

 下载:
下载:

-
Coronavirus disease 2019 (COVID-19) continues to spread around the world [1-4]. As of November 18, 2021, confirmed cases had exceeded 250 million, and more than 5 million people had died [5]. Without large-scale vaccination coverage and effective drugs [3-4], early detection and management of infected individuals and their close contacts remain an important strategy to prevent the transmission of the virus [6]. Diagnosis is typically based on exposure history, clinical symptoms, laboratory testing, and chest imaging examinations. The clinical signs and symptoms of COVID-19 are especially important for quickly identifying suspected patients and their close contacts.
The most prominent symptoms of COVID-19 are fever, dry cough, and fatigue, all of which have been widely recognized [7]. However, olfactory dysfunction (OD) has been of concern following the first case report in mid-March of 2020 [8]. The prevalence of OD varies greatly across studies and countries. Gustatory dysfunction (GD) has also been identified as a presenting symptom of COVID-19 infection [9-11]. Sudden anosmia has been shown as an early isolated COVID-19 symptom, and patient-reported olfaction has been used as a screening tool for COVID-19 infection in many institutions [12-14]. One multicenter European study showed that 85.6% of patients with COVID-19 had OD [15]; however, a survey from Korea showed that OD or GD was observed in only 15.3% of patients [16]. A report from China demonstrated that the proportion of OD among patients with COVID-19 was even lower (5.6%) [17]. The pathogenesis of COVID-19 with OD is unclear, as are its clinical treatment and care [18]. Previous studies have revealed that a majority of ambulatory patients with COVID-19 spontaneously recover olfactory function, whereas some patients develop persistent anosmia [19-20]. To date, we know little about the long-term follow-up of patients with COVID-19 and OD. Some symptoms can take several months to improve, which could lead to serious consequences [21]. Additionally, these clinical presentations could significantly impact patients’ quality of life and mental well-being [22].
In mainland China, the COVID-19 epidemic is well under control; however, the challenges caused by imported cases have increased dramatically. As of January 17, 2021, the number of imported cases had reached 4,518 [23]. Because of economic globalization, every country will likely experience imported cases and should regard these patients as a focus group. It is urgent for the global community to understand these cases, yet no studies on them have been performed to date. Here we present a study on 11 imported patients with COVID-19 with OD or GD treated at a designated hospital in a Chinese province that had no local cases reported from March to November 2020 [24]. We aimed to understand these patients’ clinical presentations, treatment outcomes during hospitalization, and 12-month follow-up after discharge.
-
We designed our research as a prospective follow-up case series study with a 12-month follow-up of all patients with COVID-19 and OD who arrived from other countries and were admitted to the COVID-19-designated hospital (Xi’an No. 8 Hospital) in Shaanxi Province, China. They were followed up between August 19, 2021, and December 12, 2021. The participants comprised 11 patients from seven countries. Diagnosis and treatment of COVID-19 were based on Chinese national guidelines for the diagnosis and treatment of COVID-19 (eighth edition) [25]. The inclusion criteria were patients arriving in China with independent expression ability and self-reported OD.
This study has been registered at the Chinese Clinical Trial Registry (
http://www.chictr.org.cn/enindex.aspx ) by the Xi’an No. 8 Hospital (chictr.org Identifier: ChiCTR2000040628). Given that the study used secondary data from the hospital’s electronic medical records, we sought a waiver for informed consent, which was approved by the relevant ethics committees. -
Fever was defined as an axillary temperature of at least 37.3 °C. COVID-19 disease severity was categorized as mild or moderate on the basis of Chinese national guidelines for the diagnosis and treatment of COVID-19 (eighth edition) [25]. Mild cases were defined as patients with mild clinical symptoms and no signs of pneumonia on imaging. Moderate cases were defined as patients showing fever and respiratory symptoms with radiological findings of pneumonia.
The duration of viral shedding was defined as the interval from the first day of a positive reverse transcription-polymerase chain reaction (RT-PCR) test to the date of the first negative test among three consecutive negative results before discharge (e.g., a positive RT-PCR on September 1, 2020, a negative RT-PCR on September 15, 2020, a negative RT-PCR on September 17, 2020, and another negative RT-PCR before discharge on September 20, 2020; with three negative RT-PCR results, the duration of viral shedding was calculated as 14 days).
Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared (kg/m2). Weight was measured with a scale, and height was obtained by self-report on admission. BMI for adults was classified into four groups as follows: underweight (BMI < 18.5), normal weight (18.5 ≤ BMI < 24.0), overweight (24.0 ≤ BMI < 28.0), and obese (BMI ≥ 28.0) [26].
-
The criteria for discharge were the absence of fever for at least 3 days, obvious improvement in respiratory symptoms, substantial improvement in pulmonary imaging, and two nasopharyngeal swab samples negative for SARS-CoV-2 obtained at least 24 h apart [17]. After discharge, the patients were isolated for another 14 days, with the same health monitoring adopted during quarantine.
-
The study collected each patient’s demographic, clinical, laboratory, and radiological data from the electronic medical records of the hospital. If the core data were missing or unclear, we contacted the attending clinician who was responsible for patient care and follow-up. A follow-up telephone survey, including OD recovery, sequelae type, and recurrent status, was performed at 1-, 6-, and 12-month after discharge.
Continuous variables were presented as median, interquartile ranges (IQRs), or simple ranges, as appropriate. Categorical variables were described as counts and percentages. All the data analyses were performed with SAS software (version 9.4, SAS Institute Inc., Cary, NC, USA). The clinical course and follow-up were drawn using the Python Matplotlib package (version 3.2.1).
-
In this study, a total of 11 patients with COVID-19 and OD were enrolled. Only one patient also had GD. All the patients were imported from other countries and treated in Xi’an No. 8 Hospital. During this period, a total of 246 imported COVID-19 cases were reported; thus, the proportion of OD among the overall imported case total was 4.5% (11/246).
The median patient age was 34 (IQR 23–46) years; 81.8% (9/11) were men, and 27.3% (3/11) had comorbidities (hypertension in two cases and hepatitis B in one case). Of the total OD cases, 54.5% (6/11) and 45.5% (5/11) had moderate and mild COVID-19, respectively. Of the 11 patients, 72.7% (8/11) had normal weight, 18.2% (2/11) were overweight, and 9.1% (1/11) had obesity. All the patients were diagnosed upon entering China; of these, 63.6% (7/11) were from Asia (two from Kazakhstan, three from Uzbekistan, and two from the United Arab Emirates), 18.2% (2/11) were from Africa (Angola and Liberia), and the other 18.2% (2/11) were from Europe (Belgium and the UK). Detailed characteristics are shown in Table 1 and Figure 1.
