. Imputation of missing values in the covariables was conducted using nearest-neighbor interpolation.
Supplementary Table S1 (available in www.besjournal.com) provides a comparison of our results before and after this procedure. Finally, 12,866 participants were included in the analysis. -
The prevalence of RD was assessed using self-reported medical history of four diseases: bronchitis, emphysema, asthma, and pneumonia. Each participant was asked the following question: “Do you currently experience symptoms of bronchitis, emphysema, asthma, or pneumonia?” Participants who responded “yes” to this question were categorized as having RD.
-
The frequency of utilization of eight household chemicals was determined using a questionnaire. Each participant was asked, “Have you ever used the following chemicals in your home? Insecticides, repellents, anti-caries agents, air fresheners, air purifiers, disinfectants, toilet cleaners, and oil removers. The responses were “rarely or never,” “seldom,” “sometimes,” and “often.” In the survey, the specific corresponding standards were as follows: “rarely or never,” non-usage; “seldom,” a frequency of use not exceeding once a week; “sometimes,” a usage frequency of at least once a week but not exceeding once daily; and “often,” a usage frequency of once daily or more. In addition, a simple score was derived to reflect the frequency of use of each product: one, “rarely or never”; two, seldom”; three, “sometimes”; and four, “often.” The scores for each product were then combined to create a total score for household chemical usage for every respondent, ranging from eight for no exposure to 32 for regular exposure to all eight products. The total score comprehensively reflected the frequency and quantity of household chemical use.
-
Based on existing studies[24-26], this study included covariates pertaining to demographic attributes (age and gender), socioeconomic status (place of residence, educational attainment, and marital status), lifestyle and health behaviors (smoking habits, drinking, and physical activity), and indoor air quality factors (horizontal distance from major traffic sources; presence of mildew or musty odors at home; kitchen ventilation during cooking activities; and seasonal ventilation of indoor windows during spring, summer, fall, and winter).
-
Continuous variables are reported as mean ± standard deviation or median with interquartile range, and categorical variables are expressed as counts and percentages (%). The baseline characteristics of the two groups (patients with and without RD) were compared using t-tests and chi-square tests.
Binary logistic regression analysis was used to investigate the association between household chemical use and RD risk, with adjustments for potential confounders. Three models were constructed: Model 1, without confounding adjustments; Model 2, adjusted for demographic characteristics and health-related behaviors; and Model 3, further adjusted for indoor air quality factors. Subgroup analyses were performed based on age (65–85 and > 85 years), gender, residence (city, town, and rural), and smoking habits (no or yes) using Model 3. Correlation analysis was conducted to explore the relationship between the frequency of use of the eight household chemicals. Restricted cubic spline analysis was employed to identify any potential nonlinear relationship between the total score and RD risk. The usage scores of the eight household chemicals were categorized into four groups (< 9, 9–16, 17–24, 25–32) to perform a trend test. Sensitivity analyses were conducted to ensure the robustness of the results, including excluding research subjects aged ≥ 105, merging the frequency of household chemicals use into three categories, and calculating E-value using methods by VanderWeele and Ding[27,28].
R version 4.2.2 was used for statistical analysis. All tests were two-tailed, and a P-value of less than 0.05 was considered statistically significant.
-
Table 1 describes the baseline characteristics of the RD and non-RD cohorts. Of the 12,866 participants included in the study, 1,453 were diagnosed with RD. The mean age of the participants was 85.5 ± 11.6 years, with 44.3% male and 55.7% female. Significant differences were observed between the RD and non-RD groups in gender, residential status, smoking, and drinking (all P < 0.05). There were statistically significant differences in indoor air quality between the two groups for kitchen ventilation during cooking, ventilation in winter, a musty smell at home, and proximity to the main road (all P < 0.05). Except for insecticides and anti-caries agents, the frequency of use of the other six household chemicals differed significantly between the two groups (all P < 0.05). Finally, a significant difference was noted in the total score of household chemical usage between the two groups (all P < 0.05).
Table 1. Baseline characteristics of participants
Variables/subgroups Total sample RD Non-RD t/χ2 P-value Total sample, n (%) 12,866 1,453 (11.3) 11,413 (88.7) − − Age (year, mean ± SD) 85.5 ± 11.6 86.1 ± 10.6 85.4 ± 11.7 −2.150 0.031 Sex, n (%) 79.538 < 0.001 Male 5,702 (44.3) 803 (55.3) 4,899 (42.9) − − Female 7,164 (55.7) 650 (44.7) 6,514 (57.1) − − Residence, n (%) 50.537 < 0.001 City 2,817 (21.9) 422 (29.0) 2,395 (21.0) − − Town 4,269 (33.2) 458 (31.5) 3,811 (33.4) − − Rural 5,780 (44.9) 573 (39.4) 5,207 (45.6) − − Smoking, n (%) 118.488 < 0.001 Yes 3,852 (29.9) 614 (42.3) 3,238 (28.4) − − No 9,014 (70.1) 839 (57.7) 8,175 (71.6) − − Drinking, n (%) 13.795 < 0.001 Yes 3,225 (25.1) 422 (29.0) 2,803 (24.6) − − No 9,641 (74.9) 1,031 (71.0) 8,610 (75.4) − − Exercised, n (%) 2.981 0.086 Yes 4,005 (31.1) 481 (33.1) 3,524 (30.9) No 8,861 (68.9) 972 (66.9) 7,889 (69.1) Education level, n (%) 2.453 0.293 0 years 6,225 (48.4) 675 (46.5) 5,550 (48.6) 1–5 years 2,957 (23.0) 348 (24.0) 2,609 (22.9) > 5 years 3,684 (28.6) 430 (29.6) 3,254 (28.5) Never married, n (%) 107 (0.8) 17 (1.2) 90 (0.8) 6.149 