

 下载:
下载:

-
The global incidence of pediatric obesity has increased rapidly over the past few decades. Scientific evidence has repeatedly shown that behavioral and emotional challenges are frequently observed in children with overweight or obesity[1,2], as evidenced by a landmark case-control design study revealing that obese children have 7.15 times higher odds of developing mental health disorders in adolescence than their normal-weight peers[1]. Failure to address behavioral problems in childhood can lead to enduring effects that extend into adulthood, adversely affecting physical and mental health.
Sleep disturbance is a prevalent psychological issue in obese children that affects their physical health and neurobehavioral well-being. Therefore, the psychological well-being and sleep quality of children with obesity require special attention in mental health management. Elevated variability and irregularities in sleep patterns have been associated with reduced physical activity levels, disrupted eating behaviors and inadequate dietary intake, metabolic dysfunction, compromised cardiac autonomic balance, and increased blood pressure among adolescents[3]. Recently, several studies have demonstrated that problematic sleep patterns contribute to the emergence and exacerbation of behavioral symptoms in young individuals[4]. However, only a few studies have focused on children with overweight and obesity. It remains unclear whether sleep problems are differentially associated with different types of childhood behavioral difficulties[5,6]. Longitudinal studies that consider objective sleep measurement methods and behavioral problems are relatively rare in children with obesity, and the possibility of bidirectional development between sleep and behavioral problems requires further clarification.
We investigated the bidirectional temporal impact of sleep and behavioral problems in children with overweight and obesity using a cross-lagged panel model (CLPM) analysis based on a large-scale research cohort with three-wave data, the Adolescent Brain Cognitive Development (ABCD) study[4]. We aimed to enable the early prevention of psychiatric disorders in obese individuals by intervening in sleep and behavioral problems.
-
As described in the literature, the ABCD study (release 5.0 https://abcdstudy.org/) is the largest long-term study (baseline 2016-2018) of brain, health, and cognitive development, with a sample of 11,875 children (aged 9–10 years) from 21 recruitment sites across the U.S. using an epidemiologically informed recruitment strategy[4]. The current study included anthropometrics (height, weight, and body mass index [BMI]), demographics (age, sex, race/ethnicity, and household income), sleep problems, and behavioral data for three waves (wave 1 [baseline], wave 2, and wave 3) in children and adolescents. BMI was calculated as weight in kilograms divided by the square height in meters and converted to a BMI z-score (BMI-Z) according to the WHO growth standards for children. The 85th and 95th percentiles of BMI for age and sex were defined as cutoffs to identify children and adolescents at risk for overweight and obesity in this study (https://www.who.int/publications/i/item/924154693X). We excluded all articipants with outlying BMI values (below 10 and above 50 kg/m2) and included only individuals with both overweight and obesity from waves 1 to 3. The final sample comprised 2166 children (48.6% girls) aged 8–14 years without past or current psychiatric problems (based on the parent Kiddie Schedule for Affective Disorders and Schizophrenia, KSADS-5). Supplementary Figure S1 presents a flow graph illustrating the enrollment process.
Sleep problems were evaluated using the Sleep Disturbance Scale for Children (SDSC), a 26-item caregiver-reported instrument rated on a Likert-type scale designed to investigate the occurrence of sleep problems during the previous 6 months[4]. The SDSC generates a total sleep disturbance score and six subscale scores targeting specific sleep issues, including arousal disturbances, sleep hyperhidrosis, sleep-related breathing disorders, sleep-wake transition disturbances, difficulties in sleep onset and maintenance, and excessive somnolence. Total scores calculated using the sum of all items, ranging from 26 to 126, were analyzed in this study.
Emotional and behavioral problems were assessed using the 113-item Child Behavior Checklist (CBCL) validated for ages 6–18 years and completed by the child’s caregiver to identify the presence of psychiatric symptoms over the past six months[4]. The CBCL includes eight syndrome scales that contribute to the composite scores for internalizing, externalizing, and overall behavioral problems. The total CBCL score ranges from 0 to 240, with t-scores below 59 classified as non-clinical, t-scores between 60 and 64 indicating risk of clinical symptoms, and t-scores of 65 or greater suggesting clinically significant symptoms. This study focused on the assessment of the five subscales of the internalizing and externalizing dimensions.
CLPM analysis is widely used in psychological research to examine the temporal and bidirectional associations between variables using longitudinal data. CLPM evaluated reciprocal, time-varying relationships, and random intercept CLPM (RI-CLPM) further distinguished between- and within-person effects across waves (waves 1–3) in Mplus 8. The CLPM and RI-CLPM included the following covariates: age, income, sex, and race/ethnicity. Full model specifications, decision rules, fit criteria, and procedures for handling missing data are reported in Supplementary Methods.
