


 下载:
下载:



-
Ebola virus disease (EVD) is a zoonotic disease. Fruit bats are considered to be the natural hosts of the Ebola virus[1]. Ebola virus is a non-segmented, single-stranded, negative-stranded RNA virus from the Filoviridae family, and consists of six species (Zaire ebolavirus, Sudan ebolavirus, Taï Forest ebolavirus, Bundibugyo ebolavirus, Bombali ebolavirus, and Reston ebolavirus)[2]. In the past decade, it was the Zaire strain of Ebola virus that mainly caused outbreaks of the epidemic[3-5].
EVD is a severe infectious disease with a case fatality rate of 50%–90% that is transmitted via direct and indirect contact. EVD poses a threat to global public health security due to its transmissibility, high epidemic potential, lack of seasonal variation, and population susceptibility[6, 7]. Greater than 40 outbreaks of EVD occurred in western and central Africa from 1976–2021, especially in the Democratic Republic of the Congo, Guinea, Uganda, and the Congo[3-5]. Most cases of EVD occurred in remote rural areas rather than suburban areas. In addition, some small outbreaks may not be reported[7]. The epidemic has spread across countries and continents[8, 9]. From 2014–2016, EVD spread from Guinea to Liberia and Sierra Leone. Then, nursing workers and travelers from the United States and Spain showed typical symptoms of EVD and were diagnosed with EVD after returning home from Africa[10]. In 2014, the World Health Organization (WHO) declared the EVD outbreak in Africa, a public health emergency of international concern[11].
Previous studies have used several different methods to assess the risk importation of EVD. Among the studies, the direct travel model[12], global network secondary outbreak model[12], and “Importation of an infection”[13] are widely-used methods; these models have primarily assessed the potential risk of EVD importation via air travel[14]. Some digital disease surveillance tools[15], including ProMED and HealthMap, have been applied to forecasting the short term importation risk of EVD and the risk-mapping method has been used to assess and prevent the cross-border transmission of EVD[16, 17]. The models and tools, however, are not comprehensive and are affected by estimation of the parameters related to transmission, and some models and tools are only valid when real-time data are available.
Because of the frequent economic trade and personnel exchanges that occur with globalization, an infectious disease in one part of the world can quickly spread to all countries. Since the implementation of China's "Silk Road Economic Belt" and "21st Century Maritime Silk Road" initiatives (hereinafter referred to as the "Belt and Road" Initiative), the economic trade and personnel exchanges between China and African countries has increased, thus, the importation risks of EVD into China cannot be ignored[18]. Although previous studies[19-21] concluded that African countries with EVD outbreaks had importation risks into China, the studies mainly focused on the assessment of one outbreak country or a possible importation method, and the methods or factors of risk assessment were limited. Therefore, our study analyzed the global epidemic status of EVD and applied the risk matrix method to assess the importation risk into China in an effort to implement EVD prevention strategies.
-
