

 下载:
下载:

-
Mycoplasma pneumoniae is a major pathogen for community-acquired pneumonia (CAP). In children, it accounts for 10%–40% of inpatients with CAP[1-3]. Besides respiratory tract infections, pharyngitis, and CAP, M. pneumoniae also damages the nervous system, heart, kidney, and many other organs[4-6]. Macrolides and related antibiotics are the first-line treatment for respiratory infections caused by M. pneumoniae[7]. Since the 2000s, macrolide-resistant M. pneumoniae has spread rapidly worldwide, especially in East Asia[8-9]. As M. pneumoniae is a genetically homogeneous species[10], molecular typing is hampered. For a long time, polymerase chain reaction-restriction fragment length polymorphism analysis of the P1 gene has been the most common genotyping method. However, this method can only identify strains classified into two groups[10]. The multiple-locus variable-number tandem-repeat (VNTR) analysis (MLVA) is a molecular typing method recently applied to M. pneumoniae. MLVA is based on the variation in the copy number of tandemly repeated sequences, called VNTRs, found at different loci in the genome[10]. The MLVA method dramatically expands the typing scheme for M. pneumoniae[11], thereby providing a powerful tool for the surveillance and epidemiology of M. pneumoniae infections. M. pneumoniae outbreaks occur every 4 to 7 years[12,13]. However, the reason for the epidemic cycles of M. pneumoniae is inconclusive. Some researchers believe that it is related to shifts in M. pneumoniae groups[14,15]. In 2016, a global epidemic of M. pneumoniae occurred in Beijing[16,17]. This study aims to understand the prevalence and drug resistance of these patients with M. pneumoniae.
-
This study was conducted from January to December 2016, in Beijing, China. Samples were collected from Peking University Third Hospital, Beijing, China; Beijing Chao-yang Hospital, Capital Medical University, Beijing, China; China Mei-tan General Hospital, Beijing, China; and Civil Aviation General Hospital, Beijing, China. The inclusion criteria were as follows: (a) outpatients and inpatients with fever, cough, sore throat, or other symptoms of respiratory tract infection; (b) patients with a course of 1 to 7 days; (c) white blood cell count of 4.0–12.0 × 109/L. The exclusion criteria were as follows: (a) parent or child who refused to be tested, and (b) bacterial or viral infection with a precise etiological diagnosis. The outpatient samples were collected from China Mei-tan General Hospital and Civil Aviation General Hospital. In contrast, the inpatient samples were collected from Peking University Third Hospital and Beijing Chao-yang Hospital.
-
Domain V of the 23S rRNA gene was amplified by polymerase chain reaction (PCR) using specific primers (forward, 5′-GACACCCGTTAGGCGCAA-3'; reverse, 5′-CTGGATAACAGTTACCAATTAGAACAGC-3')[18]. PCR was performed in a total volume of 20 µL containing 0.3 µL of forward and reverse primers, 10 µL of 10× buffer UltraSYBR Mixture (CW2601, CoWin Biosciences, Jiangsu, China), 2 µL of genomic DNA, and 7.4 µL of ddH2O. The reaction mixture was subjected to denaturation, annealing, and elongation for 2 min at 50 ℃, 10 min at 95 ℃, 15 s at 95 ℃, and 60 s at 60 ℃ for 40 PCR cycles. These steps were followed by an extension step of 15 s at 95 ℃, 60 s at 60 ℃, and 15 s at 95 ℃. PCR product sequencing was completed by Biotechnology (Shanghai) Co., Ltd, China. The sequencing results were compared with BioEdit software and the standard strain sequence of M. pneumoniae recorded on the National Center for Biotechnology Information.
-
The throat swab and bronchoalveolar lavage fluid specimens were inoculated in M. pneumoniae liquid medium, mixed evenly, and placed in an incubator at 37 °C with 5% CO2 for culture[19]. M. pneumoniae growth caused a decrease in the medium's pH that was indicated by a color change (from red to yellow)[19]. The preparation method and culture medium composition was as described in reference 19.
-
DNA extraction from the respiratory specimens was performed using the universal genomic DNA Kit (CoWin Biosciences, Jiangsu, China) following the manufacturer's instructions.
-
The minimum inhibitory concentrations (MICs) of four antibiotics: erythromycin, azithromycin, levofloxacin, and tetracycline, were determined via microdilution methods[20]. Specific methods followed the procedures mentioned in reference 20. Erythromycin, azithromycin, levofloxacin, and tetracycline were purchased from the National Institute for the Control of Pharmaceutical and Biological Products. The MIC breakpoint was according to the latest version of CSLI M43-A[21]. M. pneumoniae reference strains M129 (ATCC29342) and FH (ATCC15531) were used as macrolide-susceptible controls.
-
Primers and the PCR amplification method used were as described in the study by Dumke et al.[10]. The determination of VNTR numbers and nomenclature method followed those described previously by Chalker et al.[22].
-
A total of 535 samples were collected. Of all samples, 265 cases were collected from China Mei-tan General Hospital, 112 cases were collected from Civil Aviation General Hospital, 88 cases were collected from Peking University Third Hospital, and 70 cases were collected from Beijing Chao-yang Hospital. Of all samples, 523 cases (523/535, 97.76%) were throat swab specimens, and 12 cases (12/535, 2.24%) were bronchoalveolar lavage fluid specimens. All bronchoalveolar lavage fluid specimens were collected from Peking University Third Hospital in December 2016 (Table 1).