-
This study included 2,166 overweight and obese children from waves 1 to 3, of whom 1,053 (48.6%) were female (Supplementary Table S1). Approximately 39.8% had household incomes above the 2016 U.S. median (USD 60,309). The participants were 61.22% White, 24.84% Black, 4.62% Asian, 3.55% Indian, and 5.77% other races/ethnicities (including Hispanic, Native American, Pacific Islander, or unspecified). Table 1 presents the time-varying characteristics. The mean ages were 9.49 ± 0.51, 10.48 ± 0.63, and 11.52 ± 0.68 for waves 1–3. Anxious/depressed and withdrawn/depressed symptoms increased from wave 1 to 2 but had declined at wave 3, whereas rule-breaking and aggressive behaviors consistently decreased across waves.
Table 1. Time-varying characteristics of the sample
Variable, mean [SD] Wave 1 (n = 2166) Wave 2 (n = 2166) Wave 3 (n = 2166) Statistic1 P Effect size2 Age (years) 9.49 (0.51) 10.48 (0.63) 11.52 (0.68) 26060.766 < 0.001 0.923 Grade 4th–5th 5th–6th 6th–7th BMI 24.01 (3.67) 25.72 (4.06) 27.24 (4.51) 1607.807 < 0.001 0.426 Total sleep problems 37.43 (9.02) 37.35 (8.88) 36.92 (8.56) 1.007 0.336 0.001 Anxious/depressed 53.45 (5.76) 53.53 (5.96) 53.16 (5.71) 5.161 0.006 0.002 Withdrawn/depressed 53.80 (6.04) 54.35 (6.63) 53.98 (6.26) 8.133 < 0.001 0.004 Somatic complaints 55.43 (6.24) 55.23 (6.31) 55.18 (6.28) 1.708 0.182 0.001 Rule-breaking behavior 52.86 (4.83) 52.75 (4.75) 52.38 (4.50) 12.506 < 0.001 0.006 Aggressive behavior 53.01 (5.73) 52.79 (5.40) 52.64 (5.25) 5.724 0.004 0.003 Note. 1One-way ANOVA for continuous variables; Chi-square test (χ2) for categorical variables. 2Eta-squared(η2) for ANOVA effect size; Cramer's V for Chi-square effect size. SD, standard deviation; BMI, body mass index. Supplementary Table S2 presents the bivariate correlations between sleep and behavioral problems across the three waves. Sleep problems at each wave showed strong positive correlations (r = 0.588 – 0.676, P < 0.01), indicating stability over time. Sleep problems were also positively and significantly correlated with the internalizing and externalizing dimensions across all waves (r = 0.268 – 0.463, P < 0.01). Notably, Pearson's correlations in the same behavioral dimensions across waves (e.g., anxious/depressed, waves 1 to 2: 0.633) were stronger than the cross-dimensional correlations. As shown in Supplementary Figure S2, the autoregressive coefficients for all variables, including sleep problems and the internalizing and externalizing dimensions, were significant (P < 0.01). Sleep problems at wave 1 significantly and positively predicted the internalizing and externalizing dimensions. At wave 2, sleep problems also significantly predicted subsequent withdrawn/depressed and somatic complaints and rule-breaking.
