

 下载:
下载:

-
Antiretroviral therapy (ART), also known as highly active ART (HAART), has been widely used in the treatment of human immunodeficiency virus (HIV) infection. The roll-out of ART has dramatically reduced HIV-related morbidity, mortality, and complications and increased life expectancy, making acquired immune deficiency syndrome (AIDS) a manageable chronic disease[1]. Viral suppression by ART leads to a decline in HIV transmission at the individual and population levels[2]. Therefore, ART is highly effective in reducing the risk of HIV transmission and is currently the most effective treatment for AIDS.
In 2003, China’s government launched a National Free ART program[3]. The first guideline for diagnosing and treating HIV/AIDS was issued in 2005, stating that zidovudine (or stavudine) plus lamivudine plus efavirenz (ZDV/d4T+3TC+EFV) was the recommended first-line ART regimen for treatment-naïve adults[4]. In 2008, the first-line ART regimen was updated to azidothymidine (or stavudine) plus lamivudine plus nevirapine (or efavirenz) (AZT/d4T+3TC+NVP/EFV). In 2012, it was changed to tenofovir disoproxil fumarate (or azidothymidine) plus lamivudine plus nevirapine (or efavirenz) (TDF/AZT+3TC+EFV/NVP)[5]. As of 2020, 978,000 people living with HIV received prescribed therapy[5], accounting for 92.2% of people living with HIV[6].
Drug resistance mutations (DRMs) appear in HIV strains under treatment pressure, leading to viral rebound and treatment failure[7]. Furthermore, drug-resistant variants can be transmitted to treatment-naïve individuals, which may limit treatment options and is a significant issue for the effective treatment of HIV infection[7]. Two recent systematic reviews on HIV drug resistance (HIVDR) indicated China’s national transmitted drug resistance (TDR) ranged from 3.0% to 9.3%[8,9], and acquired drug resistance (ADR) prevalence over 17 years (2001–2017) was 44.7%[8]. Among patients with failed ART, the prevalence of HIVDR was 64.1%, 39.8%, and 51.9% in south China[10], central south China[11], and north China[12], respectively. However, the risk factors related to DR have varied in previous studies. For example, previous studies have demonstrated antiretroviral adherence[13], marital status and the duration from HIV diagnosis to initiating ART[14], age and initial regimens[15], high viral load and HIV-syphilis co-infection[16], duration on ART and educational level[17] are associated with HIVDR. The World Health Organization (WHO) guidelines recommend routine viral load monitoring and expanded DR testing[18].
Hainan Island, China’s southernmost province, has a pleasant tropical season and is one of the country’s most popular tourist destinations. In addition to many tourists, many people have migrated to Hainan Island, especially from the northeastern provinces, due to Hainan’s tropical climate and environment[19-20]. Hainan is considered one of the provinces with a low HIV prevalence in China. By the end of 2019, 3,711 HIV-infected patients in Hainan had received ART[21]. The situation has been challenged by tourism and immigration. For example, most HIV diagnoses in Hainan Island occurred among men who have sex with men (MSM) in recent years[22], which is generally consistent with the situation in the northeastern provinces of China[23-25]. However, neither HIV-1 epidemic subtypes in Hainan nor the prevalence of HIVDR (or DRMs) in patients receiving ART has been adequately studied in the last ten years. We conducted a 7-year (2014–2020) cross-sectional study to address these questions. Most importantly, we assessed for the first time the characteristics of HIV-1 subtypes and the prevalence of HIVDR and DRMs in patients with ART failure and identified the factors associated with HIVDR in Hainan Province, China.
-
A cross-sectional study was conducted on HIV/AIDS patients with ART failure from 2014 to 2020 at the Fifth People’s Hospital of Hainan Province, the largest HIV/AIDS clinical treatment center in Hainan Province. According to China’s national guidelines for HIV/AIDS management (2018), virologic failure is defined as plasma HIV-RNA ≥ 200 copies/mL after 48 weeks of initial ART (initiation or modification); or virologic rebound; or HIV-RNA appearing ≥ 200 copies/mL after complete virologic inhibition. In this study, the inclusion criteria were as follows: (1) age ≥ 18 years, (2) confirmed diagnosis (enzyme-linked immunosorbent assay and Western blot) of HIV-1 infection, (3) virologic failure with HIV-RNA load ≥ 200 copies/mL after 48 weeks of initial ART, or virologic rebound, or HIV-RNA ≥ 200 copies/mL after complete virologic inhibition.
Baseline and follow-up clinical data, including demographic characteristics (sex, age, risk factors for HIV infection, occupation, marital status, ethnicity, education, and city of residence), CD4+T cell count, plasma viral load, HIV diagnosis date, co-infection with hepatitis B/C, ART initiation date, first-line ART regimen, the time between HIV diagnosis and ART initiation were obtained from the individual’s medical records.
-
The recommended first-line ART regimens in Hainan comprised two nucleotide reverse transcriptase inhibitors (NRTIs) and one non-nucleoside reverse transcriptase inhibitor (NNRTI). In the present study, the two NRTIs were 3TC plus either TDF, d4T, or AZT, whereas the NNRTI was either EFV, NVP, or RPV. The second-line regimens comprised two NRTIs (3TC plus TDF or AZT) sequentially selected based on which NRTIs were used as the first-line and a boosted protease inhibitor (PI), lopinavir-ritonavir (LPV/r). The initial regimens were as follows: (1) TDF+3TC+EFV (56.4%, 136/241), (2) AZT+3TC+NVP (20.3%, 49/241), (3) TDF+3TC+NVP (10.8%, 26/241), (4) AZT+3TC+EFV (6.2%, 15/241), (5) d4T+3TC+NVP (3.3%, 8/241), and (6) other regimens (2.9%, 7/241).
-
Approximately 10 mL of peripheral blood was collected from participants in ethylenediaminetetraacetic acid (EDTA) vacutainer tubes and immediately processed to separate plasma by centrifugation at 3,000 rpm for 15 min. Plasma samples were frozen at −80 °C until tested for HIV-1 RNA viral load and DR. Viral RNA extraction and HIV-1 pol amplification were performed at the Guangxi Key Laboratory of AIDS Prevention and Treatment (Guangxi Medical University, Guangxi, China). The HIV-1 pol sequence (1,300 base-pairs) that encodes HIV protease and HIV reverse transcriptase (RT, amino acids 1–335) was sequenced by Sangon Biotech Company. The primers to amplify the HIV pol region using nested RT-PCR were as described previously[26].
-
HIV-1 pol sequences were assembled by Sequencher v5.1.4.6 and aligned using the online HIV align tool (
http://www.hiv.lanl.gov/content/sequence/viralign.html ) by the MAFFT model and HXB2 reference sequence. HIV-1 subtypes were determined using the automated tool COMET (https://comet.lih.lu/ ) and Recombinant Identification Program for preliminary classification and identified by the maximum likelihood phylogenetic tree (ML tree) with reference sequences (subtypes A-K+Recombinants) downloaded from the Los Alamos sequence database (http://www.hiv.lanl.gov/ ). The ML tree was constructed with the general time-reversible substitution model with a gamma-distributed rate variation and proportion of invariant sites (GTR+F+R10) using IQ tree v1.6.12 choosing the best-fit model according to Akaike Information Criterion. Subtype O.CM was set as an outgroup. The stability of the ML tree topology was tested using ultra-fast bootstrap (1,000 replicates). Ultra-fast bootstrap values ≥ 0.8 were considered significant. Finally, the tree was visualized using Fig tree v1.4.4.DR and DRMs were assessed using the HIVDR Database online platform at Stanford University (
http://hivdb.stanford.edu ). The database employs the list of major standardized HIV-1 DRMs. Cases were classified as susceptible or having low-, intermediate-, or high-level drug resistance in the three drug classes analyzed (PIs, NNRTIs, and NRTIs). -
The data analyses were performed using IBM SPSS v21.0. For data description, the numeric variables were displayed with medians and interquartile ranges (IQRs), whereas the categorical variables were presented as proportions and analyzed with χ2 test or Fisher’s exact test. Multivariate logistic regression models assessed associations between considered variables and HIVDR. If variables in the final multivariate logistic regression model with P < 0.05 were considered statistically significant and reported descriptively with a 95% confidence interval (95% CI) of adjusted odds ratio (aOR).
-
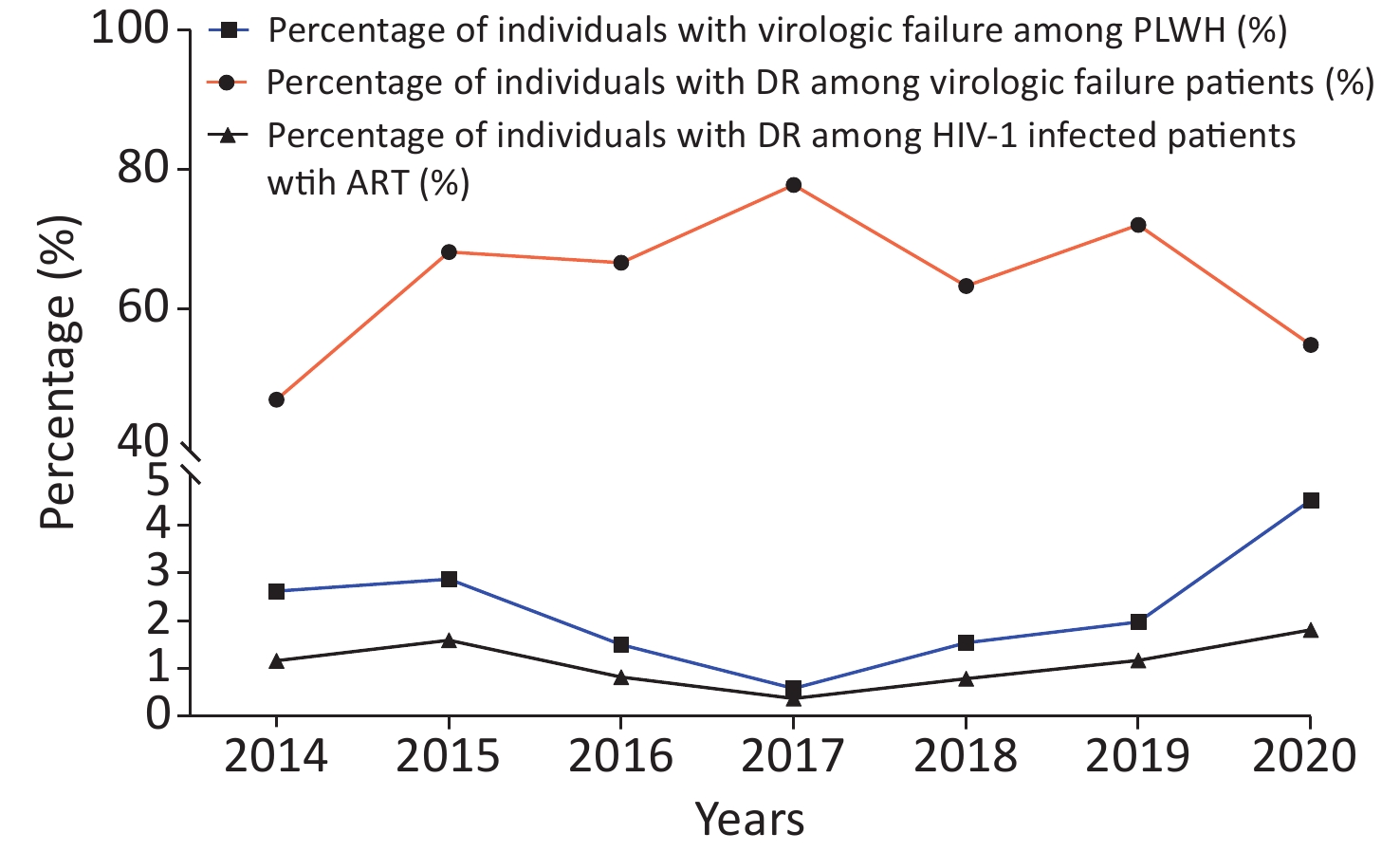
From 2014 to 2020, the annual number of patients who received ART was 687, 942, 1,467, 1,905, 2,408, 2,642, and 3,094, respectively. A total of 307 patients with virologic failure after ART were recruited. The annual prevalence of virologic failure in patients after ART was 2.62% (18/687), 2.87% (27/942), 1.50% (22/1,467), 0.58% (11/1,905), 1.54% (37/2,408), 1.97% (52/2,642), and 4.52% (140/3,094), respectively (Figure 1).
