

 下载:
下载:



-
Low birth weight (LBW) is defined as a birth weight of less than 2,500 g. It has been estimated that 15%–20% of infants (more than 20 million worldwide) were born with LBW, and 95.6% of the overall LBW infants were born in low and middle income countries[1]. Not only is LBW a crucial cause of infant mortality and morbidity, it also plays a critical role in adverse health outcomes later in life. Therefore, exploring the factors influencing LBW may have important implications for reducing maternal-child health burden.
In recent years, the global climate has been undergoing drastic changes. Pregnant women are susceptible to extreme temperature due to their hormone-related physiological changes and variations in immunity and mood[2]. Although the risk of LBW in relation to prenatal exposures to temperature has been studied previously, the findings are inconsistent due to heterogeneity in the socio-economic and environmental factors of different regions[3]. Therefore, it is necessary to explore the effects of meteorological conditions on LBW risk in specific regions.
Henan Province is an agricultural province with a rural population of 49 million people, a poor economic status, and few medical services. We speculated that the health burden of LBW in rural Henan would be heavier than that in other regions. Therefore, exploring the association between prenatal ambient temperature exposure and LBW is critical to protect public health, especially in vulnerable regions. Our study analyzed the effects of ambient temperature exposure during pregnancy on LBW and identified individual risk factors in order to provide a scientific basis for formulating policies to reduce the prevalence of LBW in rural areas.
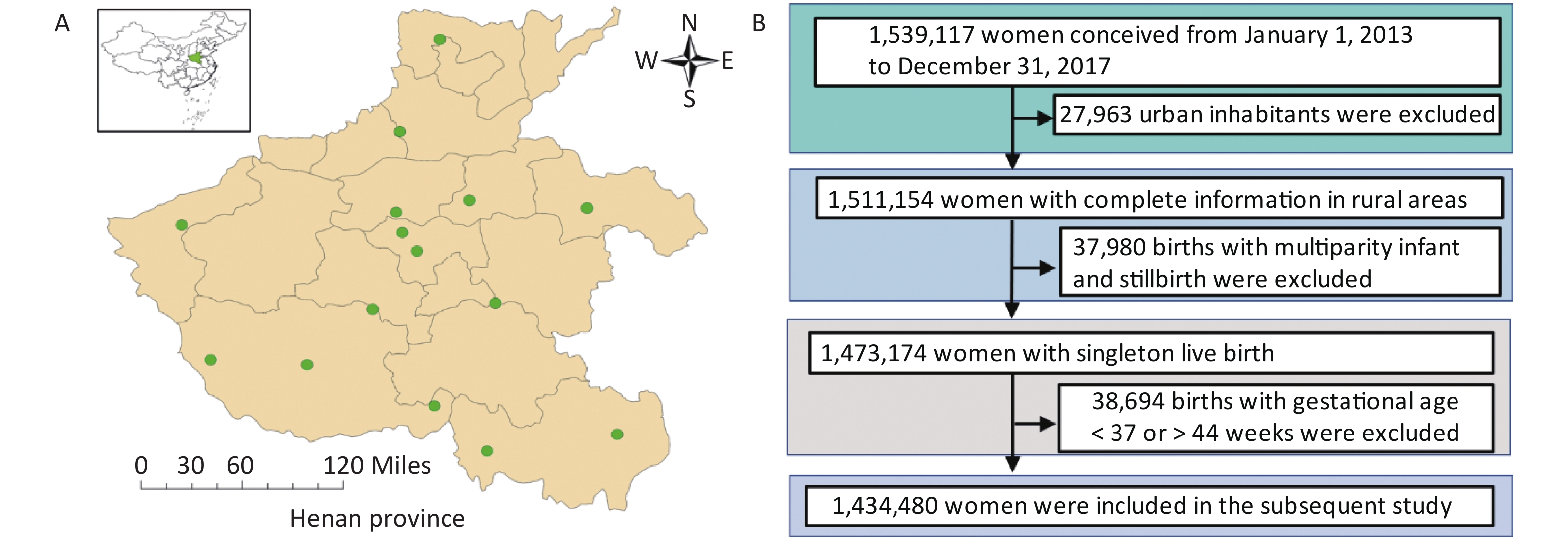
We obtained the medical records of mothers (n = 1,539,117) who conceived and gave birth between 2013 to 2017 from the National Free Preconception Health Examination Project (NFPHEP) in rural Henan. People registered as residing in urban areas, having multiple births, stillbirths, or births with gestational weeks less than 37 weeks or more than 44 weeks, were excluded. Finally, a total of 1,434,480 medical records were included in our subsequent study (Supplementary Figure S1 available in www.besjournal.com). Infants with a birth weight less than 2,500 g and gestational age between 37 weeks to 44 weeks were defined as LBW. The study design was approved by the Ethical Committee of the Henan Institute of Reproduction Health Science and Technology (HIRHST-IRB2020-02), and all participants provided written informed consent. The private information was de-identified to protect the privacy of participants.