We obtained EVD reports and relevant data from WHO reports, including the country name, outbreak time, number of cases, number of deaths, and fatality rates of 12 African countries (Supplementary Table S1, available in www.besjournal.com)[3-5]. The annual number of African students in China was obtained from the 2018 Concise Statistics of International Students in China dataset, which represented personnel flows into China from countries with EVD outbreaks, and was used to assess the possibility importation risk[22]. Specifically, the number of international students from countries with EVD outbreaks in China was 6,845 (Nigeria), 2,883 (Sudan), 2,246 (the Democratic Republic of the Congo), 2,173 (Congo), 1,570 (Uganda), 983 (Sierra Leone), 946 (C
$ \widehat{\rm{o}} $ te d'Ivoire), 861 (Guinea), 802 (Liberia), 797 (Senegal), 788 (Mali), and 518 (Gabon) in 2018[22].Table S1. The number of cases, deaths and fatality rate of EVD reported by WHO from 1976 to 2021
Year Country Cases Deaths Case fatality (%) 2021 Guinea 23* 12* 52 2021 the Democratic Republic of the Congo 8 6 75 2020 the Democratic Republic of the Congo 130 55 42 2018–2020 the Democratic Republic of the Congo 3,481 2,299 66 2018 the Democratic Republic of the Congo 54 33 61 2017 the Democratic Republic of the Congo 8 4 50 2015 Italy# 1 0 0 2014 Spain# 1 0 0 2014 UK# 1 0 0 2014 USA# 4 1 25 2014 Senegal 1 0 0 2014 Mali 8 6 75 2014 Nigeria 20 8 40 2014–2016 Sierra Leone 14,124* 3,956* 28 2014–2016 Liberia 10,675* 4,809* 45 2014–2016 Guinea 3,811* 2,543* 67 2014 the Democratic Republic of the Congo 66 49 74 2012 the Democratic Republic of the Congo 57 29 51 2012 Uganda 7 4 57 2012 Uganda 24 17 71 2011 Uganda 1 1 100 2008 Democratic Republic of the Congo 32 14 44 2007 Uganda 149 37 25 2007 the Democratic Republic of the Congo 264 187 71 2005 Congo 12 10 83 2004 Sudan 17 7 41 2003 (Nov–Dec) Congo 35 29 83 2003 (Jan–Apr) Congo 143 128 90 2001–2002 Congo 59 44 75 2001–2002 Gabon 65 53 82 2000 Uganda 425 224 53 1996 South Africa (ex-Gabon) 1 1 100 1996 (Jul–Dec) Gabon 60 45 75 1996 (Jan–Apr) Gabon 31 21 68 1995 the Democratic Republic of the Congo 315 254 81 1994 Côte d'Ivoire 1 0 0 1994 Gabon 52 31 60 1979 Sudan 34 22 65 1977 the Democratic Republic of the Congo 1 1 100 1976 Sudan 284 151 53 1976 the Democratic Republic of the Congo 318 280 88 Note: *WHO: World Health Organization; UK: the United Kingdom; USA: the United States of America; EVD: Ebola virus disease; Include Suspect, Probable and Confirmed EVD cases; #Imported Cases of EVD. -
We used descriptive epidemiologic methods to describe the epidemic status of EVD. First, the cumulative cases and cumulative fatality rates were calculated to describe the EVD epidemic by country. Cumulative cases was equal to the total number of cases in countries with EVD countries from 1976–2021. Cumulative fatality rates =
$\dfrac{\rm{Cumulative}\;{\rm{deaths}}\;{\rm{from}}\;1976\;{\rm{to}}\;2021}{\rm{Cumulative}\;{\rm{cases}}\;{\rm{from}}\;1976\;{\rm{to}}\;2021}$ × 100%. Then, the time lag in years between the latest outbreak of EVD and 2021 was calculated by country and was equal to 2021, less the outbreak year. -
We applied the risk matrix method to assess the importation risk of EVD into China based on two dimensions of importation possibility and severity[23-25], with the risk assessment indicators and scores shown in Table 1. First, the importation possibility score was equal to the score of the time from the last outbreak to 2021 plus the international student number score entering China. We derived the final importation possibility risk score in 5 levels: rare (0–2 points); unlikely (3–4 points); possible (5–6 points); very possible (7–8 points); and inevitable (9–10 points). Second, the importation severity score was equal to the cumulative case score plus the cumulative fatality rate score. We also classified the final importation severity risk score into five levels: negligible (0–2 points); minor (3–4 points); moderate (5–6 points); severe (7–8 points); and catastrophic (9–10 points). Third, according to the importation possibility and severity levels in the risk matrix assessment index table (Table 2), the importation risk of EVD into China was divided into four levels (low, moderate, high, and extremely high), which corresponded to green, yellow, orange, and red zones, respectively.