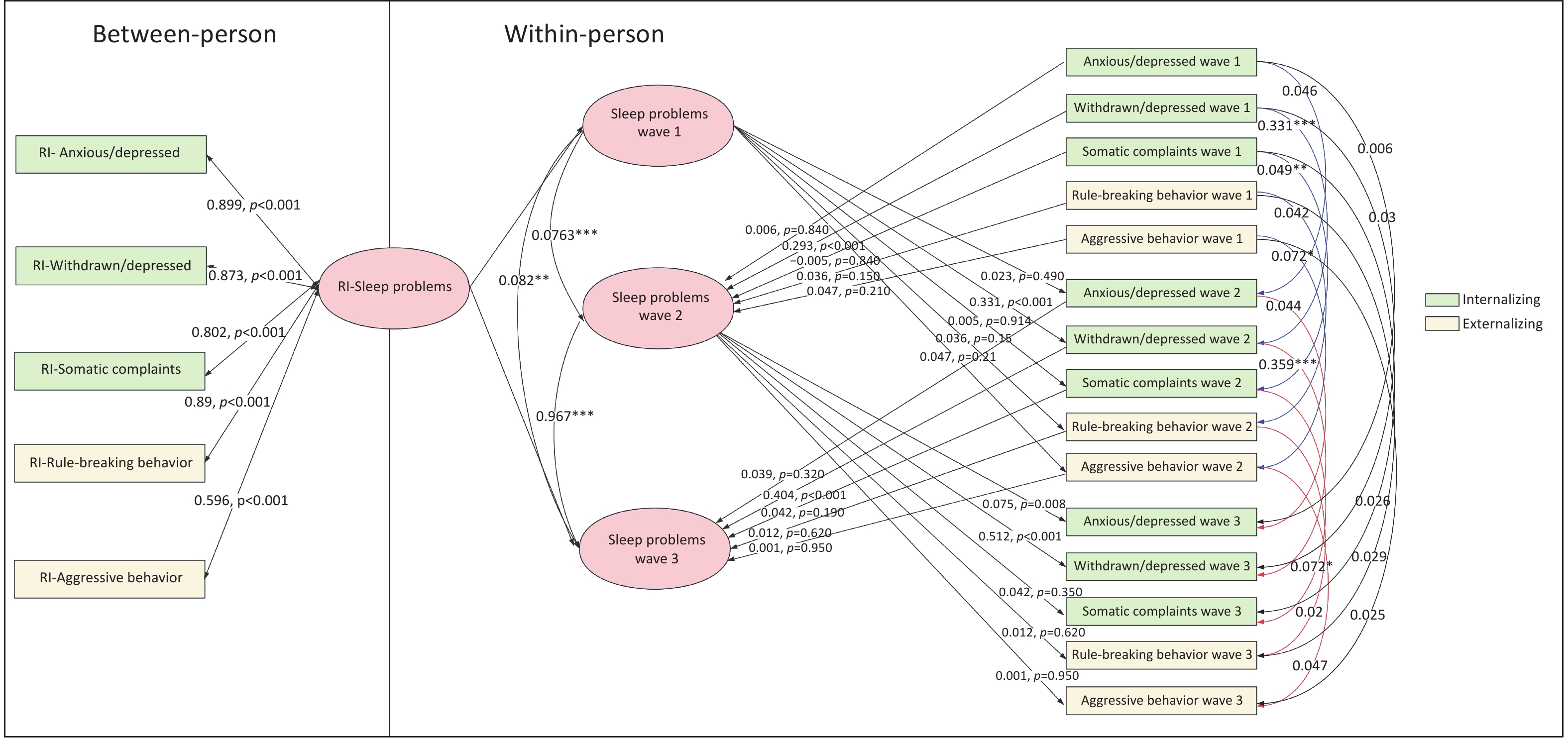
Sensitivity analyses were conducted within the CLPM framework, adjusting for age, household income, sex, and race/ethnicity. Figure 1 and Supplementary Table S3 show that sleep problems were positively associated with the internalizing and externalizing dimensions (waves 1 to 2 and waves 2 to 3) (all P < 0.05, with medium to large effect sizes). However, only withdrawn/depressed (β = 0.056, P < 0.05) in wave 1 and anxious/depressed (β = 0.076, P < 0.01) in wave 2 significantly and positively predicted sleep problem at subsequent waves.