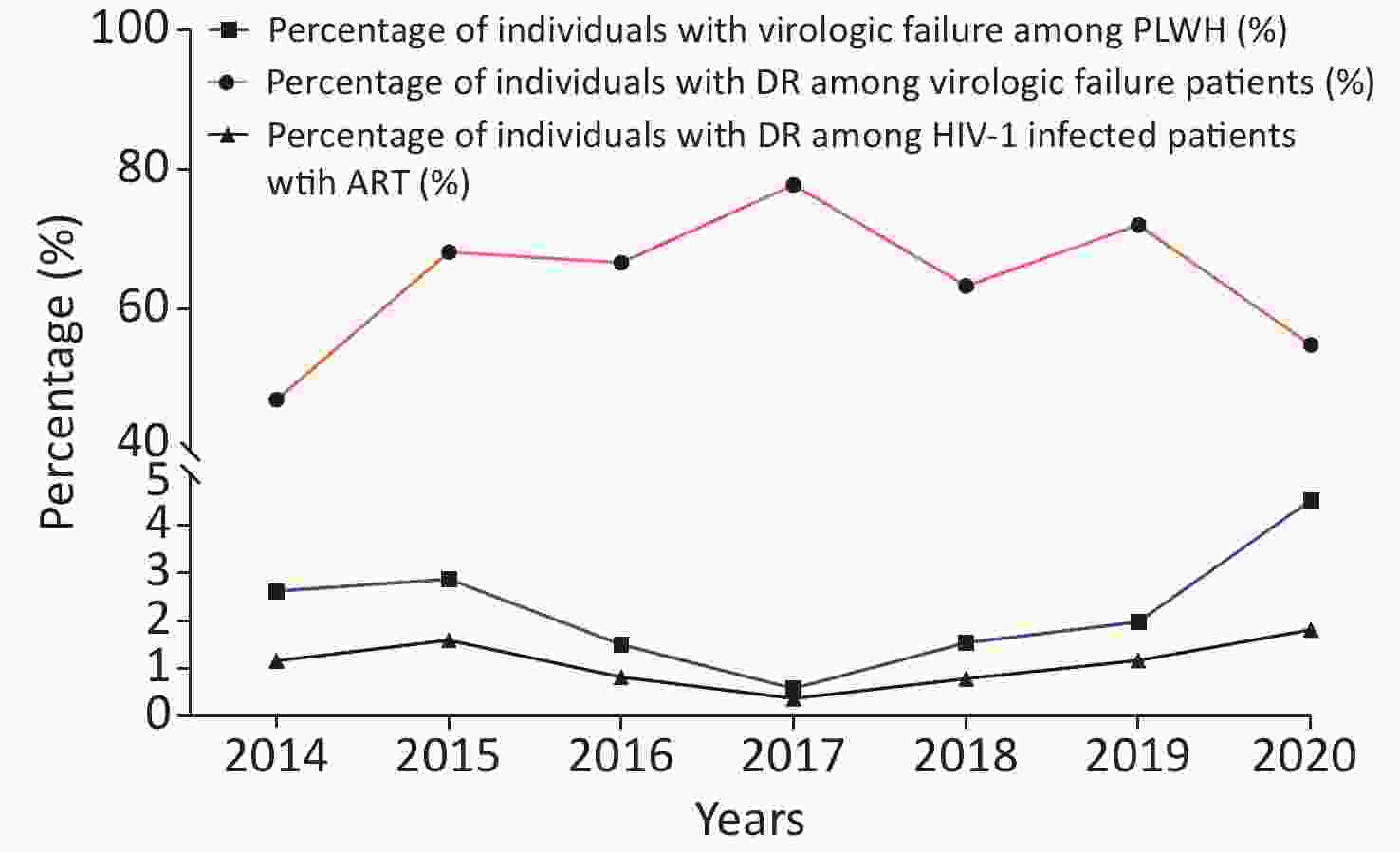
Figure 1. The prevalence of virologic failure and drug resistance (DR) over time from 2014 to 2020. PLWH, people living with HIV-1. ART, antiretroviral therapy.
Of the 307 patients with virologic failure after ART, 66 patients were excluded due to a lack of personal information or failure of HIV-1 sequencing. Finally, a total of 241 (78.5%, 241/307) HIV-1 available pol sequences and corresponding medical records were analyzed in this study. From 2014 to 2020, the annual proportion of sequences was 7.05% (17/241), 9.13% (22/241), 7.47% (18/241), 3.73% (9/241), 12.45% (30/241), 17.84% (43/241), and 42.32% (102/241), respectively. Moreover, from 2014 to 2020, the annual proportion of sequences among patients on ART varied from 0.47% to 3.33% (Figure 1).
-
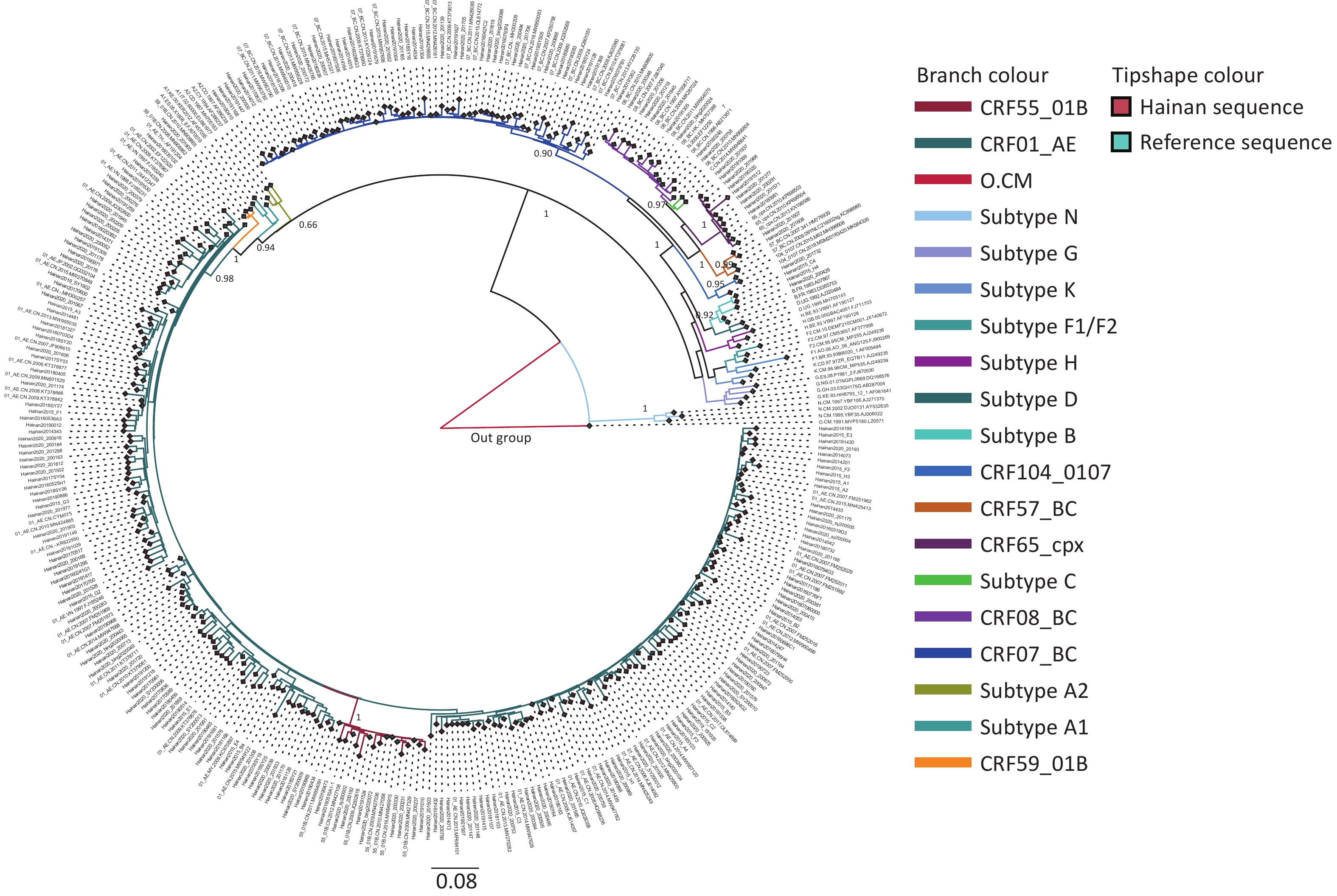
A closer inspection of the ML tree (Figure 2) revealed the HIV-1 subtype diversity in the Hainan Province. Among 241 patients, CFR01_AE accounted for 68.88% (166/241), followed by CFR07_BC (41/241, 17.01%) and CRF55_01B (10/241, 4.14%). In addition, eight CRF65_CPX strains, eight CRF08_BC strains, three subtype B strains, two CRF57_BC strains, one CRF59_01B strain, one CRF104_0107 strain, and one subtype C strain were detected.
