

 下载:
下载:


-
Kashin-Beck disease (KBD) is an endemic, progressive, and degenerative osteoarthropathy, which mainly affects the articular cartilage of the limbs. This chronic osteochondral disease had a high prevalence and morbidity in the Eastern Siberian region of Russia, Democratic People’s Republic of Korea, and the broad, diagonal, northern-east to southern-west belt in China several decades ago[1]. This narrow zone located in China includes the Beijing, Gansu, Hebei, Heilongjiang, Henan, Inner Mongolia, Jilin, Liaoning, Qinghai, Shaanxi, Shandong, Shanxi, Sichuan, and Xizang. Generally, KBD occurs in children aged 5–15 years. The typical manifestations of KBD include joint pain, morning stiffness, enlarged and shortened fingers, joint deformities, and limited motion[2,3]. With advancing age, patients with KBD begin to experience serious secondary arthritis, and often encounter social and economic problems which affect many daily activities[4,5]. The etiology of KBD remains controversial, although three major environmental hypotheses have been proposed: endemic selenium deficiency, serious cereal contamination by mycotoxin-producing fungi, and high humic acid levels in drinking water[6]. A widely considered risk factor is the exposure to T-2 toxin produced by fusaria in stored grains from KBD-affected areas[7]. Selenium deficiency is another important risk factor for KBD[8,9]. A high concentration of organic substances in drinking water has also been proposed as a risk factor for KBD. The notion that the “the etiology of KBD is food-sourced” has been accepted by most scholars[10].
In the 1990s, it was estimated that 1 million patients in China had KBD symptoms, although even higher estimates have been described[11]. The Chinese government pays significant attention to the control of KBD, and special funds have been allocated for KBD surveillance and prevention in KBD epidemic areas every year. With economic development and practicable precautions, blocking the entry of mycotoxins into the body, coupled with adequate nutrition for children, the prevalence of KBD in affected areas has declined dramatically. In 2013, there were 0.64 million patients with KBD in China[12]. However, there are now approximately 177,000 patients with KBD. In addition, 20 million people live in areas endemic for KBD. Indeed, the risk factors for KBD still exist in 2023. It is necessary to carry out KBD monitoring and prevention continuously to avoid the resurgence of KBD among children.
Several studies have examined the prevalence of KBD in areas where the disease is endemic. However, a complete analysis of nationwide KBD prevalence data in China from 1990 onward has not been reported. In this study, we analyzed surveillance data for 13 provinces from a period of 34 years to understand the prevalence rates and dynamic trends of pediatric KBD in China. We anticipate that these results would provide a scientific basis to assess the effectiveness of prevention and control strategies for the elimination of KBD in China.
-
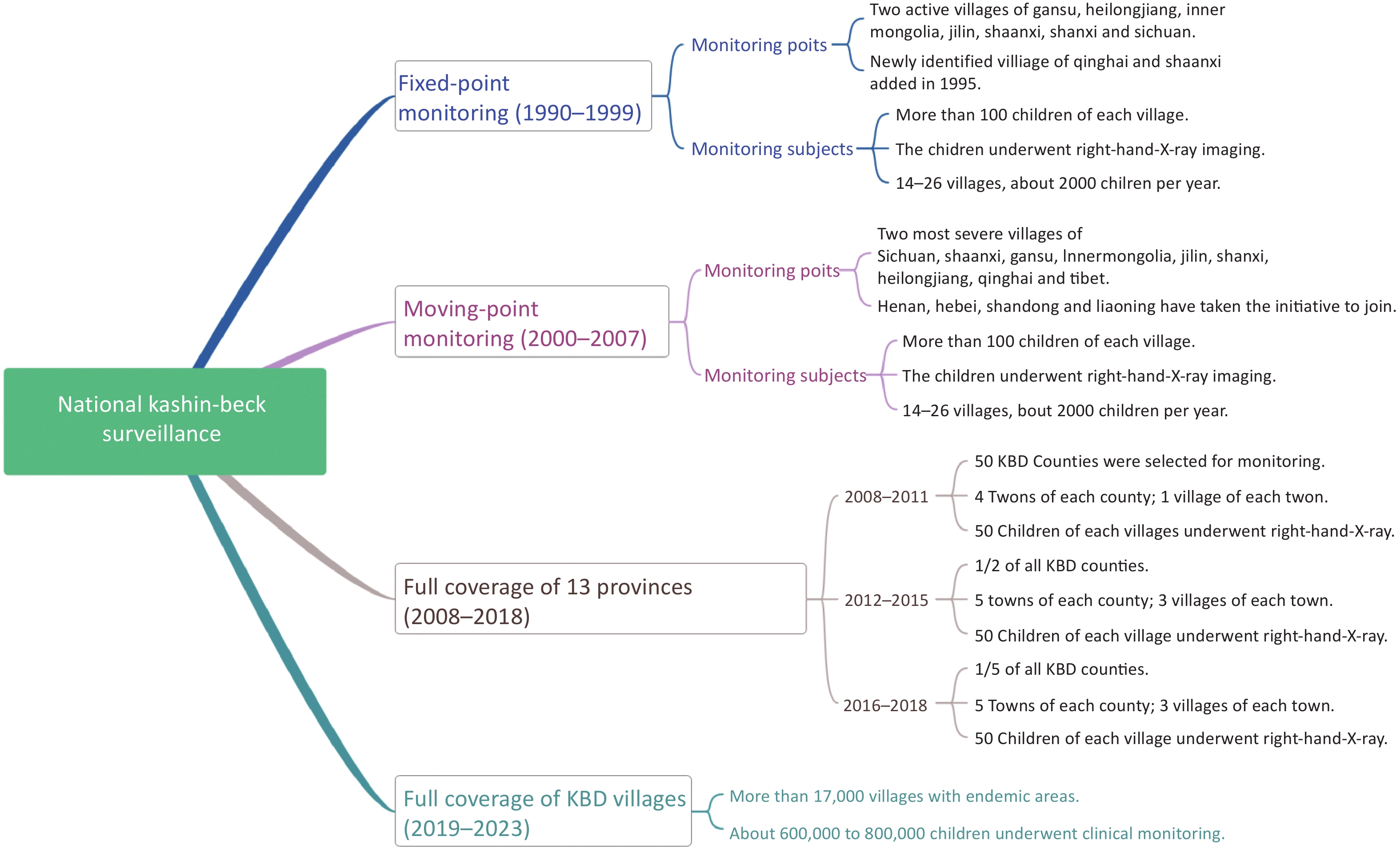
The history of KBD surveillance experienced three phases. During the first phase (1990–1999), fixed-point monitoring proceeded. Gansu, Heilongjiang, Inner Mongolia, Jilin, Shaanxi, Shanxi, and Sichuan were selected as the monitoring provinces, and two active villages severely affected by KBD in each province were selected as the monitoring points, which were followed up for 10 years. In 1995, the national KBD condition monitoring group found new KBD-affected areas and deteriorating endemic areas in Qinghai and Shaanxi provinces, and these areas were added as monitoring points.
Moving-point monitoring proceeded during the second phase (2000–2007). Therefore, villages with the most serious prevalence at that time were chosen as monitoring points. Besides the monitoring provinces in the first phase, Xizang, Henan, Hebei, Shandong, and Liaoning were included. The monitoring sample comprised more than 100 children (7–12 years old) at each monitoring point in first phase and second phase. The children underwent right-hand X-ray imaging.