Table 1. Risk assessment indicators of importation possibility and severity and the corresponding scores
Assessment indicators Factors Classification Risk scores Importation possibility The time lag between the latest outbreak
of Ebola virus disease and 2021 by
country (years)< 3 5 3–5 4 5–10 3 10–20 2 ≥ 20 1 The number of international students
entering China in 2018 (number)< 1,000 1 1,000–5,000 2 5,000–10,000 3 10,000–15,000 4 ≥ 15,000 5 Importation severity Cumulative cases (cases) < 1,000 1 1,000–5,000 2 5,000–10,000 3 10,000–15,000 4 ≥ 15,000 5 Cumulative fatality rate (%) < 10 1 10–40 2 40–70 3 70–90 4 ≥ 90 5 Table 2. Risk matrix assessment index table
Importation possibility Importation severity Negligible Minor Moderate Severe Catastrophic Inevitable H H E E E Very possible M H H E E Possible L M H E E Unlikely L L M H E Rare L L M H H Note. L, low importation risk; M, moderate importation risk; H, high importation risk; E, extremely high importation risk. -
We used the Borda count method to rank the EVD importation risks. First, the Borda points of importation risks equaled the sum of the ranks of importation possibility and severity risk levels. Then, we sorted Borda points of importation risks from the largest to the smallest and set the corresponding count as 0, 1..., N-1. The smaller the Borda count, the more likely EVD would be imported into China, and the more severe the consequences. Borda points were calculated with the following formula[25, 26]:
$$ {b}_{i}=\sum _{k=1}^{m}(N-{r}_{ik}) $$ where N equals the number of countries was 12; m equals the EVD risk assessment index, with the value set as 2; rik equals the risk for indicator i under criterion k; and
$ {b}_{i} $ equals the Borda points of the assessment indicator i. -
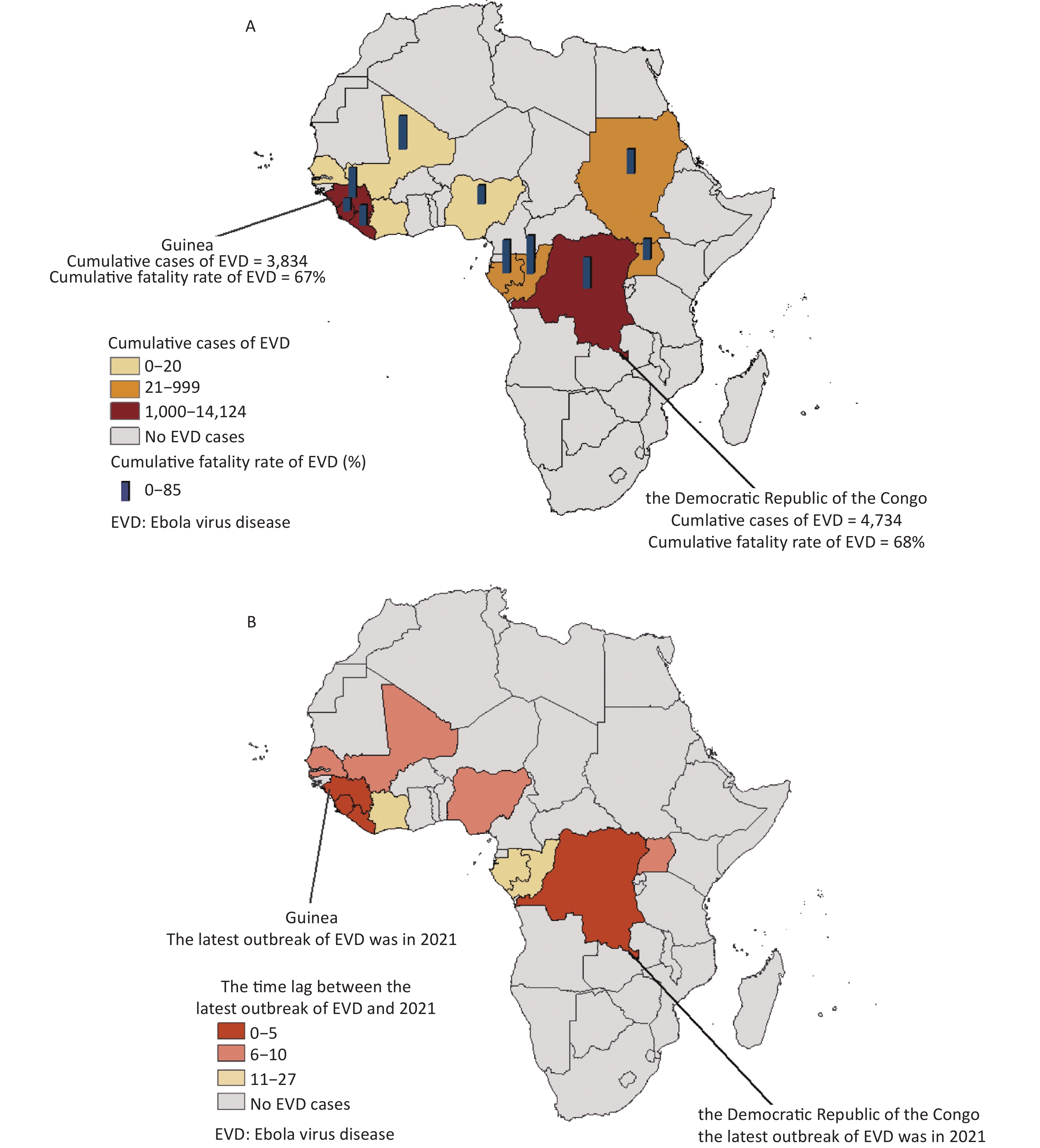
Between 1976 and 2021, EVD outbreaks were concentrated in central and western Africa. The highest number of cumulative cases of EVD was reported in Sierra Leone (14,124), followed by Liberia (10,675), Guinea (3,834), and the Democratic Republic of the Congo (4,734), while the lowest number was in Senegal (1) and C
$ \widehat{\rm{o}} $ te d'Ivoire (1). The Congo had the highest cumulative fatality rate (85%; Table 3, Figure 1). In the last 3 years, EVD occurred in the Democratic Republic of the Congo (2021) and Guinea (2021) (Table 3, Figure 1).Table 3. The global epidemic status of Ebola virus disease from 1976–2021
Country name* Cumulative cases Cumulative
fatality rate (%)Time from last outbreak
to 2021 (years)the Democratic Republic of the Congo 4,734 68 0 Guinea 3,834 67 0 Liberia 10,675 45 5 Sierra Leone 14,124 28 5 Nigeria 20 40 7 Mali 8 75 7 Senegal 1 0 7 Uganda 606 47 9 Congo 249 85 16 Sudan 336 54 17 Gabon 208 72 19 Côte d'Ivoire 1 0 27 Note. *As in Table 3, country names were ranked in ascending order of the time from the last outbreak to 2021 (years). 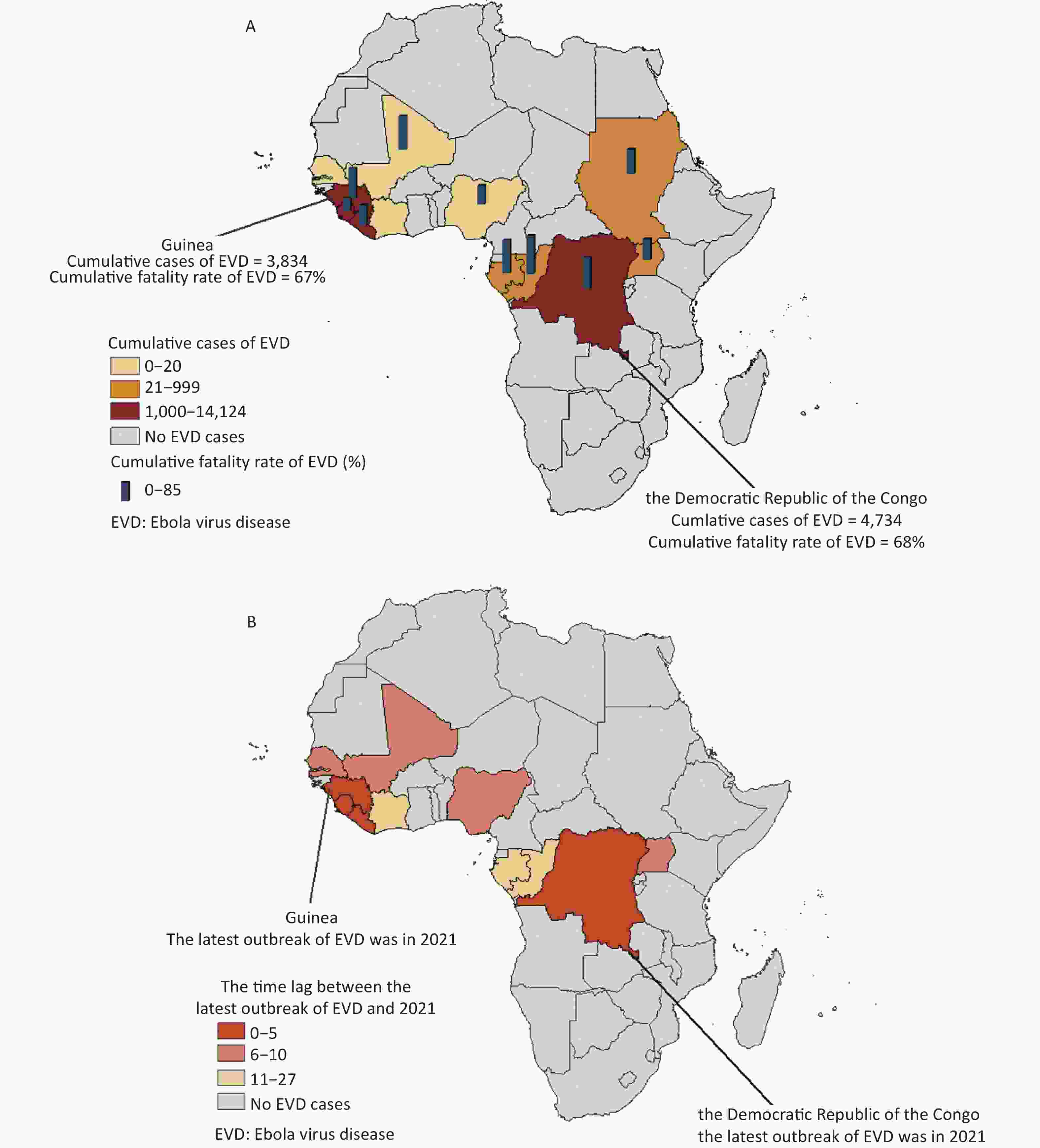
Figure 1. Cumulative cases and cumulative fatality rate (%) in countries with outbreaks of Ebola virus disease from 1976–2021 (A). The time lag between the latest outbreak of Ebola virus disease and 2021 by country (B).
