

 下载:
下载:

-
In 2017, the WHO reported that the number of new tuberculosis (TB) cases reached 10.0 million, with 1.6 million deaths. Among the new cases, it was estimated that 350, 000 cases were multidrug-resistant tuberculosis (MDR-TB) cases, defined by resistance to two main anti-TB drugs, isoniazid and rifampin. Treatment success remains low, at 55% globally[1]. Due to improper use of second-line anti-TB drugs, extensive drug-resistant tuberculosis (XDR-TB) cases caused by MDR-TB bacilli that are also resistant to fluoroquinolones and either amikacin, kanamycin, or capreomycin have increased significantly. Among patients with MDR-TB, 9.7% are XDR-TB cases with mortality rates of 65% -100% due to the lack of effective treatment regimens[1]. The emergence of MDR-TB, particularly in human immunodeficiency virus-infected patients, highlights the need for new compounds to treat these infections.
As Mycobacterium tuberculosis (Mtb) produces β-lactamase, an enzyme that hydrolyzes β-lactam antibiotics, such drugs are not clinically used to treat TB. However, in recent years the β-lactam antibiotic meropenem, a carbapenem derivative, has been reported to control MDR-TB successfully when used in combination with clavulanate (CL)[2]. Several mechanisms account for the effectiveness of this drug combination in vitro[3-6]. Furthermore, meropenem is active against XDR-TB and is well tolerated by patients[7, 8]. Biapenem (BP), a newer carbapenem, is also active against Mtb in vitro when combined with CL[9, 10]. Here we evaluated the in vitro activity of BP/CL against MDR-TB and Mtb (H37Rv) in macrophages. We then tested BP/CL in combination with other second-line anti-TB drugs for activity against MDR-TB both in vitro and in vivo in mice. The results suggest that BP/CL is a potent drug combination against MDR-TB.
-
Mtb H37Rv (ATCC 27294) and the clinical isolates (17 MDR-TB and 4 XDR-TB, all from the National Clinical Laboratory on Tuberculosis) were grown at 37 ℃ in 5% ambient CO2 for 14 days in Middlebrook 7H9 broth (Becton Dickinson, Sparks, MD, USA) supplemented with 0.2% (v/v) glycerol (Sigma, St. Louis, MO, USA), 10% (v/v) oleic acid-albumin-dextrose-catalase (OADC; Becton Dickinson) and 0.05% (v/v) Tween 80 (Sigma). The bacteria were washed, suspended in phosphate-buffered saline, and passed through a filter (8-µm pore size) to eliminate clumps. The filtrates were aliquoted and stored at -80 ℃ for use within 30 days.
-
Chemicals were purchased in pure form from various manufacturers: levofloxacin (Lfx) from Shuanghe Pharmaceutical Co., Ltd. (Beijing, China); clofazimine (CFZ) from Nanjing Liye Pharmaceutical Co., Ltd. (Nanjing, Jiangsu, China); aminosalicylate (PAS), protionamide (Pto) and capreomycin (CPM) from Shanghai Xinyi Pharmaceutical Co., Ltd. (Shanghai, China); rifampin (RIF), pyrazinamide (PZA) and isoniazid (INH) from Sigma; linezolid (LZD) from Pfizer (Andover, MA, USA); BP from Zhengda Tianqing Pharmaceutical Co., Ltd. (Jiangsu, China); and CL from Aladdin Industrial Corp. (Calhoun, GA, USA).
-
Initial stock solutions of Lfx, CPM, PAS, BP/CL, Pto, and CFZ were constituted in dimethyl sulfoxide (DMSO) at concentrations of 10 or 20 g/L. Dilutions were made from the stock solutions in 7H9 broth. To avoid solvent effects, the highest concentration of DMSO was 0.5%. BP and CL were dissolved just before use. The MICs of the antimicrobial agents were determined against H37Rv strain using a microplate Alamar Blue assay[11] with serial two-fold dilutions of the drugs. The MICs of the combinations of BP/CL and other second-line anti-TB agents were determined in 96-well microtiter plates using the dynamic checkerboard method[12]. Initial concentrations of Lfx, CPM, PAS, CFZ, LZD, and Pto were 1, 4, 1, 0.48, 1, and 2 µg/mL, respectively, and the final concentrations of the drugs (two-fold dilutions) ranged from 1/8× to 1× of the MIC of each drug.