From 2008, the third phase, moving-point monitoring continued in 14 KBD provinces and autonomous regions, including Gansu, Heilongjiang, Jilin, Liaoning, Henan, Hebei, Inner Mongolia, Qinghai Shaanxi, Shandong, Shanxi, Sichuan, and Xizang. In 2011, according to the results of an elimination assessment, Beijing was no longer treated as an endemic KBD area. In this phase, some counties (50 counties, 2008–2011; 180 counties, 2012–2015; 80 counties, 2016–2018) were selected to evaluate the KBD situation; all the children aged 7–12 years old in the monitoring spots were monitored by right-hand X-ray imaging. Since 2019, with all children aged 7–12 years in each village of all counties (n = 379) in 13 provinces enrolled in the surveillance program, full coverage of clinical monitoring has been achieved. The children were monitored by right-hand X-ray imaging when suspected clinical signs appeared to determine positivity for KBD. The flowchart of the monitoring process at different stages is shown in Figure 1.
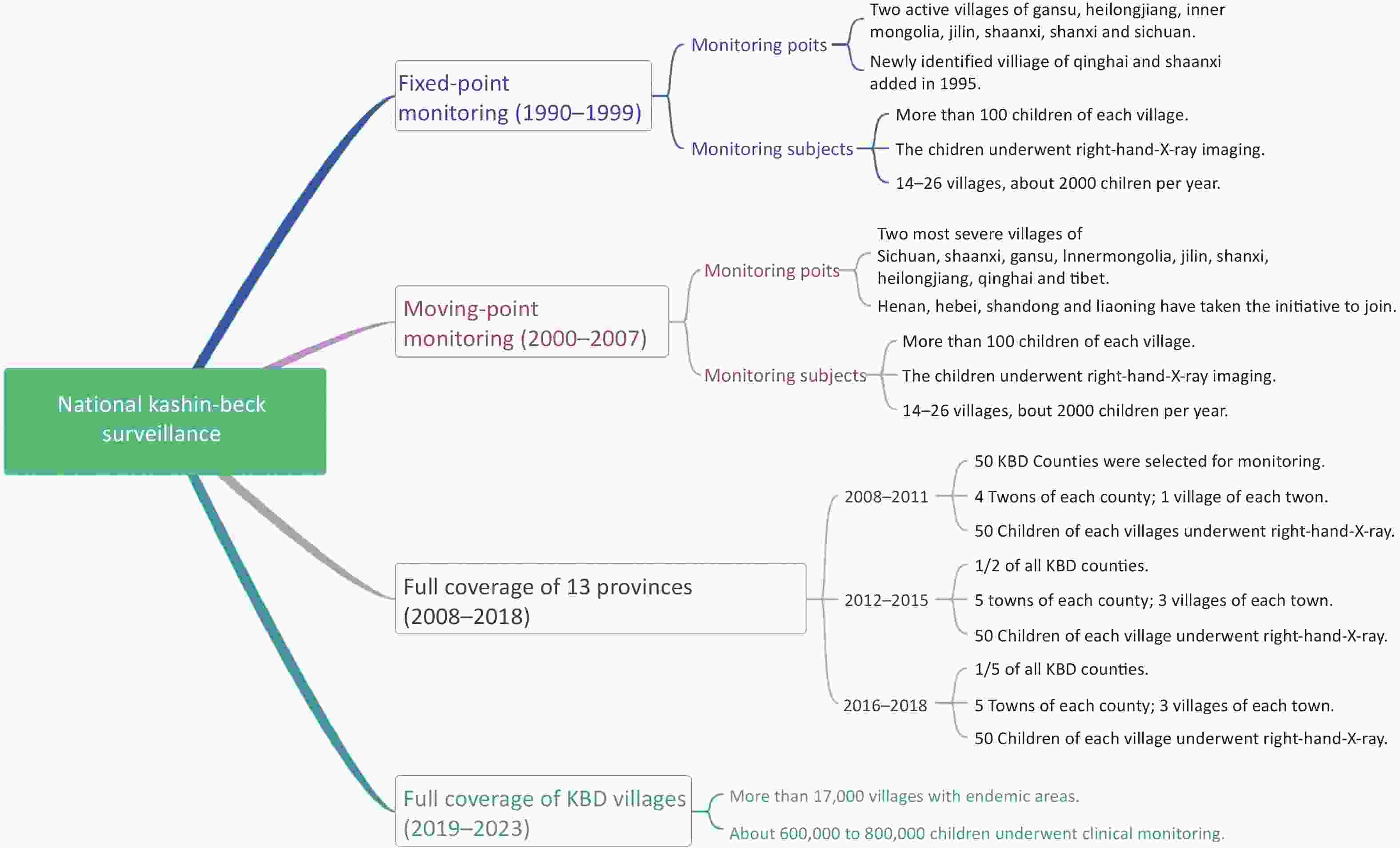
Figure 1. The flowchart of the monitoring process at different stages.
-
Orthographic X-rays of the right hands and wrists of all children were taken by Centers for Disease Control and prevention (CDC) technologists. According to the diagnostic criteria (WS/T207-2010)[13,14], KBD was clinically classified into three grades (I, II, and III). The diagnostic criteria were revised based on the previous diagnostic criteria for KBD (WS/T207-2001; GB16003-1995)[15–17]. All X-ray films were initially diagnosed by experts from each province. The final diagnosis was made by the national expert group after rechecking the positive X-ray films.
-
Statistical analyses were performed in SPSS 17.0 (IBM Corp., Armonk, NY, USA). The X-ray positive rate was calculated. The overall spatial distribution characteristic of the adult KBD patients was analyzed to determine whether spatial clustering existed in 2023. The prevalence rate of adult KBD patients in each county is calculated by dividing the number of adult KBD patients by the total population of endemic villages in the county. Moran’s I > 0 indicated a positive spatial correlation, with larger values indicating clearer spatial correlation. Moran’s I < 0 indicated a negative spatial correlation, with smaller values indicating a greater spatial difference. Otherwise, Moran’s I = 0 indicated that the data were randomly distributed in space. Getis-Ord Gi* was used for local spatial autocorrelation to describe the correlation between adult KBD patients prevalence levels in the county and its neighboring counties, and explore .Blue areas are low-value areas, i.e., “cold spots”; red areas are high-value areas, i.e., “hot spots”; and white areas indicate no agglomeration.
-
The ethical review board of Harbin Medical University and Provincial CDC and endemic disease prevention and control approved this research, and we obtained informed consent from the primary caregiver of each child.
-
Gansu, Hebei, Heilongjiang, Henan, Inner Mongolia, Jilin, Liaoning, Qinghai, Shaanxi, Shandong, Shanxi, Sichuan, and Xizang are KBD provinces, forming a narrow strip from northeast to southwest China. More than 16,000 KBD villages are distributed across the 13 provinces. Figure 2 showed the KBD villages in 13 provinces of China. Gansu, Shaanxi, and Jilin provinces have the highest number of villages affected by the disease, all exceeding 3,000; followed by Inner Mongolia and Heilongjiang, with the number of affected villages over 1,000; next in line are Shanxi, Liaoning, Henan, and Sichuan, each with more than 300 affected villages; Hebei, Shandong, Qinghai and Xizang provinces have the least, all with fewer than 100 affected villages.

Figure 2. Distribution of Kashin-Beck Disease vilages. Map approval number: GS(2019)1822.
-
During this decade, a total of 21,928 X-ray images were taken, with 175–375 individuals underwentb examination annually. Statistics were prepared according to the metaphyseal, epiphyseal, and carpal parts, respectively, and the positive rate was summarized. At the national level, the KBD X-ray detection rate decreased from 21.01% in 1990 to 7.75% in 1999.
Changes in the monitoring results can be summarized into four cases: 1) the X-ray detection rate among children in Beijing and Henan stayed very low, under 2% throughout the study period; 2) in Hebei and Jilin, the X-ray detection rate was under 10% in 1990, and decreased to under 2% in 1999; 3) in the Heilongjiang, Inner Mongolia, and Shaanxi provinces, areas severely affected by KBD, the detection rates were above 30% in 1990, but dropped significantly with time; 4) and in active areas found in the Sichuan and Qinghai provinces in the west of China, the X-ray detection rate remained above 10% (above 30% in Sichuan). Detailed information about the prevalence of KBD endemic provinces in different years is shown in Table 1.