-
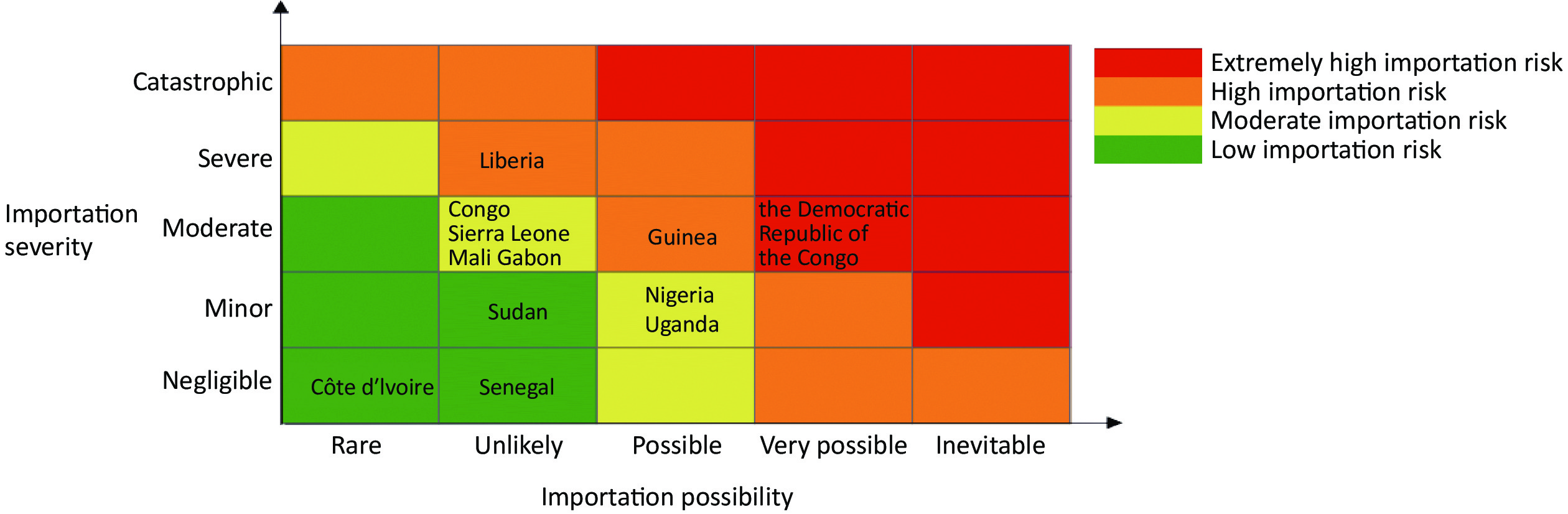
China is under the risk of EVD importation. For importation possibility, the highest risk was from the Democratic Republic of the Congo, with a score of 7, while the lowest risk was from C
$ \widehat{\rm{o}} $ te d'Ivoire, with a score of 2. For importation severity, the highest risk was from Liberia, with a score of 7, while the lowest risk was from Senegal and C$ \widehat{\rm{o}} $ te d'Ivoire, with a score of 2 each.An extremely high importation risk of EVD was from the Democratic Republic of the Congo. Two high importation risk countries were Guinea and Liberia, and six moderate importation risk countries were Nigeria, Uganda, Congo, Sierra Leone, Mali, and Gabon. Three low importation risk countries were Sudan, Senegal, and C
$ \widehat{\rm{o}} $ te d'Ivoire.The Democratic Republic of the Congo had the highest Borda points (23) and the count was 0, ranking first, while C
$ \widehat{\rm{o}} $ te d'Ivoire had the lowest Borda points (3) and the count was 11, ranking 12th (Table 4, Figure 2).Table 4. Importation risks from countries with Ebola virus disease outbreaks to China from 1976–2021
Country name* The importation
possibility scoreThe importation
severity scoreRisk levels Borda
pointsBorda count Risk sequence
of importationthe Democratic Republic of the Congo 7 5 E 23 0 1 Guinea 6 5 H 22 1 2 Liberia 4 7 H 20 2 3 Congo 4 5 M 19 3 4 Sierra Leone 4 6 M 19 3 4 Mali 4 5 M 19 3 4 Gabon 3 5 M 19 3 4 Nigeria 6 4 M 16 7 8 Uganda 5 4 M 16 7 8 Sudan 4 4 L 13 9 10 Senegal 4 2 L 10 10 11 Côte d'Ivoire 2 2 L 3 11 12 Note. *Country names were ranked in descending order of risk level. L, low importation risk; M, moderate importation risk; H, high importation risk; E, extremely high importation risk. 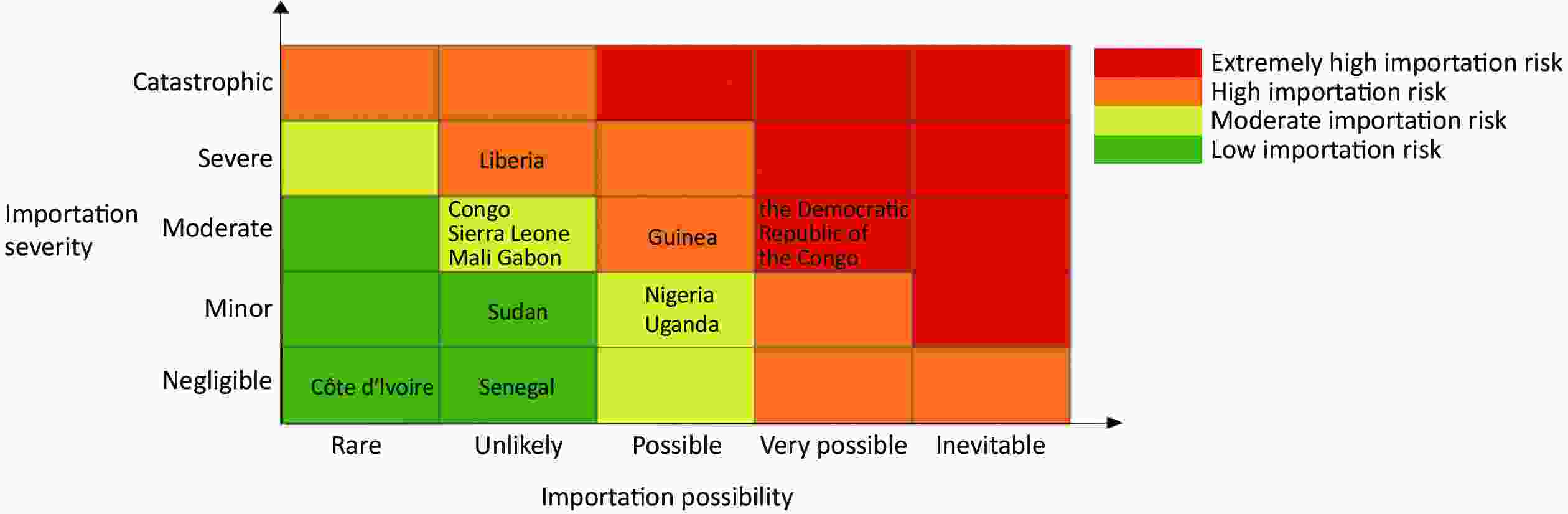
Figure 2. An importation risk matrix of Ebola virus disease from outbreak countries into China.
-
In this study we described the global epidemic status of EVD, applied the risk matrix method to assess the importation risk into China, and used the Borda count method to rank the risks. Our results showed that EVD outbreaks were more frequent in several central and western Africa countries, with the highest cumulative cases (14,124 cases) in Sierra Leone and the highest cumulative fatality rate (85%) in the Congo. We also found that the Democratic Republic of the Congo had an extremely high importation risk into China, followed by Guinea and Liberia. This was the first study to apply the risk assessment matrix method to assess the importation risk into China with two dimensions (possibility and severity). In addition, our study distinguished levels of risk and helped to identify countries with high importation risk rapidly. Finally, our results might provide more evidence for China to prevent and respond the importation risk of EVD.