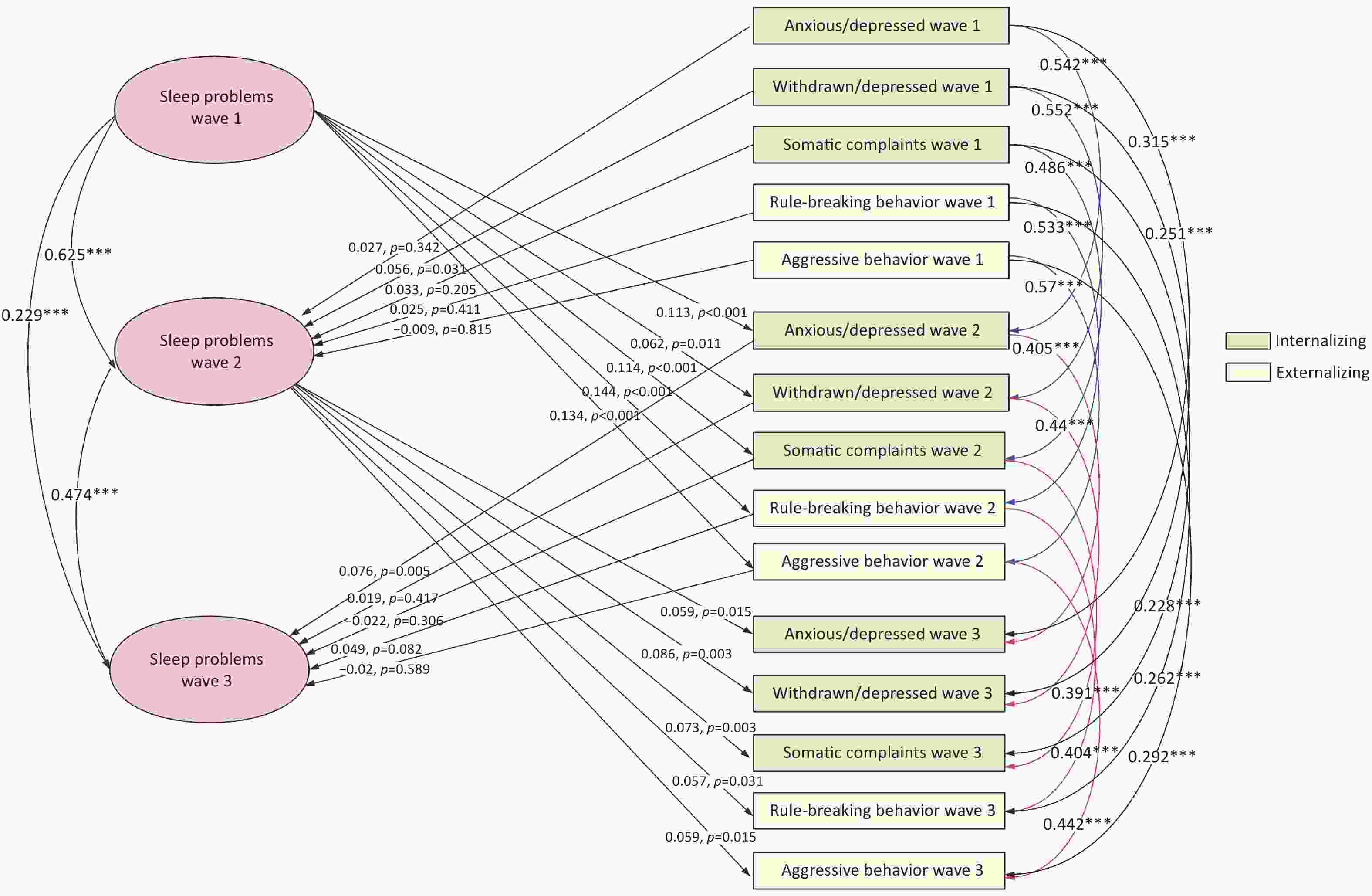
Figure 1. Cross-lagged model of sleep and behavioral problems in children and adolescents with overweight and obesity. Adjusted for age, income, sex, and race/ethnicity. *P < 0.05, **P < 0.01, ***P < 0.001.
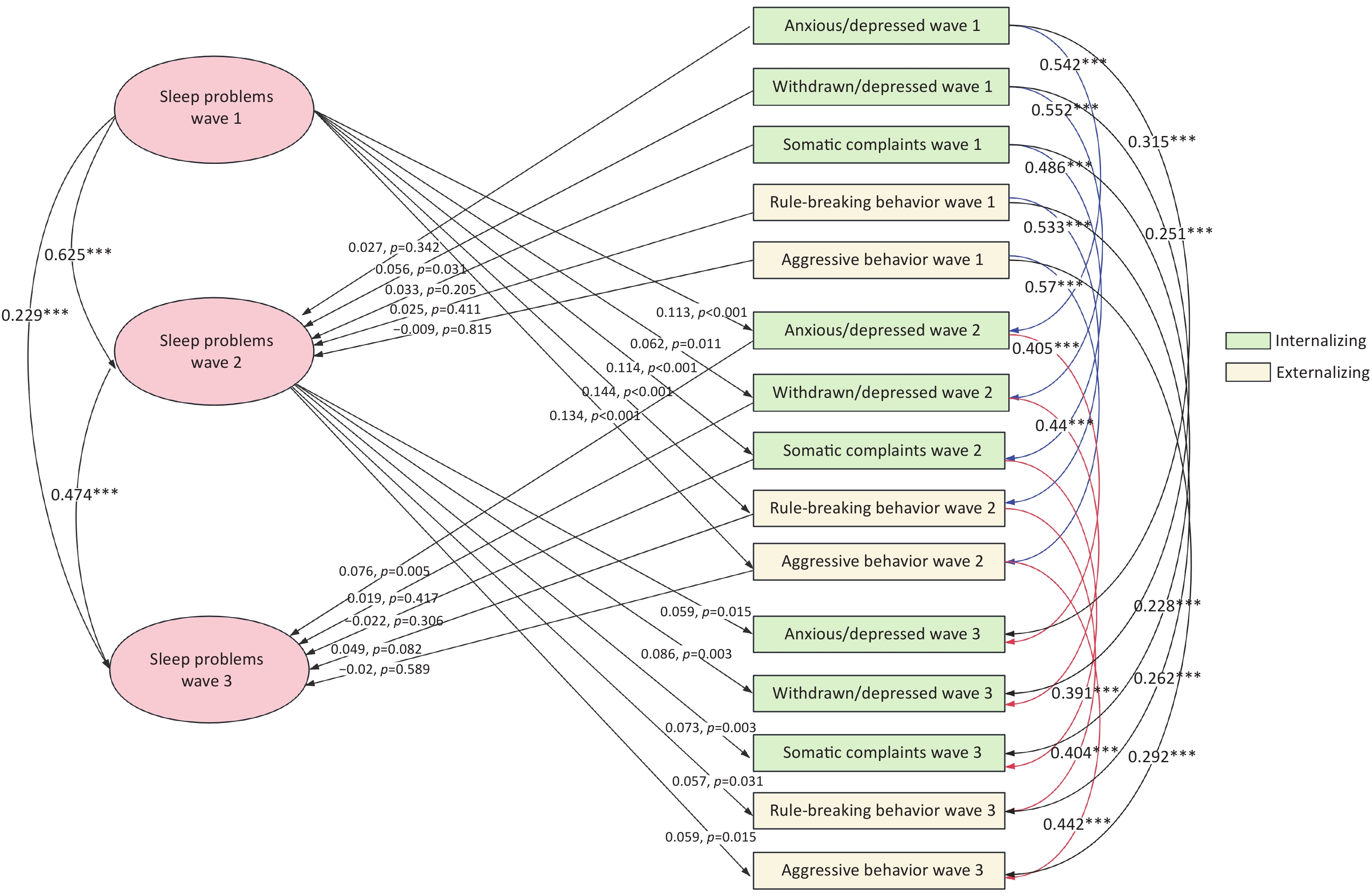
Figure 2 and Supplementary Table S4 indicate that RI-CLPM showed adequate fit (χ2/df = 16.17, P < 0.001; CFI = 0.965; TLI = 0.910; RMSEA = 0.018). After accounting for stable between-person differences, only withdrawn/depressed symptoms and sleep problems showed consistent bidirectional within-person associations. Specifically, temporary increases in sleep problems predicted later increases in withdrawn/depressed symptoms, and vice versa. A smaller unidirectional effect was observed from sleep problems at wave 2 to anxious/depressed symptoms at wave 3, whereas no other within-person paths were significant. At the between-person level, trait-like sleep problems were strongly correlated with all emotional/behavioral subscales (rs = 0.596–0.899, all P < 0.001), indicating that individuals with chronically higher sleep problems tended to have persistently elevated internalizing and externalizing difficulties. A Satorra–Bentler scaled χ2 difference test (Δχ2(38) = 20.62, P = 0.99) showed no significant differences, indicating that the stability and cross-lagged links between sleep problems and internalizing/externalizing symptoms were similar in male and female adolescents.