Table 1. X-ray detectable rate of children in all provinces from 1990 to 1999 (%)
Province 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 Beijing − − − − − − − − − 1.71 Gansu 22.69 20.85 18.89 10.13 5.24 3.85 4.02 1.05 1.02 0.84 Hebei 5.48 2.85 2.84 2.88 1.83 1.35 1.12 1.12 0 0.98 Heilongjiang 30.04 21.65 22.12 19.03 12.58 8.64 5.53 4.76 3.23 3.54 Henan − − − − 2.13 0.81 0.74 0.75 1.36 1.45 Inner Mongolia 45.82 44.12 65.27 31.27 27.05 32.26 9.59 12.57 10.39 12.81 Jilin 1.79 1.54 4.46 1.74 1.20 0.94 0.49 1.45 0.92 0.47 Qinghai − − − − 27.59 30.08 26.82 15.10 13.84 12.62 Shaanxi 54.86 38.73 44.59 21.68 23.35 3.08 0.75 0.68 0 1.02 Shanxi 1.69 4.24 2.058 1.15 0.84 5.23 11.09 6.83 4.51 5.35 Sichuan 4.72 5.36 5.75 1.48 11.35 37.31 39.53 31.45 25.59 35.16 Total (n/N) 21.01
(375/1,782)17.67
(334/1,890)21.84
(382/1,749)12.21
(217/1,777)13.75
(357/2,579)14.93
(336/2,251)12.39
(324/2,614)9.25
(211/2,282)7.51
(175/2,329)7.75
(206/2,657)Note. −: there is no data; n/N: number of X-ray positive children/number of children examined. -
During this 8-year period, the national KBD X-ray detection rate decreased from 12.61% to 4.21%, achieving the control standards at the national level (5%). In 2000, the Qinghai province had a detection rate above 30% (36.78%). The X-ray detection rates in inner Mongolia, Shaanxi, and Xizang were 21.43%, 28.26%, and 21.19, respectively, which were all above 20%. By 2007, the X-ray detection rate of all the other provinces, except Qinghai (19.89%) and Inner Mongolia (7.33%), was below 5%. Detailed information about the year-wise prevalence of KBD in the 13 endemic provinces is shown in Table 2.
Table 2. X-ray detectable rate of children in all provinces from 2000 to 2007 (%)
Province 2000 2001 2002 2003 2004 2005 2006 2007 Beijing − 0 2.51 0 1.67 2.46 4.95 2.19 Gansu 13.11 24.76 17.43 10.55 6.30 15.87 8.82 4.41 Hebei 0.95 0 0.42 0 0 0.50 1.97 0.42 Heilongjiang 2.19 3.13 2.43 3.98 5.22 1.46 3.67 3.45 Henan 0 0 0 0 0 0 3.79 1.37 Inner Mongolia 21.43 5.43 3.47 6.48 7.08 4.69 9.95 7.33 Jilin 1.45 0 2.53 2.44 1.28 1.50 1.83 1.00 Liaoning − − − 0 − − 0 1.50 Qinghai 36.78 26.01 34.32 29.79 26.76 18.33 24.51 19.89 Shaanxi 28.26 23.83 17.49 17.41 12.92 5.76 4.13 3.32 Shandong 0.57 − − 2.69 1.53 1.89 2.06 − Shanxi 0.93 0 0 0.30 2.48 0.48 3.53 2.45 Sichuan 5.63 3.17 2.48 3.94 2.40 3.14 3.24 4.05 Xizang 29.19 40.87 33.86 27.33 20.08 − − − Total (n/N) 12.61
(374/2,965)10.05
(250/2,488)11.47
(218/2,772)6.89
(202/2,931)6.94
(196/2,823)5.21
(119/2,284)5.53
(146/2,642)4.21
(108/2,566)Note. −: there is no data; n/N: number of X-ray positive children/number of children examined. The monitoring results can be summarized as follows: 1) when monitoring began, the detection rate which was 10% or less in the ward did not change, and remained at control levels, e.g., Beijing and Hebei; 2) the serious, moderate illness areas at the beginning of monitoring, such as Gansu, Shaanxi, Inner Mongolia, and Heilongjiang, achieved the controlled levels (5%); 3) Qinghai, with seriously affected areas in the 1990s, and Xizang, with the additional wards in 2000, became moderately affected areas.
-
The prevalence of KBD in Inner Mongolia (8.23%), Xizang (5.40%), and Qinghai (7.14%) reduced in 2008; however, it was higher than that specified by the controlled criteria (5%). By 2010, the prevalence in all KBD provinces was less than 5% but higher than 1% in Inner Mongolia (2.23%), Liaoning (2.49%), Sichuan (1.07%), Xizang (4.51%), Gansu (1.17%), and Qinghai (4.67%). The prevalence has been less than 1% in the other KBD provinces except for Xizang and Qinghai since 2011. Detailed information about the year-wise prevalence of KBD in the 13 endemic provinces is shown in Table 3.
Table 3. X-ray detectable rate of children in all provinces from 2008 to 2018 (%)
Province 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 Gansu 3.66 1.17 0.40 0.61 0.14 0.22 0.16 0.22 0.06 0.24 0.25 Hebei 1.05 0 0.91 0 0.12 − 0.03 − 0 0 0 Heilongjiang 2.11 0 0.05 0.07 0.01 0.11 0.07 0.13 0.04 0.01 0.03 Henan 0.99 0 0 0 0.16 − 0.15 − 0.08 0 0 Inner Mongolia 8.23 2.23 0.92 0 0.57 0.90 0.46 0.51 0.59 0.57 0.05 Jilin 1.89 0.74 0.47 0.19 0.22 0.27 0.28 0.25 0 0.13 0.06 Liaoning 1.53 2.49 0.26 0 0 − 0 − 0 0 0 Qinghai 7.14 4.67 0.85 0.91 1.32 1.68 1.39 1.28 0.97 0 0 Shaanxi 0.23 0.53 0.45 0 0.01 0 0 0.01 0.05 0.08 0.08 Shandong 0.94 − − − 0.93 − 0.69 − 0.22 − 0 Shanxi 0.83 0.25 0 0 0.06 0.05 0 0 0 0 0 Sichuan 2.69 1.07 0.47 0.69 0.09 0.23 0.27 0 0 0.12 0 Xizang 5.40 4.51 - 0.75 1.70 0.67 2.31 0.03 0.01 0.07 0 Total (n/N) 3.32
(516/
1,5551)1.64
(224/
13,364)0.38
(36/
9,536)0.36
(45/
12,580)0.17 (191/
115,529)0.22 (185/
83,080)0.21 (217/
104,561)0.13 (140/
103,822)0.07
(49/
67,461)0.12
(70/
57,838)0.06
(39/
63,635)Note. −: there is no data; n/N: number of X-ray positive children/number of children examined. -
From 2019 to 2023, 13 provinces in the country conducted clinical examinations of children aged 7–12 in all KBD villages. Suspicious cases of children with clinical positive signs of suspected KBD were subjected to bilateral hand X-ray examination. In 2019, clinical examinations were conducted on 823,000 children, among whom 869 children showed signs of KBD such as thickening of bones and joint deformation, but all cases were ruled out through x-ray examination. Therefore, starting from 2019, the detection rate of KBD in children in all village nationwide has been zero and no cases were detected in the next 3 years.
Number of KBD examined children in all provinces from 2019 to 2023 shown in Table 4.