In our study, EVD outbreaks were more frequent in several central and western Africa countries, and had severe fatality rates. Previous studies reported that both western central Africa and western Africa were high-risk outbreak regions for EVD in the future by analyzing the epidemic status and etiologic characteristics of EVD[27]. We also considered the potential outbreak in these countries. At present, EVD is not effectively controlled. In addition, zoonoses exist in epidemic areas and local fruit bats and primates carry EVD. Residents are infected by touching infected animals[28]. The WHO is of the opinion that EVD can re-emerge in the Democratic Republic of the Congo or other countries because of the endemic transmission of the epidemic and the gaps in preparedness and response capacities[4]. Previous studies [7, 29-31] have shown that active public health measures in countries at risk can control the spread of EVD and reduce the fatality rate. Despite the health and safety measures taken by the local government and health authorities, the control measures are still inadequate[9]. Local monitoring, detection, treatment, prevention, and management are insufficient, the government has not gained public trust, and the deceased are not given a safe and decent funeral, all of which spread the disease[4, 11, 27, 28, 32]. In addition, other health emergencies, such as COVID-19, cholera, and measles outbreaks, may affect the ability of countries at risk to quickly detect and respond to a renewed outbreaks of EVD[4]. Above all, the probability of an EVD epidemic in countries with outbreaks remains high.
Based on the risk assessment results, we concluded that the Democratic Republic of the Congo and other countries have a higher importation risk into China. Unlike the findings in our study, previous studies showed that importation risk may occur at a low level, and mainly focused on the assessment of one outbreak country or a possible flight importation[19-21]. Some reasons related to our results are discussed in the following. The infectious sources of EVD[28] mainly included confirmed patients, infected objects, such as blood products, and primates and their products[33]. China does not import primates, jungle meat products, or blood products. Thus the flow of people and articles is the main conduit for EVD importation into China[33]. With globalization and implementation of China's "One Belt, One Road" strategy, economic trade and personnel exchanges between China and the Democratic Republic of the Congo and other African countries are frequent, and the cross-border spread of infectious diseases is easier[34]. By 2018, China had admitted 492,000 international students, more than 50% of whom were from “Belt and Road” countries[18]. In addition, China has also permitted entry of civil servants, businessmen, and tourists from Africa[18]. China has sent a large number of medical and health workers, peacekeepers, Chinese students, and migrant workers to African countries in batches[18, 35]. Although the epidemic status had been effectively controlled, there may be an increasing importation risk if the above cross-border migrants are infected with Ebola virus. Compared with African countries, China has better public health prevention and control measures[36]; however, once Ebola virus is imported into China, the high fatality rate poses an enormous threat to the lives of Chinese people and has a huge impact on economic development and medical and health resources.
