

 下载:
下载:

-
Since the COVID-19 pandemic broke out, both the Chinese national government and the Beijing municipal government issued prevention and control measures to contain the spread of the disease. The Chinese Center for Disease Control and Prevention promptly introduced the Protocol for the Prevention and Control of COVID-19 to regulate the detection of infection and manage the close contact of those infected, while promptly updating the records. The Beijing Municipal Health Commission similarly introduced prevention and control measures and called upon the public to refrain from going outdoors as much as possible. Out of fear of COVID-19 and the unknown risks accompanying it, most residents reduced spending their time outside. Throughout their period of home quarantine, Beijing residents relied on delivery services for their necessities. This enabled smokers to take advantage of delivery services to secure cigarettes from take-out stores or online shops.
Prior to the pandemic, our research team had implemented campaigns in several Beijing communities to help people quit smoking, supporting 685 tobacco-dependent patients to quit smoking by providing smoking cessation drugs and access to regular follow-up services and online health education. However, quitting smoking is complex and closely related to social and psychological factors. According to relevant findings, the mental health of people worsened significantly during home quarantine[1]. Results of a cross-sectional survey showed an increase in anxiety levels in people in home isolation during the pandemic in China[2]. Tobacco dependency is a highly recurrent chronic disease closely affected by social, psychological, and physical factors, with changes in life potentially affecting individuals’ ability to quit smoking, and their smoking behavior in general.