Table 4. Number of KBD examined children in all provinces from 2019 to 2023
Province 2019 2020 2021 2022 2023 Nc Nx N Nc Nx N Nc Nx N Nc Nx N Nc Nx N Gansu 241,738 301 0 263,805 0 0 257,786 262 0 250,130 0 0 234,997 28 0 Hebei 3,754 0 0 2,516 4 0 2,113 0 0 1,835 0 0 1,714 0 0 Heilongjiang 76,062 13 0 69,437 0 0 60,994 0 0 56,046 0 0 48,902 0 0 Henan 11,644 5 0 12,588 0 0 13,349 0 0 12,806 0 0 10,499 0 0 Inner Mongolia 70,535 0 0 58,197 17 0 69,536 4 0 65,872 0 0 49,527 0 0 Jilin 117,204 486 0 115,230 80 0 102,749 35 0 95,588 41 0 88,690 51 0 Liaoning 32,683 30 0 31,629 67 0 31,838 95 0 30,317 56 0 27,286 42 0 Qinghai 1,025 0 0 1,028 0 0 927 0 0 1,583 32 0 1,128 0 0 Shaanxi 213,904 34 0 201,688 0 0 195,630 0 0 195,850 0 0 187,834 0 0 Shandong 319 0 0 273 0 0 228 0 0 295 0 0 287 0 0 Shanxi 16,966 0 0 15,645 0 0 13,174 0 0 11,843 0 0 11,251 0 0 Sichuan 22,693 0 0 22,521 21 0 17,689 2 0 17,553 1 0 18,190 7 0 Xizang 14,838 0 0 24,429 14 0 20,154 0 0 8,083 0 0 28,565 0 0 Total 823,365 869 0 827,986 203 0 786,167 398 0 747,801 130 0 708,870 128 0 Note. Nc: Number of clinically examined children; Nx: Number of X-ray examined children; N: Number of KBD children. KBD, Kashin-Beck disease. -
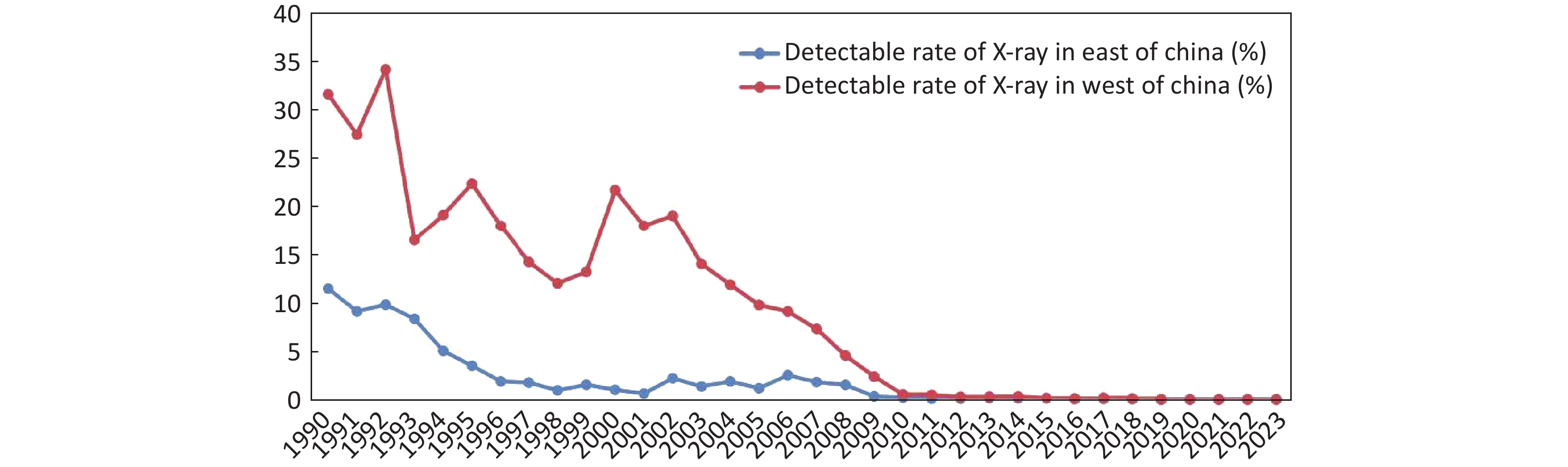
The detected rate of KBD in the western region of China is consistently higher than that in the eastern region (Eastern China: Hebei, Heilongjiang, Henan, Jilin, Liaoning, Shandong, Shanxi; Western China: Gansu, Inner Mongolia, Qinghai, Shaanxi, Sichuan, Xizang) (Figure 3). The detection rate of KBD in the eastern region has been reduced to less than 10% since 1994 and has remained below 5% since 1995. While the rate in western provinces dropped to less than 10% in 2005 and to less than 5% in 2008, at present, the detection rate in both the eastern and western regions is 0.
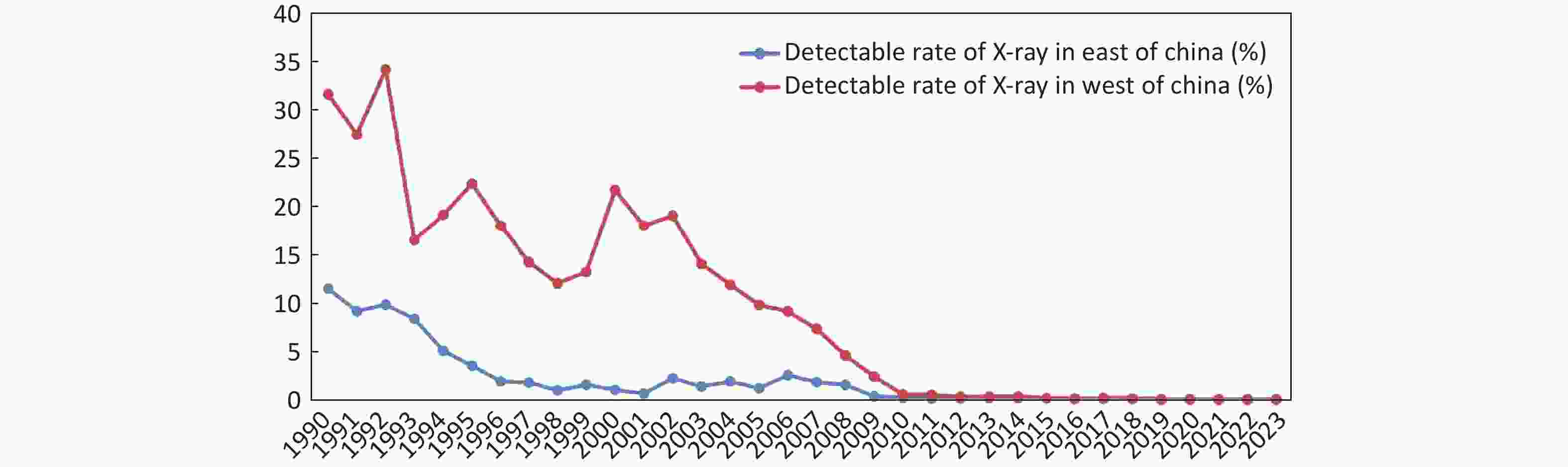
Figure 3. X-ray detection rate of children in east and west of China.
-
We used the number of adult KBD patients in each county in 2023 divided by the population of the epidemic village to calculate the prevalence rate for further analysis. The results of global spatial autocorrelation analysis indicated a spatial clustering of adult patients prevalence rate in the KBD areas. Moran’s I was 0.106 (Z = 10.038, P < 0.001) indicated a positive spatial correlation, with larger values indicating clearer spatial correlation.