Table 1. Sample collection
Category Outpatient samples Inpatient samples China Mei-tan
General HospitalCivil Aviation General Hospital Beijing Chao-yang Hospital, Capital Medical University Peking University Third Hospital Throat swabs 265 112 70 76 Bronchoalveolar lavage fluid 0 0 0 12* Total 265 112 70 88 Note. *All bronchoalveolar lavage fluid specimens were collected from Peking University Third Hospital in December 2016. -
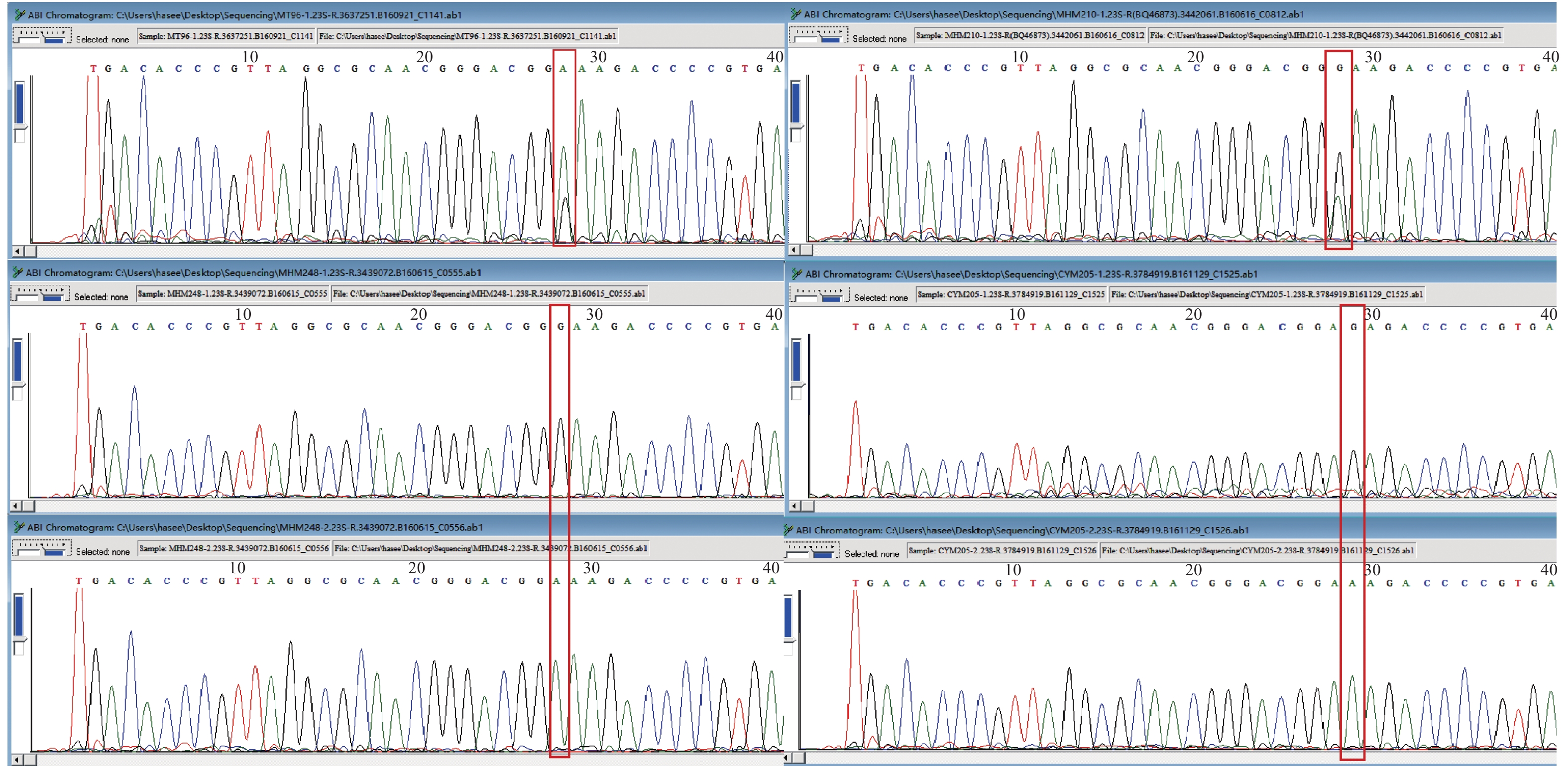
Table 1 shows that of 535 samples, 214 were detected positive by real-time PCR, and the detection rate was 40%. Furthermore, 68 samples (68/214, 31.78%) had no mutant in domain V of the 23S rRNA gene and were sensitive bacteria. Also, 142 samples (142/214, 66.36%) harbored a mutation in domain V of the 23S rRNA gene. Among these, 134 cases harbored an A2063G mutation. However, seven cases harbored an A2064G mutation, and in one case, both A2063 and A2064G mutations were detected (Figure 1). Four samples (4/214, 2%) were mixed with sensitive M. pneumoniae and macrolide-resistant M. pneumoniae. Among these, three cases (Figure 2) were mixed with sensitive and A2063G mutant M. pneumoniae, and one (Figure 2) was mixed with sensitive and A2064G mutant M. pneumoniae.

