

 下载:
下载:


-
Dementia is a major public health problem, currently affecting approximately 50 million people worldwide. Cases are projected to rise to 152 million by 2050 (World Alzheimer report 2018), with 50%–70% being Alzheimer’s dementia (AD) and 25% being vascular dementia (VD)[1,2]. As a heterogeneous neurodegenerative disease involving a complex pathogenic interplay between genetic and modifiable risk factors[3-5], the etiology of dementia remains poorly understood. This highlights an urgent need to explore novel pathways underlying the pathogenesis of dementia.
The brain-gut axis has received increasing attention in the field of dementia etiology. Inflammatory bowel disease (IBD), encompassing ulcerative colitis (UC) and Crohn’s disease (CD), is a chronic disease characterized by intestinal inflammation[6]. Previous evidence has indicated that IBD could increase the risk of developing an autoimmune disease[7], and contribute to neuroinflammation[8]. Clinical studies have shown an association between IBD and the risk of dementia. For instance, a longitudinal study in Taiwan reported a hazard ratio (HR) of 2.54 [95% confidence interval (CI) = 1.91–3.37] for dementia in IBD patients, with the greatest impact on AD (HR = 6.19, 95% CI = 3.31–11.57)[9]. However, subsequent studies did not find such large association[10,11]. Analyses using the Swedish National Patient Register and the UK Biobank data did not find any significant associations between IBD and dementia risk[12,13]. These conflicting findings highlight the uncertainty surrounding the relationship between IBD and dementia. Given the potential influence of unmeasured confounders, reverse causality, and selection bias in observational studies, the causal association between IBD and dementia remains unclear.
The Mendelian randomization (MR) approach has been widely deployed in genetic epidemiology to examine potential causal associations using observational data[14,15]. Although three MR studies have explored the causal association between IBD and AD[16-18], the findings have been inconsistent. The MR approach is still in development and faces the challenge of pleiotropy bias. To address these issues, a recently developed causal analysis using summary effect estimates (CAUSE) can effectively account for correlated and uncorrelated pleiotropic effects[19]. Additionally, genetic correlation[20,21] and co-localization analysis[22,23] are increasingly employed to assist MR analysis in elucidating causal associations.
This study aimed to update evidence on the association between IBD and dementia based on observational studies. We then explored the robustness of the results using serial MR methods, especially CAUSE, genetic correlation, and co-localization analyses. Our study sought to triangulate evidence from observational findings and genetic associations.
-
In the first part of the study, a meta-analysis was conducted and reported following the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) released in 2020 (
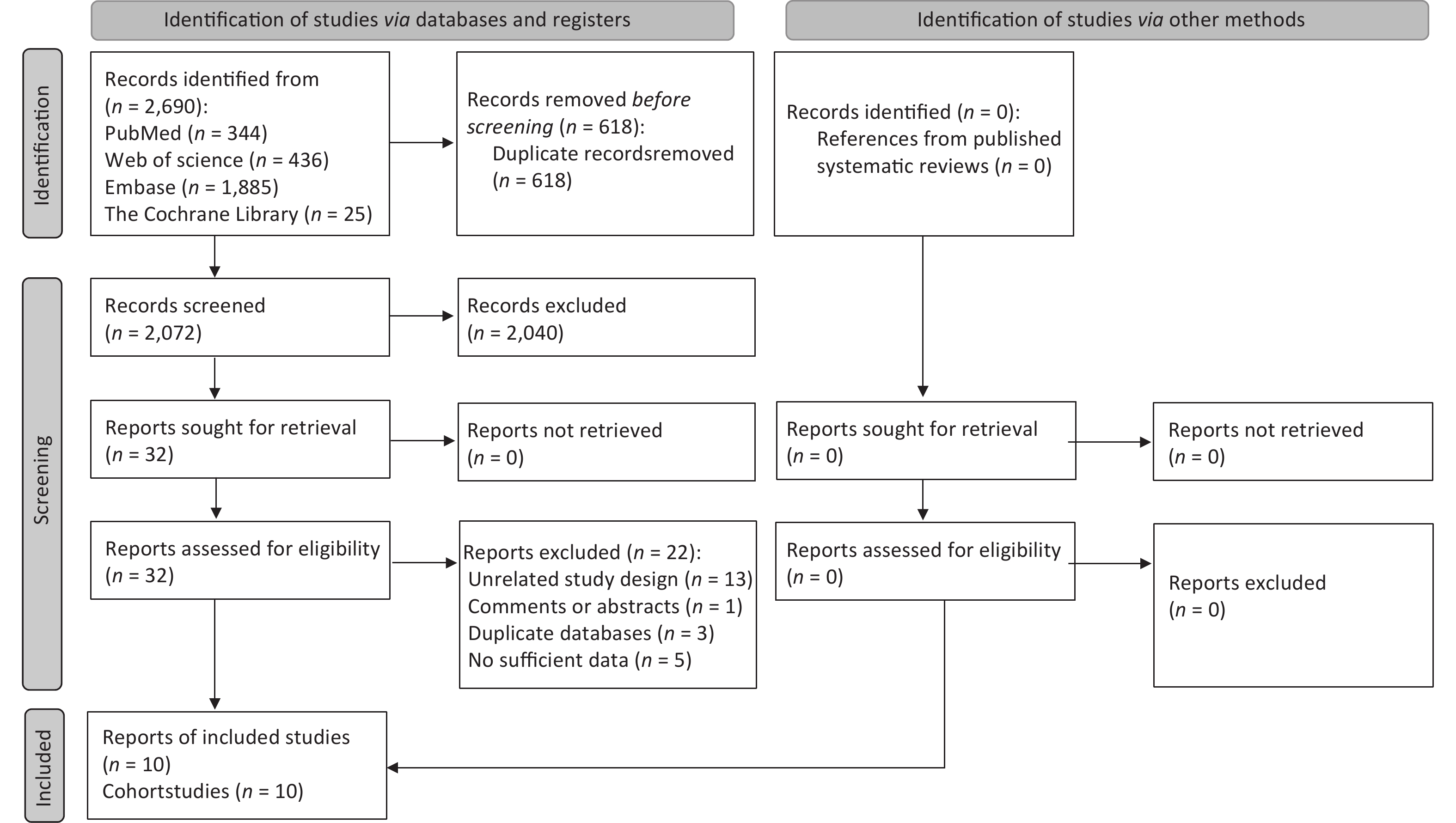
Supplementary Appendix 1 , available in www.besjournal.com)[24]. Four databases, PubMed, Web of Science, Embase, and the Cochrane Library, were searched from inception to February 2024 to identify eligible studies (the search strategies are shown inSupplementary Appendix 2 , available in www.besjournal.com). In addition, the references from relevant systematic reviews were scanned to identify eligible studies. The study selection process is presented in Figure 1.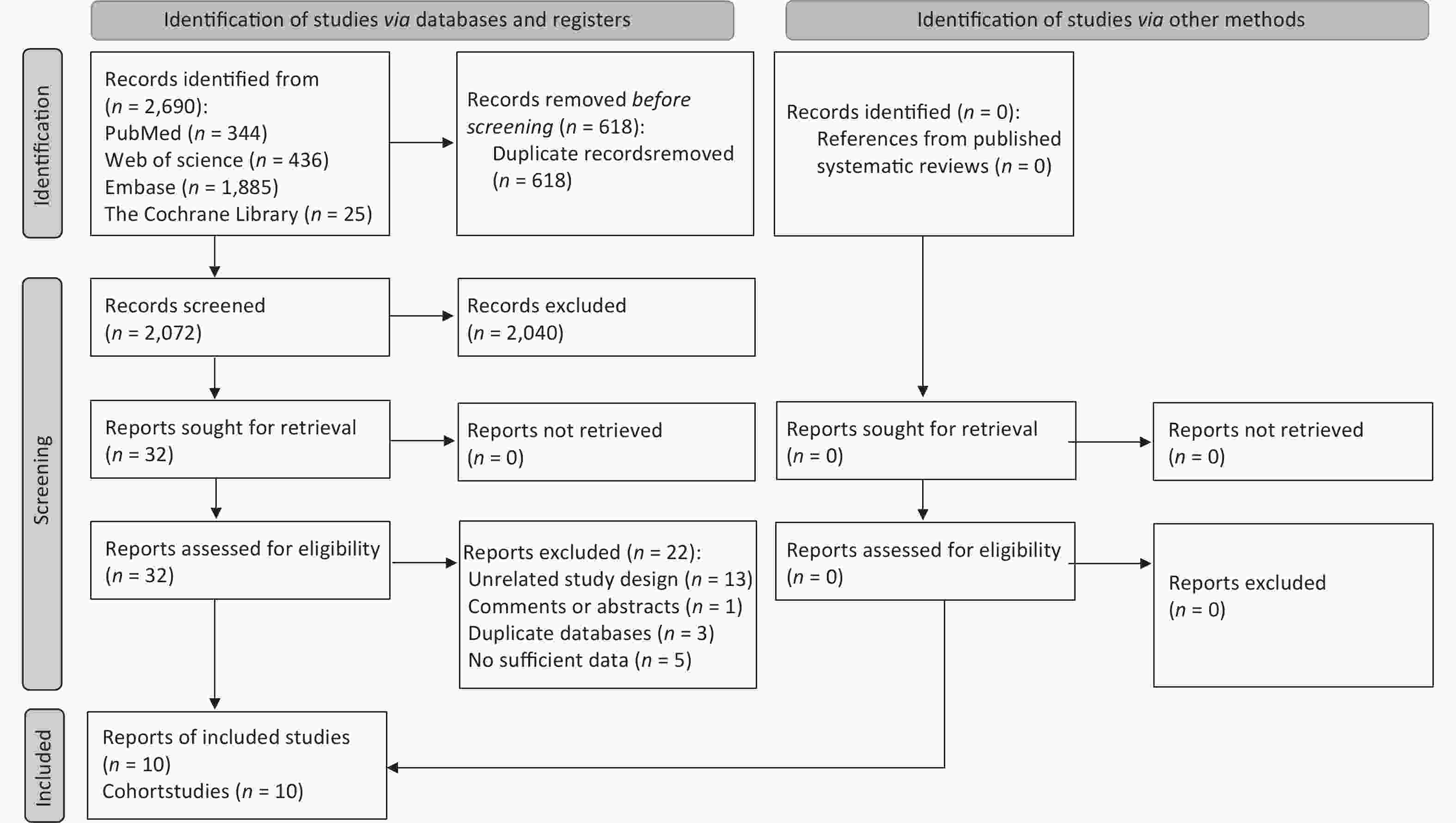
Figure 1. Flow diagram of the literature selection process.