-
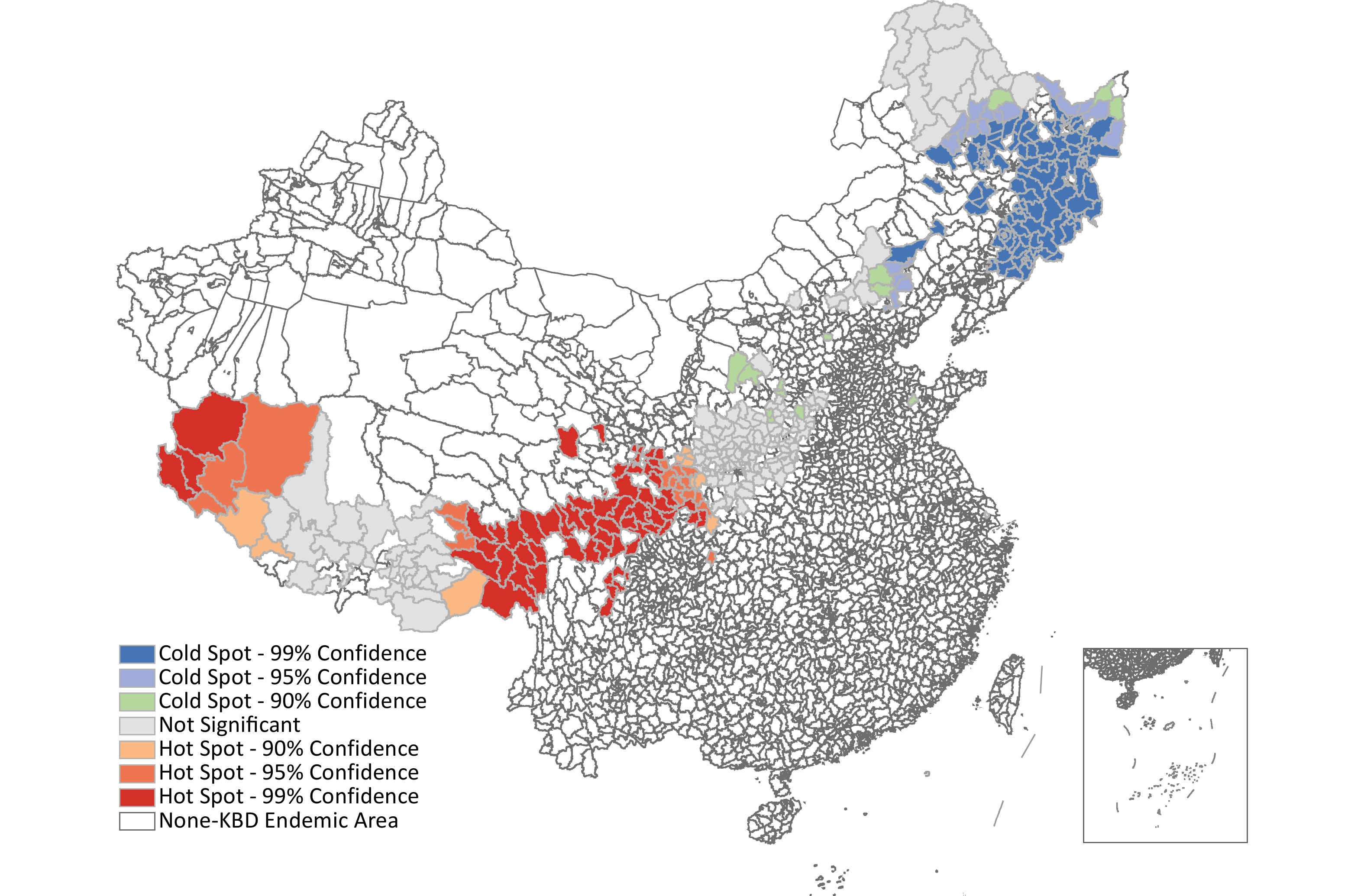
Local spatial autocorrelation analysis Getis-Ord Gi* was used for local spatial autocorrelation analysis (Z = 8.341, P < 0.001). In 2023, there was one hot spot and one cold spots (Figure 4). The hotspots are clustered in the southwest region of China, mainly including some districts in province Xizang, Sichuan, Qinghai, Gansu, Shaanxi, indicating a wider range of hot spots and higher KBD prevalence rate. The cold pots are clustered in the northeast region of China, including some districts in province Heilongjiang, Jilin, Liaoning, indicating a wider range of cold spots and lower KBD prevalence rate.
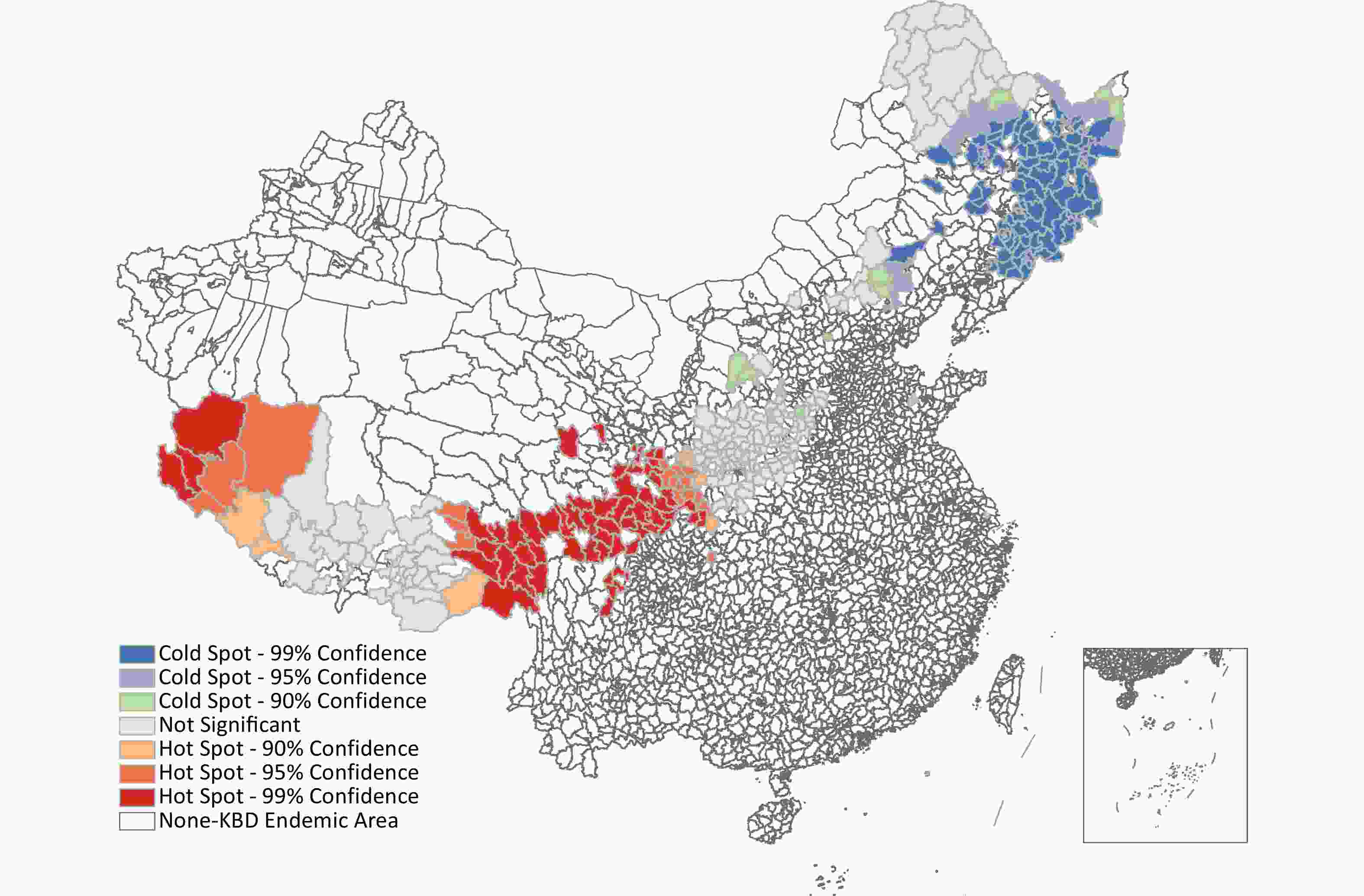
Figure 4. Local autocorrelation maps of the prevalence rate of adult KBD patients in 2023. Map approval number: GS(2019)1822.