0.186 Insecticide, n (%) 7.775 0.051 Rarely or never 8,545 (66.4) 920 (63.3) 7,625 (66.8) Seldom 2,566 (19.9) 323 (22.2) 2,243 (19.7) Sometimes 1,298 (10.1) 152 (10.5) 1,146 (10.0) Often 457 (3.6) 58 (4.0) 399 (3.5) Repellents, n (%) 8.254 0.041 Rarely or never 5,143 (40.0) 554 (38.1) 4,589 (40.2) Seldom 3,297 (25.6) 356 (24.5) 2,941 (25.8) Sometimes 2,738 (21.3) 322 (22.2) 2,416 (21.2) Often 1,688 (13.1) 221 (15.2) 1,467 (12.9) Anti−caries agent, n (%) 5.142 0.162 Rarely or never 10,924 (84.9) 1,206 (83.0) 9,718 (85.1) Seldom 1,179 (9.2) 152 (10.5) 1027 (9.0) Sometimes 519 (4.0) 62 (4.3) 457 (4.0) Often 244 (1.9) 33 (2.3) 211 (1.8) Air freshener, n (%) 8.917 0.030 Rarely or never 11,858 (92.2) 1,319 (90.8) 10,539 (92.3) Seldom 659 (5.1) 86 (5.9)) 573 (5.0) Sometimes 245 (1.9) 28 (1.9) 217 (1.9) Often 104 (0.8) 20 (1.4) 84 (0.7) Air purifier, n (%) 15.896 0.001 Rarely or never 12,272 (95.4) 1,359 (93.5) 10,913 (95.6) Seldom 380 (3.0) 62 (4.3) 318 (2.8) Sometimes 151 (1.2) 19 (1.3) 132 (1.2) Often 63 (0.5) 13 (0.9) 50 (0.4) Disinfectant, n (%) 21.344 < 0.001 Rarely or never 10,720 (83.3) 1,149 (79.1) 9,571 (83.9) Seldom 1,184 (9.2) 169 (11.6) 1,015 (8.9) Sometimes 595 (4.6) 82 (5.6) 513 (4.5) Often 367 (2.9) 53 (3.6) 314 (2.8) Toilet cleaner, n (%) 24.051 < 0.001 Rarely or never 8,542 (66.4) 887 (61.0) 7,655 (67.1) Seldom 1,726 (13.4) 228 (15.7) 1,498 (13.1) Sometimes 1,376 (10.7) 165 (11.4) 1,211 (10.6) Often 1,222 (9.5) 8.2 (11.9) 1,049 (9.2) Oil remover, n (%) 30.411 < 0.001 Rarely or never 9,160 (71.2) 953 (65.6) 8,207 (71.9) Seldom 1,440 (11.2) 183 (12.6) 1,257 (11.0) Sometimes 1,085 (8.4) 137 (9.4) 948 (8.3) Often 1,181 (9.2) 180 (12.4) 1,001 (8.8) Total score (mean ± SD) 11.45 ± 3.47 11.95 ± 3.69 11.39 ± 3.43 −5.864 < 0.001 Distance from the traffic artery, n (%) 13.131 0.011 < 50 meters 2,309 (17.9) 293 (20.2) 2,016 (17.7) > 50 meters 10,557 (82.1) 1,160 (79.8) 9,397 (82.3) Musty smell, n (%) 7.910 0.005 Yes 1,814 (14.1) 240 (16.5) 1,574 (13.8) No 11,052 (85.9) 1,213 (83.5) 9,839 (86.2) Kitchen ventilation, n (%) 9.828 0.020 No 1,144 (8.9) 113 (7.8) 1,031 (9.0) Yes 11,722 (91.1) 1,340 (92.2) 10,382 (91.0) Ventilation Winter, n (%) 10.295 0.016 No 2,684 (20.9) 302 (20.8) 2,382 (20.9) Yes 10,182 (79.1) 1,151 (79.2) 9,031 (79.1) No ventilation Spring, n (%) 652 (5.1) 72 (5.0) 580 (5.1) 1.995 0.573 No ventilation Summer, n (%) 362 (2.8) 39 (2.7) 323 (2.8) 2.275 0.517 No ventilation Autumn, n (%) 576 (4.5) 61 (4.2) 515 (4.5) 1.194 0.755 -
Table 2 describes the results of the logistic regression analysis examining the relationship between the frequency of use of eight household chemicals and RD risk. In Model 1, individuals who frequently used repellents had a 20% increased risk of RD (OR = 1.20, 95% CI 1.01–1.45), and those who often used oil removers had a 34% increased risk (OR = 1.34, 95% CI 1.09–1.66), both compared with participants who did not use or used these chemicals rarely. In Model 2, we adjusted for age, sex, residence, smoking, and drinking, and the results showed a significant association between the frequent use of repellents (OR = 1.30, 95% CI 1.08–1.57) or oil removers (OR = 1.26, 95% CI 1.02–1.56) and RD. Finally, in Model 3, we adjusted for all potentially relevant factors, and the frequent use of repellents (OR = 1.28, 95% CI 1.06–1.55) or oil removers (OR = 1.28, 95% CI 1.03–1.58) remained a significant risk factor for RD. Apart from repellents and oil removers, the frequency of use of the other six household chemicals showed no statistically significant relationship with RD risk.
Table 2. Logistic regression analysis of household chemicals usage and respiratory disease
Characteristics Model 1 Model 2 Model 3 OR 95% CI OR 95% CI OR 95% CI Insecticide Never Ref Ref Ref Seldom 1.14 0.97−1.33 1.12 0.96−1.31 1.13 0.96−1.32 Sometimes 1.02 0.83−1.25 1.02 0.83−1.25 1.02 0.84−1.26 Often 0.96 0.70−1.32 0.95 0.69−1.31 0.95 0.69−1.31 Repellents Never Ref Ref Ref Seldom 0.89 0.76−1.04 0.91 0.77−1.07 0.90 0.77−1.06 Sometimes 1.07 0.91−1.26 1.13 0.96−1.33 1.12 0.95−1.32 Often 1.20* 1.01−1.45 1.30** 1.08−1.57 1.28* 1.06−1.55 Anti−caries agent Never Ref Ref Ref Seldom 1.01 0.82−1.24 1.03 0.83−1.27 1.03 0.84−1.27 Sometimes 0.93 0.69−1.25 0.97 0.72−1.30 0.97 0.72−1.31 Often 0.98 0.66−1.46 1.00 0.67−1.49 1.00 0.67−1.48 Air freshener Never Ref Ref Ref Seldom 0.82 0.61−1.12 0.82 0.60−1.12 0.82 0.61−1.12 Sometimes 0.76 0.46−1.23 0.74 0.46−1.21 0.74 0.45−1.21 Often 1.28 0.71−2.31 1.37 0.75−2.49 1.34 0.73−2.44 Air purifier Never Ref Ref Ref Seldom 1.42 0.99−2.05 1.45 1.00−2.10 1.44 0.99−2.08 Sometimes 1.10 0.61−1.98 1.16 0.64−2.10 1.14 0.63−2.06 Often 1.27 0.60−2.66 1.15 0.54−2.43 1.18 0.56−2.50 Disinfectant Never Ref Ref Ref Seldom 1.17 0.95−1.43 1.10 0.90−1.35 1.10 0.90−1.35 Sometimes 1.23 0.94−1.60 1.18 0.91−1.55 1.19 0.91−1.56 Often 1.08 0.77−1.51 1.00 0.71−1.40 1.01 0.72−1.41 Toilet cleaner − Never Ref Ref Ref Seldom 1.15 0.95−1.39 1.09 0.89−1.32 1.10 0.91−1.34 Sometimes 1.00 0.81−1.24 0.93 0.75−1.15 0.95 0.77−1.18 Often 1.12 0.89−1.39 1.00 0.80−1.25 1.02 0.81−1.28 Oil remover Never Ref Ref Ref Seldom 1.13 0.92−1.38 1.01 0.82−1.24 1.02 0.83−1.26 Sometimes 1.16 0.93−1.44 1.06 0.84−1.32 1.07 0.85−1.34 Often 1.34** 1.09−1.66 1.26* 1.02−1.56 1.28* 1.03−1.58 Note. OR, odds ratio; CI, confidence interval; *P < 0.05; **P < 0.01; ***P < 0.001; Model 1 did not account for confounding variables; Model 2 was adjusted for age, sex, residency, smoking, and drinking; Model 3 was further adjusted for musty smell, distance from the traffic artery, kitchen ventilation, and ventilation during winter. -
Table 3 illustrates the relationship between the overall score of eight household chemicals usage and RD risk. In Model 3, all pertinent factors were taken into account, and the findings indicate a substantial link between the total score (OR = 1.03, 95% CI 1.02–1.05) and the risk of RD. This means that for every one-point increase in the total score of household chemicals, the risk of developing RD increases by 3%.