Two independent investigators (MC and WC) reviewed and selected eligible articles. Observational studies concentrated in cohorts, case-controls, and nested case-controls were considered eligible for inclusion if they investigated the associations of IBD, including UC and CD, with dementia, including AD and VD. Studies that were duplicates, unrelated to study design, systematic reviews or meta-analyses, comments or conference abstracts, published in languages other than English, and publications based on the same database, were further excluded.
-
For each eligible study, we extracted key information, including the author, year, country, sample size, adjustment model, effect estimates (e.g., risk ratio [RR] or odds ratio [OR]) with their 95% CI, and the definitions of exposures and outcomes. We recorded the effect estimates after adjusting for confounding factors. For studies based on the same database and in the same country, we extracted information from the study with the largest sample size. We applied the Newcastle-Ottawa Scale (NOS) to evaluate the quality of the included articles. Two investigators (MC and WC) independently extracted and analyzed the data, and a third investigator (DL) resolved any disagreements.
We used random-effects models with the Mantel-Hanszel method to combine effect estimates, given that heterogeneity is common in observational studies. Owing to the low incidence of dementia, the OR can approximate the RR in observational studies. I2 statistics and the Cochrane Q test were used to test for heterogeneity. Additionally, a leave-one-out sensitivity analysis, omitting one study in turn, was used to explore the studies that could potentially affect the association. Egger’s test and funnel plots were used to detect potential publication bias.
A P < 0.05 was considered statistically significant. All the data analyses were performed by “meta” package in R version 4.1.3.
-
We used the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) to evaluate the certainty of the evidence[25]. The certainty of the overall evidence was initially rated as extremely low, low, moderate, or high. The hierarchy of evidence from observational studies was deemed low-certainty and was downgraded with violation of the five domains: risk of bias, inconsistency, indirectness, publication bias, and imprecision. Conversely, evidence was upgraded if a large effect size was observed, a dose-response relationship was demonstrated, or the effect size was likely underestimated due to negative bias.
-
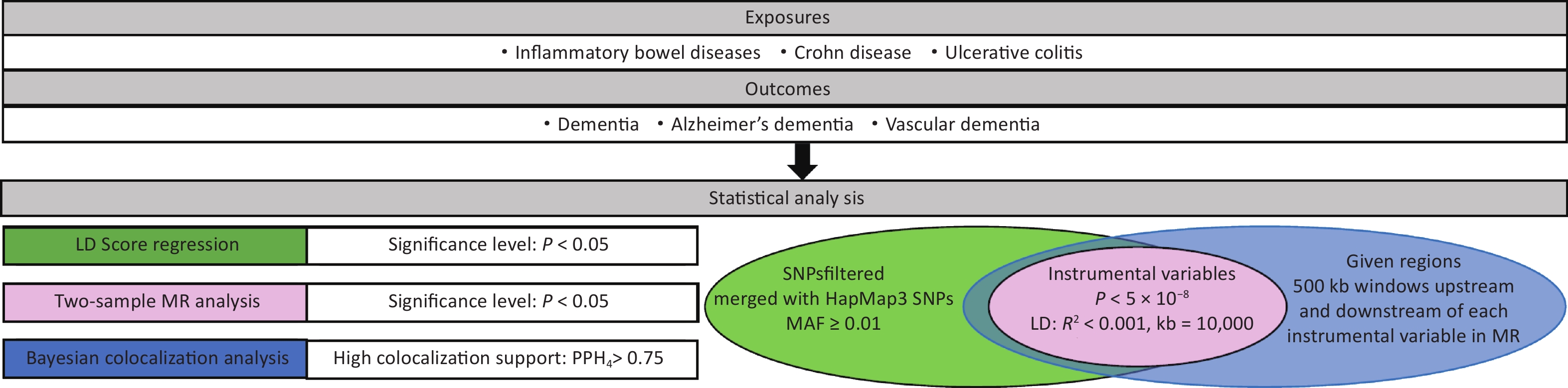
In the second part of the study, a two-sample MR analysis was performed to investigate the potential causal relationship between IBD and the risk of dementia. In addition, genome-wide linkage disequilibrium score (LDSC) was used to assess the genetic association between IBD and dementia, and co-localization analysis was used to investigate the local genetic structure shared between IBD and dementia and assess potential pleiotropy. An overview of the design and analysis process is shown in Figure 2. Since our analyses were based on summary-level genome-wide association study (GWAS) data, ethical approval and participant consent were not required.
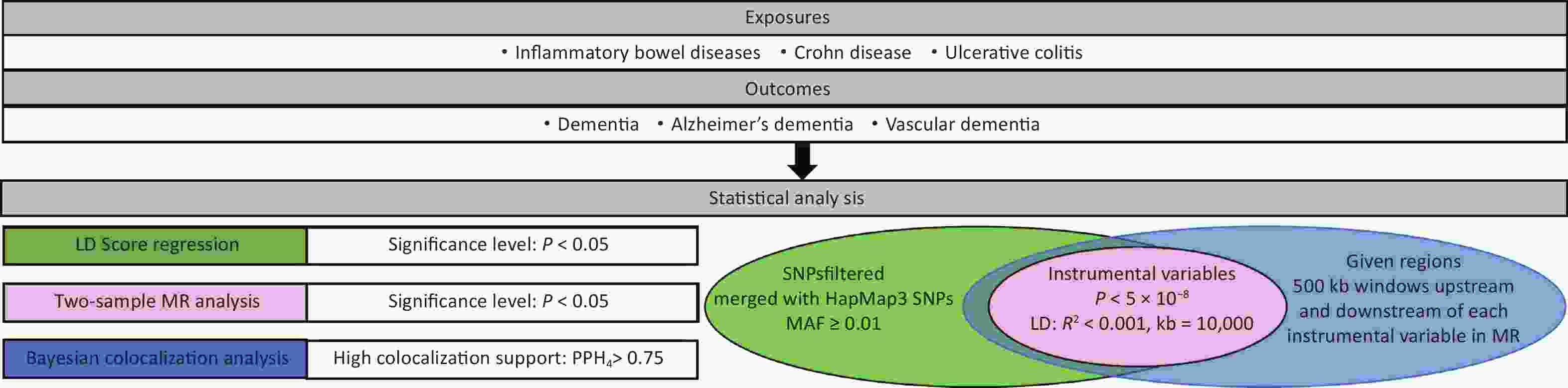
Figure 2. An overview of the MR study design. LD, linkage disequilibrium; MAF, minor allele frequency; MR, Mendelian randomization; SNPs, single nucleotide polymorphisms.
The MR study was conducted according to the STrengthening the Reporting of OBservational studies in Epidemiology using Mendelian Randomization (STROBE-MR;
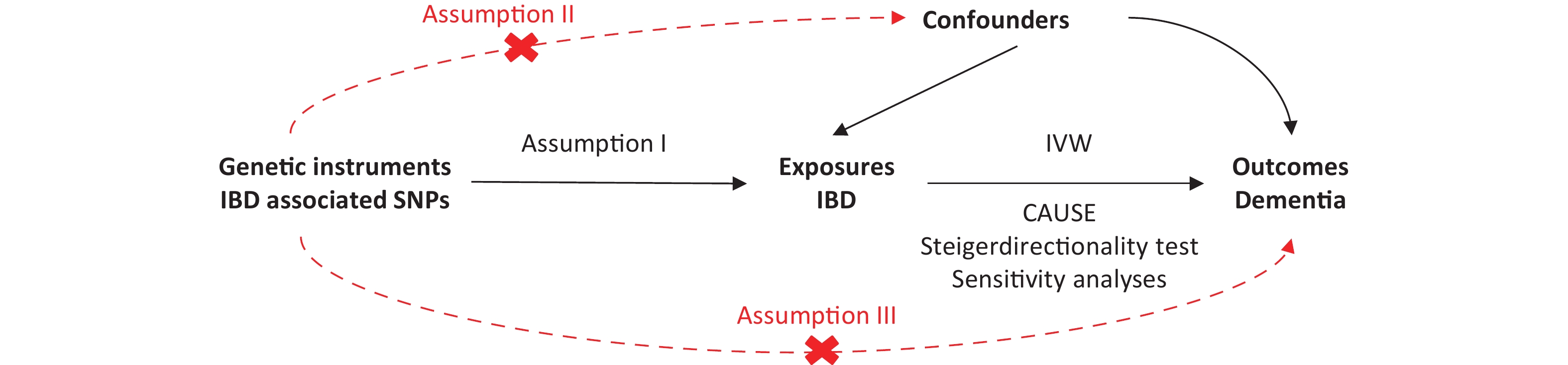
Supplementary Appendix 3 , available in www.besjournal.com)[26]. MR relies on three main assumptions[27]: (1) the instrumental variables (IVs), genetic variants, are strongly correlated with IBD; (2) the genetic variants are independent of the confounders in the IBD-dementia relationship; and (3) the genetic variants affect the risk of dementia only through IBD. The MR assumption is shown inSupplementary Figure S1 (available in www.besjournal.com). -
The summarized GWAS data for IBD and the two main forms of IBD, including UC and CD, were obtained from a published paper[28], which reported a meta-analysis of three GWASs from the UK low coverage whole genome sequencing IBD study, UK HumanCoreExome genotyped IBD study, and IIBDGC genotyped IBD study. The meta-analysis included 25,042 patients with IBD and 34,915 healthy controls, 12,194 with CD and 28,072 healthy controls, and 12,366 with UC and 33,609 healthy controls. Definitions of the IBD are shown in
Supplementary Table S1 (available in www.besjournal.com). -
The summarized GWAS data for dementia, including AD and VD, were based on FinnGen biobank analysis. The summarized data included 394,705 participants for AD and 393,024 participants for VD. Summarized GWAS data are available at https://storage.googleapis.com/finngen-public-data-r10/summary_stats/. In addition, we used GWAS-summarized data for AD, based on a meta-analysis of four large GWASs[29] (named AD-meta). The GWAS summarized data can be downloaded at https://ctg.cncr.nl/software/summary_statistics/. Additional information is provided in
Supplementary Table S1 . -
Single nucleotide polymorphisms (SNPs) significantly associated with IBD, UC, or CD (P < 5 × 10-8) were selected as candidate IVs, and linkage disequilibrium [LD] clumping (with the lowest P value having LD r2 < 0.001) was used to further select the final IVs based on the 1,000 genomes of European samples. Genetic variants with known pleiotropic effects were excluded from analyses using the Open Targets Genetics Tool.