-
It has been more than 170 years since the discovery and first report of KBD in 1849. As a typical endemic disease, the prevalence of KBD is widely distributed in China, and the formulation and implementation of its prevention and treatment strategies have been prioritized and strongly supported by the national government. National KBD monitoring as a macro-epidemiological study has obtained an ideal level of success in obtaining the distribution of KBD, its characteristics, epidemiological trends, and a series of valuable datasets, for national macro decision-making and regulation. Our findings provide an important scientific basis and technical support for government departments to formulate control countermeasures.
After decades of efforts, China finally confirmed that right-hand X-ray films are a favorable biomarker for KBD and suggested that bone end changes were specific markers and metaphyseal changes were sensitive markers[17,18]. The X-ray positive rate was calculated, which reflects the prevalence of KBD because the X-ray examination is more sensitive and more accurate compared with clinical examination in the diagnosis of KBD.
This finding reflects the characteristics of KBD as a developmental disease in children and the pathological mechanism of the transformation of KBD from early osteochondropathy to late osteoarthritis. Therefore, in the design of the national KBD surveillance program, children’s right-hand X-rays are often used as biomarkers because the X-ray examination is more sensitive and more accurate compared with clinical examination in the diagnosis of KBD.
China experienced a severe KBD epidemic from the 1960s to 1980s, which has declined since the mid-1980s. Cutting off the causal chain, health education, scientific farming, dry storage, and reducing the levels of gain pollution were promoted. Fungi pollution in the process of grain harvest and the mycotoxins produced in the process of storage were effectively reduced, and food hygiene was greatly improved. People did not eat self-produced grain, but instead ate the grain supplied from non-affected areas. In 1988, according to the endemic annual statistics, the number of people nationwide accepting the grain changing measures was nearly 1 million. From 1990 to 1999, the prevention and control of KBD achieved remarkable results, and the positive X-ray detection rate of KBD in children at the national level decreased from 21.01% to 7.75%.
Based on the historical experience of blocking etiology, the prevention and treatment strategies for KBD in China were formulated and implemented in the KBD-affected areas according to local conditions: change powder grain for rice, millet, sorghum, and other grains; plant vegetables or other cash crops and purchase food from the market; convert farmlands back to forests or grasslands; relocate to non-KBD-affected areas; centralize schooling or residential schooling; reduce the chance of fungal contamination and poisoning and improve the hygienic quality of food by improving harvest, transport, and storage in disease-affected areas; and diversify crop planting and food promotion.
Since 2000, the coverage of KBD surveillance has been expanding. Simultaneously, the active disease areas were also monitored continuously, which further improved the representation of KBD surveillance in China. In this stage, as a result of China’s rapid social and economic development, agricultural modernization enhanced continually, and living standards improved significantly. The original lifestyle of self-sufficiency in production changed, the proportion of outsourcing food increased, dietary structure diversity and food hygiene quality improved measurably, and the pathogenic factor was effectively blocked. KBD prevalence showed a declining trend across the country, but some western areas, such as Qinghai and Xizang, remained more seriously affected. A common feature of areas relatively seriously affected by illness was economic backwardness, inconvenient transportation and diets deficient in protein content. Residents’ staple food consumption includes a lower proportion of rice, while the texture, the production and storage methods of cereal grains have resulted in an abnormal accumulation of T-2 toxin. The causative agents of KBD were still active recent years, such as selenium deficiency and supernormal accumulation of T-2 toxins. A study shows that selenium content in the children’s hair samples from Ning County of Gansu in 2017 did not quite reach the standard for preventing KBD, the selenium content of the soil was in the low selenium level category[19].
In 2008, KBD surveillance was included in the central transfer payment program for endemic disease prevention and control, and the Chinese government has invested a large amount to prevent and control KBD. From 2008 to 2017, after the steady decline of KBD in China, the positive rate of KBD in children in western provinces, where the disease was more prevalent, also decreased year-by-year. Some western provinces have gradually adopted the method of closing village-level primary schools and centralized schooling and carrying out “Relocation and Education”. This strategy has protected students from the invasion of pathogenic factors and thus prevented and controlled KBD. In a relatively short period of time, the new cases of children with KBD in areas moderately and seriously affected by KBD were rapidly controlled using this strategy.
Wang’s systematic review also shows a negative correlation between KBD from 1992 to 2016 and the survey year, indicating that the mean X-ray detective rate decreased progressively[20]. The reason for these changes is to prevent and control KBD through comprehensive preventive measures, with an essential measure being grain exchange. Much research shows that changing grains had obvious effects on the prevention and treatment of KBD in children[21,22]. The experiments of grain exchange in Changdu City, Xizang achieved remarkable results[23]. The effects of eating rice from non-KBD-affected areas and selenium supplementation on the prevention and treatment of pediatric KBD in Qinghai province were also significant. The proportion of patients with X-ray lesions decreased dramatically in the intervention group; the suitable consumption of rice might be the most effective and safest intervention and should be encouraged[24].
In October 2018, the National Health Commission of China and 10 other government departments formulated and issued the Three-Year Action Plan for Endemic-Disease Prevention and Control (2018–2020), to implement key prevention and control measures as previously described, realize full coverage of disease monitoring and evaluation, and make a special effort to eliminate KBD. Thirteen KBD-affected provinces in China underwent two rounds of full-coverage monitoring and evaluation in 16,000 villages in 379 affected counties. In 2019, “zero” cases of KBD in children were reported for the first time in China[25]. No cases of KBD were detected in 2020-2023 as well, as shown by the results of a 5-year full coverage surveillance. Inner Mongolia, Gansu, Qinghai, and Xizang, which had achieved the goal of eliminating KBD by the end of the 12th Five-Year Plan with a relatively low proportion of eliminated villages, showed a continuous downward trend in the period of the 13th Five-Year Plan, and the situation regarding the spread of KBD in children has been gradually transformed from the control level to the basic elimination level.
Adult KBD is a kind of osteoarthropathy resulting from exposure to causative factors during childhood. It is clinically characterized by joint pain, enlargement, and deformation; muscle atrophy; shortened fingers, toes, and limbs; and most seriously, pygmyism and malformation, concomitant alterations in serum biomarker indicators will also be present[26-27]. In the geographical distribution of patients, we observe a hotspots clustered in the southwest region of China, mainly including some districts in province Xizang, Sichuan, Qinghai, Gansu, Shaanxi, indicating a wider range of hot spots and higher KBD prevalence rate. The reason for this situation is that the number of prevalent KBD patients is high in these counties, but the total population of the villages in the affected areas is low, resulting in a higher prevalence rate. While efforts have been made to control the current KBD epidemic, the disease and economic burden it poses are still substantial[28]. Due to the poor economic conditions in these areas, patients struggle with daily activities due to the disease, the adult KBD patients still need for policy consideration and care.
-
The evaluation results of the elimination of KBD in China for the last 5 years show that all villages in the KBD-affected areas have reached the elimination standard, and the basic elimination goal of KBD in China has been achieved. But adult patients in Western China still require more attention and care in terms of policy.