The data were interpreted by calculating the fractional inhibitory concentration (FIC) as following formula: FIC = (A/MICA) + (B/MICB), where A and B represent the MICs of each drug combination, and MICA and MICB represent the MICs of each drug alone. The FIC results reflect synergy for FIC < 0.5[13, 14].
-
After the cultured macrophage cell line J774A.1 was suspended in antibiotic-free Dulbecco's Modified Eagle Medium (DMEM and 10% fetal bovine serum), the cell suspension was added to 24-well tissue culture plates at a cell density of 5 × 105 CFU/mL. The plates were incubated at 37 ℃ for 12 h in 5% CO2. The macrophages were infected with a 100-µL bacterial suspension containing 5 × 106 CFU/mL Mtb H37Rv and incubated for 4 h. The cells were washed with prewarmed serum-free DMEM to remove extracellular bacteria from the adherent cells. Next, 1 mL of DMEM with or without drugs was added, and the plates were incubated in 5% CO2 as described above for 2 days. Wells containing cells without added drugs served as negative controls. The BP concentrations were 40 and 20 µg/mL, and the concentrations of CL and INH were 2.5 and 2 µg/mL, respectively. Due to the instability of BP and CL in medium, spent medium was replaced with new medium containing freshly constituted BP/CL twice each day. Two days after infection, each macrophage monolayer was lysed with 0.2 mL of 7H9 medium containing 0.1% SDS. Next, the lysates were serially diluted and dilutions were inoculated onto OADC-enriched 7H11 agar medium for enumeration of CFU.
-
Male 6-week-old BALB/c mice (Beijing Vital River Laboratory Animal Technology Co., Ltd., Beijing, China) were infected with the H37Rv strain using a Glas-col inhalation exposure system (Glas-col Inc., Terre Haute, IN, USA) and a fresh log-phase broth culture to implant 3 log10 CFU into the lungs of each mouse. Five mice were sacrificed the following day to determine the number of CFUs implanted in the lungs. All animal procedures were approved by the Animal Care and Use Committee of the Beijing Tuberculosis and Thoracic Tumor Institute (No. 2017009).
-
After infection, the mice were randomly assigned to one of the nine treatment groups described in Table 1. The first group was a negative control group that included infected mice receiving no treatment. The last group was a positive control group of mice treated with the standard RIF-INH-PZA (RHZ) TB-treatment regimen. Mice in the remaining groups were treated with additional antibiotics. The treatment began 15 days after infection (on day 0) to attain a high initial bacterial burden within the lungs of mice. Treatment was administered 5 days per week thereafter. For consistency, 4 weeks were considered equivalent to 1 month of treatment. Drugs were administered in the doses shown in Table 2. Based on the areas under the concentration (AUC)-time curves, these doses were chosen due to equipotency with the usual doses administered to humans and were similar to doses used in previous studies[16, 17]. All regimens were administered for 2 months. BP and CL were given by subcutaneous injection twice each day, 5 days per week. The remaining drugs were administered by gavage.