We applied the risk matrix method to assess the importation risk of countries with EVD outbreaks into China, and we integrated variables more closely related, including the time lag between the latest outbreak of EVD and 2021, the number of international students entering China, the cumulative cases, and the cumulative fatality rate. At present, the risk matrix method has been used to assess the importation risk of poliomyelitis[37] and leishmaniasis[38], the risk of plague focus areas[39], and the possibility of a COVID-19 epidemic under different external conditions[40], thus providing references for emergency decision-making of health departments. The limitations of this study included using only the number of students coming to China as representative from countries where the epidemic may occur, and did not include visitors on official business, commerce, tourism, and visiting relatives and other people in China. In addition, the study did not cover labor and engineering personnel who constructed EVD in countries with outbreaks who then returned to China. Therefore, we might have underestimated the importation risk into China.
-
In conclusion, under globalization, the epidemic status of EVD is severe and there have been several outbreaks in localized areas in recent years worldwide. China is under the risk of EVD importation, and key attention must be paid to the Democratic Republic of the Congo, Guinea, and Liberia. Therefore, it is necessary to prevent and prepare in advance for importation risk in China.
-
SHANG Wei Jing searched the literature, designed the study, collected the data, analyzed the data, interpreted the results, and drafted the article. JING Wen Zhan revised the article. LIU Jue supervised the study and revised the article. LIU Min conceived the study, designed the study, supervised the study, and revised the article.
-
The authors declare that they have no conflicts of interest regarding this work.
doi: 10.3967/bes2023.008
Global Epidemic of Ebola Virus Disease and the Importation Risk into China: An Assessment Based on the Risk Matrix Method
-
Abstract:
Objective To analyze the global epidemic status of the Ebola virus disease (EVD) and assess the importation risk into China. Methods Data from World Health Organization reports were used. We described the global epidemic status of EVD from 1976–2021, and assessed and ranked the importation risk of EVD from the disease-outbreaking countries into China using the risk matrix and Borda count methods, respectively. Results From 1976–2021, EVD mainly occurred in western and central Africa, with the highest cumulative number of cases (14,124 cases) in Sierra Leone, and the highest cumulative fatality rate (85%) in the Congo. Outbreaks of EVD have occurred in the Democratic Republic of the Congo and Guinea since 2018. The importation risk into China varies across countries with outbreaks of disease. The Democratic Republic of the Congo had an extremely high risk (23 Borda points), followed by Guinea and Liberia. Countries with a moderate importation risk were Nigeria, Uganda, Congo, Sierra Leone, Mali, and Gabon, while countries with a low importation risk included Sudan, Senegal, and C $ \widehat{\rm{o}} $ te d'Ivoire.Conclusion China is under the risk of EVD importation with the globalization and severe epidemic status of EVD. Key attention need to be paid to the Democratic Republic of the Congo, Guinea, and Liberia. Therefore, it is necessary to prevent and prepare in advance for importation risk in China. -
Key words:
- Ebola virus disease /
- Infectious disease /
- Importation risk /
- Risk matrix method
-
Figure 1. Cumulative cases and cumulative fatality rate (%) in countries with outbreaks of Ebola virus disease from 1976–2021 (A). The time lag between the latest outbreak of Ebola virus disease and 2021 by country (B).
Figure 2. An importation risk matrix of Ebola virus disease from outbreak countries into China.
S1. The number of cases, deaths and fatality rate of EVD reported by WHO from 1976 to 2021
Year Country Cases Deaths Case fatality (%) 2021 Guinea 23* 12* 52 2021 the Democratic Republic of the Congo 8 6 75 2020 the Democratic Republic of the Congo 130 55 42 2018–2020 the Democratic Republic of the Congo 3,481 2,299 66 2018 the Democratic Republic of the Congo 54 33 61 2017 the Democratic Republic of the Congo 8 4 50 2015 Italy# 1 0 0 2014 Spain# 1 0 0 2014 UK# 1 0 0 2014 USA# 4 1 25 2014 Senegal 1 0 0 2014 Mali 8 6 75 2014 Nigeria 20 8 40 2014–2016 Sierra Leone 14,124* 3,956* 28 2014–2016 Liberia 10,675* 4,809* 45 2014–2016 Guinea 3,811* 2,543* 67 2014 the Democratic Republic of the Congo 66 49 74 2012 the Democratic Republic of the Congo 57 29 51 2012 Uganda 7 4 57 2012 Uganda 24 17 71 2011 Uganda 1 1 100 2008 Democratic Republic of the Congo 32 14 44 2007 Uganda 149 37 25 2007 the Democratic Republic of the Congo 264 187 71 2005 Congo 12 10 83 2004 Sudan 17 7 41 2003 (Nov–Dec) Congo 35 29 83 2003 (Jan–Apr) Congo 143 128 90 2001–2002 Congo 59 44 75 2001–2002 Gabon 65 53 82 2000 Uganda 425 224 53 1996 South Africa (ex-Gabon) 1 1 100 1996 (Jul–Dec) Gabon 60 45 75 1996 (Jan–Apr) Gabon 31 21 68 1995 the Democratic Republic of the Congo 315 254 81 1994 Côte d'Ivoire 1 0 0 1994 Gabon 52 31 60 1979 Sudan 34 22 65 1977 the Democratic Republic of the Congo 1 1 100 1976 Sudan 284 151 53 1976 the Democratic Republic of the Congo 318 280 88 Note: *WHO: World Health Organization; UK: the United Kingdom; USA: the United States of America; EVD: Ebola virus disease; Include Suspect, Probable and Confirmed EVD cases; #Imported Cases of EVD.  下载: 导出CSV
下载: 导出CSV
Table 1. Risk assessment indicators of importation possibility and severity and the corresponding scores
Assessment indicators Factors Classification Risk scores Importation possibility The time lag between the latest outbreak
of Ebola virus disease and 2021 by
country (years)< 3 5 3–5 4 5–10 3 10–20 2 ≥ 20 1 The number of international students
entering China in 2018 (number)< 1,000 1 1,000–5,000 2 5,000–10,000 3 10,000–15,000 4 ≥ 15,000 5 Importation severity Cumulative cases (cases) < 1,000 1 1,000–5,000 2 5,000–10,000 3 10,000–15,000 4 ≥ 15,000 5 Cumulative fatality rate (%) < 10 1 10–40 2 40–70 3 70–90 4 ≥ 90 5
下载: 导出CSV
Table 2. Risk matrix assessment index table
Importation possibility Importation severity Negligible Minor Moderate Severe Catastrophic Inevitable H H E E E Very possible M H H E E Possible L M H E E Unlikely L L M H E Rare L L M H H Note. L, low importation risk; M, moderate importation risk; H, high importation risk; E, extremely high importation risk.