However, there is a lack of research concerning the impact of the early stage of COVID-19 (March–April 2020) on smoking cessation. Based on these considerations, our study explores whether prevention and control measures taken during this stage of the pandemic have affected the smoking behavior of people in Beijing who were attempting to quit smoking.
All the subjects in this study were tobacco-dependent patients from 19 communities in Beijing. They indicated a willingness to quit smoking and had successively enrolled in the quit smoking interventions campaign conducted between December 2018 and December 2019 (inclusive). In this campaign, our quit-smoking-outpatient investigators and doctors conducted surveys using face-to-face interviews and questionnaires, carbon monoxide blowing tests, and pulmonary function tests. Results of these tests allowed us to formulate a specific plan for those wanting to quit smoking. The plan included a daily dose of smoking cessation drugs, a daily smoking reduction schedule, and other precautions. By participating in this campaign, the subjects received a three-month intervention aimed at quitting smoking, and at least a six-month follow-up to update their smoking status. Through this campaign, we created a hospital-community combined smoking cessation model which closely unites hospitals and communities to provide more convenient, diversified, and healthy smoking cessation intervention services.
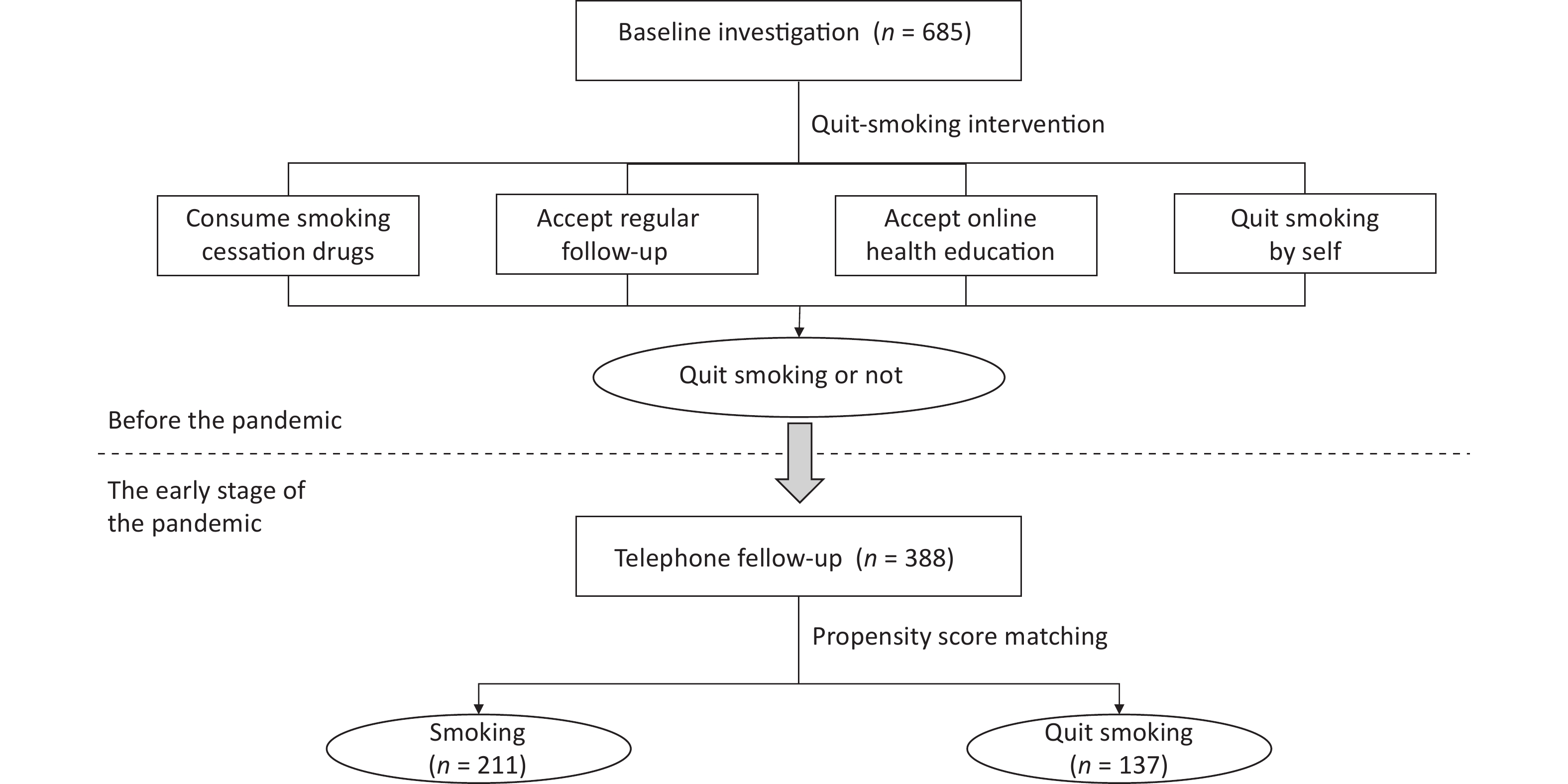
As a further exploration of this model, we conducted a telephone follow-up after the early stage of the COVID-19 pandemic (March–April 2020) to ascertain the smoking cessation status of the participants and evaluate the impact of this period on their smoking behavior. We divided the subjects into“smoking” and “quit smoking” group according to their status of smoking cessation. Since the subjects who participated in the quit-smoking campaign had received various degrees of smoking cessation intervention services before the pandemic, we conducted Propensity Score Matching (PSM) to elect homogeneous subjects for each group. All research processes are shown in Figure 1.