Table 1. Experimental Design Used in This Study
Group Drug Alone or Combinationa No. of Mice Sacrificed at Indicated Time Pointb Total No. of Mice D -14 D0 M1 M2 A Untreated 5 5 5 5 20 B BP/CL 5 5 10 C PAS 5 5 10 D Pto 5 5 10 E BP/CL + PAS 5 5 10 F BP/CL + Pto 5 5 10 G Lfx + Pto + PAS + PZA 5 5 10 H BP/CL + Lfx + Pto + PAS + PZA 5 5 10 I RIF + INH + PZA 5 5 10 Total No. of mice 5 5 45 45 100 Note. aDrugs were administered 5 days per week at the following doses: BP (100), CL (100), PAS (750), Pto (100), Lfx (200), RFP (10), INH (25), and PZA (150). bMice were sacrificed at the following times: 1 day after infection (D -14); 15 days after infection [day 0 (D0)]; 1, 2 months after treatment (M1, M2, respectively). Table 2. Dosages of Drugs Administered to the Mice
Agents Dosage (mg/kg) Agents Dosages (mg/kg) BP 100 Lfx 200 CL 100 RFP 10 PAS 750 INH 25 Pto 100 PZA 150 -
To provide baseline values, a group of five infected but untreated mice were euthanized per day on days 1 and 15 after infection (days designated: -14 and 0 in relation to initiation of treatment). The treated mice were euthanized after 1 and 2 months of treatment to determine lung CFU counts. The numbers of CFUs within the lungs were determined on days -14 and 0 and after 1 month of treatment by plating four serial 10-fold dilutions of homogenized suspensions onto OADC-enriched 7H11 agar medium. After 2 months of treatment, the entire suspension prepared from each individual organ, predicted to contain few bacilli, was plated without dilution onto OADC-enriched 7H11 agar medium. The results for the various cultures were recorded after a 4-week incubation at 37 ℃. The bactericidal effect of each treatment was defined as a significant decrease in the mean number of CFUs compared to the corresponding infected untreated control tissue CFU values.
-
CFU counts were converted to log10 values before analysis, and each was expressed as CFU log10 ± standard error. Experimental group means were compared to means of the untreated infected group by two-way analysis of variance using Fisher's exact test. Differences were considered significant at a P-value < 0.05. The data analysis was performed using the Statistical Package for the Social Sciences software (SPSS 17.0; IBM, Armonk, NY, USA).
-
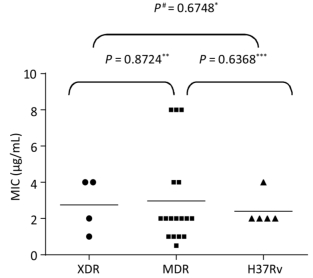
The MICs of BP/CL against H37Rv, the 17 MDR, and the four XDR isolates were determined according to a standard two-fold agar dilution method under defined conditions as described above. The MIC of BP/CL against H37Rv was 2 µg/mL and ranged between 0.5 and 8 µg/mL for the 17 MDR strains and between 1 and 4 µg/mL for the four XDR strains (Figure 1). No differences were observed between the MICs of BP/CL when compared with H37Rv, MDR-, or XDR-TB (P > 0.05).
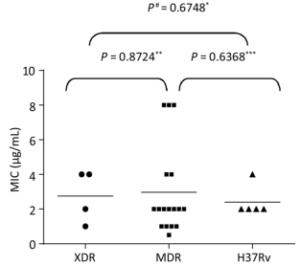
Figure 1. Minimum inhibitory concentrations (MICs) of biapenem/clavulanate (BP/CL) against extensive drug-resistant tuberculosis (XDR-TB), multidrug-resistant tuberculosis (MDR-TB), and the H37Rv strain in vitro. #Fisher's exact test. *No difference between the MICs of BP/CL against XDR-TB or H37Rv. **No difference between the MICs of BP/CL against XDR-TB or MDR-TB. ***No difference between the MICs of BP/CL against MDR-TB or H37Rv.
The dynamic checkerboard method was used to evaluate the effects of BP/CL combined with either CLF, PAS, Pto, LZD, Lfx, or CPM on MTb CFUs (Table 3). The FIC of BP/CL and pairwise combinations with either PAS, Pto, or CPM was 0.375, indicating that synergy existed between each pair of drugs tested. Combinations of BP/CL with each of the other three drugs only exhibited additive effects.