下载: 导出CSV
Table 3. The global epidemic status of Ebola virus disease from 1976–2021
Country name* Cumulative cases Cumulative
fatality rate (%)Time from last outbreak
to 2021 (years)the Democratic Republic of the Congo 4,734 68 0 Guinea 3,834 67 0 Liberia 10,675 45 5 Sierra Leone 14,124 28 5 Nigeria 20 40 7 Mali 8 75 7 Senegal 1 0 7 Uganda 606 47 9 Congo 249 85 16 Sudan 336 54 17 Gabon 208 72 19 Côte d'Ivoire 1 0 27 Note. *As in Table 3, country names were ranked in ascending order of the time from the last outbreak to 2021 (years).
下载: 导出CSV
Table 4. Importation risks from countries with Ebola virus disease outbreaks to China from 1976–2021
Country name* The importation
possibility scoreThe importation
severity scoreRisk levels Borda
pointsBorda count Risk sequence
of importationthe Democratic Republic of the Congo 7 5 E 23 0 1 Guinea 6 5 H 22 1 2 Liberia 4 7 H 20 2 3 Congo 4 5 M 19 3 4 Sierra Leone 4 6 M 19 3 4 Mali 4 5 M 19 3 4 Gabon 3 5 M 19 3 4 Nigeria 6 4 M 16 7 8 Uganda 5 4 M 16 7 8 Sudan 4 4 L 13 9 10 Senegal 4 2 L 10 10 11 Côte d'Ivoire 2 2 L 3 11 12 Note. *Country names were ranked in descending order of risk level. L, low importation risk; M, moderate importation risk; H, high importation risk; E, extremely high importation risk.
下载: 导出CSV
-
[1] Jacob ST, Crozier I, Fischer WA, et al. Ebola virus disease. Nat Rev Dis Primers, 2020; 6, 13. doi: 10.1038/s41572-020-0147-3 [2] Kiiza P, Mullin S, Teo K, et al. Treatment of Ebola-related critical illness. Intensive Care Med, 2020; 46, 285−97. doi: 10.1007/s00134-020-05949-z [3] World Health Organization. Ebola virus disease. https://www.who.int/news-room/fact-sheets/detail/ebola-virus-disease. [2021-12-24]. [4] World Health Organization. Ebola virus disease-Democratic Republic of the Congo. https://www.who.int/emergencies/disease-outbreak-news/item/2021-DON351. [2021-12-16]. [5] World Health Organization. Ebola virus disease - Guinea. https://www.who.int/emergencies/disease-outbreak-news/item/2021-DON328. [2021-06-19]. [6] Adepoju P. West Africa on alert for haemorrhagic fevers. Lancet, 2021; 398, 653. doi: 10.1016/S0140-6736(21)01863-8 [7] Malvy D, McElroy AK, De Clerck H, et al. Ebola virus disease. Lancet, 2019; 393, 936−48. doi: 10.1016/S0140-6736(18)33132-5 [8] Wiens KE, Schaeffer LE, Sow SO, et al. Oral rehydration therapies in Senegal, Mali, and Sierra Leone: a spatial analysis of changes over time and implications for policy. BMC Med, 2020; 18, 405. doi: 10.1186/s12916-020-01857-7 [9] Huber C, Finelli L, Stevens W. The economic and social burden of the 2014 Ebola outbreak in West Africa. J Infect Dis, 2018; 218, S698−704. doi: 10.1093/infdis/jiy213 [10] Nicastri E, Kobinger G, Vairo F, et al. Ebola virus disease: epidemiology, clinical features, management, and prevention. Infect Dis Clin North Am, 2019; 33, 953−76. doi: 10.1016/j.idc.2019.08.005 [11] Bennett RS, Logue J, Liu DX, et al. Kikwit Ebola virus disease progression in the rhesus monkey animal model. Viruses, 2020; 12, 753. doi: 10.3390/v12070753 [12] Cope RC, Cassey P, Hugo GJ, et al. Assessment of the risk of ebola importation to australia. PLoS Curr, 2014; 6, ecurrents. [13] Lopez LF, Amaku M, Coutinho FAB, et al. Modeling Importations and Exportations of Infectious Diseases via Travelers. Bull Math Biol, 2016; 78, 185−209. [14] Bogoch II, Creatore MI, Cetron MS, et al. Assessment of the potential for international dissemination of Ebola virus via commercial air travel during the 2014 West African outbreak. Lancet, 2015; 385, 29−35. doi: 10.1360/N972014-01201 [15] Bhatia S, Lassmann B, Cohn E, et al. Using digital surveillance tools for near real-time mapping of the risk of infectious disease spread. npj Digit Med, 2021; 4, 73. doi: 10.1038/s41746-021-00442-3 [16] Nanziri C, Ario AR, Ntono V, et al. Ebola virus disease preparedness assessment and risk mapping in Uganda, August-September 2018. Health Secur, 2020; 18, 105−13. doi: 10.1089/hs.2019.0118 [17] Nsubuga P, Masiira B, Kihembo C, et al. Evaluation of the Ebola virus disease (EVD) preparedness and readiness program in Uganda: 2018 to 2019. Pan Afr Med J, 2021; 38, 130. [18] Wang JL, Wang