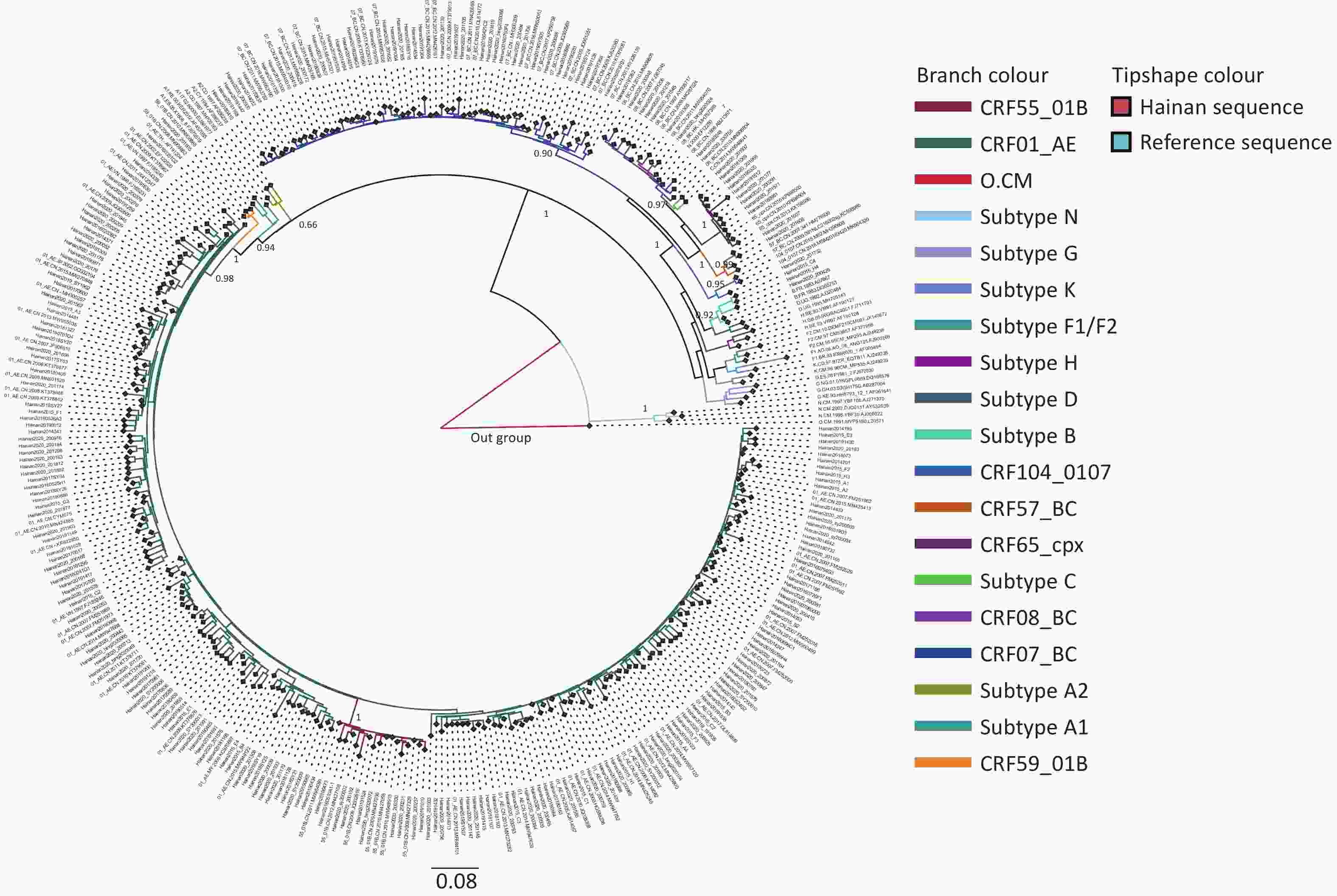
Figure 2. Phylogenetic tree of HIV-1 pol sequences obtained from patients with ART-failure in Hainan Province. The maximum likelihood phylogenetic tree (ML tree) was constructed using 365 HIV-1 pol sequences, including 241 Hainan sequences and 124 reference sequences. A total of 166 HIV-1 CRF01_AE query sequences branched with 47 HIV-1 CRF01_AE reference sequences (dark green color), bootstrap value was 0.98. Forty-one HIV-1 CRF07_BC query sequences branched with 22 reference sequences (dark blue color), bootstrap value was 0.90. Ten HIV-1 CRF55_01B query sequences were identified (dark red color), bootstrap value was 1.0. Eight HIV-1 CRF08_BC (lilac color) and eight HIV-1 CRF65_cpx (deep purple color) query sequences were identified (bootstrap value = 0.97 and 1, respectively) with nine and three reference sequences, respectively. Meanwhile, CRF57_BC (brown color), CRF59_01B (orange color), CRF104_0107 (light blue color), subtype B (blue-green color) and subtype C (bright green color) were detected. The green diamond of tip shape corresponds to Hainan sequences, and red diamond corresponds to reference sequences.
The demographic characteristics of 241 patients are described in Table 1. Among them, the median age was 32 (IQR: 26–42) years, 83.4% were male, and 67.63% were single. Ninety-nine cases (41.08%) had a middle school edducation. The main routes of HIV-1 infection were heterosexual transmission (119, 49.38%) and homosexual transmission (86, 35.68%). The majority of infections (77%) occurred between 2017 and 2020. Nearly half of the patients (49.79%) had baseline CD4 cell counts lower than 200 cells/mm3, 67.22% used TDF+3TC+EFV/NVP, and 62.66% received ART within seven months after diagnosis. The median VL was 32,529 copies/mL (IQR: 9,071–101,453 copies/mL).
Table 1. Characteristics of HIV-infected patients with virologic failure from 2014 to 2020 in Hainan Province, China
Variables Number (N) Percent (%) Total 241 100 Sex Female 40 16.60 Male 201 83.40 Age, years: median 32, IQR (26, 42) 19−29 97 40.25 30−39 73 30.29 40−49 39 16.18 ≥ 50 32 13.28 Marital Status Married and cohabiting 78 32.37 Single 163 67.63 Ethnics Han 203 84.23 Others 32 13.28 Unknown 6 2.49 Region Northern Hainan 92 38.17 Eastern Hainan 22 9.13 Southern Hainan 63 26.14 Western Hainan 39 16.18 Central Hainan 25 10.37 Education Primary school or lower 46 19.09 Secondary school 99 41.08 High school or above 90 37.34 Unknown 6 2.49 Occupation Farmer 83 34.44 Unemployment 64 26.56 Others 79 32.78 Unknown 15 6.22 Risk factors Homosexual 86 35.68 Heterosexual 119 49.38 Others 36 14.94 Sampling time, year 2014−2016 57 23.65 2017−2020 187 77.59 Basic line CD4 cell count, cells/mm3: median 195, IQR: 80–324 < 200 120 49.79 200−350 70 29.05 301−500 24 9.96 > 500 18 7.47 Unknown 9 3.73 HIV-1 subtype CRF01_AE 166 68.88 CRF07_BC 41 17 Other (B/C/CRF08_BC/CRF59_01B/CRF55_01B/CRF65_cpx /CRF57_BC/CRF104_0107) 34 14.12 Initial therapeutic regimen AZT+3TC+EFV/NVP 64 26.56 TDF+3TC+EFV/NVP 162 67.22 Others 15 6.22 Hypoimmunity or opportunistic infections Yes 76 31.54 No 165 68.46 The duration from diagnosis to ART, month: median 3, IQR: 0–20.5 < 7 151 62.66 ≥ 7 90 37.34 Time on ART, month: median 20, IQR: 10–39.5 < 13 82 34.02 13−25 58 24.07 > 25 101 41.91 Co-infection hepatitis B Yes 34 14.11 No 127 52.70 Unknown 80 33.20 Co-infection hepatitis C Yes 30 12.45 No 112 46.47 Unknown 99 41.08 Viral load, log10 copies/mL Viral load median: 32,529 copies/mL, IQR: 9,071−101,453 copies/mL 4.00−4.99 116 48.13 ≥ 5.00 62 25.73 ≤ 3.99 63 26.14 Note. IQR, interquartile range; ART, antiretroviral therapy; CRF, circulating recombinant form; AZT, zidovudine; 3TC, lamivudine; EFV, efavirenz; NVP, nevirapine; TDF, tenofovir. -
Table 2 shows the prevalence of HIVDR among the 241 patients with virologic failure. The overall prevalence of HIVDR to antiretroviral drugs was 61.41% (148/241). From 2014 to 2020, the annual prevalence of HIVDR was 47.06%, 68.18%, 66.67%, 77.78%, 63.33%, 72.09%, and 54.90%, respectively. The prevalence of HIVDR remained stable over time (χ2 = 8.824, P = 0.218, Figure 1).
