

 下载:
下载:

-
Iodine is an essential element for the synthesis of thyroid hormones. Iodine deficiency increases the burden on thyroid function and causes harm to health. The identification of convenient and reliable biomarkers for assessing iodine nutritional status is essential for evaluating iodine intake. Urinary iodine concentration (UIC) is commonly used for population level iodine status assessment but is less reliable for individuals. A 24-h urine sample is more accurate but difficult to collect[1]. Thyroid volume (Tvol) and goiter rate are suitable for evaluating the long-term iodine nutritional status in populations[2]. Blood indicator collection is an invasive procedure.
The food frequency questionnaire (FFQ) is currently the most frequently used method of estimating dietary intake in large nutritional epidemiological studies[3]. A valid and reliable iodine-specific food frequency questionnaire (I-FFQ) could serve as a valuable and effective tool for accurately estimating iodine intake in pregnant women and children[4,5]. However, dietary habits vary greatly among populations with different regional, ethnic or cultural backgrounds. Therefore, the FFQ should be tailored and validated to ensure its reliability and validity for use in a specific population. There are currently few studies on the applicability of the I-FFQ for the elderly in Gansu Province, China. This study aimed to validate the reliability and validity of the I-FFQ, which was designed based on the regional characteristics and dietary habits of Gansu Province, China, for the elderly.
The study was performed in Lanzhou city and Longxi County, Gansu Province, China. Random cluster sampling was used to select the study population between January and June 2024. A flowchart of the study is presented in Supplementary Figure S1. Inclusion criteria: (1) elderly participants aged ≥ 65 years with continuous local residency ≥ 5 years preceding enrollment; (2) college students have no travel history in the past 3 months; (3) participants who did not take iodine-containing supplements or medications. Exclusion criteria included: (1) history of serious chronic comorbidities (e.g., malignancies, cardiovascular disorders); (2) failure to complete follow-up assessments. (3) patients with hypertension and vegetarians. A total of 880 elderly individuals and 100 college students were included. Written informed consent was obtained from all the participants. The study protocol was approved by the ethics committee of Tianjin Medical University.
The semiquantitative FFQs were developed based on a review of the literature and previous FFQs established for the Chinese population. The FFQs contained informative questions about the intake frequencies of 13 types of food and water during the preceding month. A comprehensive assessment of the dietary intake among older adults was conducted using a structured, guided approach, further enhanced by a color food photography atlas[6]. Habitual iodine intake estimated from the I-FFQ was based on the equation: daily iodine intake = Σintake of each type of food × iodine concentration of each type of food + drinking water × water iodine concentration + salt intake × salt iodine concentration × (1 - 20%).
The iodine content in the food was determined by As (III)-Ce4+ catalytic spectrophotometry. The intra-assay coefficient of variation (CV) was 0.58-3.15% and the inter-assay CV was 3.40% for food iodine content. The iodine content for each food item in this study was presented in Supplementary Table S1. Urine samples were analyzed using inductively coupled plasma mass spectrometry (iCAP Q, Thermo Fisher Scientific, Frankfurt am Main, Germany). The inter- and intra-assay CVs for UIC measurements were 1.8%–2.15% and 0.93%–1.66%, respectively. Serum free thyroxine (FT4) and thyroid-stimulating hormone (TSH) were measured using the ADVIA Centaur CP fully automatic chemiluminescence immunoassay analyzer (Siemens Healthineers, Berlin, Germany). The intra-assay CV for serum FT4 and TSH was 3.44%–3.71%, 4.02%–5.19%, respectively. Tvol was measured by the professional operator using of a HaiYing HY-5511 ultrasound machine with a 7.5-MHz transducer. The diagnostic criteria for thyroid diseases are provided in Supplementary Table S2.