The inverse-variance weighted (IVW) method was used to investigate the overall causal correlation between IBD and dementia risk. The IVW Q test was performed to assess the heterogeneity of the selected IVs. Fixed-effect IVW models were used if there was no heterogeneity (P > 0.05); otherwise, random-effects IVW models were used. We also conducted sensitivity analyses, including weighted median (WM), penalized weighted median (PWM), MR-Egger, MR-Pleiotropy Residual Sum and Outlier (PRESSO), MR-Robust Adjusted Profile Score (RAPS) and CAUSE[19].
The R2 [R2 = 2 × EAF × (1-EAF) × Beta2] of each SNP was estimated, and then summed up to assess the overall R2. The F-statistics and power were calculated using the online tool https://shiny.cnsgenomic.org/mRnd.Higher R2, F-statistic, and power indicated a lower risk of weak IV bias.
A key assumption of MR is that the IVs are not associated with any confounders of IBD or dementia (Supplementary Figure S1). Therefore, we assessed the effect of potential pleiotropy on causal estimates using three analytical approaches. First, an MR-Egger analysis was performed to test for pleiotropy. Second, we used the CAUSE method to elucidate the correlated and uncorrelated horizontal pleiotropic effects[19]. Third, we combined genetic evidence from genetic correlations and Bayesian co-localization analysis.
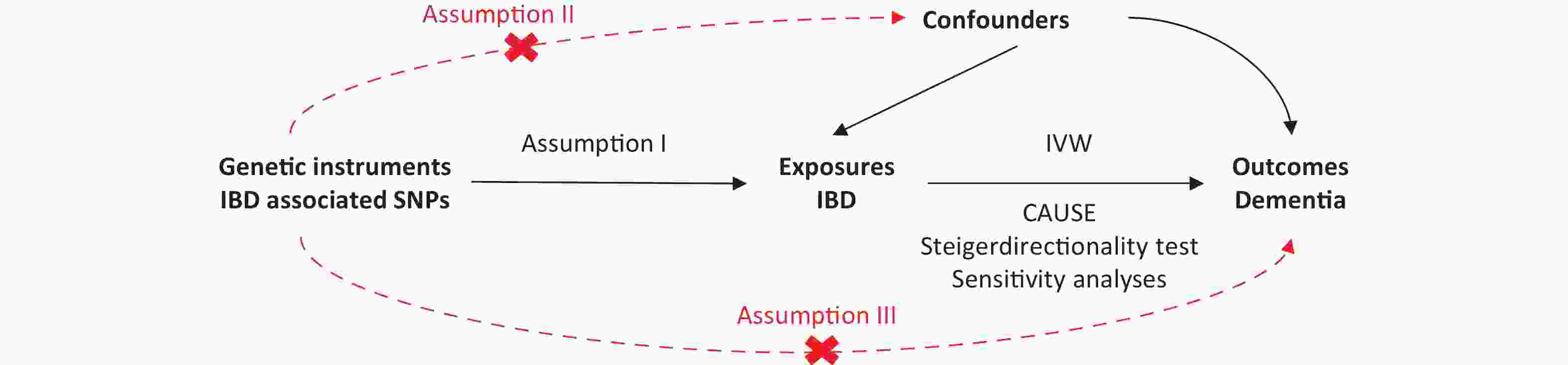
Figure S1. Mendelian randomization model.
Genome-wide LDSC[30] was used to assess genetic associations between IBD and dementia. When the proportion of heritability explained by genome-wide significant SNPs determined through MR approach is low, the accuracy of the MR results may be inferior to that of LDSC, which used all SNPs, including those that did not achieve genome-wide significance. The results of the LDSC analysis are presented as genetic correlation (rg) with standard error (SE).
Co-localization analysis was used to assess whether the two associated traits share consistent causal variants according to the included IVs and to evaluate potential pleiotropy. The involved hypotheses underlying co-localization have been reported[31], and we used the posterior probability hypothesis 4 (PPH4) to quantify the support of the hypothesis. For this analysis, the regions with 500 kb windows upstream and downstream of each instrumental variable were selected, and the average value of PPH4 across all regions was taken as the final co-localization result.
All analyses were two-sided, with P < 0.05 regarded as statistically significant unless otherwise specified. A PPH4 level exceeding 75% was considered suggestive of shared causal genetic variants between the two traits. Data analyses were performed using “TwoSampleMR”, “CAUSE” and “coloc” packages in R version 4.3.1.
-
A total of 2,072 articles were identified from the databases. Finally, ten articles met our criteria and were included in the meta-analysis (Figure 1). All ten studies were cohort studies[9-13,18,32-35]. Two articles[12,34] involved the use of the same database, but were both included in our analysis due to reporting on different exposures.
The characteristics of the included studies are presented in
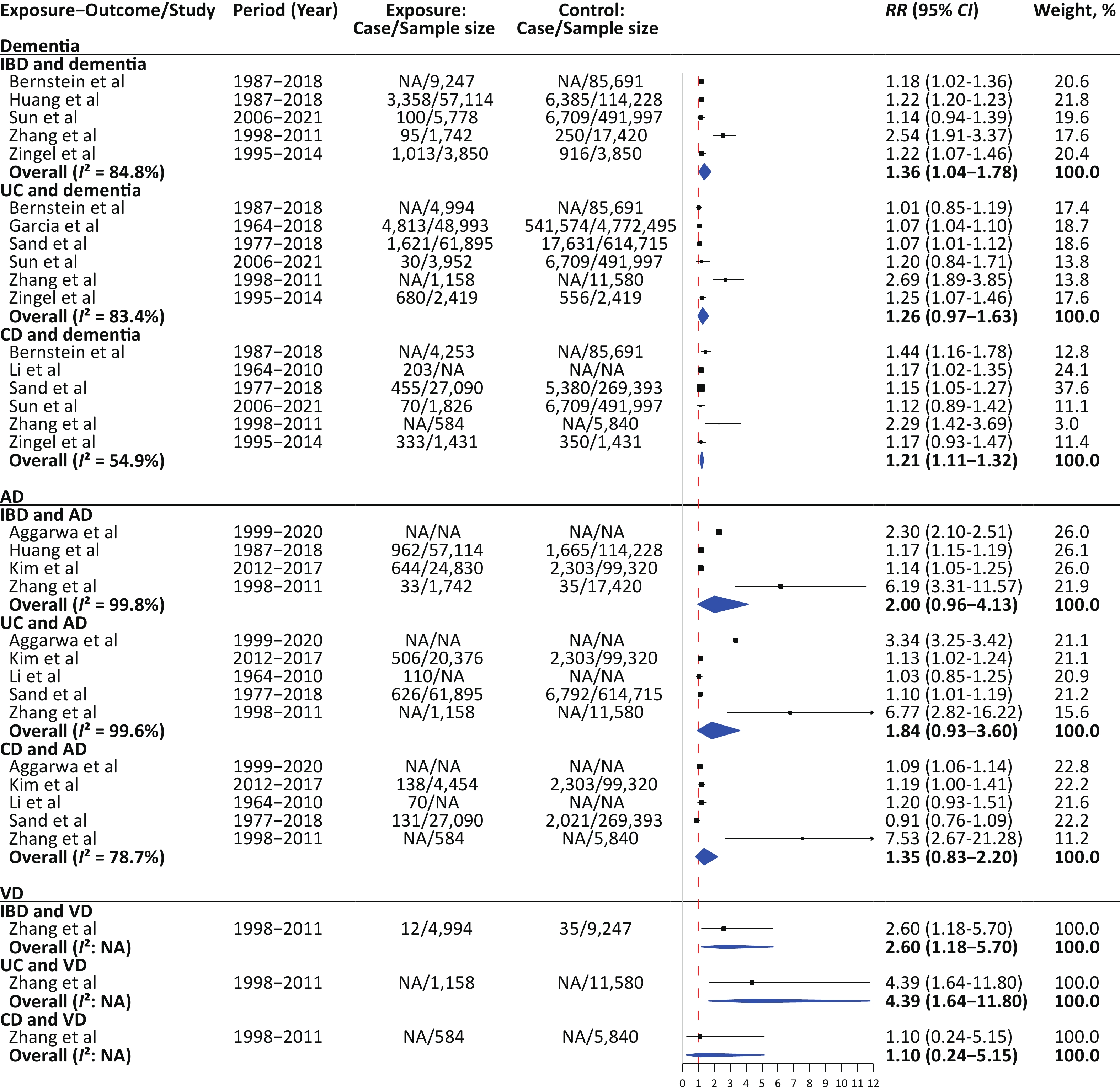
Supplementary Table S2 (available in www.besjournal.com). These studies mainly reported results from individuals of European and Asian ancestry, involving a total of 80,565,688 participants. All cohort studies were followed up for more than 5 years. The definitions of exposures and outcomes varied across the studies (Supplementary Appendix 4 , available in www.besjournal.com). The estimates for the individual studies are presented in Figure 3.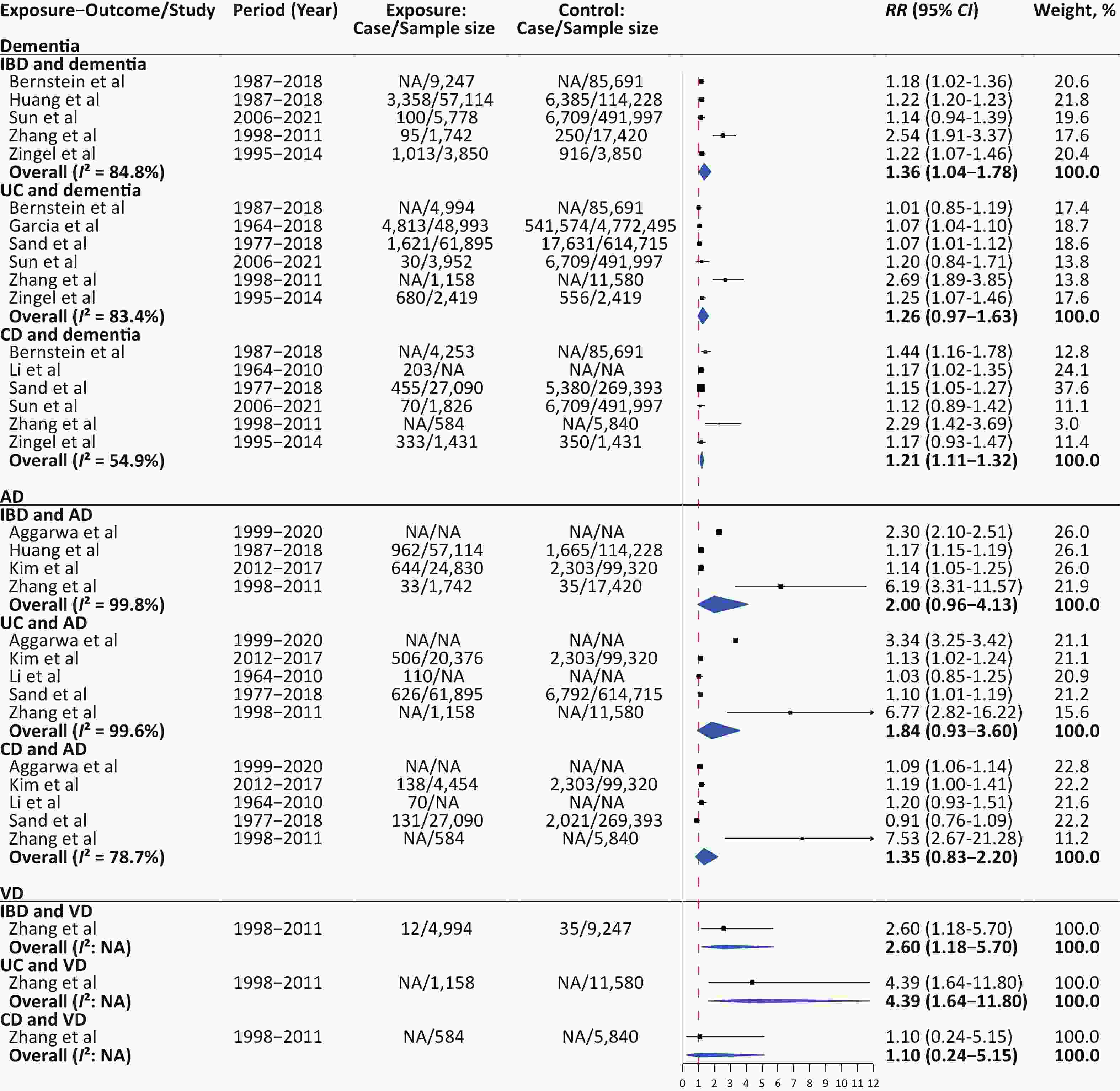
Figure 3. Forest plot for the pooled estimates of the association between inflammatory bowel disease and dementia. AD, Alzheimer’s disease; CD, Crohn’s disease; CI, confidence interval; IBD, inflammatory bowel disease; RR, risk ratio; UC, ulcerative colitis; VD, vascular dementia.