Table 1. Demographics, clinical characteristics, treatment outcomes, and follow up of 11 imported COVID-19 cases with olfactory dysfunction
Characteristics Case 1 Case 2 Case 3 Case 4 Case 5 Case 6 Case 7 Case 8 Case 9 Case 10 Case 11 Age (years) 19 52 22 37 23 23 35 24 47 46 34 Gender Male Male Male Male Male Female Male Female Male Male Male Occupation Student Salary employee Student Semi-skilled employee Salary employee Unemployed Salary employee Student Salary employee Salary employee Semi-skilled employee Body mass index (kg/m2) 24.8 23.7 23.7 24.2 20.0 18.8 20.0 22.1 28.7 22.6 23.0 Comorbidity Hypertension Hypertension No No No No No No No Hepatitis B No Complication No No No Liver injury No No No No Liver injury No No Imported country Kazakhstan Kazakhstan Britain Liberia United Arab Emirates United Arab Emirates Uzbekistan Uzbekistan Angola Uzbekistan Belgium Clinical classification Mild Moderate Mild Moderate Mild Mild Moderate Mild Moderate Moderate Moderate Symptoms and signs Hyposmia Yes No No Yes Yes No Yes No Yes No Yes Anosmia No Yes Yes No No Yes No Yes No Yes No Hypogeusia No No No No No No Yes No No No No Fever No No No No No No No No No No Yes Cough No No No Yes No No Yes Yes No Yes Yes Fatigue No Yes No No No No No No No No No Rhinorrhea No No No No No No No No No No No Nasal congestion No No No No No Yes No No No No No Sore throat No No No Yes No Yes No Yes Yes No No Myalgia No No No No No No No No No No No Diarrhea No No No No No No No No Yes No No Treatment Antiviral Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Antibiotic No No No Yes No No No No Yes No Yes Traditional Chinese medicine Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Corticosteroids No No No Yes No No No No Yes No Yes Intravenous
immunoglobinNo Yes Yes Yes Yes No Yes No Yes Yes Yes Hepatoprotective
therapyNo No No Yes No Yes Yes Yes Yes Yes Yes Treatment outcome Cured Cured Cured Cured Cured Cured Cured Cured Cured Cured Cured Follow up 1-month OD No recovery* Recovery No recovery* Recovery Recovery No recovery* Recovery Partial recovery# Recovery Recovery Recovery Other sequelae Anxiety, fatigue, difficulty sleeping No No No No Throat discomfort, Fatigue, No No Fatigue Difficulty sleeping, Fatigue