All statistical analyses were performed using SPSS 25.0 (IBM, Inc, New York, NY, USA), Microsoft Excel (2019 for Windows 10) and R software version 4.4.0 (R Foundation for Statistical Computing, Vienna, Austria). Continuous variables were tested for normality using the Kolmogorov-Smirnov test. Skewed data were presented as median (interquartile range). Categorical variables were expressed as number and percentage. The Mann-Whitney U test and Wilcoxon signed-rank test were used to compare non-normally distributed data. The χ2 test was used to compare the prevalence of goiter, thyroid dysfunction, and UIC level. Spearman correlation analyse, Bland-Altman plot, and Kappa test were used to verify the validity of the I-FFQ. The mean difference and limits of agreement (LOA) (mean difference ± 1.96 SD [standard deviation]) were calculated. Binary logistic analysis was used to evaluate the test-retest reliability of I-FFQ. All statistical tests were two-tailed, and a P value < 0.05 was considered statistically significant.
Cohen's kappa coefficient was calculated for agreement in the classification of individuals. Kappa value < 0.2 means slight agreement, Kappa value < 0.4 means fair agreement. Kappa value < 0.6 means moderate agreement, Kappa value < 0.8 means substantial agreement, and Kappa value ≤ 1 means almost perfect agreement.
This study was divided into two parts. The first part was the reliability analysis of I-FFQ, involving 100 college students. They conducted I-FFQ surveys at a one-month interval. As shown in Supplementary Table S3, the average age of college students was 25 years (interquartile range [IQR]: 23 years, 26 years). The iodine intake of college students estimated by the initial and repeat I-FFQ surveys was 194.11 μg/d (IQR: 113.31 μg/d, 270.13 μg/d) and 197.67 μg/d (IQR: 123.57 μg/d, 241.64 μg/d), respectively. The iodine intake of males was significantly higher than that of females in both I-FFQs (P < 0.05).
The second part was validity analysis, involving 411 (46.7%) elderly males and 469 (53.3%) elderly females. Supplementary Table S4 shows the characteristics, iodine status, and thyroid function of the elderly. The median urinary iodine (MUI) concentration and iodine intake among the elderly were 304.12 μg/L (IQR: 225.99 μg/L, 430.77 μg/L) and 183.56μg/d (IQR: 133.89 μg/d, 250.01 μg/d), respectively. The total prevalence rates of thyroid nodules and goiter were 54.3% and 6.7%, respectively, with a significantly higher prevalence observed in females compared to males (P all < 0.001).