According to the NOS tool, the included studies had scores between 6 and 7. Most were based on electronic medical records or Medicare databases. The lack of direct validation for exposures and outcomes, potentially introducing misclassification bias, contributed to their classification as low quality. In addition, half of the included studies did not match confounders between the IBD and non-IBD groups (
Supplementary Table S2 ). -
For dementia, the combined RR of IBD was 1.36 (95% CI = 1.04–1.78) based on random-effects model; the five studies have shown significant heterogeneity (I2 = 84.8%; Figure 3). Meta-analysis based on types of UC and CD in the six studies provided the RR of 1.26 (95% CI = 0.97–1.63; I2 = 83.4%) and 1.21 (95% CI = 1.11–1.32; I2 = 54.9%), respectively. For AD, the combined RR of IBD in the four studies was 2.00 (95% CI = 0.96–4.13; I2 = 99.8%; Figure 3). Meta-analysis based on types of UC and CD in the five studies that provided the RR of 1.84 (95% CI = 0.93–3.60; I2 = 99.6%) and 1.35 (95% CI = 0.83–2.20; I2 = 78.7%), respectively. Only one study reported an association between IBD and VD. The RR of IBD, UC and CD individually was 2.60 (95% CI = 1.18–5.70), 4.39 (95% CI = 1.64–11.80) and 1.10 (95% CI = 0.24–5.15), respectively (Figure 3).
Considering the large heterogeneity across studies, we used a leave-one-out sensitivity analysis to explore which study affected the effect size and caused heterogeneity. Excluding Zhang's study notably reduced the heterogeneity in most analyses (Table 1). After excluding Zhang's study, the combined RR for dementia was 1.22 (95% CI = 1.20–1.23; I2 = 0) in IBD patients, 1.07 (95% CI = 1.05–1.10; I2 = 14.0%) in UC patients, 1.18 (95% CI = 1.10–1.26; I2 = 0) in CD patients. The combined RR for AD was 1.45 (95% CI = 0.93–2.27; I2 = 99.6%) in IBD patients, 1.44 (95% CI = 0.83–2.51; I2 = 99.7%) in UC patients, 1.09 (95% CI 0.99–1.19; I2 = 45.0%) in CD patients.
Table 1. Sensitivity analyses for the pooled effect estimates of the association between inflammatory bowel disease and dementia
Exposure and outcome n RR (95% CI) I2, % IBD and Dementia 5 1.36 (1.04−1.78) 84.8 Omitting Bernstein et al 4 1.42 (1.00−2.00) 88.0 Omitting Huang et al 4 1.41 (0.99−2.01) 88.0 Omitting Sun et al 4 1.43 (1.02−2.00) 88.0 Omitting Zhang et al 4 1.22 (1.20−1.23) 0 Omitting Zingel et al 4 1.41 (0.99−2.00) 89.0 UC and Dementia 6 1.26 (0.97−1.63) 83.4 Omitting Bernstein et al 5 1.32 (0.97−1.80) 87.0 Omitting Garcia et al 5 1.31 (0.95−1.81) 86.0 Omitting Sand et al 5 1.31 (0.95−1.81) 87.0 Omitting Sun et al 5 1.27 (0.93−1.75) 87.0 Omitting Zhang et al 5 1.07 (1.05−1.10) 14.0 Omitting Zingel et al 5 1.27 (0.91−1.76) 85.0 CD and Dementia 6 1.21 (1.11−1.32) 54.9 Omitting Bernstein et al 5 1.17 (1.09−1.26) 49.0 Omitting Li et al 5 1.27 (1.09−1.49) 64.0 Omitting Sand et al 5 1.28 (1.10−1.49) 59.0 Omitting Sun et al 5 1.26 (1.11−1.44) 63.0 Omitting Zhang et al 5 1.18 (1.10−1.26) 0 Omitting Zingel et al 5 1.26 (1.09−1.45) 64.0 IBD and AD 4 2.00 (0.96−4.13) 99.8 Omitting Aggarwa et al 3 1.94 (0.68−5.56) 92.7 Omitting Huang et al 3 2.43 (0.96−6.16) 98.6 Omitting Kim et al 3 2.45 (0.98−6.11) 99.2 Omitting Zhang et al 3 1.45 (0.93−2.27) 99.1 UC and AD 5 1.84 (0.93−3.60) 99.6 Omitting Aggarwa et al 4 1.56 (0.73−3.36) 82.5 Omitting Kim et al 4 2.11 (0.91−4.91) 99.6 Omitting Li et al 4 2.16 (0.95−4.87) 99.7 Omitting Sand et al 4 2.13 (0.92−4.91) 99.6 Omitting Zhang et al 4 1.44 (0.83−2.51) 99.7 CD and AD 5 1.35 (0.83−2.20) 78.7 Omitting Aggarwa et al 4 1.56 (0.72−3.39) 84.0 Omitting Kim et al 4 1.53 (0.69−3.36) 83.0 Omitting Li et al 4 1.52 (0.69−3.34) 83.0 Omitting Sand et al 4 1.61 (0.79−3.28) 80.0 Omitting Zhang et al 4 1.09 (0.99−1.19) 45.0 Note. AD, Alzheimer’s disease; CD, Crohn’s disease; CI, confidence interval; IBD, inflammatory bowel disease; RR, risk ratio; UC, ulcerative colitis. -
The Egger’s test indicated no significant publication bias (P = 0.782), and the funnel plot did not display obvious asymmetry (Supplementary Figure S2, available in www.besjournal.com).