Table 3. Fractional Inhibitory Concentration (FICs) of Biapenem/Clavulanate (BP/CL) Combinations with Other Second-line Anti-tuberculosis (TB) Drugs in vitro
Agents BP/CL LZD BP/CL Pto BP/CL Lfx BP/CL PAS BP/CL CPM BP/CL CLF MICalonea 2 0.5 2 2 2 0.5 2 0.25 2 2 2 0.24 MICcombinationb 1 0.0625 0.25 0.5 1 0.0625 0.25 0.0625 0.5 0.25 1 0.06 FIC 0.625 0.375* 0.625 0.375* 0.375* 0.75 Note. aMICalone: MIC of agent alone against H37Rv; bMICcombination: MIC of agents combined against H37Rv; *FIC < 0.5 means these two drugs were synergistic. -
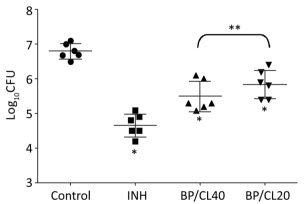
The activity of BP/CL by day 2 of treatment against H37Rv within macrophages (infected at a MOI = 1) is presented in Figure 2. BP/CL (40 and 20 µg/mL) demonstrated 1.3- and 0.9-log reductions in bacterial numbers, respectively, compared to results for untreated infected control macrophages. INH decreased CFU by 2.1-log and BP/CL40, BP/CL20, and INH were each active against H37Rv within macrophages compared to infected untreated macrophage controls (infected with H37Rv). Although a significant difference was observed between BP/CL40 and INH activities (P = 0.03), no difference was observed between the BP/CL40 and BP/CL20 treatments.
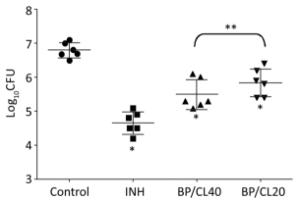
Figure 2. Efficacy of regimens against Mycobacterium tuberculosis (Mtb) H37Rv in macrophages after 2 days of treatment. Fisher's Exact Test. Biapenem/clavulanate (BP)/(CL)40: BP and CL concentrations were 40 and 25 μg/mL, respectively; BP/CL20: BP and CL concentrations were 20 and 25 μg/mL, respectively; *P < 0.05, compared with the control group; three agents decreased CFU significantly; **No difference between these two groups.
-
On the day after the aerosol infection, the lung CFU count (mean ± standard error) was 3.24 ± 0.06 log10, with a mean lung CFU count at the initiation of treatment (15 days after infection) of 4.98 ± 0.10 log10.
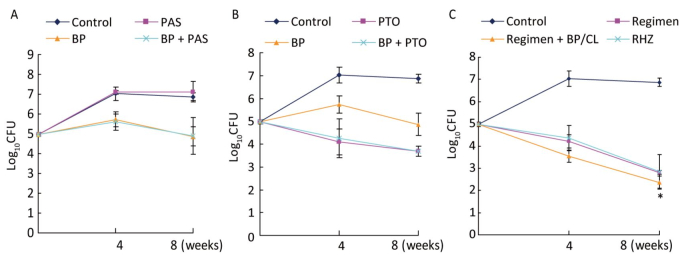
To evaluate the synergy of BP/CL with PAS and Pto in vivo, we determined the CFUs in lungs of mice after treatment with BP/CL, PAS, Pto, BP/CL + PAS; and BP/CL + Pto. After 2 months, the CFU result of the BP/CL + PAS group was no different from the results of the BP/CL, PAS and BP/CL + Pto groups. Moreover, no drug interactions were observed for any of the drug combinations administered in vivo (Figure 3A and 3B).

Figure 3. Efficacy of regimens against Mycobacterium tuberculosis (Mtb) H37Rv in mice after 1 and 2 months of treatment. Control values used in panels A, B, and C were obtained from the same control group. (A) CFU reduction by PAS, BP/CL, and PAS + BP/CL in mice; (B) CFU reduction by Pto, BP/CL, and Pto + BP/CL in mice; (C) CFU reduction of regimen (Lfx + PZA + Pto + PAS), regimen + BP/CL, RHZ in mice; *In Figure C: P = 0.0049, significant difference in CFUs between the regimen group and the regimen + BP/CL group.
At the same time, the activities of three regimens (RHZ; Lfx + PZA + Pto + PAS; and Lfx + PZA + Pto + PAS + BP/CL) against TB were determined in mice. After 2 months of treatment, the CFUs in the lungs of all groups declined significantly compared with control untreated infected lungs (Figure 3C). Lfx + PZA + Pto + PAS reduced the number of bacilli in the lungs by 4.06 log10. When BP/CL was combined with the Lfx + PZA + Pto + PAS regimen, CFUs significantly decreased further by 4.51 log10 (P = 0.0049). However, no difference was observed between the Lfx + PZA + Pto + PAS + BP/CL and RHZ groups (P = 0.2125).