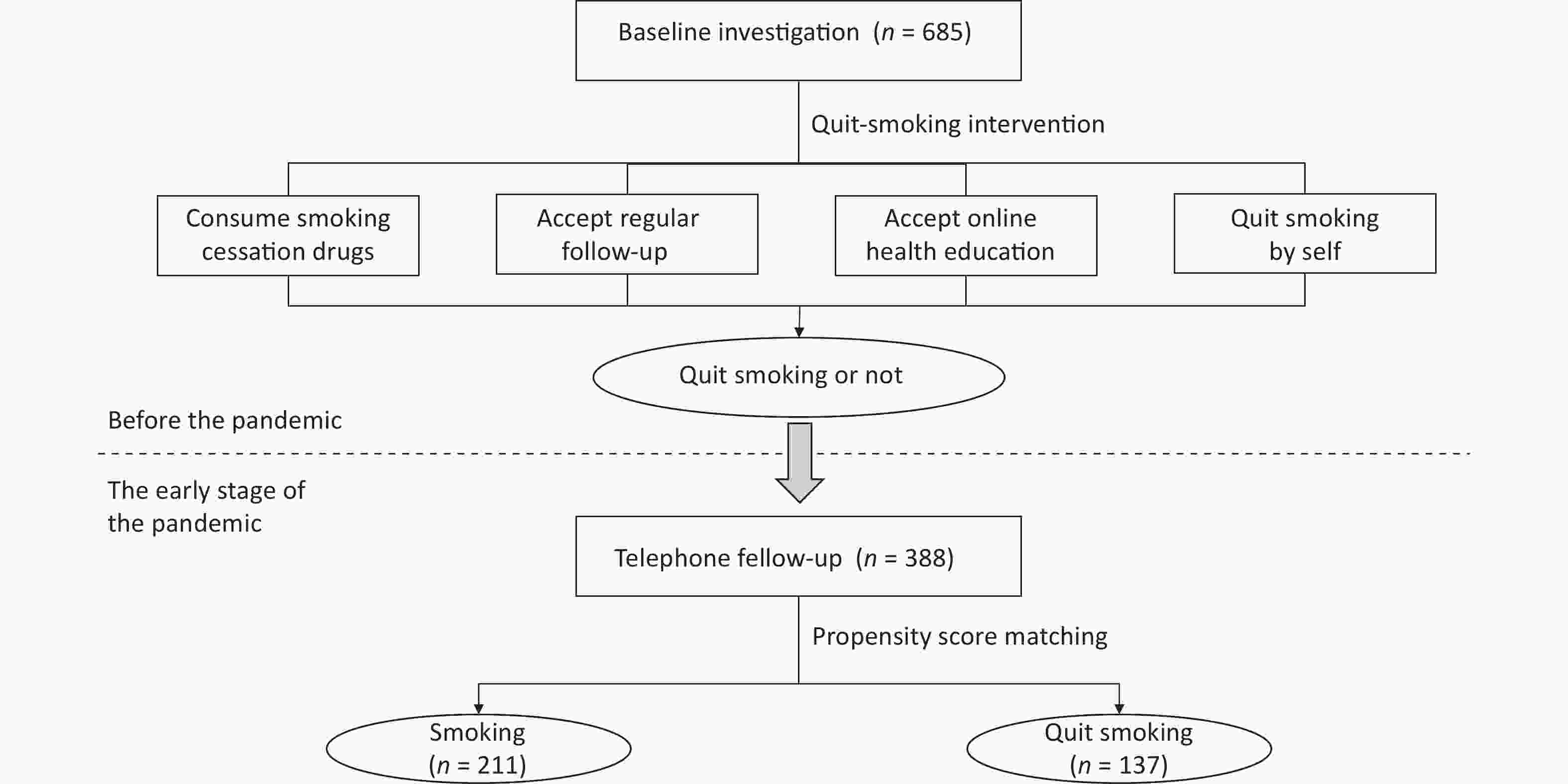
Figure 1. The invertigation process.
A total of 683 smokers participated in the quit-smoking intervention campaign, of which 388 were successfully followed up during the early stage of the pandemic (March–April 2020). Subsequently, 348 were selected via PSM.
The inclusion criteria in the sample were as follows:
A) 18 years old and above;
B) Permanent residents in Beijing (living in Beijing for at least six months);
C) Smokers, including:
a) regular smokers (smoking more than one cigarette per day, continuous or cumulative for six months[3]);
b) occasional smokers (smoking cigarettes more than four times a week but less than one cigarette per day on average); and
D) Can communicate fluently, and are willing to get involved in the survey.
The exclusion criteria were as follows:
A) Failure to belong in the artificial control or experimental groups according to the PSM; and
B) Refusal to participate in the follow-up interview.
All information was obtained via questionnaires conducted through face-to-face interviews prior to the early stage of the pandemic and telephone follow-up during that period. The questionnaire was based on the Smoking Abstinence Self-Efficacy Questionnaire (SASE), Russell’s Reasons for Smoking Questionnaire (RRSQ), and the Trait Coping Style Questionnaire (TCSQ).
The information collected prior to the early stage of the pandemic (before March 2020) includes the following:
A) Demographic information, including age, gender, marital status, education level, and others; and
B) Tobacco dependence. This includes:
a) Daily smoking amount (average daily cigarettes smoked over the last month);
b) Smoking history; and
c) Status of smoking cessation. Subjects were asked to self-report their 7-day smoking cessation rate[4] to consider quit smoking successfully or not .