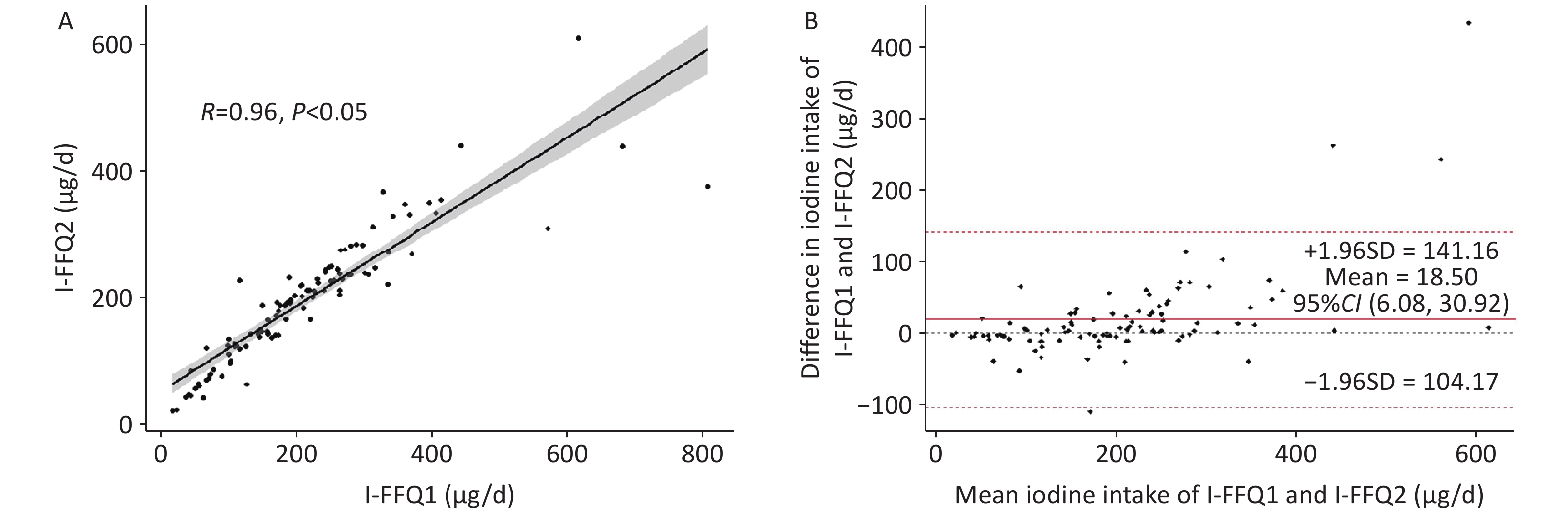
As shown in Figure 1A, the result of I-FFQ1 showed a positive correlation trend with the I-FFQ2 (R = 0.96, P < 0.05). We further explored the consistency of the two I-FFQs using a Bland-Altman plot. Bland-Altman analysis showed that the mean difference between the two I-FFQs' assessment results was 18.50 μg/d with an LOA ranging from -104.17 to 141.16 μg/d, and 4% (4 / 100) of data points fell outside the LOA (Figure 1B). The daily iodine intake of college students estimated by the I-FFQ was divided into 3 groups based on the recommended nutrient intake and tolerable upper intake level of iodine in the Chinese dietary guidelines. Kappa analysis of the two I-FFQs indicated high agreement (kappa = 0.781, P < 0.001; Table 1), suggesting good reliability between the two assessments.
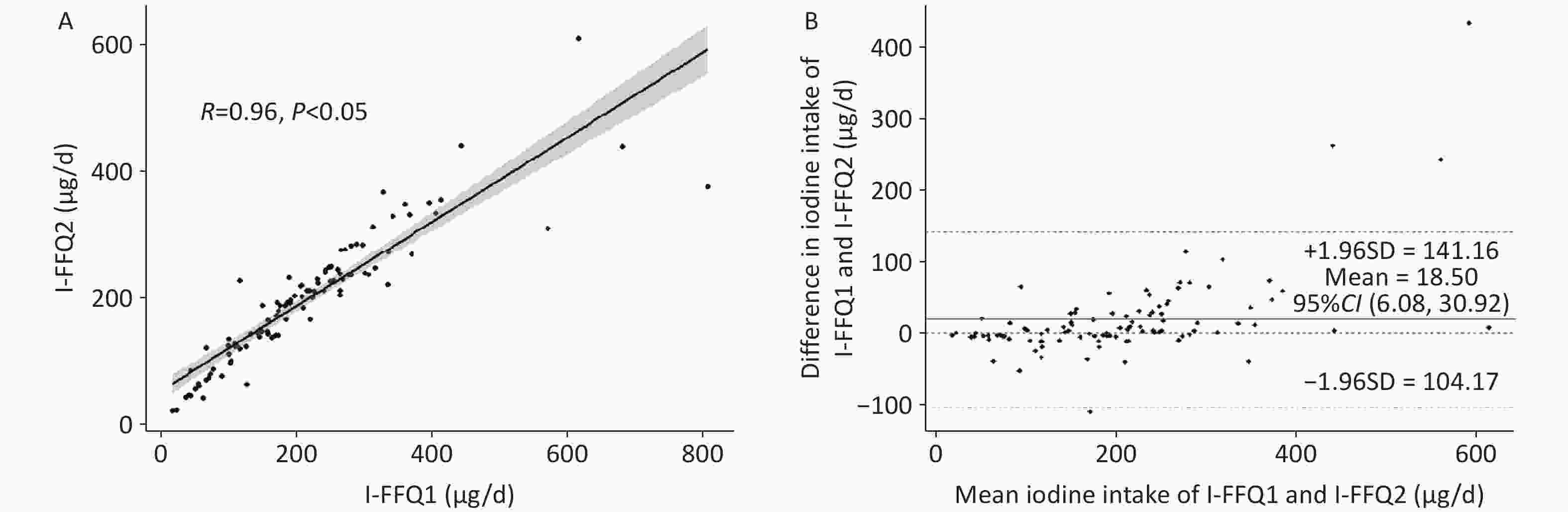
Figure 1. Iodine status of college students assessed twice by I-FFQ is consistent
Table 1. Kappa consistency tests of I-FFQs before and after one month in Chinese college students
Group Iodine intake from the I-FFQ after one month (μg/d) Total < 120 120–600 > 600 Iodine intake from the I-FFQ before one month (μg/d) < 120 21 6 0 27 120–600 1 69 0 70 > 600 0 2 1 3 Total 22 77 1 100 Note. I-FFQ, iodine-specific food frequency questionnaire. Kappa = 0.781, P < 0.001. Table 2 presented the adjusted associations between thyroid function changes and I-FFQ groups. In the model, iodine intake estimated by the I-FFQ was divided into 3 groups according to quantiles. The results of the binary logistic regression showed that when the iodine intake assessed by I-FFQ was at a relatively high level, the risk of goiter significantly increased. Specifically, compared to the control group, when the iodine intake assessed by I-FFQ was above the 80th percentile, the risk of goiter incidence increased by 2.18 times (odds ratio [OR]: 2.18, 95% confidence interval [CI]: 1.14-4.18); when it was above the 90th percentile, the risk increased by 2.58 times (OR: 2.58, 95% CI: 1.23-5.44); and when it was above the 95th percentile, the risk increased by 4.78 times (OR: 4.78, 95% CI: 2.03-11.28). These results indicate that the I-FFQ is a valuable tool for individualized iodine nutrition evaluation.
Table 2. Logistic regression analysis of thyroid function changes in the elderly by I-FFQ grouping