Figure 1. CYM188 A2063G A2064G double mutations
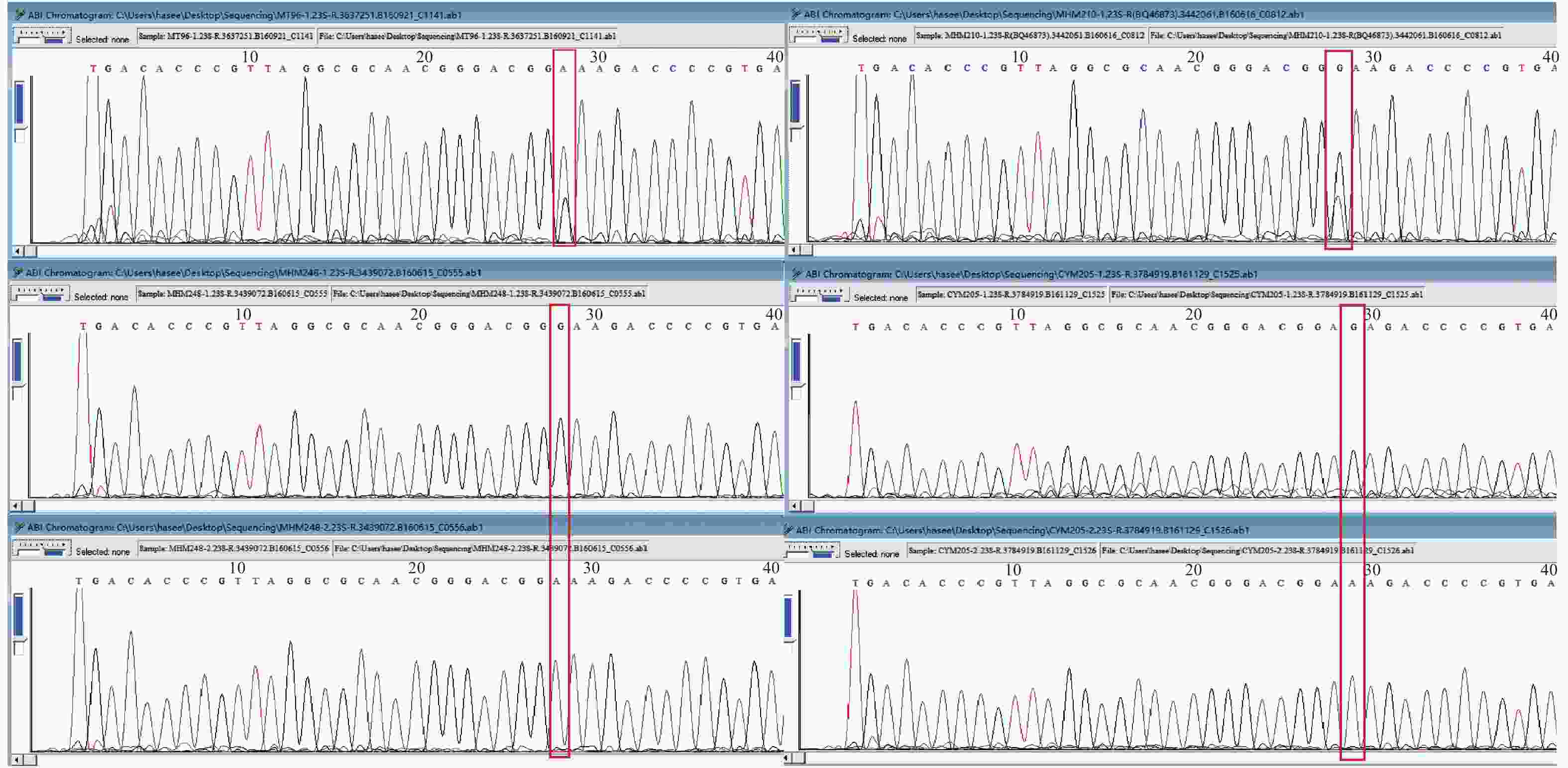
Figure 2. Gene Sequencing results of strains MT96, MHM210, MHM248, and CYM205.
A total of 377 samples were collected from outpatients, whereas 131 samples (131/377, 34.75%) were detected positive by real-time PCR. Moreover, 50 samples were nonmutated M. pneumoniae, 78 samples harbored a mutation in domain V of the 23S rRNA gene (of which 71 harbored an A2063G mutation and seven harbored an A2064G mutation), and in three cases, macrolide-susceptible as well as A2063G macrolide-resistant strains were detected (Table 2). Of the 158 samples collected from inpatients, 83 (83/158, 52.53%) were detected positive by real-time PCR. Also, 18 samples were nonmutated M. pneumoniae, 64 harbored mutation in domain V of the 23S rRNA gene (63 harbored an A2063G mutation, and one had both A2063G and A2064G mutations), whereas no mutated and A2064G mutated M. pneumoniae were detected in one sample. The detection rate of outpatient samples (131/377, 34.75%) was lower than that of inpatient samples (83/158, 52.53%), and the difference was statistically significant (P < 0.0001). The 23S rRNA gene mutation rate of outpatient samples (78/131, 59.54%) was significantly lower than that of inpatient samples (64/83, 77.11%), and the difference was statistically significant (P = 0.001)
Table 2. Detection of M. pneumoniae and 23S rRNA gene mutation
Category Outpatient Inpatient Total P Positive No mutated 50 18 68 0.001 Mutateda 78 64 142 0.001 Mixedb 3 1 4 Negative 246 75 321 < 0.0001 Total 377 158 535 Note. aIncluding A2063G and A2064G mutations; A2063G and A2064G both mutated.
bIncluding the mixture of no mutant and A2063G mutant M. pneumoniae and the mixture of no mutant and A2064G mutant M. pneumoniae. -
A total of 81 M. pneumoniae isolates were obtained from 535 patients; the detection rate was 15.14% (81/535). Among these, 12 isolates (12/81, 14.81%) were no mutant strains, and 69 isolates (69/81, 85.19%) were A2063G mutant strains (Table 3). All A2064G mutant samples, mixed samples, and double mutant samples could not be cultured. The growth rate of 23S rRNA gene mutant M. pneumoniae collected from inpatients was significantly higher than that of the 23S rRNA gene mutant M. pneumoniae collected from outpatients, no mutant samples from outpatients or inpatients; the differences were statistically significant (P < 0.0001). However, the growth rate of no mutant M. pneumoniae showed no difference between outpatients (9/50, 18%) and inpatients (3/18, 16.67%). Finally, the growth rate of no mutant samples (9/50, 18%) and mutant samples (19/78, 24.35%) collected from outpatients showed no statistically significant difference (P = 0.016).