Table 2. Factors associated with drug resistance among HIV-1 patients with virologic failure from 2014 to 2020 in Hainan Province, China
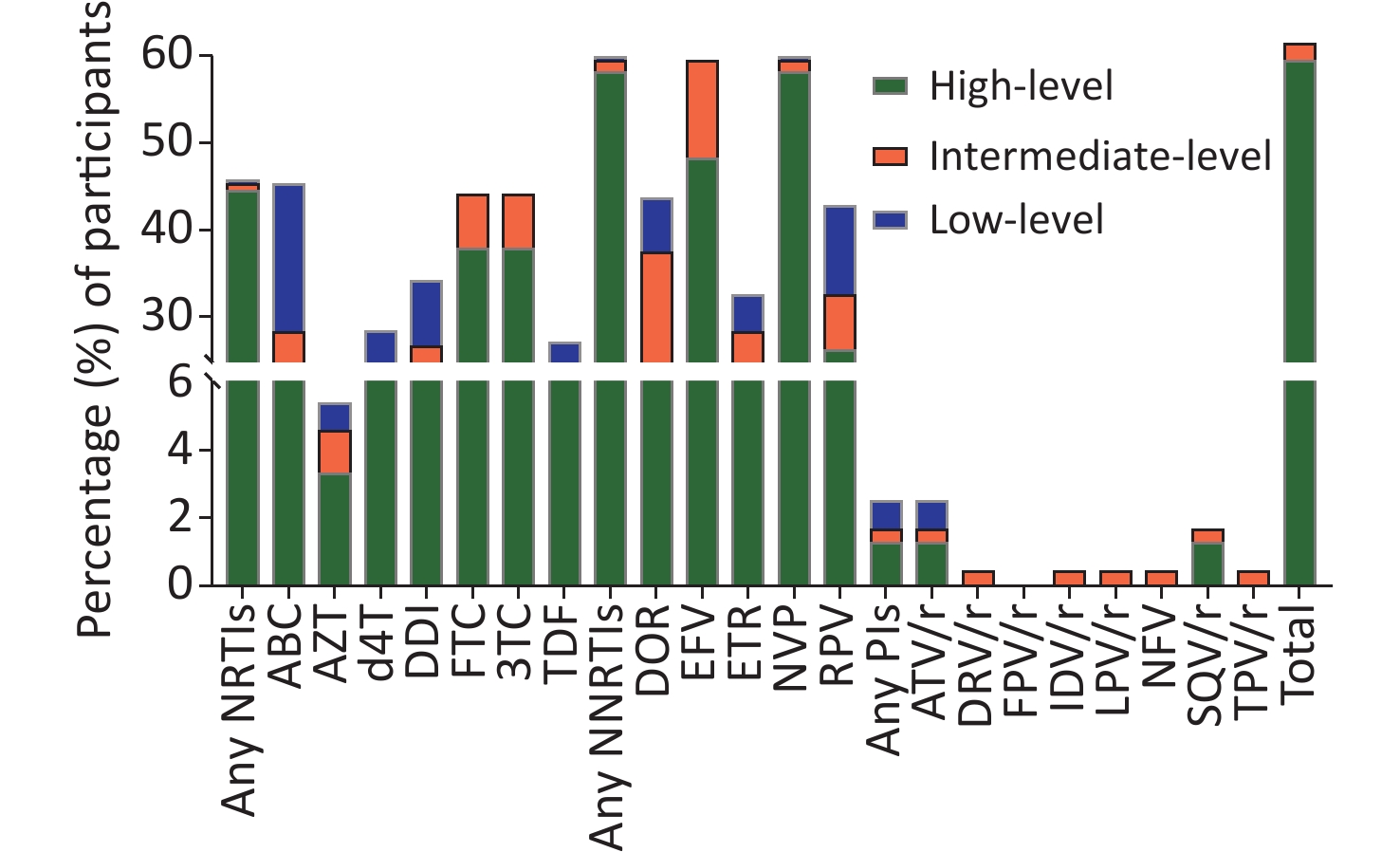
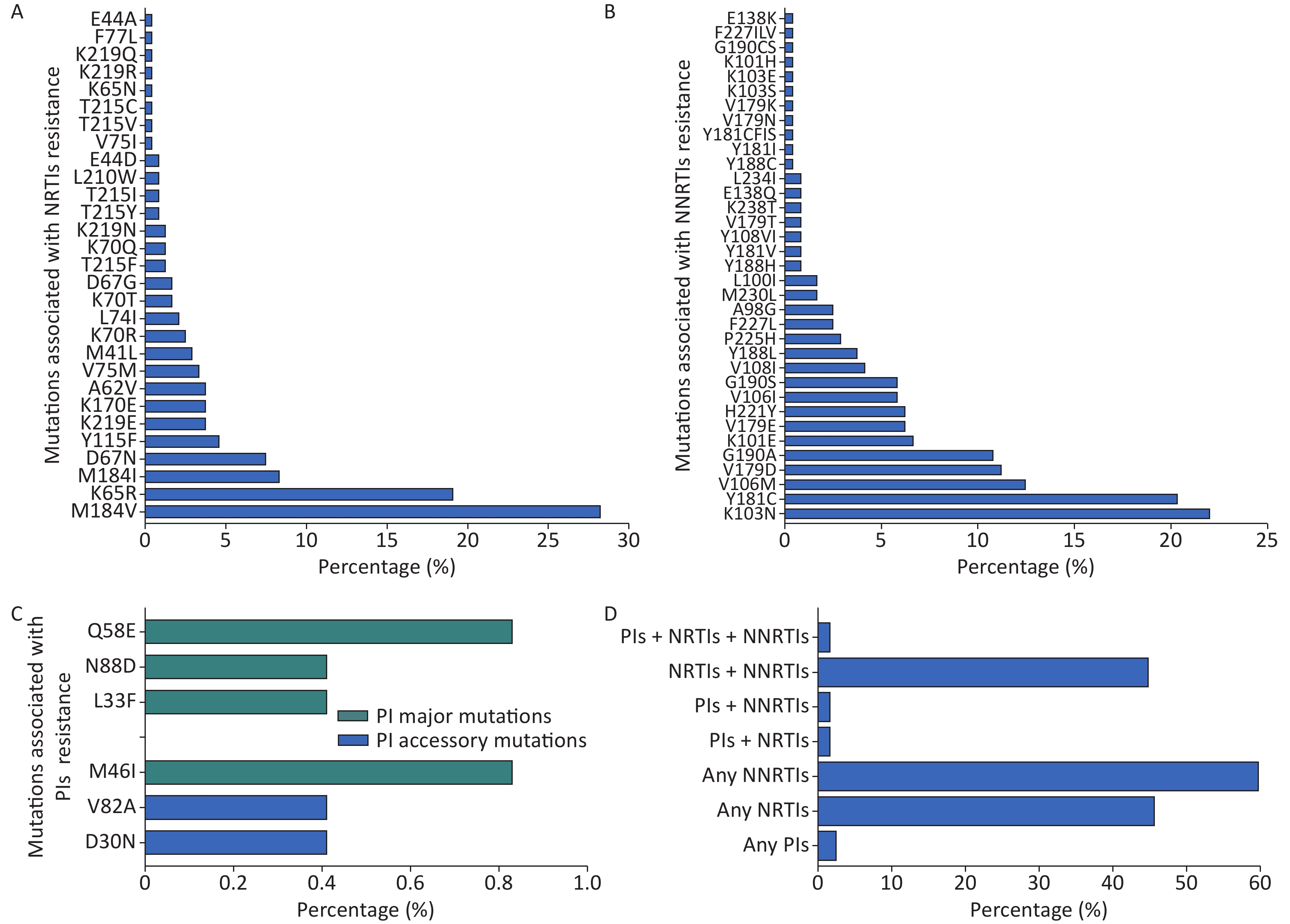
Variables N Drug resistance Univariate Multivariate Number (N) Percent (%) χ2 P1 aOR (95% CI) P2 Total 241 148 61.41 Sex Male 201 113 66.17 11.571 0.001 Ref. Female 40 15 37.50 0.11 (0.03, 0.38) 0.001 Ages, years 0.077 19−29 97 67 69.07 15.587 0.001 Ref. 30−39 73 50 68.49 1.31 (0.49, 3.46) 0.590 40−49 39 14 35.90 0.27 (0.08, 0.94) 0.039 ≥ 50 32 17 53.13 0.51 (0.13, 2.05) 0.343 Marital status Single 163 109 66.87 6.336 0.012 Ref. Married and cohabiting 78 39 50.00 0.53 (0.21, 1.32) 0.172 Ethnics Han 203 123 60.59 2.450 0.118a Ref. Others 32 24 75.00 3.386 0.083 Unknown 6 1 16.67 Region 0.467 Central Hainan 25 12 48.00 4.128 0.389 Ref. Northern Hainan 92 59 64.13 1.87 (0.45, 7.75) 0.39 Eastern Hainan 22 11 50.00 0.63 (0.11, 3.75) 0.61 Southern Hainan 63 42 66.67 2.09 (0.45, 9.76) 0.347 Western Hainan 39 24 61.54 2.08 (0.39, 11.20) 0.394 Education 0.183 Primary school or lower 46 26 56.52 1.061 0.588a Ref. Secondary school 99 62 62.63 1.34 (0.45, 4.01) 0.607 High School or above 90 59 65.56 0.48 (0.12, 1.87) 0.291 Unknown 6 1 16.67 Occupation 0.034 Farmer 83 48 57.83 4.873 0.087a Ref. Unemployment 64 48 75.00 4.32 (1.38, 13.51) 0.012 Others 79 49 62.03 1.51 (0.54, 4.19) 0.433 Unknown 15 3 20.00 Risk factors 0.321 Homosexual 86 63 73.26 10.685 0.005 Ref. Heterosexual 119 61 51.26 0.54 (0.17, 1.66) 0.282 Others 36 24 66.67 0.24 (0.04, 1.68) 0.152 Sampling time, year 2014−2016 57 35 61.40 < 0.001 0.999 Ref. 2017−2020 187 116 62.03 3.26 (1.12, 9.47) 0.030 Basic line CD4 cell count, cells/mm3 0.419 < 200 120 86 71.67 15.914 0.001a Ref. 200−350 70 38 54.29 0.44 (0.14, 1.34) 0.148 301−500 24 13 54.17 0.42 (0.10, 1.82) 0.246 > 500 18 5 27.78 0.35 (0.07, 1.83) 0.214 Unknown 9 6 66.67 HIV-1 subtype 0.001 CRF01_AE 166 115 69.28 17.634 < 0.001 Ref. CRF07_BC 41 14 34.14 0.14 (0.05, 0.40) < 0.001 Others 34 19 55.88 0.26 (0.07, 0.88) 0.031 Initial therapeutic regimen 0.006 AZT+3TC+EFV/NVP 64 43 67.19 1.230 0.541 Ref. TDF+3TC+EFV/NVP 162 96 59.26 0.15 (0.04, 0.48) 0.002 Others 15 9 60.00 0.46 (0.07, 2.92) 0.410 Hypoimmunity or opportunistic infections Yes 76 60 78.95 14.405 < 0.001 Ref. No 165 88 53.33 0.32 (0.10, 0.99) 0.049 The duration from diagnosis to ART, month < 7 151 93 61.59 0.005 0.941 Ref. ≥ 7 90 55 61.11 0.87 (0.34, 2.24) 0.769 Time on ART, month 0.610 < 13 82 53 64.63 0.594 0.743 Ref. 13−25 58 34 58.62 0.89 (0.29, 2.72) 0.843 > 25 101 61 60.40 0.60 (0.21, 1.74) 0.348 Co-infection hepatitis B 0.689 Yes 34 21 61.76 0.003 0.999 Ref. No 127 78 61.42 0.59 (0.17, 2.07) 0.407 Unknown 80 49 61.25 0.61 (0.15, 2.56) 0.501 Co-infection hepatitis C 0.361 Yes 30 18 60.00 0.108 0.947 Ref. No 112 70 62.50 0.29 (0.05, 1.59) 0.155 Unknown 99 60 60.61 0.35 (0.06, 2.13) 0.256 Viral load, log10 copies/mL 0.935 4.00−4.99 116 69 59.48 2.317 0.314 Ref. ≥ 5.00 62 43 69.35 0.97 (0.36, 2.65) 0.955 ≤ 3.99 63 36 57.14 0.84 (0.33, 2.14) 0.717 Note. aOR, adjusted odd ratio; ART, antiretroviral therapy; CRF, circulating recombinant form; AZT, zidovudine; 3TC, lamivudine; EFV, efavirenz; NVP, nevirapine; TDF, tenofovir; P1, significant values of univariate analysis; P2, significant values of multivariate logistic regression analysis; a, among the corresponding independent variables, the number of the last group is too small to be included in the analysis. Among the 241 patients, 59.34% were high-level DR, 1.24% were intermediate-level DR, and 0.83% were low-level DR. The prevalence of HIVDR to NRTIs, NNRTIs, and PIs was 45.64% (110/241), 59.75% (144/241), and 2.49% (6/241), respectively (Figure 3). For NRTI drugs, the prevalence of HIVDR against ABC was the highest (45.23%, 109/241), followed by FTC and 3TC (106/241, 43.98%). NVP (59.75%, 144/241), EFV (59.35%, 143/241), and doravirine (DOR) (43.57%, 105/241) were the most common HIVDR drugs to NNRTIs. For PIs, the highest prevalence of HIVDR was 1.66% (NFV, 4/241) (Figure 3). Among the 241 patients, four cases (1.66%) showed triple drug resistance to NRTIs, NNRTIs, and PIs, and 108 cases (44.81%) were resistant to both NRTIs and NNRTIs (Figure 4D).