Table 3. Logistic regression analysis of the total score of eight household chemicals usage and respiratory disease
Characteristics Model 1 Model 2 Model 3 OR 95% CI OR 95% CI OR 95% CI Total score 1.04*** 1.03−1.06 1.03*** 1.02−1.05 1.03*** 1.02−1.05 Age 1.01*** 1.01−1.02 1.01*** 1.01−1.02 Sex (male) 0.75*** 0.65−0.85 0.74*** 0.65−0.85 Residence (city) Town 0.71*** 0.61−0.82 0.69*** 0.60−0.80 Rural 0.67*** 0.58−0.77 0.65*** 0.57−0.75 Smoking (no) 1.71*** 1.49−1.96 1.70*** 1.48−1.95 Drinking (yes) 1.11 0.97−1.28 1.11 0.97−1.28 Musty smell (no) 0.77** 0.66−0.90 Distance from the traffic artery (< 50 m) 0.85* 0.74−0.98 Kitchen ventilation (no) 1.12 0.91−1.39 Ventilation Winter (no) 0.91 0.79−1.05 Note. OR, odds ratio; CI, confidence interval; *P < 0.05; **P < 0.01; ***P < 0.001. -
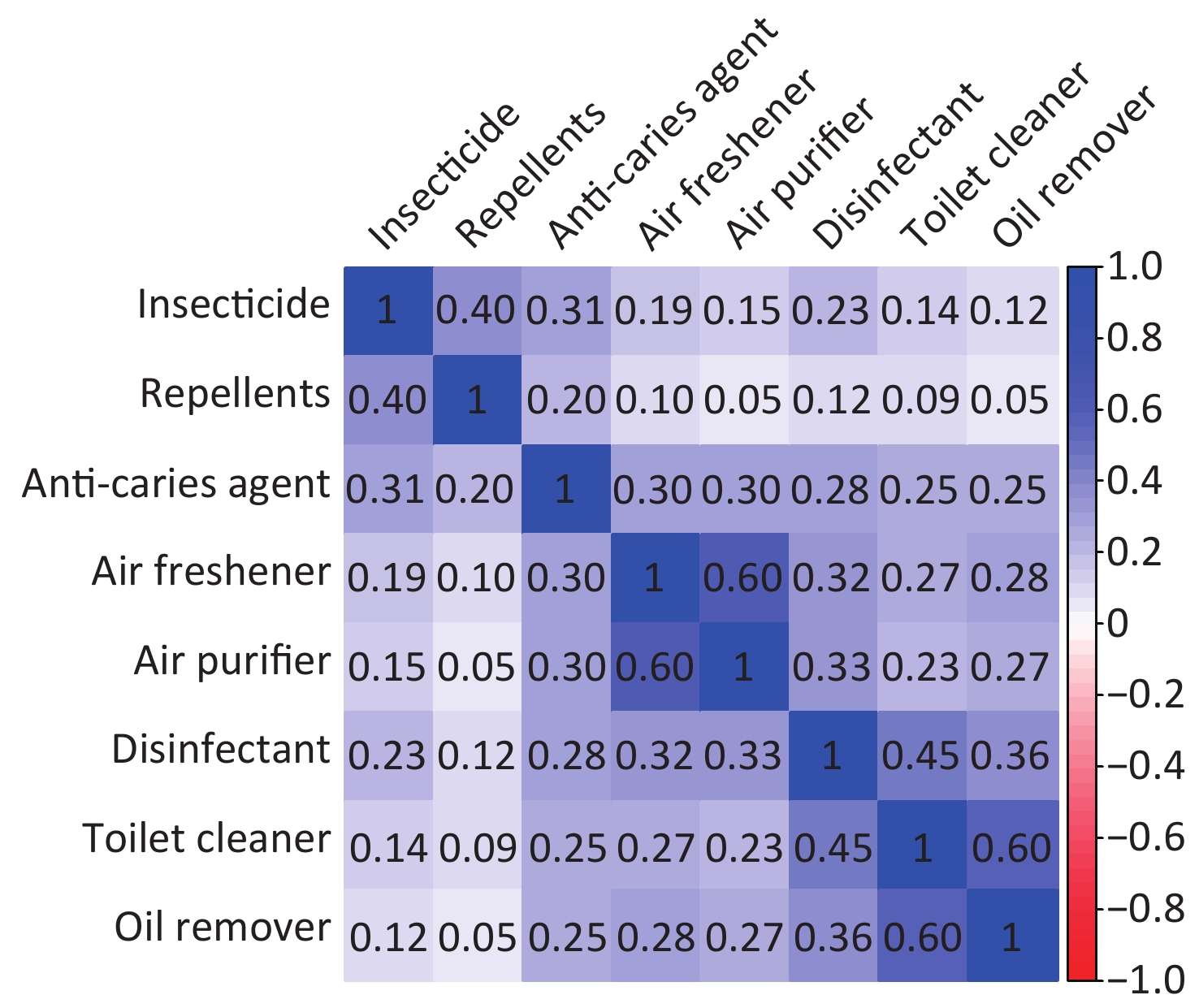
Figure 1 illustrates the correlations between the frequency of use of the eight household chemicals, showing that most chemicals exhibited low correlations with frequency of use. Specifically, the correlation coefficient between air purifiers and air fresheners was 0.6, indicating a relatively strong correlation with their frequency of use. By contrast, the correlation between air purifiers and repellents in frequency of use was minimal, with a correlation coefficient of 0.05. The correlation between the frequency of use of oil removers and toilet cleaners was relatively high, with a correlation coefficient of 0.6, and oil removers showed low correlations with the frequency of use of other chemicals.