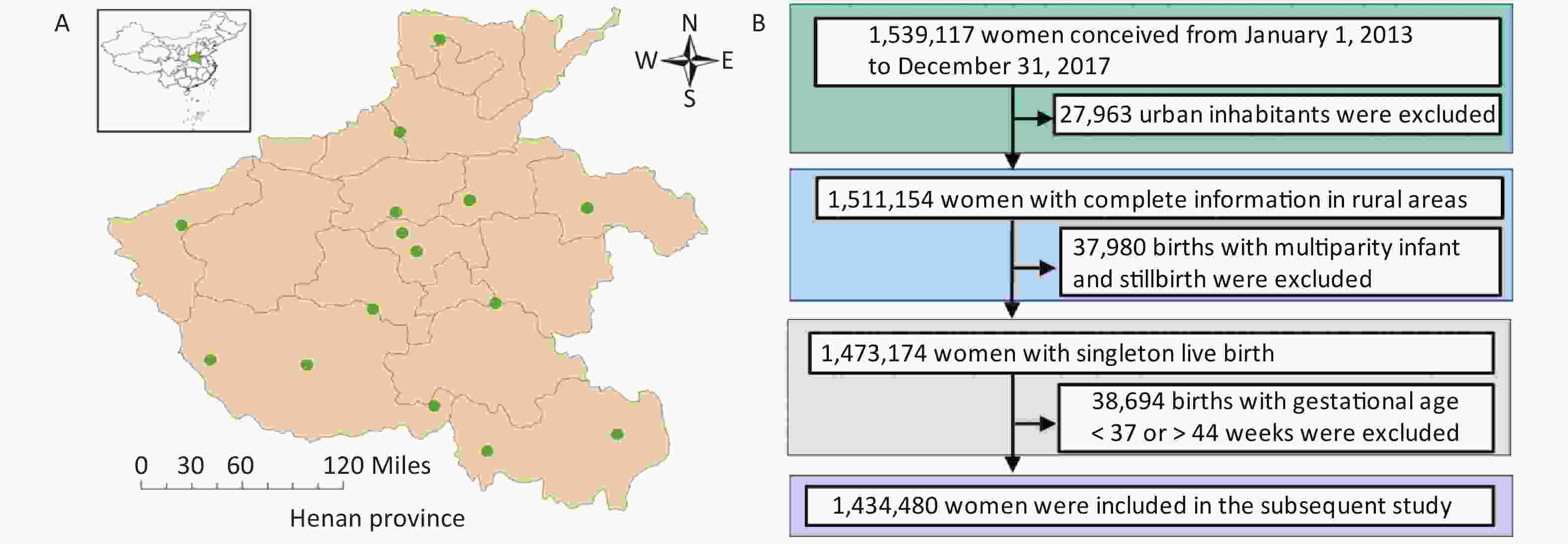
Figure S1. Spatial distribution of the study area and national meteorological stations (A), and a flow chart of the inclusion and exclusion criteria for the final study population (B).
Meteorological data, including daily mean temperature (°C) and relative humidity (%), were obtained from the China Meteorological Data Sharing Service System (
http://data.cma.cn/ ) from 15 national meteorological stations in Henan Province (Supplementary Figure S1). An inverse distance–weighted (IDW) model was used to evaluate individual daily exposure levels, similar to previous studies[4]. The weekly meteorological exposure level of each pregnant woman was calculated according to their daily exposure levels (Supplementary Table S1, available in www.besjournal.com). Then, the entire pregnancy was divided into three trimesters, including the first trimester (1–12 gestational weeks), the second trimester (13–27 gestational weeks), and the third trimester (28 gestational weeks to delivery). Extreme temperature exposure during the entire pregnancy and each trimester was defined based on all participants: “extreme cold” (< 10th percentile), “extreme heat” (> 90th percentile), and “moderate” (10th to 90th percentile).Table S1. Characteristics of mean temperature (°C) and relative humidity (%) during pregnancy by exposure period
Item x s Min 10th M 90th Max Mean temperature (°C) Trimester 1 16.44 7.88 2.09 4.51 17.84 25.96 28.46 Trimester 2 15.98 7.88 2.98 4.97 16.88 25.33 27.55 Trimester 3 14.31 8.00 1.63 4.12 13.98 25.38 28.41 Entire pregnancy 15.58 2.61 10.93 12.17 15.51 19.01 20.87 Relative humidity (%) Trimester 1 66.63 7.07 49.97 57.18 66.40 75.81 79.66 Trimester 2 67.29 6.65 53.42 57.82 68.35 75.20 78.81 Trimester 3 66.38 7.25 48.53 56.17 66.57 75.45 80.70 Entire pregnancy 66.79 2.47 60.71 63.49 66.42 70.66 72.52 Pearson's chi-square tests were used to compare the demographic characteristics between LBW and normal birth weight groups. The association between mean temperature exposure during pregnancy and the risk of LBW was first examined using a restricted cubic spline (RCS) model. Then, a logistic regression model was used to calculate the odds ratio (OR) and 95% confidence interval (CI) of the association between ambient temperature exposure during pregnancy and the risk of LBW. Finally, interaction analysis (by adding interaction terms of exposure to extreme temperature and subgroups of demographic characteristics into the regression model) was used to explore whether demographic characteristics could modify the relationship between exposure to extreme temperature during pregnancy and the risk of LBW. The statistical analysis was conducted in R 3.6.2 (R, Vienna, Austria) to analyze the database (MySQL). The significance level for interaction analysis was defined as 0.10, and the remaining P
-values were considered significant at 0.05. In this study, the incidence of LBW is 0.4% (n = 5,790) (see Table 1). A similar retrospective cohort study in rural China reported that the incidence of LBW was 4.54% during weeks 22–44 of gestation[5]. However, preterm births (less than 37 weeks gestation) are often accompanied by LBW, but the prevention and treatment are different compared to term infants. Therefore, the present study sample was limited to term infants with more than 36 weeks gestation. In addition, due to a shift in national policies, the living standards in rural areas have improved significantly, excess nutrition in rural areas might be another reason for the low proportion of LBW among term infants.