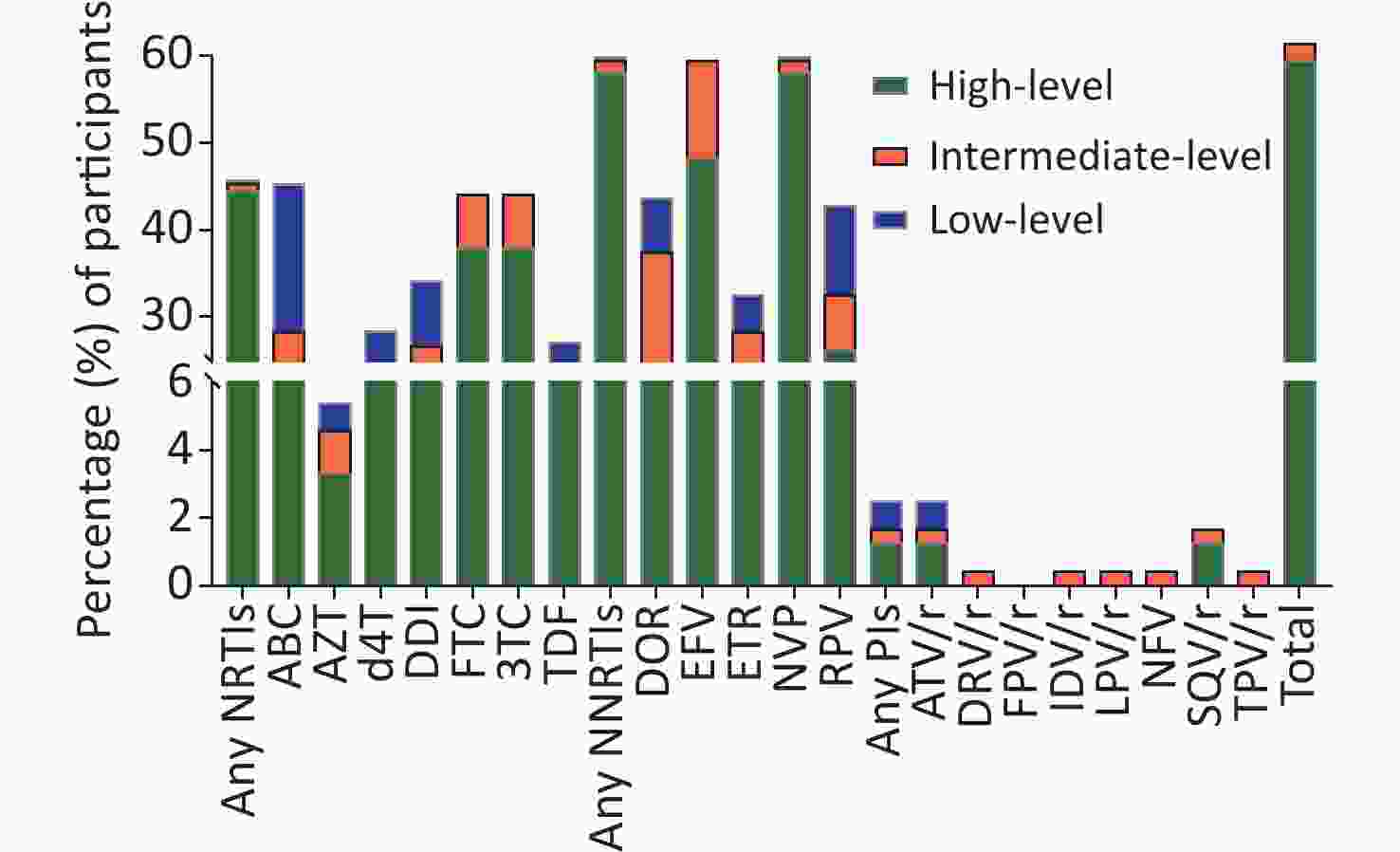
Figure 3. Drug-resistant levels against antiretroviral drugs among ART-failure individuals in Hainan Province from 2014 to 2020. Among the 241 participants, 59.34% acquired high-level drug resistance, 1.24% was intermediate-level drug resistance, and 0.83% was belong to low-level drug resistance (DR). For antiretroviral drugs, 45.29% of patients had DR to ABC, which belongs to NRTIs. About 59% of patients was DR to NVP and EFV belonging to NNRTIs. NRTIs, nucleoside reverse transcriptase inhibitors; NNRTIs, non-nucleoside reverse transcriptase inhibitors; PIs, boosted protease inhibitors. ABC, abacavir; AZT, zidovudine; d4T, sanilvudin; DDI, dideoxynosine; FTC, emtricitabine; 3TC, lamivudine; TDF, tenofovir; DOR, doravirine; EFV, efavirenz; ETR, etravirine; NVP, nevirapine; RPV, rilpivirine; ATV/r, atazanavir with ritonavir; DRV/r, darunavir with ritonavir; FPV/r, fosamprenavir with ritonavir; IDV/r, indinavir with ritonavir; LPV/r, lopinavir with ritonavir; NFV, nelfinavir; SQV/r, saquinavir with ritonavir; TPV/r, tipranavir with ritonavir.
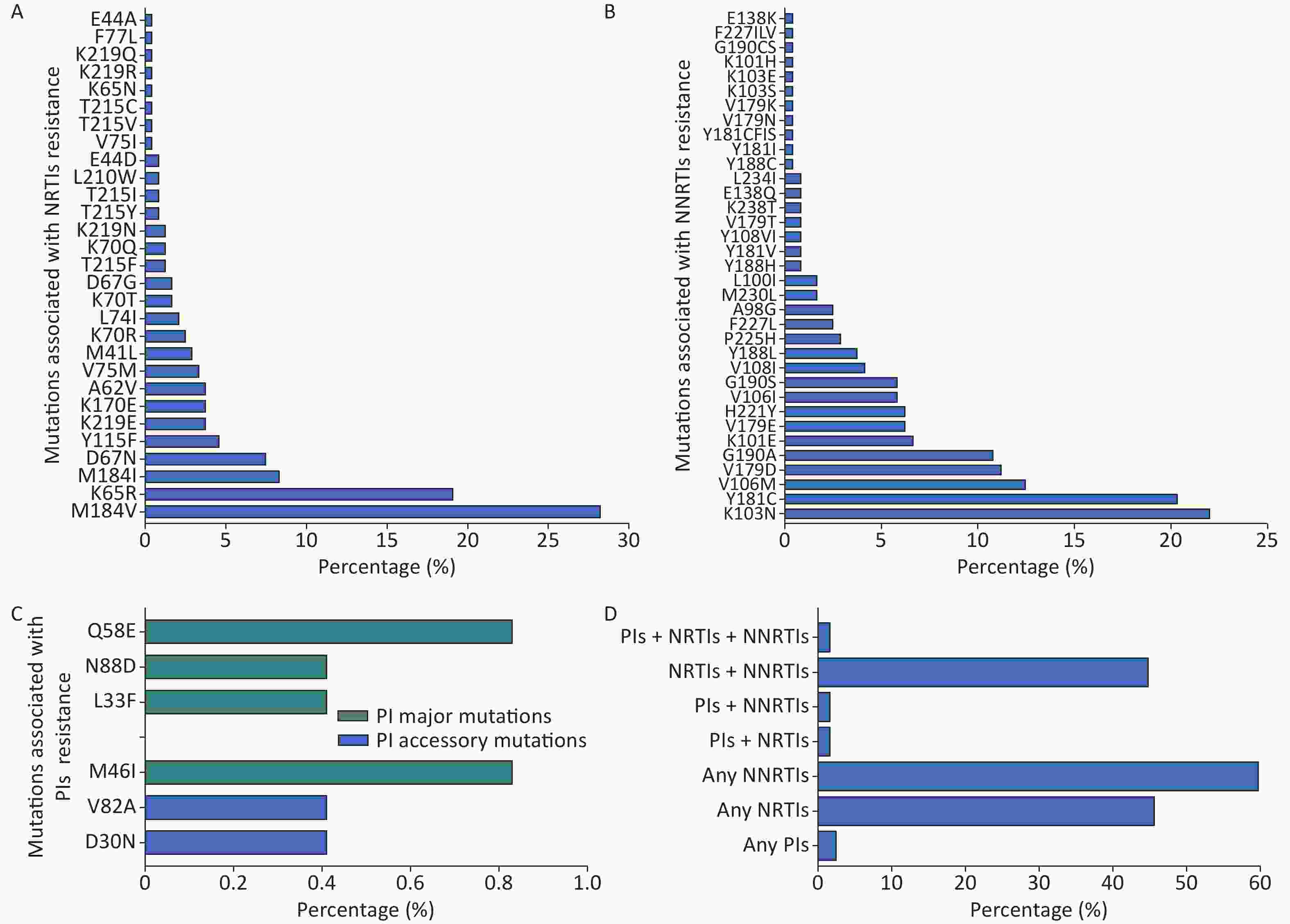
Figure 4. Frequency of drug resistance mutations (DRMs) and drug resistance prevalence among 241 patients with virologic failure after ART in Hainan Province, 2014–2020. (A) Frequency of DRMs to nucleoside reverse transcriptase inhibitors (NRTIs). (B) Frequency of DRMs to non-nucleoside reverse transcriptase inhibitors (NNRTIs). (C) Frequency of DRMs to boosted protease inhibitors (PIs). (D) Drug resistance prevalence by ART drugs.
-
In the univariate model, male patients had a higher prevalence of HIVDR than female patients (66.17% vs. 37.50%), while those aged 40–49 had the lowest prevalence (35.90%). Single participants had a higher prevalence than others (66.87% vs. 50.00%), and patients who acquired HIV through homosexual behavior and whose baseline CD4 cell counts were lower than 200 cells/mm3 had the highest prevalence of HIVDR (73.26% and 71.67%). In addition, patients infected with HIV-1 CRF01_AE strain and hypoimmunity or opportunistic infections had higher HIVDR prevalence than other patients (Table 2).
In the multivariate model, sex, initial therapeutic regimen, age, HIV-1 subtype, patient occupation, sampling time, and hypoimmunity or opportunistic infections were independently associated with HIVDR (Table 2). Compared with male patients, the aOR for female patients was 0.11 (95% CI: 0.03−0.38). HIVDR was more common in patients on TDF-based regimens than on AZT-based regimens (aOR: 0.15, 95% CI = 0.04−0.48). HIVDR was discovered less frequently in patients with CRF07 BC than in those with CRF01 AE (aOR: 0.14, 95% CI: 0.05−0.40) and in patients aged 40–49 years than in patients aged 19–29 years (aOR: 0.27, 95% CI: 0.08−0.94). Unemployed patients were more likely to be HIVDR than farmers (aOR: 4.32, 95% CI: 1.38−13.51). Similar to the samples from 2014 to 2016, the samples from 2017 to 2020 had a higher prevalence of HIVDR (aOR: 3.26, 95% CI: 1.12−9.47). We also found that patients with hypoimmunity or opportunistic infections had a lower prevalence of HIVDR (aOR: 0.32, 95% CI: 0.101−0.996).
-
Regarding DRMs against NRTIs, the most common DRM was M184V, causing high-level resistance to 3TC and FTC, found in 68 of 241 patients (28.22%); K65R, causing high-level resistance to FTC, was detected in 46 of 241 patients (19.09%) (Figure 4A). Against NNRTIs, the K103N, leading to high-level resistance against NVP, was the most common and was found in 53 of 241 patients (21.99%); Y181C and V106M were observed in 20.33% (49/241) and 12.45% (30/241) of the patients, respectively (Figure 4B). M46I and Q58E mutations, which PIs selected, occurred in 0.83% (2/241) (Figure 4C).
-
This study first investigated the prevalence of virologic failure in patients with ART in Hainan Province, China. The results showed that from 2014 to 2020, the prevalence of virological failure ranged from 0.58% to 4.52%. The highest prevalence of virologic failure was 4.52% in 2020, lower than 11.8% in China in 2014[27]. In addition, some studies found that the replacement of the ART regimen[28], male sex[29], illiteracy[30], level of baseline CD4 cell count below 100 cells/mm3, and adherence[31] were associated with a higher likelihood of virologic failure on ART. Although the prevalence of virologic failure in Hainan Province is low, the current results suggest increasing the medication guidance, strengthening the management of treatment follow-up, and following the prescribed dose[32].
In previous years, Wei Deng et al. found that CRF01_AE was the dominant HIV-1 subtype in Hainan, accounting for 84.3% of HIV-positive patients, followed by the B’ variant (9.6%)[33]. In the present study, our results showed that CRF01_AE remained the most prevalent subtype. Although the proportion decreased from 2009 to 2020 (68.9% vs. 84.3%), many novel CRFs appeared for the first time, such as CRF55_01B, CRF57_BC, CRF65_cpx, and CRF59_01B. Our study further highlights the high genetic diversity of HIV-1 in Hainan, which drives the local HIV epidemic. As a major tourism province, Hainan has attracted many tourists and immigrants, which may have contributed to the wide diversity of HIV subtypes. In addition, previous research has found that subtypes were associated with the progression of HIV/AIDS[34]. The diversity of subtypes has challenged the prevention and control of HIV/AIDS. Therefore, understanding the HIV-1 subtype is essential for guiding targeted HIV control efforts.
HIVDR remains one of the major obstacles to ART efficacy and AIDS treatment, especially in countries with limited access to ART. Among HIV-infected people on ART, between 2014 and 2020, in Hainan Province, the highest prevalence of HIVDR was 1.81% in 2020, which did not reach the threshold of low prevalence, according to the definition of WHO (5%)[35]. From 2014 to 2020, the overall prevalence of HIVDR among the patients with virologic failure was 61.41% in Hainan Province, higher than in Sichuan (45.3%)[36], Guangxi (32.4%), and the national level (51.56%)[37] China. However, it was notably lower than in KwaZulu-Natal Province (92.2%) in South Africa[38], Brazil (84.1%)[39], Ethiopia (74.4%)[40], and Russia (72.5%)[41].