-
Silu Cui, Hui Liu performed the data analyses and wrote the manuscript; Junrui Pei, Jiaxin Li, Jiao Zhe and Qing Deng helped in data curation and performed the analysis with constructive discussions; Ning Liu and Yanhong Cao contributed significantly to analysis and manuscript preparation; Jun Yu contributed to the conception of the study, writing-review and editing of the manuscript.
doi: 10.3967/bes2024.109
-
Abstract:
Objective To analyze the epidemiological characteristics and epidemic situation of children with Kashin-Beck disease (KBD) in China, and provide the basis for formulating prevention and control measures. Methods Fixed-point monitoring, moving-point monitoring, and full coverage of monitoring were promoted successively from 1990 to 2023. Some children (7–12 years old) underwent clinical and right-hand X-ray examinations every year. According to the KBD diagnosis criteria, clinical and X-ray assessments were used to confirm the diagnosis. Results In 1990, the national KBD detectable rate was 21.01%. X-ray detection decreased to below 10% in 2003 and below 5% in 2007. Between 2010 and 2018, the prevalence of KBD in children was less than 0.4%, which fluctuated at a low level, and has decreased to 0% since 2019. Spatial epidemiological analysis indicated a spatial clustering of adult patients prevalence rate in the KBD areas. Conclusion The evaluation results of the elimination of KBD in China over the last 5 years showed that all villages in the monitored areas have reached the elimination standard. While the adult KBD patients still need for policy consideration and care. -
Key words:
- Kashin-Beck disease /
- Geographic Information System /
- National surveillance /
- X-ray detective rate
&These authors contributed equally to this work.
注释:1) COMPETING INTERESTS: -
Figure 2. Distribution of Kashin-Beck Disease vilages. Map approval number: GS(2019)1822.
Figure 4. Local autocorrelation maps of the prevalence rate of adult KBD patients in 2023. Map approval number: GS(2019)1822.
Table 1. X-ray detectable rate of children in all provinces from 1990 to 1999 (%)
Province 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 Beijing − − − − − − − − − 1.71 Gansu 22.69 20.85 18.89 10.13 5.24 3.85 4.02 1.05 1.02 0.84 Hebei 5.48 2.85 2.84 2.88 1.83 1.35 1.12 1.12 0 0.98 Heilongjiang 30.04 21.65 22.12 19.03 12.58 8.64 5.53 4.76 3.23 3.54 Henan − − − − 2.13 0.81 0.74 0.75 1.36 1.45 Inner Mongolia 45.82 44.12 65.27 31.27 27.05 32.26 9.59 12.57 10.39 12.81 Jilin 1.79 1.54 4.46 1.74 1.20 0.94 0.49 1.45 0.92 0.47 Qinghai − − − − 27.59 30.08 26.82 15.10 13.84 12.62 Shaanxi 54.86 38.73 44.59 21.68 23.35 3.08 0.75 0.68 0 1.02 Shanxi 1.69 4.24 2.058 1.15 0.84 5.23 11.09 6.83 4.51 5.35 Sichuan 4.72 5.36 5.75 1.48 11.35 37.31 39.53 31.45 25.59 35.16 Total (n/N) 21.01
(375/1,782)17.67
(334/1,890)21.84
(382/1,749)12.21
(217/1,777)13.75
(357/2,579)14.93
(336/2,251)12.39
(324/2,614)9.25
(211/2,282)7.51
(175/2,329)7.75
(206/2,657)Note. −: there is no data; n/N: number of X-ray positive children/number of children examined.  下载: 导出CSV
下载: 导出CSV
Table 2. X-ray detectable rate of children in all provinces from 2000 to 2007 (%)
Province 2000 2001 2002 2003 2004 2005 2006 2007 Beijing − 0 2.51 0 1.67 2.46 4.95 2.19 Gansu 13.11 24.76 17.43 10.55 6.30 15.87 8.82 4.41 Hebei 0.95 0 0.42 0 0 0.50 1.97 0.42 Heilongjiang 2.19 3.13 2.43 3.98 5.22 1.46 3.67 3.45 Henan 0 0 0 0 0 0 3.79 1.37 Inner Mongolia 21.43 5.43 3.47 6.48 7.08 4.69 9.95 7.33 Jilin 1.45 0 2.53 2.44 1.28 1.50 1.83 1.00 Liaoning − − − 0 − − 0 1.50 Qinghai 36.78 26.01 34.32 29.79 26.76 18.33 24.51 19.89 Shaanxi 28.26 23.83 17.49 17.41 12.92 5.76 4.13 3.32 Shandong 0.57 − − 2.69 1.53 1.89 2.06 − Shanxi 0.93 0 0 0.30 2.48 0.48 3.53 2.45 Sichuan 5.63 3.17 2.48 3.94 2.40 3.14 3.24 4.05 Xizang 29.19 40.87 33.86 27.33 20.08 − − − Total (n/N) 12.61
(374/2,965)10.05
(250/2,488)11.47
(218/2,772)6.89
(202/2,931)6.94
(196/2,823)5.21
(119/2,284)5.53
(146/2,642)4.21
(108/2,566)Note. −: there is no data; n/N: number of X-ray positive children/number of children examined.
下载: 导出CSV
Table 3. X-ray detectable rate of children in all provinces from 2008 to 2018 (%)
Province 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 Gansu 3.66 1.17 0.40 0.61 0.14 0.22 0.16 0.22 0.06 0.24 0.25 Hebei 1.05 0 0.91 0 0.12 − 0.03 − 0 0 0 Heilongjiang 2.11 0 0.05 0.07 0.01 0.11 0.07 0.13 0.04 0.01 0.03 Henan 0.99 0 0 0 0.16 − 0.15 − 0.08 0 0 Inner Mongolia 8.23 2.23 0.92 0 0.57 0.90 0.46 0.51 0.59 0.57 0.05 Jilin 1.89 0.74 0.47 0.19 0.22 0.27 0.28 0.25 0 0.13 0.06 Liaoning 1.53 2.49 0.26 0 0 − 0 − 0 0 0 Qinghai 7.14 4.67 0.85 0.91 1.32 1.68 1.39 1.28 0.97 0 0 Shaanxi 0.23 0.53 0.45 0 0.01 0 0 0.01 0.05 0.08 0.08 Shandong 0.94 − − − 0.93 − 0.69 − 0.22 − 0 Shanxi 0.83 0.25 0 0 0.06 0.05 0 0 0 0 0 Sichuan 2.69 1.07 0.47 0.69 0.09 0.23 0.27 0 0 0.12 0 Xizang 5.40 4.51 - 0.75 1.70 0.67 2.31 0.03 0.01 0.07 0 Total (n/N) 3.32
(516/
1,5551)1.64
(224/
13,364)0.38
(36/
9,536)0.36
(45/
12,580)0.17 (191/
115,529)0.22 (185/
83,080)0.21 (217/
104,561)0.13 (140/
103,822)0.07
(49/
67,461)0.12
(70/
57,838)0.06
(39/
63,635)Note. −: there is no data; n/N: number of X-ray positive children/number of children examined.