Variables I-FFQ, μg/d Model 1 Model 2 OR (95% CI) P OR (95% CI) P Goiter 20%–80% (ref) < 20% 1.80 (0.93,3.48) 0.291 1.77 (0.90,3.49) 0.290 > 80% 2.20 (1.18,4.12) 0.014 2.18 (1.14,4.18) 0.019 10%–90% (ref) < 10% 1.15 (0.48,2.80) 0.752 1.12 (0.45,2.79) 0.807 > 90% 2.25 (1.11,4.56) 0.024 2.58 (1.23,5.44) 0.012 5%–95% (ref) < 5% 1.16 (0.35,3.89) 0.810 1.36 (0.39,4.79) 0.629 > 95% 4.08 (1.85,8.98) < 0.001 4.78 (2.03,11.28) < 0.001 Thyroid dysfunction 20%–80% (ref) < 20% 1.16 (0.79,1.68) 0.451 1.17 (0.80,1.70) 0.424 > 80% 0.89 (0.62,1.27) 0.514 0.90 (0.62,1.29) 0.552 10%–90% (ref) < 10% 1.31 (0.79,2.16) 0.291 1.31 (0.80,2.17) 0.290 > 90% 0.90 (0.56,1.43) 0.647 0.91 (0.57,1.45) 0.680 5%–95% (ref) < 5% 1.61 (0.78,3.30) 0.198 1.61 (0.78,3.33) 0.195 > 95% 1.26 (0.64,2.49) 0.507 1.25 (0.63,2.47) 0.520 Note. Model 1: Unadjusted model; Model 2: Additionally adjusted for age, gender and BMI based on Model 1. I-FFQ, iodine-specific food frequency questionnaire. Gansu Province, located in northwest China, was historically an area with a high prevalence of iodine deficiency disease. Longxi County, situated in the southeastern part of Gansu Province and within Dingxi City, lies along the middle and upper reaches of the Wei River. To reduce the health effects of thyroid disorders, it is essential to increase the frequency of monitoring iodine levels among local residents. Therefore, an efficient and convenient tool for assessing iodine levels is crucial to ensuring the safety of local residents' iodine levels.
The unique geographical and climatic conditions of Longxi County have shaped local dietary habits, including a preference for hot and sour foods as well as noodles. Thus, the choice and number of FFQ food types for specific nutrients are important. In our study, we conducted a survey of local dietary habits and collected food samples for iodine content analysis. Using cluster analysis and considering the dietary frequency and dietary iodine concentration of local residents, an I-FFQ with 13 food item categories was developed.
In this study, the iodine intake of college students assessed by I-FFQ before and after a one-month interval was 194.11 μg/d and 197.67 μg/d, respectively. According to the Chinese Dietary Reference Intakes, the iodine intake of college students in Gansu was appropriate. Correlation, Bland-Altman, and Kappa analyses were used to evaluate the reliability of I-FFQ. The I-FFQ showed substantial agreement.