Several factors contributed to HIVDR among patients with ART failure in this study, including sex, initial therapeutic regimen, HIV-1 subtype, occupation, sampling time, and hypoimmunity or opportunistic infections. In this study, males are more likely to be HIVDR than females. The higher proportion of male HIV-positive patients[21] and more male patients with virologic failure than females in Hainan Province can explain the higher odds of HIVDR among males. In addition, adherence to treatment plays a crucial role in the prevalence of DR, and previous research confirmed that men[42] or unemployed patients[43] have poor adherence to ART. This is in line with our finding that unemployed patients are more likely to have HIVDR than farmers. This study also found that TDF regimens had a lower HIVDR prevalence than AZT-based regimens. It may be because TDF has been used for antiviral therapy for a relatively short period and was included in first-line regimens from 2015, supported by Margot’s and Etiebet’s studies[44,45]. In addition, the HIV-1 subtype and sampling time were related to HIVDR in the present study. Patients infected with the CRF01_AE strain had a higher prevalence than CRF07_BC, which can be explained by CRF01_AE being the most prevalent subtype in Hainan. As Gao Xiaoli found in Shanxi Province, the most prevalent CRF07_BC had the highest prevalence of HIVDR in patients with failed ART[46]. Our results showed that samples from 2017 to 2020 had a higher prevalence of HIVDR than those from 2014 to 2016, which was associated with prolonged treatment time[36].
Of note, we observed that patients who were hypoimmunity or with opportunistic infections had a higher prevalence of HIVDR. HIV patients might have insufficient physical resistance due to hypoimmunity or opportunistic infections, leading to viral suppression failure and drug resistance, which may contribute to the higher prevalence of HIVDR. The results showed that drug resistance monitoring for HIV-infected patients with hypoimmunity or opportunistic infections should be strengthened. In this study, another finding was that the HIVDR was not associated with CD4 count and viral load. However, previous studies found varying results regarding the relationship between viral load, baseline CD4 count, and the presence of HIVDR in ART[11,47]. Some studies, including the present study, found that age and infection route were unrelated to HIVDR for HIV-1 infected patients with ART failure[48].
Consistent with studies conducted in other areas of China[49], the prevalence of HIVDR to NNRTIs was substantially higher than that of NRTIs and PIs among patients with ART failure in Hainan. The first-line regimens in Hainan Province consist of two NRTIs and one NNRTI. In this study, the main regimens were TDF+3TC+NVP/EFV or AZT+3TC+NVP, which account for more than 85.0%. Under the pressure of drug selection, DRMs associated with NNRTIs, and NRTIs were dominant.
NNRTIs have a low genetic barrier to resistance, and one primary mutation of NNRTIs often leads to multiple and high-level resistance to NNRTIs drugs[50]. In our study, we observed that K103N (22%) was the most common resistance mutation to NNRTIs. K103N, a nonpolymorphic mutation selected by NVP and EFV[51], can reduce NVP and EFV susceptibility[52] and cause high resistance to NVP. We also observed that the prevalence of DR to NVP was the highest in all NNRTIs drugs in this study. This study also found that ABC, FTC, and 3TC were the most critical NRTIs drugs responsible for high drug resistance. The major DR-associated mutations to NRTI were M184V and K65R. M184V, the most prevalent, is selected due to the wide use of 3TC as a first-line therapy in China[53]. The M184V mutation causes high-level resistance to 3TC and FTC and also causes low-level resistance to ABC[54].
Nevertheless, M184V could increase the susceptibility to AZT, d4T, and TDF and slow the emergence of resistance to AZT, d4T, and TDF[55]. Therefore, 3TC has been widely used in China until now[56]. K65R is selected by TDF, ABC, and 3TC, decreasing viral susceptibility to these drugs[57]. The increasing and preferential usage of TDF in clinical practice, including in a context of a failing regimen, could be the primordial reason for the significant expansion of K65R, as other studies show a higher prevalence of this mutation in patients failing ART treatment[58]. Another finding is that 2.49% of participants exhibited HIVDR to PIs in this study, indicating that PIs still work well in our settings.
Of note, 44.81% of the patients were resistant to both NRTIs and NNRTIs, and 1.66% were resistant to triple NRTIs, NNRTIs, and PI in this study. Previous studies have confirmed that multi-drug resistance can reduce susceptibility to almost all drugs, making it challenging to optimize therapy to halt viral replication in these patients. In addition, multi-drug resistance is associated with an increased risk of clinical progression and death[59]. Managing patients infected with multi-drug resistance strains are among the critical issues in HIV therapy[60].
There were several limitations to this study. First, the sample size is not large. However, these annual samples were from the vast majority of cities in Hainan Province, accounting for 78.5% of ART-failed patients in a drug resistance surveillance program, which could represent the population of HIV-1 positive patients with ART failure. Second, HIVDR could not be identified as ADR or TDR because the samples were collected after ART. Third, the year of ART failure might differ from the year of HIVDR testing. In this study, we excluded samples collected repeatedly in different years, which may underestimate the results of HIVDR.
In conclusion, we highlighted the diversity of HIV-1 subtypes and reported the prevalence of virologic failure for the first time in Hainan Province, and illustrated that the HIVDR was low in Hainan during the rapid expansion of ART from 2014 to 2020. Of note, we found that patients with hypoimmunity or opportunistic infections were more likely to develop HIVDR, suggesting that drug resistance monitoring of these patients should be strengthened in the future. Meanwhile, this study showed that NNRTIs and NRTIs resistance developed rapidly among patients with virologic failure, and the PI-based treatment regimen might be superior to NNRTIs. Our results support that HIVDR testing should be universal and mandatory as it is the best way to promote personalized selection of the most optimized ART regimen.
-
This study was approved by the Human Research Ethics Committee of Guangxi Medical University under protocol 20220207. Written informed consent was obtained from all participants prior to enrolment in the study.
-
The GenBank accession numbers of the 241 Hainan HIV-1 sequences are OP830908-OP831148.
doi: 10.3967/bes2023.077
HIV-1 Subtype Diversity and Factors Affecting Drug Resistance among Patients with Virologic Failure in Antiretroviral Therapy in Hainan Province, China, 2014–2020
-
Abstract:
Objective This study aimed to determine the HIV-1 subtype distribution and HIV drug resistance (HIVDR) in patients with ART failure from 2014 to 2020 in Hainan, China. Methods A 7-year cross-sectional study was conducted among HIV/AIDS patients with ART failure in Hainan. We used online subtyping tools and the maximum likelihood phylogenetic tree to confirm the HIV subtypes with pol sequences. Drug resistance mutations (DRMs) were analyzed using the Stanford University HIV Drug Resistance Database. Results A total of 307 HIV-infected patients with ART failure were included, and 241 available pol sequences were obtained. Among 241 patients, CRF01_AE accounted for 68.88%, followed by CRF07_BC (17.00%) and eight other subtypes (14.12%). The overall prevalence of HIVDR was 61.41%, and the HIVDR against non-nucleoside reverse transcriptase inhibitors (NNRTIs), nucleotide reverse transcriptase inhibitors (NRTIs), and protease inhibitors (PIs) were 59.75%, 45.64%, and 2.49%, respectively. Unemployed patients, hypoimmunity or opportunistic infections in individuals, and samples from 2017 to 2020 increased the odd ratios of HIVDR. Also, HIVDR was less likely to affect female patients. The common DRMs to NNRTIs were K103N (21.99%) and Y181C (20.33%), and M184V (28.21%) and K65R (19.09%) were the main DRMs against NRTIs. Conclusion The present study highlights the HIV-1 subtype diversity in Hainan and the importance of HIVDR surveillance over a long period. -
Key words:
- HIV-1 subtypes /
- Antiretroviral therapy /
- Virological failure /
- Drug resistance
The authors declare no conflicts of interest related to this study.
&These authors contributed equally to this work.
注释:1) AUTHORS’ CONTRIBUTIONS: 2) CONFLICT OF INTEREST: -
Figure 1. The prevalence of virologic failure and drug resistance (DR) over time from 2014 to 2020. PLWH, people living with HIV-1. ART, antiretroviral therapy.
Figure 2. Phylogenetic tree of HIV-1 pol sequences obtained from patients with ART-failure in Hainan Province. The maximum likelihood phylogenetic tree (ML tree) was constructed using 365 HIV-1 pol sequences, including 241 Hainan sequences and 124 reference sequences. A total of 166 HIV-1 CRF01_AE query sequences branched with 47 HIV-1 CRF01_AE reference sequences (dark green color), bootstrap value was 0.98. Forty-one HIV-1 CRF07_BC query sequences branched with 22 reference sequences (dark blue color), bootstrap value was 0.90. Ten HIV-1 CRF55_01B query sequences were identified (dark red color), bootstrap value was 1.0. Eight HIV-1 CRF08_BC (lilac color) and eight HIV-1 CRF65_cpx (deep purple color) query sequences were identified (bootstrap value = 0.97 and 1, respectively) with nine and three reference sequences, respectively. Meanwhile, CRF57_BC (brown color), CRF59_01B (orange color), CRF104_0107 (light blue color), subtype B (blue-green color) and subtype C (bright green color) were detected. The green diamond of tip shape corresponds to Hainan sequences, and red diamond corresponds to reference sequences.
Figure 3. Drug-resistant levels against antiretroviral drugs among ART-failure individuals in Hainan Province from 2014 to 2020. Among the 241 participants, 59.34% acquired high-level drug resistance, 1.24% was intermediate-level drug resistance, and 0.83% was belong to low-level drug resistance (DR). For antiretroviral drugs, 45.29% of patients had DR to ABC, which belongs to NRTIs. About 59% of patients was DR to NVP and EFV belonging to NNRTIs. NRTIs, nucleoside reverse transcriptase inhibitors; NNRTIs, non-nucleoside reverse transcriptase inhibitors; PIs, boosted protease inhibitors. ABC, abacavir; AZT, zidovudine; d4T, sanilvudin; DDI, dideoxynosine; FTC, emtricitabine; 3TC, lamivudine; TDF, tenofovir; DOR, doravirine; EFV, efavirenz; ETR, etravirine; NVP, nevirapine; RPV, rilpivirine; ATV/r, atazanavir with ritonavir; DRV/r, darunavir with ritonavir; FPV/r, fosamprenavir with ritonavir; IDV/r, indinavir with ritonavir; LPV/r, lopinavir with ritonavir; NFV, nelfinavir; SQV/r, saquinavir with ritonavir; TPV/r, tipranavir with ritonavir.
Figure 4. Frequency of drug resistance mutations (DRMs) and drug resistance prevalence among 241 patients with virologic failure after ART in Hainan Province, 2014–2020. (A) Frequency of DRMs to nucleoside reverse transcriptase inhibitors (NRTIs). (B) Frequency of DRMs to non-nucleoside reverse transcriptase inhibitors (NNRTIs). (C) Frequency of DRMs to boosted protease inhibitors (PIs). (D) Drug resistance prevalence by ART drugs.