Table 1. Demographic characteristics of the study sample
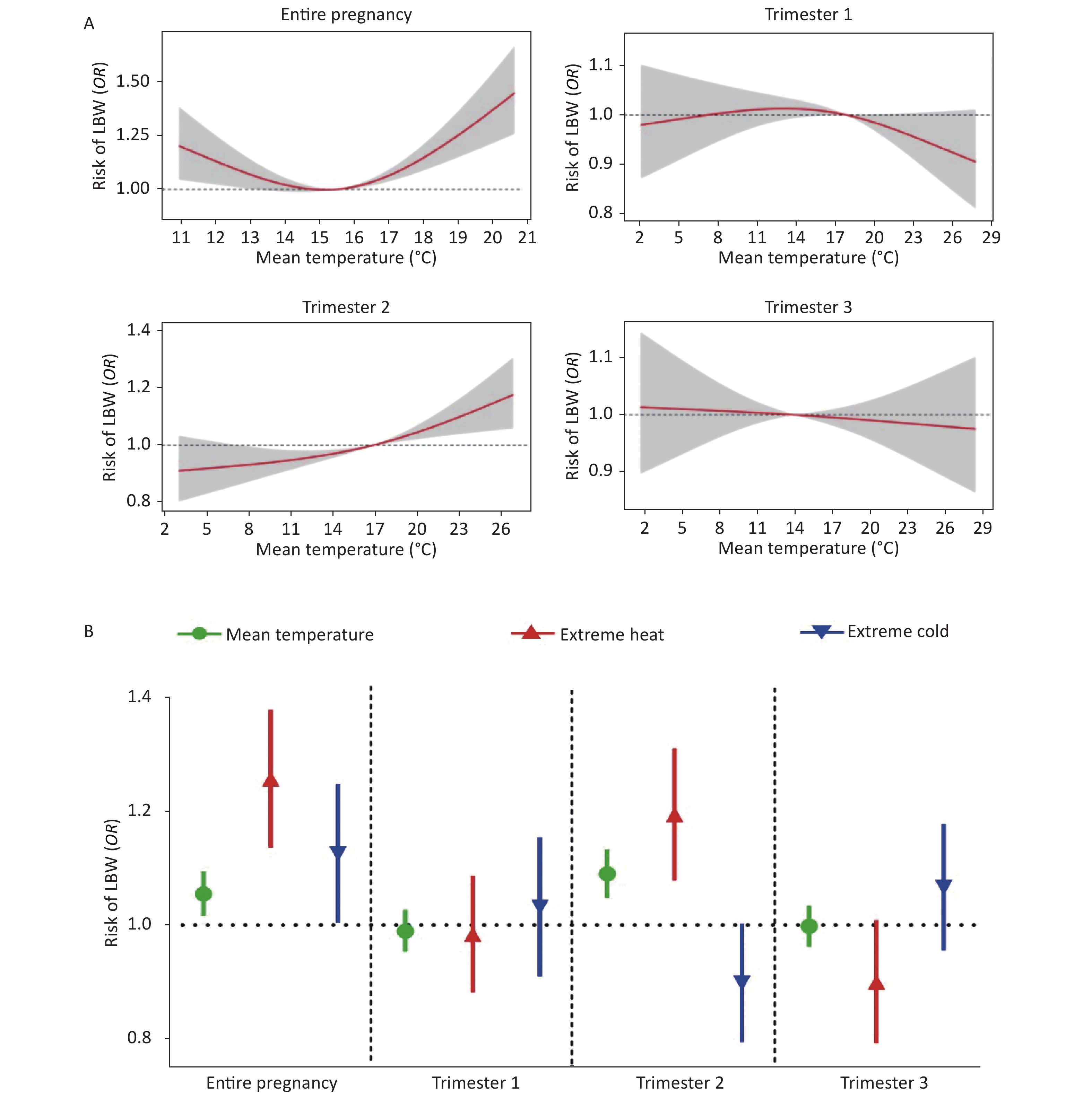
Variables Low birth weight, n (%) Normal birth weight, n (%) P n 5,790 1,428,690 Mothers Age < 0.001 < 30 4,549 (78.6) 1,170,340 (81.9) ≥ 30 1,241 (21.4) 258,350 (18.1) Pre-pregnancy BMI (kg/m2) < 0.001 < 18.5 (lean) 622 (10.7) 122,238 (8.6) 18.5–23.9 (normal) 4,068 (70.3) 1,044,199 (73.0) ≥ 24 (overweight/obesity) 1,100 (19.0) 262,253 (18.4) Education 0.292 Middle school or below 4,184 (72.3) 1,041,226 (72.9) High school or above 1,606 (27.7) 387,464 (27.1) Smoking < 0.001 Yes 396 (6.8) 83,145 (5.8) No 5,394 (93.2) 1,345,545 (94.2) Alcohol consumption 0.584 Yes 36 (0.6) 8,235 (0.6) No 5,754 (99.4) 1,420,455 (99.4) Parity 0.009 Primi-parity 3,587 (61.9) 863,529 (60.4) Multi-parity 2,203 (38.1) 565,161 (39.6) Newborns Sex < 0.001 Male 2,006 (34.7) 730,228 (51.1) Female 3,784 (65.3) 698,462 (48.9) The dose-response relationships between LBW and ambient temperature during pregnancy are shown in Figure 1A. After adjusting for the confounding factors, a U-shaped association between mean ambient temperature during the entire pregnancy and LBW was observed (Pnon-linear < 0.001). As a potential mechanism, elevated ambient temperature may reduce a pregnant woman’s ability to dissipate body heat, resulting in increased core body temperature, which may cause shunting of blood to the body surface and also lead to placental hypoperfusion[6]. Then, impaired nutrient and oxygen supply leads to disorders of placental