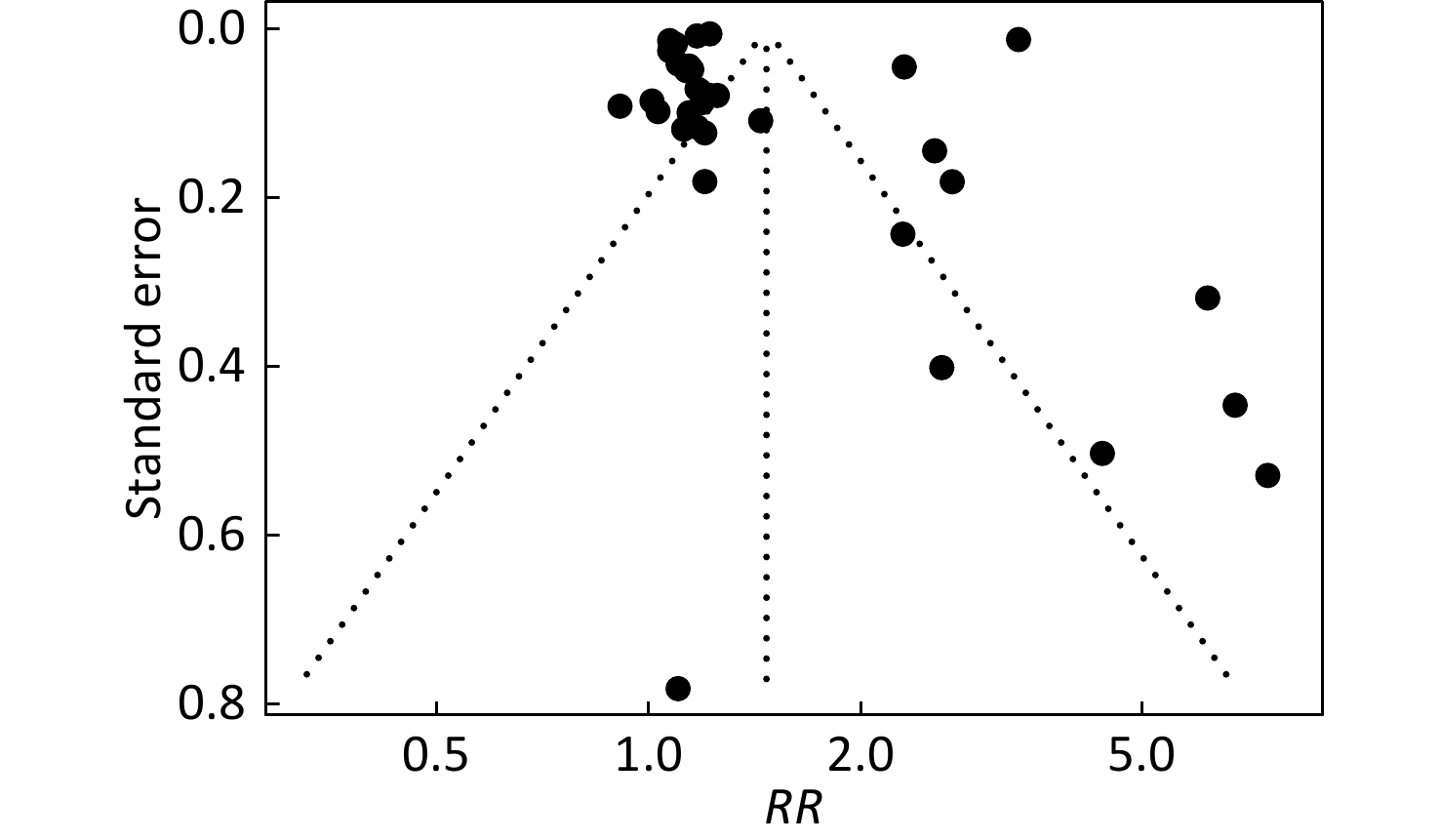
Figure S2. Funnel plot for assessment of publication bias.
-
Overall, the quality of evidence regarding the association between IBD and dementia was rated very low based on the GRADE framework (
Supplementary Table S3 , available in www.besjournal.com). The main consideration for downgrading was the high heterogeneity across studies. -
All variances explained by IVs for IBD, UC, and CD were greater than 0.5, and the F-statistics were greater than 10, indicating that the included SNPs satisfied the strong relevance assumption. Detailed information on the IVs is presented in
Supplementary Table S4 (available in www.besjournal.com).As shown in Table 2, the conventional MR analyses showed no significant genetic associations between IBD and dementia (OR = 1.01, 95% CI = 0.98–1.03). Similarly, UC and CD were not associated with the increased risk of dementia (OR = 1.00, 95% CI = 0.98–1.03; OR = 0.99, 95% CI = 0.97–1.02). The associations of IBD, UC or CD with dementia were robust in all sensitivity analyses (all P > 0.05), except that the WM and PWM analyses showed modest associations between CD and dementia (OR = 0.96, 95% CI = 0.93–0.99; OR = 0.95, 95% CI = 0.92–0.98;
Supplementary Table S5, available in www.besjournal.com). The CAUSE method used to elucidate the correlated and uncorrelated horizontal pleiotropic effects, avoiding false positives induced by correlated horizontal pleiotropy, did not find any significant causal associations between genetically instrumented IBD, UC, or CD and dementia (Table 2). These findings indicated that the modest associations of genetically instrumented IBD and CD with dementia identified by the WM and PWM analyses might be caused by horizontal pleiotropy.Table 2. The Mendelian randomization analysis for the associations between IBD and dementia
Phenotype IBD UC CD IVW CAUSE IVW CAUSE IVW CAUSE OR (95% CI) P OR (95% CI) P OR (95% CI) P OR (95% CI) P OR (95% CI) P OR (95% CI) P Dementia 1.01
(0.98−1.03)0.657 0.99
(0.98−1.01)0.870 1.00
(0.98−1.03)0.841 1.01
(0.99−1.03)0.680 0.99
(0.97−1.02)0.562 1.00
(0.98−1.02)1.000 AD 0.98
(0.95−1.01)0.156 1.00
(0.97−1.03)1.000 1.00
(0.96−1.05)0.867 1.02
(0.99−1.06)0.410 0.99
(0.96−1.02)0.628 0.99
(0.96−1.02)0.800 AD-meta 1.00
(0.99−1.00)0.506 1.00
(0.996−1.004)1.000 1.01
(1.00−1.01)0.104 1.00
(0.996−1.004)1.000 1.00
(1.00−1.01)0.952 1.00
(0.997−1.003)1.000 VD 1.02
(0.97−1.07)0.446 1.00
(0.96−1.04)1.000 1.00
(0.94−1.05)0.857 1.01
(0.96−1.06)0.990 0.97
(0.92−1.01)0.163 1.00
(0.96−1.04)1.000 Note. CAUSE, causal analysis using summary effect; CD: Crohn’s disease; CI, confidence interval; IBD, inflammatory bowel disease; IVW, inverse-variance-weighted; OR, odds ratio; SNPs, single nucleotide polymorphisms; UC, ulcerative colitis. The conventional MR analyses showed no significant association between genetically instrumented IBD, UC or CD and AD (OR = 0.98, 95% CI = 0.95–1.01; OR = 1.00, 95% CI = 0.96–1.05; OR = 0.99, 95% CI = 0.96-1.02, respectively). The robust findings in the database of AD-meta indicated no associations either (OR = 1.00, 95% CI = 0.99–1.00; OR = 1.01, 95% CI = 1.00–1.01; OR = 1.00, 95% CI = 1.00–1.01; Table 2). The associations between IBD, UC, or CD and AD were robust in all sensitivity analyses (all P > 0.05), except for the MR-Egger and MR-RAPS analyses, which showed significant associations of genetically instrumented UC with AD in the AD-meta database (OR = 1.02, 95% CI = 1.003–1.03; OR = 1.004, 95% CI = 1.00–1.01;
Supplementary Table S6 , available in www.besjournal.com). We did not find any significant causal associations between genetically instrumented IBD, UC, or CD and AD using the CAUSE method, indicating that the significant association between genetically instrumented UC and AD in the AD-meta database might be caused by horizontal pleiotropy.Likewise, the conventional MR analyses showed no significant associations of genetically instrumented IBD, UC, or CD with VD (OR = 1.02, 95% CI = 0.97–1.07; OR = 1.00, 95% CI = 0.94–1.05; OR = 0.97, 95% CI = 0.92–1.01; Table 2). Sensitivity analyses using various statistical models yielded consistent results (
Supplementary Table S7 , available in www.besjournal.com). The CAUSE method confirmed the lack of causal association between genetically instrumented IBD, UC, or CD and AD. -
The genetic correlation between IBD and dementia ranged from 0.001 to 0.043 (Table 3). There were no significant genetic correlations between IBD, CD, or UC and dementia (all P > 0.05).