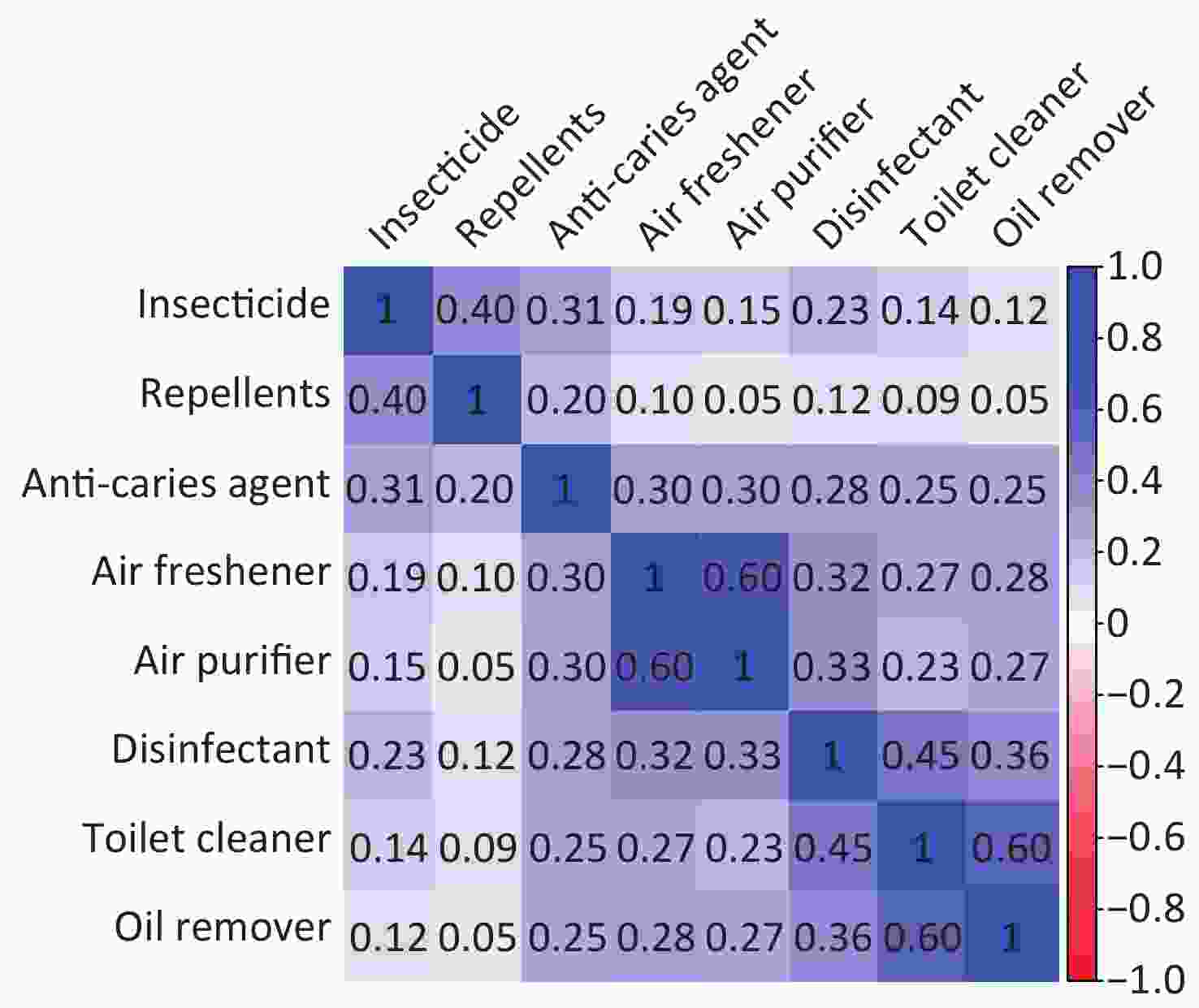
Figure 1. Correlation between the frequency of household chemicals usage.
-
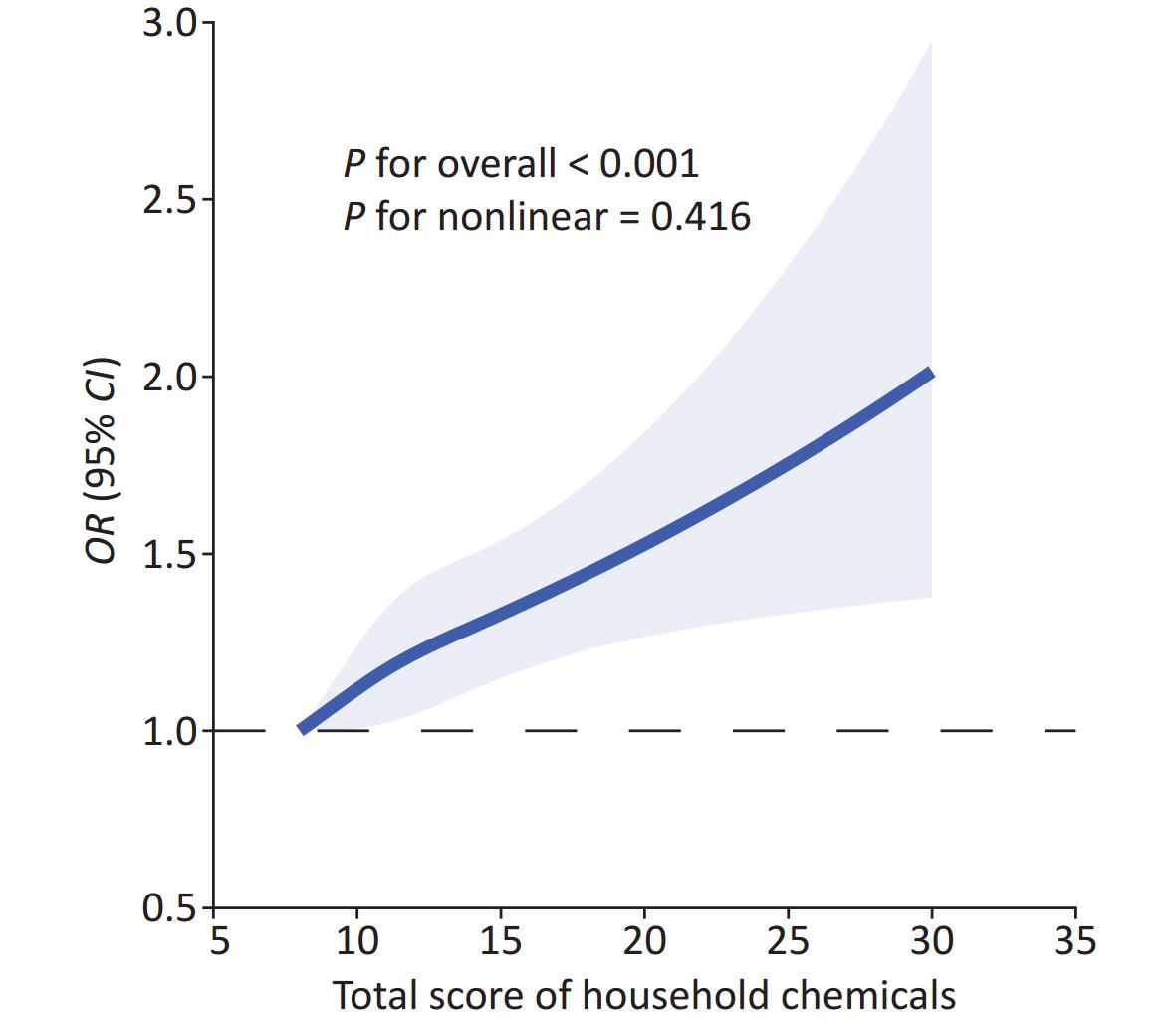
Figure 2 shows the results of the restricted cubic spline regression analysis. A linear dose-response relationship was observed between the total score of the eight household chemicals and RD risk among all participants, with no significant non-linearity observed (P > 0.05). RD risk increased substantially as the total score for household chemical use increased.