Throat discomfort Re-positive Yes No Yes No No Yes No No No No No 6-month OD Partial recovery# No Partial recovery# Recovery Recovery Partial recovery# Recovery Recovery OD Recovery Recovery Other sequelae Hair loss, anxiety, fatigue and difficulty sleeping No No No No Throat discomfort No No Fatigue Difficulty sleeping Throat discomfort, hair loss Re-positive No No No No No No No No No No No 12-month OD Partial recovery# Recovery Recovery Recovery Recovery Recovery Recovery Recovery Partial recovery# Recovery Recovery Other sequelae Hair loss, anxiety, fatigue, difficulty sleeping No No No No Throat discomfort No No Fatigue Difficulty sleeping Hair loss
, anxietyRe-positive No No No No No No No No No No No Note. *No recovery: patients with OD were considered that who do not report any improvement for smell for odors. #Partial recovery: patients with OD were considered that who subjectively start to smell some odors. OD, olfactory dysfunction. 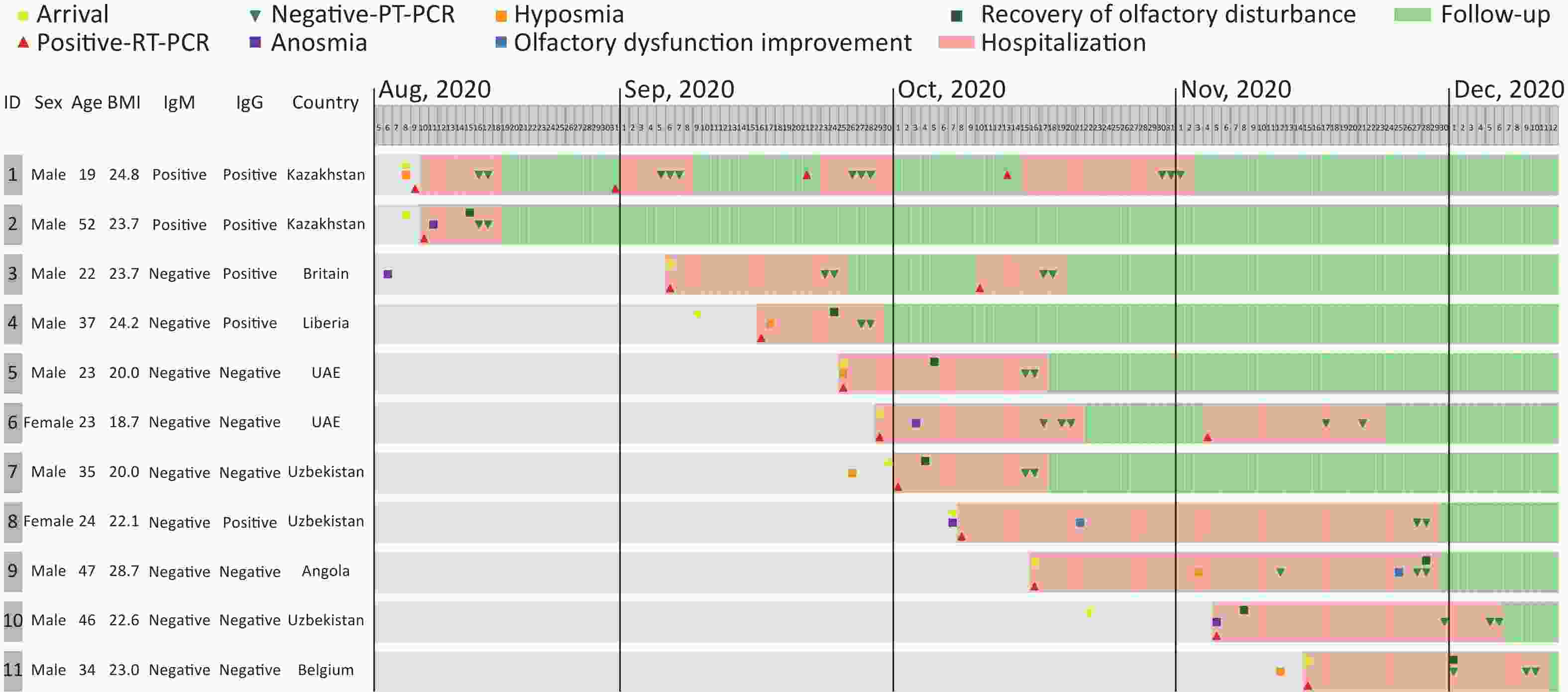
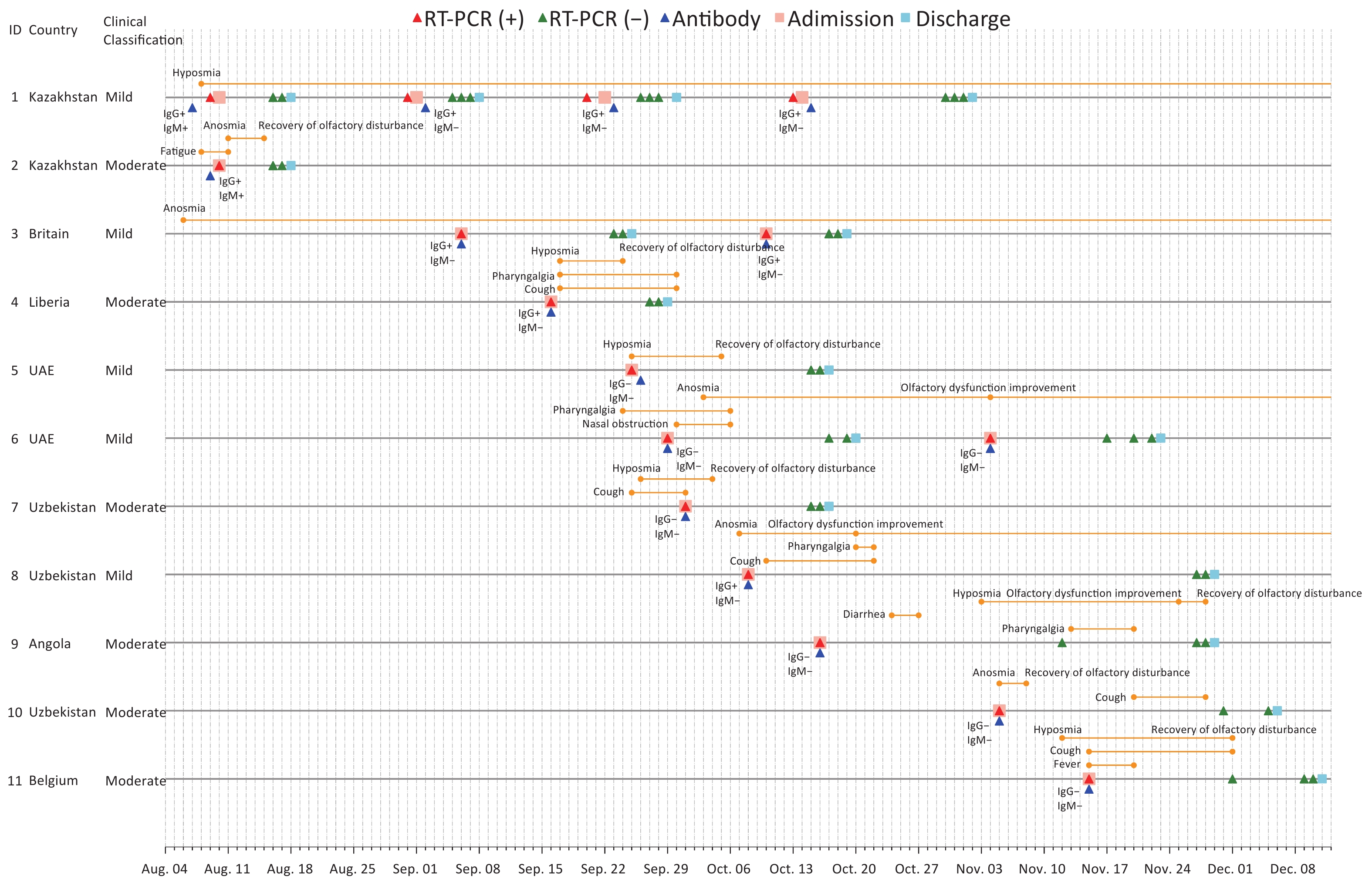
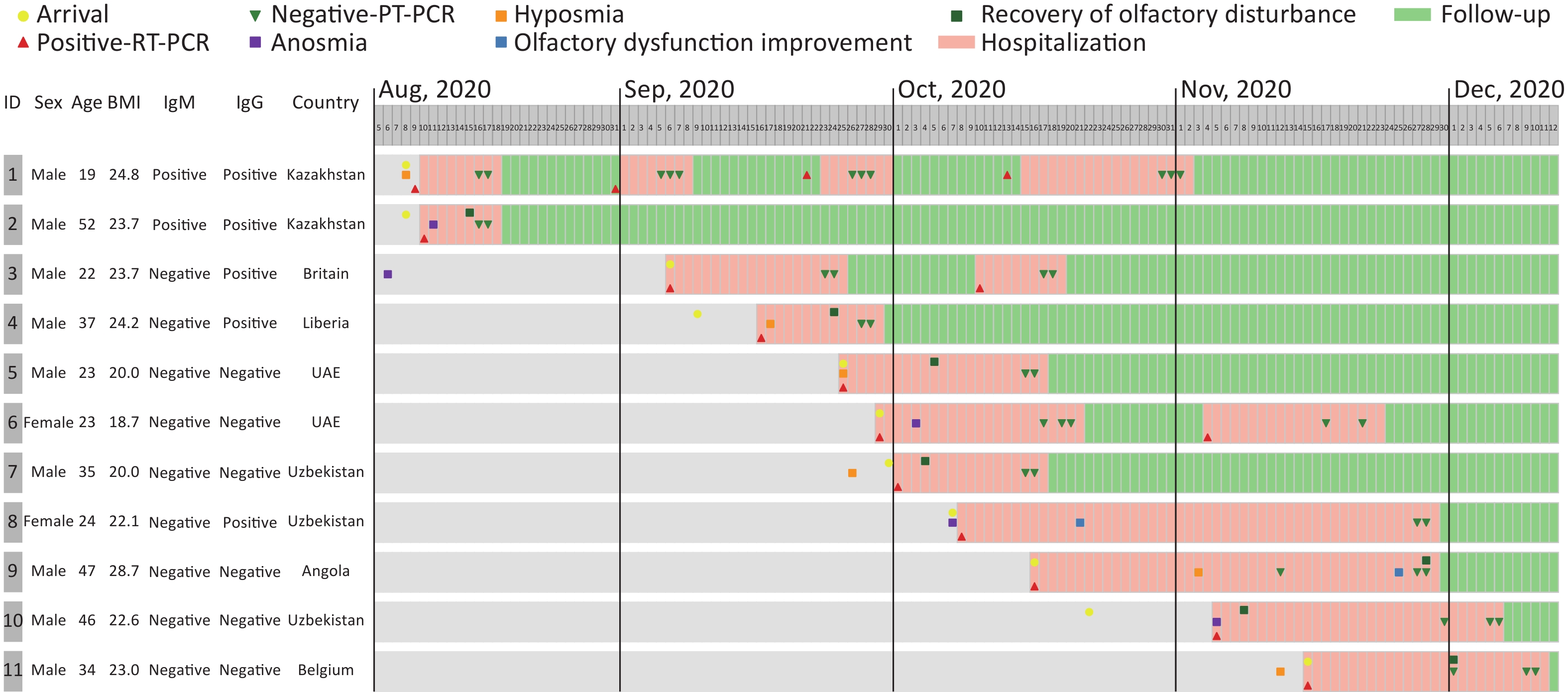
Figure 1. The clinical course of olfactory dysfunction in 11 imported COVID-19 cases. RT-PCR, reverse transcription polymerase chain reaction. Of note: Case 1 was hospitalized four times. Case 3 presented with anosmia before arrival in Xi’an (August 10, 2020), tested positive with RT-PCR, and was hospitalized. Cases 3 and 6 were hospitalized twice; both retested positive with RT-PCR after discharge and were considered mild cases at each admission. Case 7 had gustatory dysfunction in addition to olfactory dysfunction.
Of these patients, 54.5% (6/11) had hyposmia and 45.5% (5/11) had anosmia. Some 63.6% (7/11) (including the one patient reporting anosmia prior to entry) reported the onset of OD (four hyposmia and three anosmia) before or on the day of hospital admission; OD was reported as the initial symptom in those cases. Of those who reported OD as the initial symptom, 42.9% (3/7) presented OD as the only symptom. The other main symptoms included cough (5/11) and sore throat (4/11). However, none of the patients had rhinorrhea, generalized weakness, or myalgia. The patients’ symptoms and duration are shown in Table 1 and Figure 2.