Table 3. The genetic correlation and co-localization analyses for the associations between IBD and dementia
Phenotype IBD UC CD Genetic correlation Co* Genetic correlation Co* Genetic correlation Co* rg (se) P PPH4 rg (se) P PPH4 rg (se) P PPH4 Dementia −0.027 (0.022) 0.216 2.97% −0.043 (0.026) 0.096 4.00% −0.001 (0.021) 0.980 2.28% AD −0.016 (0.035) 0.645 2.29% −0.001 (0.042) 0.978 4.61% −0.020 (0.035) 0.569 1.95% AD-meta 0.005 (0.018) 0.781 1.28% −0.012 (0.023) 0.607 1.37% 0.013 (0.019) 0.504 2.75% VD 0.003 (0.037) 0.941 3.44% 0.014 (0.042) 0.734 3.02% 0.017 (0.036) 0.645 3.16% Note. *Co, co-localization analysis: the average value of PPH4 across all regions was used as the final co-localization result. CD, Crohn’s disease; CI, confidence interval; IBD, inflammatory bowel disease; SE, standard error; SNPs, single nucleotide polymorphisms; UC, ulcerative colitis. -
There was no shared causal variant to suppport the association between IBD and dementia using co-localization analysis, as indicated by the average value of PPH4 across all regions (PPH4 < 75%; Table 3). These co-localization results suggest that there may be no common biological mechanism linking IBD and dementia.
-
Our meta-analysis indicated that IBD was associated with the risk of dementia but not with the risk of AD. However, considerable heterogeneity has been observed among these studies. Our study did not provide genetic evidence of a causal association between IBD and the risk of all-cause dementia. Exposure to IBD may not independently contribute to the risk of dementia, and the increased risk of dementia observed in observational studies may be due to unobserved confounding factors or detection biases.
Five systematic reviews and meta-analyses have summarized the relationship between IBD and dementia; however, previous findings were inconsistent[36-40]. Additionally, previous meta-analyses did not consider all relevant exposures (including IBD, UC, and CD) or outcomes (including all-cause dementia, AD, and VD). Our updated meta-analysis includes all these exposures and outcomes. To minimize the possibility of publication duplication based on the same database, we carefully screened and included the largest sample available. Notably, one study based on the UK Biobank did not support a significant association between IBD and dementia[13], while another study based on the same database showed that IBD was associated with early-onset dementia[41]. These findings suggest that different confounding factors and dementia types may have affected the study results. Our meta-analysis suggested that great heterogeneity was mainly driven by Zhang et al. ’s study, possibly due to differences in individual study characteristics (i.e., symptom severity, treatment, inclusion criteria, race, ethnicity, and other potential confounders).
Considering unobserved confounding factors, we performed genetic analyses to further clarify the association between IBD and dementia. By combining genetic evidence from MR, genetic correlation, and co-localization analyses, we found a lack of evidence to support the causality between IBD and dementia risk. Our findings are somewhat inconsistent with those of previous MR studies. A recent MR study showed that genetically instrumented IBD is associated with a decreased AD risk[16], whereas two other studies did not provide evidence for this association[17,18]. Considering that pleiotropy poses a challenge in interpreting MR results, we used the CAUSE method to correct for correlated and uncorrelated horizontal pleiotropic effects[19]. The CAUSE analysis showed no significant causal associations of genetically instrumented IBD, UC, or CD with dementia or AD, indicating that the significant associations observed in the recent MR study, as well as in our sensitivity analyses, might be caused by horizontal pleiotropy. In addition, we combined genetic evidence from MR with genetic correlation and co-localization analyses to simultaneously address the limitations of MR, such as its limited power due to the small number of SNPs and potential pleiotropy.
Evidence triangulation in our study suggests that the association between IBD and dementia found in some observational studies may not be causal. Some potential explanations may be as follows. First, IBD and dementia have many shared risk factors such as an unhealthy lifestyle, social class, institutionalization, and medical comorbidities, which could lead to residual confounding. Second, if IBD occurs secondary to a pre-dementia state or subclinical dementia, reverse causation could also occur, inducing false causal associations. Third, a greater number of medical examinations in patients with IBD than in the control population induces detection bias and results in a false association between IBD and dementia, as most observational studies are based on electronic medical record databases. Finally, the use of an elderly population may contribute to selection bias, particularly due to survival bias and the competing risk of dementia.
In terms of the shared factors for IBD and dementia, environmental and behavioral factors may play a significant role. The combination of lifestyle and drugs for the treatment of IBD has been shown to alleviate cognition in dementia and may represent the most promising way to prevent and treat dementia. Increasing evidence highlights the mutual connection between the gut and central nervous system, known as the “gut-brain axes”[42-44]. Intestinal homeostasis is associated with many psychiatric and neurological syndromes through the gut-brain axis, which describes the signaling between the microbiome, gut, and central nervous system[42,43,45-50]. The gut microbiome, in particular, is crucial in mediating the relationship between IBD and dementia[50,51]. Additionally, previous studies have shown that smoking increases the risk of IBD and dementia, whereas physical activity decreases the risk of IBD and AD[4,52]. Furthermore, a higher intake of ultra-processed foods is correlated with the risk of IBD and AD[53,54]. Because the association between IBD and dementia is unlikely to be causal, further studies are warranted to investigate the shared factors contributing to the comorbidities of IBD and dementia.
Our evidence triangulation from a meta-analysis of observational studies and genetic associations provided a deeper understanding of the association between IBD and dementia. However, this study had some limitations. First, the heterogeneity observed in our meta-analysis was high and largely unexplainable. While this may be attributed to the differences in individual characteristics (i.e., race, ethnicity, symptom severity, medical comorbidities associated with IBD treatment, and diagnostic criteria), study duration, adjusting factors, and sample size, the limited number of studies prevented us from exploring heterogeneity sources by subgroup analysis or meta-regression. Furthermore, we did not obtain individual-level data and were unable to control for more confounding factors. While MR studies are less prone to certain biases, they may still be affected by weak instruments and pleiotropic biases. Despite leveraging GWAS data with large sample sizes, our study was limited in its ability to detect small effects. To enhance the robustness of our findings, we combined the genetic correlation and MR methods and conducted multiple supplementary and sensitivity analyses. Finally, we used GWAS data from individuals of European ancestry, even though the clinical and genetic characteristics of IBD and dementia may differ between cultural and ethnic groups. Therefore, our findings may not be generalizable to other racially or ethnically diverse populations.
-
Overall, our meta-analysis suggests that IBD is associated with the risk of dementia but not with an increased risk of AD, with considerable heterogeneity across studies. However, genetic evidence suggests no causal association between IBD and dementia. The observed association between IBD and dementia in observational studies may be influenced by unobserved confounding factors or detection biases. Further exploration of the shared factors underlying the comorbidity of IBD and dementia may help identify potential targets for the prevention of IBD-dementia comorbidity via the gut-brain axis.
doi: 10.3967/bes2024.149
Inflammatory Bowel Disease and Dementia: Evidence Triangulation from a Meta-Analysis of Observational Studies and Mendelian Randomization Study
-
Abstract:
Objective Observational studies have found associations between inflammatory bowel disease (IBD) and the risk of dementia, including Alzheimer’s dementia (AD) and vascular dementia (VD); however, these findings are inconsistent. It remains unclear whether these associations are causal. Methods We conducted a meta-analysis by systematically searching for observational studies on the association between IBD and dementia. Mendelian randomization (MR) analysis based on summary genome-wide association studies (GWASs) was performed. Genetic correlation and Bayesian co-localization analyses were used to provide robust genetic evidence. Results Ten observational studies involving 80,565,688 participants were included in this meta-analysis. IBD was significantly associated with dementia (risk ratio [RR] =1.36, 95% CI = 1.04–1.78; I2 = 84.8%) and VD (RR = 2.60, 95% CI = 1.18–5.70; only one study), but not with AD (RR = 2.00, 95% CI = 0.96–4.13; I2 = 99.8%). MR analyses did not supported significant causal associations of IBD with dementia (dementia: odds ratio [OR] = 1.01, 95% CI = 0.98–1.03; AD: OR = 0.98, 95% CI = 0.95–1.01; VD: OR = 1.02, 95% CI = 0.97–1.07). In addition, genetic correlation and co-localization analyses did not reveal any genetic associations between IBD and dementia. Conclusion Our study did not provide genetic evidence for a causal association between IBD and dementia risk. The increased risk of dementia observed in observational studies may be attributed to unobserved confounding factors or detection bias. -
Key words:
- Dementia /
- Inflammatory bowel disease /
- Meta-analysis /
- Observational studies /
- Mendelian randomization /
- Genetic evidence /
- Evidence triangulation
The authors declare that they have no competing interests.
Our study did not include individual data from the human participants. The analyses for this study were based on publicly available summary datasets, and no additional ethical approval or consent to participate was required.
注释:1) Authors’ Contributions: 2) Competing Interests: 3) Ethics: -
Figure 2. An overview of the MR study design. LD, linkage disequilibrium; MAF, minor allele frequency; MR, Mendelian randomization; SNPs, single nucleotide polymorphisms.
S1. Mendelian randomization model.