Our research shows that the estimated iodine intake calculated from the FFQ was much lower than that estimated from UIC. This might be because the dietary assessment by FFQ aims to measure the long-term average iodine intake from daily diet. Dietary assessment using FFQs largely depends on the participants' memory and perceptions[7]. As with all self-reporting dietary data, the present dietary assessment can be affected by an external bias caused by social desirability and memory lapses[8]. Conversely, UIC reflects recent iodine intake and is subject to significant daily variations.
Iodine malnutrition may impair the function of the thyroid gland in the human body. Laurberg et al.[9] study has shown that thyroid function is impaired in the elderly when iodine intake is high, which is consistent with our research results. Some studies have also reported no correlation between iodine intake level and thyroid autoantibody positivity[10]. In this study, this finding is also observed. This variation may occur because the study population represented diverse iodine nutritional backgrounds, and the iodine-deficient and excessive intake subgroups had limited sample sizes.
There were several limitations. Firstly, dietary assessments were not repeated. Secondly, FT4 levels were measured only in cases with abnormal TSH levels, thereby restricting the scope of observations and precluding a more comprehensive analysis. Lastly, the temporal differences between recent iodine intake (assessed via I-FFQ) and goiter incidence (a long-term indicator) were not fully accounted for in the analysis of their association. Consequently, while these results provide valuable insights, they do not establish direct causality. Nonetheless, the strength of this study lies in its verification of the applicability of the I-FFQ in Gansu Province for the first time. The combination of subjective (I-FFQ) and objective (biomarker) measures enhances the robustness of the study's findings.
In conclusion, the I‐FFQ can be used as a useful tool for assessing habitual iodine intake in the elderly in Gansu. The I‐FFQ demonstrated reasonable validity and good reproducibility. When assessing the iodine intake of the elderly in other regions of China, it is necessary to reformulate the local I-FFQ according to the dietary habits, which requires further investigation in future studies.
doi: 10.3967/bes2025.074
Validation and Reproducibility of an Iodine-Specific Food Frequency Questionnaire for Evaluating Dietary Iodine Intake in the Elderly Population of Gansu Province, China
-
Conceptualization: Wenxing Guo, Yanling Wang and Wanqi Zhang; Investigation: Qi Jin, Tao Wang, Meina Ji, Jizun Wang, Xing Ma, Xinyi Wang, Jiaqi Wang and Hexi Zhang; Writing- Original draft preparation: Qi Jin and Tao Wang; Writing- Reviewing and Editing: Wenxing Guo.
The authors declare that there are no conflicts of interests.
The study protocol was approved by the ethics committee of Tianjin Medical University (TMUHMEC2022013). All procedures performed in the studies were in accordance with the 1964 Helsinki Declaration and its later amendments.
&These authors contributed equally to this work.
注释:1) Authors’ Contributions: 2) Competing Interests: 3) Ethics: -
Figure 1. Iodine status of college students assessed twice by I-FFQ is consistent
(a) Spearman correlation between I-FFQ1 with the I-FFQ2. (b) Bland-Altman plot characterizes the deviation of the two I-FFQs. The solid red line represents the mean difference between the 2 I-FFQs (18.50 μg/d) and the red dotted lines represents the limits of agreements (LOA) corresponding to ± 1.96 SD (lower agreement: -104.17 μg/d, upper agreement: 141.16 μg/d). I-FFQ, iodine-specific food frequency questionnaire; SD, standard deviation.