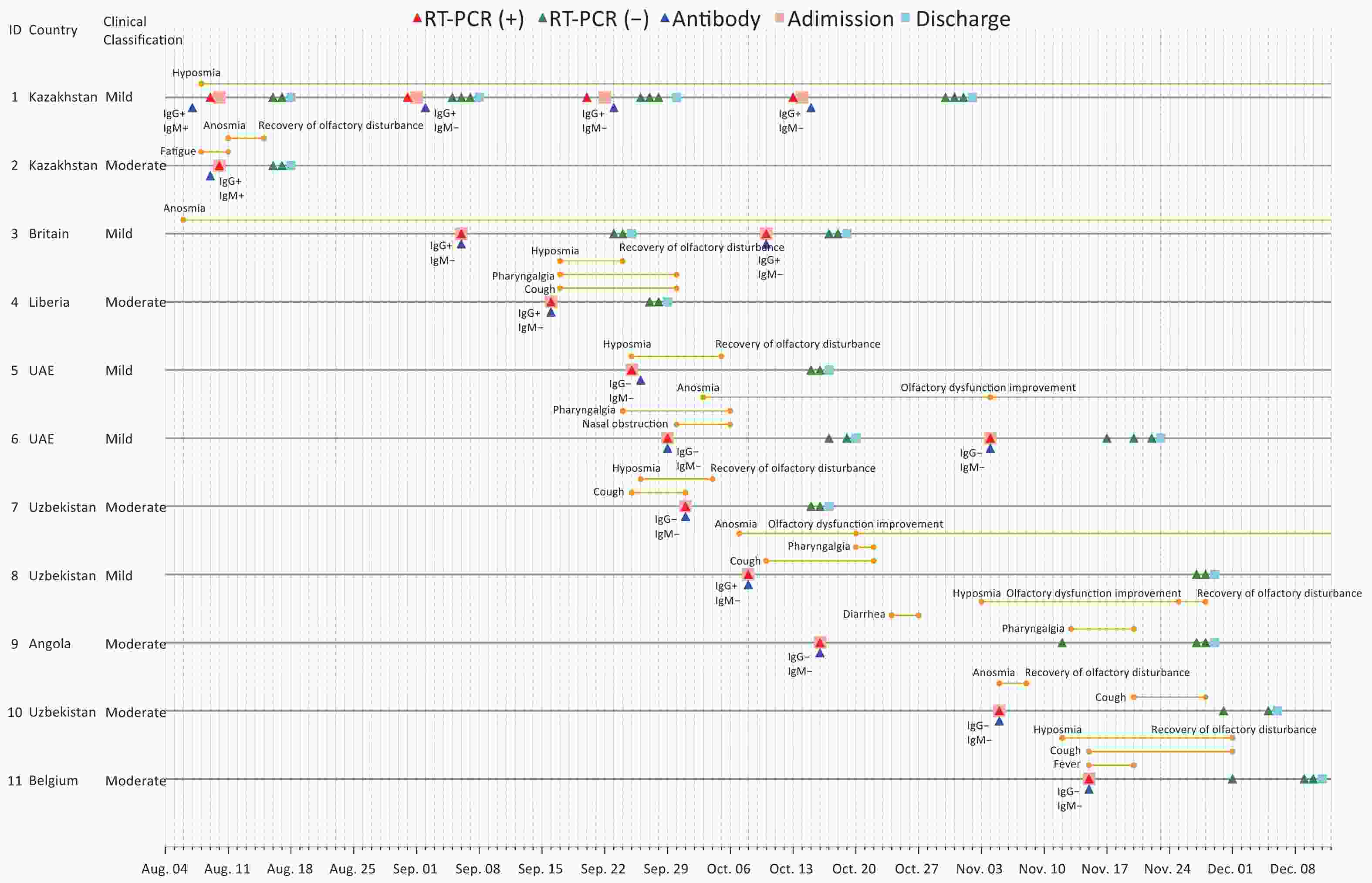
Figure 2. Chronology of symptom onset and duration, RT-PCR, and serology testing of 11 imported COVID-19 cases with olfactory dysfunction. IgM, immunoglobulin M; RT-PCR, reverse transcription polymerase chain reaction; UAE, United Arab Emirates.
Table 2 shows the laboratory and radiological findings on admission. All patients had normal peripheral white blood cell counts and procalcitonin. The lymphocyte count was low in one patient, and more than one-third (36.4%, 4/11) had elevated erythrocyte sedimentation rates. Elevated levels of C-reactive protein, liver enzymes, and creatine kinase were present in two patients, elevated lactate dehydrogenase was found in one patient, and D-dimer was found in one patient.
Table 2. Laboratory and radiological findings of 11 imported COVID-19 cases with olfactory dysfunction, China
Variables Case 1 Case 2 Case 3 Case 4 Case 5 Case 6 Case 7 Case 8 Case 9 Case 10 Case 11 Laboratory tests; (normal range) WBC count, ×109/L; (3.97–9.15) 7.02 6.38 7.99 7.55 4.07 7.75 5.69 5.85 5.59 4.25 4.18 Neutrophil count, ×109/L; (2.0–7.0) 3.65 3.73 4.35 4.58 2.66 4.38 3.82 2.57 3.28 2.84 2.94 Lymphocyte count, ×109/L; (0.8–4.0) 2.85 2.04 2.85 2.22 0.68 2.85 1.44 2.69 1.71 0.94 0.73(↓) Platelet count, ×109/ L; (85–303) 245 254 204 188 173 309(↑) 168 229.4 298 215 174 Hemoglobin, g/L; (131.0–172.0) 150 149 148 159.4 148 122 151 117 138 168 152.4 Prothrombin time, s; (11.0–15.0) 11.86 12.39 13.13 11.88 12.91 14.41 11.34 9.64(↓) 11.21 12.15 13.57 Activated partial thromboplastin
time, s; (24.0–38.0)34.66 39.37(↑) 35.03 36.14 35.38 33.35 33.11 31.86 33.78 29.35 32.38 D-dimer, μg/mL; (0.0–0.4) 0.21 0.16 0.08 0.39 0.21 0.26 0.35 0.4 0.11 0.44(↑) 0.35 Fibrinogen, g/dL; (2.0–4.0) 2.81 2.72 2.08 4.26(↑) 2.77 2.46 3.34 1.61(↓) 2.54 3.46 2.83 Albumin, g/L; (38.0–54.0) 46.5 45.38 44.99 40.39 46.02 47.44 41.98 37.62(↓) 42.72 46.8 45.3 Bilirubin, μmol/L; (5.1–19.0) 11.59 7.79 14.33 8.74 8.26 9.13 8.75 15.35 17.44 12.94 7.84 Alkaline phosphatase, U/L; (42–128) 95.73 81.34 83.87 50.31 70.71 69.35 78.39 37.42 80.94 103.5 65.4 ALT, U/L; (0.0–41.0) 19.87 15.5 17.35 26.3 9.73 14.42 132.15(↑) 6.17 102.83(↑) 25.1 10.9 AST, U/L; (0.0–37.0) 18.22 20.18 19.82 23.07 14.09 13.79 69.11(↑) 11.51 48.13(↑) 36.8 14.4 Urea, mmol/L; (1.7–8.3) 4.64 6.09 4.95 3.66 4.37 2.53 4.76 2.62 4.95 5.61 3.81 Creatinine, μmol/L; (70–115) 79.44 108.36 83.57 111.13 79.58 47.4 82.66 54.5 73.98 101.2 100.3 Sodium, mmol/L; (137–147) 142.85 141.74 141.05 135.35(↓) 141.74 141.01 139.36 143.16 141.22 143.6 139.5 Potassium, mmol/L; (3.5–5.3) 4.54 3.82 3.77 3.81 3.91 3.8 4.02 4.23 3.85 3.69 4.23 Creatine kinase, U/L; (24–190) 110.3 155 262.53(↑) 144.77 138.13 58.98 51.6 74.35 339.18(↑) 67.6 127 LDH, U/L; (115–220) 145.66 195.84 153.28 202.75 143.77 155.58 240.54(↑) 145.99 190.02 178.2 190.7 CRP, mg/L; (0.0–6.0) 1.28 2.11 0.77 11.77(↑) 1.01 0.33 3.09 0.2 1.5 0.1 9.4(↑) ESR, mm/h; (0.0–15.0) 5.0 8.0 4.0 21.0(↑) 8.0 7.0 40.0(↑) 20.0(↑) 7.0 41.0(↑) 6.0 Procalcitonin, ng/L; (0.0–0.5) < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 Blood glucose, mmol/L; (3.36–6.11) 4.56 5.15 5.31 4.63 5.33 4.17 4.61 3.7 5.21 6.45(↑) 7.15(↑) Chest CT findings No abnormal lesions Yes No Yes No Yes Yes No Yes No No No Bilateral pulmonary lesions No No No Yes No No No No No No No Unilateral pulmonary lesions No Yes No No No No Yes No Yes Yes Yes Note. ALT, alanine aminotransferase; AST, aspartate aminotransferase; CRP, C-reactive protein; CT, computerized tomography; ESR, erythrocyte sedimentation rate; LDH, lactate dehydrogenase; WBC, white blood cell; ↑ above normal range; ↓ below normal range. Available relevant laboratory data, CT findings, and treatment at admission are presented. -
All the patients received a combined treatment of traditional Chinese medicine (primarily lung cleansing and detoxifying decoction) and Western medicine. In terms of Western medicine, 100% of the patients received an antiviral treatment (primarily Abidol and interferon-α), 72.7% (8/11) received intravenous immunoglobin treatment (thymalfasin), 63.6% (7/11) received hepatoprotective therapy (compound glycyrrhizin or glutathione), and 27.3% (3/11) received antibiotic (ceftriaxone or ceftazidime) and corticosteroid (methylprednisolone) treatment (Table 1).