function, thus affecting the growth and development of the fetus. For the effects of exposure to extreme cold on LBW risk, a few studies have suggested that low ambient temperature was associated with peripheral vasoconstriction and increased blood viscosity, which might reduce placental perfusion and result in adverse effects on the developing fetus[7].
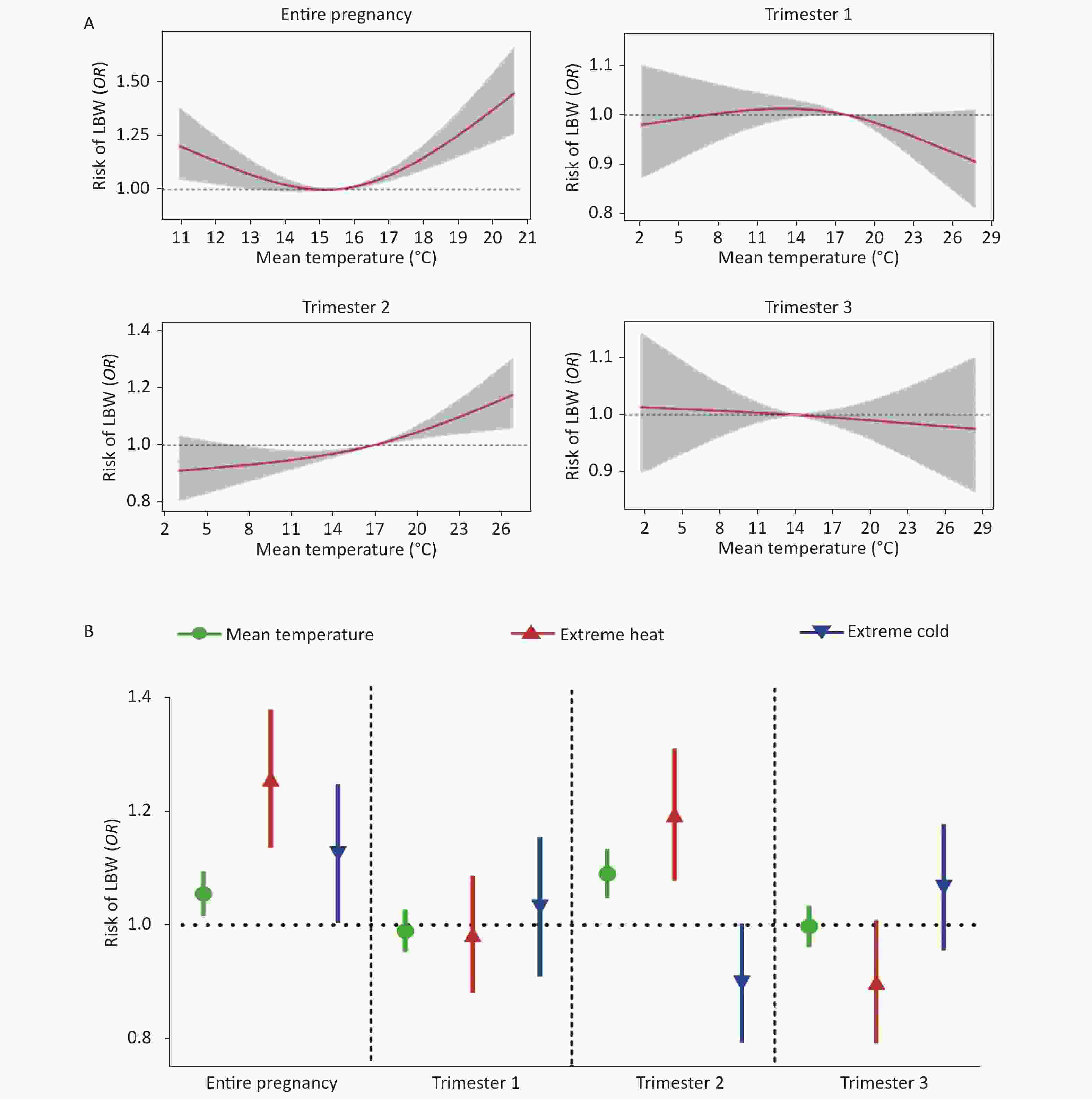
Figure 1. The dose-response relationships between the risk of LBW and mean ambient temperature during pregnancy (A). The association between the risk of LBW and exposure to ambient temperature during pregnancy (B). Models were adjusted for relative humidity, maternal age, pre-pregnancy BMI, education level, smoking status, alcohol consumption, parity, and the sex of the newborn.
A logistic regression model was used to evaluate the effects of ambient temperature on the risk of LBW. The risk of LBW was positively associated with each standard deviation unit increment in mean ambient temperature during the entire pregnancy (OR = 1.054, 95% CI: 1.016–1.094), especially during the second trimester (OR = 1.089, 95% CI: 1.048–1.133; Figure 1B), which was consistent with several previous studies. Exposure to mean temperature during the second trimester was negatively associated with placental weight and volume, which indicates that the second trimester may be a critical period for heat stress to have adverse effects on placental transport efficiency, resulting in the occurrence of LBW infants[6]. Compared to