-
Most drugs to treat MDR-TB exhibit low efficacy and are accompanied by side effects. For example, LZD exhibits hematologic toxicity[18], while cycloserine exhibits central nervous system toxicity[19]. Therefore, carbapenem drugs, with high efficacy and low toxicity, are attracting strong interest as potential therapies against drug-resistant Mtb. Based on our research, BP could kill Mtb in vitro with a MIC of 2-4 µg/mL, regardless of whether it was H37Rv, MDR-TB, or XDR-TB.
As Mtb is a typical intracellular parasite that can survive and reproduce in macrophages, intracellular Mtb can only be killed by drugs that enter macrophages. Therefore, we investigated the antibacterial activity of BP against Mtb within macrophages and found that BP/CL exhibited a killing effect at concentrations of 20 and 40 µg/mL. The CFU counts decreased by 0.9-log and 1.3-log after 2 days of BL/CL administration, respectively, which was significantly different compared to the infected untreated control group. However, no significant difference was found in bactericidal activity between the 20 and 40 µg/mL groups. The dosing regimen for intravenous BP is usually 300-600 mg Q12H in clinical practice and the serum Cmax value is between 14.7-15.6 µg/mL and 31.5-35.7 µg/mL[20]. According to our study, no difference was found in the bactericidal killing function between these two concentrations, therefore the 600 mg BP dosing regimen of Q12H is feasible.
The WHO has recommended a MDR-TB regimen that consists of five to six drugs. If there is a synergistic effect among the drugs, this would increase the antibacterial activity of individual drugs and reduce side effects[21]. Research has shown that meropenem combined with CL can decrease the MIC of meropenem against Mtb, ultimately improving the antibacterial activity of meropenem. Another study revealed a synergistic effect between BP and RIF[10] and our results here show synergy (FIC = 0.375) between BP/CL and the second-line anti-TB drugs PAS, CPM, and Pto. Such synergistic effects may be due to the destruction of the Mtb cell wall by BP/CL, leading to increased drug entry into the bacteria.
The in vitro antibacterial activities or synergistic effects of drugs do not always guarantee the same effects in vivo. Therefore, we investigated the interactions between BP/CL and either PAS or Pto in mice. The results showed that although there were synergistic effects in vitro between BP/CL and PAS or between BP/CL and Pto, neither pairwise combination exhibited synergy in reducing lung tissue CFU counts in vivo. This discrepancy may be related to the poor tissue-penetrating ability of PAS[15], resulting in far lower amounts entering tissues than effective tissue concentrations needed for achieving synergy with BP/CL. Nevertheless, the reason behind the lack of synergy in vivo between BP/CL and Pto remains unclear.
In addition, we investigated the therapeutic effect of Lfx + PZA + Pto + PAS, an anti-Mtb chemotherapeutic regimen commonly used clinically, to investigate its therapeutic effect against TB in mice when combined with BP/CL. The results showed that adding BP/CL significantly reduced the CFU counts in mouse lung tissue, achieving activity similar to that observed for the classical RHZ therapeutic scheme. However, neither of these therapies eliminated the bacteria in mouse lungs after 2 months of treatment.
Several factors might have affected drug efficacy in vivo. First, because the antibacterial activity of BP is time-dependent, BP must be injected subcutaneously into mice twice a day, causing greater stress and a poor mental state in the animals. Second, although BP does not require additional administration of cilastatin to inhibit renal dehydropeptidase-I, BP is pharmacokinetically reduced via hydrolysis faster in mice than in humans due to higher kidney dehydrogenation enzyme activity in mice. This appears to also be true in rabbits, as England et al. reported significantly reduced Cmax, t1/2 and AUC-time curve of meropenem in rabbits[22]. Therefore, underestimating the antibacterial activity of BP is a possible when using a murine TB model. Third, BP and CL are easily hydrolyzed, even if freshly prepared just prior to administration, resulting in reduced efficacy.