All the patients recovered and were discharged; none developed aggravation during hospitalization. 72.7% (8/11) had full or partial recovery at discharge, and the median duration was 9 (IQR 4.75 to 17.75) days; most improvements occurred in the first 2 weeks [in 7/9 patients (77.8%)] after onset. See the clinical course of the 11 patients in Figure 1.
-
Of the 11 cases, 72.7% (8/11) had recovered completely or recovered partially at the 1-month follow-up; 45.5% (5/11) of patients reported at least one sequela; 3 cases had more than two sequelae, such as anxiety, fatigue, difficulty sleeping, and throat discomfort; and 3 cases had been recurrent.
At the 6-month follow-up, 54.5% (6/11) had recovered completely and 27.3% (3/11) had recovered partially; however, one recovered patient with OD developed OD again, with long-term fatigue. Of the aforementioned sequelae at the 1-month follow-up, one patient had hair loss. There were no recurrent cases.
In terms of OD recovery at the 12-month follow-up, all the patients had a favorable outcome, including 81.8% (9/11) who recovered completely and 18.2% (2/11) who recovered partially. 45.5% (5/11) of the patients reported at least one sequela, and there were no recurrent cases (Figure 1 and Table 1).
-
Our data demonstrated that 54.5% (6/11) of the patients had hyposmia and 45.5% (5/11) had anosmia. All the patients with OD had a favorable outcome for OD recovery, including 81.8% with full recovery and 18.2% with partial recovery. 45.5% (5/11) of the patients reported at least one sequela, and there were no recurrent cases at the 12-month follow-up.
The proportion of OD among patients with COVID-19 varies widely across studies. Examination methods and the attention paid to these symptoms by both patients and clinicians vary as well. Some studies have suggested that the differences between Asian and White patients can be explained by polymorphisms in angiotensin converting enzyme-2 expression [27-28]. Our results suggest that OD is more prevalent in patients with mild to moderate COVID-19, which is similar to the findings of other studies [15,29].
We found that 63.6% (7/11) of the patients reported OD as the initial symptom and 42.9% (3/7) of these presented OD as the only symptom. Other studies showed that OD can precede the onset of respiratory symptoms, especially in mild to moderate cases [14,30-31], and the sudden onset of OD, whether hyposmia or anosmia, should be recognized as an important symptom of SARS-CoV-2 infection [15,31]. Given that all people entering China must quarantine for 14 days, those presenting with OD should be immediately considered suspects for SARS-CoV-2 infection to avoid delayed diagnosis or misdiagnosis and to prevent transmission.
A review of the literature reveals the short-term nature of OD related to COVID-19: most cases recovered or improved within a month [32-34], which was similar to our findings. Long-term follow-up studies are still limited. One study reported that 32.6% (29/89) of cases still presented OD at the 2-month follow-up [29]. Another study found that 24.0% (30/125) of patients reported persistent OD at the 6-month follow-up; of these, 70.0% (21/30) reported partial recovery and 23.3% (7/30) had no recovery at all [35]. Oscolo-Rizzo et al. reported that 69.5% had complete recovery after 12 months, 21.9% had partial recovery, and 8.6% had no improvement [36]. In the present study, we observed that all the patients had a favorable outcome, including 81.8% (9/11) who recovered completely and 18.2% who recovered partially. We also observed that most improvements occurred in the first 2 weeks after onset. These results were in line with previous studies from Egypt and the UK [37-38].
Although the mechanism of COVID-19 with OD is unclear, symptom recovery could be related to viral clearance. Therefore, we recommend regular nucleic acid testing for inpatients, especially when patients report regaining their sense of smell. Additionally, 75% (3/4) of the incompletely recovered patients had anosmia, which suggests that severe OD might result in a long-term recovery process or persistent loss [39]. In our study, a recovered patient with OD at discharge developed OD again at the 6-month follow-up; possible reasons should be explored in future studies.
Previous studies have explored the associations between patient characteristics, including age, sex, and poor OD recovery. A recent study found that the presence of persistent OD was significant only between age (≥ 50 years) and the persistence of the OD[40], and another by Abdelalim et al. revealed that there was a statistically significant positive correlation between age and only the duration of anosmia/hyposmia, not the degree of olfactory loss [41]. Brandao Neto et al. reported that being female was associated with slower olfactory recovery [42], and Amer MA et al. observed that > 70% of those who completely recovered were women [43]. Other studies had reported no association between recovery and sex [44-45]. In our study, given that only 11 patients with OD enrolled and the median age was 34 (19–52) years, we did not further analyze the association between age and OD recovery. Notably, only two patients were women; they had not fully recovered at the 1-month follow-up but had fully recovered at the 12-month follow-up.
Of note, in our study, three patients did not recover and retested positive (using RT-PCR) after discharge: one was hospitalized four times, whereas the other two were hospitalized twice; these three had been mild patients. Given that discharged patients are put under strict isolation and local cases are rare, their positive results are presumed to be persistent viral shedding rather than reinfection. Notably, there were no recurrent cases at the 6- and 12-month follow-ups.
Of further note, one of the persistent OD cases in our study appeared for treatment late, suggesting that timely treatment might influence recovery. A separate case-control study found that corticosteroids can reduce the prevalence of long-lasting OD [46]; however, studies on the efficacy of available treatments for patients with COVID-19-related OD are limited [47].
-
One limitation of our study is the accuracy of self-reported symptoms, given it was not feasible for all patients in emergency circumstances to use validated olfactory evaluation methods. Another limitation is that a subgroup analysis was not performed because of the small sample size.
-
We found that the olfactory recovery was within 2 weeks after onset among imported COVID-19 cases, and these patients had a favorable outcome at the 12-month follow-up after discharge. A better understanding of the pathogenesis and appropriate treatment of OD is urgently needed to guide clinicians in the care of these patients.