Telephonic follow-ups during the pandemic included:
A) Home isolation (daily average time spent staying at home in the past two weeks whose answers include:
a) almost all day;
b) 80%–90% of the time;
c) 50%–80% of the time; and
d) less than 50% of the time)
B) Mood, including suspicion, anxiety, panic, distress, calmness, and “the same as usual” (“calmness” refers to the ability to think rationally about the pandemic, whereas “the same as usual” refers to an indifferent attitude); and
C) Smoking behavior, including:
a) daily smoking amount
b) status of smoking cessation: Subjects were asked to self-report their 7-day smoking cessation rate. Those who stopped smoking for at least 7 days were categorized as “Quit Smoking” group. By contrast, those who were still smoking at the time of the survey, including those who had relapsed after quitting, were categorized as “Smoking” group.
c) Smoking or relapsed reasons (because they wanted to feel “refreshed,” to dispel depression and boredom, for recreation, as a social activity, to imitate others, to relieve pressure, due to addiction, and due to habit),
The participants’ answers to these questions were self-evaluations. To prevent the participants from providing wrongful cognition or feedback to the questions during the investigation, all face-to-face and telephonic enumerators were given collective training. Simultaneously, a quality review and double data entry were implemented after the investigation to ensure the authenticity of the investigation information.
IBM SPSS Statistics 22.0 and R 2.15.3 were used for PSM and other statistical analyses. PSM was used to mitigate the influence of confounding biases, and make a comparison between“smoking” and “quit smoking” groups. Nearest Neighbor Matching was used, which was based on the following variables:
A) consumption of a quit smoking drug; and
B) receipt of regular follow-up service.
We used descriptive statistics to analyze the overall distribution of daily average time spent at home, psychological moods, smoking behavior, and others. The measurement data are expressed as x̅ ± s (95% CI), and the t-test was used to analyze the difference between the artificial control and experimental groups. The count data are expressed by percentage (%). The χ2 and the rank sum tests were used to conduct a correlation analysis of daily average time spent at home, psychological moods, the reasons for quitting smoking, and change in smoking behavior, before and after pandemic. All statistically significant differences were evaluated at P < 0.05.
Of the 348 subjects, 137 were categorized as quitters and 211 as non-quitters. There were 315 males, accounting for 90.5% of the sample size; 143 were 60 years old or above, accounting for 41.1% of the sample size; 308 subjects were married, accounting for 88.5% of the sample size; and 198 were senior high school graduates, accounting for 56.9% of the sample size. The difference between“smoking” and “quit smoking” groups were not statistically significant (P > 0.05), as shown in Table 1.
Table 1. Subjects basic demographic information [n (%)]
Variable Smoking (n = 211) Quit smoking (n = 137) t/χ2 P Gender-Male 193 (91.5) 122 (89.1) 0.319 0.572 Age [M (P25, P75)] 56 (40, 72) 59 (44, 74) −1.535 0.126 Marital status Married 180 (85.3) 128 (93.4) 6.125 0.190 Single* 31 (14.7) 9 (6.6) Education level Junior high school and below 11 (5.2) 6 (4.4) 1.639 0.441 Senior high school 125 (59.2) 73 (53.3) College degree and above 75 (35.5) 58 (42.3) Take smoking cessation drugs No 40 (19.0) 40 (29.2) 4.358 0.177 Yes 171 (81.0) 97 (70.8) Accept regular follow-up No 78 (37.0) 46 (33.6) 0.282 0.596 Yes 133 (63.0) 91 (66.4) Note. *Single include un-married, separated, divorced, and widowed. During the pandemic, the quitters’ change in their smoking behaviors was reflected in the reduction or increase of their daily smoking consumption amount. Of the 348 subjects included in this study, 85 reported that they quit smoking successfully before the pandemic, and 137 during the pandemic. More people have quit successfully under prevention and control during the early stages of the pandemic. The daily smoking amount decreased either from 11.06 ± 9.819 per day before the pandemic to 7.92 ± 8.900 per day during the pandemic. Both “smoking” and “quit smoking” groups have decreased their daily smoking amount, and the difference between before and after the pandemic were statistically significant (t = 4.96, 5.88, all P < 0.05). These results were consistent with the research results in other Chinese regions of Mao[5]. An American research states that though almost half of the subjects reported no change, the pandemic prompted about a quarter of respondents to reduce their tobacco use, and more than a third to have increased motivation to quit smoking[6]. This indicates that smokers generally had better smoking cessation status, or were better at quitting smoking during the pandemic than before it. The social aspects of the pandemic prevention measures may promote smoking cessation. People going outdoors (which became increasingly stunted during the pandemic and due to the quarantine) wore masks as a compulsory requirement, thereby making smoking inconvenient and unsafe. We should seize this opportunity to encourage more smokers to quit, strengthen health education on smoking, and establish a smoke-free environment.