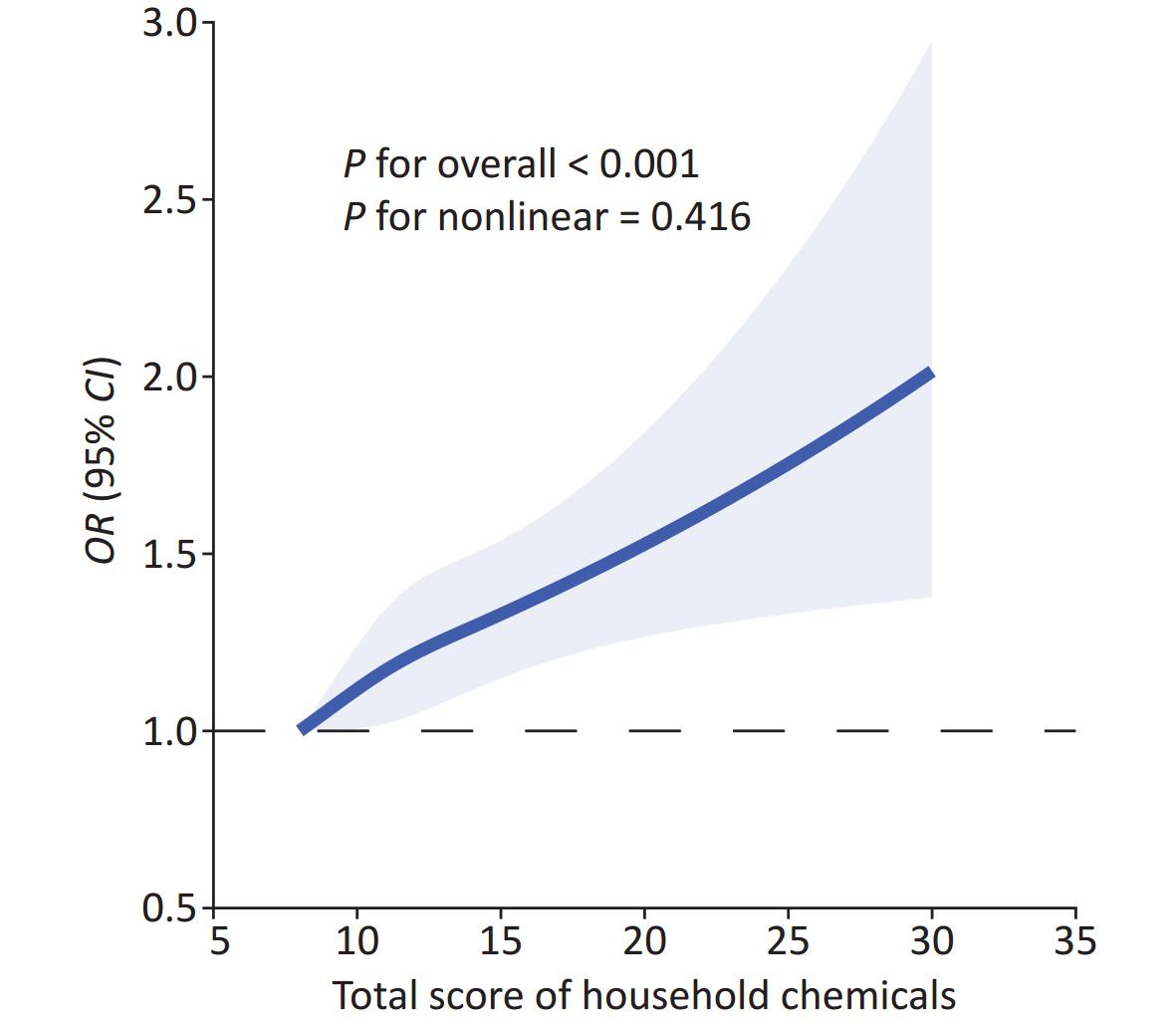
Figure 2. A dose-response relationship was observed between the overall score of household chemicals and RD in a restricted cubic spline regression model. The model was adjusted for age, gender, residential status, smoking and drinking, presence of musty smell, distance from traffic artery, kitchen ventilation, and winter ventilation. The model was constructed using three knots at the 20th, 50th, and 80th percentiles of the total household chemicals score, with the minimum score as the reference. Solid lines represent OR; shaded areas represent 95% confidence intervals (CIs).
Table 4 describes the results of trend tests performed after stratifying the total scores. After controlling for all confounding factors, a significant linear trend was observed between the total score and RD risk (P for trend = 0.01). This result indicates that as the frequency and quantity of household chemical usage increase, the RD risk increases. Using patients with the total score below 9 as a reference, the OR for patients with the total score ranging from 25 to 32 is 2.33 (95% CI 1.25–4.09).