Table 3. Cultures of outpatient and inpatient samples
Category Outpatient Inpatient No mutant 23S rRNA mutationa Mixedb No mutant 23S rRNA mutationa Mixedb PCR 50 78 3 18 64 1 Cultures 9 19 0 3 50 0 Growth Rate 18% 24.36% 0 16.67% 78.13% 0 Note. aIncluding A2063G and A2064G mutations; A2063G and A2064G both mutated.
bIncluding the mixture of no mutant and A2063G mutant M. pneumoniae and the mixture of no mutant and A2064G mutant M. pneumoniae. -
A total of 67 strains were randomly selected from all 81 isolates to test the MICs of erythromycin, azithromycin, levofloxacin, and tetracycline. The MIC of erythromycin for no mutant M. pneumoniae strains was 0.002–0.003 µg/mL. In contrast, the MIC for A2063G mutant M. pneumoniae was 8–1,024 µg/mL; the MIC90 was 512 µg/mL, and the MIC50 was 256 µg/mL. All erythromycin-resistant isolates also showed resistance to azithromycin. The MIC of azithromycin for no mutant M. pneumoniae strains was 0.0005–0.004 µg/mL, whereas the MIC for the A2063G mutant M. pneumoniae was 8–512 µg/mL; the MIC90 was 256 µg/mL, and the MIC50 was 128 µg/mL. All 67 selected isolates in this study were susceptible to tetracycline and levofloxacin.
-
MLVA genotyping was performed on 65 A2063G mutation samples and nine no mutant samples (Table 4). Except for one A2063G mutation sample, the remaining 73 samples were successfully typed, including ten cases with type 3-5-6-2 and 63 were type 4-5-7-2. Among the type 3-5-6-2 samples, three had an A2063G mutation, and seven had no mutant. In contrast, among the type 4-5-7-2 samples, 61 had the A2063G mutation, and two had no mutant.
Table 4. MLVA genotyping and the mutation
Category 3-5-6-2 4-5-7-2 Failed Total No mutant 7 2 1 10 A2063G mutation 3 61 0 64 Total 10 63 1 74 -
In 2001, the first macrolide-resistant M. pneumoniae strain was isolated from clinical samples in Japan[23,24]. Since then, macrolide-resistant strains of M. pneumoniae have been isolated in many countries[25-30]. East Asia has the highest resistance rate of M. pneumoniae around the world[8,31]. According to reports, the macrolide resistance rate of M. pneumoniae is more than 90%[32]. However, in Europe and the United States, it is much lower[33-36]. The macrolide resistance rate of M. pneumoniae in Beijing was reported previously[37]. In 2014, it was 69.21%, which was significantly lower than it was in the past. However, in 2016, the detection rate of M. pneumoniae (40%) and the macrolide resistance rate of M. pneumoniae (66%) both decreased compared with these rates in 2014. Regarding the macrolide resistance rate of M. pneumoniae, Beijing remains the leader compared with the macrolide resistance rate of M. pneumoniae in Taiwan, China (23.89%), Osaka, Japan (42.68%), or any other country or region[8,38].
The mutation of A → G in the 2063 or 2064 gene of the 23S rRNA V region is the primary mechanism of macrolide resistance in M. pneumoniae[35]. The A2063G mutation is the most common in macrolide-resistant M. pneumoniae, whereas the A2064G mutation and other mutations were relatively few[24,30]. In this study, the A2063G mutation was the primary mutation, accounting for 94.37%. The A2064G mutation accounted for 4.93%; no other mutations such as 2067 were found. However, in one clinical sample, both A2063G and A2064G mutations were detected; unfortunately, this sample could not be cultured. All seven A2064G mutation samples were collected from outpatients, implying that A2064G mutant strains might cause a mild infection. However, further research is needed to confirm the results because of the study's small sample size. Besides this, the present study found mixed infections of no mutant and mutant strains in the four samples. At first, mixed infections were reported as case reports[24,37,38]. In these reports, patients were first infected by the macrolide-sensitive M. pneumoniae. After a period of treatment (usually more than one week), the 23S rRNA gene mutation was found. However, whether these four patients had received macrolide antibiotics before sample collection was not confirmed. Therefore, these patients might have developed macrolide resistance during treatment, or mixed strains might have infected them. More research is needed in this regard.