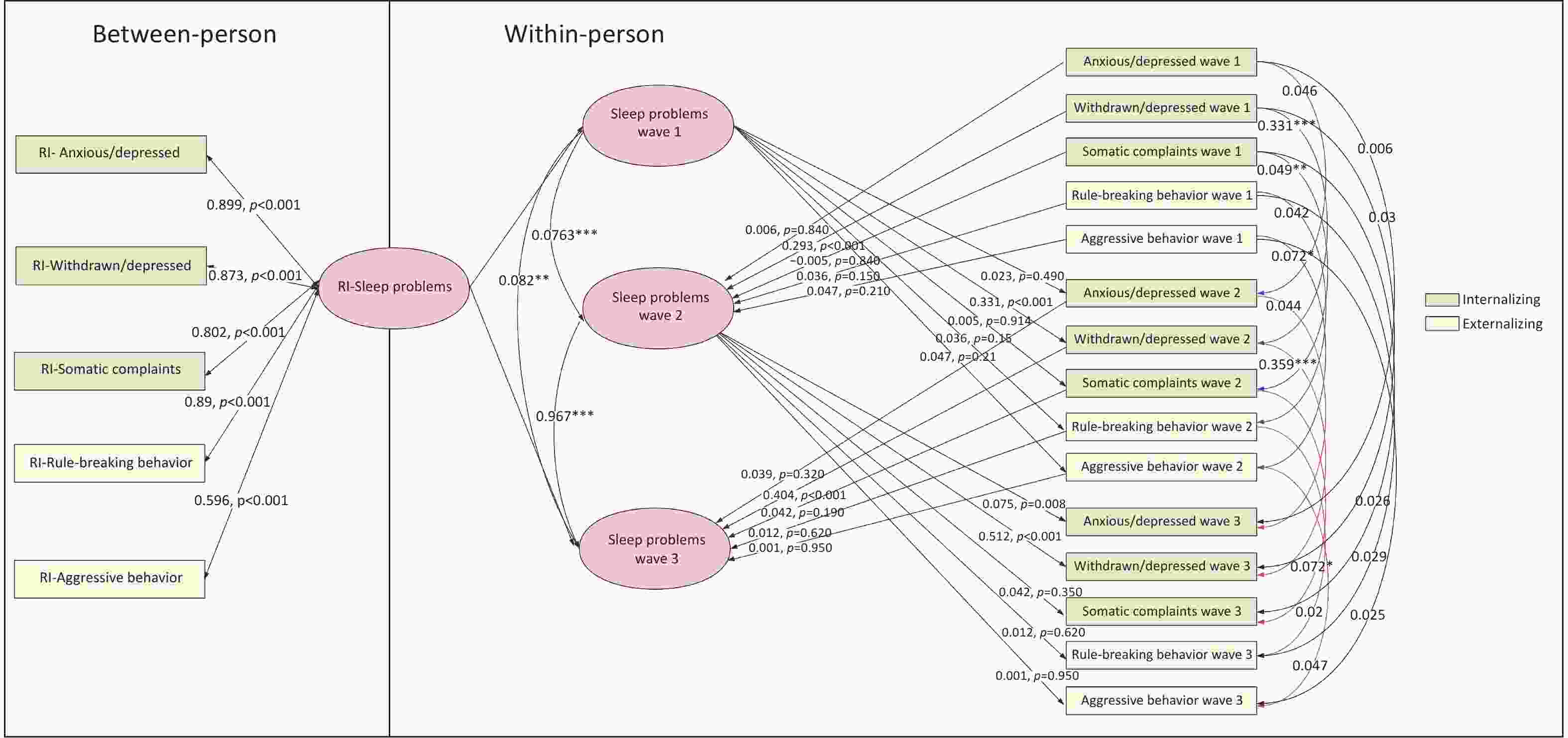
Figure 2. Random intercept cross-lagged model of sleep and behavioral problems in children and adolescents with overweight and obesity. Adjusted for age, income, sex, and race/ethnicity. *P < 0.05, **P < 0.01, ***P < 0.001.
-
This longitudinal study examined bidirectional associations between sleep and behavioral problems in children with overweight or obesity aged 9–10 years, using CLPM and RI-CLPM analyses across three waves (ages 9.49–11.52). These findings underscore that sleep problems contribute to behavioral difficulties, emphasizing the need to address sleep issues when managing the psychological well-being of children with overweight or obesity. Our results showed that sleep problems emerged as a significant predictor of subsequent internalizing symptoms, whereas withdrawn/depressed symptoms and sleep problems showed consistent bidirectional within-person associations across all waves. Several cross-sectional studies have found that sleep problems are closely associated with internalizing behavior problems, whereas the associations with externalizing behavior problems are inconsistent[5,6]. Another large longitudinal cohort study based on all children in the ABCD database revealed that sleep problems during the transition to adolescence were associated with subsequent internalizing and externalizing symptoms in the general population, but not vice versa[4]. Internalizing behaviors are characterized by distress responses, demonstrating a degree of stability across the lifespan[7], whereas externalizing behaviors are marked by overt distress responses and are more commonly observed in early life, but tend to show significant declines throughout childhood[7]. Thus, understanding the dynamic bidirectional relationship between poor sleep quality and behavior issues is important for early intervention.