Although the experiment demonstrated that BP/CL had anti-TB activity, this study had several limitations. First, the mice only received the treatments for 2 months. As long-term treatment efficacy remains unclear, future studies on the long-term treatment effects will be conducted by our group. Moreover, although BP/CL showed an anti-tuberculosis effect in vivo, the difference in effect between human and mouse kidney dehydrogenase on drug efficacy was not addressed and may have impacted our drug efficacy estimates. Another limitation of our study was that only the standard H37Rv MTB strain was used to access in vivo activity of BP/CL against MTB rather than a drug-resistant MTB strain. A further in vivo study with drug-resistant MTB strains will extend our knowledge of the in vivo anti-TB efficacy of this combination.
-
Our study demonstrated that BP/CL has antibacterial activity against Mtb, and thus may serve as a new clinical treatment option for treating MDR-TB.
doi: 10.3967/bes2019.033
-
Abstract:
Objective To assess the activities of biapenem against multidrug-resistant and extensively drug-resistant Mycobacterium tuberculosis. Methods Biapenem/clavulanate (BP/CL) was evaluated for in vitro activity against Mycobacterium tuberculosis (Mtb) multidrug-resistant (MDR) isolates, extensively drug-resistant (XDR) isolates, and the H37RV strain. BP/CL activity against the H37Rv strain was assessed in liquid cultures, in macrophages, and in mice. Results BP/CL exhibited activity against MDR and XDR Mtb isolates in liquid cultures. BP/CL treatment significantly reduced the number of colony forming units (CFU) of Mtb within macrophages compared with control untreated infected macrophages. Notably, BP/CL synergized in pairwise combinations with protionamide, aminosalicylate, and capreomycin to achieve a fractional inhibitory concentration for each pairing of 0.375 in vitro. In a mouse tuberculosis infection model, the efficacy of a cocktail of levofloxacin + pyrazinamide + protionamide + aminosalicylate against Mtb increased when the cocktail was combined with BP/CL, achieving efficacy similar to that of the positive control treatment (isoniazid + rifampin + pyrazinamide) after 2 months of treatment. Conclusion BP/CL may provide a new option to clinically treat MDR tuberculosis. -
Key words:
- Biapenem /
- Clavulanate /
- Multidrug resistant /
- Extensive drug-resistant /
- Mycobacterium tuberculosis /
- Activity /
- Macrophage /
- Synergy
-
Figure 1. Minimum inhibitory concentrations (MICs) of biapenem/clavulanate (BP/CL) against extensive drug-resistant tuberculosis (XDR-TB), multidrug-resistant tuberculosis (MDR-TB), and the H37Rv strain in vitro. #Fisher's exact test. *No difference between the MICs of BP/CL against XDR-TB or H37Rv. **No difference between the MICs of BP/CL against XDR-TB or MDR-TB. ***No difference between the MICs of BP/CL against MDR-TB or H37Rv.
Figure 2. Efficacy of regimens against Mycobacterium tuberculosis (Mtb) H37Rv in macrophages after 2 days of treatment. Fisher's Exact Test. Biapenem/clavulanate (BP)/(CL)40: BP and CL concentrations were 40 and 25 μg/mL, respectively; BP/CL20: BP and CL concentrations were 20 and 25 μg/mL, respectively; *P < 0.05, compared with the control group; three agents decreased CFU significantly; **No difference between these two groups.
Figure 3. Efficacy of regimens against Mycobacterium tuberculosis (Mtb) H37Rv in mice after 1 and 2 months of treatment. Control values used in panels A, B, and C were obtained from the same control group. (A) CFU reduction by PAS, BP/CL, and PAS + BP/CL in mice; (B) CFU reduction by Pto, BP/CL, and Pto + BP/CL in mice; (C) CFU reduction of regimen (Lfx + PZA + Pto + PAS), regimen + BP/CL, RHZ in mice; *In Figure C: P = 0.0049, significant difference in CFUs between the regimen group and the regimen + BP/CL group.