During the pandemic, 63.8% of the subjects said that they stayed at home almost all day, with some reporting that they experienced anxiety, distress, panic, and feelings of suspicion. The status of smoking cessation (“smoking” group vs. “quit smoking” group) and feelings due to the pandemic (Worried, χ2 = 6.27, P < 0.05; Calm, χ2 = 7.00, P < 0.05; and “Almost as usual,” χ2 = 4.57, P < 0.05) were independent, as shown in Table 2. Although suffering through the pandemic, the participants generally reported an optimistic mood. However, some also expressed negative emotions like anxiety, depression, panic, and doubt. In this study, we found that incidences of smoking increased among those experiencing a depressed mood, while calm emotions led to positive changes in smoking behaviors. During the telephonic follow-up, some reported that they had experienced negative psychological effects, such as anxiety and depression, due to the pandemic, causing them to continue smoking. A contemporaneous related study about e-cigarette usage during the pandemic-induced lockdown in Italy showed that new smokers were more likely to report symptoms of anxiety[7]. A California research shows that cigarette users may be smoking more during the lockdown because of their increased stress levels[8]. When a smoker is depressed, the stimulation due to smoking becomes amplified. For those people trying to quit smoking, correct emotional management methods should be implemented to avoid using tobacco as a mood enhancer[1]. Therefore, it is necessary to conduct online health education and psychological counseling for those who want to quit smoking, encouraging healthy lifestyles and good mental health.
Table 2. Comparison of daily home stay time and psychological moods of subjects [n (%)]
Variable All subjects (n = 348) Smoking (n = 211) Quit smoking (n = 137) χ2 P Daily home stay time Almost all day 222 (63.8) 135 (64.0) 87 (63.5) 1.643 0.650 80%–90% 35 (10.1) 18 (8.5) 17 (12.4) 50%–80% 43 (12.4) 27 (12.8) 16 (11.7) Less than 50% 48 (13.8) 31 (14.7) 17 (12.4) Moods (multiple choice) Suspected 4 (1.1) 4 (1.9) 0 (0.0) 1.224 0.269 Worried 60 (17.2) 45 (21.3) 15 (10.9) 6.270 0.012* Panic 16 (4.6) 10 (4.7) 6 (4.4) 0.025 0.876 Depressed 26 (7.5) 18 (8.5) 8 (5.8) 0.870 0.351 Calm 165 (47.8) 88 (41.7) 77 (56.2) 7.003 0.008* Almost as usual 283 (81.3) 164 (77.7) 119 (86.9) 4.565 0.033* Smoke craving because of the pandemic No 306 (87.9) 185 (87.7) 121 (88.3) 0.032 0.857 Yes 42 (12.1) 26 (12.3) 16 (11.7) Smoking/relapse reason (multiple choice) Refreshing 4 (1.1) 4 (1.9) 0 (0.0) 1.224 0.269 Dispelling depression and boredom 51 (14.7) 46 (21.8) 5 (3.6) 21.881 < 0.001* Recreation 56 (16.1) 52 (24.6) 4 (2.9) 29.035 < 0.001* Social activities 18 (5.2) 17 (8.1) 1 (0.7) 9.092 0.003* Imitating 2 (0.6) 2 (0.9) 0 (0.0) 2.009 0.156 Reliving pressure 16 (4.6) 15 (7.1) 1 (0.7) 7.706 0.006* Addiction and habits 75 (21.6) 72 (34.1) 3 (2.2) 50.101 < 0.001* Note. *P-value < 0.05. In terms of the reasons attributed to continued smoking or relapsing, the status of smoking cessation (“smoking” group vs. “quit smoking” group) was independent with dispelling depression and boredom (χ2 = 21.88, P < 0.05), recreation (χ2 = 29.03, P < 0.05), social activities (χ2 = 9.09, P < 0.05), relieving pressure (χ2 = 7.70, P < 0.05), and addiction and habits (χ2 = 50.10, P < 0.05), as shown in Table 2). As the time spent at home increased, those trying to quit smoking tended to intensify their desire and dependence on tobacco. Smoking occurs due to certain environmental temptations, and is strengthened by long-term repeated reinforcement. A lot of leisure time at home made theses temptations increased. In quitting smoking, an individual needs to break these addictions and habits. However, environmental temptations often lead to failure in attempting to quit smoking. As a result, smokers may start smoking unconsciously when resting or after waking up in the morning. The results of a cross-sectional study about home isolation and lifestyle in Italy between April and June 2020 makes the same argument[9]. During the period of home isolation, the risk factor of environmental temptation was amplified. Smoking cessation behavior therapy should be used to break the connection between smoking behavior and certain activities, directing attention toward cultivating new interests and enjoying alternative behavior instead of smoking.