Neuroendocrine dysregulation, particularly hypothalamic–pituitary–adrenal axis alterations and elevated cortisol levels, has been repeatedly linked to disturbed sleep. Increased cortisol reactivity in stressful situations and blunted recovery following a stressor may be biological substrates of depression, leading to heightened emotional reactivity and difficulties in stressful situations that manifest as poor coping responses to stressors and may lead to increased depression symptoms over time. Evidence has shown that central administration of corticotropin-releasing hormone or systemic administration of glucocorticoids can lead to arousal and sleeplessness[8,9]. Furthermore, converging evidence implicates the mesolimbic reward circuitry in depression-related anhedonia and sleep–wake regulation. Therefore, disruptions in reward processing may contribute to sleep initiation and maintenance problems in withdrawn/depressed youth, while sleep disturbance can further blunt reward responsiveness[10]. In addition, physiological and cognitive hyperarousal, which are common in depression and anxiety, directly impair sleep initiation and maintenance[11].
Collectively, these mechanisms offer a coherent explanation for why the internalizing domains (withdrawn/depressed and anxious/depressed) are uniquely predictive of subsequent sleep problems, whereas the other domains show weaker or null prospective effects. However, the effect size of somatic complaints on sleep problems was not significant. The non-significant effect of somatic complaints on sleep problems might be because children’s somatic symptoms sometimes manifest as transient complaints rather than chronic pain, and the CBCL does not assess additional pain dimensions, such as intensity, duration, and functional impact[12]. Future studies should incorporate more comprehensive pain assessment tools to better understand the relationship between somatic complaints and sleep problems.
This study had several limitations. First, causal relationships between sleep and behavioral problems could not be inferred. CLPM can suggest temporal associations but cannot establish definitive causality or fully account for unmeasured confounding factors. Second, the SDSC was used to measure sleep problems based on caregiver reports, which can be influenced by individual, cultural, and psychosocial factors. Wearable monitoring devices could be widely used in future studies. In addition, the effects of various sleep disorders and obesity severity on behavioral problems have not been thoroughly investigated. BMI changed over time in this cohort; however, this study did not include time-varying BMI in the primary CLPM or RI-CLPM because BMI changes may lie on the causal pathway, and routine adjustment could bias estimates toward the null. Future studies should incorporate time-updated BMI z-scores in sensitivity analyses and use models that distinguish confounding versus mediation to test whether changes in BMI co-evolve with changes in sleep and behavioral outcomes. Furthermore, the ABCD study is ongoing, suggesting that future research incorporating more data waves could better address these issues. Finally, racial and ethnic diversity in sleep problems is poorly understood and should be explored in future studies.
In conclusion, this study demonstrated a reciprocal relationship between sleep and behavioral problems in overweight and obese early adolescents. Sleep problems consistently predicted subsequent internalizing and externalizing difficulties, with a bidirectional association observed between sleep problems and internalizing symptoms, particularly withdrawn/depressed behaviors. These findings emphasize the clinical significance of early identification and intervention for sleep problems as a potential strategy to mitigate the development of emotional and behavioral problems, thereby supporting the incorporation of targeted sleep interventions in pediatric obesity management.
doi: 10.3967/bes2026.055
A Cross-lagged Panel Analysis of Sleep and Behavioral Problems in Children and Adolescents with Overweight and Obesity
-
Natural Science Foundation of Beijing Municipality under Grant No. 7232057.
The authors state no conflict of interest.
ABCD study received ethical approval in accordance with the ethical standards of the 1964 Declaration of Helsinki, and the informed consent of parents and the assent of children of all participants were collected.
Dongmei Wang and Wanling Zhang: Conceptualization, Methodology, Software, Data curation, Methodology, Writing- Original draft preparation. Hui Xu: Visualization, Project administration. Na Hu and Xiao Leng: Methodology, Investigation. Aihua Wang and Di Wu: Supervision, Validation, Writing- Reviewing and Editing. Ying Li: Software, Data curation, Writing- Reviewing and Editing.
&These authors contributed equally to this work.
注释:1) Funding: 2) Competing Interests: 3) Ethics: 4) Authors’ Contributions: -
Figure 1. Cross-lagged model of sleep and behavioral problems in children and adolescents with overweight and obesity. Adjusted for age, income, sex, and race/ethnicity. *P < 0.05, **P < 0.01, ***P < 0.001.
Figure 2. Random intercept cross-lagged model of sleep and behavioral problems in children and adolescents with overweight and obesity. Adjusted for age, income, sex, and race/ethnicity. *P < 0.05, **P < 0.01, ***P < 0.001.