Table 1. Kappa consistency tests of I-FFQs before and after one month in Chinese college students
Group Iodine intake from the I-FFQ after one month (μg/d) Total < 120 120–600 > 600 Iodine intake from the I-FFQ before one month (μg/d) < 120 21 6 0 27 120–600 1 69 0 70 > 600 0 2 1 3 Total 22 77 1 100 Note. I-FFQ, iodine-specific food frequency questionnaire. Kappa = 0.781, P < 0.001.  下载: 导出CSV
下载: 导出CSV
Table 2. Logistic regression analysis of thyroid function changes in the elderly by I-FFQ grouping
Variables I-FFQ, μg/d Model 1 Model 2 OR (95% CI) P OR (95% CI) P Goiter 20%–80% (ref) < 20% 1.80 (0.93,3.48) 0.291 1.77 (0.90,3.49) 0.290 > 80% 2.20 (1.18,4.12) 0.014 2.18 (1.14,4.18) 0.019 10%–90% (ref) < 10% 1.15 (0.48,2.80) 0.752 1.12 (0.45,2.79) 0.807 > 90% 2.25 (1.11,4.56) 0.024 2.58 (1.23,5.44) 0.012 5%–95% (ref) < 5% 1.16 (0.35,3.89) 0.810 1.36 (0.39,4.79) 0.629 > 95% 4.08 (1.85,8.98) < 0.001 4.78 (2.03,11.28) < 0.001 Thyroid dysfunction 20%–80% (ref) < 20% 1.16 (0.79,1.68) 0.451 1.17 (0.80,1.70) 0.424 > 80% 0.89 (0.62,1.27) 0.514 0.90 (0.62,1.29) 0.552 10%–90% (ref) < 10% 1.31 (0.79,2.16) 0.291 1.31 (0.80,2.17) 0.290 > 90% 0.90 (0.56,1.43) 0.647 0.91 (0.57,1.45) 0.680 5%–95% (ref) < 5% 1.61 (0.78,3.30) 0.198 1.61 (0.78,3.33) 0.195 > 95% 1.26 (0.64,2.49) 0.507 1.25 (0.63,2.47) 0.520 Note. Model 1: Unadjusted model; Model 2: Additionally adjusted for age, gender and BMI based on Model 1. I-FFQ, iodine-specific food frequency questionnaire.
下载: 导出CSV
-
[1] König F, Andersson M, Hotz K, et al. Ten repeat collections for urinary iodine from spot samples or 24-hour samples are needed to reliably estimate individual iodine status in women. J Nutr, 2011; 141, 2049−54. doi: 10.3945/jn.111.144071 [2] Zimmermann MB, Jooste PL, Pandav CS. Iodine-deficiency disorders. Lancet, 2008; 372, 1251−62. doi: 10.1016/S0140-6736(08)61005-3 [3] Satija A, Yu E, Willett WC, et al. Understanding nutritional epidemiology and its role in policy. Adv Nutr, 2015; 6, 5−18. doi: 10.3945/an.114.007492 [4] Ma YH, Tan J, Tan ZJ, et al. Validity and reliability of semiquantitative food frequency questionnaires for assessing nutrient intake among preschool children in northwest China. J Healthc Eng, 2022; 2022, 1677252. [5] Combet E, Lean MEJ. Validation of a short food frequency questionnaire specific for iodine in UK females of childbearing age. J Hum Nutr Diet, 2014; 27, 599−605. doi: 10.1111/jhn.12219 [6] Wang ZX. Retrospective Dietary Survey-Assisted Food Atlas Measurement. Nanjing: Jiangsu Phoenix Science & Technology Publishing House. 2021. (In Chinese) [7] Biró G, Hulshof KFAM, Ovesen L, et al. Selection of methodology to assess food intake. Eur J Clin Nutr, 2002; 56 Suppl 2, S25-32. [8] Althubaiti A. Information bias in health research: definition, pitfalls, and adjustment methods. J Multidiscip Healthc, 2016; 9, 211−7. [9] Laurberg P, Pedersen KM, Hreidarsson A, et al. Iodine intake and the pattern of thyroid disorders: a comparative epidemiological study of thyroid abnormalities in the elderly in Iceland and in Jutland, Denmark. J Clin Endocrinol Metab, 1998; 83, 765−9. doi: 10.1210/jcem.83.3.4624 [10] Nagata K, Takasu N, Akamine H, et al. Urinary iodine and thyroid antibodies in Okinawa, Yamagata, Hyogo, and Nagano, Japan: the differences in iodine intake do not affect thyroid antibody positivity. Endocr J, 1998; 45, 797−803. doi: 10.1507/endocrj.45.797 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 15
- HTML全文浏览量: 6
- PDF下载量: 1
- 被引次数: 0

 Quick Links
Quick Links