Table 1. Experimental Design Used in This Study
Group Drug Alone or Combinationa No. of Mice Sacrificed at Indicated Time Pointb Total No. of Mice D -14 D0 M1 M2 A Untreated 5 5 5 5 20 B BP/CL 5 5 10 C PAS 5 5 10 D Pto 5 5 10 E BP/CL + PAS 5 5 10 F BP/CL + Pto 5 5 10 G Lfx + Pto + PAS + PZA 5 5 10 H BP/CL + Lfx + Pto + PAS + PZA 5 5 10 I RIF + INH + PZA 5 5 10 Total No. of mice 5 5 45 45 100 Note. aDrugs were administered 5 days per week at the following doses: BP (100), CL (100), PAS (750), Pto (100), Lfx (200), RFP (10), INH (25), and PZA (150). bMice were sacrificed at the following times: 1 day after infection (D -14); 15 days after infection [day 0 (D0)]; 1, 2 months after treatment (M1, M2, respectively).  下载: 导出CSV
下载: 导出CSV
Table 2. Dosages of Drugs Administered to the Mice
Agents Dosage (mg/kg) Agents Dosages (mg/kg) BP 100 Lfx 200 CL 100 RFP 10 PAS 750 INH 25 Pto 100 PZA 150
下载: 导出CSV
Table 3. Fractional Inhibitory Concentration (FICs) of Biapenem/Clavulanate (BP/CL) Combinations with Other Second-line Anti-tuberculosis (TB) Drugs in vitro
Agents BP/CL LZD BP/CL Pto BP/CL Lfx BP/CL PAS BP/CL CPM BP/CL CLF MICalonea 2 0.5 2 2 2 0.5 2 0.25 2 2 2 0.24 MICcombinationb 1 0.0625 0.25 0.5 1 0.0625 0.25 0.0625 0.5 0.25 1 0.06 FIC 0.625 0.375* 0.625 0.375* 0.375* 0.75 Note. aMICalone: MIC of agent alone against H37Rv; bMICcombination: MIC of agents combined against H37Rv; *FIC < 0.5 means these two drugs were synergistic.
下载: 导出CSV
-
[1] World Health Organization. Global tuberculosis report 2018. https://apps.who.int/iris/bitstream/handle/10665/274453/9789241565646-eng.pdf?ua=1[2018-11-18] [2] Tiberi S, Sotgiu G, D'Ambrosio L, et al. Effectiveness and safety of meropenem/clavulanate-containing regimens in the treatment of MDR- and XDR-TB. Eur Respir J, 2016; 47, 1235-43. doi: 10.1183/13993003.02146-2015 [3] Tremblay LW, Fan F, Blanchard JS. Biochemical and structural characterization of Mycobacterium tuberculosis β-Lactamase (BlaC) with the carbapenems Ertapenem and Doripenem. Biochemistry, 2010; 49, 3766-73. doi: 10.1021/bi100232q [4] Hugonnet JE, Blanchard JS. Irreversible inhibition of the Mycobacterium tuberculosis beta-lactamase by clavulanate. Biochemistry, 2007; 46, 11998-2004. doi: 10.1021/bi701506h [5] Kumar P, Arora K, Lloyd JR, et al. Meropenem inhibits D, D-carboxypeptidase activity in Mycobacterium tuberculosis. Molecular Microbiology, 2012; 86, 367-81. doi: 10.1111/j.1365-2958.2012.08199.x [6] Lavollay M, Arthur M, Fourgeaud M, et al. The Peptidoglycan of Stationary-Phase Mycobacterium tuberculosis Predominantly Contains Cross-Links Generated by L, D-Transpeptidation. J Bacteriol, 2008; 190, 4360-6. doi: 10.1128/JB.00239-08 [7] Payen MC, Wit WC, Martin C, et al. Clinical use of the meropenem-clavulanate combination for extensively drug-resistant tuberculosis. International J Tuberculosis Lung Disease, 2012; 16, 558-60. doi: 10.5588/ijtld.11.0414 [8] De Lorenzo S, Alffenaar JW, Sotgiu G, et al. Efficacy and safety of meropenem/clavunate added to linezolid containing regimens in the treatment of MDR/XDR-TB. Eur Respir J, 2013; 41, 1386-92. doi: 10.1183/09031936.00124312 [9] Zhang D, Wang Y, Lu J, et al. In vitro activity of β-lactams in combination with β-lactams inhibitors against multidrug-resistant Mycobacterium tuberculosis isolates. AAC, 2015; 60, 393-9. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=c49de4fae597a324029ccd3f617a8d04 [10] Kaushik A, Ammerman NC, Tasneen R, et al. In vitro and in vivo activity of biapenem against drug-susceptible and rifampicin-resistant Mycobacterium tuberculosis. J Antimicrob Chemother, 2017; 72, 2320-5. doi: 10.1093/jac/dkx152 [11] Collins L, Franzblau SG. Microplate Amamar blue assay versus BACTEC 460 system for high-throughput screening of compounds against Mycobacterium tuberculosis and Mycobacterium avium. AAC, 1997; 41, 1004-9. doi: 10.1128/AAC.41.5.1004 [12] Sweeney MT, Zurenko GE. In vitro activities of linezolid combined with other antimicrobial agents against staphylococci, enterococci, pneumococci, and selected Gram-negative organisms. AAC, 2003; 47, 1902-6. doi: 10.1128/AAC.47.6.1902-1906.2003 [13] Reddy VM, Einck L, Andries K, et al. In Vitro Interactions between New Antitubercular Drug Candidates SQ109 and TMC207. AAC, 2010; 54, 2840-6. doi: 10.1128/AAC.01601-09 [14] Rey-Jurado E, Tudó G, de la Bellacasa JP, et al. In vitro effect of three-drug combinations of antituberculous agents against multidrug-resistant Mycobacterium tuberculosis isolates. Int J Antimicrob Agents, 2013; 41, 278-80. doi: 10.1016/j.ijantimicag.2012.11.011 [15] S Majumdar, SK Basu. Killing of intracellular Mycobacterium tuberculosis by receptor-mediated drug delivery. AAC, 1991; 35, 135-40. doi: 10.1128/AAC.35.1.135 [16] Yamada K, Yamamoto Y, Yanagihara K, et al. In vivo efficacy and pharmacokinetics of biapenem in a murine model of ventilator-associated pneumonia with Pseudomonas aeruginosa. J Infect Chemother, 2012; 18, 472-8. doi: 10.1007/s10156-011-0359-2 [17] Veziris N, Truffot C, Mainardi JL, et al. Activity of carbapenems combined with clavulanate against murine tuberculosis. AAC, 2011; 55, 2597-600. doi: 10.1128/AAC.01824-10 [18] Lee J, Carroll MW, Choi H, et al. Linezolid for treatment of chronic extensively drug-resistant tuberculosis. N Engl J Med, 2012; 367, 1508-18. doi: 10.1056/NEJMoa1201964 [19] Zareifopoulos N, Panayiotakopoulos G. Neuropsychiatric Effects of Antimicrobial Agents. Clin Drug Investig, 2017; 37, 423-7. doi: 10.1007/s40261-017-0498-z [20] Nakashima M, Uematsu T, Ueno K, et al. phase I study of L-627, biapenem, a new parenteral carbapenem antibiotic. Int J Clin Pharmacol Ther Toxicol, 1993; 31, 70-6. http://cn.bing.com/academic/profile?id=5bc7eeb7315aa7ff965d950199b42668&encoded=0&v=paper_preview&mkt=zh-cn [21] Abate G, Hoffner SE. Synergistic antimycobacterial activity between ethambutol and the beta-lactam drug cefepime. Diagn Microbiol Infect Dis, 1997; 28, 119-22. doi: 10.1016/S0732-8893(97)00012-6 [22] England K, Boshoff HI, Arora K, et al. Meropenem-clavulanic acid shows activity against Mycobacterium tuberculosis in vivo. AAC, 2012; 56, 3384-7. doi: 10.1128/AAC.05690-11 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 2691
- HTML全文浏览量: 723
- PDF下载量: 96
- 被引次数: 0

 Quick Links
Quick Links