Table 4. Linear trend test between total score of household chemicals usage and respiratory disease
Total chemical score Case/N Model 1 Model 2 Model 3 < 9 308/3,145 Ref Ref Ref 9−16 992/8,611 1.20 (1.05−1.37) 1.13 (0.99−1.30) 1.13 (0.98−1.29) 17−24 138/1,037 1.41 (1.14−1.75) 1.21 (0.97−1.50) 1.21 (0.97−1.51) 25−32 15/73 2.38 (1.29−4.13) 2.28 (1.22−4.00) 2.33 (1.25−4.09) P for trend < 0.001 0.01 0.01 Note. Data are expressed as odds ratio (confidence interval); Model 1 did not account for confounding variables; Model 2 was adjusted for age, sex, residency, smoking, and drinking; Model 3 was further adjusted for musty smell, distance from the traffic artery, kitchen ventilation, and winter ventilation. -
Subgroup analysis was performed to evaluate the correlation between the overall score and RD risk among specific subpopulations based on various demographic characteristics. Table 5 demonstrates that, after controlling for all relevant factors as mentioned earlier, a significant association between the overall score and RD risk was observed in individuals aged > 85 years (OR = 1.05, 95% CI 1.03–1.07, P < 0.001), females (OR = 1.03, 95% CI 1.01–1.06, P = 0.005), males (OR = 1.04, 95% CI 1.01–1.06, P = 0.002), city residents (OR = 1.04, 95% CI 1.01–1.06, P = 0.010), town residents (OR = 1.05, 95% CI 1.02–1.08, P = 0.001), smoking (OR = 1.05, 95% CI 1.02–1.07, P < 0.001), and non-smoking (OR = 1.03, 95% CI 1.01–1.05, P = 0.004) but not in those aged 65–85 years and rural residents.
Table 5. Subgroup analysis of the total score of eight household chemicals usage and respiratory disease
Characteristics OR 95% CI P-value Full sample (n = 12,866) 1.034 1.018–1.050 < 0.001 Age 65–85 1.021 0.998–1.044 0.077 > 85 1.048 1.025–1.070 < 0.001 Sex Male 1.035 1.013–1.058 0.002 Female 1.033 1.010–1.056 0.005 Residence City 1.035 1.008–1.063 0.010 Town 1.048 1.019–1.078 0.001 Rural 1.019 0.992–1.047 0.174 Smoking No 1.031 1.010–1.053 0.004 Yes 1.048 1.022–1.074 < 0.001 Note. OR, odds ratio; CI, confidence interval; model adjusted for age, sex, residency, smoking, drinking, musty smell, distance from the traffic artery, kitchen ventilation, and winter ventilation. The sensitivity analysis results of the two groups aligned with the primary results (Supplementary Tables S2, S3, and S4, available in www.besjournal.com). The outcomes of the E-values are provided in Supplementary Tables S5 and S6 (available in www.besjournal.com), which provide an estimate of the relative risk necessary for any unmeasured confounders to overcome the observed correlation between household chemical usage and RD in this study.
Table S2. Logical regression after deleting participants older than 105 years old
Characteristics Before deletion After deletion OR 95% CI OR 95% CI Insecticide Rarely or never 1 1 Seldom 1.13 0.96–1.32 1.15 0.98–1.35 Sometimes 1.02 0.84–1.26 1.01 0.82–1.24 Often 0.95 0.69–1.31 0.95 0.68–1.30 Repellents Rarely or never 1 1 Seldom 0.90 0.77–1.06 0.91 0.77–1.07 Sometimes 1.12 0.95–1.32 1.14 0.97–1.35 Often 1.28* 1.06–1.55 1.29** 1.07–1.57 Anti–caries agent Rarely or never 1 1 Seldom 1.03 0.84–1.27 1.00 0.80–1.23 Sometimes 0.97 0.72–1.31 0.96 0.71–1.29 Often 1.00 0.67–1.48 0.97 0.64–1.43 Air freshener Rarely or never 1 1 Seldom 0.82 0.61–1.12 0.84 0.61–1.13 Sometimes 0.74 0.45–1.21 0.75 0.45–1.20 Often 1.34 0.73–2.44 1.4 0.74–2.52 Air purifier Rarely or never 1 1 Seldom 1.44 0.99–2.08 1.42 0.97–2.05 Sometimes 1.14 0.63–2.06 1.15 0.62–2.04 Often 1.18 0.56–2.5 1.08 0.48–2.28 Disinfectant Rarely or never 1 1 Seldom 1.10 0.9–1.35 1.09 0.89–1.34 Sometimes 1.19 0.91–1.56 1.18 0.89–1.54 Often 1.01 0.72–1.41 0.99 0.69–1.38 Toilet cleaner Rarely or never 1 1 Seldom 1.10 0.91–1.34 1.11 0.91–1.35 Sometimes 0.95 0.77–1.18 0.95 0.77–1.18 Often 1.02 0.81–1.28 1.02 0.81–1.27 Oil remover Rarely or never 1 1 Seldom 1.02 0.83–1.26 1.03 0.83–1.26 Sometimes 1.07 0.85–1.34 1.08 0.86–1.35 Often 1.28* 1.03–1.58 1.28* 1.03–1.58 Note. OR, odds ratio; CI, confidence interval; *, P < 0.05; **, P < 0.01; ***, P < 0.001; Model was adjusted for age, sex, residency, smoking, drinking, musty smell, distance from the traffic artery, kitchen ventilation and ventilation Winter. Table S3. Logical regression after deleting participants older than 105 years old
Characteristics Before deletion After deletion OR 95% CI OR 95% CI Total score 1.03*** 1.02–1.05 1.03*** 1.02–1.05 Age 1.01*** 1.01–1.02 1.01*** 1.01–1.02 Sex (male) 0.74*** 0.65–0.85 0.75*** 0.65–0.86 Residence (city) Town 0.69*** 0.60–0.80 0.70*** 0.60–0.81 Rural 0.65*** 0.57–0.75 0.66*** 0.57–0.77 Smoking (no) 1.70*** 1.48–1.95 1.70*** 1.47–1.95 Drinking (yes) 1.11 0.97–1.28 1.12 0.97–1.28 Musty smell (no) 0.77** 0.66–0.90 0.75** 0.65–0.88 Distance from the traffic artery (< 50 m) 0.85* 0.74–0.98 0.87 0.76–1.00 Kitchen ventilation (no) 1.12 0.91–1.39 1.11 0.90–1.37 Ventilation Winter (no) 0.91 0.79–1.05 0.92 0.80–1.06 Note. OR, odds ratio; CI, confidence interval; *, P < 0.05; **, P < 0.01; ***, P < 0.001; Table S4. Logistic regression analysis of household chemicals and RD
Characteristics OR 95% CI Insecticide Low 1 Medium 1.09 0.95– 1.26 High 0.96 0.69– 1.31 Repellents Low 1 Medium 1.00 0.87– 1.14 High 1.26* 1.04– 1.52 Anti–caries agent Low 1 Medium 1.00 0.84– 1.20 High 1.01 0.67– 1.48 Air freshener Low 1 Medium 0.80 0.60– 1.05 High 1.35 0.72– 2.41 Air purifier Low 1 Medium 1.33 0.95– 1.85 High 1.18 0.54– 2.43 Disinfectant Low 1 Medium 1.13 0.95– 1.35 High 0.99 0.70– 1.38 Toilet cleaner Low 1 Medium 1.03 0.87– 1.22 High 1.03 0.82– 1.28 Oil remover Low 1 Medium 1.04 0.87– 1.23 High 1.27* 1.02– 1.57 Note. OR, odds ratio; CI, confidence interval; *, P < 0.05; **, P < 0.01; ***, P < 0.001; Model was adjusted for age, sex, residency, smoking, drinking, musty smell, distance from the traffic artery, kitchen ventilation and ventilation Winter. Table S5. E–value