下载: 导出CSV
Table 4. Number of KBD examined children in all provinces from 2019 to 2023
Province 2019 2020 2021 2022 2023 Nc Nx N Nc Nx N Nc Nx N Nc Nx N Nc Nx N Gansu 241,738 301 0 263,805 0 0 257,786 262 0 250,130 0 0 234,997 28 0 Hebei 3,754 0 0 2,516 4 0 2,113 0 0 1,835 0 0 1,714 0 0 Heilongjiang 76,062 13 0 69,437 0 0 60,994 0 0 56,046 0 0 48,902 0 0 Henan 11,644 5 0 12,588 0 0 13,349 0 0 12,806 0 0 10,499 0 0 Inner Mongolia 70,535 0 0 58,197 17 0 69,536 4 0 65,872 0 0 49,527 0 0 Jilin 117,204 486 0 115,230 80 0 102,749 35 0 95,588 41 0 88,690 51 0 Liaoning 32,683 30 0 31,629 67 0 31,838 95 0 30,317 56 0 27,286 42 0 Qinghai 1,025 0 0 1,028 0 0 927 0 0 1,583 32 0 1,128 0 0 Shaanxi 213,904 34 0 201,688 0 0 195,630 0 0 195,850 0 0 187,834 0 0 Shandong 319 0 0 273 0 0 228 0 0 295 0 0 287 0 0 Shanxi 16,966 0 0 15,645 0 0 13,174 0 0 11,843 0 0 11,251 0 0 Sichuan 22,693 0 0 22,521 21 0 17,689 2 0 17,553 1 0 18,190 7 0 Xizang 14,838 0 0 24,429 14 0 20,154 0 0 8,083 0 0 28,565 0 0 Total 823,365 869 0 827,986 203 0 786,167 398 0 747,801 130 0 708,870 128 0 Note. Nc: Number of clinically examined children; Nx: Number of X-ray examined children; N: Number of KBD children. KBD, Kashin-Beck disease.
下载: 导出CSV
-
[1] Yamamuro T. Kashin-Beck disease: a historical overview. Int Orthop, 2001; 25, 134−7. doi: 10.1007/s002640000178 [2] Huang Q, Zhou ZK, Ma J, et al. The arthropathic and functional impairment features of adult Kashin-Beck disease patients in Aba Tibetan area in China. Osteoarthritis Cartilage, 2015; 23, 601−6. doi: 10.1016/j.joca.2015.01.005 [3] Xiong G. Diagnostic, clinical and radiological characteristics of Kashin-Beck disease in Shaanxi Province, PR China. Int Orthop, 2001; 25, 147−50. doi: 10.1007/s002640100248 [4] Li Y, Zhou ZK, Shen B, et al. Clinical features of Kashin-Beck disease in adults younger than 50 years of age during a low incidence period: severe elbow and knee lesions. Clin Rheumatol, 2013; 32, 317−24. doi: 10.1007/s10067-012-2115-0 [5] Schepman K, Engelbert RHH, Visser MM, et al. Kashin Beck disease: more than just osteoarthrosis: a cross-sectional study regarding the influence of body function-structures and activities on level of participation. Int Orthop, 2011; 35, 767−76. doi: 10.1007/s00264-010-1043-3 [6] Cao CX, Zhang YG, Wu SX, et al. Association of clinical features of bone and joint lesions between children and parents with Kashin-Beck disease in Northwest China. Clin Rheumatol, 2013; 32, 1309−16. doi: 10.1007/s10067-013-2267-6 [7] Li DY, Han J, Guo X, et al. The effects of T-2 toxin on the prevalence and development of Kashin-Beck disease in China: a meta-analysis and systematic review. Toxicol Res, 2016; 5, 731−51. doi: 10.1039/C5TX00377F [8] Zhang W, Neve J, Xu J, et al. Selenium, iodine and fungal contamination in Yulin District (People’s Republic of China) endemic for Kashin-Beck disease. Int Orthop, 2001; 25, 188−90. doi: 10.1007/s002640100242 [9] Wang J, Wang XY, Li HR, et al. Spatial distribution and determinants of health loss from Kashin-Beck disease in Bin County, Shaanxi Province, China. BMC Public Health, 2021; 21, 387. doi: 10.1186/s12889-021-10407-6 [10] Wang KW, Yu J, Liu H, et al. Endemic Kashin-Beck disease: a food-sourced osteoarthropathy. Semin Arthritis Rheum, 2020; 50, 366−72. doi: 10.1016/j.semarthrit.2019.07.014 [11] Zhai SS, Kimbrough RD, Meng B, et al. Kashin-Beck disease: a cross-sectional study in seven villages in the people’s republic of China. J Toxicol Environ Health, 1990; 30, 239−59. doi: 10.1080/15287399009531427 [12] Guo X, Ma WJ, Zhang F, et al. Recent advances in the research of an endemic osteochondropathy in China: Kashin-Beck disease. Osteoarthritis Cartilage, 2014; 22, 1774−83. doi: 10.1016/j.joca.2014.07.023 [13] Liu N, Yang JB, Wang ZW, et al. Diagnosis of Kaschin-Beck disease. Natl stand China WS/T 207-2010, 2010. (In Chinese) [14] Yu FF, Ping ZG, Yao C, et al. Evaluation of the sensitivity and specificity of the new clinical diagnostic and classification criteria for Kashin-Beck disease, an endemic osteoarthritis, in China. Biomed Environ Sci, 2017; 30, 150−5. [15] Ministry of Health P. R. China. Type and scale on X-ray sings of Kashin-Beck disease. WS/T 207-2001, 2004. (In Chinese) [16] Ministry of Health. Diagnostic criteria of Kashin Beck disease. GB 16003-1995, 2004. (In Chinese) [17] Zhang YN, Wei XL, Cao CX, et al. Identifying discriminative features for diagnosis of Kashin-Beck disease among adolescents. BMC Musculoskelet Disord, 2021; 22, 801. doi: 10.1186/s12891-021-04514-z [18] Liu HX, Zhang XY, Li FZ, et al. The emotions of X-ray image changes of children with Kaschin-Beck disease. Chin J Control Endem Dis, 2014; 29, 15−8. (In Chinese) [19] Sun LY, Yuan LJ, Fu Y, et al. Prevalence of Kaschin-Beck disease among Tibetan children in Aba Tibetan and Qiang autonomous prefecture: a 3-year epidemiological survey. World J Pediatr, 2012; 8, 140−4. doi: 10.1007/s12519-012-0351-7 [20] Wang X, Ning YJ, Liu AM, et al. BMC Musculoskelet Disord, 2019; 20, 78. [21] Han J, Yu FF, Chang ZP, et al. Changing grains for the prevention and treatment of Kashin-Beck disease in children: a meta-analysis. Biomed Environ Sci, 2015; 28, 308−11. [22] Yu FF, Qi X, Shang YN, et al. Prevention and control strategies for children Kashin-Beck disease in China: a systematic review and meta-analysis. Medicine, 2019; 98, e16823. doi: 10.1097/MD.0000000000016823 [23] Li H, Liu Q, Li QW, et al. Prevalence of pediatric Kashin-Beck disease in Tibet. Clin Rheumatol, 2021; 40, 3717−22. doi: 10.1007/s10067-021-05669-9 [24] Sun LY, Meng FG, Li Q, et al. Effects of the consumption of rice from non-KBD areas and selenium supplementation on the prevention and treatment of paediatric Kaschin-Beck disease: an epidemiological intervention trial in the Qinghai Province. Osteoarthritis Cartilage, 2014; 22, 2033−40. doi: 10.1016/j.joca.2014.09.013 [25] Cui SL, Deng Q, Pei JR, et al. Summary report of a national survey of Kashin-Beck disease prevalence in 2019. Chin J Endemiol, 2021; 40, 545−50. (In Chinese) [26] Wang YM, Wang WY, Sun LY, et al. Serum metabolomic indicates potential biomarkers and metabolic pathways of pediatric kashin-beck disease. Biomed Environ Sci, 2020; 33, 750−9. [27] Qi F, Cui SL, Zhang B, et al. A study on atypical Kashin-Beck disease: an endemic ankle arthritis. J Orthop Surg Res, 2023; 18, 328. doi: 10.1186/s13018-023-03633-8 [28] Cui SL, Que WJ, Jiao Z, et al. Disease and economic burden of Kashin-beck disease-China, 2021. China CDC Wkly, 2024; 6, 40−4. doi: 10.46234/ccdcw2024.009 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 1595
- HTML全文浏览量: 717
- PDF下载量: 70
- 被引次数: 0

 Quick Links
Quick Links