moderate ambient temperature exposures, exposure to extreme heat resulted in a 25.3% increased LBW risk, while exposure to extreme cold increased LBW risk by 12.1% (Figure 1B). Furthermore, exposure to extreme heat in the second trimester increased the risk of LBW (OR = 1.190, 95% CI: 1.080–1.312; Figure 1B). Pregnant women in rural areas generally took measures to keep warm in cold environments (e.g., burning fuels and donning additional clothing), which might partly reduce the risk of LBW caused by exposure to extreme cold. Notably, the utilization of air conditioners is relatively low in rural areas (
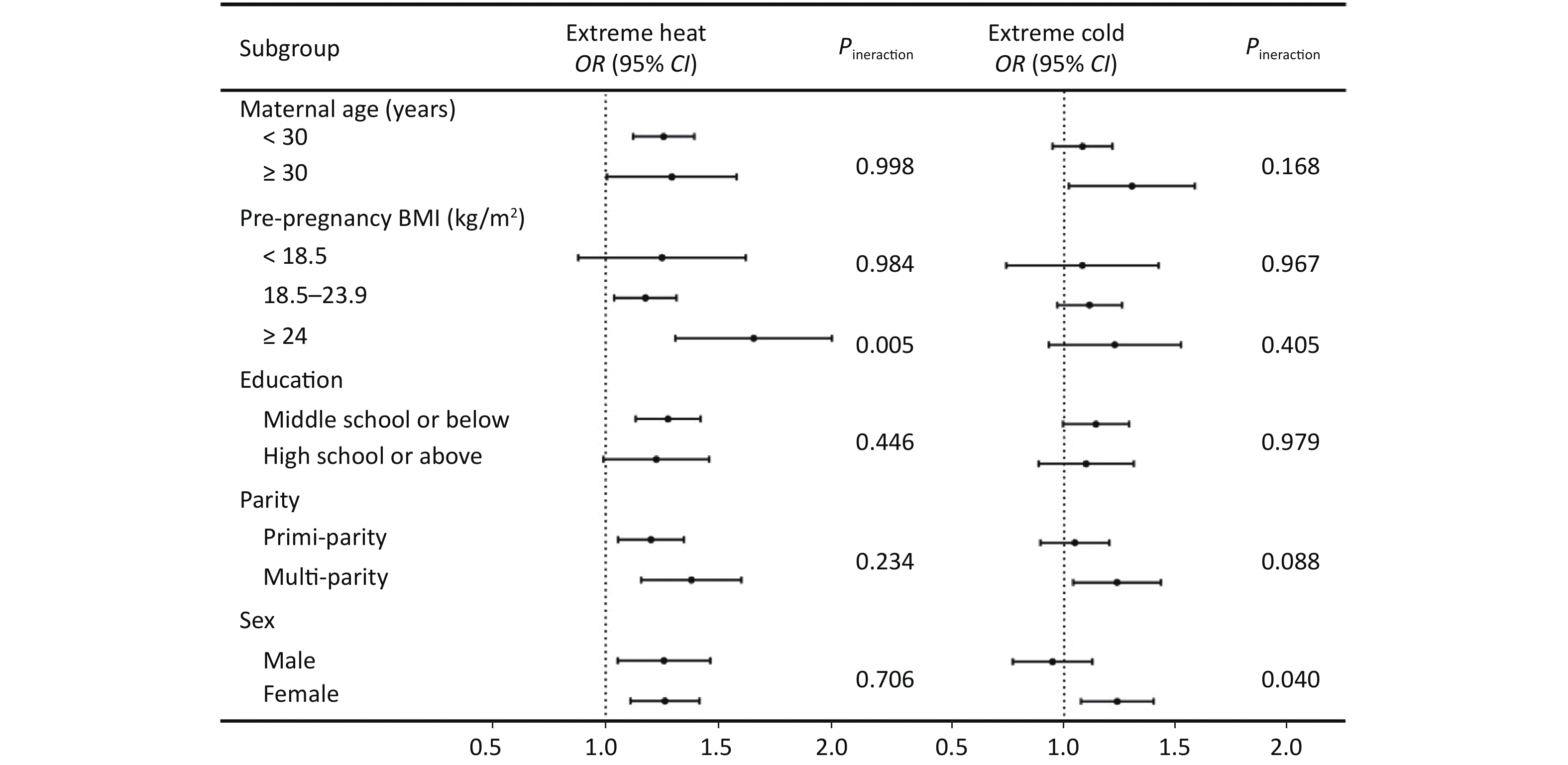
http://www.stats.gov.cn/tjsj/ndsj/ ), as traditional practices in most rural areas prohibit pregnant women from using air-conditioning for cooling. Therefore, most pregnant women in rural areas are helpless when exposed to high temperature, which may cause intrauterine growth retardation through heat stress or other means.Figure 2 shows the interaction effects between exposure to extreme temperature during the entire pregnancy and demographic characteristics on the risk of LBW. The association between exposure to extreme heat and the risk of LBW was stronger among newborns who were delivered by overweight mothers (Pinteraction = 0.005). Previous research has reported that, due to increased fat deposition and a decreased surface area to body mass ratio, the core temperature of overweight pregnant women increases and leads to a reduction in the capacity for heat dissipation by sweating[3]. Therefore, overweight pregnant women have a poor ability for heat dissipation and are more likely to be affected by exposure to extreme heat, thereby increasing the risk of giving birth to LBW infants. The risk of LBW induced by exposure to extreme cold was higher in infants who were female or who were born from a multi-parity woman (Pinteraction = 0.040, Pinteraction = 0.088, respectively). Previous studies have found that multi-parity mothers are generally older, lower education levels, higher pre-pregnancy BMI, higher incidence of gestational diabetes and other adverse events during pregnancy, which make them more likely to have adverse pregnancy outcomes[8]. It has been reported that placenta undergoes fine-tuning to ensure optimal fetal survival and growth in response to adverse environmental exposure. Maintaining growth under adverse environmental exposure may be a risky approach that could result in higher embryonic lethality[9]. The female fetus appears to follow a conservative approach, generating a smaller placenta to ensure the survival of the offspring. However, the small placenta may lead to the insufficient nutrition and oxygen supply, resulting in the occurrence of LBW[9]. This could explain why the effects of extreme temperature on the risk of LBW was stronger among female infants. Our findings implicated that feasible measure should be provided to protect vulnerable pregnant women from exposure to extreme temperature to reduce the health burden of LBW.