Table 1. Characteristics of HIV-infected patients with virologic failure from 2014 to 2020 in Hainan Province, China
Variables Number (N) Percent (%) Total 241 100 Sex Female 40 16.60 Male 201 83.40 Age, years: median 32, IQR (26, 42) 19−29 97 40.25 30−39 73 30.29 40−49 39 16.18 ≥ 50 32 13.28 Marital Status Married and cohabiting 78 32.37 Single 163 67.63 Ethnics Han 203 84.23 Others 32 13.28 Unknown 6 2.49 Region Northern Hainan 92 38.17 Eastern Hainan 22 9.13 Southern Hainan 63 26.14 Western Hainan 39 16.18 Central Hainan 25 10.37 Education Primary school or lower 46 19.09 Secondary school 99 41.08 High school or above 90 37.34 Unknown 6 2.49 Occupation Farmer 83 34.44 Unemployment 64 26.56 Others 79 32.78 Unknown 15 6.22 Risk factors Homosexual 86 35.68 Heterosexual 119 49.38 Others 36 14.94 Sampling time, year 2014−2016 57 23.65 2017−2020 187 77.59 Basic line CD4 cell count, cells/mm3: median 195, IQR: 80–324 < 200 120 49.79 200−350 70 29.05 301−500 24 9.96 > 500 18 7.47 Unknown 9 3.73 HIV-1 subtype CRF01_AE 166 68.88 CRF07_BC 41 17 Other (B/C/CRF08_BC/CRF59_01B/CRF55_01B/CRF65_cpx /CRF57_BC/CRF104_0107) 34 14.12 Initial therapeutic regimen AZT+3TC+EFV/NVP 64 26.56 TDF+3TC+EFV/NVP 162 67.22 Others 15 6.22 Hypoimmunity or opportunistic infections Yes 76 31.54 No 165 68.46 The duration from diagnosis to ART, month: median 3, IQR: 0–20.5 < 7 151 62.66 ≥ 7 90 37.34 Time on ART, month: median 20, IQR: 10–39.5 < 13 82 34.02 13−25 58 24.07 > 25 101 41.91 Co-infection hepatitis B Yes 34 14.11 No 127 52.70 Unknown 80 33.20 Co-infection hepatitis C Yes 30 12.45 No 112 46.47 Unknown 99 41.08 Viral load, log10 copies/mL Viral load median: 32,529 copies/mL, IQR: 9,071−101,453 copies/mL 4.00−4.99 116 48.13 ≥ 5.00 62 25.73 ≤ 3.99 63 26.14 Note. IQR, interquartile range; ART, antiretroviral therapy; CRF, circulating recombinant form; AZT, zidovudine; 3TC, lamivudine; EFV, efavirenz; NVP, nevirapine; TDF, tenofovir.  下载: 导出CSV
下载: 导出CSV
Table 2. Factors associated with drug resistance among HIV-1 patients with virologic failure from 2014 to 2020 in Hainan Province, China
Variables N Drug resistance Univariate Multivariate Number (N) Percent (%) χ2 P1 aOR (95% CI) P2 Total 241 148 61.41 Sex Male 201 113 66.17 11.571 0.001 Ref. Female 40 15 37.50 0.11 (0.03, 0.38) 0.001 Ages, years 0.077 19−29 97 67 69.07 15.587 0.001 Ref. 30−39 73 50 68.49 1.31 (0.49, 3.46) 0.590 40−49 39 14 35.90 0.27 (0.08, 0.94) 0.039 ≥ 50 32 17 53.13 0.51 (0.13, 2.05) 0.343 Marital status Single 163 109 66.87 6.336 0.012 Ref. Married and cohabiting 78 39 50.00 0.53 (0.21, 1.32) 0.172 Ethnics Han 203 123 60.59 2.450 0.118a Ref. Others 32 24 75.00 3.386 0.083 Unknown 6 1 16.67 Region 0.467 Central Hainan 25 12 48.00 4.128 0.389 Ref. Northern Hainan 92 59 64.13 1.87 (0.45, 7.75) 0.39 Eastern Hainan 22 11 50.00 0.63 (0.11, 3.75) 0.61 Southern Hainan 63 42 66.67 2.09 (0.45, 9.76) 0.347 Western Hainan 39 24 61.54 2.08 (0.39, 11.20) 0.394 Education 0.183 Primary school or lower 46 26 56.52 1.061 0.588a Ref. Secondary school 99 62 62.63 1.34 (0.45, 4.01) 0.607 High School or above 90 59 65.56 0.48 (0.12, 1.87) 0.291 Unknown 6 1 16.67 Occupation 0.034 Farmer 83 48 57.83 4.873 0.087a Ref. Unemployment 64 48 75.00 4.32 (1.38, 13.51) 0.012 Others 79 49 62.03 1.51 (0.54, 4.19) 0.433 Unknown 15 3 20.00 Risk factors 0.321 Homosexual 86 63 73.26 10.685 0.005 Ref. Heterosexual 119 61 51.26 0.54 (0.17, 1.66) 0.282 Others 36 24 66.67 0.24 (0.04, 1.68) 0.152 Sampling time, year 2014−2016 57 35 61.40 < 0.001 0.999 Ref. 2017−2020 187 116 62.03 3.26 (1.12, 9.47) 0.030 Basic line CD4 cell count, cells/mm3 0.419 < 200 120 86 71.67 15.914 0.001a Ref. 200−350 70 38 54.29 0.44 (0.14, 1.34) 0.148 301−500 24 13 54.17 0.42 (0.10, 1.82) 0.246 > 500 18 5 27.78 0.35 (0.07, 1.83) 0.214 Unknown 9 6 66.67 HIV-1 subtype 0.001 CRF01_AE 166 115 69.28 17.634 < 0.001 Ref. CRF07_BC 41 14 34.14 0.14 (0.05, 0.40) < 0.001 Others 34 19 55.88 0.26 (0.07, 0.88) 0.031 Initial therapeutic regimen 0.006 AZT+3TC+EFV/NVP 64 43 67.19 1.230 0.541 Ref. TDF+3TC+EFV/NVP 162 96 59.26 0.15 (0.04, 0.48) 0.002 Others 15 9 60.00 0.46 (0.07, 2.92) 0.410 Hypoimmunity or opportunistic infections Yes 76 60 78.95 14.405 < 0.001 Ref. No 165 88 53.33 0.32 (0.10, 0.99) 0.049 The duration from diagnosis to ART, month < 7 151 93 61.59 0.005 0.941 Ref. ≥ 7 90 55 61.11 0.87 (0.34, 2.24) 0.769 Time on ART, month 0.610 < 13 82 53 64.63 0.594 0.743 Ref. 13−25 58 34 58.62 0.89 (0.29, 2.72) 0.843 > 25 101 61 60.40 0.60 (0.21, 1.74) 0.348 Co-infection hepatitis B 0.689 Yes 34 21 61.76 0.003 0.999 Ref. No 127 78 61.42 0.59 (0.17, 2.07) 0.407 Unknown 80 49 61.25 0.61 (0.15, 2.56) 0.501 Co-infection hepatitis C 0.361 Yes 30 18 60.00 0.108 0.947 Ref. No 112 70 62.50 0.29 (0.05, 1.59) 0.155 Unknown 99 60 60.61 0.35 (0.06, 2.13) 0.256 Viral load, log10 copies/mL 0.935 4.00−4.99 116 69 59.48 2.317 0.314 Ref. ≥ 5.00 62 43 69.35 0.97 (0.36, 2.65) 0.955 ≤ 3.99 63 36 57.14 0.84 (0.33, 2.14) 0.717 Note. aOR, adjusted odd ratio; ART, antiretroviral therapy; CRF, circulating recombinant form; AZT, zidovudine; 3TC, lamivudine; EFV, efavirenz; NVP, nevirapine; TDF, tenofovir; P1, significant values of univariate analysis; P2, significant values of multivariate logistic regression analysis; a, among the corresponding independent variables, the number of the last group is too small to be included in the analysis.
下载: 导出CSV
-
[1] Thompson MA, Aberg JA, Hoy JF, et al. Antiretroviral treatment of adult HIV infection: 2012 recommendations of the international antiviral society–USA panel. JAMA, 2012; 308, 387−402. [2] Cohen MS, Chen YQ, McCauley M, et al. Antiretroviral therapy for the prevention of HIV-1 transmission. N Engl J Med, 2016; 375, 830−9. doi: 10.1056/NEJMoa1600693 [3] Zhao DC, Wen Y, Ma Y, et al. Expansion of China’s free antiretroviral treatment program. Chin Med J, 2012; 129, 3514−21. [4] China M O H O. Guidelines for diagnosis and treatment of AIDS. Word Clin Drugs, 2005; 26, 454−9. (In Chinese [5] Zhang FJ, Zhao Y, Ma Y, et al. Progress and achievements of free antiretroviral treatment for AIDS in China. Chin J AIDS STD, 2022; 28, 6−9. (In Chinese [6] Hao Y, Chen QF, Han MJ, et al. The initiation and development of free antiretroviral treatment for AIDS in China - a path of antiretroviral treatment with Chinese characteristics. Chin J AIDS STD, 2022; 28, 1−5. (In Chinese [7] Blassel L, Zhukova A, Villabona-Arenas CJ, et al. Drug resistance mutations in HIV: new bioinformatics approaches and challenges. Curr Opin Virol, 2021; 51, 56−64. doi: 10.1016/j.coviro.2021.09.009 [8] Zuo LL, Liu K, Liu HL, et al. Trend of HIV-1 drug resistance in China: a systematic review and meta-analysis of data accumulated over 17 years (2001-2017). eClinicalMedicine, 2020; 18, 100238. doi: 10.1016/j.eclinm.2019.100238 [9] Guo CX, Wu YX, Zhang Y, et al. Transmitted drug resistance in antiretroviral therapy-naive persons with acute/early/primary HIV infection: a systematic review and meta-analysis. Front Pharmacol, 2021; 12, 718763. doi: 10.3389/fphar.2021.718763 [10] Lan Y, Deng XZ, Li LH, et al. HIV-1 drug resistance and genetic transmission networks among MSM failing antiretroviral therapy in South China 2014-2019. Infect Drug Resist, 2021; 14, 2977−89. doi: 10.2147/IDR.S317187 [11] Zou XB, He JM, Zheng J, et al. Prevalence of acquired drug resistance mutations in antiretroviral- experiencing subjects from 2012 to 2017 in Hunan Province of central South China. Virol J, 2020; 17, 38. doi: 10.1186/s12985-020-01311-3 [12] Lu XL, Zhao HR, Zhang YQ, et al. HIV-1 drug-resistant mutations and related risk factors among HIV-1-positive individuals experiencing treatment failure in Hebei Province, China. AIDS Res Ther, 2017; 14, 4. doi: 10.1186/s12981-017-0133-3 [13] Gardner EM, Burman WJ, Steiner JF, et al. Antiretroviral medication adherence and the development of class-specific antiretroviral resistance. AIDS, 2009; 23, 1035−46. doi: 10.1097/QAD.0b013e32832ba8ec [14] Zhang FD, Liu L, Sun MY, et al. An analysis of drug resistance among people living with HIV/AIDS in Shanghai, China. PLoS One, 2017; 12, e0165110. doi: 10.1371/journal.pone.0165110 [15] Yan LT, Yu FT, Liang JM, et al. Drug resistance profiles and influencing factors among HIV-infected children and adolescents receiving long-term ART: a multicentre observational study in China. J Antimicrob Chemother, 2022; 77, 727−34. doi: 10.1093/jac/dkab430 [16] Musema GMA, Akilimali PZ, Za Balega TKN, et al. Predictive factors of HIV-1 drug resistance and its distribution among female sex workers in the Democratic Republic of the Congo (DRC). Int J Environ Res Public Health, 2022; 19, 2021. doi: 10.3390/ijerph19042021 [17] Omooja J, Nannyonjo M, Sanyu G, et al. Rates of HIV-1 virological suppression and patterns of acquired drug resistance among fisherfolk on first-line antiretroviral therapy in Uganda. J Antimicrob Chemother, 2019; 74, 3021−9. doi: 10.1093/jac/dkz261 [18] WHO. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: recommendations for a public health approach. 2nd ed. WHO. 2016. [19] Zhao ZY. The analysis of the willingness to reside of Hainan's floating population and it's influencing factors. Jilin University. 2020. (In Chinese) [20] Wang Y. A study on the health problems and the influencing factors of climate migrant population in winter in Sanya city. Chinese Center for Disease Control and Prevention. 