LL, Song YD, et al. Exploration of strengthening international cooperation in public health under the"Belt and Road"Initiative. Chin J of Public Health Manage, 2021; 37, 110-4. (In Chinese [19] Li Q, Zhuo QB, Huang YX, et al. Research status of Ebola virus disease. Chin J Infect Dis, 2015; 33, 316-8. (In Chinese [20] Lai S, Miniota J, Wang LP, et al. Assessing potential airlines and the risk of Ebolavirus importation from west African countries into China. Chin Sci Bull (Chin Ver), 2014; 59, 3572−80. doi: 10.1007/s11538-015-0135-z [21] Chang YT, Guo MR, Zhang LP, et al. Rapid risk assessment of the Ebola virus disease outbreak in Democratic Republic of Congo in May 2020. Chin J Front Health Quarant, 2020; 43, 317−20. (In Chinese [22] Ministry of Education, Department of International Cooperation and Exchange. Concise statistics of international students in 2018. Ministry of Education, Department of International Cooperation and Exchange. 2018; 348. (In Chinese) [23] Yang Y, Sun H, Kang Z, et al. Health emergency assessment: risk matrix and Borda sequence value method. Chin J Public Health, 2016; 32, 815−7. (In Chinese [24] Kang LY, Liu J, Liu M. Progress in researches on methods for risk assessment of infectious diseases. Chin J Public Health, 2021; 37, 1454−8. (In Chinese [25] Yun L, Wang FC, Zhang QF, et al. Integrated application of risk matrix method and Borda sequence value method to assess the risks of vectors for 2016 International Horticultural Exposition. Chin J Vect Bio Control, 2017; 28, 557−60. (In Chinese [26] Przybyła-Kasperek M, Marfo KF. Neural network used for the fusion of predictions obtained by the k-nearest neighbors algorithm based on independent data sources. Entropy, 2021; 23, 1568. doi: 10.3390/e23121568 [27] Baseler L, Chertow DS, Johnson KM, et al. The pathogenesis of Ebola virus disease. Annu Rev Pathol Mech Dis, 2017; 12, 387−418. doi: 10.1146/annurev-pathol-052016-100506 [28] Delgado R, Simón F. Transmission, human population, and pathogenicity: the Ebola case in point. Microbiol Spectr, 2018; 6, 1−12. [29] Burki T. Are we learning the lessons of the Ebola outbreak? Lancet Infect Dis, 2016; 16, 296−7. [30] Aceng JR, Ario AR, Muruta AN, et al. Uganda’s experience in Ebola virus disease outbreak preparedness, 2018-2019. Global Health, 2020; 16, 24. doi: 10.1186/s12992-020-00548-5 [31] Cáceres VM, Sidibe S, Andre M, et al. Surveillance training for Ebola preparedness in Côte D'Ivoire, Guinea-Bissau, Senegal, and Mali. Emerg Infect Dis, 2017; 23, S174−82. [32] Coltart CEM, Lindsey B, Ghinai I, et al. The Ebola outbreak, 2013-2016: old lessons for new epidemics. Philos Trans R Soc Lond B Biol Sci, 2017; 372, 20160297. doi: 10.1098/rstb.2016.0297 [33] Xu SQ, Wang Y. Theory and practice of emergency public health risk assessment. People's Medical Publishing House. 2017; 167. (In Chinese) [34] Liu J, Liu M. Challenges to public health risk prevention and responses in the context of building the Belt and Road. Chin J Epidemiol, 2019; 40, 255−8. (In Chinese [35] National Bureau of Statistics. China statistical yearbook 2019. China Statistics Press. 2019. (In Chinese) [36] Wang YL, Wang JJ, Shen YH. To strengthen inspection and quarantine in China port to prevent the Ebola entry. Chin J Health Educ, 2015; 31, 1073−6. (In Chinese [37] Han TL, Duan XJ, Wang Y, et al. Risk assessment of poliomyelitis imported into China from Afghanistan using risk matrix. Int J Virol, 2021; 28, 321−4. (In Chinese [38] Hao YW, Tian T, Zhu ZL, et al. Transmission risk matrix assessment of imported leishmaniasis in China. Chin J Schistosom Control, 2018; 30, 428−32. (In Chinese [39] Cong XB, Man TF, Ju C, et al. Application of risk matrix on plague risk assessment. Chin J Control of Endem Dis, 2014; 29, 321−3. (In Chinese [40] Abuhabib AA, Abu-Aita SN, Procter C, et al. Unique situation of Gaza Strip dealing with COVID-19 crisis. Int J Infect Dis, 2020; 100, 149−51. doi: 10.1016/j.ijid.2020.08.070 -
 22106Supplementary Materials.pdf
22106Supplementary Materials.pdf

-

 点击查看大图
点击查看大图
计量
- 文章访问数: 1416
- HTML全文浏览量: 538
- PDF下载量: 114
- 被引次数: 0










 Quick Links
Quick Links