Moreover, as people who attempt to quit smoking spend more time at home, the supervision and support of family members, along with rules not allowing to smoke at home, played a positive role in reducing smoking behavior. Recent research from Japan shows that, during the lockdown, people who worked from home or lived alone might have changed their smoking behavior for the worse[10]. Therefore, it is necessary to build a supportive “smoke-free family environment,” where family members give maximum encouragement to those seeking to quit smoking successfully.
Despite our findings, this study has certain limitations. The participants in this study were mostly male, old, and retired. It may lead to less stress in these subjects. In the same way, during periods of isolation, younger people are under greater levels of stress from work and jobs than older people, showing an increase in cigarette consumption. Moreover, as this study was based on further explorations of smoking cessation campaigns, all the respondents were participants in smoking cessation interventions before. The willingness to quit smoking was higher among participants of the current study than that of other smokers in general.
Thus, during pandemic-induced home isolation, more people have successfully quit smoking in Beijing, with daily smoking consumption decreasing significantly. Maintaining a calm psyche was conducive to successful smoking cessation. Building a smoke-free family environment is recommended, where family members give smokers greater support, encouragement, and supervision to enhance their determination and confidence in quitting smoking. In the recurrence of a pandemic, those wanting to quit smoking may suffer from more negative emotions like depression. Thus, smoking cessation services should provide more convenient guidance on alleviating negative emotions, and help individuals break the existing connection between their smoking habits and specific situations, letting them enjoy a healthy smoke-free life.
doi: 10.3967/bes2023.054
-
The authors declare no conflicts of interest in the present study.
注释:1) Conflict of Interest: -
Table 1. Subjects basic demographic information [n (%)]
Variable Smoking (n = 211) Quit smoking (n = 137) t/χ2 P Gender-Male 193 (91.5) 122 (89.1) 0.319 0.572 Age [M (P25, P75)] 56 (40, 72) 59 (44, 74) −1.535 0.126 Marital status Married 180 (85.3) 128 (93.4) 6.125 0.190 Single* 31 (14.7) 9 (6.6) Education level Junior high school and below 11 (5.2) 6 (4.4) 1.639 0.441 Senior high school 125 (59.2) 73 (53.3) College degree and above 75 (35.5) 58 (42.3) Take smoking cessation drugs No 40 (19.0) 40 (29.2) 4.358 0.177 Yes 171 (81.0) 97 (70.8) Accept regular follow-up No 78 (37.0) 46 (33.6) 0.282 0.596 Yes 133 (63.0) 91 (66.4) Note. *Single include un-married, separated, divorced, and widowed.  下载: 导出CSV
下载: 导出CSV
Table 2. Comparison of daily home stay time and psychological moods of subjects [n (%)]