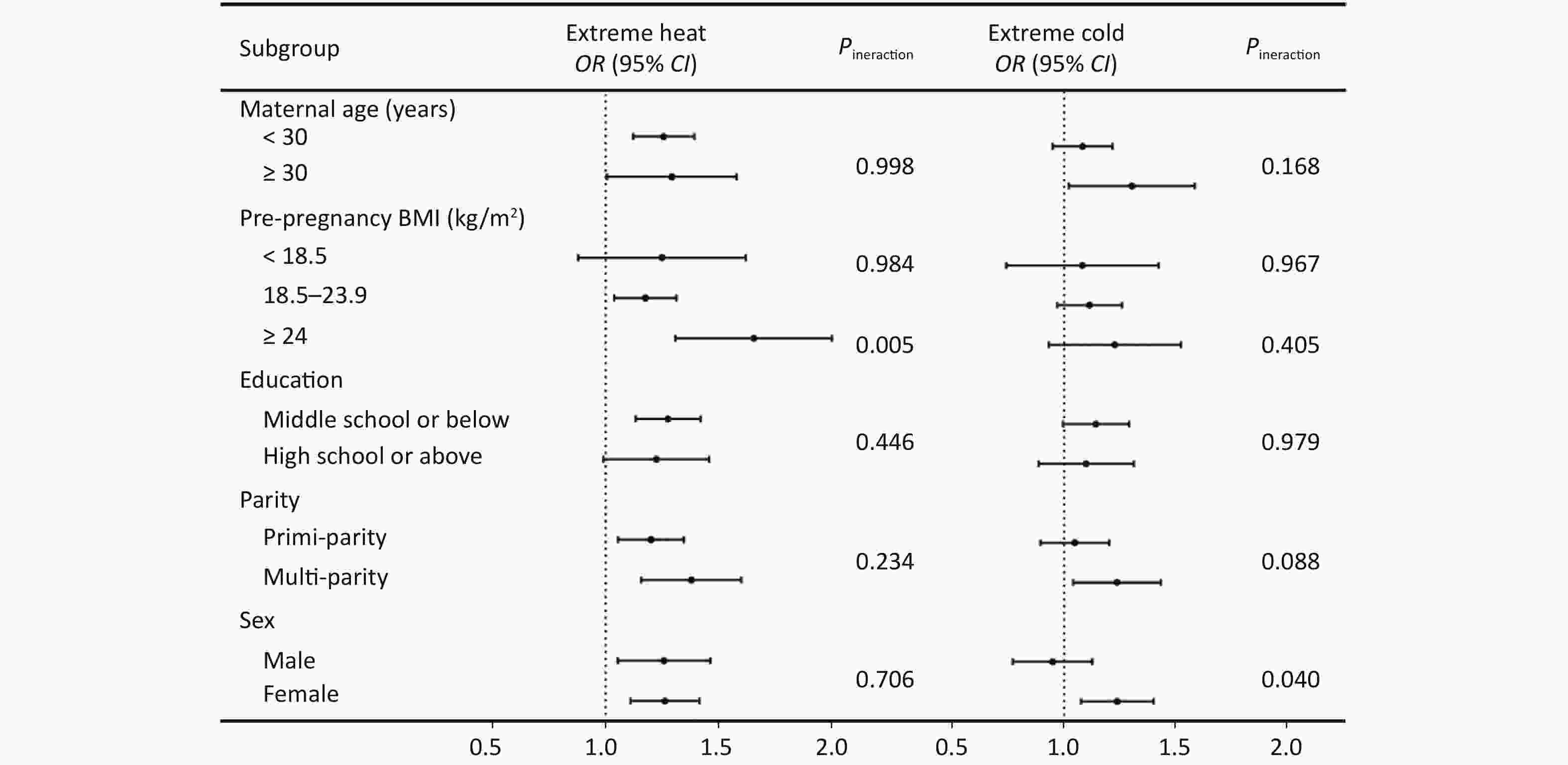
Figure 2. The interaction effects between exposure to extreme temperature during the entire pregnancy and demographic characteristics on the risk of LBW. Models were adjusted for relative humidity, maternal age, pre-pregnancy BMI, education level, smoking status, alcohol consumption, parity, and the sex of the newborn.
In acknowledgement of the limitations of this study, the housing conditions or indoor environment were not included as confounding factors of the association between ambient temperature and the risk of LBW, as the data were unavailable[10]. More information will be obtained in future studies.
In conclusion, we observed that the risk of LBW was increased by prenatal exposure to extreme temperature, especially during the second trimester. Our findings suggest that it is necessary for vulnerable mothers to implement prevention and treatment strategies to reduce the effects of temperature change on LBW.
Competing Interests None declared.
Acknowledgements We appreciated the National Free Preconception Health Examination Project in Henan Province. Thanks for all staffs who contributed to this research during the investigation and data curation.
doi: 10.3967/bes2021.124
The Association between Outdoor Ambient Temperature and the Risk of Low Birth Weight: A Population-Based Cohort Study in Rural Henan, China
-
&These authors contributed equally to this work.
注释: -
S1. Spatial distribution of the study area and national meteorological stations (A), and a flow chart of the inclusion and exclusion criteria for the final study population (B).
Figure 1. The dose-response relationships between the risk of LBW and mean ambient temperature during pregnancy (A). The association between the risk of LBW and exposure to ambient temperature during pregnancy (B). Models were adjusted for relative humidity, maternal age, pre-pregnancy BMI, education level, smoking status, alcohol consumption, parity, and the sex of the newborn.
Figure 2. The interaction effects between exposure to extreme temperature during the entire pregnancy and demographic characteristics on the risk of LBW. Models were adjusted for relative humidity, maternal age, pre-pregnancy BMI, education level, smoking status, alcohol consumption, parity, and the sex of the newborn.