2017. (In Chinese) [21] Feng YT, Xu YJ, Ma YR, et al. Epidemiology characteristics among HIV/AIDS patients receiving initial antiretroviral therapy in Hainan, 2005-2019. China Trop Med, 2021; 21, 681−5. (In Chinese [22] Zeng XM, Fu P, Wang ZQ, et al. Analysis on the characteristics and transmission routes of AIDS epidemic in Hainan. China Trop Med, 2020; 20, 735−8. (In Chinese [23] Ma J, Tong X, Hui S, et al. Analysis on HIV/AIDS Epidemic Situation in HeiLongJiang Province From 2012 to 2017. Harbin Med J, 2018; 38, 222−4. (In Chinese [24] Yu L, Hui S, Li T, et al. Epidemiological characteristics of AIDS patients receiving free antiviral treatment for the first in Heilongjiang, 2014-2018. Chin J Public Health Manag, 2019; 35, 375−7. (In Chinese [25] Zhou JL, Wang L, Zhou D, et al. Prevalence characteristics of HIV/AIDS in Liaoning province, 1993 to 2015. Chin J Public Health, 2017; 33, 1209−12. (In Chinese [26] Chen RF, Liang BY, Wen BB, et al. No difference in prevalence of transmitted drug resistance between injection drug users and non-injection drug users: a cross-sectional study among antiretroviral treatment-naïve HIV patients. Intervirology, 2018; 61, 281−91. doi: 10.1159/000499367 [27] Dou ZZ, Zhang FJ, Zhao Y, et al. Progress on China’s national free antiretroviral therapy strategy in 2002-2014. Chin J Epidemiol, 2015; 36, 1345−50. (In Chinese [28] Kyaw NTT, Harries AD, Kumar AMV, et al. High rate of virological failure and low rate of switching to second-line treatment among adolescents and adults living with HIV on first-line ART in Myanmar, 2005-2015. PLoS One, 2017; 12, e0171780. doi: 10.1371/journal.pone.0171780 [29] Tran DA, Wilson DP, Shakeshaft A, et al. Determinants of virological failure after 1 year's antiretroviral therapy in Vietnamese people with HIV: findings from a retrospective cohort of 13 outpatient clinics in six provinces. Sex Transm Infect, 2014; 90, 538−44. doi: 10.1136/sextrans-2013-051353 [30] Bulage L, Ssewanyana I, Nankabirwa V, et al. Factors associated with virological non-suppression among HIV-positive patients on antiretroviral therapy in Uganda, August 2014-July 2015. BMC Infect Dis, 2017; 17, 326. doi: 10.1186/s12879-017-2428-3 [31] Alave J, Paz J, González E, et al. Risk factors associated with virologic failure in HIV- infected patients receiving antiretroviral therapy at a public hospital in Peru. Rev Chilena Infectol, 2013; 30, 42−8. doi: 10.4067/S0716-10182013000100006 [32] Louis FJ, Buteau J, François K, et al. Virologic outcome among patients receiving antiretroviral therapy at five hospitals in Haiti. PLoS One, 2018; 13, e0192077. doi: 10.1371/journal.pone.0192077 [33] Deng W, Fu P, Bao LL, et al. Molecular epidemiological tracing of HIV-1 outbreaks in Hainan island of southern China. AIDS, 2009; 23, 977−85. doi: 10.1097/QAD.0b013e328329217d [34] Chu MJ, Zhang WH, Zhang X, et al. HIV-1 CRF01_AE strain is associated with faster HIV/AIDS progression in Jiangsu Province, China. Sci Rep, 2017; 7, 1570. doi: 10.1038/s41598-017-01858-2 [35] Jordan MR, Bennett DE, Wainberg MA, et al. Update on World Health Organization HIV drug resistance prevention and assessment strategy: 2004-2011. Clin Infect Dis, 2012; 54 Suppl 4, S245-9. [36] Dong K, Ye L, Leng Y, et al. Prevalence of HIV-1 drug resistance among patients with antiretroviral therapy failure in Sichuan, China, 2010-2016. Tohoku J Exp Med, 2019; 247, 1−12. doi: 10.1620/tjem.247.1 [37] Zuo ZB, Liang S, Sun XG, et al. Drug resistance and Virological failure among HIV-infected patients after a decade of antiretroviral treatment expansion in eight provinces of China. PLoS One, 2016; 11, e0166661. doi: 10.1371/journal.pone.0166661 [38] Chimukangara B, Lessells RJ, Singh L, et al. Acquired HIV drug resistance and virologic monitoring in a HIV hyper-endemic setting in KwaZulu-Natal Province, South Africa. AIDS Res Ther, 2021; 18, 74. doi: 10.1186/s12981-021-00393-5 [39] Santos-Pereira A, Triunfante V, Araujo PMM, et al. Nationwide study of drug resistance mutations in HIV-1 infected individuals under antiretroviral therapy in Brazil. Int J Mol Sci, 2021; 22, 5304. doi: 10.3390/ijms22105304 [40] Arimide DA, Amogne MD, Kebede Y, et al. High level of HIV drug resistance and Virologic Nonsuppression among female sex workers in Ethiopia: a nationwide cross-sectional study. J Acquir Immune Defic Syndr, 2022; 89, 566−74. doi: 10.1097/QAI.0000000000002908 [41] Shchemelev AN, Ostankova YV, Zueva EB, et al. Detection of patient HIV-1 drug resistance mutations in Russia's northwestern federal district in patients with treatment failure. Diagnostics, 2022; 12, 1821. doi: 10.3390/diagnostics12081821 [42] Cauldbeck MB, O'connor C, O'connor MB, et al. Adherence to anti-retroviral therapy among HIV patients in Bangalore, India. AIDS Res Ther, 2009; 6, 7. doi: 10.1186/1742-6405-6-7 [43] Suryana K, Suharsono H, Antara IGPJ. Factors associated with adherence to anti-retroviral therapy among people living with HIV/AIDS At Wangaya hospital in Denpasar, Bali, Indonesia: a cross-sectional study. HIV AIDS, 2019; 11, 307−12. [44] Etiebet MAA, Shepherd J, Nowak RG, et al. Tenofovir-based regimens associated with less drug resistance in HIV-1-infected Nigerians failing first-line antiretroviral therapy. AIDS, 2013; 27, 553−61. doi: 10.1097/QAD.0b013e32835b0f59 [45] Margot N, Lu B, Cheng A, et al. Resistance development over 144 weeks in treatment-naive patients receiving tenofovir disoproxil fumarate or stavudine with lamivudine and efavirenz in Study 903. HIV Med, 2006; 7, 442−50. doi: 10.1111/j.1468-1293.2006.00404.x [46] Guo XL, Zhang F, Liu XX, et al. Analysis of HIV-1 genotype resistance test of HIV antiviral therapy failures, 2019-2020, in Shanxi province. Chin J Exp Clin Virol, 2022; 36, 176−82. (In Chinese [47] Henerico S, Mikasi SG, Kalluvya SE, et al. Prevalence and patterns of HIV drug resistance in patients with suspected virological failure in North-Western Tanzania. J Antimicrob Chemother, 2022; 77, 483−91. doi: 10.1093/jac/dkab406 [48] Scriven YA, Mulinge MM, Saleri N, et al. Prevalence and factors associated with HIV-1 drug resistance mutations in treatment-experienced patients in Nairobi, Kenya: A cross-sectional study. Medicine, 2021; 100, e27460. doi: 10.1097/MD.0000000000027460 [49] Yu DE, Liang BY, Yang Y, et al. Prevalence of drug resistance and genetic transmission networks among human immunodeficiency virus/acquired immunodeficiency syndrome patients with antiretroviral therapy failure in Guangxi, China. AIDS Res Hum Retroviruses, 2022; 38, 822−30. doi: 10.1089/aid.2021.0181 [50] La Rosa AM, Harrison LJ, Taiwo B, et al. Raltegravir in second-line antiretroviral therapy in resource-limited settings (SELECT): a randomised, phase 3, non-inferiority study. Lancet HIV, 2016; 3, e247−58. doi: 10.1016/S2352-3018(16)30011-X [51] Reuman EC, Rhee SY, Holmes SP, et al. Constrained patterns of covariation and clustering of HIV-1 non-nucleoside reverse transcriptase inhibitor resistance mutations. J Antimicrob Chemother, 2010; 65, 1477−85. doi: 10.1093/jac/dkq140 [52] Melikian GL, Rhee SY, Varghese V, et al. Non-nucleoside reverse transcriptase inhibitor (NNRTI) cross-resistance: implications for preclinical evaluation of novel NNRTIs and clinical genotypic resistance testing. J Antimicrob Chemother, 2014; 69, 12−20. doi: 10.1093/jac/dkt316 [53] CDC. National free AIDS ART guideline. 4th ed. People's Health Publishing House. 2016. (In Chinese) [54] Kulkarni R, Babaoglu K, Lansdon EB, et al. The HIV-1 reverse transcriptase M184I mutation enhances the E138K-associated resistance to Rilpivirine and decreases viral fitness. J Acquir Immune Defic Syndr, 2012; 59, 47−54. [55] Ross L, Parkin N, Chappey C, et al. Phenotypic impact of HIV reverse transcriptase M184I/V mutations in combination with single thymidine analog mutations on nucleoside reverse transcriptase inhibitor resistance. AIDS, 2004; 18, 1691−6. doi: 10.1097/01.aids.0000131355.44834.e4 [56] Gagliardini R, Ciccullo A, Borghetti A, et al. Impact of the M184V resistance mutation on Virological efficacy and durability of lamivudine-based dual antiretroviral regimens as maintenance therapy in individuals with suppressed HIV-1 RNA: a cohort study. Open Forum Infect Dis, 2018; 5, ofy113. doi: 10.1093/ofid/ofy113 [57] Petropoulos CJ, Parkin NT, Limoli KL, et al. A novel phenotypic drug susceptibility assay for human immunodeficiency virus type 1. Antimicrob Agents Chemother, 2000; 44, 920−8. doi: 10.1128/AAC.44.4.920-928.2000 [58] Ayitewala A, Kyeyune F, Ainembabazi P, et al. Comparison of HIV drug resistance profiles across HIV-1 subtypes A and D for patients receiving a tenofovir-based and zidovudine-based first line regimens in Uganda. AIDS Res Ther, 2020; 17, 2. doi: 10.1186/s12981-020-0258-7 [59] Zaccarelli M, Tozzi V, Lorenzini P, et al. Multiple drug class-wide resistance associated with poorer survival after treatment failure in a cohort of HIV-infected patients. AIDS, 2005; 19, 1081−9. doi: 10.1097/01.aids.0000174455.01369.ad [60] Lombardi F, Giacomelli A, Armenia D, et al. Prevalence and factors associated with HIV-1 multi-drug resistance over the past two decades in the Italian ARCA database. Int J Antimicrob Agents, 2021; 57, 106252. doi: 10.1016/j.ijantimicag.2020.106252 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 675
- HTML全文浏览量: 304
- PDF下载量: 66
- 被引次数: 0

 Quick Links
Quick Links