Solid arrows indicate causal effects; dashed arrows indicate causal effects prohibited by MR assumptions II and III. Assumption I: Genetic instruments are associated with exposure, Assumption II: Genetic instruments are independent of confounding factors, and Assumption III: Genetic instruments affect outcomes only through exposure. CAUSE, Causal Analysis Using Summary Effect; IBD, inflammatory bowel disease; IVW, inverse-variance-weighted.
Figure 3. Forest plot for the pooled estimates of the association between inflammatory bowel disease and dementia. AD, Alzheimer’s disease; CD, Crohn’s disease; CI, confidence interval; IBD, inflammatory bowel disease; RR, risk ratio; UC, ulcerative colitis; VD, vascular dementia.
S2. Funnel plot for assessment of publication bias.
Each point represents an association between IBD and dementia. IBD: Inflamm Bowel Dis; RR: risk ratio.
Table 1. Sensitivity analyses for the pooled effect estimates of the association between inflammatory bowel disease and dementia
Exposure and outcome n RR (95% CI) I2, % IBD and Dementia 5 1.36 (1.04−1.78) 84.8 Omitting Bernstein et al 4 1.42 (1.00−2.00) 88.0 Omitting Huang et al 4 1.41 (0.99−2.01) 88.0 Omitting Sun et al 4 1.43 (1.02−2.00) 88.0 Omitting Zhang et al 4 1.22 (1.20−1.23) 0 Omitting Zingel et al 4 1.41 (0.99−2.00) 89.0 UC and Dementia 6 1.26 (0.97−1.63) 83.4 Omitting Bernstein et al 5 1.32 (0.97−1.80) 87.0 Omitting Garcia et al 5 1.31 (0.95−1.81) 86.0 Omitting Sand et al 5 1.31 (0.95−1.81) 87.0 Omitting Sun et al 5 1.27 (0.93−1.75) 87.0 Omitting Zhang et al 5 1.07 (1.05−1.10) 14.0 Omitting Zingel et al 5 1.27 (0.91−1.76) 85.0 CD and Dementia 6 1.21 (1.11−1.32) 54.9 Omitting Bernstein et al 5 1.17 (1.09−1.26) 49.0 Omitting Li et al 5 1.27 (1.09−1.49) 64.0 Omitting Sand et al 5 1.28 (1.10−1.49) 59.0 Omitting Sun et al 5 1.26 (1.11−1.44) 63.0 Omitting Zhang et al 5 1.18 (1.10−1.26) 0 Omitting Zingel et al 5 1.26 (1.09−1.45) 64.0 IBD and AD 4 2.00 (0.96−4.13) 99.8 Omitting Aggarwa et al 3 1.94 (0.68−5.56) 92.7 Omitting Huang et al 3 2.43 (0.96−6.16) 98.6 Omitting Kim et al 3 2.45 (0.98−6.11) 99.2 Omitting Zhang et al 3 1.45 (0.93−2.27) 99.1 UC and AD 5 1.84 (0.93−3.60) 99.6 Omitting Aggarwa et al 4 1.56 (0.73−3.36) 82.5 Omitting Kim et al 4 2.11 (0.91−4.91) 99.6 Omitting Li et al 4 2.16 (0.95−4.87) 99.7 Omitting Sand et al 4 2.13 (0.92−4.91) 99.6 Omitting Zhang et al 4 1.44 (0.83−2.51) 99.7 CD and AD 5 1.35 (0.83−2.20) 78.7 Omitting Aggarwa et al 4 1.56 (0.72−3.39) 84.0 Omitting Kim et al 4 1.53 (0.69−3.36) 83.0 Omitting Li et al 4 1.52 (0.69−3.34) 83.0 Omitting Sand et al 4 1.61 (0.79−3.28) 80.0 Omitting Zhang et al 4 1.09 (0.99−1.19) 45.0 Note. AD, Alzheimer’s disease; CD, Crohn’s disease; CI, confidence interval; IBD, inflammatory bowel disease; RR, risk ratio; UC, ulcerative colitis.  下载: 导出CSV
下载: 导出CSV
Table 2. The Mendelian randomization analysis for the associations between IBD and dementia
Phenotype IBD UC CD IVW CAUSE IVW CAUSE IVW CAUSE OR (95% CI) P OR (95% CI) P OR (95% CI) P OR (95% CI) P OR (95% CI) P OR (95% CI) P Dementia 1.01
(0.98−1.03)0.657 0.99
(0.98−1.01)0.870 1.00
(0.98−1.03)0.841 1.01
(0.99−1.03)0.680 0.99
(0.97−1.02)0.562 1.00
(0.98−1.02)1.000 AD 0.98
(0.95−1.01)0.156 1.00
(0.97−1.03)1.000 1.00
(0.96−1.05)0.867 1.02
(0.99−1.06)0.410 0.99
(0.96−1.02)0.628 0.99
(0.96−1.02)0.800 AD-meta 1.00
(0.99−1.00)0.506 1.00
(0.996−1.004)1.000 1.01
(1.00−1.01)0.104 1.00
(0.996−1.004)1.000 1.00
(1.00−1.01)0.952 1.00
(0.997−1.003)1.000 VD 1.02
(0.97−1.07)0.446 1.00
(0.96−1.04)1.000 1.00
(0.94−1.05)0.857 1.01
(0.96−1.06)0.990 0.97
(0.92−1.01)0.163 1.00
(0.96−1.04)1.000 Note. CAUSE, causal analysis using summary effect; CD: Crohn’s disease; CI, confidence interval; IBD, inflammatory bowel disease; IVW, inverse-variance-weighted; OR, odds ratio; SNPs, single nucleotide polymorphisms; UC, ulcerative colitis.
下载: 导出CSV
Table 3. The genetic correlation and co-localization analyses for the associations between IBD and dementia
Phenotype IBD UC CD Genetic correlation Co* Genetic correlation Co* Genetic correlation Co* rg (se) P PPH4 rg (se) P PPH4 rg (se) P PPH4 Dementia −0.027 (0.022) 0.216 2.97% −0.043 (0.026) 0.096 4.00% −0.001 (0.021) 0.980 2.28% AD −0.016 (0.035) 0.645 2.29% −0.001 (0.042) 0.978 4.61% −0.020 (0.035) 0.569 1.95% AD-meta 0.005 (0.018) 0.781 1.28% −0.012 (0.023) 0.607 1.37% 0.013 (0.019) 0.504 2.75% VD 0.003 (0.037) 0.941 3.44% 0.014 (0.042) 0.734 3.02% 0.017 (0.036) 0.645 3.16% Note. *Co, co-localization analysis: the average value of PPH4 across all regions was used as the final co-localization result. CD, Crohn’s disease; CI, confidence interval; IBD, inflammatory bowel disease; SE, standard error; SNPs, single nucleotide polymorphisms; UC, ulcerative colitis.