S1. Characteristics of mean temperature (°C) and relative humidity (%) during pregnancy by exposure period
Item x s Min 10th M 90th Max Mean temperature (°C) Trimester 1 16.44 7.88 2.09 4.51 17.84 25.96 28.46 Trimester 2 15.98 7.88 2.98 4.97 16.88 25.33 27.55 Trimester 3 14.31 8.00 1.63 4.12 13.98 25.38 28.41 Entire pregnancy 15.58 2.61 10.93 12.17 15.51 19.01 20.87 Relative humidity (%) Trimester 1 66.63 7.07 49.97 57.18 66.40 75.81 79.66 Trimester 2 67.29 6.65 53.42 57.82 68.35 75.20 78.81 Trimester 3 66.38 7.25 48.53 56.17 66.57 75.45 80.70 Entire pregnancy 66.79 2.47 60.71 63.49 66.42 70.66 72.52  下载: 导出CSV
下载: 导出CSV
Table 1. Demographic characteristics of the study sample
Variables Low birth weight, n (%) Normal birth weight, n (%) P n 5,790 1,428,690 Mothers Age < 0.001 < 30 4,549 (78.6) 1,170,340 (81.9) ≥ 30 1,241 (21.4) 258,350 (18.1) Pre-pregnancy BMI (kg/m2) < 0.001 < 18.5 (lean) 622 (10.7) 122,238 (8.6) 18.5–23.9 (normal) 4,068 (70.3) 1,044,199 (73.0) ≥ 24 (overweight/obesity) 1,100 (19.0) 262,253 (18.4) Education 0.292 Middle school or below 4,184 (72.3) 1,041,226 (72.9) High school or above 1,606 (27.7) 387,464 (27.1) Smoking < 0.001 Yes 396 (6.8) 83,145 (5.8) No 5,394 (93.2) 1,345,545 (94.2) Alcohol consumption 0.584 Yes 36 (0.6) 8,235 (0.6) No 5,754 (99.4) 1,420,455 (99.4) Parity 0.009 Primi-parity 3,587 (61.9) 863,529 (60.4) Multi-parity 2,203 (38.1) 565,161 (39.6) Newborns Sex < 0.001 Male 2,006 (34.7) 730,228 (51.1) Female 3,784 (65.3) 698,462 (48.9)
下载: 导出CSV
-
[1] Khan JR, Islam MM, Awan N, et al. Analysis of low birth weight and its co-variants in Bangladesh based on a sub-sample from nationally representative survey. BMC Pediatr, 2018; 18, 100. doi: 10.1186/s12887-018-1068-0 [2] Rylander C, Odland JO, Sandanger TM. Climate change and the potential effects on maternal and pregnancy outcomes: an assessment of the most vulnerable - the mother, fetus, and newborn child. Global Health Action, 2013; 6. [3] Strand LB, Barnett AG, Tong S. The influence of season and ambient temperature on birth outcomes: a review of the epidemiological literature. Environ Res, 2011; 111, 451−62. doi: 10.1016/j.envres.2011.01.023 [4] Zhou G, Yang M, Chai J, et, al. Preconception ambient temperature and preterm birth: a time-series study in rural Henan, China. Environ Sci Pollut Res Int, 2020; 28, 9407−16. [5] Chen S, Yang Y, Qv Y, et al. Paternal exposure to medical-related radiation associated with low birthweight infants: A large population-based, retrospective cohort study in rural China. Medicine (Baltimore), 2018; 97, e9565. doi: 10.1097/MD.0000000000009565 [6] Wang J, Liu X, Dong M, et al. Associations of maternal ambient temperature exposures during pregnancy with the placental weight, volume and PFR: A birth cohort study in Guangzhou, China. Environ Int, 2020; 139, 105682. doi: 10.1016/j.envint.2020.105682 [7] Li S, Wang J, Xu Z, et al. Exploring associations of maternal exposure to ambient temperature with duration of gestation and birth weight: a prospective study. BMC Pregnancy Childbirth, 2018; 18, 513. doi: 10.1186/s12884-018-2100-y [8] Liu X, Xiao J, Sun X, et al. Associations of maternal ambient temperature exposures during pregnancy with the risk of preterm birth and the effect modification of birth order during the new baby boom: A birth cohort study in Guangzhou, China. Int J Hyg Environ Health, 2020; 225, 113481. doi: 10.1016/j.ijheh.2020.113481 [9] Matheson H, Veerbeek JH, Charnock-Jones DS, et al. Morphological and molecular changes in the murine placenta exposed to normobaric hypoxia throughout pregnancy. J Physiol, 2016; 594, 1371−88. doi: 10.1113/JP271073 [10] Lu C, Zhang W, Zheng X, et al. Combined effects of ambient air pollution and home environmental factors on low birth weight. Chemosphere, 2020; 240, 124836. doi: 10.1016/j.chemosphere.2019.124836 -
 21049Supplementary Materials.pdf
21049Supplementary Materials.pdf

-

 点击查看大图
点击查看大图
计量
- 文章访问数: 1637
- HTML全文浏览量: 565
- PDF下载量: 98
- 被引次数: 0

 Quick Links
Quick Links