Samples from outpatients and inpatients were significantly different in several ways. First, the detection rate of outpatient samples (34.75%) was significantly lower than inpatient samples (52.53%). This difference indicated that M. pneumoniae infection was more common in inpatients. Second, the macrolide resistance rate of M. pneumoniae in outpatients was 59.54%, which was significantly lower than fin inpatients (77.11%). The reason for this was probably because of the following factors: (1) macrolide-resistant M. pneumoniae might have caused a relatively serious infection, leading to the hospitalization of children. (2) It might also be related to the course of the infection. Inpatients usually had a longer course of infection compared with outpatients and might have been treated with macrolide antibiotics before hospitalization. Before a hospitalization, macrolide-sensitive M. pneumoniae was eliminated during treatment, whereas macrolide-resistant M. pneumoniae survived. Also, macrolide-sensitive M. pneumoniae might have developed mutations during treatment. Both situations could lead to an increase in the macrolide resistance rate in inpatients. Third, a specific difference was observed between outpatient samples and inpatient samples in culture. Compared with samples collected from outpatients, whether they had had the 23S rRNA mutation or not, and the nonmutation samples collected from inpatients, the A2063G mutation samples collected from inpatients were easier to culture, and the difference was statistically significant. However, the growth rate of nonmutation inpatient samples, nonmutation outpatient samples, and 23S rRNA mutation outpatient samples showed no statistically significant difference. This difference might be related to the fact that inpatients had relatively serious diseases, with more M. pneumoniae in their oropharynx. When taking samples, the inpatient samples had more pathogens. Further research is needed to identify other influencing factors. All seven A2064G mutant strains could not be cultured. Therefore, it was speculated that the A2064G mutant strains might be more difficult to culture compared with the nonmutated strains and the A2063G mutant strains. The reason remains unknown, requiring further exploration.
No strains resistant to tetracycline or levofloxacin were found in this study. Whether it is necessary to use tetracycline and levofloxacin in children infected with macrolide-sensitive M. pneumoniae remains debatable[8]. However, it is undeniable that these two antibiotics still have good in vitro activity against M. pneumoniae. While treating macrolide-resistant M. pneumoniae, the aforementioned two antibiotics are usually used as an alternative treatment plan. In many CAP guidelines for adults[39,40], tetracyclines and quinolones have replaced macrolides as first-line treatments. However, because of their low MIC and the safety in young children, macrolides remain the first-line treatment of M. pneumoniae pneumonia (MPP), even in areas with a high macrolide resistance rate. The guiding principles for treating MPP by the Committee of Japanese Society of Mycoplasmology in 2014[41] still recommend macrolides as the first-line drug of choice for treating MPP. However, the efficacy of macrolides should be assessed with relatively high accuracy by the presence or absence of effervescence within 48–72 h after the initiation of macrolide treatment. Tetracyclines are relatively contraindicated in children younger than eight years of age. When using antimicrobial agents other than macrolides is considered necessary for the treatment of MPP in this age group, tosufloxacin should be used. In recent years, the macrolide resistance rate in Japan has decreased significantly; reports show that the current macrolide resistance rate of M. pneumoniae is less than 30%[16]. Macrolides have played a vital role in controlling the macrolide resistance rate. In China, the guidelines recommend macrolides as the first-line drug of choice; tetracyclines are recommended only for children older than eight years of age[42]. However, China's guidelines did not mention the efficacy assessment of macrolides and tosufloxacin; hence, they never appeared on the market. The use of quinolone antibiotics among minors is prohibited by law in China. In 2017, the Guangdong Pharmaceutical Association formulated the 'Expert consensus on the application of fluoroquinolone antibacterial drugs in children',[43] that submitted some principles and requirements for using quinolone antibiotics in children. However, the expert consensus also emphasizes that quinolone antibiotics should not be used as routine medicines to treat childhood infections.
In recent years, the MLVA typing method has been widely used in the study of M. pneumoniae, thus providing a new tool for the molecular epidemiology of M. pneumoniae. It is a typing system with high discriminatory power[10]. Since the establishment of MLVA typing of M. pneumoniae, the relationship between the MLVA type of M. pneumoniae and macrolide resistance has increased the interest of many researchers. Some studies[31,44-46] analyzed the correlation between MLVA typing and macrolide resistance. A few researchers found an association between MLVA type 4-5-7-2 and macrolide resistance, whereas type 3-5-6-2 might be related to macrolide susceptibility[31,44]. The present study had similar conclusions. However, does this correlation exist? First, when the MLVA typing method was established, Dumke et al.[10] selected five repetitive sequences, namely MPN1, MPN13, MPN14, MPN15, and MPN16. Subsequently, the MPN1 sequence was abandoned because of its instability[22,47]. MPN13, MPN14, MPN15, and MPN16 were retained. All four retained VNTRs were located in open reading frames, MPN14, MPN15, and MPN16 encoded hypothetical proteins, and MPN13 was located in the intergenic region[10]. These VNTRs were not related to the primary mechanism of macrolide resistance in the gene sequence. Second, studies in areas with a low macrolide resistance rate, such as Cuba and Finland, do not support this conclusion[30,36]. The studies that supported this conclusion mostly came from East Asia, where the macrolide resistance rate was relatively high[31,44,45,46]. Third, in most studies, type 4-5-7-2 was the most common[36], followed by 3-5-6-2. However, the macrolide resistance rate in these areas varied greatly, from 0% to 87%[36,48]. If type 4-5-7-2 is related to macrolide resistance, then why is the macrolide resistance rate of M. pneumoniae in Europe[35,49] and North America[33,34], which is also dominated by the 4-5-7-2 subtype, much lower than that in East Asia[18,25,50]. Therefore, whether a correlation exists between MLVA type and macrolide resistance needs further investigation. We believed that no relationship exists between MLVA type and macrolide resistance. The macrolide resistance rate of M. pneumoniae in East Asia was very high, and so was the percentage of type 4-5-7-2. The high macrolide resistance rate of M. pneumoniae in East Asia and the high percentage of MLVA type 4-5-7-2 were two independent phenomena that co-occurred. Therefore, it was concluded that the two had a statistical correlation rather than an essential correlation.