-
We would like to thank all the participants who took part in this study.
-
GUO Ya Ling, WANG Xiao Hong, WANG Ni, YANG Ming Bo, YANG Pu Ye, and CHEN Ren Bo contributed to conceive and design the research. ZHANG Yan, XU You, LIU Si Hong, LU Heng Yi, FU Qing Qing, and FAN Yi Pin collected and input data. HUANG Fei, SHI Nan Nan, and MA Yan analyzed the data. WANG Ni, YANG Ming Bo, YANG Pu Ye, and CHEN Ren Bo drafted the manuscript. GUO Ya Ling, WANG Xiao Hong, SHI Nan Nan, and MA Yan contributed to the writing of the manuscript. All authors have read and approved the manuscript.
-
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
doi: 10.3967/bes2022.056
A Case Series of Olfactory Dysfunction in Imported COVID-19 Patients: A 12-Month Follow-Up Study
-
Abstract:&These authors contributed equally to this work.
Objective The scientific community knows little about the long-term influence of coronavirus disease 2019 (COVID-19) on olfactory dysfunction (OD). With the COVID-19 pandemic ongoing worldwide, the risk of imported cases remains high. In China, it is necessary to understand OD in imported cases. Methods A prospective follow-up design was adopted. A total of 11 self-reported patients with COVID-19 and OD from Xi’an No. 8 Hospital were followed between August 19, 2021, and December 12, 2021. Demographics, clinical characteristics, laboratory and radiological findings, and treatment outcomes were analyzed at admission. We surveyed the patients via telephone for recurrence and sequelae at the 1-, 6-, and 12-month follow-up. Results Eleven patients with OD were enrolled; of these, 54.5% (6/11) had hyposmia and 45.5% (5/11) had anosmia. 63.6% (7/11) reported OD before or on the day of admission as their initial symptom; of these, 42.9% (3/7) described OD as the only symptom. All patients in the study received combined treatment with traditional Chinese medicine and Western medicine, and 72.7% (8/11) had partially or fully recovered at discharge. In terms of OD recovery at the 12-month follow-up, 45.5% (5/11) reported at least one sequela, 81.8% (9/11) had recovered completely, 18.2% (2/11) had recovered partially, and there were no recurrent cases. Conclusions Our data revealed that OD frequently presented as the initial or even the only symptom among imported cases. Most OD improvements occurred in the first 2 weeks after onset, and patients with COVID-19 and OD had favorable treatment outcomes during long-term follow-up. A better understanding of the pathogenesis and appropriate treatment of OD is needed to guide clinicians in the care of these patients.
注释: -
Figure 1. The clinical course of olfactory dysfunction in 11 imported COVID-19 cases. RT-PCR, reverse transcription polymerase chain reaction. Of note: Case 1 was hospitalized four times. Case 3 presented with anosmia before arrival in Xi’an (August 10, 2020), tested positive with RT-PCR, and was hospitalized. Cases 3 and 6 were hospitalized twice; both retested positive with RT-PCR after discharge and were considered mild cases at each admission. Case 7 had gustatory dysfunction in addition to olfactory dysfunction.
Figure 2. Chronology of symptom onset and duration, RT-PCR, and serology testing of 11 imported COVID-19 cases with olfactory dysfunction. IgM, immunoglobulin M; RT-PCR, reverse transcription polymerase chain reaction; UAE, United Arab Emirates.
Table 1. Demographics, clinical characteristics, treatment outcomes, and follow up of 11 imported COVID-19 cases with olfactory dysfunction
Characteristics Case 1 Case 2 Case 3 Case 4 Case 5 Case 6 Case 7 Case 8 Case 9 Case 10 Case 11 Age (years) 19 52 22 37 23 23 35 24 47 46 34 Gender Male Male Male Male Male Female Male Female Male Male Male Occupation Student Salary employee Student Semi-skilled employee Salary employee Unemployed Salary employee Student Salary employee Salary employee Semi-skilled employee Body mass index (kg/m2) 24.8 23.7 23.7 24.2 20.0 18.8 20.0 22.1 28.7 22.6 23.0 Comorbidity Hypertension Hypertension No No No No No No No Hepatitis B No Complication No No No Liver injury No No No No Liver injury No No Imported country Kazakhstan Kazakhstan Britain Liberia United Arab Emirates United Arab Emirates Uzbekistan Uzbekistan Angola Uzbekistan Belgium Clinical classification Mild Moderate Mild Moderate Mild Mild Moderate Mild Moderate Moderate Moderate Symptoms and signs Hyposmia Yes No No Yes Yes No Yes No Yes No Yes Anosmia No Yes Yes No No Yes No Yes No Yes No Hypogeusia No No No No No No Yes No No No No Fever No No No No No No No No No No Yes Cough No No No Yes No No Yes Yes No Yes Yes Fatigue No Yes No No No No No No No No No Rhinorrhea No No No No No No No No No No No Nasal congestion No No No No No Yes No No No No No Sore throat No No No Yes No Yes No Yes Yes No No Myalgia No No No No No No No No No No No Diarrhea No No No No No No No No Yes No No Treatment Antiviral Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Antibiotic No No No Yes No No No No Yes No Yes Traditional Chinese medicine Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Corticosteroids No No No Yes No No No No Yes No Yes Intravenous
immunoglobinNo Yes Yes Yes Yes No Yes No Yes Yes Yes Hepatoprotective
therapyNo No No Yes No Yes Yes Yes Yes Yes Yes Treatment outcome Cured Cured Cured Cured Cured Cured Cured Cured Cured Cured Cured Follow up 1-month OD No recovery* Recovery No recovery* Recovery Recovery No recovery* Recovery Partial recovery# Recovery Recovery Recovery Other sequelae Anxiety, fatigue, difficulty sleeping No No No No Throat discomfort, Fatigue, No No Fatigue Difficulty sleeping, Fatigue Throat discomfort Re-positive Yes No Yes No No Yes No No No No No 6-month OD Partial recovery# No Partial recovery# Recovery Recovery Partial recovery# Recovery Recovery OD Recovery Recovery Other sequelae Hair loss, anxiety, fatigue and difficulty sleeping No No No No Throat discomfort No No Fatigue Difficulty sleeping Throat discomfort, hair loss Re-positive No No No No No No No No No No No 12-month OD Partial recovery# Recovery Recovery Recovery Recovery Recovery Recovery Recovery Partial recovery# Recovery Recovery Other sequelae Hair loss, anxiety, fatigue, difficulty sleeping No No No No Throat discomfort No No Fatigue Difficulty sleeping Hair loss