下载: 导出CSV
-
[1] GBD 2017 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet, 2018; 392, 1859−922. doi: 10.1016/S0140-6736(18)32335-3 [2] GBD 2016 Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol, 2019; 18, 459−80. doi: 10.1016/S1474-4422(18)30499-X [3] DeTure MA, Dickson DW. The neuropathological diagnosis of alzheimer's disease. Mol Neurodegener, 2019; 14, 32. doi: 10.1186/s13024-019-0333-5 [4] Bellou V, Belbasis L, Tzoulaki I, et al. Systematic evaluation of the associations between environmental risk factors and dementia: an umbrella review of systematic reviews and meta-analyses. Alzheimers Dement, 2017; 13, 406−18. doi: 10.1016/j.jalz.2016.07.152 [5] Sims R, Hill M, Williams J. The multiplex model of the genetics of alzheimer's disease. Nat Neurosci, 2020; 23, 311−22. doi: 10.1038/s41593-020-0599-5 [6] Hodson R. Inflammatory bowel disease. Nature, 2016; 540, S97. doi: 10.1038/540S97a [7] Wilson JC, Furlano RI, Jick SS, et al. Inflammatory bowel disease and the risk of autoimmune diseases. J Crohns Colitis, 2016; 10, 186−93. doi: 10.1093/ecco-jcc/jjv193 [8] Lakhan SE, Kirchgessner A. Neuroinflammation in inflammatory bowel disease. J Neuroinflammation, 2010; 7, 37. doi: 10.1186/1742-2094-7-37 [9] Zhang B, Wang HE, Bai YM, et al. Inflammatory bowel disease is associated with higher dementia risk: a nationwide longitudinal study. Gut, 2021; 70, 85−91. doi: 10.1136/gutjnl-2020-320789 [10] Zingel R, Bohlken J, Kostev K. Association between inflammatory bowel disease and dementia: a retrospective cohort study. J Alzheimers Dis, 2021; 80, 1471−8. doi: 10.3233/JAD-210103 [11] Kim GH, Lee YC, Kim TJ, et al. Risk of neurodegenerative diseases in patients with inflammatory bowel disease: a nationwide population-based cohort study. J Crohns Colitis, 2022; 16, 436−43. doi: 10.1093/ecco-jcc/jjab162 [12] Li XJ, Sundquist J, Zöller B, et al. Dementia and alzheimer's disease risks in patients with autoimmune disorders. Geriatr Gerontol Int, 2018; 18, 1350−5. doi: 10.1111/ggi.13488 [13] Sun YH, Geng JW, Chen XJ, et al. Association between inflammatory bowel disease and dementia: a longitudinal cohort study. Inflamm Bowel Dis, 2022; 28, 1520−6. doi: 10.1093/ibd/izab300 [14] Davies NM, Holmes MV, Davey Smith G. Reading mendelian randomisation studies: a guide, glossary, and checklist for clinicians. BMJ, 2018; 362, k601. [15] Larsson SC, Traylor M, Malik R, et al. Modifiable pathways in alzheimer's disease: mendelian randomisation analysis. BMJ, 2017; 359, j5375. [16] Guo XZ, Chong L, Zhang X, et al. Letter to the editor: genetically determined IBD is associated with decreased risk of alzheimer's disease: a mendelian randomisation study. Gut, 2022; 71, 1688−9. [17] Jiang L, Li JC, Shen L, et al. Association between inflammatory bowel disease and alzheimer's disease: multivariable and bidirectional mendelian randomisation analyses. Gut, 2023; 72, 1797−9. doi: 10.1136/gutjnl-2022-327860 [18] Huang J, Su BW, Karhunen V, et al. Inflammatory diseases, inflammatory biomarkers, and alzheimer disease: an observational analysis and mendelian randomization. Neurology, 2023; 100, e568−81. [19] Morrison J, Knoblauch N, Marcus JH, et al. Mendelian randomization accounting for correlated and uncorrelated pleiotropic effects using genome-wide summary statistics. Nat Genet, 2020; 52, 740−7. doi: 10.1038/s41588-020-0631-4 [20] Austin-Zimmerman I, Levey DF, Giannakopoulou O, et al. Genome-wide association studies and cross-population meta-analyses investigating short and long sleep duration. Nat Commun, 2023; 14, 6059. doi: 10.1038/s41467-023-41249-y [21] Prince C, Sharp GC, Howe LD, et al. The relationships between women's reproductive factors: a mendelian randomisation analysis. BMC Med, 2022; 20, 103. doi: 10.1186/s12916-022-02293-5 [22] Hu JY, Lu JW, Lu QH, et al. Mendelian randomization and colocalization analyses reveal an association between short sleep duration or morning chronotype and altered leukocyte telomere length. Commun Biol, 2023; 6, 1014. doi: 10.1038/s42003-023-05397-7 [23] Zuber V, Grinberg NF, Gill D, et al. Combining evidence from Mendelian randomization and colocalization: review and comparison of approaches. Am J Hum Genet, 2022; 109, 767−82. doi: 10.1016/j.ajhg.2022.04.001 [24] Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ, 2021; 372, n71. [25] Schünemann HJ, Mustafa R, Brozek J, et al. GRADE Guidelines: 16. GRADE evidence to decision frameworks for tests in clinical practice and public health. J Clin Epidemiol, 2016; 76, 89−98. doi: 10.1016/j.jclinepi.2016.01.032 [26] Skrivankova VW, Richmond RC, Woolf BAR, et al. Strengthening the reporting of observational studies in epidemiology using mendelian randomisation (STROBE-MR): explanation and elaboration. BMJ, 2021; 375, n2233. [27] Lawlor DA, Harbord RM, Sterne JA, et al. Mendelian randomization: using genes as instruments for making causal inferences in epidemiology. Stat Med, 2008; 27, 1133−63. doi: 10.1002/sim.3034 [28] de Lange KM, Moutsianas L, Lee JC, et al. Genome-wide association study implicates immune activation of multiple integrin genes in inflammatory bowel disease. Nat Genet, 2017; 49, 256−61. doi: 10.1038/ng.3760 [29] Jansen IE, Savage JE, Watanabe K, et al. Genome-wide meta-analysis identifies new loci and functional pathways influencing alzheimer’s disease risk. Nat Genet, 2019; 51, 404−13. doi: 10.1038/s41588-018-0311-9 [30] Bulik-Sullivan B, Finucane HK, Anttila V, et al. An atlas of genetic correlations across human diseases and traits. Nat Genet, 2015; 47, 1236−41. doi: 10.1038/ng.3406 [31] Giambartolomei C, Vukcevic D, Schadt EE, et al. Bayesian test for colocalisation between pairs of genetic association studies using summary statistics. PLoS Genet, 2014; 10, e1004383. doi: 10.1371/journal.pgen.1004383 [32] Bernstein CN, Nugent Z, Shaffer S, et al. Comorbidity before and after a diagnosis of inflammatory bowel disease. Aliment Pharmacol Ther, 2021; 54, 637−51. doi: 10.1111/apt.16444 [33] Aggarwal M, Alkhayyat M, Abou Saleh M, et al. Alzheimer disease occurs more frequently in patients with inflammatory bowel disease: insight from a nationwide study. J Clin Gastroenterol, 2023; 57, 501−7. doi: 10.1097/MCG.0000000000001714 [34] Garcia-Argibay M, Hiyoshi A, Montgomery S. Association between dementia risk and ulcerative colitis, with and without colectomy: a Swedish population-based register study. BMJ Open, 2023; 13, e074110. doi: 10.1136/bmjopen-2023-074110 [35] Rønnow Sand J, Troelsen FS, Horváth-Puhó E, et al. Risk of dementia in patients with inflammatory bowel disease: a Danish population-based study. Aliment Pharmacol Ther, 2022; 56, 831−43. doi: 10.1111/apt.17119 [36] Fu PF, Gao M, Yung KKL. Association of intestinal disorders with parkinson's disease and alzheimer's disease: a systematic review and meta-analysis. ACS Chem Neurosci, 2020; 11, 395−405. doi: 10.1021/acschemneuro.9b00607 [37] Liu MS, Li DX, Hong X, et al. Increased risk for dementia in patients with inflammatory bowel disease: a systematic review and meta-analysis of population-based studies. Front Neurol, 2022; 13, 813266. doi: 10.3389/fneur.2022.813266 [38] Liu NY, Wang Y, He LY, et al. Inflammatory bowel disease and risk of dementia: an updated meta-analysis. Front Aging Neurosci, 2022; 14, 962681. doi: 10.3389/fnagi.2022.962681 [39] Zamani M, Ebrahimtabar F, Alizadeh-Tabari S, et al. Risk of common neurological disorders in adult patients with inflammatory bowel disease: a systematic review and meta-analysis. Inflamm Bowel Dis, 2024; izae012. [40] Zhang MN, Shi YD, Jiang HY. The risk of dementia in patients with inflammatory bowel disease: a systematic review and meta-analysis. Int J Colorectal Dis, 2022; 37, 769−75. doi: 10.1007/s00384-022-04131-9 [41] Yuan S, Dan LT, Zhang Y, et al. Digestive system diseases, genetic risk, and incident dementia: a prospective cohort study. Am J Prev Med, 2024; 66, 516−25. doi: 10.1016/j.amepre.2023.10.017 [42] Raskov H, Burcharth J, Pommergaard HC, et al. Irritable bowel syndrome, the microbiota and the gut-brain axis. Gut Microbes, 2016; 7, 365−83. doi: 10.1080/19490976.2016.1218585 [43] Osadchiy V, Martin CR, Mayer EA. The gut-brain axis and the microbiome: mechanisms and clinical implications. Clin Gastroenterol Hepatol, 2019; 17, 322−32. doi: 10.1016/j.cgh.2018.10.002 [44] Mayer EA. Gut feelings: the emerging biology of gut-brain communication. Nat Rev Neurosci, 2011; 12, 453−66. [45] Bonaz BL, Bernstein CN. Brain-gut interactions in inflammatory bowel disease. Gastroenterology, 2013; 144, 36−49. doi: 10.1053/j.gastro.2012.10.003 [46] Sampson TR, Debelius JW, Thron T, et al. Gut microbiota regulate motor deficits and neuroinflammation in a model of parkinson's disease. Cell, 2016; 167, 1469-80. e12. [47] Rea K, Dinan TG, Cryan JF. The microbiome: a key regulator of stress and neuroinflammation. Neurobiol Stress, 2016; 4, 23−33. doi: 10.1016/j.ynstr.2016.03.001 [48] Quigley EMM. Microbiota-brain-gut axis and neurodegenerative diseases. Curr Neurol Neurosci Rep, 2017; 17, 94. doi: 10.1007/s11910-017-0802-6 [49] Fang P, Kazmi SA, Jameson KG, et al. The microbiome as a modifier of neurodegenerative disease risk. Cell Host Microbe, 2020; 28, 201−22. doi: 10.1016/j.chom.2020.06.008 [50] Lavelle A, Sokol H. Gut microbiota-derived metabolites as key actors in inflammatory bowel disease. Nat Rev Gastroenterol Hepatol, 2020; 17, 223−37. doi: 10.1038/s41575-019-0258-z [51] Wang XY, Sun GQ, Feng T, et al. Sodium oligomannate therapeutically remodels gut microbiota and suppresses gut bacterial amino acids-shaped neuroinflammation to inhibit alzheimer's disease progression. Cell Res, 2019; 29, 787−803. doi: 10.1038/s41422-019-0216-x [52] Piovani D, Danese S, Peyrin-Biroulet L, et al. Environmental risk factors for inflamm bowel dis: an umbrella review of meta-analyses. Gastroenterology, 2019; 157, 647-59. e4. [53] Narula N, Wong ECL, Dehghan M, et al. Association of ultra-processed food intake with risk of inflammatory bowel disease: prospective cohort study. BMJ, 2021; 374, n1554. [54] Więckowska-Gacek A, Mietelska-Porowska A, Wydrych M, et al. Western diet as a trigger of alzheimer's disease: from metabolic syndrome and systemic inflammation to neuroinflammation and neurodegeneration. Ageing Res Rev, 2021; 70, 101397. doi: 10.1016/j.arr.2021.101397 -

 点击查看大图
点击查看大图
计量
- 文章访问数: 395
- HTML全文浏览量: 163
- PDF下载量: 31
- 被引次数: 0

 Quick Links
Quick Links