Characteristics Model 1 E–value OR 95% CI Point CI Insecticide Rarely or never 1 Seldom 1.13 0.96–1.32 Sometimes 1.02 0.84–1.26 Often 0.95 0.69–1.31 Repellents Rarely or never 1 Seldom 0.9 0.77–1.06 Uometimes 1.12 0.95–1.32 Often 1.28* 1.06–1.55 1.88 1.31 Anti–caries agent Rarely or never 1 Seldom 1.03 0.84–1.27 Sometimes 0.97 0.72–1.31 Often 1.00 0.67–1.48 Air freshener Rarely or never 1 Seldom 0.82 0.61–1.12 Sometimes 0.74 0.45–1.21 Often 1.34 0.73–2.44 Air purifier Rarely or never 1 Seldom 1.44 0.99–2.08 Sometimes 1.14 0.63–2.06 Often 1.18 0.56–2.5 Disinfectant Rarely or never 1 Seldom 1.10 0.9–1.35 Sometimes 1.19 0.91–1.56 Often 1.01 0.72–1.41 Toilet cleaner Rarely or never 1 Seldom 1.10 0.91–1.34 Sometimes 0.95 0.77–1.18 Often 1.02 0.81–1.28 Oil remover Rarely or never 1 Seldom 1.02 0.83–1.26 Sometimes 1.07 0.85–1.34 Often 1.28* 1.03–1.58 1.88 1.21 Note. OR, odds ratio; CI, confidence interval; *, P < 0.05; **, P < 0.01; ***, P < 0.001; Model 1 was adjusted for age, sex, residency, somking, drinking, musty smell, distance from the traffic artery, kitchen ventilation and ventilation Winter. Table S6. E–value
Characteristics Model 1 E–value OR 95% CI Point CI Total score 1.04*** 1.03–1.06 1.24 1.21 Note. OR, odds ratio; CI, confidence interval; *, P < 0.05; **, P < 0.01; ***, P < 0.001; Model 1 was adjusted for age, sex, residency, smoking, drinking, musty smell, distance from the traffic artery, kitchen ventilation and ventilation Winter. -
In this cross-sectional analysis, we investigated the association between the frequency of household chemical use and RD in a nationally representative sample of 12,866 older adults in China. Our study results confirmed the hypothesis that after accounting for relevant confounding factors, older individuals who regularly used repellents or oil removers had a 28% higher risk of developing RD than those who did not use repellents or oil removers. Moreover, the overall burden of the use of eight household chemicals was associated with an increased risk of RD, exhibiting a linear dose-response relationship.
Our study revealed that older individuals who frequently used repellents had a 28% increased risk of developing RD. Commonly used products in China include mosquito coils, Florida water, and mosquito repellent liquids, all of which contain DEET, citronella oil, permethrin, and other similar ingredients[29]. Permethrin, a typical class I pyrethroid insecticide, has been linked to neuroinflammation and immunotoxicity[30,31]. Moreover, increased doses of permethrin negatively affect the levels of anti-inflammatory cytokines, which are related to the development of atopic diseases and allergic reactions[31]. Studies have shown that inhalation of permethrin can lead to respiratory distress, cough, sore throat, and other respiratory symptoms[32]. Long-term exposure to permethrin has been linked to an increased incidence of asthma and chronic bronchitis in women[33,34]. Citronella oil, another common repellent ingredient, is known to cause respiratory and eye irritation and can pose a risk for allergic contact dermatitis[35]. The smoke produced by mosquito coil incense contains harmful substances such as formaldehyde and polycyclic aromatic hydrocarbons[36]. Animal experiments have revealed lung injuries in rats exposed to mosquito coil smoke, including interstitial accumulation, pulmonary edema, and emphysema[37]. Furthermore, indoor levels of PM2.5 and carbon monoxide from burning mosquito coil incense are higher than those from biomass fuel for cooking[38], which can contribute to RD caused by the use of mosquito coils. However, because of the wide variety and complex composition of repellents, further research is necessary to fully understand the association between repellent use and RD and the underlying mechanisms involved.
Our study observed that older adults who frequently used oil removers had a 28% increased risk of developing RD, which aligns with existing research findings[18]. However, our results suggest that the relationship between disinfectants and RD is not statistically significant, which contrasts with several studies indicating that occupational exposure to disinfectants increases RD risk[17,39]. A study of young Germans revealed that high usage of disinfectants was associated with more than twice the risk of asthma development compared with those who did not use disinfectants[21]. This inconsistency in research results might be attributed to several factors. First, our study solely focused on individuals aged 65 and older in 2018. At that time, awareness of household disinfection practices was lower than it is today, leading to a lower frequency of disinfectant usage in 2018 than today. In our study, only 2.9% of participants reported frequent use of disinfectants. Second, because our study adopted a cross-sectional design, we were unable to determine the duration of exposure. It is plausible that older adults who reported using disinfectants had short exposure durations. Thus, a large cohort study is necessary to validate the association between disinfectants and RD in older populations.