, anxietyRe-positive No No No No No No No No No No No Note. *No recovery: patients with OD were considered that who do not report any improvement for smell for odors. #Partial recovery: patients with OD were considered that who subjectively start to smell some odors. OD, olfactory dysfunction.  下载: 导出CSV
下载: 导出CSV
Table 2. Laboratory and radiological findings of 11 imported COVID-19 cases with olfactory dysfunction, China
Variables Case 1 Case 2 Case 3 Case 4 Case 5 Case 6 Case 7 Case 8 Case 9 Case 10 Case 11 Laboratory tests; (normal range) WBC count, ×109/L; (3.97–9.15) 7.02 6.38 7.99 7.55 4.07 7.75 5.69 5.85 5.59 4.25 4.18 Neutrophil count, ×109/L; (2.0–7.0) 3.65 3.73 4.35 4.58 2.66 4.38 3.82 2.57 3.28 2.84 2.94 Lymphocyte count, ×109/L; (0.8–4.0) 2.85 2.04 2.85 2.22 0.68 2.85 1.44 2.69 1.71 0.94 0.73(↓) Platelet count, ×109/ L; (85–303) 245 254 204 188 173 309(↑) 168 229.4 298 215 174 Hemoglobin, g/L; (131.0–172.0) 150 149 148 159.4 148 122 151 117 138 168 152.4 Prothrombin time, s; (11.0–15.0) 11.86 12.39 13.13 11.88 12.91 14.41 11.34 9.64(↓) 11.21 12.15 13.57 Activated partial thromboplastin
time, s; (24.0–38.0)34.66 39.37(↑) 35.03 36.14 35.38 33.35 33.11 31.86 33.78 29.35 32.38 D-dimer, μg/mL; (0.0–0.4) 0.21 0.16 0.08 0.39 0.21 0.26 0.35 0.4 0.11 0.44(↑) 0.35 Fibrinogen, g/dL; (2.0–4.0) 2.81 2.72 2.08 4.26(↑) 2.77 2.46 3.34 1.61(↓) 2.54 3.46 2.83 Albumin, g/L; (38.0–54.0) 46.5 45.38 44.99 40.39 46.02 47.44 41.98 37.62(↓) 42.72 46.8 45.3 Bilirubin, μmol/L; (5.1–19.0) 11.59 7.79 14.33 8.74 8.26 9.13 8.75 15.35 17.44 12.94 7.84 Alkaline phosphatase, U/L; (42–128) 95.73 81.34 83.87 50.31 70.71 69.35 78.39 37.42 80.94 103.5 65.4 ALT, U/L; (0.0–41.0) 19.87 15.5 17.35 26.3 9.73 14.42 132.15(↑) 6.17 102.83(↑) 25.1 10.9 AST, U/L; (0.0–37.0) 18.22 20.18 19.82 23.07 14.09 13.79 69.11(↑) 11.51 48.13(↑) 36.8 14.4 Urea, mmol/L; (1.7–8.3) 4.64 6.09 4.95 3.66 4.37 2.53 4.76 2.62 4.95 5.61 3.81 Creatinine, μmol/L; (70–115) 79.44 108.36 83.57 111.13 79.58 47.4 82.66 54.5 73.98 101.2 100.3 Sodium, mmol/L; (137–147) 142.85 141.74 141.05 135.35(↓) 141.74 141.01 139.36 143.16 141.22 143.6 139.5 Potassium, mmol/L; (3.5–5.3) 4.54 3.82 3.77 3.81 3.91 3.8 4.02 4.23 3.85 3.69 4.23 Creatine kinase, U/L; (24–190) 110.3 155 262.53(↑) 144.77 138.13 58.98 51.6 74.35 339.18(↑) 67.6 127 LDH, U/L; (115–220) 145.66 195.84 153.28 202.75 143.77 155.58 240.54(↑) 145.99 190.02 178.2 190.7 CRP, mg/L; (0.0–6.0) 1.28 2.11 0.77 11.77(↑) 1.01 0.33 3.09 0.2 1.5 0.1 9.4(↑) ESR, mm/h; (0.0–15.0) 5.0 8.0 4.0 21.0(↑) 8.0 7.0 40.0(↑) 20.0(↑) 7.0 41.0(↑) 6.0 Procalcitonin, ng/L; (0.0–0.5) < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 < 0.05 Blood glucose, mmol/L; (3.36–6.11) 4.56 5.15 5.31 4.63 5.33 4.17 4.61 3.7 5.21 6.45(↑) 7.15(↑) Chest CT findings No abnormal lesions Yes No Yes No Yes Yes No Yes No No No Bilateral pulmonary lesions No No No Yes No No No No No No No Unilateral pulmonary lesions No Yes No No No No Yes No Yes Yes Yes Note. ALT, alanine aminotransferase; AST, aspartate aminotransferase; CRP, C-reactive protein; CT, computerized tomography; ESR, erythrocyte sedimentation rate; LDH, lactate dehydrogenase; WBC, white blood cell; ↑ above normal range; ↓ below normal range. Available relevant laboratory data, CT findings, and treatment at admission are presented.
下载: 导出CSV
-
[1] Zhao Y, Sun DL, Bouchard HC, et al. Coronavirus disease 2019 versus influenza a in children: an observational control study in China. Biomed Environ Sci, 2020; 33, 614−9. [2] Ma Y, Zhu DS, Chen RB, et al. Association of overlapped and un-overlapped comorbidities with COVID-19 severity and treatment outcomes: a retrospective cohort study from nine provinces in China. Biomed Environ Sci, 2020; 33, 893−905. [3] Ji YL, Wu Y, Qiu Z, et al. The pathogenesis and treatment of COVID-19: a system review. Biomed Environ Sci, 2021; 34, 50−60. [4] Liu SH, Ma Y, Shi NN, et al. Qingfei Paidu decoction for COVID-19: a bibliometric analysis. Biomed Environ Sci, 2021; 34, 755−60. [5] World Health Organization. Weekly operational update on COVID-19. World Health Organization. https://www.who.int/redirect-pages/page/novel-coronavirus-(covid-19)-situation-dashboard. [2021-11-19]. [6] Li ZJ, Chen QL, Feng LZ, et al. Active case finding with case management: the key to tackling the COVID-19 pandemic. Lancet, 2020; 396, 63−70. doi: 10.1016/S0140-6736(20)31278-2 [7] Huang CL, Wang YM, Li XW, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet, 2020; 395, 497−506. doi: 10.1016/S0140-6736(20)30183-5 [8] Eliezer M, Hautefort C, Hamel AL, et al. Sudden and complete olfactory loss of function as a possible symptom of COVID-19. JAMA Otolaryngol Head Neck Surg, 2020; 146, 674−5. doi: 10.1001/jamaoto.2020.0832 [9] Menni C, Valdes AM, Freidin MB, et al. Real-time tracking of self-reported symptoms to predict potential COVID-19. Nat Med, 2020; 26, 1037−40. doi: 10.1038/s41591-020-0916-2 [10] Centers for Disease Control and Prevention (CDC). Symptoms of coronavirus. CDC.https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html. [2021-05-18]. [11] World Health Organization (WHO). Coronavirus disease (COVID-19). WHO. https://www.who.int/health-topics/coronavirus#tab=tab_3. [2021-05-18]. [12] Yan CH, Faraji F, Prajapati DP, et al. Self-reported olfactory loss associates with outpatient clinical course in COVID-19. Int Forum Allergy Rhinol, 2020; 10, 821−31. doi: 10.1002/alr.22592 [13] Spinato G, Fabbris C, Polesel J, et al. Alterations in smell or taste in mildly symptomatic outpatients with SARS-CoV-2 Infection. JAMA, 2020; 323, 2089−90. doi: 10.1001/jama.2020.6771 [14] Lechien JR, Chiesa-Estomba CM, Hans S, et al. Loss of smell and taste in 2013 European patients with mild to moderate COVID-19. Ann Intern Med, 2020; 173, 672−5. doi: 10.7326/M20-2428 [15] Lechien JR, Chiesa-Estomba CM, De Siati DR, et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): a multicenter European study. Eur Arch Otorhinolaryngol, 2020; 277, 2251−61. doi: 10.1007/s00405-020-05965-1 [16] Lee Y, Min P, Lee S, et al. Prevalence and duration of acute loss of smell or taste in COVID-19 patients. J Korean Med Sci, 2020; 35, e174. doi: 10.3346/jkms.2020.35.e174 [17] Mao L, Jin HJ, Wang MD, et al. Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol, 2020; 77, 683−90. doi: 10.1001/jamaneurol.2020.1127 [18] Xydakis MS, Dehgani-Mobaraki P, Holbrook EH, et al. Smell and taste dysfunction in patients with COVID-19. Lancet Infect Dis, 2020; 20, 1015−6. doi: 10.1016/S1473-3099(20)30293-0 [19] Paderno A, Mattavelli D, Rampinelli V, et al. Olfactory and gustatory outcomes in COVID-19: a prospective evaluation in nonhospitalized subjects. Otolaryngol Head Neck Surg, 2020; 163, 1144−9. doi: 10.1177/0194599820939538 [20] Niklassen AS, Draf J, Huart C, et al. COVID-19: recovery from chemosensory dysfunction. a multicentre study on smell and taste. Laryngoscope, 2021; 131, 1095−100. [21] Marshall M. COVID’s toll on smell and taste: what scientists do and don’t know. Nature, 2021; 589, 342−3. doi: 10.1038/d41586-021-00055-6 [22] Wan YM, Deng X, Tan EK. Olfactory dysfunction and COVID-19. Lancet Psychiat, 2020; 7, 663. [23] China National Health Commission. Epidemic situation of China (up to January 17, 2021). http://www.nhc.gov.cn/xcs/yqfkdt/202101/8cb5929b31064955ba742815baf48f51.shtml. [2021-01-17]. [24] Shaanxi Provincial Health Commission. Health key news. http://sxwjw.shaanxi.gov.cn/sy/wjyw/index_8.html. [2021-01-17]. (In Chinese) [25] China National Health Commission. Diagnosis and treatment guidelines for 2019 novel coronavirus pneumonia (Trial version 8). http://www.nhc.gov.cn/cms-search/downFiles/a449a3e2e2c94d9a856d5faea2ff0f94.pdf. (In Chinese) [26] Coorperative Meta-Analysis Group of China Obesity Task Force. Predictive values of body mass index and waist circumference to risk factors of related diseases in Chinese adult population. Chin J Epidemiol, 2002; 23, 5−10. (In Chinese [27] Lechien JR, Hsieh J, Barillari MR, et al. Patient-reported outcome questionnaires for the evaluation of olfactory and gustatory dysfunctions in COVID-19. Eur Arch Otorhinolaryngol, 2020; 277, 2393−4. doi: 10.1007/s00405-020-06083-8 [28] Lv H, Zhang W, Zhu ZY, et al. Prevalence and recovery time of olfactory and gustatory dysfunction in hospitalized patients with COVID-19 in Wuhan, China. Int J Infect Dis, 2020; 100, 507−12. doi: 10.1016/j.ijid.2020.09.039 [29] Carvalho-Schneider C, Laurent E, Lemaignen A, et al. Follow-up of adults with noncritical COVID-19 two months after symptom onset. Clin Microbiol Infect, 2021; 27, 258−63. doi: 10.1016/j.cmi.2020.09.052 [30] World Health Organization (WHO). Clinical Management of COVID-19. Geneva: WHO, 2020. [31] Haehner A, Draf J, Dräger S, et al. Predictive value of sudden olfactory loss in the diagnosis of COVID-19. ORL J Otorhinolaryngol Relat Spec, 2020; 82, 175−80. doi: 10.1159/000509143 [32] Whitcroft KL, Hummel T. Olfactory dysfunction in COVID-19: diagnosis and management. JAMA, 2020; 323, 2512−4. doi: 10.1001/jama.2020.8391 [33] Sahoo PR, Sahu M, Surapaneni PS, et al. Evolution of olfactory and gustatory dysfunctions in COVID-19 patients in India. Eur Arch Otorhinolaryngol, 2021; 278, 2875−81. doi: 10.1007/s00405-020-06563-x [34] Boscolo-Rizzo P, Borsetto D, Fabbris C, et al. Evolution of altered sense of smell or taste in patients with mildly symptomatic COVID-19. JAMA Otolaryngol Head Neck Surg, 2020; 146, 729−32. doi: 10.1001/jamaoto.2020.1379 [35] Nguyen NN, Hoang VT, Lagier JC, et al. Long-term persistence of olfactory and gustatory disorders in COVID-19 patients. Clin Microbiol Infect, 2021; 27, 931−2. doi: 10.1016/j.cmi.2020.12.021 [36] Oscolo-Rizzo P, Guida F, Polesel J, et al. Self-reported smell and taste recovery in coronavirus disease 2019 patients: a one-year prospective study. Eur Arch Otorhinolaryngol, 2021; 279, 515−20. [37] Teaima AA, Salem OM, El Monem Teama MA, et al. Patterns and clinical outcomes of olfactory and gustatory disorders in six months: prospective study of 1031 COVID-19 patients. Am J Otolaryngol, 2022; 43, 103259. doi: 10.1016/j.amjoto.2021.103259 [38] Hopkins C, Surda P, Whitehead E, et al. Early recovery following new onset anosmia during the COVID-19 pandemic - an observational cohort study. J Otolaryngol Head Neck Surg, 2020; 49, 26. doi: 10.1186/s40463-020-00423-8 [39] Lechien JR, Journe F, Hans S, et al. Severity of anosmia as an early symptom of COVID-19 infection may predict lasting loss of smell. Front Med, 2020; 7, 582802. doi: 10.3389/fmed.2020.582802 [40] Petrocelli M, Cutrupi S, Salzano G, et al. Six-month smell and taste recovery rates in coronavirus disease 2019 patients: a prospective psychophysical study. J Laryngol Otol, 2021; 135, 436−41. doi: 10.1017/S002221512100116X [41] Abdelalim AA, Mohamady AA, Elsayed RA, et al. Corticosteroid nasal spray for recovery of smell sensation in COVID-19 patients: a randomized controlled trial. Am J Otolaryngol, 2021; 42, 102884. doi: 10.1016/j.amjoto.2020.102884 [42] Brandão Neto D, Fornazieri MA, Dib C, et al. Chemosensory dysfunction in COVID-19: prevalences, recovery rates, and clinical associations on a large Brazilian sample. Otolaryngol Head Neck Surg, 2021; 164, 512−8. doi: 10.1177/0194599820954825 [43] Amer MA, Elsherif HS, Abdel-Hamid AS, et al. Early recovery patterns of olfactory disorders in COVID-19 patients; a clinical cohort study. Am J Otolaryngol, 2020; 41, 102725. doi: 10.1016/j.amjoto.2020.102725 [44] Bulğurcu S, Öztutgan T, Baz E, et al. Assessment of smell and taste disorders in COVID-19: a cross-sectional study. J Craniofac Surg, 2021; 32, e298−301. doi: 10.1097/SCS.0000000000007284 [45] Chary E, Carsuzaa F, Trijolet JP, et al. Prevalence and recovery from olfactory and gustatory dysfunctions in Covid-19 infection: a prospective multicenter study. Am J Rhinol Allergy, 2020; 34, 686−93. doi: 10.1177/1945892420930954 [46] Vaira LA, Hopkins C, Petrocelli M, et al. Efficacy of corticosteroid therapy in the treatment of long- lasting olfactory disorders in COVID-19 patients. Rhinology, 2021; 59(1), 21−5. [47] Luers JC, Rokohl AC, Loreck N, et al. Olfactory and gustatory dysfunction in coronavirus disease 2019 (COVID-19). Clin Infect Dis, 2020; 71, 2262−4. doi: 10.1093/cid/ciaa525 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 782
- HTML全文浏览量: 329
- PDF下载量: 64
- 被引次数: 0

 Quick Links
Quick Links