-
In 2016, the detection rate of M. pneumoniae among children in Beijing was 40%, and the macrolide resistance rate was 66%. A specific decrease was found in the rate of macrolide resistance, but it remains at a high level. The primary resistance mechanism is an A2063G mutation in the 23S rRNA V region, whereas the A2064G mutation is rare. The detection rate and macrolide resistance rate of outpatients are lower than those of inpatients. At the same time, the macrolide-resistant M. pneumoniae from inpatients are easier to isolate and culture. Its growth rate is significantly different from that of macrolide-sensitive M. pneumoniae of outpatients and inpatients and macrolide-resistant M. pneumoniae of outpatients. This might be related to the severity and duration of infection. No strains resistant to tetracycline or levofloxacin were found in vitro. The A2063G M. pneumoniae mutant has high levels of resistance to erythromycin and azithromycin. The primary type of MLVA is 4-5-7-2, followed by 3-5-6-2; no other types have been detected.
-
None.
-
We thank International Science Editing (
http://www.internationalscienceediting.com ) for editing this manuscript.
doi: 10.3967/bes2020.125
Mycoplasma pneumoniae Macrolide Resistance and MLVA Typing in Children in Beijing, China, in 2016: Is It Relevant?
-
Abstract:
Objective The aim of this study is to investigate the macrolide resistance rate and molecular type with multiple-locus variable-number tandem-repeat analysis (MLVA) of Mycoplasma pneumoniae of Beijing in 2016 in pediatric patients. Methods Real-time quantitative polymerase chain reaction (PCR) was used to identify M. pneumoniae, and MLVA was performed. The domain V of the 23S rRNA was sequenced to detect macrolide-resistant point mutations. We also investigated the activities of antibiotics against M. pneumoniae isolates in vitro. Results The PCR detection rate of M. pneumoniae in children in Beijing was 40%, and the macrolide resistance rate was 66%. The A2063G mutation in the 23S rRNA V region is the dominant mutation (137/146, 93.84%), whereas the A2064G mutation is rare (9/146, 6.16%). Seventy-three samples were typed successfully by MLVA typing, including 86.3% (63/73) were MLVA type 4-5-7-2, and 13.7% (10/73) were MLVA type 3-5-6-2. No other types were found. No strains were resistant to levofloxacin or tetracycline. Conclusion In 2016, a specific decrease in the macrolide resistance rate occurred in Beijing. The detection rate and macrolide resistance rate of outpatients are lower than those of inpatients. The A2063G mutants M. pneumoniae have high levels of resistance to erythromycin and azithromycin. The primary MLVA type is 4-5-7-2, followed by 3-5-6-2. No other MLVA types were detected. No strains resistant to tetracycline or levofloxacin were found in vitro. -
Key words:
- Culture /
- Macrolide resistance /
- MLVA type /
- Mycoplasma pneumoniae
注释: -
Table 1. Sample collection
Category Outpatient samples Inpatient samples China Mei-tan
General HospitalCivil Aviation General Hospital Beijing Chao-yang Hospital, Capital Medical University Peking University Third Hospital Throat swabs 265 112 70 76 Bronchoalveolar lavage fluid 0 0 0 12* Total 265 112 70 88 Note. *All bronchoalveolar lavage fluid specimens were collected from Peking University Third Hospital in December 2016.  下载: 导出CSV
下载: 导出CSV
Table 2. Detection of M. pneumoniae and 23S rRNA gene mutation
Category Outpatient Inpatient Total P Positive No mutated 50 18 68 0.001 Mutateda 78 64 142 0.001 Mixedb 3 1 4 Negative 246 75 321 < 0.0001 Total 377 158 535 Note. aIncluding A2063G and A2064G mutations; A2063G and A2064G both mutated.
bIncluding the mixture of no mutant and A2063G mutant M. pneumoniae and the mixture of no mutant and A2064G mutant M. pneumoniae.
下载: 导出CSV
Table 3. Cultures of outpatient and inpatient samples
Category Outpatient Inpatient No mutant 23S rRNA mutationa Mixedb No mutant 23S rRNA mutationa Mixedb PCR 50 78 3 18 64 1 Cultures 9 19 0 3 50 0 Growth Rate 18% 24.36% 0 16.67% 78.13% 0 Note. aIncluding A2063G and A2064G mutations; A2063G and A2064G both mutated.
bIncluding the mixture of no mutant and A2063G mutant M. pneumoniae and the mixture of no mutant and A2064G mutant M. pneumoniae.