Variable All subjects (n = 348) Smoking (n = 211) Quit smoking (n = 137) χ2 P Daily home stay time Almost all day 222 (63.8) 135 (64.0) 87 (63.5) 1.643 0.650 80%–90% 35 (10.1) 18 (8.5) 17 (12.4) 50%–80% 43 (12.4) 27 (12.8) 16 (11.7) Less than 50% 48 (13.8) 31 (14.7) 17 (12.4) Moods (multiple choice) Suspected 4 (1.1) 4 (1.9) 0 (0.0) 1.224 0.269 Worried 60 (17.2) 45 (21.3) 15 (10.9) 6.270 0.012* Panic 16 (4.6) 10 (4.7) 6 (4.4) 0.025 0.876 Depressed 26 (7.5) 18 (8.5) 8 (5.8) 0.870 0.351 Calm 165 (47.8) 88 (41.7) 77 (56.2) 7.003 0.008* Almost as usual 283 (81.3) 164 (77.7) 119 (86.9) 4.565 0.033* Smoke craving because of the pandemic No 306 (87.9) 185 (87.7) 121 (88.3) 0.032 0.857 Yes 42 (12.1) 26 (12.3) 16 (11.7) Smoking/relapse reason (multiple choice) Refreshing 4 (1.1) 4 (1.9) 0 (0.0) 1.224 0.269 Dispelling depression and boredom 51 (14.7) 46 (21.8) 5 (3.6) 21.881 < 0.001* Recreation 56 (16.1) 52 (24.6) 4 (2.9) 29.035 < 0.001* Social activities 18 (5.2) 17 (8.1) 1 (0.7) 9.092 0.003* Imitating 2 (0.6) 2 (0.9) 0 (0.0) 2.009 0.156 Reliving pressure 16 (4.6) 15 (7.1) 1 (0.7) 7.706 0.006* Addiction and habits 75 (21.6) 72 (34.1) 3 (2.2) 50.101 < 0.001* Note. *P-value < 0.05.
下载: 导出CSV
-
[1] Ma KX, Zhang YD, Hou TY, et al. Investigation of physical and mental health in isolated people during the outbreak of novel coronavirus pneumonia. Chin J Clin Med, 2020; 27, 36−40. (In Chinese [2] Li J, Wang SH, Yu RH, et al. Compliance of home quarantine protection and its effect on anxiety degree during the epidemic outbreak period of COVID-19. Chin J Infect Control, 2020; 19, 404−10. (In Chinese [3] Qian JC, Cai M, Gao J, et al. Trends in smoking and quitting in China from 1993 to 2003: national health service survey data. Bull World Health Organ, 2010; 88, 769−76. doi: 10.2471/BLT.09.064709 [4] Jiang B, He Y, Zuo F, et al. Effectiveness of Varenicline with counseling programs on smoking cessation in a targeted clinical setting in China. Chin J Epidemiol, 2014; 35, 1349−53. (In Chinese [5] Mao YM, Zheng PP, Wang B, et al. Cognition of the relationship between smoking and COVID-19 and its impact on daily cigarette consumption among smokers. Fudan Univ J Med Sci, 2020; 47, 830−6. (In Chinese [6] Klemperer EM, West JC, Peasley-Miklus C, et al. Change in tobacco and electronic cigarette use and motivation to quit in response to COVID-19. Nicotine Tob Res, 2020; 22, 1662−3. [7] Gallus S, Stival C, Carreras G, et al. Use of electronic cigarettes and heated tobacco products during the Covid-19 pandemic. Sci Rep, 2022; 12, 702. doi: 10.1038/s41598-021-04438-7 [8] Gonzalez M, Epperson AE, Halpern-Felsher B, et al. Smokers are more likely to smoke more after the COVID-19 California lockdown order. Int J Environ Res Public Health, 2021; 18, 2582. doi: 10.3390/ijerph18052582 [9] Ferrante G, Camussi E, Piccinelli C, et al. Did social isolation during the SARS-CoV-2 epidemic have an impact on the lifestyles of citizens? Epidemiol Prev, 2020; 44, 353−62. [10] Koyama S, Tabuchi T, Okawa S, et al. Changes in smoking behavior since the declaration of the COVID-19 state of emergency in Japan: A cross-sectional study from the Osaka Health App. J Epidemiol, 2021; 31, 378−86. doi: 10.2188/jea.JE20200533 -

 点击查看大图
点击查看大图
图(1) / 表ll (2)
计量
- 文章访问数: 765
- HTML全文浏览量: 318
- PDF下载量: 19
- 被引次数: 0

 Quick Links
Quick Links