Table 1. Time-varying characteristics of the sample
Variable, mean [SD] Wave 1 (n = 2166) Wave 2 (n = 2166) Wave 3 (n = 2166) Statistic1 P Effect size2 Age (years) 9.49 (0.51) 10.48 (0.63) 11.52 (0.68) 26060.766 < 0.001 0.923 Grade 4th–5th 5th–6th 6th–7th BMI 24.01 (3.67) 25.72 (4.06) 27.24 (4.51) 1607.807 < 0.001 0.426 Total sleep problems 37.43 (9.02) 37.35 (8.88) 36.92 (8.56) 1.007 0.336 0.001 Anxious/depressed 53.45 (5.76) 53.53 (5.96) 53.16 (5.71) 5.161 0.006 0.002 Withdrawn/depressed 53.80 (6.04) 54.35 (6.63) 53.98 (6.26) 8.133 < 0.001 0.004 Somatic complaints 55.43 (6.24) 55.23 (6.31) 55.18 (6.28) 1.708 0.182 0.001 Rule-breaking behavior 52.86 (4.83) 52.75 (4.75) 52.38 (4.50) 12.506 < 0.001 0.006 Aggressive behavior 53.01 (5.73) 52.79 (5.40) 52.64 (5.25) 5.724 0.004 0.003 Note. 1One-way ANOVA for continuous variables; Chi-square test (χ2) for categorical variables. 2Eta-squared(η2) for ANOVA effect size; Cramer's V for Chi-square effect size. SD, standard deviation; BMI, body mass index.  下载: 导出CSV
下载: 导出CSV
-
[1] Beltrán-Garrayo L, Solar M, Blanco M, et al. Examining associations between obesity and mental health disorders from childhood to adolescence: a case-control prospective study. Psychiatry Res, 2023; 326, 115296. doi: 10.1016/j.psychres.2023.115296 [2] Tsai SY, Tung YC, Huang CM, et al. Sleep and its variability in relation to behavioral outcomes in school-age children with overweight and obesity. Res Nurs Health, 2023; 46, 289−98. doi: 10.1002/nur.22308 [3] Morales-Ghinaglia N, Fernandez-Mendoza J. Sleep variability and regularity as contributors to obesity and cardiometabolic health in adolescence. Obesity (Silver Spring), 2023; 31, 597−614. doi: 10.1002/oby.23667 [4] Cooper R, Di Biase MA, Bei B, et al. Associations of changes in sleep and emotional and behavioral problems from late childhood to early adolescence. JAMA Psychiatry, 2023; 80, 585−96. doi: 10.1001/jamapsychiatry.2023.0379 [5] Guerlich K, Gruszfeld D, Czech-Kowalska J, et al. Sleep duration and problem behaviour in 8-year-old children in the Childhood Obesity Project. Eur Child Adolesc Psychiatry, 2022; 31, 519−27. doi: 10.1007/s00787-021-01731-8 [6] Torres-Lopez LV, Cadenas-Sanchez C, Migueles JH, et al. Associations of sleep-related outcomes with behavioral and emotional functioning in children with overweight/obesity. J Pediatr, 2022; 246, 170-8. e2. [7] Quiñones-Camacho LE, Hoyniak CP, Wakschlag LS, et al. Getting in synch: unpacking the role of parent-child synchrony in the development of internalizing and externalizing behaviors. Dev Psychopathol, 2022; 34, 1901−13. doi: 10.1017/S0954579421000468 [8] Opp MR. Corticotropin-releasing hormone involvement in stressor-induced alterations in sleep and in the regulation of waking. Adv Neuroimmunol, 1995; 5, 127−43. doi: 10.1016/0960-5428(95)00004-L [9] Chrousos GA, Kattah JC, Beck RW, et al. Side effects of glucocorticoid treatment: experience of the optic neuritis treatment trial. JAMA, 1993; 269, 2110−2. [10] Casement MD, Keenan KE, Hipwell AE, et al. Neural reward processing mediates the relationship between insomnia symptoms and depression in adolescence. Sleep, 2016; 39, 439−47. doi: 10.5665/sleep.5460 [11] Dressle RJ, Riemann D. Hyperarousal in insomnia disorder: current evidence and potential mechanisms. J Sleep Res, 2023; 32, e13928. doi: 10.1111/jsr.13928 [12] Van Dyk TR, Krietsch KN, King CD, et al. Prevalence of somatic and pain complaints and associations with sleep disturbance in adolescents with insomnia presenting to a behavioral sleep medicine clinic. J Clin Sleep Med, 2022; 18, 151−60. doi: 10.5664/jcsm.9522 -

 点击查看大图
点击查看大图
图(2) / 表ll (1)
计量
- 文章访问数: 19
- HTML全文浏览量: 8
- PDF下载量: 0
- 被引次数: 0

 Quick Links
Quick Links