下载: 导出CSV
Table 4. MLVA genotyping and the mutation
Category 3-5-6-2 4-5-7-2 Failed Total No mutant 7 2 1 10 A2063G mutation 3 61 0 64 Total 10 63 1 74
下载: 导出CSV
-
[1] Wang, K, Gill P, Perera R, et al. Clinical symptoms and signs for the diagnosis of Mycoplasma pneumoniae in children and adolescents with community-acquired pneumonia. Cochrane Database Syst Rev, 2012; 10, CD009175. [2] Jain S, Williams DJ, Arnold SR, et al. Community-Acquired Pneumonia Requiring Hospitalization among U.S. Children. N Engl J Med, 2015; 372, 835−45. [3] Liu WK, Liu Q, Chen DH, et al. Epidemiology of Acute Respiratory Infections in Children in Guangzhou: A Three-Year Study. PLoS One, 2014; 9, e96674. [4] Yang TI, Chang TH, Lu CY, et al. Mycoplasma pneumoniae in pediatric patients: Do macrolide-resistance and/or delayed treatment matter? J Microbiol Immunol Infect, 2019; 52, 329−35. [5] Curtiss, P, Melnick L, Sicco KL, et al. Mycoplasma pneumoniae, more than a lung disease. Dermatol Online J, 2018; 24, 13030/qt8w993185. [6] Ma LD, Chen B, Dong Y, et al. Rapid mycoplasma culture for the early diagnosis of Mycoplasma pneumoniae infection. J Clin Lab Anal, 2010; 24, 224−9. [7] Cécile Bébéar, Sabine Pereyre, Olivia Peuchant. Mycoplasma pneumoniae: susceptibility and resistance to antibiotics. Future Microbiology, 2011; 6, 423−31. [8] Yang HJ. Benefits and risks of therapeutic alternatives for macrolide resistant Mycoplasma pneumoniae pneumonia in children. Korean J Pediatr, 2019; 62, 199−205. [9] Kawai Y, Miyashita N, Kubo M, et al. Nationwide Surveillance of Macrolide-Resistant Mycoplasma pneumoniae Infection in Pediatric Patients. Antimicrob Agents Chemother, 2013; 57, 4046−9. [10] Dégrange S, Cazanave C, Charron A, et al. Development of Multiple-Locus Variable-Number Tandem-Repeat Analysis for Molecular Typing of Mycoplasma pneumoniae. J Clin Microbiol, 2009; 47, 914−23. [11] Waites KB, Xiao L, Liu Y, et al. Mycoplasma pneumoniae from the Respiratory Tract and Beyond. Clin Microbiol Rev, 2017; 30, 747−809. [12] Taylor-Robinson D. Infections due to species of Mycoplasma and Ureaplasma: an update. Clin Infect Dis, 1996; 23, 671−82. [13] Diaz MH, Winchell JM. Winchell, The Evolution of Advanced Molecular Diagnostics for the Detection and Characterization of Mycoplasma pneumoniae. Front Microbiol, 2016; 7, 232. [14] Sasaki T, Kenri T, Okazaki N, et al. Epidemiological study of Mycoplasma pneumoniae infections in japan based on PCR-restriction fragment length polymorphism of the P1 cytadhesin gene. J Clin Microbiol, 1996; 34, 447−9. [15] Kenri T, Okazaki N, Yamazaki T, et al. Genotyping analysis of Mycoplasma pneumoniae clinical strains in Japan between 1995 and 2005: type shift phenomenon of M. pneumoniae clinical strains. J Med Microbiol, 2008; 57, 469−75. [16] Oishi T, Takahashi K, Wakabayashi S, et al. Comparing Antimicrobial Susceptibilities among Mycoplasma pneumoniae Isolates from Pediatric Patients in Japan between Two Recent Epidemic Periods. Antimicrob Agents Chemother, 2019; 63, e02517−18. [17] Katsukawa C, Kenri T, Shibayama K, et al. Genetic characterization of Mycoplasma pneumoniae isolated in Osaka between 2011 and 2017: Decreased detection rate of macrolide-resistance and increase of p1 gene type 2 lineage strains. PLoS One, 2019; 14, e0209938. [18] Guo DX, Hu WJ, Li D, et al. Development of real-time fluorescence quantitative PCR for the detection of Mycoplasma pneumoniae. Infectious Disease Information, 2016; 29, 52−6. (In Chinese) [19] Liu X, Jiang Y, Chen XG, et al. Drug Resistance Mechanisms of Mycoplasma pneumoniae to Macrolide Antibiotics. Biomed Res Int, 2014; 2014, 320801. [20] Tian XJ, Dong YQ, Dong XP, et al. P1 gene of Mycoplasma pneumoniae in clinical isolates collected in Beijing in 2010 and relationship between genotyping and macrolide resistance. Chin Med J (Engl), 2013; 126, 3944−8. [21] Waites KB, Bade DJ, Bébéar C, et al. Methods for Antimicrobial Susceptibility Testing for Human Mycoplasmas; Approved Guideline. CLSI Standards: Guidelines for Health Care Excellence. 2011, Wayne (PA): Clinical and Laboratory Standards Institute. Report No.: M43-A. [22] Chalker VJ, Pereyre S, Dumke R, et al. International mycoplasma pneumoniae typing study: interpretation of m. pneumoniae multilocus variable-number tandem-repeat analysis. New Microbes New Infect, 2015; 7, 37−40. [23] Okazaki N, Narita M, Yamada S, et al. Characteristics of macrolide-resistant Mycoplasma pneumoniae strains isolated from patients and induced with erythromycin in vitro. Microbiol Immunol, 2001; 45, 617−20. [24] Dumke R, Stolz S, Jacobs E, et al. Molecular characterization of macrolide resistance of a Mycoplasma pneumoniae strain that developed during therapy of a patient with pneumonia. Int J Infect Dis, 2014; 29, 197−9. [25] Xin DL, MI ZH, Han X, et al. Molecular mechanisms of erythromycin resistance in mycoplasma pneumonia. Journal of applied clinical pediatrics, 2005; 20, 666−7. (In Chinese) [26] Pereyre S, Charron A, Renaudin H, et al. First report of macrolide-resistant strains and description of a novel nucleotide sequence variation in the P1 adhesin gene in Mycoplasma