In the subgroup analysis, RD risk increased with the frequency and type of household chemical usage among individuals aged > 85 years. However, this relationship was not statistically significant among individuals aged 65–85 years. This result may be attributable to older individuals spending more time indoors[9], leading to prolonged exposure to household chemicals and a higher risk of developing RD. Furthermore, the relationship between the total score for household chemical usage and RD in rural areas was not significant, which might be due to larger living areas and better ventilation in rural households than in urban and suburban households. Studies have demonstrated that the severity of indoor air pollution increases as home size decreases, with residents of relatively small houses using mosquito coil incense, which has a significantly higher incidence of RD[12,38]. The study revealed that opening doors and windows reduced PM2.5 and carbon monoxide levels generated by burning mosquito coils by 95%[38], and the overall airtightness of rural houses was less than that of the residences in cities and towns. Therefore, these factors should be considered in further research.
In this study, we observed an OR of 1.03 between the total score of household chemical usage and RD, indicating that the risk of developing RD increases with the frequency and quantity of household chemical use among older adults. A study of adults showed that the use of household chemicals increases the risk of developing asthma by 49%[18]. Similar findings have been observed in preschool children[20], confirming that household chemicals have emerged as a significant risk factor for RD. Therefore, developing strategies and interventions aimed at reducing RD risk is imperative. Specific preventive measures may include: first, enhance publicity and education to raise awareness among older adults about the safe use of household chemicals; second, research and promote the use of household chemicals that are harmless or have low toxicity; third, advocate for wearing protective gear such as masks and gloves when using household chemicals to prevent harmful substances from entering the body through the respiratory system or skin; fourth, advise not remaining indoors after using insecticide or repellents to reduce exposure to harmful substances.
This study has several additional limitations. First, it is a cross-sectional study that cannot establish a causal relationship between household chemical usage and RD[40]. Second, the self-reported frequency of household chemical use may have inaccuracies, potentially biasing the analysis and leading to erroneous results. Third, RD in the CLHLS refers to a summed series of diseases occurring in the trachea, bronchi, lungs, and chest, including bronchitis, emphysema, asthma, and pneumonia, prohibiting a detailed discussion of each subdivided illness. Further research is warranted to explore the relationship between household chemical use and various RD.
Despite these constraints, the study has several advantages. First, it specifically investigated the association between household chemical usage and RD in older adults in China, an area that has been overlooked in existing research. Second, with a large sample size and nationwide representation, the study’s findings can be extrapolated to a certain extent. Third, the comprehensive CLHLS questionnaire enables us to control various confounding factors and enhance the robustness of the outcomes. Additionally, we not only examine the individual effects of eight household chemicals but also evaluate their overall burden, comprehensively analyzing the relationship between household chemical usage and RD.
-
This cross-sectional study revealed that in China, the frequent use of repellents and oil removers in households increased RD risk in older individuals aged ≥ 65 years, with the risk escalating in a dose-dependent manner with an increase in the frequency and quantity of chemical usage. Therefore, recognizing the health hazards of household chemicals and mitigating these risks through enhanced health education, advocating protective gear usage, and other preventive measures are essential. Additionally, further research is necessary to Identify the specific components of household chemical exposure and elucidate the underlying mechanisms.
-
Table S1. Comparison of results before and after missing data interpolation
Characteristics Non– interpolation Interpolation OR 95% CI OR 95% CI Insecticide Rarely or never 1 1 Seldom 1.16 0.98–1.37 1.13 0.96–1.32 Sometimes 1.01 0.82–1.26 1.02 0.84–1.26 Often 0.95 0.68–1.33 0.95 0.69–1.31 Repellents Rarely or never 1 1 Seldom 0.88 0.74–1.04 0.9 0.77–1.06 Sometimes 1.08 0.91–1.29 1.12 0.95–1.32 Often 1.32* 1.08–1.61 1.28* 1.06–1.55 Anti–caries agent Rarely or never 1 1 Seldom 1.13 0.90–1.40 1.03 0.84–1.27 Sometimes 1.11 0.82–1.50 0.97 0.72–1.31 Often 0.99 0.65–1.50 1.00 0.67–1.48 Air freshener Rarely or never 1 1 Seldom 0.82 0.59–1.15 0.82 0.61–1.12 Sometimes 0.77 0.47–1.26 0.74 0.45–1.21 Often 1.58 0.83–2.98 1.34 0.73–2.44 Air purifier Rarely or never 1 1 Seldom 1.49 1.01–2.19 1.44 0.99–2.08 Sometimes 1.19 0.64–2.19 1.14 0.63–2.06 Often 0.91 0.39–2.12 1.18 0.56–2.5 Disinfectant Rarely or never 1 1 Seldom 1.06 0.85–1.31 1.10 0.9–1.35 Sometimes 1.22 0.92–1.62 1.19 0.91–1.56 Often 0.89 0.60–1.30 1.01 0.72–1.41 Toilet cleaner Rarely or never 1 1 Seldom 1.08 0.88–1.33 1.10 0.91–1.34 Sometimes 0.88 0.70–1.11 0.95 0.77–1.18 Often 0.97 0.76–1.23 1.02 0.81–1.28 Oil remover Rarely or never 1 1 Seldom 0.98 0.79–1.23 1.02 0.83–1.26 Sometimes 1.07 0.85–1.36 1.07 0.85–1.34 Often 1.28* 1.02–1.60 1.28* 1.03–1.58 Age 1.01*** 1.01–1.02 1.01*** 1.01–1.02 Sex(male) 0.73*** 0.63–0.84 0.74*** 0.65–0.85 Residence(city) Town 0.69*** 0.58–0.81 0.69*** 0.58–0.81 Rural 0.65*** 0.55–0.77 0.65*** 0.56–0.77 Smoking(no) 1.70*** 1.49–1.96 1.70*** 1.48–1.96 Drinking(yes) 1.09 0.94–1.26 1.11 0.97–1.28 Musty smell(no) 0.79** 0.67–0.94 0.78** 0.67–0.91 Distance from the traffic artery(<50m) 0.87* 0.75–1.01 0.85* 0.74–0.97 Kitchen ventilation(no) 1.04 0.83–1.30 1.12 0.91–1.39 Ventilation Winter(no) 0.96 0.83–1.12 0.91 0.79–1.05 Note. OR, odds ratio; CI, confidence interval; *, P < 0.05; **, P < 0.01; ***, P < 0.001;
全文HTML
Data Sources and Study Population
Dependent Variable
Independent Variable
Covariables
Statistical Analysis
Baseline Characteristics
Logistic Regression Analysis of Household Chemicals Usage and RD
Logistic Regression Analysis of the Total Score of Eight Household Chemicals and RD
Correlation Analysis
Dose-response Relationship
Subgroup Analysis and Sensitivity Analysis
 24073+.pdf
24073+.pdf
|

|

 Quick Links
Quick Links