pneumoniae clinical strains isolated in France over 12 years. J Clin Microbiol, 2007; 45, 3534−9. [27] Dumke R, Von BH, Lück PC, et al. Occurrence of macrolide-resistant Mycoplasma pneumoniae strains in Germany. Clin Microbiol Infect, 2010; 16, 613−6. doi: 10.1111/j.1469-0691.2009.02968.x [28] Almasri M, Diza E, Papa A, et al. Mycoplasma pneumoniae respiratory tract infections among Greek children. Hippokratia, 2011; 15, 147−52. [29] Maffeis L, Dilena R, Guez S, et al. Pseudotumour cerebri associated with mycoplasma pneumoniae infection and treatment with levofloxacin: a case report. BMC Pediatr, 2019; 19, 4. [30] Rodriguez N, Mondeja B, Sardiñas R, et al. First detection and characterization of macrolide-resistant Mycoplasma pneumoniae strains in Cuba. Int J Infect Dis, 2019; 80, 115−7. [31] Lu CY, Yen TY, Chang LY. Multiple-locus variable-number tandem-repeat analysis (MLVA) of macrolide-susceptible and -resistant Mycoplasma pneumoniae in children in Taiwan. J Formos Med Assoc, 2020; 119, 1539−45. [32] Liu Y, Ye X, Zhang H, et al. Characterization of macrolide resistance in Mycoplasma pneumoniae isolated from children in Shanghai, China. Diagn Microbiol Infect Dis, 2010; 67, 355−8. (In Chinese) [33] Diaz MH, Benitez AJ, Cross KE, et al. Molecular detection and characterization of Mycoplasma pneumoniae among patients hospitalized with community-acquired pneumonia in the United States. Open Forum Infect Dis, 2015; 2, ofv106. [34] Diaz MH, Benitez AJ, Winchell JM. Investigations of Mycoplasma pneumoniae infections in the United States: trends in molecular typing and macrolide resistance from 2006 to 2013. J Clin Microbiol, 2015; 53, 124−30. [35] Pereyre S, Goret J, Bébéar C. Mycoplasma pneumoniae: Current knowledge on macrolide resistance and treatment. Front Microbiol, 2016; 7, 974. [36] Satu K, Mirja P, Kati H, et al. Mycoplasma Pneumoniae Outbreak, Southeastern Finland, 2017-2018: Molecular Epidemiology and Laboratory Diagnostic Lessons. Eur J Clin Microbiol Infect Dis, 2019; 38, 1867−71. [37] Itagaki T, Suzuki Y, Seto J, et al. Two cases of macrolide resistance in Mycoplasma pneumoniae acquired during the treatment period. J Antimicrob Chemother, 2013; 68, 724−5. [38] Cardinale F, Chironna M, Dumke R, et al. Macrolide-resistant mycoplasma pneumoniae in paediatric pneumonia. Eur Respir J, 2011; 37, 1522−4. [39] Chou CC, Shen CF, Chen SJ, et al. Recommendations and guidelines for the treatment of pneumonia in Taiwan. J Microbiol Immunol Infect, 2019; 52, 172−99. (In Chinese) [40] Infectious Diseases Group, Respiratory Disease Branch of Chinese Medical Association. Expert consensus on diagnosis and treatment of adult Mycoplasma pneumoniae pneumonia. Chinese Journal of Tuberculosis and Respiratory Diseases, 2010; 33, 643−5. (In Chinese) doi: 10.3760/cma.j.issn.1001-0939.2010.09.002 [41] The committee of Japanese Society of Mycoplasmology. Guiding principles for treating Mycoplasma pneumoniae pneumonia. 5(23), 2014. (In Japanese) [42] Respiratory Branch of Chinese Pediatric Society of Chinese Medical Association, Editorial Board of Chinese Journal of Applied Clinical Pediatrics. Expert consensus on diagnosis and treatment of mycoplasma pneumoniae pneumonia in children (2015). Chinese Journal of Applied Clinical Pediatrics.30(), 2015, 09.1304-8. (In Chinese) [43] Guangdong Pharmaceutical Association. Expert consensus on the application of fluoroquinolone antibacterial drugs in children. Pharmacy Today, 2018.01.1-10. Doi:10.12048/j.issn.1674-229X.2018.01.001.(In Chinese) [44] Yan C, Sun H, Lee S, et al. Comparison of Molecular Characteristics of Mycoplasma pneumoniae Specimens Collected from the United States and China. J Clin Microbiol, 2015; 53, 3891−3. [45] Suzuki Y, Seto J, Shimotai Y, et al. Multiple-Locus Variable-Number Tandem-Repeat Analysis of Mycoplasma pneumoniae Isolates between 2004 and 2014 in Yamagata, Japan: Change in Molecular Characteristics during an 11-year Period. Jpn J Infect Dis, 2017; 70, 642−6. [46] Qu J, Chen S, Bao F, et al. Molecular characterization and analysis of Mycoplasma pneumoniae among patients of all ages with community-acquired pneumonia during an epidemic in China. Int J Infect Dis, 2019; 83, 26−31. [47] Benitez AJ, Diaz MH, Wolff BJ, et al. Multilocus variable-number tandem-repeat analysis of Mycoplasma pneumoniae clinical isolates from 1962 to the present: a retrospective study. J Clin Microbiol, 2012; 50, 3620−6. [48] Sun H, Xue G, Yan C, et al. Changes in Molecular Characteristics of Mycoplasma pneumoniae in Clinical Specimens from Children in Beijing between 2003 and 2015. PLoS One, 2017; 12, e0170253. [49] Voronina EN, Gordukova MA, Turina IE, et al. Molecular characterization of Mycoplasma pneumoniae infections in Moscow from 2015 to 2018. Eur J Clin Microbiol Infect Dis, 2020; 39, 257−63. [50] Zhao F, Liu J, Shi W, et al. Antimicrobial susceptibility and genotyping of Mycoplasma pneumoniae isolates in Beijing, China, from 2014 to 2016. Antimicrob Resist Infect Control, 2019; 8, 18. -

 点击查看大图
点击查看大图

图(2) / 表ll (4)
计量
- 文章访问数: 1122
- HTML全文浏览量: 493
- PDF下载量: 153
- 被引次数: 0

 Quick Links
Quick Links